Embed Size (px)
Citation preview

STRUCTURE, INJURY & HEALING
ARTICULARCARTILAGE
Nadhaporn SaengpetchDivision of Sports Medicine,
Department of Orthopaedics,
Faculty of Medicine Ramathibodi Hospital,
Mahidol University

COMPOSITION
• Extracellular matrix and sparse cells
• No blood vessel, lymphatic vessel and nerve
• limit response to any metabolic response
• Frictionless

CHONDROCTYE
• Endoplasmic reticulum and Golgi apparatus (matrix synthesis)
• Intracytoplasmic filament, lipid, glycogen, secretary vesicles (maintenance of matrix structure)

CHONDROCYTE: DIFFERENT BY LAYERS
• Surface layer: elongated and resemble fibroblasts
• Transitional layer: round and actively for chemistry
• Deeper layer: cells in radial pattern
• Tidemark: non-functional cells

COLLAGEN FIBRILS

CHONDROCYTE: FUNCTION
• NOT participate in water distribution
• Maintenance and structural competence
• Producing and replacing appropriate macromolecules (degradation, mechanical demand placed on the surface, synthesizing)
• Assembling as an highly
ordered framework

CARTILAGE ZONES

EXTRACELLULAR MATRIX (ECM)
• 2 components
1. Tissue fluid
2. Framework of structural macromolecule
• Interaction -> stiffness and resilience

ECM
• Water 80% by weight
• Gel forming = lubrication system
• Large aggregation of Proteoglycans (maintain fluid within the matrix and e’lyte concentration)

ECM MOVEMENT
Na+
Na+Cl-
Cl-
inorganic ion tissue osmolarity
STRUCTURAL MACROMOLECULES
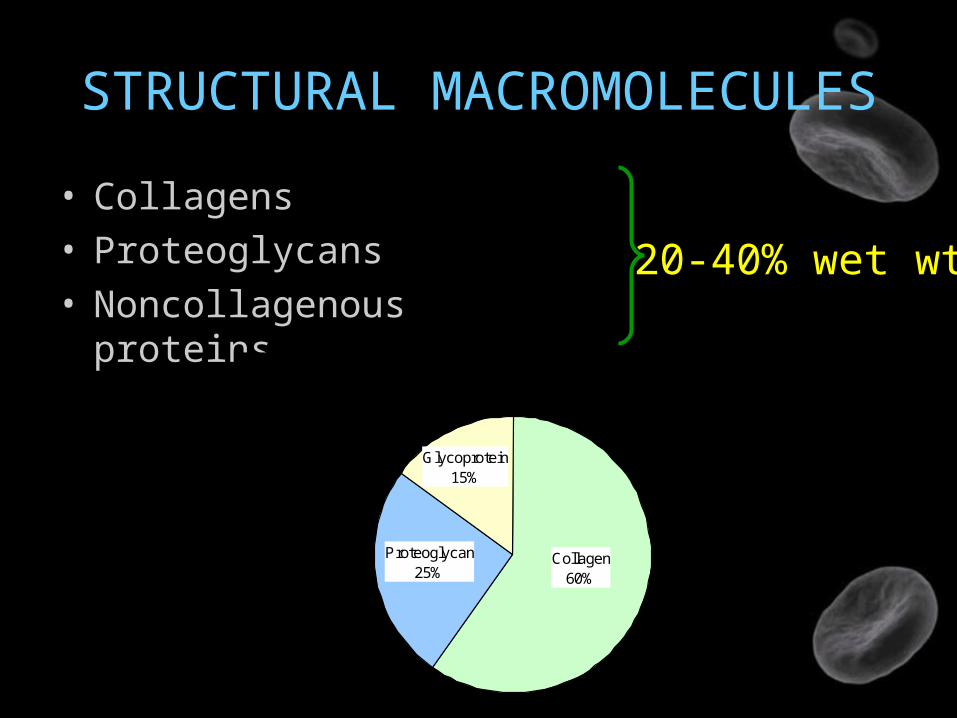
STRUCTURAL MACROMOLECULES
• Collagens• Proteoglycans• Noncollagenous
proteins
20-40% wet wt.
Collagen60%
Proteoglycan25%
Glycoprotein15%
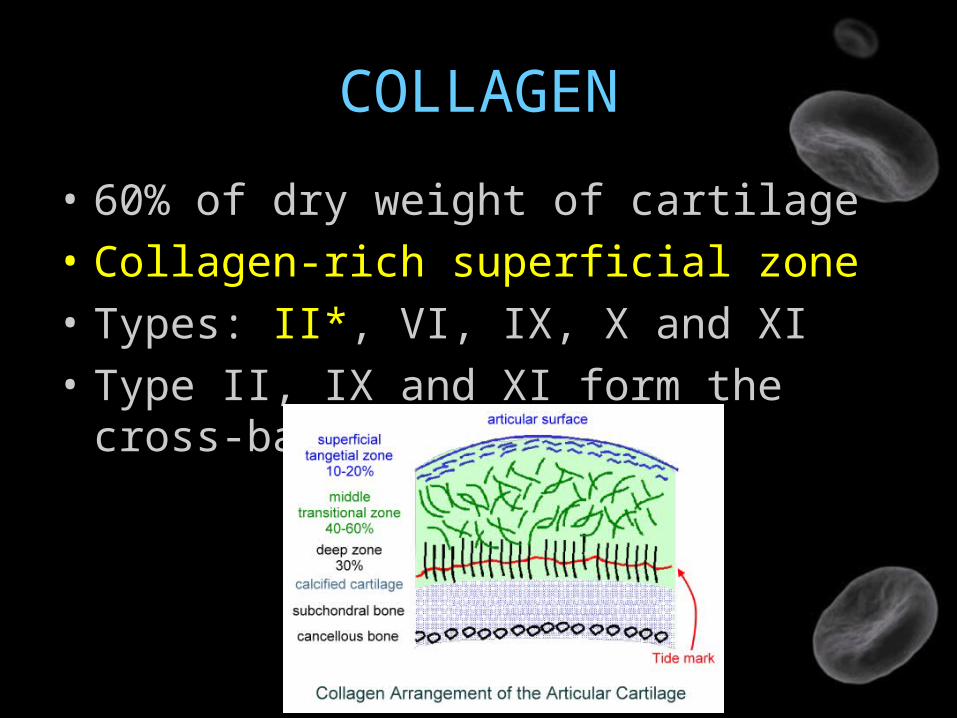
COLLAGEN
• 60% of dry weight of cartilage
• Collagen-rich superficial zone
• Types: II*, VI, IX, X and XI
• Type II, IX and XI form the cross-band fibrils

TIGHT MESHWORKCollagen fibrils organization
Tensile stiffness & cartilage strength
Large proteoglycans entrapment
Cohesiveness of tissue

TYPE II COLLAGEN
• 90-95% of cartilage collagen
• The primary component of cross-banded fibrils

TYPE VI COLLAGEN
• Forms an important part of surrounding chondrocytes
• Helps chondrocyte attach to matrix
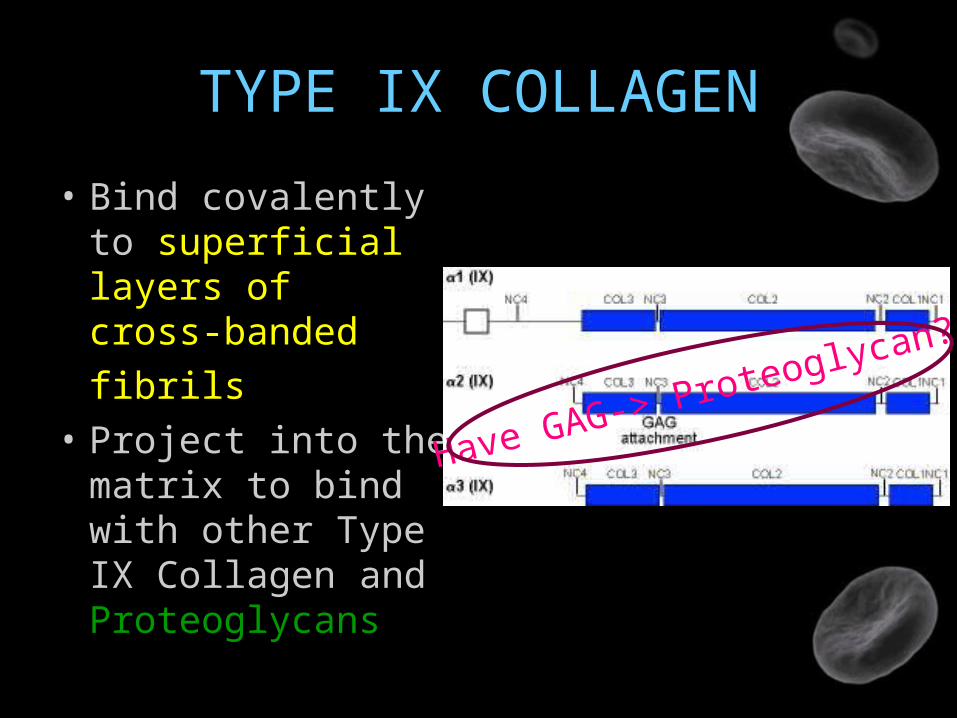
TYPE IX COLLAGEN
• Bind covalently to superficial layers of cross-banded
fibrils
• Project into the matrix to bind with other Type IX Collagen and Proteoglycans
Have GAG-> Proteoglycan?

TYPE X COLLAGEN
• Found only near cartilage calcified zone and hypertrophic zone of growth plate (start to mineralize)
• Cartilage mineralization
TYPE XI COLLAGEN
• Bind covalently to Type II
• May form part of interior structure of cross-banded fibrils
PROTEOGLYCANS
• A protein core & Glycosaminoglycans (GAG) chains (unbranched polysaccharide)
• GAG: Hyaluronic acid, chondroitin sulfate, glucosamine sulfate, dermatan sulfate

ARTICULARPROTEOGLYCAN
Aggrecans*(large)
DecorinBiglycan
Fibromodulin(small)

AGGRECANS
• Mostly fill in the interfibrillar space of matrix• 90% of Pg mass• Noncovalently bind with HA & monomer• Help anchor Pg in the matrix, prevent
displacement during deformation, organize and stabilize Pg & collagen

DECORINS
• One dermatan sulfate chain

BIGLYCAN & FIBROMODULIN
• Two dermatan sulfate chains
• Several dermatan sulfate chains
Biglycan
Fibromodulin

ARTICULARPROTEOGLYCAN
Aggrecans*(large)
DecorinBiglycan
Fibromodulin(small)
Transforming growth factor β
- Healing+ Degradative enzymes

HYALURONIC ACID
• Backbone for matrix aggregation• Bind aggrecans non-covalently and link proteins• This aggregation helps anchor Pg within the
matrix• Prevent displacement during deformation • Stabilize relationships of Pg and collagen
meshwork

NONCOLLAGENOUS PROTEINS & GLYCOPROTEINS
• Stabilize the matrix framework
• Help chondrocytes bind to the macromolecules of matrix
• Anchorin CII collagen-binding chondrocytes surface protein (anchor)
• Cartilage oligomeric protein (COMP) is in chondrocyte territorial matrix, have capacity to bind to chondrocyte

ZONES OF ARTICULAR CARTILAGE

SUPERFICIAL ZONE
• Thinnest zone• Two sub layers:
– sheet of fine fibrils (acellular)– flattened ellipsoid-shape chondrocyte +
fibroblast
• Collagen is lying parallel to the joint surface (resist compressive force)-> OA
• High collagen, low Pg• “cartilage skin”

TRANSITIONAL ZONE
• Large volume
• cells: synthetic organelles (ER, Golgi)
spheroidal shape
• Lower collagen & water concentration
• Higher Pg concentration

MIDDLE(RADIAL/DEEP) ZONE
• Chondrocytes align in columns perpendicular to the joint surface (resist shear stress)
• Largest diameter collagen• Highest Pg• Lowest water• Collagen fibers pass into the tidemark
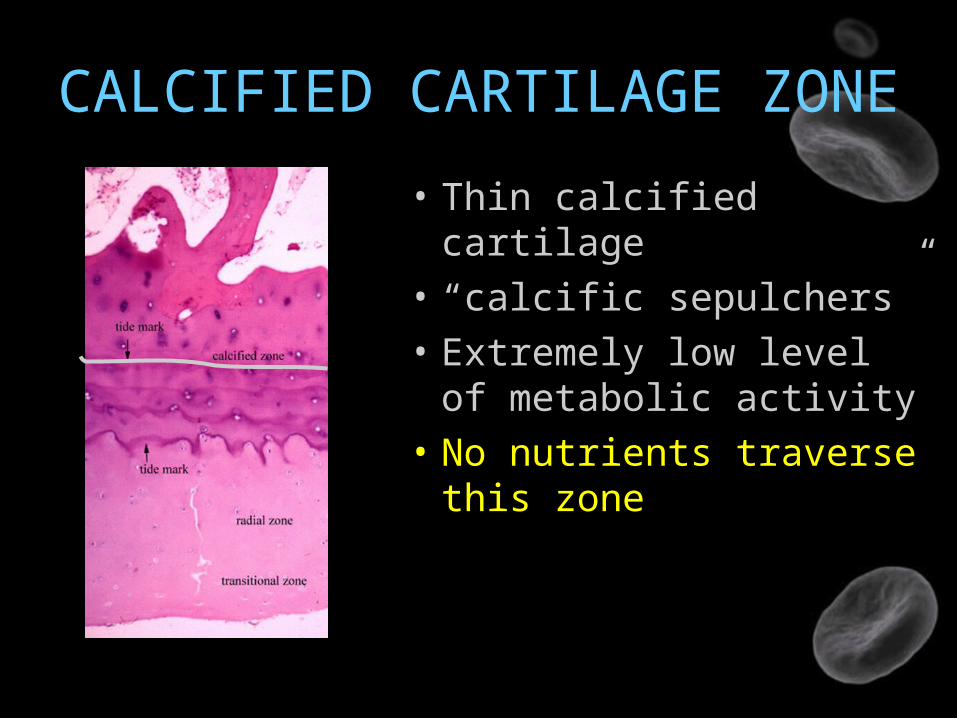
CALCIFIED CARTILAGE ZONE
• Thin calcified cartilage
• “calcific sepulchers”
• Extremely low level of metabolic activity
• No nutrients traverse this zone

MATRIX REGIONS
• Pericellular
• Territorial
• Interterritorial >>>
• Bind cell membranes to matrix macromolecules
• Protect deformation force• Transmit mechanical
signals to chondrocytes
• Provide the mechanical properties of tissue

CHONDROCYTE-MATRIX INTERACTIONS
• Matrix protects chondrocytes from mechanical damage and maintain shape and phenotype
• Matrix : metabolic products/cytokines and growth factors
• Insulin-dependent growth factor I (IGF-I) & Transforming growth factor β (TGF β) + matrix synthesis & cell proliferation

CHONDROCYTE-MATRIX INTERACTIONS
IGF-ITGF β
+
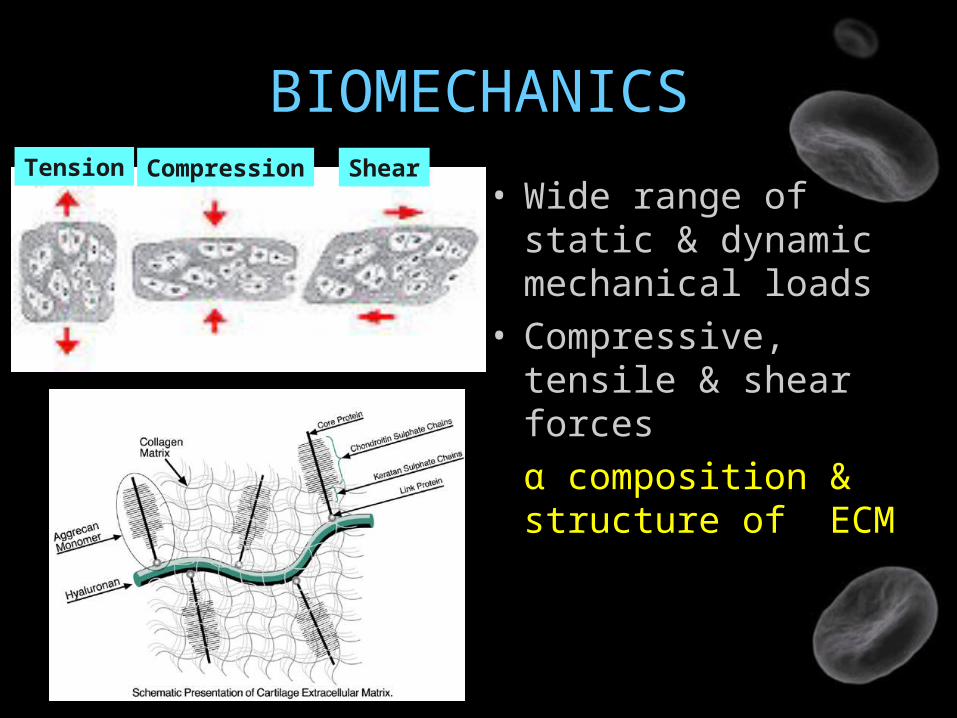
BIOMECHANICS
• Wide range of static & dynamic mechanical loads
• Compressive, tensile & shear forces
α composition & structure of ECM
Tension Compression Shear

TENSILE & SHEAR FORCE
• These forces are resisted by rope-like collagen fibrils

COMPRESSIVE FORCE
• Resisted by highly charged GAG such as aggrecan molecules

LOADING vs IMMOBILIZATION
Induced wide range of metabolic response
Decreased in matrix synthesis

CARTILAGE REGENERATION
Static compression
Reversibly inhibit cartilage matrix
synthesis
Cyclical compressive
Stimulate aggrecan core protein &
protein synthesis
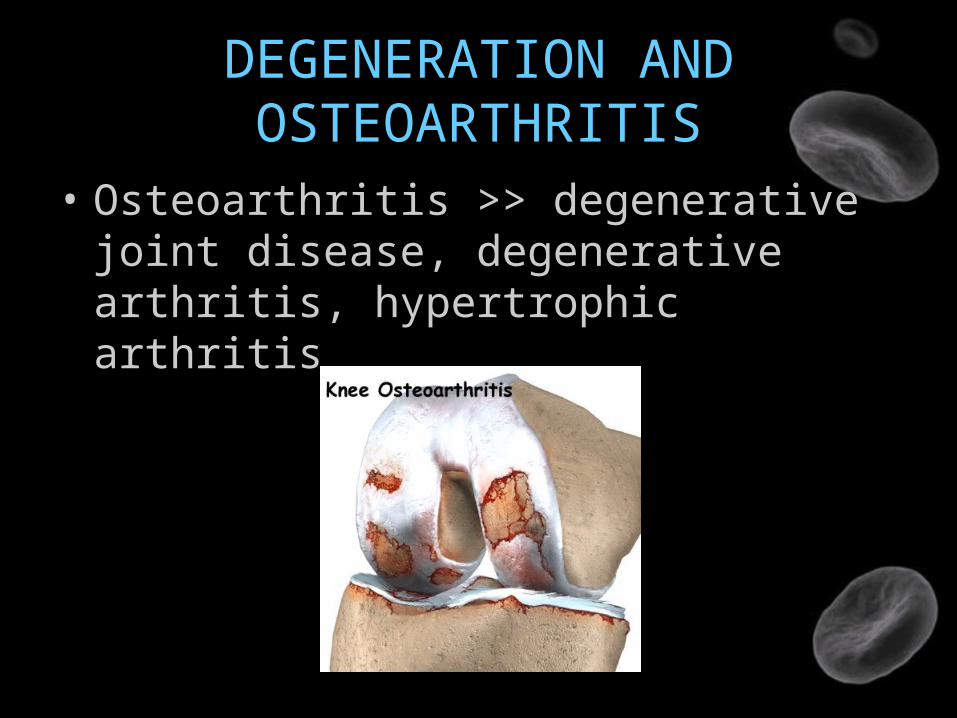
DEGENERATION AND OSTEOARTHRITIS
• Osteoarthritis >> degenerative joint disease, degenerative arthritis, hypertrophic arthritis

HOW THEY CHANGE?

OA: 3 OVERLAPPING PROCESSES
1. Cartilage matrix damage
2. Chondrocyte response to tissue damage
3. Decline of the chondrocyte synthetic response

STAGE 1 MATRIX DAMAGE
Water
Aggrecan & GAG length
Permeability
& Matrix stiffness
Other causes: inflammation, tissue’s metabolicchanges that interferes matrix maintenance

STAGE 2 CHONDROCYTE RESPONSE
• Chondrocytes detect tissue damage
Anabolic & mitogenic growth factors
chondrocyte proliferation & ECM+
Catabolic enzymes (proteases)
Reversible- Spontaneous- Intervention
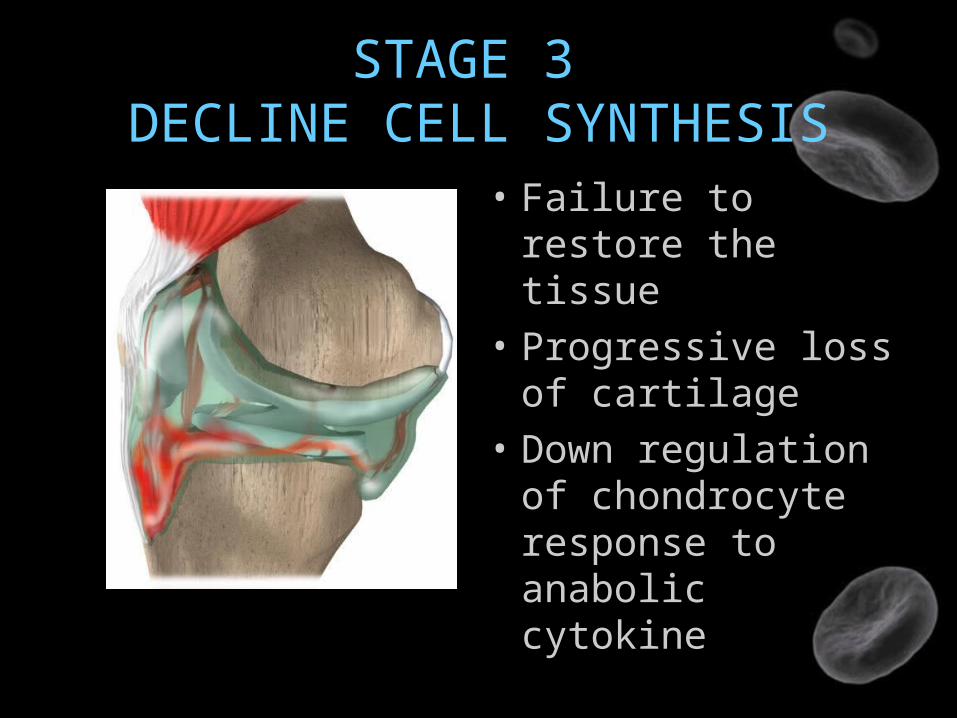
STAGE 3 DECLINE CELL SYNTHESIS
• Failure to restore the tissue
• Progressive loss of cartilage
• Down regulation of chondrocyte response to anabolic cytokine

JOINT INJURY &POSTTRAUMATIC OA
• Ligament reconstruction (ex. ACL-R) can restore mechanical stability but not greatly reduce the risk for OA development because….
The initial traumatic event may have irreversible effects on the joint tissues and residents cells

Good Luck




















![1877.] Medicine. 241 MEDICINE](https://img.pdfslide.net/doc/110x75/6248decce7f255195063a334/1877-medicine-241-medicine.jpg)






