-
8/7/2019 Study of growth factors and receptors in carcinoma
1/8
Study of growth factors and receptors in carcinoma
ex pleomorphic adenoma
Cristiane Furuse1, Lucyene Miguita1, Ana Cla udia Garcia Rosa1,
Andresa Borges Soares1, Elizabeth FerreiraMartinez1, Albina
Altemani2, Vera Cavalcanti de Arau jo1
1Department of Oral Pathology, Sao Leopoldo Mandic Institute and
Research Center, Campinas, Sao Paulo, Brazil;2Department of
Pathology, School of Medicine, State University of Campinas
(UNICAMP), Campinas, Sao Paulo, Brazil
SUMMARY
Carcinoma ex pleomorphic adenoma (CXPA) is a rare
malignant salivary gland tumor derived from a pre-
existing pleomorphic adenoma. It is a good model to
study the evolution of carcinogenesis, starting with in situ
areas to frankly invasive carcinoma. Growth factors are
associated with several biological and neoplastic pro-
cesses by transmembrane receptors. In order to investi-
gate, by immunohistochemistry, the expression of some
growth factors and its receptors [EGF receptor, fibro-
blast growth factor, fibroblast growth factor receptor 1,
fibroblast growth factor receptor 2, hepatocyte growth
factor, c-Met, transforming growth factor (TGF) b1,TGFbR-II and
insulin-like growth factor receptor 1] in the
progression of CXPA, we have used ten cases of CXPA in
several degrees of invasion- intracapsular, minimally and
frankly invasive carcinoma- with only epithelial compo-
nent. Slides were qualitatively and semi-quantitatively
evaluated according to the percentage of stained tumor
cells from 0 to 3 (0 = less than 10%; 1 = 1025%; 2 = 25
50%; 3 = more than 50% of cells). Malignant epithelial
cells starting with in situ areas showed stronger expres-
sion than luminal cells of pleomorphic adenoma for all
antibodies. Most of the intracapsular, minimally and
frankly invasive CXPA presented score 3. However, score
2 was more evident in the frankly invasive one. In smallnests of
invasive carcinoma, negative cells were observed
probably indicating that the proliferative process is re-
placed by the invasive mechanism. Altogether this data
infers that these factors may contribute to cell prolifer-
ation during initial phases of the tumor.
J Oral Pathol Med(2010)
Keywords: carcinoma ex pleomorphic adenoma; growth factors
Abbreviations: rRNA, ribosomal ribonucleic acid; ErbBHER,
epidermal growth factor receptor family; PDGFR-a, platelet
growth factor receptor type a; FGFR2b, fibroblast growth
factor
receptor isoform 2b; FGFR2c, fibroblast growth factor
receptor
isoform 2c; GTPase, guanosine triphosphate hydrolase enzyme;
GEP100, guanine-nucleotide exchange protein 100; TGF-a,
transforming growth factor a.
Introduction
According to the World Health Organization thecarcinoma ex
pleomorphic adenoma (CXPA) is definedas an epithelium malignization
derived from a pleomor-phic adenoma (1). The structural diversity
of CXPAenables us to an important template study of theevolution of
carcinogenesis, from benign to malignanttumor (27).
Several growth factors are involved in carcinomainitiation and
progression including fibroblast growthfactor (FGF), hepatocyte
growth factor (HGF), epider-mal growth factor (EGF), insulin-like
growth factor(IGF) and transforming growth factor b (TGFb)
(817).Growth factors and their receptors have been intensely
studied in tumorigenesis of mammary, skin, prostateand bladder
carcinomas (1821), blood cancer (8, 22),neural astrocytoma (23),
but rarely studied in salivarygland tumors (2427).
Among them, the FGF-2 is a member of a family ofheparan-biding
polypeptides, localized in extracellularmatrix, cytoplasm and
nucleus of the cells (2830). Itacts on cells by intracrine,
paracrine and autocrinemechanisms (28, 31, 32) activating
intracelullar path-ways by tyrosine kinase receptors (FGFR-1 and
FGFR-2) (29, 30, 33, 34), or by internalization to cytoplasmand
translocation to nucleus acting directly on nucleo-lus where FGF-2
participates in rRNA transcription(35, 36). In the nucleus, FGF-2
promotes mitogenic
Correspondence: Vera Cavalcanti de Araujo, Rua Vicente
Leporace,1220 apt. 91, Sao Paulo, SP, Brazil, 04619-033. Tel: +55
11 5044 0762,Fax: +55 11 5041 2992, E-mail:
[email protected] for publication September 30,
2009
doi: 10.1111/j.1600-0714.2009.00858.x
J Oral Pathol Med
2010 John Wiley & Sons A/S All rights reserved
interscience.wiley.com/journal/jop
Journal of
Oral Pathology & Medicine
-
8/7/2019 Study of growth factors and receptors in carcinoma
2/8
function, cell differentiation, angiogenesis,
phenotypictransformation (35, 37), and survival of tumor and
stemcells (8, 3840).
HGF is a cytokine that induces many biologicalfunctions not only
in hepatocytes but also in manyepithelial cells (41, 42) by
activating a tyrosine kinasesignaling cascade after binding to the
proto-oncogenicC-Met receptor (43). In normal tissue, HGF plays a
rolein the dynamic construction and reconstruction oftissues during
organogenesis and tissue regeneration(44, 45). In mature tissues,
HGF has an organotrophicrole in regeneration and protection of
various tissues(44). HGF also has angiogenic activity for
vascularendothelial cells (46). In tumor tissues, cells utilize
thebiological actions of HGF for their dissociative, invasiveand
metastatic behavior.
EGF receptor (EGFR) is a member of ErbBHERtransmembrane protein
family that performs manybiological functions in normal cells, as
proliferation,adhesion and migration (47, 48). Many growth
factorsof EGF family can activate EGFR on cell surface,
resulting in a downstream cascade of proteins
whichpromotespromoting signal transduction (48). In neo-plastic
cells, the super-expression of receptor as well asmutations of its
cytoplasmatic domain contributes toconstitutive signalization which
appears to be relevant inthe growth and progression of many cancers
(49).
IGF plays an important role in normal cellulargrowth and
development and it has been implicatedin the regulation of tumor
growth (5052). One ofits receptors, insulin-like growth factor
receptor 1(IGFR-1), is a transmembrane receptor with tyrosinekinase
activity, and regulates cell growth and meta-bolism (53, 54).
TGFb-1 family encompasses a group of structurally
related growth and differentiation factors which havediverse
activities in the regulation of cell growth,differentiation,
embryonic induction and morphogenesisin a wide range of cells and
tissues (55, 56). It has alsobeen implicated in carcinogenesis
progression in differ-ent tumors (5759). TGFb-1 signals through the
type Ireceptor (TGFbR-I) and the type II receptor (TGFbR-II) (9,
12) and it usually stimulates mesenchymal cellsgrowth but inhibits
epithelial cell proliferation (60). Incancer, it plays a major role
by suppressing tumorgrowth in the early phase of neoplasia, while
promotingtumor progression and metastasis in later phases (61).
Based on the important role of growth factors and
their receptors in many tumors, the aim of the presentstudy was
to investigate the participation of thesegrowth factors in CXPA
with different evolution stagesby immunohistochemistry.
Materials and methods
The present study protocol was approved by the EthicsCommittee
of School of Medicine of the State Univer-sity of Campinas, SP,
Brazil. The CXPA cases wereretrieved from the files of the
Pathology Department atthe School of Medicine of the State
University ofCampinas, Campinas, Brazil. The tumors were
classified
according to the presence of epithelial andor myoepi-thelial
cells using immunohistochemistry for cytokera-tins (epithelial
cells), vimentin and a-smooth muscleactin (myoepithelial cells) as
previously described inAltemani et al. (2). Tumors with epithelial
componentswere selected in a total of 10 cases (Table 1)
andclassified according to Brandwein et al. (62) taking intoaccount
the extension of invasion beyond the previouspleomorphic adenoma
capsule as intracapsular (withoutinvasion), minimally invasive (1.5
mm of invasion) andfrankly invasive. In addition, luminal cells
from residualpleomorphic adenoma present in the CXPA specimensand 4
cases of pleomorphic adenoma without malignanttransformation,
retrieved from the files of the Depart-ment of Oral Pathology of
Sao Leopoldo MandicInstitute and Research Center, Campinas, SP,
Brazil,were also analysed.
Serial sections, 3 lm thick, were obtained fromparaffin-embedded
samples and the dewaxed sectionswere processed for epitope
desmasking. Endogenousperoxidase was blocked by incubation in 3%
hydrogen
peroxide. After washing, the sections were incubatedwith primary
polyclonal antibodies to FGF-2, FGFR-1,FGFR-2, HGF-A, C-Met,
TGFb-1, EGFR and IGFR-1, and primary monoclonal antibody to
TGFbR-II(Table 2). Proper positive controls were utilized for
eachantibody. Omission of the primary antibody constitutedthe
negative control. Signal detection was performedusing the DAKO
EnVision Peroxidase procedure(DAKO, Carpinteria, CA, USA), followed
by a dia-minobenzidine chromogen solution and counterstainingwith
Mayers hematoxylin.
The labeled sections were qualitatively and semi-quantitatively
evaluated by six independent examiners.The qualitative analysis was
performed evaluating the
positive cells in different areas including in situ
andperipheral areas of both intracapsular and minimallyinvasive
tumors, large and small groups of cells of thefrankly invasive
carcinoma. For semi-quantitative eval-uation, we followed the
recommendation of the Mem-bers of Ad-Hoc Committee on
ImmunohistochemistryStandardization (63). The scores for the
expression ofeach protein were assigned according to the
percentage
Table 1 Sex, age, localization, and degree of invasion of
thecarcinoma ex pleomorphic adenoma
Caseno. Sex
Age(years)
Salivarygland
Degree ofinvasion
1 Male 58 Parotid Intracapsular2 Female 50 Parotid
Intracapsular3 Female 37 Submandibular Intracapsular4 Female 51
Parotid Intracapsular5 Female 65 Parotid Minimally invasive6 Female
43 Parotid Minimally invasive7 Male 74 Parotid Minimally invasive8
Female 62 Submandibular Frankly invasive9 Male 66 Parotid Frankly
invasive
10 a a Parotid Frankly invasive
aData not available.
Study of growth factors and receptors in carcinoma
Furuse et al.
Oral Pathol Med
-
8/7/2019 Study of growth factors and receptors in carcinoma
3/8
of stained tumor cells from 0 to 3 (0,
-
8/7/2019 Study of growth factors and receptors in carcinoma
4/8
A B
C D
E F
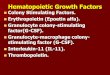
Figure 1 Immunohistochemical staining of growth factors and
receptors in carcinoma ex pleomorphic adenoma. (A) Positive
staining of TGF b inmalignant cells of CXPA. Note negative
expression in residual pleomorphic adenoma (200). (B) expression of
HGFA in in situ areas ofintracapsular type (400). (C, D) Large
blocks of carcinoma cells in minimally invasive type of CXPA. In
(C), staining for IGFR (200), and in (D)for FGFR2 (200). (E, F)
Small nests of carcinoma cells in minimally invasive type of CXPA.
In (E), negative carcinoma cells are evident usingFGF2 antibody
(400). In (F), EGFR expression is shown (400).
Table 3 Semi-quantitative analysis of the growth factors and
their receptors in residual pleomorphic adenoma of carcinoma ex
pleomorphicadenomas and in pleomorphic adenoma without malignant
transformation
Tumors FGF-2 FGFR-1 FGFR-2 TGF b-1 TGF bR-II IGFR EGFR HGF-A
c-Met
PA luminal cells 1 1 1 (nuclei) 0 0 0 1 3 0CXPA
intracapsular
#1 3 2 2 3 3 3 3 3 3
#2 3 3 3 3 3 3 3 3 3#3 3 3 3 3 3 3 3 3 3#4 3 3 0 3 3 3 0 3 3
CXPA minimally invasive#5 3 3 3 3 3 3 3 3 3#6 3 3 3 3 3 3 3 3
3#7 3 3 3 3 3 3 3 3 3
CXPA frankly invasive#8 3 3 2 3 3 2 3 3 3#9 2 3 0 3 2 3 3 3 3#10
3 3 2 3 2 3 3 2 3
PA, pleomorphic adenoma; CXPA, carcinoma ex-pleomorphic
adenoma.Scores: 0 = less than 10% of tumor cells; 1 = staining of
1025% of tumor cells; 2 = staining of 2550% of cells; 3 = staining
of more than 50%of cells.
Study of growth factors and receptors in carcinoma
Furuse et al.
Oral Pathol Med
-
8/7/2019 Study of growth factors and receptors in carcinoma
5/8
FGFR-2 was not present in pleomorphic adenoma butwas strongly
expressed in CXPA cases. FGFR-2 isassociated with increased risk of
breast cancer (14, 74,78, 79). Gene amplification or missense
mutation ofFGFR2 occurs in gastric cancer, lung cancer,
breastcancer, ovarian cancer, and endometrial cancer (80).This
evidences raise the possibility that this receptor,FGFR-2, might be
related with a malignant phenotypeof epithelial cells.
In the present study, TGFb-1 was observed in allcarcinoma cells,
but negative in epithelial and myo-epithelial pleomorphic adenoma
cells. TGFb has adual role in carcinogenesis, initially it acts as
a tumorsuppressor and causes growth arrest of epithelial cellsand
in the early stages of cancer, but in an establishedtumor, TGF-b
exerts an effect which contributes for thesurvival, progression and
metastasis of the tumor bypromoting epithelial-mesenchymal
transition (EMT),angiogenesis and escape from immune
surveillance(12). TGFb-1 is found in adenocarcinoma (12),
carci-noma-associated fibroblast (81), but negative in pleo-
morphic adenoma (25). In human breast cancer cells,TGFb has been
shown to induce breast tumorigenesisand metastatic progression
(82).
HGF-A and c-Met were strongly expressed in allCXPA cases. HGF-A
(also known as scatter factor) andits receptor (c-Met, a
proto-oncogene also known asHGFR), play an important role in
angiogenesis andtumor growth (83). HGF is expressed in many
malig-nant tumor as osteosarcoma, rabdomyosarcoma (11),adenoid
cystic carcinoma (84, 85) and breast cancer (86).While c-Met
overexpression is evidenced in colorectalcarcinomas,
hepatocarcinomas, gastrinomas, and carci-nomas of the pancreas,
stomach, prostate, ovary andbreast (11), and also found in lung
adenocarcinoma,
colorectal, ovarian, head and neck squamous cellcarcinoma, liver
glioma, renal clear cell and papillarycancer, stomach cancer,
melanoma (87), papillary car-cinoma of thyroid (88), sporadic
papillary renal cancer,childhood hepatocellular carcinoma,
osteosarcoma andrabdomyosarcoma (11). In pleomorphic adenoma,HGF-A
was also present, probably playing a role incell differentiation as
demonstrated by Niranjan et al.(89).
In the present study, IGFR-1 was observed in allcarcinoma cells.
Expression of IGF and IGFR-1 hasbeen detected in various human
malignancies, such asbrain (90), colorectal (17), breast (50) and
oral (91)
carcinomas, suggesting that these molecules induce
cellproliferation and inhibition of apoptosis in an autocrineor
paracrine manner (50, 54, 92, 93). In addition, IGFR-1 has shown to
be involved in malignant transformationand the frequent detection
of IGFR-1 expression inhuman cancer has fired the efforts to
develop IGFR-1targeted therapy (51, 94, 95).
Invasive tumors showed absence of the staining insome small
nests and in isolated cells. Only EGFR waspresent in these nests.
The absence of the antibodiesFGF-2, FGFR-1, FGFR-2, HGF-A, c-Met,
TGFb-Iand TGFbR-I in these areas is in accordance with otherstudies
which have pointed out that the cells lose their
proliferative capacity in order to invade (96, 97). It
isbelieved that cancer cells cannot move and
proliferatesimultaneously, a mechanism known as the go-or
growhypothesis (96). When there is no cell motility, tumorcell
exclusively proliferates, and when movement initi-ates it changes
the fitness landscape on which the cellpopulation evolves (6, 7,
97).
Meanwhile, the expression of studied growth factorswere lost in
the small nests of cells, this fact was lessevident for EGFR. The
phosphorylation of EGFRactivates multiple biological processes
including cellmotility and invasion, by EGFR-GEP100-Arf6 path-way,
activating matrix invasion and deranging E-cadh-erin (98). Advanced
stage colorectal carcinoma presentssignificantly higher
co-expression of EGFR, TGF-a andprotein S6K, a ribosomal protein
that regulates celladhesion and invasiveness (99). EGFR is vastly
studiedin breast tumors (98, 100, 101), colorectal cancer
(17),pancreatic and oral carcinoma (100), gastric carcinoma(102)
and also salivary gland tumors (103105). Severaltherapies have been
developed to inactivate the EGFR
pathway including monoclonal antibodies against theextracellular
domain of EGFR (106).In conclusion, the obtained results
demonstrated that
carcinoma cells from CXPA presented the expression ofall growth
factors and receptors in a derisive way. Weobserved that EGFR,
FGF-2, FGFR-1, FGFR-2,HGF-A, c-Met, TGFb-1, TGFbR-II and IGFR-1
weremore expressed in carcinomatous cells of CXPA than inepithelial
cells of pleomorphic adenoma ductal areas.Moreover, this expression
was more intense in intra-capsular and minimally invasive CXPA,
than franklyinvasive ones, probably contributing to cell
proliferationduring initial phases of the tumor and demonstrating
theself-sufficiency of carcinomatous cells. In frankly inva-
sive tumors we also identified strong EGFR expressionin small
nests of peripheral borders of invasive CXPA,indicating that this
receptor may be related to invasive-ness and cell detachment of
CXPA.
References
1. Gnepp DR, Brandwein-Gensler MS, El-Naggar AK,et al. Carcinoma
ex pleomorphic adenoma. In: Barnes L,Eveson JW, Reichart P,
Sidransky D eds World HealthOrganization classification of tumours.
Pathology & genet-ics. Head and neck tumors. Lyon: IARC Press,
2005;2423.
2. Altemani A, Martins MT, Freitas L, Soares F,
Araujo NS, Araujo VC. Carcinoma ex pleomorphicadenoma (CXAP):
immunoprofile of the cells involvedin carcinomatous progression.
Hystopathol 2005; 46:63541.
3. Martins MT, Altemani A, Freitas L, Araujo VC.
Maspinexpression in carcinoma ex pleomorphic adenoma. J ClinPathol
2005; 58: 13114.
4. Araujo VC, Altemani A, Furuse C, Martins MT, AraujoNS.
Immunoprofile of reactive salivary myoepithelialcells in areas of
in situ carcinoma ex-pleomorphicadenoma. Oral Oncol 2006; 42:
10116.
5. Soares AB, Juliano PB, Araujo VC, Metze K, AltemaniA.
Angiogenic switch during tumor progression of
Study of growth factors and receptors in carcinoma
Furuse et al.
J Oral Pathol M
-
8/7/2019 Study of growth factors and receptors in carcinoma
6/8
carcinoma ex-pleomorphic adenoma. Virchows Arch2007; 451:
6571.
6. Araujo VC, Furuse C, Cury PR, Altemani A, Alves VA,Araujo NS.
Tenascin and fibronectin expression incarcinoma ex pleomorphic
adenoma. Appl Immunohisto-chem Mol Morphol 2008; 16: 4853.
7. Araujo VC, Demasi AP, Furuse C, et al. Collagen type Imay
influence the expression of E-cadherin and beta-
catenin in carcinoma ex-pleomorphic adenoma. ApplImmunohistochem
Mol Morphol 2009; 17(4): 3128.8. Gabrilove JL. Angiogenic growth
factors: autocrine and
paracrine regulation of survival in hematologic malig-nancies.
Oncologist 2001; 6: 47.
9. Bowmick NA, Neilson EG, Moses HL. Stromal fibro-blasts in
cancer initiation and progression. Nature 2004;432: 3327.
10. Grose R, Dickson C. Fibroblast growth factor signalingin
tumorigenesis. Cytokine Growth Factor Rev 2005; 16:17986.
11. Boccaccio C, Comoglio PM. Invasive growth: a MET-driven
genetic programme for cancer and stem cells. NatRev Cancer 2006; 6:
63745.
12. Ranganathan P, Agrawal A, Bhushan R, et al. Expres-
sion profiling of genes by TGFb: differential regulation
innormal and tumor cells. BMC Genomics 2007; 8: 98.13. Yang F,
Strand DW, Rowley DR. Fibroblast growth
factor-2 mediates transforming growth factor-b actionin prostate
cancer reactive stroma. Oncogene 2008; 27:4509.
14. Liang J, Chen P, Hu Z, et al. Genetic variants infibroblast
growth factor receptor 2 (FGFR2) contributeto susceptibility of
breast cancer in Chinese women.Carcinogenesis 2008; 29: 23416.
15. Sato T, Oshima T, Yoshihara K, et al. Overexpression ofthe
fibroblast growth factor receptor-1 gene correlateswith liver
metastasis in colorectal cancer. Oncol Rep 2009;21: 2116.
16. Tsunoda S, Sakurai H, Saito Y, Ueno Y, Koizumi K,
Saiki I. Massive T-lymphocyte infiltration into the hoststroma
is essential for fibroblast growth factor-2-pro-moted growth and
metastasis of mammary tumors vianeovascular stability. Am J Pathol
2009; 174: 67183.
17. Takahari D, Yamada Y, Okita NT, et al. Relationshipsof
insulin-like growth factor-1 receptor and epidermalgrowth factor
receptor expression to clinical outcomes inpatients with colorectal
cancer. Oncology 2009; 76: 428.
18. Volm M, Kooma gi R, Mattern J, Stammier G. Prognos-tic value
of basic fibroblast growth factor an its receptor(FGFR-1) in
patients with non-small cell lung carcino-mas. Eur J Cancer 1997;
33: 6913.
19. Wakulich C, Jackson-Boeters L, Daley TD, Wysocki
GP.Immunohistochemical localization of growth factorsfibroblast
growth factor-1 and fibroblast growth factor-
2 and receptors fibroblast growth factor receptor-2
andfibroblast growth factor receptor-3 in normal oralepithelium,
epithelial dysplasias, and squamous cellcarcinoma. Oral Surg Oral
Med Oral Pathol Oral RadiolEndod 2002; 93: 5739.
20. Chaffer CL, Dopheide B, Savagner P, Thompson EW,Williams ED.
Aberrant fibroblast growth factor receptorsignaling in bladder and
other cancers. Differentiation2007; 75: 83142.
21. Korah R, Das K, Lindy ME, Hameed M, Wieder R.Coordinate loss
of fibroblast growth factor 2 andlaminina 5 expression during
neoplastic progressionof mammary duct epithelium. Human Pathol
2007; 38:15460.
22. Ko nig A, Menzel T, Lynen S, et al. Basic fibroblastgrowth
factor (bFGF) upregulates the expression of bcl-2in B cell chronic
lymphocytic leukemia cell lines resultingin delaying apoptosis.
Leukemia 1997; 11: 25865.
23. Yamaguchi F, Saya H, Bruner JM, Morrison RS.Differential
expression of two fibroblast growth factor-receptor genes is
associated with malignant progression inhuman astrocytomas. Proc
Natl Acad Sci1994; 91: 4848.
24. Azuma M, Yuki T, Motegi K, Sato M. Enhancement ofbFGF export
associated with malignant progression ofhuman salivary gland cell
clones. Int J Cancer 1997; 71:8916.
25. Kusafuka K, Yamaguchi A, Kayano T, Takemura
T.Immunohistochemical localization of members of thetransforming
growth factor (TGF)-b superfamily innormal human salivary glands
and pleomorphic adeno-mas. J Oral Pathol Med 2001; 30: 41320.
26. Sumitomo S, Okamoto Y, Mizutani G, Kudeken W,Mori M, Takai
Y. Immunohistochemical study of fibro-blast growth factor-2 (FGF-2)
and fibroblast growthfactor receptor (FGF-R) in experimental
squamous cellcarcinoma of rat submandibular gland. Oral Oncol
1999;35: 98104.
27. Yura Y, Yoshioka Y, Yamamoto S, et al. Enhancingeffects of
fibroblast growth factor on the proliferation ofsalivary gland
carcinoma cells and salivary gland carci-nogenesis. J Oral Pathol
Med 2001; 30: 15967.
28. Delrieu I. The high molecular weight isoforms of
basicfibroblast growth factor (FGF-2): an insight into anintracrine
mechanism. FEBS Lett 2000; 468: 610.
29. Ornitz DM, Itoh N. Fibroblast growth factors proteinfamily
review. Genome Biol 2001; 2: 3005. 112.
30. Itoh N, Ornitiz DM. Evolution of the Fgf and FGFr
genefamilies. Trends Genet 2004; 20: 5639.
31. Maher PA. Nuclear Translocation of fibroblast growthfactor
(FGF) receptors in response to FGF-2. J Cell Biol1996; 134:
52936.
32. Arese M, Chen Y, Florkiewicz RZ, Gualandris A, Shen
B, Rifkin DB. Nuclear activities of basic fibroblastgrowth
factor: potentiation of low-serum growth medi-ated by natural or
chimeric nuclear localization signals.Mol Biol Cell 1999; 10:
142944.
33. Ornitz DM, Xu J, Colvin JS, et al. Receptor specificity
offibroblast growth factor family. J Biol Chem 1996;
271:152927.
34. Eswarakumar VP, Lax I, Schlessinger J. Cellular signal-ing
by fibroblast growth factor receptors. CytokineGrowth Factor Rev
2005; 16: 13949.
35. Baldin V, Roman A, Bosc-Bierne I, Amalric F, BoucheG.
Translocation of bFGF to the nucleus is G1 phase cellcycle specific
in bovine aortic endothelial cells. EMBO J1990; 9: 15117.
36. Sheng Z, Liang Y, Lin CY, Comai L, Chirico WJ. Direct
regulation of rRNA transcription by fibroblast growthfactor 2.
Mol Cell Biol 2005; 25: 941926.
37. Yu Z, Biro S, Fu Y, et al. Localization of basic
fibroblastgrowth factor in bovine endothelial cells:
immunohisto-chemical and biochemical studies. Exp Cell Res
1993;204: 24759.
38. Dow JK, deVERE White RW. Fibroblast growth factor2: its
structure and property, paracrine function, tumorangiogenesis, and
prostate-related mitogenic and onco-genic functions. Urology 2000;
55: 8006.
39. Presta M, Dellera P, Mitola S, Moroni E, Ronca R,Rusnati M.
Fibroblast Growth factorfibroblast growthfactor receptor system in
angiogenesis. Cytokine GrowthFactor Rev 2005; 16: 15978.
Study of growth factors and receptors in carcinoma
Furuse et al.
Oral Pathol Med
-
8/7/2019 Study of growth factors and receptors in carcinoma
7/8
40. Yeoh JSG, Haan G. Fibroblast growth factors asregulators of
stem cell self-renewal and aging. MechAgeing Dev 2007; 128:
1724.
41. Miyazawa K, Tsubouchi H, Naka D, et al. Molecularcloning and
sequence analysis of cDNA for humanhepatocyte growth factor.
Biochem Biophys Res Commun1989; 163: 96773.
42. Nakamura T, Nishizawa T, Hagiya M, et al. Molecular
cloning and expression of human hepatocyte growthfactor. Nature
1989; 342: 4403.43. Niranjan B, Buluwela L, Yant J, et al. HGFSF: a
potent
cytokine for mammary growth, morphogenesis anddevelopment.
Development 1995; 121: 2897908.
44. Matsumoto K, Nakamura T. Hepatocyte growth factor(HGF) as a
tissue organizer for organogenesis andregeneration. Biochem Biophys
Res Commun 1997; 239:63944.
45. Birchmeier C, Gherardi E. Developmental roles ofHGFSF and
its receptor, the c-Met tyrosine kinase.Trends Cell Biol 1998; 8:
40410.
46. Bussolino F, Di Renzo MF, Ziche M, et al. Hepatocytegrowth
factor is a potent angiogenic factor whichstimulates endothelial
cell motility and growth. J Cell
Biol 1992; 119: 62941.47. Fallon JH, Seroogy KB, Loughlin SE, et
al. Epidermalgrowth factor immunoreactive material in the
centralnervous system: location and development. Science 1984;224:
11079.
48. Singh AB, Harris RC. Autocrine, paracrine and juxta-crine
signaling by EGFR ligands. Cell Signal 2005; 17:118393.
49. Harari PM. Epidermal growth factor receptor
inhibitionstrategies in oncology. Endocr Relat Cancer 2004;
11:689708.
50. Yu H, Rohan T. Role of the insulin-like growth factorfamily
in cancer development and progression. J NatlCancer Inst 2000; 92:
147289.
51. Cappuzzo F, Toschi L, Tallini G, Ceresoli GL, Domeni-
chini I, Bartolini S. Insulin-like growth factor receptor
1(IGFR-1) is significantly associated with longer survivalin
non-small-cell lung cancer patients treated with gefi-tinib. Ann
Oncol 2006; 17: 11207.
52. Kumamoto H, Ooya K. Immunohistochemical detectionof
insulin-like growth factors, platelet-derived growthfactor, and
their receptors in ameloblastic tumors. J OralPathol Med 2007; 36:
198206.
53. Jones JI, Clemmons DR. Insulin-like growth factors andtheir
binding proteins: biological actions. Endocr Rev1995; 16: 334.
54. Werner H, Leroith D. The role of the insulin-like
growthfactor system in human cancer. Adv Cancer Res 1996;
68:183223.
55. Smith AJ, Matthews JB, Hall RC. Transforming growth
factor-beta1 (TGF-beta1) in dentine matrix. Ligandactivation and
receptor expression. Eur J Oral Sci 1998;106: 17984.
56. Tziafas D, Papadimitriou S. Role of exogenous TGF-beta in
induction of reparative dentinogenesis in vivo. EurJ Oral Sci 1998;
106: 1926.
57. Coffey RJJR, Goustin AS, Soderquist AM, et al. Trans-forming
growth factor alpha and beta expression inhuman colon cancer lines:
implications for an autocrinemodel. Cancer Res 1987; 47: 45904.
58. Truong LD, Kadmon D, Mccune BK, Flanders KC,Scardino PT,
Thompson TC. Association of transform-ing growth factor-beta 1 with
prostate cancer: an immu-nohistochemical study. Hum Pathol 1993;
24: 49.
59. Maiorano E, Loverro G, Viale G, Giannini T, Napoli A,Perlino
E. Insulin-like growth factor-I expression innormal and diseased
endometrium. Int J Cancer 1999;80: 18893.
60. Forino M, Torregrossa R, Ceol M, et al. TGFbeta1induces
epithelial-mesenchymal transition, but not myo-fibroblast
transdifferentiation of human kidney tubularepithelial cells in
primary culture. Int J Exp Pathol 2006;
87: 197208.61. Prudhomme GJ. Pathobiology of transforming
growthfactor beta in cancer, fibrosis and immunologic disease,and
therapeutic considerations. Lab Invest 2007; 87:107791.
62. Brandwein M, Huvos AG, Dardick I, Thomas MJ,Theise ND.
Noninvasive and minimally invasive carci-noma ex mixed tumor: a
clinicopathologic and ploidystudy of 12 patients with major
salivary tumors of low (orno?) malignant potential. Oral Surg Oral
Med OralPathol Oral Radiol Endod 1996; 81: 65564.
63. Goldstein NS, Hewitt SM, Taylor CR, Yaziji H, HicksDG.
Members of Ad-Hoc Committee On Immuno-histochemistry
Standardization. Recommendations forimproved standardization of
immunohistochemistry.
Appl Immunohistochem Mol Morphol 2007; 15: 12433.64. Tarin D,
Thompson EW, Newgreen DF. The fallacy ofepithelial mesenchymal
transition in neoplasia. CancerRes 2005; 65: 59966000.
65. Huber MA, Kraut N, Beug H. Molecular requirementsfor
epithelial-mesenchymal transition during tumor pro-gression. Curr
Opin Cell Biol 2005; 17: 54858.
66. Thompson EW, Newgreen DF, Tarin D. Carcinomainvasion and
metastasis: a role for epithelial-mesenchy-mal transition? Cancer
Res 2005; 65: 59915.
67. Thiery JP. Epithelial-mesenchymal transitions in
tumourprogression. Nat Rev Cancer 2002; 2: 44254.
68. Demasi APD, Furuse C, Soares AB, Altemani A, AraujoVC.
Peroxiredoxin 1, platelet-derived growth factor A,and
platelet-derived growth factor receptor a are over-
expressed in carcinoma ex pleomorphic adenoma: asso-ciation with
malignant transformation. Hum Pathol2009;40: 3907.
69. Behrens C, Lin HY, Lee JJ, et al.
Immunohistochemicalexpression of basic fibroblast growth factor and
fibroblastgrowth factor receptors 1 and 2 in the pathogenesis
oflung cancer. Clin Cancer Res 2008; 14: 601422.
70. Cebulla CM, Jockovich ME, Pin a Y, et al. Basic fibro-blast
growth factor impact on retinoblastoma progressionand survival.
Invest Ophthalmol Vis Sci 2008; 49: 521521.
71. Flores-Stadler EM, Chou P, Walterhouse D, Bourtsos
E,Gonzalez-Crussi F. Hemangiopericytoma of the
liver:immunohistochemical observations, expression of angio-genic
factors, and review of the literature. J Pediatr
Hematol Oncol 1997; 19: 44954.72. Vacca A, Ribatti D, Roccaro
AM, Frigeri A, Dammacco
F. Bone marrow angiogenesis in patients with activemultiple
myeloma. Semin Oncol 2001; 28: 54350.
73. Billottet C, Elkhatib N, Thiery JP, Jouanneau J. Targetsof
fibroblast growth factor 1 (FGF-1) and FGF-2signaling involved in
the invasive and tumorigenicbehavior of carcinoma cells. Mol Biol
Cell 2004; 15:472534.
74. Lappi DA. Tumor targeting through fibroblast growthfactor
receptors. Semin Cancer Biol 1995; 6: 27988.
75. Ueba T, Takahashi JA, Fukumoto M, et al. Expressionof
fibroblast growth factor receptor-1 in human gliomaand meningioma
tissues. Neurosurgery 1994; 34: 2215.
Study of growth factors and receptors in carcinoma
Furuse et al.
J Oral Pathol M
-
8/7/2019 Study of growth factors and receptors in carcinoma
8/8
76. Myoken Y, Myoken Y, Okamoto T. et al. Immunohis-tochemical
localization of fibroblast growth factor-1(FGF-1), FGF-2 and
fibroblast growth factor receptor-1 (FGFR-1) in pleomorphic adenoma
of the salivaryglands. J Oral Pathol Med 1997; 26: 1722.
77. Kusafuka K, Yamaguchi A, Kayano T, Takemura
T.Immunohistochemical localization of fibroblast growthfactors
(FGFs) and FGF receptor-1 in human normal
salivary glands and pleomorphic adenomas. J Oral PatholMed 1998;
27: 28792.78. Moffa AB, Tannheimer SL, Ethier SP. Transforming
potential of alternatively spliced variants of fibroblastgrowth
factor receptor 2 in human mammary epithelialcells. Mol Cancer Res
2004; 2: 64352.
79. Meyer KB, Maia A-T, Oreilly M, et al.
Allele-specificup-regulation of FGFR2 increases susceptibility to
breastcancer. PLoS Biol 2008; 6: 1098103.
80. Katoh M. Cancer genomics and genetics of FGFR2. Int JOncol.
2008; 33: 2337.
81. Rosenthal E, Mccrory A, Talbert M, Young G, Murphy-Ullrich
J, Gladson C. Elevated expression of TGF-beta1in head and neck
cancer-associated fibroblasts. MolCarcinog 2004; 40: 11621.
82. Muraoka-Cook RS, Shin I, Yi JY, et al. Activated type
ITGFbeta receptor kinase enhances the survival of mam-mary
epithelial cells and accelerates tumor progression.Oncogene 2006;
25: 340823.
83. You WK, Mcdonald DM. The hepatocyte growthfactorc-Met
signaling pathway as a therapeutic targetto inhibit angiogenesis.
BMB Rep 2008; 41: 8339.
84. Suzuki K, Cheng J, Watanabe Y. Hepatocyte growthfactor and
c-Met (HGFc-Met) in adenoid cystic carci-noma of the human salivary
gland. J Oral Pathol Med2003; 32: 849.
85. Hara S, Nakashiro K, Goda H, Hamakawa H. Role ofAkt isoforms
in HGF-induced invasive growth of humansalivary gland cancer cells.
Biochem Biophys Res Commun2008; 370: 1238.
86. Klosek SK, Nakashiro K, Hara S, Li C, Shintani S,Hamakawa H.
Constitutive activation of Stat3 corre-lates with increased
expression of the c-MetHGFreceptor in oral squamous cell carcinoma.
Oncol Rep2004; 12: 2936.
87. Christensen JG, Burrows J, Salgia R. c-Met as a targetfor
human cancer and characterization of inhibitors fortherapeutic
intervention. Cancer Lett 2005; 225: 126.
88. Ruco LP, Stoppacciaro A, Ballarini F, Prat M, ScarpinoS. Met
protein and hepatocyte growth factor (HGF) inpapillary carcinoma of
the thyroid: evidence for apathogenetic role in tumourigenesis. J
Pathol 2001; 194:48.
89. Niranjan B, Buluwela L, Yant J, et al. HGFSF: a
potentcytokine for mammary growth, morphogenesis and
development. Development 1995; 121: 2897908.90. Arcaro A,
Doepfner KT, Boller D, et al. Novel role for
insulin as an autocrine growth factor for malignant braintumour
cells. Biochem J 2007; 406: 5766.
91. Brady G, Crean SJ, Naik P, Kapas S. Upregulation ofIGF-2 and
IGF-1 receptor expression in oral cancer celllines. Int J Oncol
2007; 31: 87581.
92. Nakanishi Y, Mulshine JL, Kasprzyk PG, et al. Insulin-like
growth factor-I can mediate autocrine proliferationof human small
cell lung cell lines in vitro. J Clin Invest1988; 82: 3549.
93. Ouban A, Muraca P, Yeatman T, Coppola D. Expressionand
distribution of insulin-like growth factor-1 receptorin human
carcinomas. Hum Pathol 2003; 34: 8038.
94. Brodt P, Samani A, Navab R. Inhibition of the type
Iinsulin-like growth factorreceptor expression and signal-ing:
novel strategies for antimetastatic therapy. BiochemPharmacol 2000;
60: 11017.
95. Valentinis B, Baserga R. IGF-I receptor signalling in
transformation and differentiation. Mol Pathol 2001; 54:1337.96.
Giese A, Bjerkvig R, Berens ME, Westphal M. Cost of
migration: invasion of malignant gliomas and implica-tions for
treatment. J Clin Oncol 2003; 21: 162436.
97. Gerlee P, Anderson AR. Evolution of cell motility in
anindividual-based model of tumour growth. J Theor Biol2009; 259:
6783.
98. Sabe H, Hashimoto S, Morishige M, Hashimoto A,Ogawa E. The
EGFR-GEP100-Arf6 pathway in breastcancer: full invasiveness is not
from the inside. Cell AdhMigr 2008; 2: 713.
99. Tampellini M, Longo M, Cappia S, et al. Co-expressionof EGF
receptor, TGFalpha and S6 kinase is significantlyassociated with
colorectal carcinomas with distant meta-
stases at diagnosis. Virchows Arch 2007; 450: 3218.100. Santini
D, Ceccarelli C, Tardio ML, Taffurelli M,Marrano D.
Immunocytochemical expression of epider-mal growth factor receptor
in myoepithelial cells of thebreast. Appl Immunohistochem Mol
Morphol 2002; 10:2933.
101. Talley L, Chhieng DC, Bell WC, Grizzle WE, Frost
AR.Immunohistochemical detection of EGFR, p185 (erbB-2), Bcl-2 and
p53 in breast carcinomas in pre-menopausaland post-menopausal
women. Biotech Histochem 2008;83: 514.
102. Sugiyama K, Yonemura Y, Miyazaki I. Immunohisto-chemical
study of epidermal growth factor and epidermalgrowth factor
receptor in gastric carcinoma. Cancer 1989;63: 155761.
103. Mori M, Naito R, Tsukitani K, Okada Y, Hayashi T,Kato K.
Immunohistochemical distribution of humanepidermal growth factor in
salivary gland tumours.Virchows Arch A 1987; 411: 499507.
104. Yamada K, Iwai K, Okada Y, Mori M. Immunohisto-chemical
expression of epidermal growth factor receptorin salivary gland
tumours. Virchows Archiv A Pathol Anat1989; 415: 52331.
105. Dodd RL, Slevin NJ. Salivary gland adenoid cysticcarcinoma:
a review of chemotherapy and moleculartherapies. Oral Oncol 2006;
42: 75969.
106. Capdevila J, Elez E, Macarulla T, Ramos FJ, Ruiz-echarri M,
Tabernero J. Anti-epidermal growth factorreceptor monoclonal
antibodies in cancer treatment.Cancer Treat Rev 2009; 35:
35463.
Acknowledgements
The authors wish to thank Audrey Jordao Basso and Jeruza
Pinheiro da
Silveira Bossonaro for their excellent technical expertise and
assistance.
This work was supported by FAPESP grant no. 0407960-0
Conflict of interest statement
None declared.
Study of growth factors and receptors in carcinoma
Furuse et al.
Oral Pathol Med



![CARCINOMA DUCTAL IN SITU DE MAMA: AVALIAÇÃO DE … · SUMMARY Cagnacci Neto R. [Ductal carcinoma in situ of the breast: assessment of potential prognostic factors].São Paulo; 2014](https://img.pdfslide.net/doc/110x75/5f238ed366495b3ab35c9909/carcinoma-ductal-in-situ-de-mama-avaliafo-de-summary-cagnacci-neto-r-ductal.jpg)