Embed Size (px)
Citation preview

i
STUDY OF DERMATOGLYPHICS PATTERN IN
CONGENITAL HEART DISEASE
IN CHILDREN AT GOVERNMENT RAJAJI HOSPITAL
MADURAI
DISSERTATION SUBMITTED FOR THE DEGREE OF
M.D BRANCH VII
(PAEDIATRIC MEDICINE)
APRIL 2017
THE TAMILNADU
D.R M.G.R MEDICAL UNIVERSITY
CHENNAI, TAMILNADU

ii
CERTIFICATE
This is to certify that the dissertation entitled “STUDY OF
DERMATOGLYPHICS PATTERN IN CONGENITAL HEART
DISEASE IN CHILDREN AT GOVERNMENT RAJAJI HOSPITAL
MADURAI” is the bonafide work of Dr.S.R.RAJA in partial fulfilment of the
university regulations of the Tamil Nadu Dr. M.G.R Medical University,
Chennai, for M.D Degree Branch VII – PAEDIATRIC MEDICINE
examination to be held in April 2017.
.
Dr. M.R. VAIRAMUTHURAJU M.D.,
Dean,
Madurai Medical College,
Government Rajaji Hospital,
Madurai.

iii
CERTIFICATE
This is to certify that the dissertation entitled “STUDY OF
DERMATOGLYPHICS PATTERN IN CONGENITAL HEART
DISEASE IN CHILDREN AT GOVERNMENT RAJAJI HOSPITAL
MADURAI” is the bonafide work of Dr.S.R.RAJA in partial fulfilment of the
university regulations of the Tamil Nadu Dr. M.G.R Medical University,
Chennai, for M.D Degree Branch VII – PAEDIATRIC MEDICINE
examination to be held in April 2017
PROF. DR. K. MATHIARASAN M.D., D.C.H.
DIRECTOR
Institute of Child Health & Research Centre,
Madurai Medical College,
Madurai – 625020

iv
DECLARATION
I, DR.S.R.RAJA., solemnly declare that the dissertation titled “STUDY
OF DERMATOGLYPHICS PATTERN IN CONGENITAL HEART
DISEASE IN CHILDREN AT GOVERNMENT RAJAJI HOSPITAL
MADURAI” has been conducted by me at the Institute of Child Health and
Research centre, Madurai under the guidance and supervision of my unit Chief
PROF. DR. K. MATHIARASAN M.D., D.C.H.
This is submitted in part of fulfilment of the award of the degree of M.D
(Pediatrics) for the April 2017 examination to be held under the Tamil Nadu
Dr. M.G.R Medical University, Chennai. This has not been submitted
previously by me for any Degree or Diploma from any other University.
Place: Madurai
Date:
Dr.S.R.RAJA

v
ACKNOWLEDGEMENT
I sincerely thank Prof. Dr.M.R.Vairamuthuraju, the Dean,
Government Rajaji Hospital and Madurai Medical College for permitting me to
do this study.
I express my profound gratitude to Prof. Dr. K. Mathiarasan, Professor
and Director, Institute of Child Health & Research Centre, Madurai, for his able
supervision, encouragement, valuable suggestions and support for this study.
I express my sincere thanks to Prof.Dr.M. Nagendran, Prof. Dr. S.
Balasankar, Prof. Dr. Rajarajeshwaran, Prof. Dr. M. Kulandaivel, Prof.
Dr. S. Shanmugasundaram, Prof. Dr. N. Muthukumaran , for their
guidance and encouragement throughout the study.
I would like to extend my sincere thanks to former Director, Prof. Dr. G.
Mathevan for his valuable suggestions and guidance in doing this study.
I would like to express my sincere gratitude to former Chiefs Prof.
Dr.S.Sampath, Prof DR.Chitra Ayappan, for their timely support and
encouragement.
I would like to thank the Registrar Dr. D. Rajkumar M.D for his
valuable suggestions throughout the study.

vi
I wish to express my sincere thanks to my guide and assistant professors
Dr. P. Murugalatha, and Dr.S.Murugesalakshmanan, for their invaluable
guidance, support and suggestions at every stage of this study.
I also express my gratitude to all other assistant professors of our
department and my fellow post graduates for their kind cooperation in carrying
out this study.
I also thank the members of the Ethical Committee, Government, Rajaji
Hospital and Madurai Medical College, Madurai for allowing me to do this
study.
I express my sincere thanks to my parents and my better half Dr.
M.Nirmala for their unending support throughout my study.
Last but not the least, I submit my heartfelt thanks to the children and
their parents for extending full co –operation to complete my study successfully.
Dr.S.R.Raja

vii
ABBREVIATIONS
CHD Congenital heart diseases
UL Ulnar loop
RL Radial loop
atd Rt atd angle right side
atd Lt atd angle left side
TFRC Total finger ridge count
a–bRC Rt a-b ridge count right side
a–bRC Lt a-b ridge count left side
M Male
F Female
VSD Ventricular septal defect
ASD Atrial Septal defect
PDA Patent ductus Arteriosus
TOF Tetralogy of Fallot
COA Coarctation of Aorta
MS Mitral Stenosis
DORV Double outlet right ventricle
TGV Transposition of great vessels
ALCAPA Abnormal origin of left coronary artery from pulmonaryArtery

viii
ABSTRACT
Background and objectives:
Dermatoglyphics patterns develop between 6 -18 weeks of intrauterine
life which is a common period for cardiac embryogenesis, thus any prenatal
insult during that period may have an influence on the dermatoglyphics patterns.
Therefore dermatoglyphics study was carried out to elucidate the significance of
their presence in congenital heart diseases (CHD).
Methods:
A hospital based case control study was conducted. 100 cases of proven
congenital heart diseases who were admitted paediatric wards and OPD at
Institute of Child Health and Research Centre, Government Rajaji Hospital
Madurai. Another 100 normal children were included as controls. The palms
and fingers were smeared with printer’s ink to bring out the dermatoglyphics
patterns which were subsequently studied.
Results:
There was increased number of Whorls and decreased number of Arches in the
congenital heart disease patients compared with normal children. Total finger
ridge counting (TFRC) is increased in congenital heart diseases children, both
male and female children. Distal placement of axial triradius is seen in
congenital heart disease patients, with increase in the ‘atd’ angle.

ix
Conclusion:
The dermatoglyphics variation in CHD may be suggestive of external
imprint of genetic variation and may help as a diagnostic tool.
Key words: Dermatoglyphics, Congenital heart disease.

x
TABLE OF CONTENTS
Sl.No. Chapters Page No.
1 Introduction 1
2 Objectives 4
3 Review of literature 5
4 Methodology 37
5 Observation & Results 48
6 Discussion 74
7 Conclusion 78
8 Summary 79
9 Bibliography 81
10
Annexure
Proforma of the study
Master chart

1
INTRODUCTION
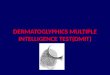
DERMATOGLYPHICS originates “from the Greek words ‘DERMA’
which means SKIN and ‘GLYPHE’ which means” to CARVE. The “term
‘Dermatoglyphics’ was coined by Cummins and Midlo. Dermatoglyphics is the
study of epidermal ridges and their configurations on the palmar and the
plantar”regions. The fine ridge patterns of the fingers, palms and soles have
intrigued humans since primitive times. The “skin on the palmar and plantar
surfaces of humans is not smooth. It is grooved by numerous ridges which form
a variety of configurations. The ridge configurations have attracted the attention
of common man for” centuries.
“Papillary ridges are confined to the palms and soles and the flexor
surfaces of the fingers and toes where they form narrow parallel or curved
arrays separated by narrow furrows. The epidermal ridges correspond to an
underlying interlocking pattern of dermal papillae, an arrangement which helps
to anchor the two layers firmly together. The pattern of dermal papillae
determines the development of the epidermal ridges. This arrangement is stable
throughout life, unique to the individual and therefore significant as a means of
identification1”.
From cradle to grave, ‘Hastarika’ the science of palmistry, is a legacy
bequeathed to humanity by ancient seers & saints of India. The roots of this
science can be traced to the Ancient East – according to Kunagusu Minakatas
notes in Nature. Chinese records mention the use of fingerprints in very ancient

2
times in India. Ancient system of Indian palmistry called ‘Samudrik Mudra’
classified ridge patterns into Padma (lotus), Sankha (conch shell) and Chakra
(wheel). These patterns are also found expressed on the palms, soles and digits
of the sculptured images of Lord Buddha seen in Indian museum at Kolkata.
Bidloo provided a description of ridge patterns in the Seventeenth century. Later
on, “additional information has been added by anthropologists, biologists,
geneticists and anatomists2.”
During “the last century, the fact that each individual’s ridge patterns are
unique has been” utilized “as a means of personal identification especially” for
legal purposes. Medical interest in epidermal ridge patterns have increased in
the last few “decades when it” was found” that many patients with
chromosomal aberrations had unusual ridge” patterns. “Inspection of epidermal
ridge patterns therefore provided a simple, inexpensive means” “of information
to determine whether a patient could have a particular chromosomal”
abnormality. Geneticists were able to demonstrate that the inheritance of the
dermal ridge conformations depended on multiple gene effect.3
Abnormal variations in epidermal ridge patterns are noticed in genetic
disorders like Down syndrome, Turner syndrome, Klinefelter syndrome. Lately
association of epidermal ridge patterns with congenital heart disease, leukaemia,
idiopathic mental retardation, dental caries and in many other diseases where
aetiology is obscure has been studied4.

3
Congenital heart diseases are a heterogeneous group of diseases in which
aetiology, importance of genetic as well as environmental factors have been
recognized. These defects show a familial tendency but no Mendelian pattern of
inheritance has been described.5
The mode of inheritance is represented by somatic traits such as
dermatoglyphics as supported by some earlier studies showing association of
epidermal ridge patterns with congenital heart defects by Hale A. R(1961)6, A
Cascos (1964)7, Brurghat W (1968)8, Mutalik G S (1968)9, Magotra ML
(1976)10 ,Renuka Nair (1986)11, Brijendra Singh (1996)12 , Anita khalil (1998)13
.
In the present study finger and palmar dermatoglyphic patterns in
congenital heart diseases are studied and compared with controls. An attempt is
made to determine a significant finger and palmar dermatoglyphic pattern
criteria applicable to patients with congenital heart disease, which can be used
as a diagnostic tool in the identification of congenital heart diseases.

4
AIMS AND OBJECTIVES
The present study is undertaken with the following aims and objectives;
1. To study the finger and palmar dermatoglyphic patterns in patients with
congenital heart diseases.
2. To evaluate and compare finger and palmar dermatoglyphic
configurations of children with congenital heart disease and that of
normal healthy children.
3. To find out whether a specific finger and palmar dermatoglyphic traits in
children with congenital heart disease is significant.
4. To use finger and palmar dermatoglyphic patterns as a tool for diagnosis
and counselling purpose.

5
REVIEW OF LITERATURE
A HISTORICAL REVIEW
Dermatoglyphics arises from the ancient art of palmistry which was
practiced from ancient times and is still followed throughout India by the Joshi
caste. It appears that the art of palmistry was initially practiced by great seers
and saints who lived in the ancient Hindu temples. From here, this art has
spread throughout the world.
In Greek civilization “cheir”, the finger and palmar ridge patterns were
studied in depth. Anaxagoras taught and practiced palmistry in 423 BC. This
dermatoglyphics study was sanctioned and encouraged by Aristotle and other
great minds like Pliny. Albertus Magnus and Emperor Augustus Anaxagorus
have said, “The superiority of man is owing to his hands". In Aristotle has
written "the hand is the organ of organs, the active agent of the passive powers
of the entire system".14
The early records show that our ancestors had acquaintance with the
traceries of fine ridges on fingers, palms and soles long before the period of
scientific study. One example of this is aboriginal Indian carving found at the
edge of Kejimkoojik Lake in Canada. It shows a human hand carved in stone
with lines representing epidermal ridges and flexion creases. This pictograph is

6
atleast several centuries old. Such ancient stone epidermal ridge cravings are
found throughout the world.
Another example is Utah Basketmaker pictograph which consists of
several human figures accompanied by designs of questionable significance
including four isolated concentric and spiral patterns resembling whorl pattern
of finger prints. The most famous of ancient “finger print” designs is the carving
on the walls of Neolithic burial passage situated in the island of Brittany15.
A Chinese seal belonging to third century B.C showed recording of a
finger print in clay which could have been imprinted on documents, letters or
packages. De Barras has mentioned that Chinese in 16th century has a custom
of recording ink prints of fingers on the deeds of sale16.
Thomas Bewick, an engraver and a naturalist had made wood engravings
of his own fingers patterns. Evidently, he was among the few persons of his
time who had good knowledge of dermatoglyphics.17

7
EARLY SCIENTIFIC RECORDS
A scientific approach to dermatoglyphics was made long before the first
records about them were written. A clear cut demarcation cannot be made
between what that is considered as scientific knowledge of dermatoglyphics and
the primitive knowledge. The evidence for this is the aborigines who carved the
hand in a rock at the edge of Kejimkoojik Lake in Nova Scotia. This carving is
truly scientific in spirit and in method according to the author.15
In the later part of the 17th century scientific interest in epidermal ridges
aroused. Mehemiah Grewin in 1684 presented before the Royal society of
London a description regarding the sweat pores and the epidermal ridge
arrangements of fingers and palms along with a drawing showing the
configurations of dermatoglyphics of hand. Later in 1685, his book on human
anatomy ‘Bidloo’ included an account on epidermal ridges of hand.18
In 1686, Malphigi briefly described the configuration of epidermal ridge
patterns of fingers19. In the eighteenth century, Hintz did several works in
Dermatoglyphics. In 1747, along with Albinus and Mayer, Hintz described
papillary ridges of the feet.
In the early years of 19th century, Purkinje classified epidermal patterns
of fingers into nine configurations of Rugae and Sulci on the terminal phalanges
of fingers. SirFrancis Galton, in the year 1890 pointed out that the complex
pattern of parallel ridges and furrows of fingers and palms remain unchanged

8
throughout life, thus making finger prints areal means of personal
identification.13
Dermatoglyphic patterns has now been increasingly analyzed to establish
its importance in clinical medicine. Though interest in the study of epidermal
ridges in relation to clinical medicine increased during the later part of 17th
century, progress in the study was slow due to absence of a well defined
classification.
Systematic and well defined classification of the epidermal ridge pattern
of fingers, palms and soles was given by Sir Francis Galton in 1892. He
developed a subject on good scientific basis which we now know as
dermatoglyphics. It was Harold Cummins who first started making use of
epidermal ridge patterns of palms and fingers in clinical medicine. In 1936 he
reported that patients with Downs syndrome showed characteristic
dermatoglyphic patterns.21
Holt reported that the total epidermal ridge count was determined by the
cumulative effect of genes. Abnormal dermatoglyphics pattern has been
established in Trisomy 13 and 18 by Holt. It is found that dermatoglyphic
patterns are under genetic control. There are reports of fingers and palm
epidermal ridge pattern studies in relation to inherited chromosomal disorders
such as Wilson’s disease, Mental Retardation, Leukaemia, Congenital heart
diseases and Indian Childhood cirrhosis.22

9
EMBRYOGENESIS OF DERMAL RIDGES
Dermal ridge differentiation takes place early in fetal development. The
resulting ridge configurations are genetically controlled and influenced by
environmental factors. The final epidermal ridge patterns of an adult are found
to be intimately related to the fetal volar pads because epidermal ridge patterns
form at the sites of these volar pads.
Fetal volar pads have mound-shaped elevations of mesenchymal tissue
above the proximal ends of the distal phalanges on each finger, in each
interdigital area, in the thenar and hypothenar areas of the palms and soles and
in the calcar region of the sole. The development of these pads is first visible on
the fingertips during 6th to 7th week of embryogenesis. The pads become very
prominent during the subsequent weeks, decrease in size during the 5th month
and disappear completely in the 6th month. The presence of volar pads, as well
as their size and location are responsible for the configuration of papillary ridge
patterns17.
4-6 weeks: Early lines develop; arm buds appear, hands and feet develop, digits
separate.
6-8 weeks: Volar Pads appear in the following order: III, IV interdigital areas,
central palmar area, digital apex, thenar and hypothenar, proximal phalanges.

10
10-12 weeks: Beginning of volar pad regression, ridges appear at dermo-
epidermal junction.
13 weeks: Ridge formation increases, identifiable configurations noted on skin
surfaces.
21 weeks: Definite epidermal ridge patterns formed by this time.
The epidermal ridge patterns are formed only after the sixth intrauterine
month when the glandular folds are fully developed and after the sweat gland
secretion and keratinization have begun. At this time, the configurations on the
skin surface start to develop to reflect the underlying patterns. The surface
epidermal furrows correspond to the furrow folds of the stratum germinativum
and each epidermal ridge is develops above a glandular fold. Ridge
differentiation progresses from the apical region of digits proximally and in a
radio-ulnar, tibio-fibular direction. The embryogenesis of the epidermal ridges
on the feet is identical to that of the hand, except that each step occurs 2 or 3
weeks later.
Several hypotheses have been postulated regarding the factors that are
responsible for the development of specific ridge patterns. It was speculated that
the epidermal ridge configurations were the result of physical and topographic
growth forces23. It is believed that the tensions and pressures in the skin during
early embryogenesis determine the directions of the epidermal ridges. Some
workers believed that the finger tip epidermal patterns depended on the

11
arrangement of underlying peripheral nerves, while others suggested that the
ridges followed lines of greatest convexity of the embryonic epidermis.
The” present knowledge concerning the” formation “of glandular folds
and in turn the formation of epidermal ridges” was made” based on
observations” of arrangements of the blood vessel – nerve pairs under the
smooth corium border of epidermis which exists shortly before the formation of
the glandular folds24. It has been proved that insufficient”supply of oxygen to
the tissues”, defects” in the formation and distribution of sweat glands,
disturbances in proliferation of the epithelial basal layer and defects in
keratinization of the epithelium are the other factors that may influence
epidermal ridge patterns. Even environmental factors such as external pressure
on the fetal volar pads and fetal movements particularly finger” movements
influences ridge formation.
There is wide agreement that the mechanism of inheritance of many
dermatoglyphic patterns is due to the polygenic system with each gene
contributing a small additive effect. Examples of these dermatoglyphic traits are
the transversality of the ridges on the palm25,26, the a-b ridge count27,28,and the
atd angle29.
Information on the loci that influence dermatoglyphics is still uncertain
but various reports implicate chromosome 21 in the determination of finger
ridge count30,31and the position of the axial triradius31. Other chromosomal loci

12
of genes determining dermatoglyphics include the X chromosome32,33 and
chromosome1834.
Recently, it has been reported that exogenous environmental factors, such
as rubella infection may also derange dermatoglyphics and so can be helpful in
providing evidence of such an exposure in the fetal period.35-37
Figure No. 1. The development of epidermal ridges.

13
METHODS OF RECORDING DERMATOGLYPHICS
Dermatoglyphic patterns are seen by the naked eye preferably with a
magnifying lens, “but permanent impressions are necessary for quantitative
“analysis.
“To enhance the quality of the prints, it is necessary to remove sweat, oil
and dirt from the skin by washing the ridged areas with soap and water and with
ethyl alcohol or ether. Care must be taken to print the ridged areas completely
by rolling the digits, palms, and soles to ensure obtaining a” print of the whole
pattern.38
STANDARD METHODS
Ink Method:
“It is the standard method used by law enforcement agencies for
identification purposes”. The necessary “equipment consists of printer’s ink, a
roller, a glass or metal inking slab, a sponge rubber pad, and good quality
paper”. After the area is inked perfectly, the palm is rolled over a paper covered
cylinder” to avoid imperfect printing of hollow areas39”.
Inkless method:
This method makes use of a commercially available patented solution and
specially treated sensitized paper. The “method is suitable for printing hands or

14
feet with well-demarcated dermal patterns, such as those of older children
andadults40.”
Transparent Adhesive Tape Method:
In this method, the print is produced by applying a dry colouring pigment
to the skin and lifting it off with the transparent adhesive tape. The colouring
agent may be coloured chalk dust, Indian ink, standard ink, carbon paper,
graphite stick or powdered graphite, common oil pasted crayon etc. This
method is inexpensive, rapid and easy to use with all types of patients. Prints are
clear and not smudged. They can be preserved for an indefinite period of time41.
Photographic method:
This technique is based on the principle of frustrated total internal
reflection which occurs when an object is pressed against a prism. The
magnified image is photographed by a Polaroid camera. It needs relatively
expensive equipment. Recently, even ordinary photographic method has been
tried out42.
Special methods:
These methods are not widely used. However, they may have some
advantages that the standard methods cannot offer, such as allowing the study of
the correlation between the epidermal patterns and the underlying bone
structures (radio/dermatography)43, study of sweat pores
(hygrophotography)44,or study of the spatial shape of ridged skin areas, for eg,
in primates (plastic mould method)45.

15
In 1989, some authors have developed a method wherein the
investigating region is blackened with graphite smeared on a piece of cardboard.
The print is taken by the Tesa film and then adhered to a transparent film strip
or photo printing foil. Such a negative could be enlarged five to six times. An
automatic apparatus for taking finger prints without ink and also to count ridge
numbers between any 2 given points was developed in 199046.
Technologies have been improved in the finger print identification. With
a single small chip, technology provides the basis for fingerprint identification
devices that can prove the users identity using a fingerprint. Optical fingerprint
scanner is a device for computer security featuring superior performance,
accuracy, durability based on unique NITGEN fingerprint Biometric
Technology.
“DERMATOGLYPHIC PATTERN CONFIGURATIONS47:”
“Numerous investigators have proposed rules, principles and definitions
that allow reliable analysis of dermatoglyphic data. The widespread interest in
this field and a need for a standardized dermatoglyphic terminology stimulated
an international symposium. As a result, “A Memorandum on Dermatoglyphic
Nomenclature” was published in 1968. The memorandum listed and defined
dermatoglyphic features, outlined accepted methods of dermatoglyphic analysis
and provided a nomenclature that was intended to serve as a universal
standard.”

16
Ridge detail (Minutiae):48
“The intricate details of ridge structure, termed minutiae by Galton, are highly
variable and their number, type, shape and position are unique to the individual.
The minutiae therefore, are valuable and reliable tools for personal
identification.”
Six common types of minutiae were initially used in dermatoglyphics and
they are – Island or point, short ridge, fork, enclosure, end and interstitial line
with addition of one more type later, called comb.
Figure No. 2. The nomenclature of minutiae.

17
Finger tip Pattern Configurations2;
The ridge patterns on the distal phalanges of the fingertips are generally
categorized into following groups ;
1. Arch
2. Loop
3. Whorl
4. Composite
ARCH:
The ridges pass from one margin of the digit to the other with a gentle
distally bowed sweep which gives the name to the pattern type. It is actually
pattern less as there is no triradius and the topographic zones of the other
fingerprint type are lacking. Galton has described many types of arches
depending on the shape. These are plain arch, tented arch, arch with ring etc.
The plain arch is composed of ridges which pass across the finger with a slight
bow distally. There is no triradius.
Tented arch has a triradius located in or near the mid axis of the digit. The
erect distal radiant is associated with abrupt elevation of the transversely
curving ridges forming the tent which gives the name to the pattern15.
LOOP:
It possesses only one triradius. Instead of coursing in complete circuits as
in whorl, the ridge course around only one extremity of pattern forming the

18
head of the loop, from the opposite extremity the pattern ridges flow to the
margin of the digit. This extremity of the pattern may be considered as open. If
the loop opens to the Ulnar margin it is called an Ulnar loop (U, Lu) and if it
opens to the Radial margin it is a Radial loop(R, Lu ).
According to the flow of the ridges of loop, loops can be further differentiated
into the following types.
Plane loops: Composed of succession of ridges which regularly follow a looped
course.
Transitional loops: Present more complex pattern. These are associated with
degenerated loops.
WHORL:
The Whorl is regarded as the primitive pattern from which loops and
arches are formed, as simplification of design. The majority of ridges make
circuits around the core in the pattern area. The Whorl is completely and
continuously circumscribed by the type lines. These type lines are radiants
extending from the two triradii. This area enclosed by type lines is the pattern
area. The type lines are considered as the skeleton of the pattern. That proximal
to the pattern area is proximal transverse system and distal one is the distal
transverse system.

19
Typically Whorls have two triradii. Each triradii is placed at either side of
pattern area, where three ridge systems meet i.e.:
(1) Pattern area
(2) Proximal transverse system
(3) Distal transverse system
Whorl core is an internal feature of pattern. In a typical Whorl the core
may appear as an island, a short straight ridge, a hook shaped ridge or a circle or
an ellipse.
TYPES:
Concentric whorls- The ridges are arranged as concentric rings or ellipse
(around the core)
Spiral whorl – The ridges spiral around the core in clockwise or anticlockwise
direction.
Mixed whorl- It contains circle and ellipse or spirals in the same pattern.
Central pocket whorl- It contains a smaller whorl within a loop. It is sub
classified as Ulnar and Radial according to the side on which outer loop opens.
Lateral pocket whorl or twin loop-These types are morphologically similar,
have2 triradii. In lateral pocket whorl, both ridges emanating from each core
emerge on the same side of the pattern. In twin Loop whorl, the ridges
emanating from each core open towards the opposite of margin of the finger.

20
Accidentals (whorls) - Complex patterns, which cannot be classified as one of
the above patterns are called accidentals, they represent a combination of two or
more configurations.
COMPOSITES22:
The composites form a heterogeneous pattern. Two or more designs are
combined in one pattern area. Two or more triradii are present. There are four
types:
(1) Central pocket loops
(2) Lateral pocket loops
(3) Twin loops
(4) Accidentals
Simple Arch Tented Arch
Figure No. 3 Finger pattern Arch

21
Ulnar loop Radial loop
Figure No. 4. Finger pattern Loop
Single pocket whorl Double pocket whorl
Figure No. 5. Finger pattern Whorl
RADIANTS:
The” three basic dermatoglyphic landmarks found on the fingertip
patterns are the triradii, cores and radiants.”
The three radiants of a triradius are traced on the print “by following the ridges
which issue from the triradius.” In some triradii these rays are easily defined as
the starting points for tracing.

22
From their typical association with pattern the three radiants are named
according to their relation with the finger and with the pattern;
1. Marginal radiant passing to the digital border.
2. Distal pattern radiant distal relation to the pattern area.
3. Proximal pattern radiant proximal relation to the pattern area.
TRIRADII:
A triradius is the central meeting point of the three opposing ridge
system. In a typical whorl or loop such a point occurs at the confluence of three
topographic zones- the pattern area, the distal transverse system, and the
proximal transverse system. These three ridges are radiating from a common
point.
Figure No. 6. Triradii
“

23
PALMAR PATTERN CONFIGURATIONS2”
“In order to carry out dermatoglyphic analysis that can be compared
indifferent individuals, the palm has been divided into several anatomically
defined areas. The areas approximate the sites of” embryonic volar pads and
include the thenar area, four interdigital areas (designed I1 I2 I3 I4 from radial
to ulnar side)and the hypothenar area.
Figure No. 7. Palmar pattern configurations
“Palmar flexion Creases49”
“Flexion creases represent the location of firmer attachment of the skin to
indulging structures. Although they differ in origin from the epidermal ridges
and do not belong strictly to the dermatoglyphic system, palmar creases are
usually included in routine dermatoglyphic analysis because their alterations
may be of diagnostic value in a variety of medical disorders.”

24
The palmar creases are divided “into three groups: major, minor and
secondary”creases.
1. Major creases: There are three major creases –
- The radial longitudinal crease.
- The proximal transverse crease.
- The distal transverse crease.
“The first to appear is the radial longitudinal crease that borders the
thenar eminence, followed by the proximal transverse crease (PTC) and distal
transverse crease. Sometimes the proximal and distal transverse creases are
replaced or joined into one single crease that traverses the whole palm. This
single transverse flexion crease is usually referred to as Simian crease or line.”
“Variants of single palmar crease have been noted. They are transitional
type I(proximal and distal creases connected by the bridging crease) and
transitional type2 (fusion of the transverse creases with branching proximal and
distal segments, incomplete single palmar crease). A variation in appearance of
PTC is the Sydney line (SL) after the city in Australia where it was observed
first. Sydney line represents proximal transverse crease beyond hypothenar
eminence to the ulnar margin of the palm.”

25
Figure No. 8. Palmar flexion creases
Figure No. 9. Simian crease & Sydney line

26
Figure No. 10. Palmar dermatoglyphic areas
2. “Minor creases: In addition to major creases, several minor creases are often
present on the palm.” The most commonly reported minor creases are;
a)” Three longitudinal creases running from the central part of the wrist towards
the 3rd, 4th and 5th digits.”
b) The accessory distal crease “found under the 3rd and 4th digits, beyond the
distal transverse crease.”
c) “‘E line’ located at the distal ulnar edge of the palm between the origin of the
distal transverse crease and the metacarpophalangeal creases of 5th digit.”

27
d) “A hypothenar crease in the hypothenar eminence, running in a proximal to
distal direction concave toward the ulnar side of the palm.”
3. Secondary creases: “Any visible palmar creases other than major and minor
creases. Their number, length, depth and direction vary widely in different
individuals.”For the present study, only major flexion creases are included.
RIDGE COUNT:
The characteristics of dermatoglyphics can be described quantitatively
i.e., by counting the number of ridges within a pattern and measuring angles or
distances between specified points of triradii.
The counting was done along a straight line connecting the triradii point
to the point of core. Ridge counts were recorded in order, beginning with thumb
to little finger of both right hand and left hand.

28
Figure No. 11. Ridge counting in finger patterns
The Total Finger Ridge Count (TFRC)
The TFRC was derived by adding the ridge counts on all ten fingers. In a
loop, there is one triradius and so one ridge count. In a whorl with two triradii,
there are two counts and the higher is used. Only the“ larger count was used on
those digits with more than one ridge count. For an” arch, the score is zero. For
double loop whorls, the ridge numbers between the two cores was added to the
conventional count.
“Absolute Finger Ridge Count (AFRC)”
The AFRC was calculated by summing up the ridge counts of all the“fingers.
The TFRC and AFRC are the same if no whorls are present.”

29
a-b Ridge Count :
The ridge count most frequently obtained is the a-b ridge count. Counting
was carried out along a straight line connecting the triradii ‘a’ and ‘b’. The
count excludes the ridges forming the triradii.“When an accessory triradius ‘a’
is present in the second interdigital area, counting is still done from the ‘a’
triradius which is invariably the more radial of the two.”
Figure No. 12. Method of a-b ridge count
The ‘atd’ Angle :
It was recorded by drawing lines from the digital triradius ‘a’ to the axial
triradius ‘t’ and from this to digital triradius ‘d’. In palms with more than one
triradius, the atd angle originating from each axial triradius was measured.

30
Figure No. 13. Method of measuring atd angle
CONGENITAL MALFORMATIONS OF DERMATOGLYPHICS
Dermatoglyphics are studied in congenital malformations and as a
physical sign in pediatrics diagnosis. It is not often recognized, that they can be
malformed also. They pass either unrecognized or abandoned as freak pattern.

31
There are five classified malformations.
1. Aplasia
2. Hypoplasia
3. Dissociations
4. Off the end
5. Off the end with ridge dissociation.
APLASIA: Congenital absence of ridges over entire palm, plantar surfaces.
Palmar, interphalangeal flexion creases remain normal or with great excess of
very small creases. It is thought to be autosomal dominantly inherited. It may be
due to disordered keratin production.
RIDGE HYPOPLASIA : Ridges are not absent but reduced in height. It is
confused with ridge atrophy seen in mental retardation, old age, celiac diseases.
It probably indicates hidden celiac diseases. It is seen in autosomal aneuploidy.
It is thought to be autosomal dominant trait.
RIDGE DISSOCIATION: Ridges instead of running neatly in parallel lines
are broken into dots, short ridges and are completely disorganized, mostly seen
on the thumb and palmar triradius, followed by index, middle, ring, and little
finger in the order of frequency. It is autosomal dominant trait or sporadically
inherited. It is confused with scarring after burns. In 430 patients with
congenital heart disease, two had this ridge dissociation. One had multiple
cardiac defects and the other had Truncus Arteriosus, VSD and harelip. It is
sometimes seen in normal people4.

32
OFF THE END RIDGES: Ridges instead of running transversely are vertical
to the end of finger tip.
OFF THE END RIDGES WITH DISSOCIATION: It is rare. No disease is
associated with it. Hypoplasia of the ridges is the commonest.
CONGENITAL HEART DISEASES
Incidence & Prevalence:
The incidence of congenital heart disease at birth is estimated to be 6 to
8per 1000 live birth in the western countries. The prevalence of congenital
cardiac lesions in India is not known. Recently it has been realized that the
incidence is higher, specially, if all of the newborns are followed up to the age
of one year, Since some of the conditions may not manifest in the first few
weeks oflife51.
INCIDENCE OF COMMON CONGENITAL CARDIAC LESIONS50
Left to right shunt
Ventricular septal defect 36%
Atrial septal defect 5%
Patent ductus Arteriosus 9%
Atrioventricular septal defect 4%
Obstructive lesions
Pulmonary stenosis 9%
Aortic stenosis 5%
Coarctation of Aorta 5%

33
Cyanotic lesions
Transposition of great vessels 4%
Tetralogy of Fallot 4%
ETIOLOGY:
It is often considered POLYGENIC INHERITENCE, in which inherited
and environmental factors combine to cause the malformation.
INHERITED OR GENETIC FACTORS:
Cardiac defects are associated with large number of chromosomal and
genetic factors, 40% of infants with Trisomy 21 have congenital heart diseases.
It is usually Atrio-ventricular defect or Ventricular septal defect52. There is high
incidence of congenital heart diseases in Trisomy13, Trisomy18 and Turner’s
syndrome is associated with left heart lesions. Some of the cardiac diseases
have autosomal inheritance. In DeGeorge syndrome inherited as autosomal
dominant, 75% of these children have cardiac (conotrucal) defects. Noonan
syndrome, Holt Orm syndrome and Williams syndrome are transmitted
autosomal dominantly have congenital heart diseases. Autosomal recessively
transmitted disorders are Pompe’s and Friedreich’s ataxia which have
congenital cardiac diseases5.
TERATOGENS:
In early pregnancy, maternal infections, illness or ingestion of certain
drug can result in cardiac abnormality. Congenital Rubella syndrome is

34
commonly associated with peripheral pulmonary stenosis or PDA. Uncontrolled
Maternal Phenyl Ketonuria is associated with heart defects. Maternal ingestion
of Lithium (Ebsteins anomaly), Phenytoin (semilunar valve stenosis, COA) are
also known to cause to CHD. Thus cardiac embryogenesis and dermatoglyphics
development and differentiation takes place at the same time (6 weeks to
18weeks). The analysis of family history will help to unravel the interplay of
genetic and environmental factors. Dermatoglyphics study can be carried out to
elucidate the significance of their presence in congenital heart disease5.
DERMATOGLYPHICS AND CONGENITAL HEART DISEASE:
Hale (1961), studied 287 pairs of palmar prints, of which 157 had CHD
and 143 as control group (NO CHD). He found that in CHD patients, the
frequency of occurrence of axial tri-radius in the distal position in
approximately double than that found in control group6. Sanchez Cascos (1964),
studied fingerprints & palmar prints of 150 congenital heart disease pts and 50
normal subjects. He reported Ulnar loops in 60 % - 70% of CHDs, of which
75% were VSD, Whorls were seen in 15 % of CHD, of which 30% were AS,
COA, TOF, Radial loops were seen in 3% of CHD. In case of palmar prints in
the same patients, Sanchez found that distal and radial displacement of axial
triradius inmost of congenital heart diseases7.
Burghat.W. Collard, (1968), studied palm prints of 98 CHD patients as
compared to 198 normal children. According to this study, single transverse
palmar crease was abnormally common. ‘atd’ angle of both hands were widened

35
in many pts with CHD owing to distal displacement of axial triradius, more in
VSD& PDA as compared to other forms of CHD8. G .S Mutalik and
Lokhandwala,(1968) studied 12 cases of CHD in which loops were more
common in ASD, whereas whorls were more common in VSD9.
Magotra and Chakraborti (1976), studied Dermatoglyphics in 50 cases of
congenital heart diseases and 100 cases of normal children. He found out that
Ulnar loops were predominant in all cases of congenital heart diseases, more so
in VSD, whorl patterns were found more in ASD & TOF, increased Arch
patterns in Pulmonary stenosis. In their data, position of axial tri-radius in
congenital heart diseases when compared with normal controls, didn’t show any
significantdifference10.
Renuka Nair (1986), studied 927 pts with CHD, 169 blood donors were
taken as normal sample for comparison. The study showed increase in
frequency of Sydney line (6-24%of in males &12- 23% in females with CHD
compared to7&10% in normal males and females respectively. Distally placed
axial triradius was more frequent in male CHD Patients. Another interesting
thing in this study was Dermatoglyphics of pts were compared with
dermatoglyphics of the parent sand they found uniform patterns in III &IV
interdigital areas11.
Brijendra Singh, (1996) studied Dermatoglyphics of 50 CHD patients
comparing them with 50 normal children dermatoglyphics. This study showed
increase in whorls (55-80%) as compared to control, Total finger ridge

36
count(TFRC) was increased in CHD pts, especially in VSD& ASD. The ‘atd’
angle was widened (distally placed ‘t’ triradius) in CHD12.
Anita Khalil, 1998, studied Dermatoglyphics in congenital heart diseases
in 50 cases as compared to 50 normal children. This study showed increased
frequency of Ulnar loop patterns and decreased frequency of whorl patterns in
male cyanotic and female cyanotic and acyanotic groups. Decrease TFRC was
significant in CHD, more so in males patients13.

37
MATERIALS AND METHODS
Study design:
Type of study: Hospital based case control study.
Duration of study: March 2014 – August 2016
Source of Data:
The study was carried out at Institute of Child Health and Research Centre,
Madurai Medical College, Madurai.
Inclusion Criteria:
Children having congenital heart diseases (cyanotic and acyanotic) proven by
echo-cardio graphy were included in the study.
Exclusion criteria
1. Children having doubtful congenital heart diseases.
2. Children having acquired heart diseases.
3. Children having deformities of the hand.
METHODS
Dermatoglyphics are studied in 100 children with congenital heart
diseases, both males and females, who were admitted in paediatric wards and
OPD at Institute of Child Health and Research Centre, Madurai Medical
College, Madurai. For each of congenital heart diseases child included in the
study, detailed history including consanguinity, birth order of child, drug intake

38
during prenatal period and family history of congenital heart diseases were
taken.
Electrocardiogram, X-Ray chest were obtained. A provisional diagnosis
of congenital heart disease was made and later confirmed by echocardiography.
The control group consisted of 100 healthy children, both males and
females, who were thoroughly examined clinically for any other congenital
anomalies or having acquired heart diseases. Those having them were excluded
from the study.
The dermatoglyphic patterns of palms and fingers were studied and the
information was recorded systematically
METHOD OF RECORDING DERMATOGLYPHIC PATTERNS:
The ‘INK METHOD’ was selected from the various methods described in
literature because of following advantages:
• Simple Technique.
• Low cost.
• Clarity of prints.
• Less time consuming.
MATERIALS USED:
• Camel quick drying duplicating ink.
• Rubber roller.

39
• Inking slab-thick sheet fixed over wooden support.
• Century board.
• White ‘map Litho’ paper with a glazed surface on one side.
• Pressure pad made up of rubber foam.
• Cotton puff and spirit.
• Scale.
• Pencil pen.
• Protractor- To measure the ‘atd’ angle.
• Needle with a sharp point for ridge counting.
• Magnifying lens (X5 Magnification).
• Readings on: overhead projector, scanning, computerized
magnification.
TECHNIQUE OF RECORDING DERMATOGLYPHIC PATTERNS:
PROCEDURE:
The hands of the subject are first cleaned with soap and water and dried.
Subsequently the hands are wiped with spirit lightly to remove any greasy
particles. A smaller “amount of ink is placed on the ink slab and spread with the
roller to a thin film”-not too thick or too light. The subject is made to relax,
giving the operator complete freedom in manipulations. The whole of the palm
and fingers are covered with ink using the roller directly.

40
PALMS:
Either the palm alone or palm and fingers are taken first. While inking the
following areas require special attention- the zone of flexion creases on the
wrist, the Ulnar margins, the Flexor creases where the finger join the palm and
the central hollow of the palm. After inking, the operator brings the ulnar
margins of the subject’s hand, rolled palm downwards, against the paper on the
curved pressure pad. Pressure is exerted specially over the central region of the
handover the knuckles, to ensure printing of the hallow of the palm and distal
border.
FINGERS PRINTS:
Two types of prints are taken – plain and rolled prints.
A PLAIN print is made by contact of the ball of the finger without rotation of
the finger.
A ROLLED print involves rotation of the finger both in inking and in printing.
In plain prints the details are sharp, but often incomplete and this is the reason
for rolled prints, to avoid erroneous classification. In making a rolled print, the
finger is first placed edge down on the ink film and then rolled until the
opposite margins are in contact. For ease, the thumb should be placed
downwards and rolled towards the body and the other fingers placed radial edge
downwards and rolled away from the body. Soon after the print is taken, it
should be examined for details and clarity in the different fingers and the palmar
areas. The ink is easily removed from the hand by washing with soap and water.

41
There are many inkless methods for taking prints. But for medical
purposes the above method is simple and adequate.
Further the impression is analyzed either by magnifying lens, or by
scanning and computerized reading, or by Xerox, on overhead projector, or
using compound microscope.
The prints are studied for the following features:
• Frequency of finger patterns- whorls, loops, arches etc.
• Total finger ridge count (TFRC) obtained by summing of ridges from
the core to radius of each finger and for whorls having two triradii the
larger count was considered.
• ‘a-b’ ridge count
• ‘atd’ angle measured separately for each hand.
• Presence of Simian creases and Sydney lines.

42
Figure No. 14. Materials used to record dermatoglyphic patterns
Figure No. 15. Method of recording palmar dermatoglyphic patterns

43
Figure No. 16. Right & Left hand rolled patterns

44
Figure No. 17. Measurement of left & right atd angle

45
STATISTICAL METHODS:53,54,55,56.
Data was entered into Ms excel and analyzed using SPSS v20. Qualitative
data were summarized as frequencies and percentages. Quantitative data were
checked for normality. Normally distributed data were summarized using mean
and standard deviation. Non-normally distributed data were summarized using
Median and inter-quartile range.
Interquartile range (IQR), also called the mid spread or middle fifty, or
technically H-spread, is a measure of statistical dispersion, being equal to the
difference between the upper and lower quartiles, IQR = Q3 − Q1. In other
words, the IQR is the 1st quartile subtracted from the 3rd quartile; these
quartiles can be clearly seen on a box plot on the data. It is a trimmed estimator,
defined as the 25% trimmed range, and is the most significant basic robust
measure of scale.
The interquartile range (IQR) is a measure of variability, based on dividing a
data set into quartiles. Quartiles divide a rank-ordered data set into four equal
parts. The values that divide each part are called the first, second, and third
quartiles; and they are denoted by Q1, Q2, and Q3, respectively.

46
Association between qualitative variables was tested using chi-square
test. The chi-square test for independence is used to determine the relationship
between two variables of a sample. In this context independence means that the
two factors are not related. In the chi-square test for independence the degree of
freedom is equal to the number of columns in the table minus one multiplied by
the number of rows in the table minus one.

47
Difference in distribution of quantitative variables across two groups was
tested using independent t test and Mann Whitney U test for normal and non-
normally distributed variables respectively. The Mann–Whitney U test (also
called the Mann–Whitney–Wilcoxon (MWW), Wilcoxon rank-sum test,
or Wilcoxon–Mann–Whitney test) is anon parametric test of the null
hypothesis that two samples come from the same population against
an alternative hypothesis, especially that a particular population tends to have
larger values than the other.
Statistical significance was interpreted using an arbitrary cut off p=0.005.

48
RESULTS
It is a Case-control study consisting 100 congenital heart disease patients
and 100 controls undertaken to study the pattern of dermatoglyphics in
congenital heart diseases.
In our study, it is observed that males constitute about 55% in CHD group and
57% in Control group, females 45% in CHD group and 43% in control group
respectively. It is shown in Table No.1.
Table 1: Gender distribution of study participants
Sex CHD Controls
Male 55 57
Female 45 43
Pictorial representation of gender distribution is depicted in Figure No.
Figure18 : Gender distribution among GHD and control group
As VSD is the most common CHD about 43% in our study. Of which it
occurred in about 58.1% among male children and 41.9% among female
55%45%
CHD
male
female 57%
43%
control
male
female

49
children. The second most common CHD is ASD occurred in about 29% of
children. Of which it occurred in about 51.7% among male children and 48.3%
among female children. Below table represents gender distribution of CHD.
Table2: Distribution of CHD according to gender
CHD Male N(%) Female N(%) N /%
ALCAPA 0 1(100) 1
AS 1(33.3) 2(66.7) 3
ASD 15(51.7) 14(48.3) 29
DORV 2(100) 0 2
PDA 3(75) 1(25) 4
TGV 2(50) 2(50) 4
TOF 7(50) 7(50) 14
VSD 25(58.1) 18(41.9) 43
TOF constitute about 14% of CHD children with equal distribution among both
gender. PDA occurred in about 4% of CHD children with predominance among
male children. TGV occurred in about 4% of CHD children. The incidence of
AS, DORV and ALCAPA is about 3%, 2% and 1% respectively.

50
Pictorial representation of distribution of CHD according to gender is shown
below.
Figure19: Distribution of CHD according to gender
25
15
7
32 2
10
18
14
7
10
2 21
0
5
10
15
20
25
30
VSD ASD TOV PDA DORV TGV AS ALCAPA
Number
Male Female

51
Figure20: Gender wise distribution of CHD- Component Bar diagram

52
Figure21: Distribution of CHD among cases- Pie chart
VSD is common followed by ASD among congenital heart diseases

53
Table3: Distribution of finger patterns across various CHDs
Pattern AS
Median
(IQR)
ASD
Median
(IQR)
DORV
Median
(IQR)
PDA
Median
(IQR)
TGV
Median
(IQR)
TOF
Median
(IQR)
VSD
Median
(IQR)
UL 3() 3(5) 6() 4.5(6) 4.5(7) 5.5(4) 5(2)
RL 1() 0(1) 0(1) 0.5(1) 0.5(1) 0(1)
Arches 0(1) 0.5(1) 0.5(1) 0(2) 0(1) 0(1)
Whorls 6() 6(5) 3.5() 4(5) 5(8) 2(4) 4(3)
A narrow Inter Quartile Range indicates that data are very consistent.
Table4: Comparison of finger patterns among CHD and controls
Finger
Pattern
Controls CHD P*
Median IQR Median IQR
UL 6 4 5 4 <.0001
RL 0 1 0 1 0.847
Arches 1 1 0 1 0.010
Whorls 2 3 4 5 <0.0001
In both, the cases and controls group, it is found that the majority are ulnar
loops followed by whorls and then the arches. The increase in ulnar loops and
whorls in congenital heart diseases is statistically significant with p value
<0.0001.

54
Figure22: Comparison of finger patterns among CHD and controls
Table5: Comparison of finger patterns among cases and controls- Males
Pattern Controls Cases P*
Median IQR Median IQR
UL 6 4 5 3 0.006
RL 0 1 0 1 0.276
Arches 1 1 0 1 0.002
Whorls 2 4 4 4 <0.0001
From the above table the ulnar loops, whorls and arches were statistically
significant when normal male children compared with male congenital heart
disease children. Arches were not significant.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
UL RL ARCHES WHORLS
control
CHD

55
Figure 23: Comparison of finger patterns among cases and controls- Males
Table6: Comparison of finger patterns among cases and controls- Females
Pattern Controls Cases P*
Median IQR Median IQR
UL 6 3 4 5 0.002
RL 0 1 0 1 0.330
Arches 0 1 0 1 0.639
Whorls 2 2 4 6 <0.0001
From the above table ulnar loops and whorls patterns have significant
difference when normal female children compared with female congenital heart
disease children. Arches and radial loops were not significant.
0
1
2
3
4
5
6
7
UL RL Arches Whorls
controls
cases

56
Figure24: Comparison of finger patterns among cases and controls-
Females
0
1
2
3
4
5
6
7
UL RL Arches Whorls
controls
cases

57
Figure25: 95% CI Comparing finger patterns among male and female
CHD children
This figure demonstrates the distribution of finger patterns among male
and female congenital heart disease children lying between the 95% confidence
interval.

58
Table7: Distribution of finger patterns between cyanotic and acyanotic
heart diseases
Finger
pattern
Cases N Mean Std.
Deviation
Pvalue
UL Cyanotic 20 5.10 2.553 0.193
Acyanotic 80 4.40 2.369
RL Cyanotic 20 .45 .510 0.686
Acyanotic 80 .55 .654
ARCHES Cyanotic 20 .70 1.218 0.539
Acyanotic 80 .46 .826
WHORLS Cyanotic 20 3.70 3.028 0.114
Acyanotic 80 4.59 2.589
When comparing finger patterns between cyanotic and acyanotic heart diseases
there is no statistical significance.
Figure26: Distribution of finger patterns between cyanotic and acyanotic
heart diseases
0
1
2
3
4
5
6
UL RL ARCHES WHORLS
Cyanotic
Acyanotic

59
Figure27: Prediction of CHD by Finger pattern- ROC curve

60
Table8: Prediction of CHD by finger pattern
Parameter AUC Pvalue Cut off Sensitivity Specificity
UL 0.667 <0.0001 6.5 75 44
RL 0.507 0.864
Arches 0.594 0.021 0.5 63 51
Whorls 0.723 <0.0001 2.5 71 63
Area under Receiver Operating Characteristic curve is significant predictor of
CHD for Ulnar loop and Whorl pattern with significant p-value.

61
Table9: Comparison of dermatoglyphic patterns among cases and controls
Parameter Group Mean Std. Deviation P value
atdRT Controls 37.10 2.740 <0.0001
Cases 47.65 7.161
atdLT Controls 37.97 3.365 <0.0001
Cases 47.58 5.802
TFRC Controls 122.28 18.830 <0.0001
Cases 164.59 33.879
abRT Controls 33.07 3.397 <0.0001
Cases 37.64 5.112
abLT Controls 33.94 3.623 <0.0001
Cases 38.11 3.864
In my study, the atd angle in right and left hand, a-b ridge count in right
and left hand and total finger ridge count of congenital heart disease children
were significantly increased when compared to the normal children. Axial
triradius is distally placed in congenital heart disease children than controls.

62
Figure 28: Comparison of dermatoglyphic patterns among cases and
controls
0
10
20
30
40
50
60
controls cases
atd RT
atd RT
0
10
20
30
40
50
controls cases
atdLT
atdLT
30
31
32
33
34
35
36
37
38
controls cases
abRT
abRT
31
32
33
34
35
36
37
38
39
controls cases
abLT
abLT

63
Figure29: 95% CI Comparing dermatoglyphic patterns among cases and
controls
This figure demonstrates the distribution of dermatoglyphic patterns
among cases and controls lying between the 95% confidence interval.
0
50
100
150
200
controls cases
TFRC
TFRC

64
Table10: Comparison of dermatoglyphic patterns among cases and
controls- Male
parameter Group Mean Std. Deviation P value
atdRT Controls 37.39 2.569 <0.0001
Cases 47.93 5.805
atdLT Controls 38.25 3.587 <0.0001
Cases 48.45 4.780
TFRC Controls 117.61 19.427 <0.0001
Cases 170.02 31.873
abrt Controls 33.16 3.110 <0.0001
Cases 38.25 5.289
ablt Controls 33.72 3.483 <0.0001
Cases 38.49 4.149
From the above table, the atd angle in right and left hand, a-b ridge count
in right and left hand and total finger ridge count of male congenital heart
disease children were significantly increased when compared to the normal
male children.
Figure 30: Comparison of dermatoglyphic patterns among cases and
controls- Male

65
0
10
20
30
40
50
60
controls cases
atdRT
atdRT
0
10
20
30
40
50
60
controls cases
atdLT
atdLT
30
31
32
33
34
35
36
37
38
39
controls cases
abRT
abRT
31
32
33
34
35
36
37
38
39
controls cases
abLT
abLT
0
20
40
60
80
100
120
140
160
180
controls cases
TFRC
TFRC

66
Table11: Comparison of dermatoglyphic patterns among cases and
controls-Female
Parameter group Mean Std. Deviation P value
atdRT Controls 36.72 2.938 <0.0001
Cases 47.31 8.591
atdLT Controls 37.60 3.048 <0.0001
Cases 46.51 6.751
TFRC Controls 128.47 16.244 <0.0001
Cases 157.96 35.410
abrt Controls 32.95 3.779 <0.0001
Cases 36.89 4.839
ablt Controls 34.23 3.822 <0.0001
Cases 37.64 3.472
From the above table, the atd angle in right and left hand, a-b ridge count
in right and left hand and total finger ridge count of female congenital heart
disease children were significantly increased when compared to the normal
female children.

67
Figure 31: Comparison of dermatoglyphic patterns among cases and
controls-Female
0
5
10
15
20
25
30
35
40
45
50
controls cases
atdRT
atdRT
0
5
10
15
20
25
30
35
40
45
50
controls cases
atdLT
atdLT
30
31
32
33
34
35
36
37
38
controls cases
abRT
abRT
32
33
34
35
36
37
38
controls cases
abLT
abLT
0
20
40
60
80
100
120
140
160
180
controls cases
TFRC
TFRC

68
Figure32: 95% CI Comparing dermatoglyphic patterns among male and
female CHD children
This figure demonstrates the distribution of dermatoglyphics patterns among
male and female congenital heart disease children lying between the 95%
confidence interval.

69
Figure33: 95% CI Comparing TFRC among male and female CHD
children
This figure demonstrates the distribution of TFRC patterns among male
and female congenital heart disease children lying between the 95% confidence
interval.

70
Table12: Distribution of dermatoglyphic patterns between cyanotic and
acyanotic heart diseases
Pattern
Group N Mean Std.
Deviation
Pvalue
atdRT Cyanotic 20 48.75 10.442
Acyanotic 80 47.38 6.136 0.445
atdLT Cyanotic 20 45.50 4.707
Acyanotic 80 48.10 5.957 0.073
TFRC Cyanotic 20 165.50 39.347
Acyanotic 80 164.36 32.646 0.894
abrt Cyanotic 20 38.05 4.796
Acyanotic 80 37.54 5.212 0.691
ablt Cyanotic 20 38.50 4.123
Acyanotic 80 38.01 3.817 0.616
From the above table, there is no significant change in the atd angle in
right and left hand, a-b ridge count in right and left hand and total finger ridge
count of acyanotic congenital heart disease children when compared with
cyanotic congenital heart disease children.

71
Figure34: Distribution of dermatoglyphic patterns between cyanotic and
acyanotic heart diseases
Table13: Distribution of dermatoglyphic patterns across various CHDs
Pattern AS
Median
(IQR)
ASD
Median
(IQR)
DORV
Median
(IQR)
PDA
Median
(IQR)
TGV
Median
(IQR)
TOF
Median
(IQR)
VSD
Median
(IQR)
atdRT 42() 44(6) 42.5() 52(21) 52(31) 44.5(7) 48(9)
atdLT 49() 45(7) 45() 51.5(14) 46(11) 46(11) 49(7)
TFRC 198 172(4
6)
175() 183.5(59
)
167(10
8)
180.5(6
3)
163(29)
a-bRT 37() 37(4) 33.5() 39(8) 34(11) 37(6) 37(6)
a-bLT 39() 37(7) 33.5 40(7) 36.5(7) 39(4) 37(5)
A narrow Inter Quartile Range indicates that data are very consistent.
0
20
40
60
80
100
120
140
160
180
atdRT atdLT TFRC abRT abLT
cyanotic
acyanotic

72
Figure35: Prediction of CHD by Dermatoglyphics- ROC curve
Table14: Prediction of CHD by Dermatoglyphics
Parameter AUC Pvalue Cut off Sensitivty Specificity
TFRC 0.878 <0.0001 130 88 67
ATD- R .958 <0.0001 40.5 92 88
ATD-L .932 <0.0001 40.5 92 78
AB-R .775 <0.0001 34.5 74 71
AB-L .803 <0.0001 35.5 75 75
Area under Receiver Operating Characteristic curve is significant predictor of
CHD for all dermatoglyphic patterns with significant p-value.

73
Table15 : Presence of simian crease and Sydney line among cases and
controls
Creases Controls Cases
N % N %
Simian
crease
0 0 1 100
Sydney
crease
1 50 1 50
Occurrence of Simian creases in the cases (1%) of CHD group, so a
larger sample is required to ascertain the significance. Sydney line in the cases
and controls is almost similar with no statistical significance.

74
DISCUSSION
The association of altered dermatoglyphic patterns with various
congenital disorders including congenital heart disease was well known, as
reported by several workers. In this section an attempt is made to compare the
observations seen in our study with previous studies conducted to compare the
dermatoglyphic patterns in congenital heart diseases in children.
Finger tip patterns:
The present study showed increased numbers of Whorls and decreased
numbers of Arches in patients with congenital heart diseases which were in
agreement with the studies conducted by Mutalik et al (1968)9, M.L. Magotra
etal (1976)10, Brijendra Singh et al (1996)12
Comparison of finger print patterns in congenital heart diseases
Name of the study
No of
cases
Ulnar
loops
Radial
loops
Whorls Arches
Present study (2016) 100 +* X +* _*
Mutalik et al9 (1968) 12 X X +* _*
Magotra et al10 (1976) 50 X + +* _*
Brijendra et al10
(1996)
50 + X +* _*
(+) Increased, (-) decreased, (x) no significant change, (*) statistically
significant

75
Further analysis of the finger patterns shows, increased Whorls in both
males and females of congenital heart diseases group, which is different from
the Anita Khalil et al study (1998)13 which showed decreased whorls in both
males and females of congenital heart diseases. Most of the study did not show
any statistical significance between the male and the female group of the
congenital heart diseases.
The ‘atd’ angle :
In the present study the ‘atd’ angle was increased in both right and left
palms of the congenital heart disease patients due to distal placement of tri
radius when compared o normal children, which correlates with many studies
done previously like Alfred Hale et al6 study, Sanchez Cascos et al7 study,
Burghat Collard et al8 study, Brijendra Singh et al12 study.
Study No of cases
Increased ‘atd’ angle
Right Left
Present study (2016) 100 Present Present
Alfred Hale et al (1961) 143 Present Present
Sanchez Cascos et al (1964) 150 Present Present
Burghat Collard et al (1968) 98 Present Present
Brijendra Singh et al (1996) 50 Present Present

76
Total finger ridge count (TFRC)
In present study, TFRC is increased in congenital heart diseases as
compared to controls which correlates with Brijendra Singh et al study, whereas
Anita Khalil et al13 study showed decreased in TFRC in all congenital heart
diseases.
Comparison of TFRC in different studies
Study TFRC in different studies
Present Study (2016) Increased, p=0.001(p<0.05)
Brijendra Singh et al (1996) Increased, p=0.001(p<0.05)
Anita Khalil et al (1998) Decreased, p=0.003(p<0.05)
a - b ridge count:
In our present study, a - b ridge count both in right and left hand is found
to have increased in congenital heart disease children which is statistically
significant. Interestingly a-b ridge count is found to have no statistically
significance in the Alter M et al2 study (1967), and Anita Khalil et al study13
(1998).
So a study on a larger sample is required to ascertain the findings.

77
Simian crease and Sydney line:
In our study, Simian crease and Sydney line were found to have no
significant change in cases as compared to the controls which is consistent with
Renuka Nair et al11 study, Anita khalil et al13 study.
Name of the Study No of cases Simian crease Sydney line
Present Study (2016) 100 Not signicant Not signicant
Renuka Nair et al (1985) 927 Not signicant Not signicant
Anita khalil et al (1998) 50 Not signicant Not signicant

78
CONCLUSION
The dermatoglyphic patterns of 100 congenital heart diseases patients
have been studied and compared with those of 100 normal control children.
Increased number of Whorls and decreased number of Arches are seen in the
congenital heart disease children. Total finger ridge counting (TFRC) is
increased in congenital heart diseases children, both male and female children.
Distal placement of axial triradius is seen in congenital heart disease patients,
with increase in the ‘atd’ angle.
The above parameters may help as a diagnostic aid in diagnosis of
congenital heart diseases in children. They may also help in distinguishing
congenital heart diseases from the functional and acquired heart diseases.‘ a–b’
ridge count is found to have significant difference when compared between the
congenital heart disease group and the normal control group. But as there are
other studies in which there is no significant difference in ‘a-b’ ridge count
when compared between the congenital heart disease group and the normal
control group, a larger sample study is required to ascertain the value of this
dermatoglyphic parameter as a diagnostic tool in congenital heart diseases in
children.

79
SUMMARY
Dermal ridge differentiation takes place during fetal development. Hence
the resulting ridge configurations are genetically determined and influenced by
prenatal insult during the period of formations of these ridges, which can be
studied by method of dermatoglyphics. Thus dermatoglyphics is helpful as a
diagnostic aid in diseases which have a strong genetic background such as
congenital heart diseases.
Dermatoglyphics are studied in 100 children with congenital heart
diseases who were admitted in paediatric wards and OPD at Institute of
childhealth and research centre, Madurai Medical College, Madurai.
Increased number of Whorls and decreased number of Arches, are seen in
the congenital heart disease children. Total finger ridge counting (TFRC) is
increased among children with congenital heart diseases irrespective of sex.
Distal placement of axial triradius is seen in congenital heart disease patients,
with increase in the ‘atd’ angle.
Thus dermatoglyphic patterns may provide a means of identifying the
genetically determined fraction of patients of congenital heart diseases and may
also be of some diagnostic value.

80
RECOMMENDATION
(1) In this study, only palm and finger print dermatoglyphic patterns were
studied. A study of plantar prints could provide additional information.
(2) The study of dermatoglyphics of congenital heart diseases patients with
relation to the dermatoglyphics of their parents would throw further light on the
relationship between genetic influence on the causation of congenital heart
diseases and dermatoglyphic patterns.

81
BIBLIOGRAPHY
1. Standring Susan(chief editor): Gray’s Anatomy, In Skin and its appendages,
39thedition. Elsevier, Churchill Linvingstone, 2005, 174.
2. Schaumann B, Alter M. Dermatoglyphics in Medical disorders. New York:
Springer – Verlag; 1976; 27- 85.
3. Stough T R, Seely J R.: Dermatoglyphics in medicine, Clinical pediatrics,
1969; 8 (1): 32-41.
4. Alter M, Schulenburg A.: Dermatoglyphics analysis as a diagnostic
medicine, Birth defects, 1969; 5(3): 103-105.
5. Goldmuntz.E, Clarke B J, Mitchell L E.: The genetic basis of pediatrics
heart diseases, Journal of American College of cardiology, 1995; 27: 289-
300.
6. Alfred Hale, John H, Philips & George E Burch.: Features of
dermatoglyphics in congenital heart disease, J A M A, 1961; 176: 41-45.
7. Sanchez Cascos A.: Finger prints in congenital heart diseases, British
Heart Journal, 1964; 26: 9-11.
8. Brurghat W, Collard P.: Dermatoglyphics in congenital heart diseases,
Lancet, 1968; 11:106.
9. Mutalik G.S and Lokhandwala V.A.: Application of Dermatoglyphical
studies in Medical diagnosis, Journal of Association of Physicians of India,
1968; 16: 925-932.

82
10.Magotra M L & Chakraborti N C.: Dermatoglyphics in Clinical practice,
JInd Ped, 1976; 13:355-358.
11.Nair Renuka R.: Dermatoglyphics diversity in congenital heart defects”
Indian Journal of Medical research, 1986; 83: 56-57.
12.Singh Brijendra, Jain Longia, Thomas Kumar P.: Dermatoglyphics in
congenital heart diseases, 1996; 45:111-117.
13.Khalil Anita, Gera Rani, Bhuwalka Ashoka, Bharadwaj Shashi.: Asian
journal of Pediatric practice, 1998; vol1, no 49:53.
14.Lockard joanS.,Arthur A.Ward jr., Epilepsy –A Window to brain
mechanism1916
15.Cummins H & Mildo C.: Finger prints, palms and soles. An introduction to
dermatoglyphics, Dover publication. INC, New York, 1961:36-48.
16.Herschel w J: The origin of finger printing, American J Phys Anthropology,
1978; 48: 21-28.
17.Bonnievie K: Studies on the Papillary pattern of human fingers,
Genetics,1924: 15:1-23.
18.Uchida I A, Soltan H C.: Evaluation of dermatoglyphics in medical
Genetics, Pediatric Clinics of N America, 1963; 10:409-422.
19.David T J: Congenital malformations of human dermatoglyphics, Arch dis
child, 1976; 48:191-198
20.Cummins H, Leebe S, McClure K.: Bimanual variation in palmar
dermatoglyphics, American J anatomy, 1931; 48:199.

83
21.Holt S B, Lindstein J.: Dermatoglyphics Anomalies in Turner’s syndrome,
Ann Hum Gene, 1976; 28:87.
22.James R.Miller & Jean Girous.: Dermatoglyphics in pediatrics Practice
Med Progress, 1969: 2: 302-310.
23.Cummins H. The topographic history of the volar pads in the human embryo.
Contr Embryol Carneg Inst (Wash) 1929 ; 20 : 103.
24.Hirsch W, Schweichel JU. Morphological evidence concerning the problem
ofskin ridge formation. J Ment Defic Res 1973 ; 17: 58.
25.Pons J: Genetics of bilateral asymmetry of palmar main line transverseness.
Proceedings of the II International Congress of Human Genetics 3: 1503,1963
26.Glanville EV: Heredity and line A of palmar dermatoglyphics. Amer J Hum
Genet 17: 420, 1965
27.Fang TC: A comparative study of the a-b ridge count on the palms of mental
defectives and the general British population. J Ment Sci 95: 401, 1949
28.Pons J: Genetics of the a-b ridge count on the human palm. Ann Hum Genet
37:273, 1964
29.Penrose LS: The distal triradius t on the hands of parents and sibs of mongol
imbeciles. Ann Hum Genet 19: 10, 1954
30.Holt SB: Finger-print patterns in mongolism. Ann Hum Genet 27: 279, 1964
31.Penrose LS, Delhanty JPA: Familial Langdon- Down anomaly with
chromosomalfusion. Amer J Hum Genet 25: 243, 1961
32.Alter M: Is hyperploidy of sex chromosomes associated with reduced total

84
fingerridge count? Amer J Hum Genet 17: 473, 1965
33.Penrose LS: Medical significance of finger-prints and related phenomena
BritMed J 2: 321,1968
34.De Grouchy J: Chromosome 18: A topological approach. J Pediat 66: 414,
1965
35.Alter M, Schulenberg R: Dermatoglyphics in the rubella syndrome. JAMA
197:685,1966
36.Achs R, Harper RG, Siegel M: Unusual dermatoglyphic findings associated
withrubella embryopathy. New Eng J Med 274: 148. 1966
37.Purvis-Smith SG, Menser MA: Dermatoglyphics in adults with congenital
rubella.Lancet 2: 141, 1968
38.Taking Dermatoglyphics prints a self instruction manual. Department of
medical Genetics, Indiana University school of Medicine, Indiana Polis,
USA
2002
39.Purvis-smithS.G. Finger and palm printing technique for clinician.Medical
journalof Austria,1969;2;189 as quoted by schuamen and alter,1976
40.Walker NF. The use of dermal configurations in the diagnosis of
mongolism.JPediatr 1957 ; 50 : 19.
41.Book JA. A finger print method for genetical studies. Hereditas 1948 ;
34:368.
42. Harrick NJ. Fingerprinting via total internal reflection. Philips Tech Rev

85
1962–1963 ; 24 : 271.
43. Poznanski AK, Gall JC, Garn SM. Radiodermatography. Simultaneous
demonstration of dermatoglyphics and osseous structures in the hands.
Invest
Radiol 1969 ; 4: 340.
44. Sivadjian J. Application de l’hygrophoto/graphie aux etudes
dermatogiyphiques.Dermatologica 1970 ; 140: 93
45. Sutarman, Thomson ML. A new technique for enumerating active
sweatglands inman. J Physiol (Lond) 1952 ; 117 : 51.
46. Trauring M. Automatic comparison of finger ridge patterns. Nature 1963;
197 :938.
47. Holt SB. The Significance of dermatoglyphics in Medicine. Clinical
Pediatrics.1973; 471 – 484.
48. Penrose LS. Memorandum on dermatoglyphic nomenclature. Birth defects.
1968;4(3): 1.
49. Alter M. Variation in Palmar Creases. Am J Dis Child 1970; 120 : 424.
50.Johnson M.C. Payne R.M, Grant J W, Strauss A W.: The genetic basis of
pediatrics heart diseases, Ann Med, 1995; 27:289-300.
51.Bahl V K: Non –coronary cardiac interventions, Registry of India, Indian
Heart Journal, 1997, 49: 97-101.
52.Rath Aeibes, Rita G Harper.: Dermatoglyphics summary and evaluation in
specific syndromes, American J Obst Gynaec, 1968; 101:1006.

86
53.Bernard Rosner (2000), Fundamentals of Biostatistics, 5th Edition, Duxbury,
page80-240
54.Robert H Riffenburg (2005), Statistics in Medicine, second edition,
Academicpress. 85-125.
55.Sunder Rao P S S , Richard J : An Introduction to Biostatistics, A manual for
students in health sciences , New Delhi: Prentice hall of India. 86-160
56.John Eng (2003), Sample size estimation: How many Individuals Should be
Studied? Radiology 227: 309-313

87

88
PROFORMA
Dermatoglyphics in congenital heart diseases in children
NAME: DOA:
AGE: DOE:
SEX: I.P/O.P:
Mother’s Education:
Father’s Education:
ADDRESS:
Presenting complaints:
History of present Illness:
Repeated respiratory infections:
Breathlessness:
Cyanosis:
Feeding difficulties:

89
Edema:
Past History:
Family History:
Antinatal History:
Consanguineous / non Consanguineous:
Mother’s age at birth of child:
Father’s age at the birth of the child:
Birth order of child:
History of drug intake during pregnancy:
History of Exanthematous Fevers:
Histroy of exposure to X-rays:
History of oral pills:
History of smoking:
Natal History:
Post natal History:
Developmental History:
Immunization history:

90
General Examination:
Anthropometry:
Cardiovascular system:
Major findings:
HR
RR
Cyanosis
Clubbing
Pedal Edema
Cardiac auscultation:
Respiratory system:
Abdomen:
CNS:
Congenital anomalies:
X-ray chest:
ECG:

91
Clinical diagnosis:
Echocardiography Diagnosis:
RECORD OF DERMATOGLYPICS
FINGER PATTERNS
Right hand rolled prints
Thumb Index Middle Ring Little
Left hand rolled prints
Thumb Index Middle Ring Little

92
TOTAL FINGER RIDGE COUNT:
SIMIAN CREASE:
SYDNEY LINE:
‘atd’ ANGLE:
a-b Ridge count:
KEYNOTE TO MASTER CHART
CHD Congenital heart diseases
UL Ulnar loop
RL Radial loop
atd Rt atd angle right side
atd Lt atd angle left side
TFRC Total finger ridge count
a–b RC Rt a-b ridge count right side
a–b RC Lt a-b ridge count left side
M Male
F Female
VSD Ventricular septal defect
ASD Atrial Septal defect
PDA Patent ductus Arteriosus

93
TOF Tetra logy of Fallot
COA Coarctation of Aorta
MS Mitral Stenosis
DORV Double outlet right ventricle
TGV Transposition of great vessels
ALCAPA Abnormal origin of left coronary artery from pulmonary artery

94
MASTER CHART
Normal children (control group) n=100
S.
NO SEX UL RL Arches Whorls
atd
RT
atd
LT TFRC
a-b
RC
RT
a-b
RC
LT
Simian
crease
Sydney
crease
1 M 6 4 0 0 35 32 121 33 32 0 0
2 M 8 1 0 1 32 39 123 34 36 0 0
3 M 6 0 1 3 33 35 119 22 21 0 0
4 M 7 2 1 0 38 40 120 33 35 0 0
5 M 5 0 0 5 39 40 136 33 31 0 0
6 M 8 0 0 2 41 41 132 34 37 0 0
7 M 7 0 1 2 39 41 112 36 37 0 0
8 M 10 0 0 0 39 41 97 37 33 0 0
9 M 4 1 1 4 32 39 127 32 34 0 0
10 M 5 1 2 2 37 39 129 32 34 0 0
11 M 7 0 3 0 33 33 78 34 33 0 0
12 M 5 1 2 2 42 43 111 34 33 0 0
13 M 9 1 0 0 37 37 116 33 33 0 0
14 M 9 1 0 0 37 40 116 34 35 0 0
15 M 4 0 2 4 37 35 97 28 36 0 0
16 M 10 0 0 0 36 36 107 34 33 0 0
17 M 9 1 0 0 39 39 124 33 32 2 0
18 M 5 0 5 0 37 42 119 35 34 0 0
19 M 4 0 2 4 37 35 92 32 33 0 0
20 M 7 1 1 1 39 39 102 33 34 0 0
21 M 2 0 0 8 34 34 128 33 33 0 0
22 M 5 0 1 4 36 38 133 35 32 0 0
23 M 9 0 0 1 36 38 107 32 33 0 0
24 M 6 0 0 4 40 38 137 35 34 0 0
25 M 6 0 3 1 37 42 94 32 33 0 0
26 M 6 0 0 4 37 32 127 34 34 0 0
27 M 0 0 0 10 41 41 129 33 33 0 0
28 M 4 0 1 5 43 42 135 32 33 0 0
29 M 4 0 0 5 38 39 132 35 37 0 0
30 M 7 0 1 2 38 49 117 36 33 0 0
31 M 7 0 1 2 38 39 144 26 30 0 0
32 M 4 0 1 5 40 40 133 30 32 0 0
33 M 9 0 0 1 43 43 127 33 32 0 0
34 M 8 0 1 1 39 30 123 34 36 0 0
35 M 3 1 0 6 38 36 138 32 34 0 0
36 M 4 0 0 6 38 36 83 28 30 0 0
37 M 2 1 0 7 36 35 107 29 31 0 0
38 M 7 0 1 2 36 40 133 28 32 0 0

95
S.
NO SEX UL RL Arches Whorls
atd
RT
atd
LT TFRC
a-b
RC
RT
a-b
RC
LT
Simian
crease
Sydney
crease
39 M 3 0 1 6 36 36 118 37 35 0 0
40 M 8 0 1 1 37 35 76 34 34 0 0
41 M 7 1 0 2 37 33 126 33 34 0 0
42 M 3 0 1 6 37 38 142 32 33 0 0
43 M 8 0 0 2 32 38 138 36 32 0 0
44 M 3 4 2 1 42 40 142 37 35 0 0
45 M 5 0 5 0 33 35 68 37 43 0 0
46 M 9 0 1 0 40 43 136 40 42 0 0
47 M 9 0 1 0 36 38 124 33 34 0 0
48 M 4 2 3 1 40 42 136 36 32 0 0
49 M 9 0 0 1 35 36 112 36 36 0 0
50 M 5 1 2 2 38 40 97 38 37 0 0
51 M 8 0 1 1 38 32 102 32 30 0 0
52 M 4 0 1 5 36 37 124 32 32 0 0
53 M 7 1 0 2 38 43 87 30 26 2 0
54 M 10 0 0 0 35 35 143 32 33 0 0
55 M 3 1 0 6 38 36 136 35 32 0 0
56 M 3 4 2 1 38 43 69 29 43 0 0
57 M 7 2 1 0 38 42 123 38 41 0 0
58 F 3 0 5 2 41 41 137 34 39 0 0
59 F 3 0 5 2 41 41 138 32 33 0 0
60 F 9 0 1 0 37 36 98 32 33 0 0
61 F 8 2 0 0 40 34 136 31 36 0 0
62 F 5 1 2 2 28 32 126 28 29 0 0
63 F 4 0 0 6 39 42 116 38 37 0 0
64 F 5 0 0 5 38 34 97 30 32 0 0
65 F 7 0 0 3 36 34 116 24 28 0 0
66 F 8 0 1 1 42 38 108 34 32 0 0
67 F 9 0 1 0 42 47 138 34 38 0 0
68 F 8 2 0 0 33 38 134 38 40 0 0
69 F 6 1 0 3 32 37 128 30 24 0 0
70 F 9 0 0 1 36 34 163 34 35 0 0
71 F 8 0 0 2 36 38 123 31 33 0 0
72 F 6 0 0 4 37 38 118 35 37 0 0
73 F 6 0 3 1 35 37 102 32 33 0 0
74 F 5 1 2 2 34 35 127 38 35 0 0
75 F 9 0 0 1 36 34 123 34 35 0 0
76 F 4 1 1 4 37 39 142 40 36 0 0
77 F 7 0 0 3 37 39 121 36 39 0 0
78 F 10 0 0 0 40 41 147 32 33 0 0
79 F 6 1 0 3 34 35 128 30 24 0 2
80 F 8 0 1 1 37 41 119 36 32 0 0

96
S.
NO SEX UL RL Arches Whorls
atd
RT
atd
LT TFRC
a-b
RC
RT
a-b
RC
LT
Simian
crease
Sydney
crease
81 F 5 3 0 2 40 40 120 28 32 0 0
82 F 4 0 0 6 42 43 129 32 33 0 0
83 F 3 0 2 5 37 39 129 39 42 0 0
84 F 8 1 0 1 38 40 148 35 33 0 0
85 F 5 3 0 2 39 40 129 28 32 0 0
86 F 8 0 2 0 39 40 112 30 34 0 0
87 F 5 2 0 3 35 35 146 40 35 0 0
88 F 6 1 0 3 34 38 113 28 32 0 0
89 F 6 0 0 4 36 38 127 34 37 0 0
90 F 4 0 0 6 33 38 134 36 40 0 0
91 F 5 3 1 1 39 40 123 28 32 0 0
92 F 7 0 3 0 36 37 133 32 34 0 0
93 F 5 1 3 1 33 36 112 30 33 0 0
94 F 5 1 0 4 34 35 120 33 33 0 0
95 F 8 1 0 1 37 33 133 29 35 0 0
96 F 4 1 1 4 37 37 178 33 33 0 0
97 F 6 1 1 2 36 37 121 34 39 0 0
98 F 8 1 1 0 35 35 157 33 35 0 0
99 F 5 1 2 2 36 37 129 31 34 0 0
100 F 4 3 0 3 35 34 146 41 41 0 0

97
MASTER CHART
Congenital heart disease (case group) n=100
S.
NO Sex CHD UL RL Arches Whorls
atd
RT
atd
LT TFRC
a-b
RC,
RT
a-b
RC,
LT
Simian
crease
Sydney
crease
1 M TOF 5 1 0 4 44 47 187 37 43 0 0
2 M TOF 0 0 0 10 45 52 198 37 41 0 0
3 M VSD 6 0 0 4 47 49 154 33 36 0 0
4 M ASD 7 0 0 3 47 49 156 33 36 0 0
5 M VSD 6 0 0 4 47 52 154 35 36 0 0
6 M VSD 5 0 0 5 49 48 163 32 28 0 0
7 M VSD 5 1 0 4 44 51 164 31 32 0 0
8 M ASD 3 0 0 7 44 51 172 32 36 0 0
9 F VSD 7 0 1 2 44 47 184 35 36 0 0
10 M VSD 1 0 0 9 45 45 188 33 39 0 0
11 F TOF 5 1 0 4 42 45 197 36 38 0 0
12 F VSD 1 0 1 8 47 49 187 38 38 0 0
13 M TGV 0 1 0 9 53 51 147 33 34 0 0
14 M VSD 4 2 0 4 44 49 147 37 41 0 0
15 F VSD 1 0 0 9 49 47 145 27 29 0 0
16 F AS 3 1 0 6 42 44 201 37 38 0 0
17 M VSD 8 1 1 0 48 53 167 41 41 0 0
18 F VSD 8 0 0 2 55 57 137 29 35 0 0
19 F VSD 2 1 0 7 56 59 242 39 41 0 0
20 F VSD 4 0 1 5 54 63 161 43 39 0 0
21 F VSD 6 1 0 3 57 47 187 41 37 0 0
22 M VSD 5 1 0 4 61 59 143 33 37 0 0
23 M VSD 5 2 0 3 47 45 133 29 31 0 0
24 M VSD 8 0 1 1 51 49 123 37 41 0 0
25 M VSD 6 2 0 2 51 59 147 33 37 0 0
26 M ASD 7 0 1 2 45 45 179 39 41 0 0
27 F TOF 8 1 1 0 53 47 187 37 39 0 0
28 M PDA 2 0 1 7 57 59 203 39 38 0 0
29 M PDA 9 0 0 1 63 52 164 47 43 0 0
30 M ASD 6 1 1 2 51 53 145 39 43 1 0
31 F ASD 1 0 0 9 43 47 187 39 42 0 0
32 F VSD 8 0 1 1 57 61 169 33 35 0 0
33 F VSD 4 2 1 3 49 51 183 51 42 0 0
34 F VSD 0 1 0 9 53 55 163 29 31 0 0
35 F VSD 4 1 0 5 53 59 148 32 36 0 0
36 M VSD 8 0 1 1 45 44 164 43 39 0 0
37 F VSD 8 0 0 2 43 41 170 33 34 0 0
38 M ASD 2 2 0 6 46 49 166 53 47 0 0

98
S.
NO Sex CHD UL RL Arches Whorls
atd
RT
atd
LT
TFR
C
a-b
RC
RT
a-b
RC
LT
Simian
crease
Sydney
crease
39 M VSD 4 2 0 3 53 48 175 33 35 0 0
40 M ASD 1 1 1 7 53 49 187 39 37 0 0
41 M VSD 1 0 0 9 49 48 198 39 41 0 0
42 M TOF 3 1 0 6 49 49 190 39 38 0 0
43 F ASD 2 1 0 7 39 44 193 37 42 0 0
44 F ASD 1 1 0 8 49 47 190 38 35 0 0
45 F ASD 2 0 0 8 41 40 185 39 34 0 0
46 M VSD 8 0 1 1 43 41 158 35 38 0 0
47 M TOF 3 0 0 7 43 41 197 37 39 0 0
48 F VSD 6 0 0 4 47 51 176 37 37 0 0
49 M TOF 5 0 0 5 44 47 179 43 39 0 0
50 M VSD 4 0 1 6 57 48 153 43 37 0 0
51 M ASD 4 1 0 5 43 53 194 40 43 0 0
52 F ASD 2 0 0 8 44 44 154 34 36 0 0
53 M VSD 4 1 0 5 48 52 156 41 39 0 0
54 M VSD 6 1 0 3 55 48 168 39 40 0 0
55 M VSD 6 0 0 4 49 48 167 39 35 0 0
56 M VSD 3 1 0 6 58 56 187 39 41 0 0
57 F AS 7 0 0 3 42 49 178 37 39 0 0
58 M DORV 8 0 1 1 43 43 163 35 37 0 0
59 F ASD 6 0 1 3 43 44 141 37 37 0 0
60 F ASD 1 0 1 8 46 45 188 36 41 0 0
61 F ASD 3 1 0 6 37 42 137 37 38 0 0
62 M VSD 6 0 0 4 43 47 187 36 42 0 0
63 M ASD 3 1 0 6 48 47 178 37 37 0 0
64 M ASD 7 0 0 3 43 40 179 39 35 0 0
65 F TOF 8 0 1 1 43 44 123 33 34 0 0
66 M TOF 7 1 0 2 41 42 182 37 39 0 0
67 M ASD 6 0 1 3 43 44 126 43 35 0 0
68 F VSD 7 0 0 3 47 43 137 37 37 0 0
69 F TOF 3 0 5 1 47 36 83 43 38 0 0
70 F TOF 7 0 1 2 53 47 160 37 35 0 0
71 F PDA 3 1 1 4 47 51 163 39 42 0 0
72 M ASD 0 0 1 10 49 53 211 37 43 0 0
73 M ASD 2 0 0 8 43 45 232 37 35 0 0
74 M TOF 6 1 1 2 43 44 131 47 49 0 0
75 M ASD 5 0 0 5 49 43 232 49 39 0 0
76 F ALCAPA 6 0 2 2 43 51 117 39 38 0 0
77 M VSD 6 1 0 3 44 52 187 41 45 0 0
78 F VSD 6 0 0 4 41 40 166 38 38 0 0
79 M ASD 7 1 1 1 59 57 147 46 44 0 0
80 F TGV 7 1 0 2 89 43 187 33 39 0 0

99
S.
NO Sex CHD UL RL Arches Whorls
atd
RT
atd
LT
TFR
C
a-b
RC
RT
a-b
RC
LT
Simian
crease
Sydney
crease
81 F ASD 6 1 1 2 43 49 148 32 36 0 2
82 M VSD 5 0 1 4 59 49 169 39 39 0 0
83 M VSD 7 1 0 2 36 42 142 46 38 0 0
84 M DORV 4 0 0 6 42 47 187 32 30 0 0
85 M PDA 6 0 0 4 38 41 229 37 35 0 0
86 F VSD 4 1 4 1 49 49 62 43 43 0 0
87 M TGV 2 0 0 8 51 49 239 47 41 0 0
88 F VSD 4 0 0 6 39 37 138 27 37 0 0
89 F ASD 4 1 1 4 38 37 111 36 35 0 0
90 F ASD 0 0 1 9 49 41 137 32 32 0 0
91 F VSD 1 1 0 8 39 37 159 37 37 0 0
92 F ASD 5 1 1 3 48 42 97 43 41 0 0
93 M VSD 4 2 1 3 47 43 92 34 34 0 0
94 M ASD 4 1 5 0 43 43 67 27 33 0 0
95 F ASD 4 1 0 5 47 49 197 45 47 0 0
96 F TOF 7 0 2 1 46 41 97 36 39 0 0
97 F TGV 7 0 2 1 49 39 109 35 34 0 0
98 F TOF 7 1 0 2 55 56 167 47 44 0 0
99 F ASD 1 0 0 9 32 36 160 37 39 0 0
100 M AS 2 1 0 7 54 55 198 46 45 0 0

100

101

102