Embed Size (px)
Citation preview
STUDYING FAMILY MEMBERSUSING ADMINISTRATIVE DATA
James M. Bolton, MDAssociate Professor, University of ManitobaDepartments of Psychiatry, Psychology, Community Health SciencesMedical Director, WHRA Crisis Response Centre
Research Summer SchoolDepartment of PsychiatryJuly 14, 2015
Disclosures• Relationships with commercial interests:
• Grants/Research Support:• Canadian Institutes of Health Research
• New Investigator Award (113589)
• Brain and Behavior Research Foundation (NARSAD)• Young Investigator Award
• Speakers Bureau/Honoraria: Nil• Consulting Fees: Nil• Other: Nil
Acknowledgments• Wendy Au BSc• Dan Chateau PhD• Randy Walld BSc• William D. Leslie MSc, MD• Jessica Enns BSc• Patricia J. Martens PhD• Murray Enns MD• Laurence Y. Katz MD• Sarvesh Logsetty MD• Jitender Sareen MD
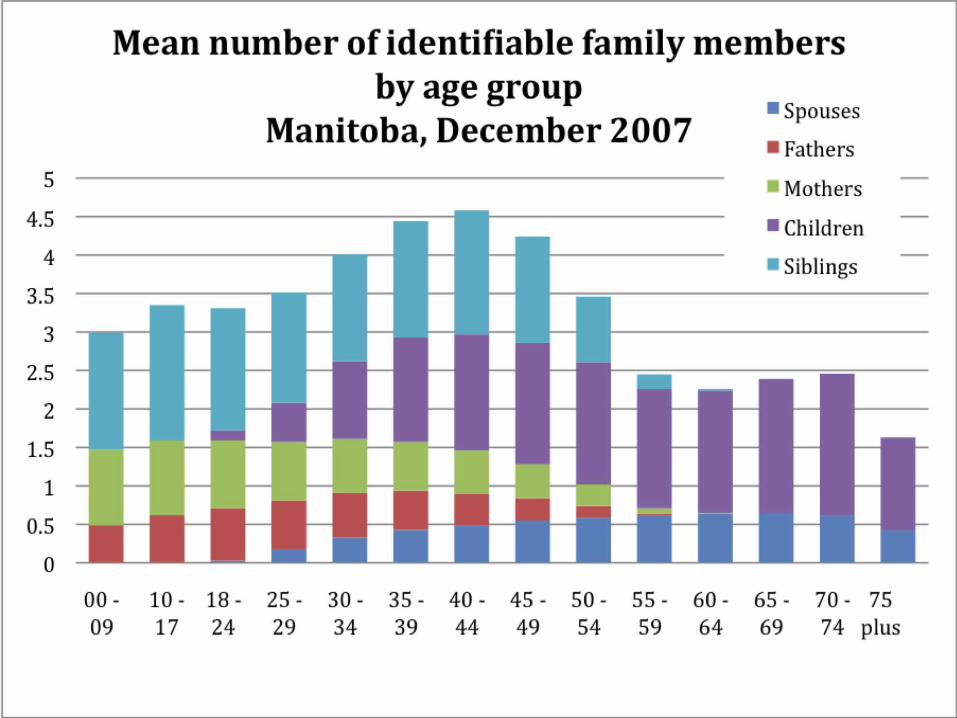
Strengths of Administrative Data
• Can examine a large number of family members• Overcomes the sampling bias in many family studies
• People who respond to bereavement surveys may be healthier and more recovered
• Integrity of diagnoses• Physician-generated• Not subject to recall bias
• Can examine longitudinal outcomes• Representative of the general population

Current State of Knowledge• Sibling bereavement is understudied
• <25 studies
• Limitations in existing literature• Small sample sizes• Selection bias
• Nationwide studies in Sweden• Increased risk of all-cause mortality after sibling death
• risk of subsequent suicide of the bereaved sibling
• No population studies of non-fatal health outcomes among bereaved siblings
Rostila M et al. Soc Psychiatry Psychiatr Epidemiol 2014
Rostila M et al. Am J Epidemiol 2012
Objective• Examine the health outcomes of bereaved siblings in the
general population• Focus on deaths of people 18 years of age and younger
(potentially more intense grief)• Adjust for pre-existing health and social confounders
Methods• Data Sources
• Manitoba Centre for Health Policy (MCHP) data repository• Vital statistics (mortality), physician billings and hospital discharge abstracts
(disorders and treatment use), census (age, sex, region)• Health Registry (family linkages: identification of siblings)
• Study Period• 1984-2009
• Cohort Formation• All people who died who were <19 years old at time of death and had a
sibling• Bereaved Siblings (n=7243)
• Bereaved siblings were matched 1:3 with people who were siblings, had not had a sibling or parent die• Non-bereave controls (n=21,729)
• Matched on sex, age, age of index sibling, relation of index sibling (brother/sister), family income level, region of residence
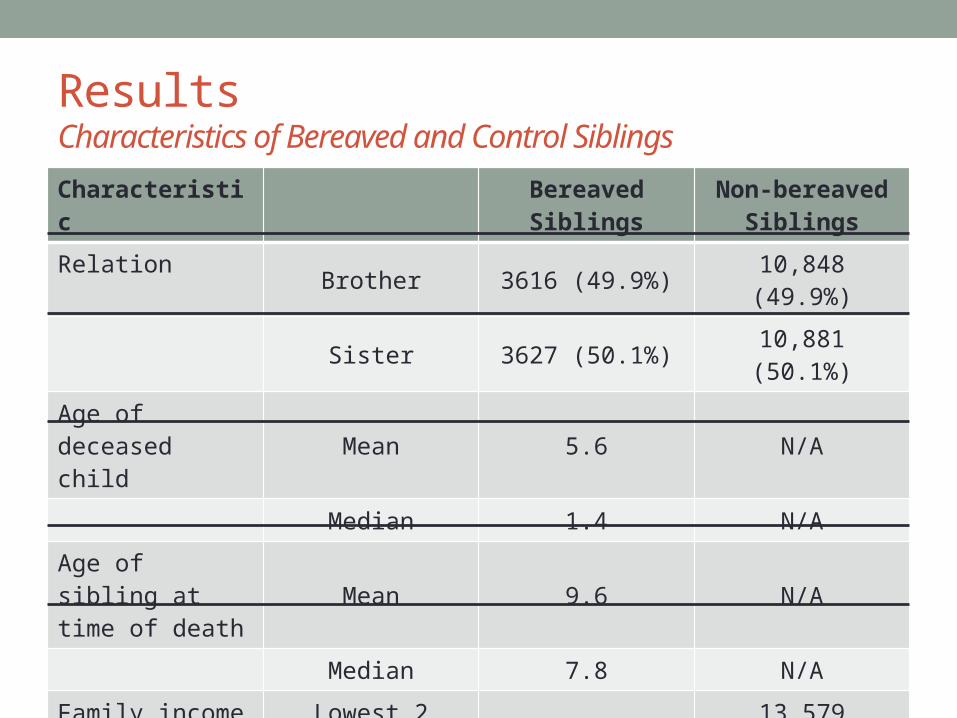
ResultsCharacteristics of Bereaved and Control Siblings
CharacteristicBereaved Siblings
Non-bereaved Siblings
Relation Brother 3616 (49.9%) 10,848 (49.9%)
Sister 3627 (50.1%) 10,881 (50.1%)
Age of deceased child
Mean 5.6 N/A
Median 1.4 N/A
Age of sibling at time of death
Mean 9.6 N/A
Median 7.8 N/A
Family income Lowest 2 quintiles 4514 (62.3%) 13,579 (62.5%)
Highest 3 quintiles 2651 (36.6%) 7957 (36.5%)
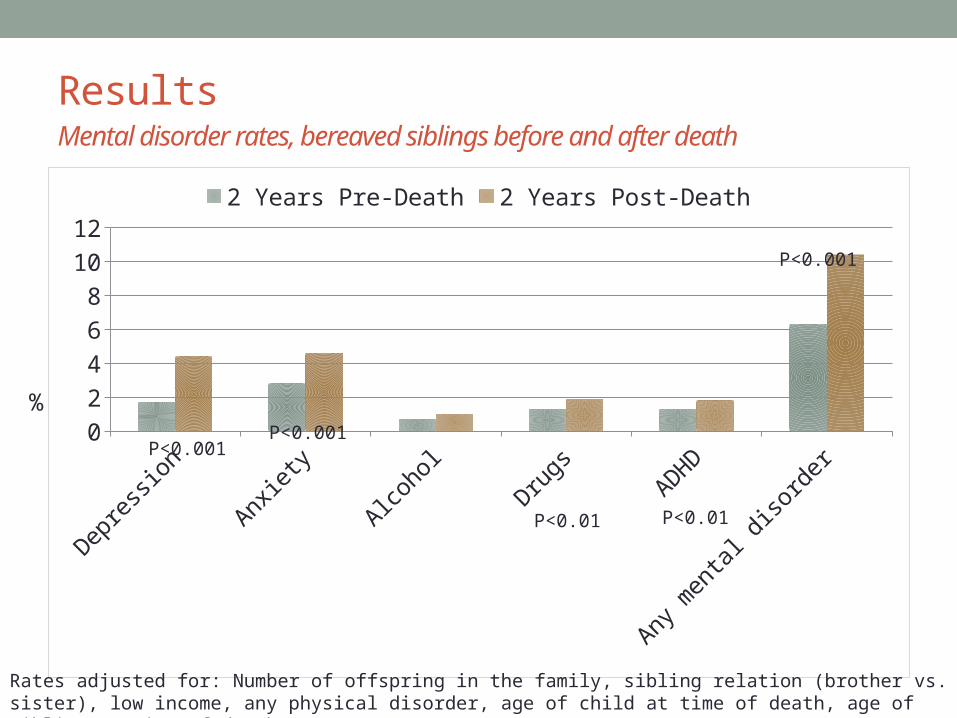
ResultsMental disorder rates, bereaved siblings before and after death
Depression Anxiety Alcohol Drugs ADHD Any mental disorder
0
2
4
6
8
10
12
2 Years Pre-Death 2 Years Post-Death
P<0.001P<0.001
P<0.001
P<0.01P<0.01
%
Rates adjusted for: Number of offspring in the family, sibling relation (brother vs. sister), low income, any physical disorder, age of child at time of death, age of sibling at time of death
Age
• Age stratified at 13• Significant age interactions observed on several measures
• The effect of sibling loss was different for adolescents and children
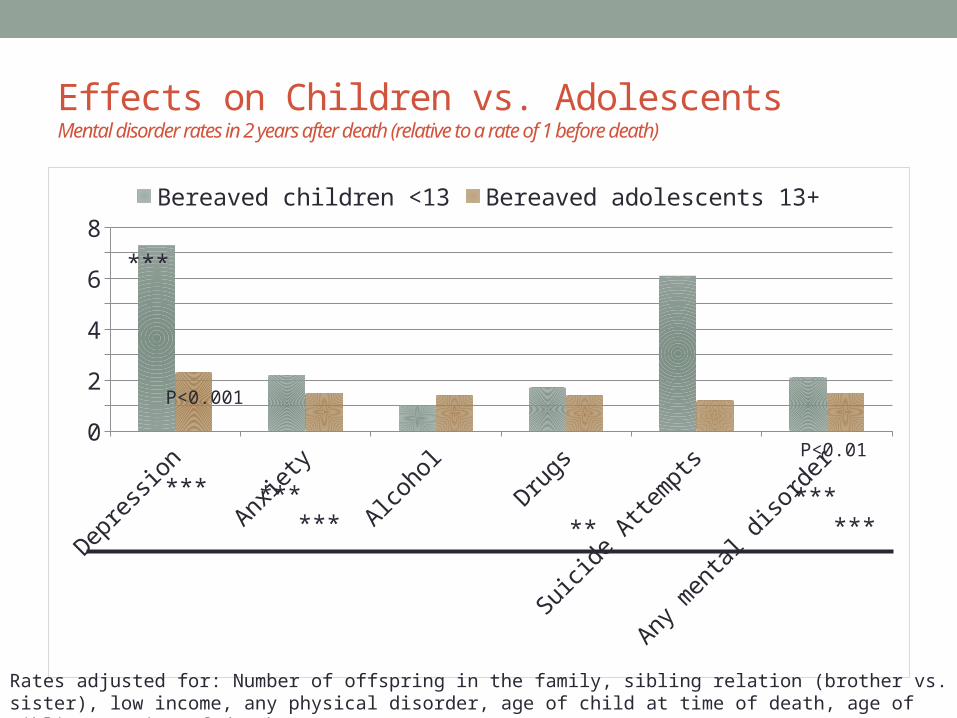
Effects on Children vs. AdolescentsMental disorder rates in 2 years after death (relative to a rate of 1 before death)
Depre
ssion
Anxiet
y
Alcoho
l
Drugs
Suicide
Atte
mpt
s
Any m
enta
l diso
rder
012345678
Bereaved children <13 Bereaved adolescents 13+
P<0.001
P<0.01
Rates adjusted for: Number of offspring in the family, sibling relation (brother vs. sister), low income, any physical disorder, age of child at time of death, age of sibling at time of death
***
***
****** ***
*****
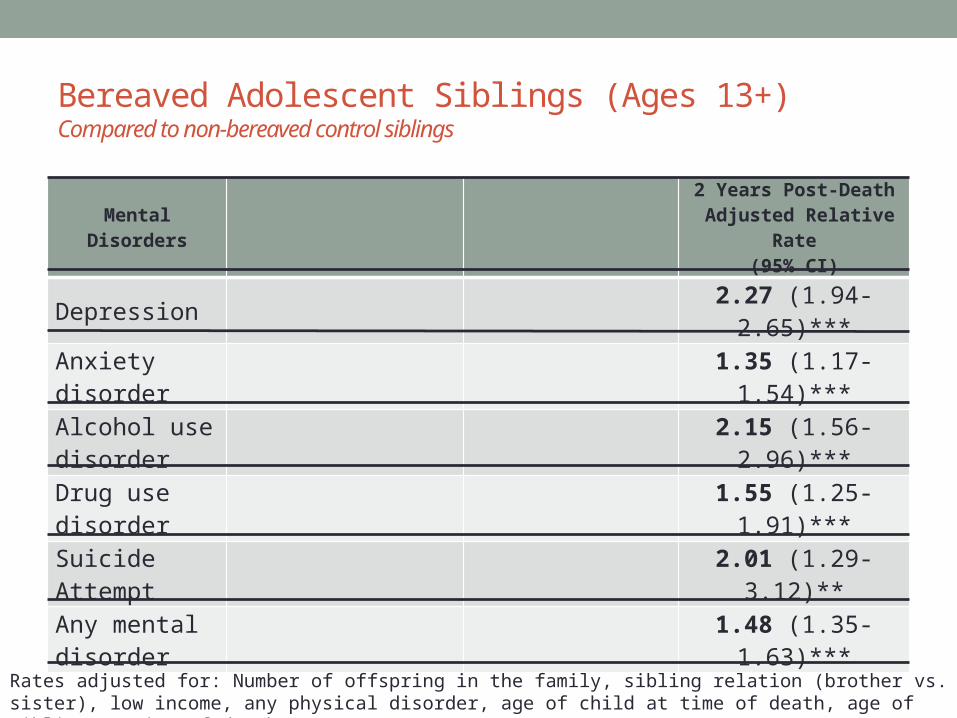
Bereaved Adolescent Siblings (Ages 13+)Compared to non-bereaved control siblings
Mental Disorders2 Years Post-Death
Adjusted Relative Rate(95% CI)
Depression 2.27 (1.94-2.65)***
Anxietydisorder
1.35 (1.17-1.54)***
Alcohol use disorder
2.15 (1.56-2.96)***
Drug use disorder
1.55 (1.25-1.91)***
Suicide Attempt
2.01 (1.29-3.12)**
Any mental disorder
1.48 (1.35-1.63)***
Rates adjusted for: Number of offspring in the family, sibling relation (brother vs. sister), low income, any physical disorder, age of child at time of death, age of sibling at time of death
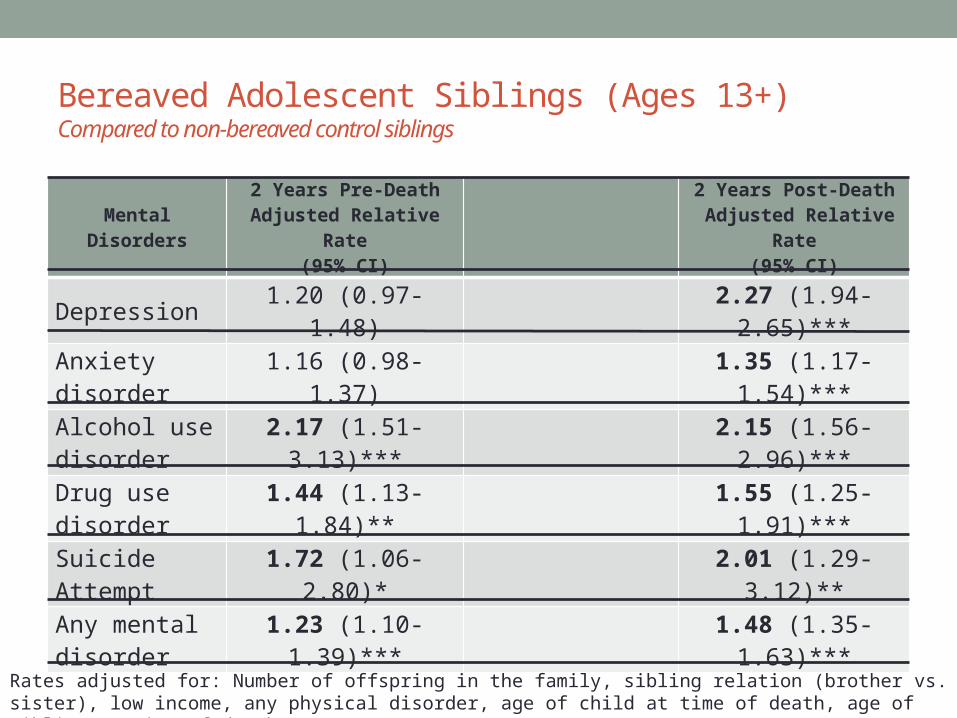
Bereaved Adolescent Siblings (Ages 13+)Compared to non-bereaved control siblings
Mental Disorders2 Years Pre-Death
Adjusted Relative Rate(95% CI)
2 Years Post-Death Adjusted Relative Rate
(95% CI)
Depression 1.20 (0.97-1.48) 2.27 (1.94-2.65)***
Anxietydisorder
1.16 (0.98-1.37) 1.35 (1.17-1.54)***
Alcohol use disorder
2.17 (1.51-3.13)*** 2.15 (1.56-2.96)***
Drug use disorder
1.44 (1.13-1.84)** 1.55 (1.25-1.91)***
Suicide Attempt
1.72 (1.06-2.80)* 2.01 (1.29-3.12)**
Any mental disorder
1.23 (1.10-1.39)*** 1.48 (1.35-1.63)***
Rates adjusted for: Number of offspring in the family, sibling relation (brother vs. sister), low income, any physical disorder, age of child at time of death, age of sibling at time of death
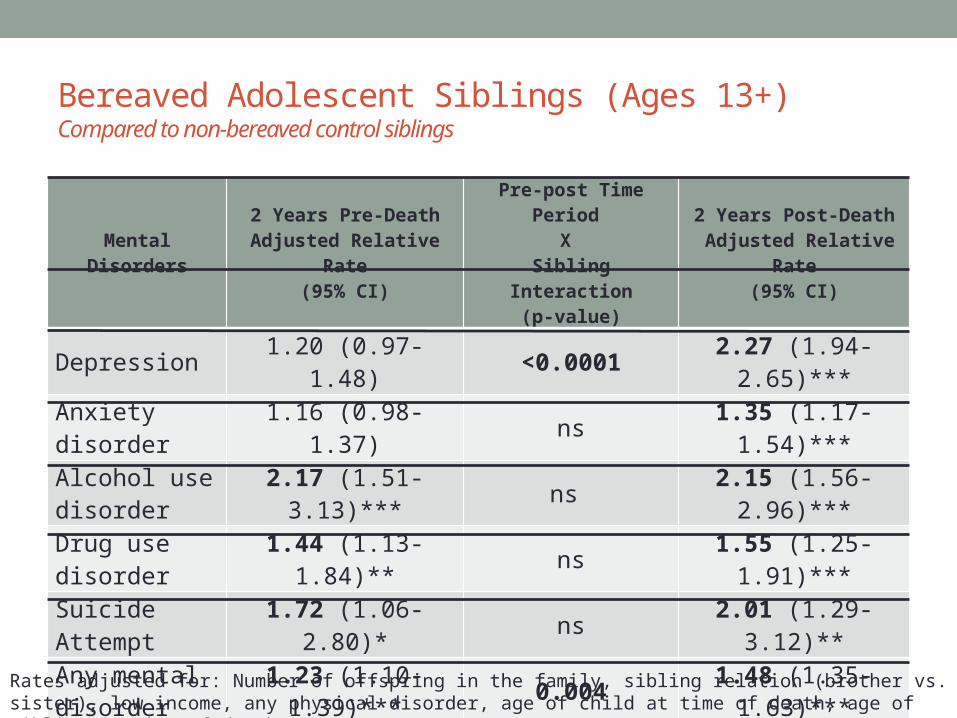
Bereaved Adolescent Siblings (Ages 13+)Compared to non-bereaved control siblings
Mental Disorders2 Years Pre-Death
Adjusted Relative Rate(95% CI)
Pre-post Time Period X
Sibling Interaction(p-value)
2 Years Post-Death Adjusted Relative Rate
(95% CI)
Depression 1.20 (0.97-1.48) <0.0001 2.27 (1.94-2.65)***
Anxietydisorder
1.16 (0.98-1.37) ns 1.35 (1.17-1.54)***
Alcohol use disorder
2.17 (1.51-3.13)*** ns 2.15 (1.56-2.96)***
Drug use disorder
1.44 (1.13-1.84)** ns 1.55 (1.25-1.91)***
Suicide Attempt
1.72 (1.06-2.80)* ns 2.01 (1.29-3.12)**
Any mental disorder
1.23 (1.10-1.39)*** 0.004 1.48 (1.35-1.63)***
Rates adjusted for: Number of offspring in the family, sibling relation (brother vs. sister), low income, any physical disorder, age of child at time of death, age of sibling at time of death
Summary• Losing a sibling is associated with significant mental
illness outcomes within 2 years• Age of sibling at time of death is important
• Children under the age of 13 have much higher rate increases in depression
• Bereaved adolescents have a very concerning profile of mental disorder morbidity compared to non-bereaved age-matched counterparts
• Adolescents that experience the death of a sibling have high rates of mental illness even prior to the loss• Common etiologic links between low income, childhood mortality,
mental disorders?

After the Suicide of an Offspring• Compared to the time before the suicide death of their
offspring, in the 2 years that follow, parents have increased rates of:• Single marital status
• Adjusted Relative Rate=1.18 (1.13-1.23)
• Depression• ARR=2.14 (1.88-2.43)
• Anxiety• ARR=1.41 (1.24-1.60)
• Outpatient physician contacts for mental illness• ARR=1.91 (1.61-2.26)
Model covariates: deceased child was an only child, parental status (mother vs. father), marital status, poverty, any mental disorder, any physical disorder, age of child at time of death, age of parent at time of child’s death
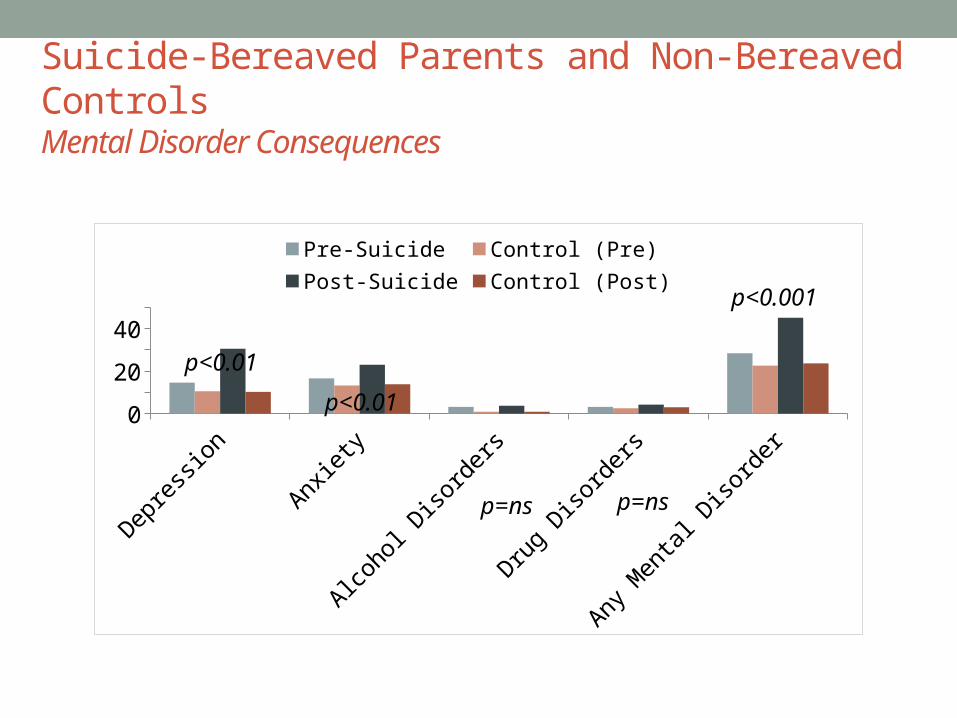
Suicide-Bereaved Parents and Non-Bereaved ControlsMental Disorder Consequences
Depre
ssio
n
Anxiet
y
Alco
hol D
isor
ders
Drug
Disor
ders
Any
Men
tal D
isor
der
0
15
30
45
Pre-Suicide Control (Pre) Post-Suicide Control (Post)
p<0.01
p<0.001
p=ns p=ns
p<0.01
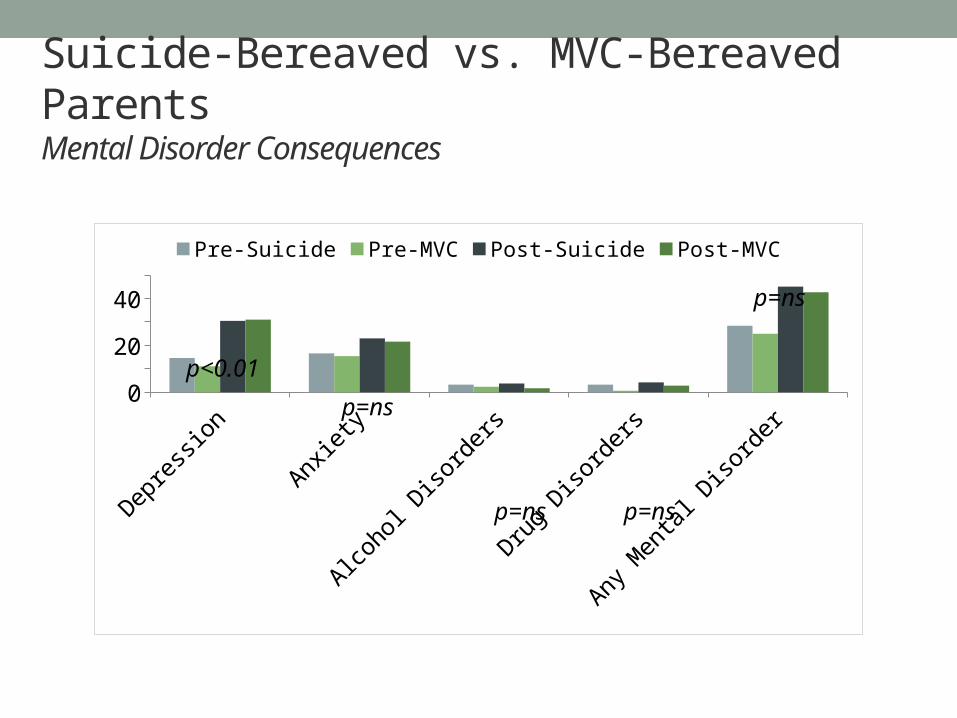
Suicide-Bereaved vs. MVC-Bereaved ParentsMental Disorder Consequences
Depre
ssio
n
Anxiet
y
Alco
hol D
isor
ders
Drug
Disor
ders
Any
Men
tal D
isor
der
0
15
30
45
Pre-Suicide Pre-MVC Post-Suicide Post-MVC
p=ns
p=ns p=ns
p=ns
p<0.01
Parents of Offspring who Die by SuicidePre-Death Observations
• Compared to the parents that will lose an offspring in an MVC, parents who will lose an offspring to suicide have higher rates of:• Depression (ARR=1.30)• Cardiovascular disease (ARR=1.54)• COPD (ARR=1.68)• Hypertension (ARR=1.37)• Diabetes (ARR=1.45)• Poverty (ARR=1.34)• Single marital status (ARR=1.21)• Hospitalization for physical disease (ARR=1.7)
Model covariates: deceased child was an only child, parental status (mother vs. father), marital status, poverty, any mental disorder, any physical disorder, age of child at time of death, age of parent at time of child’s death
Synthesis of Findings• The sudden death of a child has many negative
consequences on parents• Risk of depression, anxiety, marital break-up
• Alcohol and drugs do not appear to be coping mechanisms for grieving parents
• This study did not find differences between suicide and MVC bereavement• May be related to study design
• Parents of offspring who eventually die by suicide appear to have health and social vulnerabilities even prior to their offspring’s death
Limitations of administrative data• Identification of certain family relations
• Type of relation and age• Marriages are frequently not registered
• Measures in administrative data• Capture of suicide deaths• Certain outcomes are poorly recorded (or not at all)
• PTSD, grief, personality disorders
• Mental and physical disorders are dependent on treatment-seeking





























