Embed Size (px)
Citation preview

Stroke Level III Hospital Data Collection Webinar Sheryl Martin-Schild, MD, PhD, FANA, FAHA
Stroke Medical Director for the State of Louisiana Louisiana Emergency Response Network (LERN)

LERN Stroke Strategic Priority
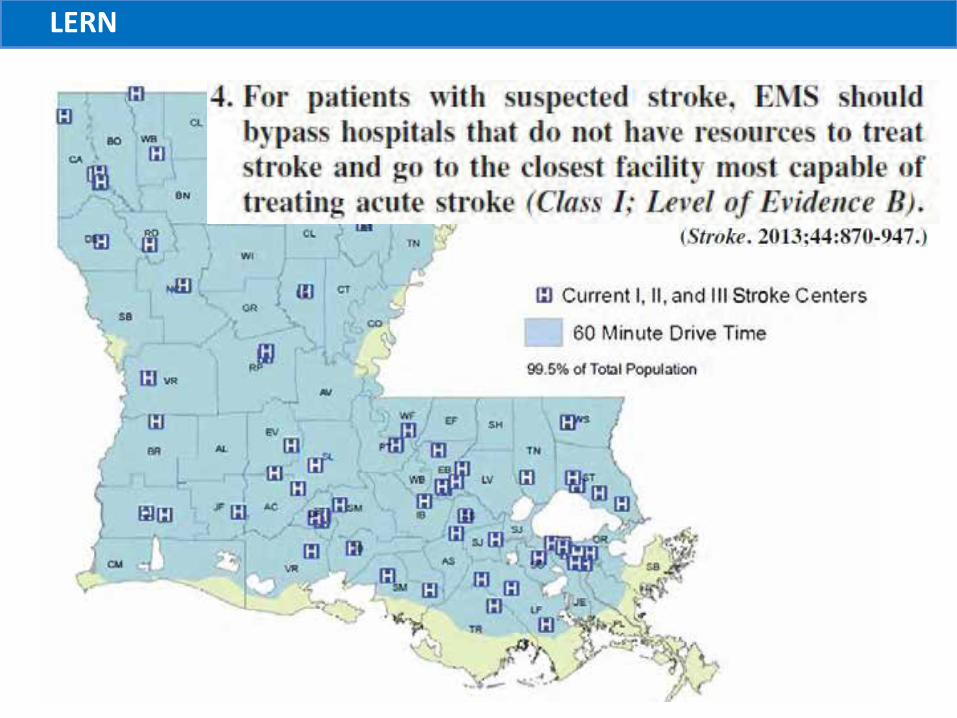
• Develop a statewide system of stroke care to improve outcomes for Louisiana citizens regardless of where they live in the state.

N D
MN SD
W Y
RI
U T
I L
K Y
A Z
N M
O K
N C
L A
LERN
AHA/ASA: Expanded Systems of Care 12 states and DC have enacted policies around the recognition of stroke facility designations
D.C.

LERN
How are LERN Stroke Hospital Levels defined?
• Level I = Comprehensive Stroke Centers • Level II = Primary Stroke Centers • Level III = Acute Stroke Ready Hospitals • Level IV = Stroke Bypass Hospitals

LERN
2 16 -> 15

LERN
LERN

LERN
Hospital Criteria LERN Level III
ER staffed by physician 24/7 Evaluates within 10min and contacts neurological expertise within 15min of arrival
Neurological expertise Within 15 min of arrival, by phone or telemedicine
CT scan available 24/7 within 25min of arrival
And have scan interpreted within 45min of arrival
Labs resulted <45min of arrival CBC, platelets, PT/INR/PTT, and chemistry
Proficient tPA delivery Able to administer tPA within 60min of arrival; appropriate transfers for higher level
Protocols for stroke care Guidelines, algorithms, critical care pathways, NIHSS training; plan for secondary transfer
Quality control Involvement in GWTG-Stroke or submission of data to LERN
LERN
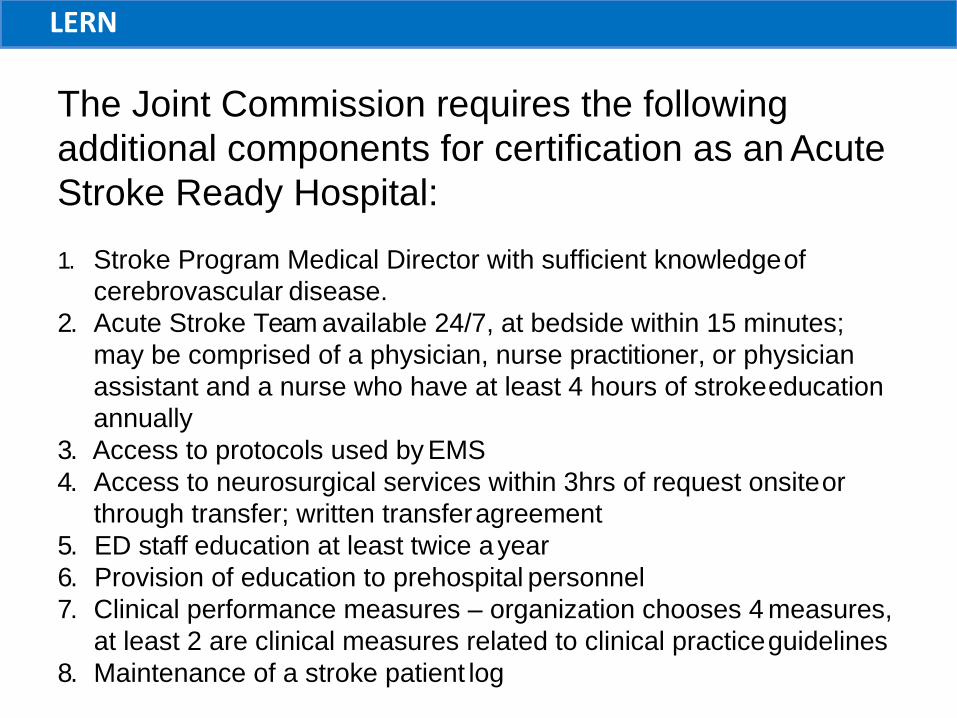
The Joint Commission requires the following additional components for certification as an Acute Stroke Ready Hospital:
1. Stroke Program Medical Director with sufficient knowledge of cerebrovascular disease.
2. Acute Stroke Team available 24/7, at bedside within 15 minutes; may be comprised of a physician, nurse practitioner, or physician assistant and a nurse who have at least 4 hours of stroke education annually
3. Access to protocols used by EMS 4. Access to neurosurgical services within 3hrs of request onsite or
through transfer; written transfer agreement 5. ED staff education at least twice a year 6. Provision of education to prehospital personnel 7. Clinical performance measures – organization chooses 4 measures,
at least 2 are clinical measures related to clinical practice guidelines 8. Maintenance of a stroke patient log

LERN
Who monitors performance of LERN Stroke Hospitals ?
• Level I = Comprehensive Stroke Centers – TJC, DNV
• Level II = Primary Stroke Centers – TJC, DNV, HFAP
• Level III = Acute Stroke Ready Hospitals – TJC or HFAP (if certified) – LERN
• Level IV = Stroke Bypass Hospitals – Not applicable

LERN
How is LERN data submission different than participation in GWTG-Stroke?
• LERN data elements are exclusively focused on what happens in the ED – Efficient evaluation, treatment, and triage
• GWTG-Stroke is an in-hospital program for improving delivery of optimal stroke care based on treatment guidelines – Includes the most LERN data elements – Many other benefits of participating
• The quarterly stroke data report card provides tailored feedback and recommendations.

LERN
GWTG-Stroke user
If a GWTG-Stroke participating center wants to receive the LERN feedback report…
– Query the recorded LERN data elements from GWTG-Stroke
– Transfer the fields into the stroke data point entry form
– Submit for review
Most of the work was already done!

LERN
Region 1
Dr. Sheryl Martin-Schild
Submitting data to LERN?
PSC
PSC
Yes
No
CSC No
No
PSC/Yes
CSC
Yes
PSC
No

LERN
Region 2
Dr. Joseph Acosta
Submitting data to LERN?
PSC
Yes
No
No
PSC
Yes
Pending….
Yes
Yes

LERN
Region 3
Dr. Digvijaya Navalkele
Submitting data to LERN?
n/a
Yes
Yes
n/a Yes
No
No/GWTG
Yes
Yes
No/GWTG
No

LERN Submitting data to LERN?
No
Region 4 n/a
Yes
n/a
No
No
No
PSC
Dr. Leo n/a DeAlvare Yes
No
n/a
PSC
n/a
Yes
n/a
n/a
LERN
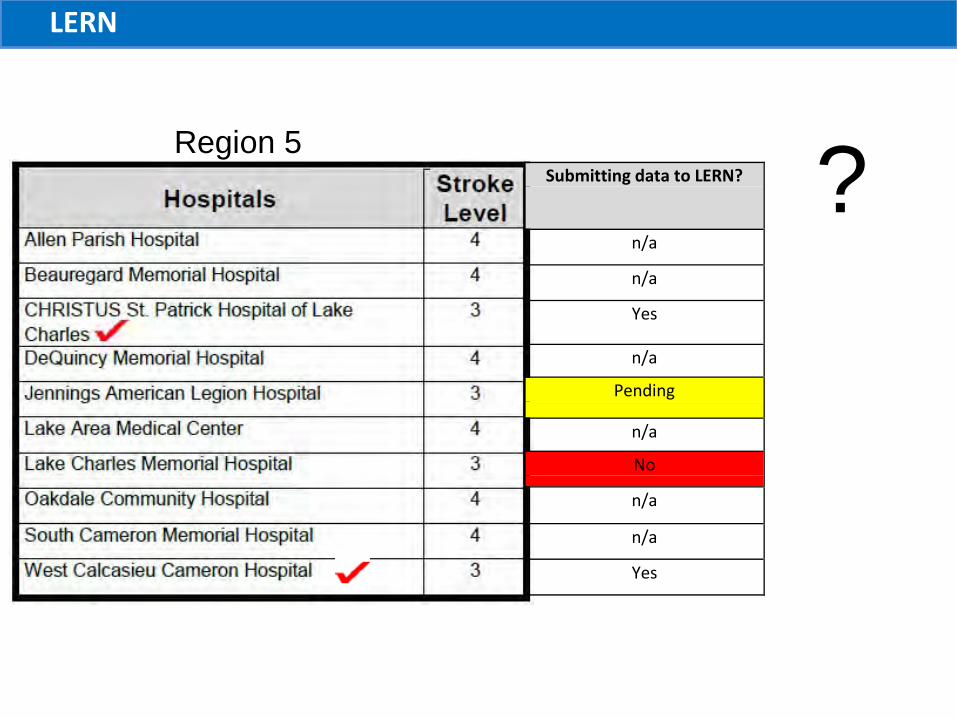
Region 5 Submitting data to LERN?
n/a
n/a
Yes
n/a
Pending
n/a
No
n/a
n/a
Yes
?

LERN
Region 6
Dr. Gonzalo Hidalgo
Submitting data to LERN?
n/a
n/a
n/a
No
PSC
No
n/a
PSC
n/a
Yes
2
LERN Submitting data to LERN?
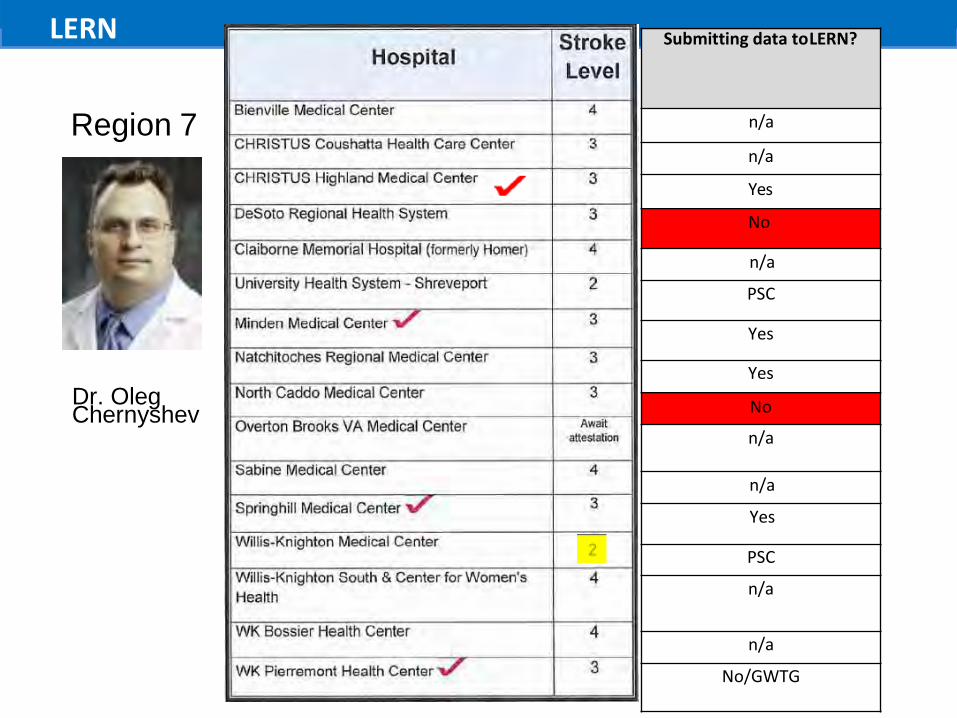
Region 7 n/a
n/a
Yes
No
n/a
PSC
Yes
Yes Dr. Oleg Chernyshev
n/a
n/a
Yes
PSC
n/a
n/a
No/GWTG
No

Regi?on
8
Submitting data to LERN?
n/a
n/a
n/a Yes
No
No
n/a
n/a
n/a
Dr. Jeffrey Harris
n/a
n/a
n/a
No/GWTG

n/a

LERN
Region 9
Dr. Ramy El Khoury
Submitting data to LERN?
n/a
Yes
PSC
n/a PSC
PSC
No
Yes
n/a
n/a
PSC
No/GWTG

LERN
• Example of sustained improvement.

LERN

LERN

LERN
• What is taking so long after labs and CT?

LERN

LERN

LERN

LERN LERN data submission
EQuIPPED = Electronic Quality Improvement Participating Emergency Department

LERN
LERN data submission the problem
• Some centers set the standard • Some centers are demonstrating improvement • Some centers have consistent problems • Some centers have submitted very few cases
All of these centers were considered “confirmed”

LERN
To address the problem….
The LERN Board approved a change in nomenclature to EQuIPPED = Electronic Quality Improvement Program Participating Emergency Department
All report cards will be sent to CEOs Action plans will be required to maintain EQuIPPED status • Require improvement within next 2 quarters

The data entry form
Which patients get entered into the spreadsheet?
ALL patients seen in the ED with suspected stroke.
However, if a patient arrives >3 hours after last seen normal, the last field which needs to be populated is Column F (Arrival Time at Door).

• The hospital identifier is a 3 letter code assigned by LERN.
• The hospital ID should only be entered in cell A5. • It will automatically fill in all after that,
as cases are entered. • If you are trying to enter the ID
in any other cell, it will appear blank. • Enter the ID in A5 only.

• Q will = 1, 2, 3, or 4 based on 1 = Jan – March 2 = April – June 3 = July – September 4 = October – December
• Do not enter Q • Do not enter 01, 02, 03, or 04 • YY will equal the last 2 digits
of the year (currently 17) • Q1 of 2017 should be
entered as 1-17 • not Q1-17 • not 01-17 • not 1-2017

• The date which should be recorded is the date the patient arrives to the hospital.
• The format should be Mo/Da/Yr.
• For example, January 1st, 2017
should be recorded as 01/01/17. • Two digits/two digits/two digits. • Not 1/1/2017. • Not Jan-01-17.

• The patient ID # should be a “Dummy ID” without any identifier, yet facility-dependent.
• Patient identifiers should not be included in the dataset to LERN.
• Please use the Hospital Identifier, followed by the quarter, followed by 001.
• For example, if your hospital identifier is CCC, and it is 3rd quarter of 2017, your first patient's Dummy ID should be: CCC-3-17-001. The next patient would be: CCC-3-17-002, and so on.

• LSN is the time (military time) that the patient was last known to be at his or her normal neurological condition.
• LSN time = the time of onset for: • a person who was awake at
onset and can provide his or her own history
• a person with witnessed onset. • If the LSN time is unknown, leave
the cell blank. • If the LSN time is the day prior
and more than 3 hours before the time of arrival, simply enter “>3 hours.”

• If the LSN date is before the arrival date and the patient arrives less than 3 hours after LSN, the earlier date will be assumed.
• For example, if the patient was LSN at 22:00 on 02/02/17 and arrives at 00:20 on 02/03/17, it will be assumed that the patient arrived 2 hours and 20 minutes after LSN on the date – 1.

Arrival Time at Door - This is the time (military time) that the patient was first acknowledged as being present at the LERN Level III Stroke Center. • If the patient arrives by
ambulance, this is the time the ambulance arrives at the LERN Level III Stroke Center.
• If the patient arrives by private vehicle or as a walk-in, this is the time stamp on the ED triage form.

LERN
If the arrival date/time is > 3hours after the date/time of LSN….
You are DONE submitting data for
this patient NO further data elements should
be recorded

LERN
Why register patients whose arrival date/time is > 3hours after the
date/time of LSN? • Determine the % of all stroke patients who
present to the hospital within the “window of opportunity”
• Determine the hospital’s tPA treatment rate – Missed opportunities? – Track the proportion presenting “in the window”
over time as you provide community education.

• Let’s take an example of a patient who develops symptoms while in the ED or had resolution (TIA) and then recurrence while in the ED… the LSN time would be after the arrival time.
• A patient had L sided weakness which had resolved before arrival at 23:00 on 02/03/17. The nurse sees the patient normal at 00:30 on 02/04/17. The nurse finds the patient with L sided weakness at 01:00.

• If the true arrival time was documented, it would be assumed that the patient presented 22 hours after onset of L sided weakness and question administration of tPA.
• To address this scenario, if LSN is after arrival, change the Arrival Date in Column C and Arrival Time in Column F to = date and time when the patient was LSN. • The Date recorded in Column C
should be 02/04/17. • LSN should be 00:30. • Arrival time should be when
symptoms were noted (01:00).

• This is the time (military time) the ED physician first documents a face-to-face encounter with the patient with suspected stroke who presents within the first 3 hours after last seen normal.
• If the patient presented > 3hours after LSN, don’t record anything!
• The goal is 10 minutes from the Time of Arrival to the Emergency Department until the Time the ED physician evaluates the patient.
• The median time among patients presenting < 2hours is 5min.
• Communication with Neurological Expertise Time is the time the neuro expert was first reached to make them aware of the stroke code.
• If the patient presented > 3hours after LSN, don’t record anything!
• The goal is 15 minutes from the time of arrival to time the expert is contacted.
• Among LERN Level III EQuIPPED centers, the median time was 34 minutes for patients presenting <2 hours from LSN.
• Telestroke “readiness” is a barrier. • It is all about the door-to-needle time.
• 3% neuro • 2% intens
• LERN recognizes that physicians have variable experience and expertise with acute stroke management
• A neurological expert may be a provider other than a neurologist
• Emergency medicine • Hospitalist • Intensivist • Neurosurgeon • Nurse Practitioner • Physician Assistant • Resident Physician
• Among LERN Level III EQuIPPED centers, 85% responded to this data element
• 77% neurologist • 18% emergency medicine
If the patient presented > 3hours after LSN, don’t record anything!
surgeon ivist/hospitalist

•
Time CT Performed • This is the time (military time) of the time
If the patient presented > 3hours after LSN, don’t record anything!
stamp on the baseline CT scan of the head. The goal is 25 minutes from the Time of Arrival to the Emergency Department.
• Among LERN Level III EQUiPPED centers, the medium time was 14.5 minutes for patients presenting <2 hours from LSN.
Time CT Interpreted • This is the time (military time) when the
interpretation of the baseline CT scan of the head becomes available
• Provider credentialed for interpretation of neuroimaging at the center.
• The goal is 45 minutes from the Time of Arrival to the Emergency Department.
• Among LERN Level III EQuIPPED centers, the median time was 31 minutes for patients presenting <2 hours from LSN.

Time to Completed Labs • This is the time (military time) when appropriate
laboratory values are available for patients with suspected stroke who present within the first 3 hours after LSN.
• AHA/ASA recommends CBC with platelet count, PT/INR/PTT, and chemistry with glucose.
If the patient presented > 3hours after LSN, don’t record anything!
• The goal is 45 minutes from the Time of Arrival to the Emergency Department Door.
• Among LERN Level III EQuIPPED centers, the median time was 47 minutes for patients presenting <2 hours from LSN.

Time of tPA Bolus • This is the time (military time) when the bolus of tPA
is pushed IV in the patient with suspected stroke. • The goal is 60 minutes from the Time of Arrival to
the Emergency Department and represents the “Door-to-Needle time”.
• Every minute matters - up to 2 million brain cells are destroyed each minute during a large artery occlusive stroke.
• The effectiveness of tPA depends on early administration.
• Among LERN Level III EQuIPPED centers, the median time was 70 minutes for patients presenting <2 hours from LSN.
• Systematic improvement in the Door-to-Needle time should be a priority for all LERN Level I, II, and III Stroke Centers.
• LERN recognizes the new target door-to-needle time of 45min (AHA Target Stroke).
• Will work with your center to trim your DTN time

FDA – Contraindications and Warnings & Precautions AHA/ASA 2013 – Exclusions and Relative Exclusions AHA/ASA 2015 – Scientific Rational paper
Among LERN Level III EQuIPPED centers, the most common cited reason were: •Outside of the window – 49.1% • TIA – 10.5% •Hemorrhage on CT – 4.3% Among the remaining patients: • Not documented – 37.6% • Minimal deficit – 15.8% • Unable to treat within 4.5hrs – 8.1% • Refusal – 7.7% • Other - 5.7% • Coagulopathy – 4.3% • Seizure – 4.3%

GWTG-Stroke has an option to select justifiable reasons for a delay in tPA administration • Patients with justifiable reasons do not contribute to
median times LERN has added this data element and recognizes these barriers to efficient tPA use: • Hypertension requiring aggressive control with IV
medications • Management of concomitant emergent/acute conditions • Further dx evaluation to confirm stroke in patient w/
blood glucose <50, seizures, or major metabolic disorders thought to be mimics
• Delay in determining eligibility • Timeline evolved • Need to obtain additional information
• Patient/Family Consent • Delayed diagnosis • Equipment related delay

L O U III SI A N A
" MERGENCY RESPONSE N TWO K STROKE DATA POilN T STATISTIC
2
Door to ED d:OC in hctUTS & minut es
3
D oor to r,kuro logic:aI Exp er t ise il'l hours & m Jnute:s
Do.or to CT Perform ed in hours& minutes
DODrto.CT Inte rpret ed in hours& m
inute :sc
Door ta Complet ed
Labs in hours & minutes
S6of pat ients Wit h I.a t:ts m rnp te.re d' wit hin 4 S m in of
arrival
p.at i ents arr ive,d •1it h i n 2 hours of
LSN
' 0:11 0:24 0:47 i
6
8
0:48 '
: 1:16
WALUE!
1 :51 LSNlw itihin 2 hours
' ! W ALUE!
' jWALUE!
' 0:20 0:31 0:17 L3 os c,omplet e w/ in 4 S m inut e1
'' ...''',
LOUI SIANA
0:42 ,t P/\ w / in 60 minut e. t PA w,/in 3 hours , ! LSNlw itih in 2 h our s. ' '
' ifNALUE!
, EMERGENCYRESPONSENETWORK STROK NS AND PERCENTAGES
P nP ?
Total
Number of
Patients
# of patients arrived within 2 hours of LSN
Door to ED doc MEDIAN time
in hours & minutes
Neurological
Expert ise MEDIAN time
in hours&
Performed MEDIAN time
in hours & minutes
Interpreted MEDIAN time
in hours & minutes
Door to Completed
Labs MEDIAN time
in hours&
Door to Needle MEDIAN time
in hours & minutes
% of patients with labs
completed within 45 min
of arrival
% patients treated with tPAwho are treated within
60 min of
% patients receivi ngtPA within 3 hours
of LSN who arrived withn 2
Doo r to
;i, p,at ients t reat BCI
-%p,at ients
.r,eceiving t f'A Ne edl e wit h t PA w ho·a,r e i t hin 3hoursof
inhour. s& t neatB d' w ithin '60 LSr-lwh arr ived mi nut es m in of arr iva l Wit hn 2 hoursof
LSN
minutes minutes arrival hours of LSN 6 6 0:11 0:37 0:26 0:39 0:25 1:00 67% 60% 50%

LERN
Quarter Patients Patients Patients % of all % of patients presenting
:::2hrs from LSN
treated with tPA
Mean registered :::2hrs from
LS.N tre.ated with
tPA patients
registered who·were
doo:r-to- needle time
treated with tPA
Q2 2016 22 7 5 31.8 71.4
Q3 2016 10 7 5 5(}.0 71.4
The target . time has historically been <60min; the American Heart Association/American Stroke Association (AHA/ASA) is now reconunending a target time <45min from arrival to treatment. h1 EQuIP PED Level ill hosp itals, the median door -to-needle (DTN) time is 70min. Only 40% of treated patients received alteplase within 60min; ouly 16% were treated within 45min.

LERN
Tips for data collection
• Designated person/s • Register in real time • Template for documentation for elements
that are difficult to determine retrospectively – LSN – Arrival of ED doc – Communication with
neuro expertise – Reason why tPA delayed

LERN
Summary
• Patients deserve to get what a hospital says it can provide
• Quality improvement program participation is necessary to reach the standards – Becoming EQuIPPED is a simple mechanism
• LERN data submission is not labor-intensive and not intended to be punitive

LERN
QUESTIONS???
Special thanks to Elizabeth Marcotte, RN, SCRN, CBIS, Neuroscience Program Coordinator for OLOLake Regional Medical Center, for content review and feedback on this presentation





























