Embed Size (px)
Citation preview

NESC – incorporating Oxford and Wessex Deaneries NHS Education South Central (NESC) is part of the South Central Strategic Health Authority
Strategy for Clinical Simulation Training
2008 - 2011

Version C
Page 1 of 24
Executive Summary
This paper describes how NHS South Central has arrived at its current position with regard to clinical simulation training and its plans to develop it further. NESC is committed to providing high quality and relevant training to its staff; training that meets the changing needs of the NHS but also results in measurable improvements in patient care and safety.
The key drivers for increased use of simulation training across the South Central region include: Modernising Medical Careers (MMC), the European Working Time Directive (EWTD), service redesign, revalidation of existing clinicians and of course, the continuous improvement of patient care. Clinical simulation training has been used for decades and is becoming an accepted part of training curricula. The advantages of using simulation scenarios are considerable and include: a risk-free environment for improving patient safety, a realistic but safe environment in which practitioners can review, repeat and reassess their performance without compromising patient safety and the ability to plan training sessions in advance hence students do not need to wait for a particular emergency to present.
A workshop which included approximately 50 delegates from across the region identified NHS South Central’s priorities for investment as: training, staffing, facilities and equipment. Investment in these areas would allow us to develop a pool of trainers which would help to achieve widespread implementation of simulation training across the South Central region in a cost-effective manner. Investment should also be based on reducing identified risks to patients and it was agreed that implementation of simulation should focus initially on those areas in which it can maximise benefits and also in acknowledged high risk situations, for example, the rapidly deteriorating patient. Our strategy outlines the activities and actions that will support these objectives and considers the resources available to deliver them; it addresses future workforce need while ensuring high quality education and value for money.
Prof Lord Ara Darzi: “We need to do more to grasp the potential of education as a lever for service improvement”

Version C
Page 2 of 24
Contents
Introduction
4
What is simulation training?
5
Key drivers: why do we need simulated training
5
Vision
7
Background Use of simulation in healthcare Simulation training in the UK Simulation training in NHSSC
Audit Workshop Critical success factors
Allocation of funds 2008/9 Development plans Priorities
7 7 8 8 8 9 9 10 10 11
National Patient Safety Agency
11
Implementation of simulation training Who What How
13 15 15
Recommendations
16
References
18
Appendix one: Summary of Workshop Findings
19

Version C
Page 3 of 24
Introduction
NHS Education South Central [NESC] was established in April 2007 as part of South Central SHA’s long term aspirations to support the development of health staff in order to attract and retain outstanding clinicians, managers and health workers.
NESC was established with the purpose of creating learning and development opportunities, realizing potential and achieving excellence for all. This emphasis on training and education is crucial if the SHA is to achieve its long term aspirations to improve the health of its population, reduce health inequalities and enhance patient safety.
The mission for NESC is to provide high quality and relevant training where and when it is needed, that meets the changing needs of the NHS and our workforce and leads to measurable improvements in patient care.
NESC includes the Wessex and Oxford Deaneries which are responsible for delivering clinical postgraduate education for doctors, dentists and consultant practitioners to ensure they are competent and fit to practice. The Deaneries also implement national policy on modernising clinical careers and health care, and promote access to inter-professional and multi-professional education.
The Education Commissioning Team within NESC works with a range of education providers and health care organisations to commission education and training programmes and practice learning for nurses and health care professionals across a wide range of undergraduate programmes. By doing so, it aims to prepare sufficient numbers of health care staff with the appropriate skills to provide the range and quality of services demanded by the local health community within a changing clinical landscape.
NESC is striving to develop innovative and effective educational and training solutions which enable us to respond to the changing needs of the health economy and ensure our workforce are highly competent and fit for purpose. Our strategy addresses future workforce need; ensures high quality education and provides value for money.
As part of this vision we are aiming to develop an integrated approach to simulation training which
builds on the expertise already available in the region; encourages a multi-professional approach to
learning and development ; uses research methodologies to evaluate the effectiveness of simulation
training and provides funding for the longer term to support the training requirements for Trusts and
PCT’s. Our target audience is primarily junior doctors in training, dentists in training, nurses,
midwives and AHP’s.

Version C
Page 4 of 24
What is simulation training? Professor David Gaba (2004) offers the following definition of simulation training “Simulation is a technique—not a technology—to replace or amplify real experiences with guided experiences that evoke or replicate substantial aspects of the real world in a fully interactive manner. While two of our own South Central practitioners suggest that:
“In its broadest sense, simulation can include the use of role play, simulated patients, part-task trainers, virtual reality devices (usually with haptic - or tactile - feedback) and electronic manikins (controlled either by humans - e.g. SimMan - or with full physiological and pharmacological computer control - METI HPS). All of these can be used alone or in combination to produce simulated scenarios”. Professor Gary Smith, TEAM Centre, Portsmouth Hospitals Trust.
“Simulation is doing or experiencing something in a way that resembles reality. Medical simulation may involve individuals or groups of healthcare professionals and simulators are the tools with which we create the simulation." Dr Helen Higham, OxSim, Oxford Radcliffe Hospitals Trust.
Key Drivers: why do we need simulation training?
The Calman Report (1993) began the changes in junior doctors’ training by placing the endpoint of training as the achievement of competence and by placing the burden of proof onto trainees and trainers to demonstrate achievement of competence.
This was followed in 2005 by Modernising Medical Careers (MMC), an initiative which radically changed the way we train doctors; the speed and quality with which we do it and the end product of that process. It examines the opportunities for streamlining training and increasing flexibility.
Another big change that will impact doctors training is the European Working Time Directive (EWTD) which comes into effect in August 2009. This reduction in the number of hours and patient experiences has forced NESC to think about how to provide effective training i.e. achieve competence and has therefore increased the requirement for formal work-based assessment as part of training programmes.
In Lord Darzi’s report; Next Stage Review: A High Quality Workforce, it specifically references the use of simulation type training;

Version C
Page 5 of 24
“We need to use modern education techniques if we are to fulfil our ambition to widen participation in learning and to enhance the learning environment for those both in training and those undertaking CPD. We will therefore review the appropriate use of e-learning and other modern education techniques, such as high-fidelity simulation suites, to develop a strategy for the appropriate use of e-learning, simulation, clinical skills facilities and other innovative approaches to healthcare education”.
The White Paper; Building a Health Service fit for the future (2005) describes a fundamental shift in ways of working to ensure care is quicker, more personal and closer to home, it stresses the need to reduce inequality, improve patient safety and develop new clinical roles. In addition, patients are becoming less willing to allow inexperienced staff to practise on them. According to the National Patient Safety Agency (NPSA), patient accidents, incidents associated with treatments or procedures and medication incidents were most commonly reported with communication factors and lack of teamwork being cited as major contributing factors. The composition and skills of the healthcare workforce must respond to these changes in demand and in clinical practice; additionally today, many patients having surgical procedures spend less time in hospital resulting in reduced availability of patients for traditional bedside teaching.
Safer patient care can be achieved by informing, supporting and influencing healthcare practitioners and organisations, for example: The National Patient Safety Agency (NPSA) recently issued a patient safety alert requiring all healthcare organisations to implement the WHO Surgical Safety Checklist for every patient undergoing a surgical procedure. The checklist was piloted during a twelve month period in eight countries, including St Mary’s Hospital in London, which saw surgical deaths and complications reduce by one third when the checklist was used. Lord Darzi, who chaired a WHO working group that played a key role in developing the Safe Surgery Checklist in 2008, said: “The beauty of the surgical safety checklist is its simplicity and – as a practising surgeon – I would urge surgical teams across the country to use it. Operating theatres are high-risk environments. By using the checklist for every operation we are improving team communication, saving lives and helping ensure the highest standard of care for our patients”. This resulted in a patient safety alert for the NHS issued in 2009.
In addition, over the next few years, the General Medical Council (GMC) and the General Dental
Council (GDC) will be changing the way doctors and dentists within the UK are regulated to practise
medicine and dentistry. Revalidation is the process where they will have to demonstrate regularly to
the GMC and GDC that they are fit to practice medicine; clinical simulation training is a useful method
of demonstrating and evaluating competence. Simulation training may also be used to equip staff with
the skills they need to take on new roles under service
redesign and it allows the trainees to develop and practice new skills in a safe and constructive environment.

Version C
Page 6 of 24
Vision That all staff in NHS SC should have routine and timely access to appropriate simulated clinical environments as part of induction, training, continuing professional development and assessment to reduce risks to patients and increase confidence and competence. This may range from simulated simple clinical interventions involving little additional equipment to total immersion with highly sophisticated high fidelity manikins in a replica clinical environment (e.g. ward, theatre, whole department). Where feasible, simulation should involve whole teams and simulated patients, so that the technical aspects are simulated in a ‘real life’ scenario allowing interaction and feedback.
Background 1. Use of simulation in healthcare Simulation training has been used for decades and has become increasing sophisticated. The medical and dental professions have traditionally used cadaveric materials and dental trainees have used phantom heads since the early twentieth century and basic simulation training for Basic Life Support (BLS) and Advanced Life Support (ALS) is ubiquitous and well established. The advantages of simulation scenarios are considerable and include first and foremost a risk-free environment for improving patient safety. It provides students and trainees with a realistic but safe environment which can help practitioners move from theory to practice and allows them to review, repeat and reassess their performance without compromising patient safety. Simulation training can be planned in advance and students do not need to wait for a particular emergency to present. It allows access to a wide variety of cases and simulates rare complications; it also allows objective assessment of student’s performance and is incorporated into some training curriculums already. “Simulation offers a safe environment within which learners can repeatedly practise a range of clinical skills without endangering patients. Comprehensive simulated environments allow a move away from isolated tasks to more complex clinical situations, recreating many of the challenges of real life”. Kneebone et al.
2. Simulation training in the UK Simulated training scenarios have been used in the aviation industry for more than 20 years and there is evidence that, when integrated into a managed educational programme, simulation is an effective way to learn from errors in a safe environment. In healthcare High Fidelity Simulation centres first appeared in the UK during the late 1990s and the number of centres is increasing steadily. The National Association of Medical Simulators (NAMS) now has 15 members from NHS Trusts. Simulation training is becoming an accepted part of training curricula allowing maximum educational opportunities in clinical skills units and helping to address reduced training time. Following publication

Version C
Page 7 of 24
of the Nursing and Midwifery Council (NMC) Simulation and Practice Learning project in December 2007 (NMC 2007) there are two main recommendations that can be implemented within the Pre-registration Nursing curriculum from September 2008:
� Simulated learning opportunities within an audited simulated practice learning environment
(skills suites) will be incorporated across all 4 branches of the pre-registration undergraduate nursing programmes
� Simulation and practice learning will be used to provide clinical training in support of providing
direct care in the practice setting; a maximum of up to 300 hours of simulated and practice learning hours may be used in support of direct care hours during the complete nursing programme. This will contribute to the NMC requirement to complete a minimum of 2300 direct care hours within the Pre-Registration Nursing Programme
3. Simulation training in NHS South Central In early 2008 NESC formed a Clinical Simulation Training steering group. The main purpose of this group was to examine how NESC could develop an integrated approach to simulation training, building on the expertise that is already available in the region.
Audit of facilities An initial audit of NHS Trusts and PCTs was undertaken during June 2008 to establish existing current capacity for simulation training and a needs analysis to get a better understanding of the range and volume of simulation training required in the South Central region.
The audit showed that clinical simulation training is currently provided by all individual Trusts including Higher Education Institutions (HEI) facilities within Trusts but not routinely by PCTs. It demonstrated that there are specialised centres of excellence but there may also be duplication of effort and investment where Trusts and HEIs operate independently. (The audit did not specifically include all HEIs but where these operate in Trust premises they were included.)
In addition, the audit exercise revealed that there was a wide disparity amongst Trusts across South Central regarding availability of simulation training. Some areas were already well resourced and routinely providing training in high fidelity simulation suites while other trusts had little more than a basic resuscitation department.
Investment Priorities Workshop In July 2008, all NHS Trusts and PCTs from across the region were invited to send a nominee to attend a one-day workshop to identify priorities for investment in clinical simulation training. Approximately 50 people attended from 16 South Central Trusts, PCTs and HEIs. Attendees included Anaesthetists and Surgeons, Dentists, Post Graduate Centre

Version C
Page 8 of 24
and Human Resources Managers, Tutors, SHA Quality and Education/ Commissioning and Deanery and NESC Leads. (Appendix One – Summary of Workshop Findings) The following critical success factors were identified:
� A clear definition of what is meant by simulation training to ensure that both low and high fidelity training is included
� Identification of funding streams i.e. to ensure adequate and equitable funding and efficient use of resources
� Clear plans for training i.e. Train the Trainers etc in both educational theory and practice ensuring this is applied in the clinical simulation setting
� Establish communication networks for sharing g of good practice and best use of limited resources
� Effective partnerships and understanding of shared priorities for investment between PCTs, NESC, HEIs and Trusts
� Applied research and evaluation i.e. evidence based approach to simulation skills education and training to be used with specific research commissioned if required
� Ensure we are training and educating the people with the right skills mix and in the right numbers to support the planned changes in service delivery
� Develop a partnership approach across South Central � Achieve a basic level of simulation training for all Trusts before developing centres
of expertise
Four main priorities for investment emerged from the workshop: equipment, facilities, staffing and training. When delegates were asked what aspect of simulation training was the most important; training was clearly identified as the number one concern. N =(51)
Funding Priority N %
Equipment 2 4
Facilities 4 8
Staffing 12 23
Training of trainers 33 66
4. Allocation of Development Funds 2008/9 Following the workshop, bids were invited from all NHS Trusts and PCTs across NHSSC to provide a minimum standard of simulation training, equipment, facilities and staffing. Principles for allocation were agreed and following a rigorous bid process the NESC Senior Management team approved a total of £1,287,000 to be allocated to 8 South Central Trusts and two Primary Care Trusts; of which £622,780 was invested in Equipment, £170,720 in Staffing and £493,500 in facilities and development.

Version C
Page 9 of 24
5. Developing plans for 2009/10 onwards 5.1 A small advisory group comprising individuals from across South Central with detailed experience and expertise in simulation training has met to consider the key areas for a simulation strategy. 5.2 Intended benefits to patients:
� Higher patient safety and satisfaction, fewer complaints, more comfortable caring interventions
� Calmer, more effective clinicians, especially in an emergency situation � Clinicians communicating more clearly with each other and with supporting staff,
improved teamwork and higher levels of accountability � Fewer cancelled or repeat procedures as clinicians get things right first time more
often Intended benefits to staff
� Safer training environment � Supportive, non-threatening experience � Reduced working hours and time, fewer cancelled or repeat procedures as clinicians
get things right first time more often

Version C
Page 10 of 24
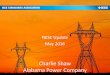
Priorities It was agreed that implementation of simulation training should focus initially on areas with potential to maximize benefits and in acknowledged high risk situations, for example, identifying and managing the rapidly deteriorating patient. In addition, in high risk situations, while individual expertise is vital in ensuring the right diagnosis and giving the right treatment, it is a good healthcare team that reduces the chance that patients will be harmed through error and it is for this reason that the NPSA is encouraging continued improvements in teamwork because the benefits can be felt by everyone. In fact, according to the NPSA, a lack of teamwork is frequently cited as a major contributing factor in untoward incidents. During the period: July 2007 – June 2008 more than 800,000 patient safety incidents were reported to NPSA, of those 11,369 resulted in severe harm or death (see table and chart below).
National Patient Safety Agency
Incident type Severe Death Total
Other 654 1615 2269
Treatment, procedure 1315 373 1688
Patient accident 1254 177 1431
Infection control incident 753 322 1075
Self-harming behaviour 393 472 865
Implementation of care and ongoing monitoring/review 697 116 813
Access, admission, transfer, discharge 616 152 768
Clinical Assessment 478 128 606
Infrastructure 418 39 457
Medication 373 51 424
Consent, communication, confidentiality 239 38 277
Medical device/equipment 210 40 250
Disruptive, aggressive behaviour 208 19 227
Documentation 125 12 137
Patient abuse (by staff or third party) 63 19 82
Total 7796 3573 11369
* The incidents highlighted in yellow, a total of 6,269, is more than half of the total number of serious incidents and are those most likely to benefit from effective clinical simulation training.

Version Control code
Page 1 of 24
National Patient Safety Agency - Incidents reported resulting in severe harm or death
(1 July 2007 to 30 Jun 2008)
0
500
1000
1500
2000
2500
Other
Trea
tmen
t, proc
edure
Patie
nt acc
iden
t
Infection co
ntrol inc
iden
t
Self-ha
rming be
haviou
r
Implem
entatio
n of care an
d on
going mon
itorin
g/review
Acce
ss, a
dmission
, trans
fer, disc
harge
Clin
ical A
sses
smen
tInfra
structure
Med
ication
Con
sent, c
ommun
ication, con
fiden
tiality
Med
ical dev
ice/eq
uipm
ent
Disruptive, agg
ress
ive be
haviou
rDoc
umen
tatio
n
Patie
nt abu
se (b
y staff o
r third party)
Incidents
Number of Incidents
Severe
Death
Total

Version C
Page 1 of 24
Implementation of simulation training It is proposed that NESC focus on the following areas: 1. Who
1. Recent graduates who are new to independent clinical practice: F1 and F2 doctors, DF1 and DF2 dentists, nurses and AHPs in Preceptorship who are at a critical stage in development. 2. Induction/return to work programmes in the NHS for overseas trained practitioners and those returning after a break in clinical practice. 3. Trainees and other clinicians with particular learning needs (e.g. trainees undergoing a period of targeted training and established clinicians undertaking remedial training). Medical and Dental Training Numbers 2009
Profession
Number training in
South Central per year
Current
number of days simulation
training (approx)
Current
cost per day per person (approx)
Foundation Doctors Y1
390 Variable From a half day –
3 days
£200
Foundation Doctors Y2
222 Variable From a half day –
3 days
£200
Vocational Dental Posts
39 3-5 days
£200
MMC ST1-2 428 tbc
MMC ST3-7 134 tbc
MMC GPs 1-3 423 tbc
Dental SHOs 20 1 day £200
Dental SPRs 7 1 day £200
Overseas trained Drs
40
Return to work Doctors
Overseas trained Dentists
32 2 days £200
Return to work Dentists
2-3 yr 3-4 days £500

Version C
Page 2 of 24
* Data obtained from South Central Strategic Health Authority: Madel Student training Numbers
Non Medical Education Commissioning 2009
Profession
Number training in South Central
Current number of hours
simulation training (approx)
Current cost
per day/per person (approx)
Allied Health Professionals
504
Variable from 0 to 16
hours
£200
Dental Therapy 34 tbc £200
Dental Nurses 45 tbc £200
Operating department Practitioners
49
Pre-reg Pharmacy 36
Pharmacy techs 29
NURSING
Adult Nursing 903 150 £125
Child Nursing 133 150
Learning Disability Nursing
57 tbc
Mental health Nursing
175 tbc
Thorn Mental Health
28
Midwifery – 3yr 160 150
Midwifery 18 month
32
Total number of trainees per year (non-medical)
2185
* Data obtained from South Central Strategic Health Authority
The table above shows the non-medical undergraduate education commissioning numbers by profession for 2009. The majority of training courses are 3 years in length therefore these numbers (approximately) will out turn in 2012.

Version C
Page 3 of 24
Qualified Staff across South Central (September 2007)
Profession
Number in South Central
Nurses, Midwives and Health Visitors 30,259
Allied Health Professionals 8,369
Healthcare Scientists
2,744
Healthcare Assistants
9,845
Ambulance staff
1,455
GPs
2,931
Medical and dental staff; including consultants, Public Health and Community Health Services
6,699
The amount of simulated training available for qualified staff is variable between Trusts but the potential uptake of simulated training is great, however, more work needs to be done to establish future needs and realistic usage. 2. What
1 Patient safety: in particular incidents that may be avoided through simulated training, such as those attributed to: a particular treatment/procedure, a medication error, problems with consent/communication, with the use of piece of medical equipment/device/equipment or with the management of the rapidly deteriorating patient. 2. Widely used intervention procedures e.g. laparoscopy, endoscopy, arthroscopy involving use of relatively recently introduced medical equipment.
3. How

Version C
Page 4 of 24
1. Interprofessional learning where appropriate, i.e. improving multidisciplinary teamwork, (lack of teamwork being cited as major contributing factors in untoward incidents). 2. Introduce commonly used and educationally valid workplace based assessments (WPBA) tools for simulation training (e.g. DOPS, MiniCEX). 3. Development of a pool of appropriately skilled trained trainers. 4. Widespread implementation across the South Central region 5. Recruit and train a pool of simulated patients (actors) 6. Evaluation and applied educational research into simulation training programme funded by NESC 7. Overcoming the barriers to implementation:
� reducing the level of non-attendance and improving efficiency � improved efficiency will result in less time away from the workplace � Increased use simulation techniques and the resulting benefits will lower the
resistance from more senior clinicians that may not be completely familiar with simulation training
� Improved facilities and availability of equipment and training staff will allow greater access for trainees.
Recommendations for 2009/10 Investments should be based on reducing identified risks to patients and maximising benefits.
1. Monitor outcomes and progress from investments in 2008/9 to ensure that a sound foundation for simulation training is being established.
2. Seek proposals to overcome barriers and promote wide implementation of simulation
training:
2.1 Identify areas for implementation of simulation i.e. induction, overseas recruits and returning clinicians. 2.2 Communication and Best Practice: Identify South Central Clinical Champions; develop a website/electronic forum for sharing good practice; organize an annual meeting for key simulation training staff across South Central. 2.3 Increased use of simulation training within Foundation level training programmes

Version C
Page 5 of 24
2.4 Address high-risk procedures and reduce the number of untoward patient incidents by: a) commissioning training programmes for trainers in simulation and b) commissioning specific training packages which address training curricula and high risk procedures (scenarios); both to be accessible via NESC website for use by simulation educators in Trusts. 2.5 Establish Research and Evaluation group to advise on commissioning evaluation research of funded projects e.g. Impact on training; Patient outcomes and Trainee outcomes; Evaluatitive research, how we can ensure that the use of simulation as a teaching method will be practically meaningful to students. 2.6. Introduce WPBA tools as a routine part of simulation training.

Version C
Page 6 of 24
References
A High Quality Workforce: NHS Next Stage Review. London Department of Health, 2008
The Calman Report: Implications and Costs Meadows. S. Health Manpower Management: 1996 v22 I 3 23-26.
Gaba D. The future vision of simulation in healthcare. Qual. Saf. Heath Care 2004; 12-20. High Quality Care For All: NHS Next Stage Review Final Report London Department of Health, London 2008
Hospital Doctors: Training for the Future. Health Publications Unit, London 1993.
Kneebone. R, Scott. W, Darzi. A, Horrocks. M, Simulation and clinical practice: strengthening the relationship. Medical Education; 38: 1095-1102 Kohn et al. To Err is Human – Building a Safer Health System. National Academy Press, Washington 1999 National Patient Safety Agency: Reporting and Learning Summary, Quarterly Data Summary, Nov 2008 Nursing and Midwifery Council (NMC) Simulation and Practice Learning Project December 2007

Version Control code
Page 1 of 24
APPENDIX ONE
Summary of workshop findings:
What are the key issues we need to address in implementing a NESC simulation strategy?
Issue Definition/Example Obstacles/Barriers Outstanding questions/notes
1. Definition of what
we mean by
simulation training
1. What are you trying to
achieve, what is the
vision?
Define objectives of simulation training by
trust, professional groups,
interprofessional activity in different
departments etc.
2. Definition of simulation Spectrum from one man looking down a
laparoscope to a team managing a
trauma patient.
3. What are we trying to
achieve?
Getting most benefit for most people –
multi-professional team learning about
skills that are in each one’s roles.
4. What is the product?

Version Control code
Page 2 of 24
5. Should all trusts be
brought to a minimum
level?
all high fidelity – how many
centres are necessary
within SC SHA area – will
some areas benefit from just
skills labs -low fidelity
important
6.? Centres of excellence Consider the patient journey - not just
acute areas
2. Funding 1. Need criteria to allocate
funding
1. Money; equipment not
cheap, procurement not
quick.
Avoid underuse, avoid waste. Look at
utilisation rate of centres
2. Inequitable funding 2. Lack of senior level buy-
in
Sustainability of initiatives
3. Cost effective - financial
constraints
Share experience and equipment; access
courses around region
4. Financial restraints and
how to access training
resources
5. Funding doesn't feel like
it is anyone’s responsibility
3. Centres of excellence
or all trusts having a bit
4. Categories

Version Control code
Page 3 of 24
3. Training: training
the trainers and the
clinicians
1. Have we got the people
with the skills to deliver
the training?
1. Medical staff have
dedicated time – nurses and
AHPs don’t.
2. Distance in accessing
learning
Focus on team and leadership skills
3. Service commitments scenarios to be stored – METI/ SIMMAN
4. Different regulatory
bodies
Multi disciplinary scenarios
Staff development –
commitment
Medics rule ok perception
Lack of
trainers/expertise/credibility
Technical support crucial
Can't release staff for
training
Finding protected time
2. How do we know they
are all skilled to the same
level?
1. Accreditation of training
to assure consistent
standards.
Network of trainers
Regional working group
2.Educators fit to train; to
use equipment
6. Standardised – train the trainer
Mapping skills to curricula
3. Faculty and facility to run
training on an appropriate
scale

Version Control code
Page 4 of 24
4. Lack of appropriate
trained faculty – how do you
release them from their day
job.
Revalidation link
3. Space and appropriate
facilities
1. Facilities to run training
on appropriate scale.
Geography/travel: advantage of being
sent somewhere; you can't be called back
4. TIME – proper
feedback, and time to go
back and practice
Historically lack of appropriate
infrastructure, driven by enthusiasts.
4. Assessment is key 1.recognise outcomes
2.Evaluation
3. Mandated element of
training and simulation
should have objective for
training retraining and
assessment.
Address issues of on-going change in
health professions
4. Map simulation to
professional competencies
and learning outcomes.
/curricula
Remote access to support elearning
Human factors trainers/ training
Updating scenarios/equipment

Version Control code
Page 5 of 24
4. Communication 1. Lack of communication
between and within trusts.
1. Accessibility across
training sites (different trusts
sharing equipment)
Partnership working with close trusts
2. Lack of trust overcome
by transparency and
sharing
2. Working isolation SIMMAN user groups/user network
3. User groups within trusts
- duplication of information
User group - advertising
4. How do we access
training resources
Tetchy competitions between sites
offering similar opportunities
Want to marry up resources within region
to objectives - a pooling of resources
Move away from a few key enthusiasts –
able to network
3. improve awareness improve communication
More networking
Sharing of specialist resources – people
and equipment
Co-ordination and collaboration!
5. Roles of certain
group: NESC,
Trusts, HEIs
1. Where do HEIs fit in the
equation?
2. Trusts and HEIs
working to address the

Version Control code
Page 6 of 24
same issues
3. How do PCTs access
these facilities?
6. Research 1. How do we know this is
an effective method of
education/training?
Benchmark - industry standard
2.. Research – evidence
informed practice
3. Simulation as a science
must be better understood
across the medical
profession and seen to be
relevant and realistic to all
the healthcare
professionals.
4. Must satisfy customer
needs and we don’t know
what those are
5. Is there a natural
aversion to or enthusiasm
for simulation? Do people
believe in it?