Embed Size (px)
Citation preview

www.mghcme.org
Thomas J. Spencer, MD Massachusetts General Hospital
Harvard Medical School
Stimulant Treatment of Pediatric ADHD

www.mghcme.org
2
Disclosures
Dr. Spencer receives research support from Royalties and Licensing fees on copyrighted ADHD scales through MGH Corporate Sponsored Research and Licensing.
Dr. Spencer has a US Patent Application pending (Provisional Number 61/233. 686), through MGH corporate licensing, on a method to prevent stimulant abuse.

www.mghcme.org
3 nida.gov

www.mghcme.org 4
Effects of Methylphenidate (3 mg/kg i.p.) on Extracellular Levels of Monoamines in the Rat Prefrontal Cortex
Time in hours
-1 0 1 2 3 4
% B
ase
line
0
50
100
150
200
250
300
350
400 Dopamine Norepinephrine
Methylphenidate 3 mg/kg i.p.
*=P<0.05 versus baseline
* *
From Bymaster et al., Neuropsychopharmacology, 2002

www.mghcme.org
Mechanism of Action MPH: Insights from PET Imaging Studies
(Volkow et al. J Att Dis. 2002;(suppl)1)
– Because DA enhances task-specific neuronal
signaling and decreases noise, MPH-induced
increases in DA could improve attention and
decrease distractibility
– Since DA modulates motivation, the increases in
DA would also enhance the saliency of the task
facilitating the “interest it elicits” and thus
improving performance

www.mghcme.org 6
Superior Parietal Cortex
DLPFC
DLPFC
Dorsal ACC
VLPFC
Methylphenidate (Concerta) Increases dACC & DLPFC fMRI Activation in ADHD during MSIT
Bush et al. AGP - 2008
Concerta (N=11) vs Placebo (N=10)

www.mghcme.org
7
ADHD Practice Parameters. JAACAP 1997;36:85S. Zametkin and Ernst. N Eng J Med 1999;340:40.
In ADHD Stimulants Found to Improve
• Inattention
• Impulsivity
• Hyperactivity
• Noncompliance
• Impulsive aggression
• Social interactions
• Academic efficiency
• Academic accuracy
AND Core Symptoms

www.mghcme.org 8
ADHD and Methylphenidate: Dose Effects on Attention in Clinic and Classroom
15
25
35
45
55
65
placebo 5 10 15 20
Wee
kly
T-Sc
ore
Methylphenidate Dose
CPT
ADHD Comprehensive Teachers Rating Score
% Academic Efficiency
% On Task
Rapport, et al. 1987

www.mghcme.org
––– CC ––– Beh ––– MedMgt ––– Comb
Parent Teacher
Assessment Point (Days)
0
0.5
1
1.5
2
2.5
3
0 100 200 300 400
0
0.5
1
1.5
2
2.5
3
0 100 200 300 400
MTA: Treatment Effects on Inattention Scores (SNAP) [MTA Group, Arch General Psychiatry, 1999]
Ave
rage
Sco
re
Ave
rage
Sco
re

www.mghcme.org 10
Effectiveness Factors in MTA Randomized Treatment Groups on Meds
Variable
MedMGt (n=131)
CC Group (n=94)
t value P
Severity CTQ-Total
52.4(17.4) 51.1 (16.6) -0.65 NS
% Time on MPH
89.0 (28.3) 41.1 (39.7) -11.70 <.0001
Average doses/day
2.9 (0.4) 2.1 (0.6) -11.61 <.0001
Total Daily Dose
32.8 (12.9) 18.7 (12.8) -7.75 <.0001
Total Visits 10.3 (4.3) 2.7 (3.5) -16.07 <.0001
Months on MPH
9.9 (3.9) 5.5 (5.4) -7.58 <.0001

www.mghcme.org
Indirect Effects of Medication on Parents, Teachers and Peers
(Barkley et al., Cunningham et al.)
• Social changes in Parents and Teachers • (Barkley et al., Pelham et al., Whalen et al.)
– Decreased rate of commands and degree of supervision
– Increased praise and positive responsiveness
• Social changes in Peers • (Cunningham et al., Whalen et al.)
– Decreased negative and aggressive behavior on stimulants
– Leads to greater acceptance by peers
– Leads to further positive benefit to the child

www.mghcme.org

www.mghcme.org
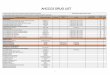
Methylphenidate (MPH) in ADHD: Optimizing Dosing
*May exceed FDA approved dose. Wilens TE, et al. Postgrad Med. 2010;122(5):97-109. www.drugs.com.
Medication StartingDoseMaximumDose*UsualDosing
Duration
RitalinIR® 5mgQD/BID 2mg/kg/day 4hr/BID
Focalin® 2.5mgQD/BID 1mg/kg/day 4–5hr/BID–TID
FocalinXR® 5mgQD 1mg/kg/day 10–12hrQD
Daytrana® 10mg
6–16hr
Concerta® 18mgQD 2mg/kg/day 12hr/once
MetadateCD® 20mgQD
8hr/once
RitalinLA® 20mgQD
8hr/once
Quillivant® <10mgQD
12hr/once
Quillichew™ <10mgQD
8hr/once
AptensioXR 10mgQD
12hr/once

Long Acting MPH formulations

www.mghcme.org
Bioavailability from two MPH extended-release formulations . Gonzalez et al. Int J Clin Pharmacol Ther 40(4):175–184

MPH ER Individual PK Plots
0
5
10
15
20
0 2 4 6 8 10
Co
nc (
ng
/mL
)
Time (hrs)

www.mghcme.org
Pharmacological Dissociation Between The Robust Effects Of Methylphenidate On ADHD Symptoms And Weaker Effects On Working Memory
Biederman et al. Eur Neuropsychopharmacol 2011

www.mghcme.org
Amphetamine (AMPH) in ADHD: Optimizing Dosing
*May exceed FDA approved dose (eg, > 20 to 30 mg/day). Wilens TE, et al. CNS News. 2007. Wilens TE, et al. Postgrad Med. 2010;122(5):97-109. www.drugs.com.
Medication Starting Dose Maximum Dose*
Usual Dosing Duration
Adderall® 2.5–5 mg QD 1.5 mg/kg/day 6 hr / BID
Adderall XR® 2.5–5 mg QD 12 hr / QD
Vyvanse® 30 mg QD 12–14 hr / QD
Dexedrine Tablets® 2.5–5 mg BID 1.5 mg/kg/day 3–5 hr / BID–QID
Evekeo® 2.5–5 mg BID 3–5 hr / BID–QID
Dexedrine Spansule® 5 mg QD 6 hr / QD–BID
Dyanavel XR™
(suspension) 2.5–5 mg QD 1.5 mg/kg/day 12 hr / QD
Adzenys XR™ (disintegrating tab)
6.3–12.5 mg QD Not established 12 hr / QD

www.mghcme.org 19
Best Response
(Percent)
Dextroamphetamine Methylphenidate Equal response to either stimulant
Meta-analysis of Within-Subject Comparative Trials Evaluating Response to Stimulant Medications
0
10
20
30
40
25% 23%
52% 50 6 studies N=274
Spencer et al. Arch of Gen Psych 2001

www.mghcme.org
MAS XR Efficacy: Academic Productivity
Randomized, Double-Blind, Placebo-Controlled Study
Placebo
MAS 10 mg
MAS XR 30 mg
MAS XR 10 mg
MAS XR 20 mg
McCracken JT, et al. J Am Acad Child Adolesc Psychiatry. 2003;42(6):673-683.
Number of Math Problems Completed Correctly
40
60
80
100
120
140
0.0 1.5 3.0 4.5 6.0 7.5 9.0 10.5 12.0
Time Postdose (h)
PER
MP
Nu
mb
er C
orr
ect
N = 49

www.mghcme.org
21
-10
-5
0
5
10
15
Adderall XR Study in Youth with ADHD: CGIS-T Mean Total Score Afternoon
Placebo Add XR
10 mg
Add XR
20 mg
Add XR
30 mg
Baseline
Endpoint
Change
ITT Population
* *
* *P<0.001 (Dunnett test compared to placebo following ANCOVA with baseline score as covariate)
-1.2
-5.4 -6.8 -7.2
(Biederman et al., Pediatrics 2003)

www.mghcme.org
22
LDX Chemistry
LDX
Site of cleavage
l-lysine d-amphetamine
H N 2
O
N H
NH 2
CH 3 H N 2
O
OH
NH 2
H N 2
CH 3

www.mghcme.org
LDX Extraction, Pharmacokinetic and Abuse Liability Studies: Results
• Amphetamine is very difficult to extract from LDX prodrug
• Intravenous administration does not result in appreciable serum amphetamine levels in rat and human studies
• Intranasal administration does not result in appreciable serum amphetamine levels in rat and human studies
• Apparent “saturation” of LDX in gut limits ultimate serum amphetamine levels (e.g., overdose implications)
• Marginally less likeability in human studies
Jasinski D, et al. Posters presented at CPDD Meeting, June, 2006, Scottsdale, AZ.; Biederman J, et al. Poster presented at Annual APA Meeting, May 24, 2006, Toronto, Ontario, Canada. Boyle L, et al. Presented at NCDEU, June 12-15, 2006, Boca Raton, FL.

www.mghcme.org
0.0
0.5
1.0
1.5
2.0
2.5
3.0
1.0 2.0 3.0 4.5 6.0 8.0 10.0 12.0 1.0 2.0 3.0 4.5 6.0 8.0 10.0 12.0
LDX Adderall XR Placebo
LDX : Duration of Action SKAMP Time Course
LS
Mean S
KA
MP
Score
* * * * * *
* ** ** ** ** ** **
**
*P < .0001, **P < .01, LDX and Adderall XR vs placebo;
LS = Least Square.
Postdose (h)
N=50

www.mghcme.org
25
Adverse Effects of Stimulants
• Adverse effects (AEs) are similar for all stimulants
- Decreased appetite
- Insomnia
- Headache
- Stomachache
- Irritability/rebound phenomena
• Rates of these “Aes” may be high prior to any medical intervention; thus, baseline levels should always be obtained
Wilens T, Spencer T. In: Child and Adolescent Psychiatric Clinics of North America. Philadelphia, Pa:
Saunders Press; 2000:573-604.

Blood Pressure and Heart Rate
Over 10 Years in the MTA
(Vitiello et al. JAMA 2012)
No significant treatment-by-time effect was observed on systolic or diastolic blood pressure.
A significant treatment-by-time effect was observed on heart rate (p=0.02), with significantly higher mean heart rates in the groups receiving medication at 14 months, but not afterward.

Cooper et al. 2011 NEJM

www.mghcme.org
Gutgesell H, et al. Circulation. 1999:99:979-982.
Schubiner H, et al. J Atten Disord. 2006;10:205-211.
Screening for Cardiac Risk: AHA Guidelines
• Medical history − Personal congenital or acquired cardiac disease history
− Family history of cardiac disease (<50 years of age)
− Palpitations, chest pain, fainting, seizures, post-exercise symptoms
− Ask about other medications (including OTC)
• Routine medical exam
• Monitor BP and pulse at baseline and follow-up, especially in adults
• ECG is reasonable but not mandatory
• Routine check of Holter, ECHO is not necessary

29
-2
-1
0
1
Year Prior to Tx First Year Tx Second Year Tx Third Year Tx
Boys (n = 68)
Girls (n = 16)
Growth Over Time in Children Treated With MPH
Lisska MC, Rivkees SA. J Pediatr Endocrinol Metab. 2003;16:711-718.
Gro
wth
Vel
oci
ty Z
Sco
res
Duration of Tx

30
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 25
Stimulant Treated
Not Stimulant Treated
Onset of Tic Disorders in ADHD Probands Stratified by Stimulant Treatment
Age in Years (Spencer et al., Arch Gen Psych, 1999)

31
0
5
10
15
20
25
0 1 2 3 4 5 6 7 8 9 10
Time (hrs)
Feel
an
Eff
ect
IR-MPH
OROS-MPH
Feel an Effect (average±SEM)
a
a
a b
a p < 0.05 b P < 0.01
Spencer, Biederman et al. Am J Psych 2006.
a

www.mghcme.org
32
Early ADHD Treatment Reduces Marijuana Use
Population risk
Stimulant use started prior to 9 years of age
Stimulant use started between 10-14
years of age
Stimulant use started after 15 years of age
20% 30% 40% 50% 60%
Past Year Use
15 year follow-up study (N=40,358; 10% with ADHD)
* p<0.001 vs controls
*
*
McCabe, West, Dickinson, Wilens. J Am Acad Child Adoles Psych 2016: 55:479-486

33
Protective Effect of Stimulants on Comorbidity
Biederman et al. Pediatrics. 2009.
2(1) = 19.7, p < 0.001 2
(1) = 17.8, p < 0.001
2(1) = 3.5, p = 0.063

34
Psychostimulant Treatment and the Developing Cortex in ADHD
Shaw et al 2009

www.mghcme.org
PI: Thomas Spencer, MD
Sarah Kassabian, at (617) 726-0481 [email protected].
FDA PK/PD Classroom Study