Embed Size (px)
Citation preview

Scand J Haematol(l977) IS, 348-352
Streptokinase Resistance in Medical Patients in Oslo
HARALD ARNESEN, MARIE RYGH, BERNT LY & ERLING JAKOBSEN
Haematological Research Laboratory, Medical Department I X , Ullevdl Hospital, University Clinic, Oslo, Norway
The streptokinase titrated initial dose (TID) was estimated in 312 patients consecu- tively admitted to a medical department in Oslo. 93 % had a TID below 250,000 IU, 97 % below 425,000 IU and 98.5 % below 650,000 IU. N o differences were found be- tween the two sexes. The highest values were found in patients 50-60 years old. Other- wise, no differences were found between different age groups from 10 to 90 years of age. Two patients with extremely high TID values were both anamnestically prone to streptococcal infections. It is concluded that our standard initial dose of 250,000 IU of streptokinase is suf- cient for the great majority of our patients. Pre-treatment test for TID is recom- mended only when recent streptococcal infections are suspected.
Key words: fibrinolytic therapy - streptokinase - titrated initial dose
Accepted for publication November 17, 1976
Correspondence to: Harald Arnesen, M.D., Medical Department VIII, Ullevil Hospital, Oslo, Norway
The fibrinolytic activator streptokinase is widely used in the treatment of selected cases with recent thrombo-embolic disease. Its capacity to enhance the lysis of venous thrombi, especially acute ones, is well documented (Gormsen & Laursen 1967, Browse et a1 1968, Robertson et a1 1968, Kakkar et a1 1969, Schmutzler 1969, Hirsh et a1 1970a).
Streptokinase is antigenic in man, and in- dividual variations in the level of strepto- kinase antibodies exist (Fletcher et a1 1958, Schmutzler 1969, Hirsh et a1 1970b). Thus, the level increases after streptococcal infec- tions (as streptococcal antibodies cross-react with streptolkinase, Fletcher et a1 1958), and
after treatment with streptokinase (Fletcher et a1 1959).
Most likely, the circulating antibodies against streptokinase must be neutralized before effective thrombolysis can be achieved (Fletcher et a1 1959, Hirsch et a1 1970b). Ideally, therefore, the initial dose of strepto- kinase should be given after titration of the streptokinase antibodies in a given patient. For this purpose a streptokinase resistance test has been recommended (Johnson et a1 1957, Fletcher et a1 1959, Deutsch & Fischer 1960, Schmutzler 1969). Empirically, the amount of streptokinase that is necessary to dissolve a clot made from 1 ml of the patients blood or plasma in 10 min at 37OC.

SK-TID IN OSLO 349
multiplied by the blood or plasma volume, is taken as the titrated initial dose (TID) of the individual (Deutsch & Fischer 1960, Schmutzler 1969).
For practical reasons, however, standard dosage schemes for the routine administra- tion of streptokinase have been widely adopted. In Medical Department IX, Ulle- vil Hospital, we have adopted a standard schedule using an initial dose of 250,000 IU. In most regions where observations are published, this dose has been shown to be higher than the TID in about 90 % of the population (Schmutzler 1969, Hirsh et a1 1970b, James 1973, Aznar et a1 1976). As pointed out by Hirsh et a1 (1970b), geo- graphical variations may exist, for instance in relation to the frequency of streptococcal infections.
The present study was therefore under- taken to determine the TID of streptokinase in medical patients in Oslo.
PATIENTS AND METHODS
312 patients consecutively admitted to Medical Department IX, UllevHl Hospital, were included
in the study. There were 175 men and 137 wo'men with an age distribution of 13-95 years (mean 61.8) and 13-92 years (mean 66.9), respectively.
Blood samples were drawn on the first hospital day as follows: 9 vol of blood were collected into precooled ( + 4 O C) plastic tubes containing 1 vol of 0.1 M sodium citrate. Citrated plasma was pro- cessed by centrifugation at 2000 g for 20 min. The plasma was pipetted off and kept at -20° C until tested within 3 months. Titrated Znitial Dose (TID) was calculated as follows: to 0.2 ml of citrated plasma was added 0.2 ml of streptokinase (Test- Streptase, Behringwerke, M a r b u r a a h n , West Ger- many) in serial dilutions, before clotting with 0.2 ml of thrombin (Topostasine, Hoffmann-LaRoche, Basle, Switzerland) (30 NIH-dml) at 37O C. Lysis time was registered, and the streptokinase concen- tration sufficient to give a lysis time of 10 min was calculated. This concentration was multiplied with the total plasma volume, 3000 ml taken as a mean, to give the TID.
RESULTS
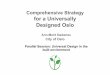
As shown in Figure 1, the great majority of patients (87.5 %) had a TID below 150,000 IU. 93 % had a TID below 250,000 IU, 97 % below 425,000 IU and 98.5 % below 650,000 IU.
120 1 2 100 z W
4
- c 80
n
Y 60 0
a m B
4 0
2 20
1) + I t + 875 950 1500 2160 50100 250 650
S K - T I D I I U J X 1 0 3
Figure 1. The distribution of streptokinase TID among 312 patients consecutively admitted to a medical department in Oslo. 93 % had a TID below 250,000 IU, corresponding to our standard initial dose of streptokinase, marked with a dotted line.

350 H. ARNESEN, M. RYGH, B. LY #& E. JAKOBSEN
2 patients showed extremely high TID values, 1,500,000 IU and 2,150,000 IU, re- spectively. Both patients were men aged 48 and had several features in common. Both were chronic alcoholics without permanent work or homes. Both had been hospitalized frequently because of infected wounds, bron- chitis and intojxications during the recent years. Both were prone to streptococcal in- fections, and 1 of them had an empyema from where streptococci were cultured.
S K - T . 1 . D (IU)X103
I - - 9 4 5 I f
60 0
500
4 0 0
3 0 0
200
100
f.
I I I
I
I I
I
~
ji
L - ~ O P V I ~ - ~ V
A g e : 0 0 0 0 0 0
( y e a i s ) o
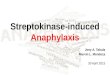
Figure 2. The age and sex distribution of strepto- kinase TID. The mean values (columns) and ranges (lines) are illustrated. n: number of patients in each age group and sex.
These 2 patients were withdrawn from the calculation of TID mean values.
The age and sex distributions are shown in Figure 2. The highest levels were seen in patients 50-60 years old for both sexes, that is when the two1 extreme patients mentioned above were excluded. The few patients be- low 40 years oaf age do not permit firm con- clusions, but no marked differences seemed to exist between the TID of patients below 50 years and those above 60 years in Oslo. Furthermore, no differences were found be- tween the two sexes as regards the level of TID.
DISCUSSION
It has been suggested that the level of strep- tokinase antibodies, as for instance evalu- ated by the streptokinase resistance test giving the TID, might show geographical variations, probably related to the degree and distribution of streptococcal infections (Hirsh et a1 1970b). In Scandinavia, pre- vious studies on this topic are few. From Sweden, Nilsson & Olow (1962) reported the 'MD to vary between 50,000 IU and 1,000,000 IU in 67 patients with deep venous thromboasis, and Olow et a1 (1970) found 95 % of 119 similar patients to have a TID below 600,000 IU. These figures are in good agreement with our present results from Oslo, where 98.5 % of patients ad- mitted to1 a department of internal medicine had a TID below 650,000 IU. The present results also seem to be in accordance with studies from other parts of Europe (Schmutz- ler 1969, Samama & Conard 1970, James 1973, Aznar et a1 1976) and Australia (Hirsh et a1 1970b, O'Sullivan 1973). Thus, no important differences seem to ex- ist in the level of TID between populations

SK-TID IN OSLO 351
within wide geographical limits. The present results neither showed dif-
ferences between the two1 sexes, nor between patients of different ages from 10 to 100 years, although the number of patients in the age groups below 40 years was small. The latter finding is in contrast to the find- ings of Aznar et a1 (1976) in Spain, where lower TID was encountered for people more than 50 years old as compared with the younger ones. The reason for this discrep- ancy is unknown.
In relation to fibrinolytic therapy with streptokinase, nothing is really known about the thrombolytic effectiveness of different dosage schedules as related to the TID of the patients. Nevertheless, it seems to be accepted that patients with very high TID need higher initial doses in order to achieve thrombolysis. If the empirically constructed TID should correspond to the given initial dose of streptokinase to achieve optimal thrombolysis, a standard dosage of 250,000 IU would be suilicient €or the great majority of our patients. According to Hirsh et al (1970b), this initial dosage would also be fibrinolytically effective in patients with somewhat higher values of TID, although after a somewhat longer time (a few hours).
The patients with extremely high values of TID would probably be resistant to thrombolytic therapy with streptokinase. In our study, the only 2 patients with extreme- ly high values had histories of proneness to streptococcal infections. If this is represen- tative, it seems sufficient to perform a strep- tokinase resistance test only where recent streptococcal infections are known or sus- pected.
REFERENCES
Aznar 3, Delgado F, Estelles A & Gilabert J (1976)
Streptokinase resistance test in a group of Medi- terranean people and its possible variations as regards sex and age. Scand J Haematol 16, 383- 86.
Browse N L, Thomas M & Pim H P (1968) Strep- tokinase and deep vein thrombosis. Br Med J 3,
Deutsch E & Fischer M (1960) Die Wirkung intra- venos applizierte Streptokinase auf Fibrinolyse und Blutgerinnung. Thromb Diath Haemorrh 4,
Fletcher A P, Alkjaersig N & Sherry S (1958) The clearance of heterologous protein from the cir- culation of normal and immunized man. J Clin Invest 37, 1306-15.
Fletcher A P, Alkjaersig N & Sherry S (1959) The maintenance of a sustained thrombolytic state in man. I. Induction and effects. J Clin Invest 38, 1096-1110.
Gormsen J & Laursen B (1967) Treatment of acute phlebothrombosis with streptase. Acta Med Scand 181, 373-83.
Hirsh J, McDonald I G & Hale G S (1970a) Streptokinase in the treatment of major pul- monary embolism - experience with twenty- five patients. Aust Ann Med 19 (Suppl l), 54-59.
Hirsh J, OSullivan E F & Martin M (1970b) Eval- uation of a standard dosage schedule with strep- tokinase. Blood 35, 341-49.
James D C 0 (1973) Anti-streptokinase levels in various hospital patient group. Postgrad Med J , Aug Suppl 26-29.
Johnson A J, Fletcher A P, McCarty W R & Til- lett W S (1957) The intravascular use of strepto- kinase. Ann N Y Acad Sci 68, 201-06.
Kakkar V V, Flanc C, Howe C T, O’Shea M & Flute P T (1969) Treatment of deep vein throm- bosis. A trial of heparin, streptokinase and arvin. Br Med J 1, 806-10.
Nilsson I M & Olow B (1962) Fibrinolysis induced by streptokinase in man. Acta Chir Scand 123, 247-66.
Olow B, Johansson C, Anderson J & Eklof B (1970) Deep venous thrombosis treated with a standard dosage of streptokinase. Acta Chir Scand 136, 181-89.
OSullivan E F (1973) Practical management of streptokinase therapy. Postgrad Med J, Aug
Robertson B R, Nilsson I M & Nylander G (1968) Value of streptokinase and heparin in treatment
717-20.
482-506.
Suppl 39-42.

352 H. ARNESEN, M. RYGH, B. LY & E. JAKOBSEN
of acute deep venous thrombosis. Acta Chir international sur la streptokinase, Lyon. Scand 134, 203-08.
Samama M & Conard J (1970) La necessitk et la paradoxe apparent des fortes doses. Colloque
Schmutzler R (1969) Klinik der thrombolytischen Behandlung. Der Internist 10, 21-29.
B O O K S
Haemoglobin: structure, function and synthesis (1976) Br Med Bull 32, Number 3, 193- 291. Describes current H b research in Great Britain such as biosynthesis and pathology of Hb. Brit Council, 65 Davies, London W1Y 2AA.
Z Lojda, R Gossrau .& T H Schiebler (1976) Enzymhistochemische Methoden. About 100 methods are described for demonstrating about 50 different enzymes in normal and pathological tissues. Springer Verlag, Berlin, Heidelberg, New York; p 300, US $ 23.80.
J Aleksandrowicz & J Lisiewicz (1976) Haematology of infectious diseases (3rd ed). Systematical description of cellular response and immunoglobulin changes in diseases caused by viruses, bacteriae, fungi, protozoa and parasites. P 259. For sale (US $ 9.00) through the National Technical Information Science. Department of Commerce 5285 Post Royal Road, Springfield, Virg. 22161, USA.
Charles Bishop (1976) Overview of blood. A blood information service (BLDIS) which goal is to assemble all scientific and clinical information in one year on the field of blood and make that accessible. P 335. Blood Information Service. 508 Getzville Rd. Buffalo, N.Y. 14226. US $ 10, postpaid anywhere.
Robert A Kyle & Edwin D Byard (1976) The monoclonal gammapathies. American Lecture series. Charles Thomas Publ. Springfield, USA. P 414. Prize US $ 36.75. Well-written, balanced, pedagogical, well-illustrated and up-to-date monography written by two haematologists who for many years have directed their attention to several aspects of these disorders. The subjects are dealt with in a thorough manner and are also based on 869 cases seen at the Mayo Clinic. Highly recommendable. Aa. Vi.
J-S Abbatucci (+ 21 co-workers) (1976) Sche'mas thirapeutiques de Cance'rologie du Centre. Franfois Baclesse, i Caen (1976). Expansion Scientifique Fransaise, Pans. P 197. Prize 100 Fr.
Hemoglobin, International Journal o f Hemoglobin Research. Edited by T H J Huisman, Laboratory of Protein Chemistry, Medical College of Georgia, Augusta, Georgia 30902, USA. 8 issues per vol. $ 65.00 per vol + $ 10 outside USA.