Embed Size (px)
Citation preview

1
Submission
To: the Inquiry into the supply and use of methamphetamines, particularly ‘Ice’, in Victoria
From: the Victorian Aboriginal Community Controlled Health Organisation
Date: 18 October 2013

2
Contents1.Introduction ................................................................................................................. 2
2.Recommendations ....................................................................................................... 3
3.Victorian Aboriginal people and methamphetamine a snapshot ................................. 3
4.Data on Victorian Aboriginal people and methamphetamines ................................... 4
5.Victorian Aboriginal people and methamphetamine treatment .................................. 7
6.Evidence-based Drug and Alcohol Education Strategies .......................................... 11
7.Economic cost and the justice system ....................................................................... 12
1. Introduction
The Victorian Aboriginal Community Controlled Health Organisation (VACCHO)
was established in 1996 as the peak representative Aboriginal health body in Victoria.
VACCHO’s work is driven by the priorities of our members, Victoria’s Aboriginal
Community Controlled Health Organisations (ACCHOs) located across the state and
just over the border into New South Wales. By joining together under VACCHO’s
umbrella, ACCHOs gain strength, share knowledge and speak with a united voice.
VACCHO champions community control and health equality for Aboriginal
communities. We are a centre of expertise, policy advice, training, innovation and
leadership in Aboriginal health. VACCHO advocates for the health equality and
optimum health of all Aboriginal people in Victoria.
Methamphetamine issues are frequently raised by the VACCHO membership as issues
of urgent concern and VACCHO is involved in collating better evidence and
supporting member organisations in this space. Below we outline evidence collated
that focuses on Aboriginal Victorians and methamphetamines and provide associated
recommendations.

3
2. Recommendations
A. Improve understanding of effectiveness of treatment processes and treatment
outcomes for Aboriginal people with methamphetamine dependence
B. Increase diversionary options from the Justice System to Drug Treatment and
Mental Health support
C. Strengthen Aboriginal Community Controlled Health Services to deliver
evidenced based harm reduction approaches suited to local community needs
D. Strengthen Aboriginal Community Controlled Health Services to provide
evidenced based methamphetamine dependence treatment suited to local
community needs
E. Improve access to drug treatments, including timeliness to detoxification and
rehabilitation that address specific needs of methamphetamine, for example,
longer detoxification periods
F. The enquiry assess sustainable and systematic service provision that meets client
need
3. Victorian Aboriginal people and methamphetamine a snapshot
• 1 in 10 young Aboriginal people use methamphetamine compared to 1 in 20 young non-Aboriginal people
• Of young Aboriginal people who use methamphetamine 1 in 2 use daily or weekly compared to 1 in 10 non Aboriginal people
• Numbers of Aboriginal people in Victorian prisons have doubled in the last 10 years, almost all have drug dependence and this worsens after imprisonment
• Health providers in Aboriginal Community Controlled health Organisations request in regard to methamphetamine treatment- professional development- improved partnerships and- more timely access to detox and rehabilitation
• Aboriginal families with methamphetamine dependent members request improved support and skills in dealing with methamphetamine dependence
• Little evidence of effectiveness of methamphetamine health education and prevention programs that work with Aboriginal people
• Little evidence about effectiveness of methamphetamine treatment with Aboriginal people

4
• Concern that 'moral panic' about ICE, such as, ICE forums may further marginalise and deter methamphetamine users from help seeking behaviour. More targeted and solution focussed activities are required.
4. Data on Victorian Aboriginal people and methamphetamines
There is little information and data available about Victorian Aboriginal people and
methamphetamine use. The Victorian Aboriginal Health Service has just begun to
develop a research project planning to interview methamphetamine users. Below we
have outlined available data on Aboriginal Australians and methamphetamines.
GOANNA Survey, 2013
The GOANNA surveyi was conducted by the Kirby Institute in partnership with
VACCHO and others. The survey sample included Victorian Aboriginal young people.
Nationally the survey found that compared to the Australia Household Drug Survey ii
Both cannabis (21.3% vs 32%) and methamphetamine (5% vs 10%) use was
higher for Aboriginal young people
Higher everyday use of cannabis (11.2% vs 38%) and methamphetamine
(11.3% vs 53%) among Aboriginal young people
Similar rates of drug use to the GOANNA survey were identified in the National
Aboriginal and Torres Strait Islander Health Surveyiii (Figure 1).
Figure 1: Illicit substance use among Indigenous people aged 15 years and over

5
Notes: 1) Pain-killers/analgesics are for non-medicinal use.2) Estimate for LSD or synthetic hallucinogens in last 12 months has a relative standard error of between 25 and 50% and should be used with caution.
Source: Australian Government. National Aboriginal and Torres Strait Islander Health Survey, 2008
Qualitative study
A qualitative study with Aboriginal methamphetamine users in Sydney found that
most participants had reduced or were planning to reduce their drug use, or "at least
have it under control". Motivators for seeking treatment were to "keep out of jail",
"keep children", and because of a genuine desire to make positive changes in their
life. Some did not want their children to know of their drug use, or to become
involved with drugs themselves. Around half had tried residential rehabilitation in the
past and found it beneficial, all had relapsed.
Barriers to accessing treatment services focused on the rules and lack of freedom that
these services offer.
"I don't want to have to follow their rules."
"No freedom."
"I feel the program is judging me, as in preaching"iv.
VACCHO Ice forums
“Please don't produce any more resources it's a waste of money!!The mainstream and existing information is efficient”
In 2013 VACCHO ran three forums with Aboriginal Community Controlled Health
Organisations. Participants were a mixture of service providers and Aboriginal
community members and audience size varied from over 100 to 15. Participants were
asked to fill in evaluations with one question asking ‘what would you like more
information about’. Participants’ responses are grouped into themes in Table 1. In
particular, health staff requested professional development in methamphetamine

6
treatment and families wanted support to deal with methamphetamine dependent
family members and their behaviours. Rather than promoting ICE forums VACCHO
now recommends more targeted solution based workshops. There are also concerns
that 'ICE Forums' create moral panic and marginalise ICE users further potentially
deterring them from help seeking behaviour.
Table 1: Ice forum participant responses to the question, ‘What would you like more information about?’
Prevention
Participants thought early intervention for young at risk clients,
providing self-care, and holistic programs for young people were
important interventions.
Treatment
Participants wanted clarity on what harm reduction and treatment
options should be implemented for clients. More places in detox and
rehabilitation were needed. Family
support
Participants asked for better support and advice about how they can
make a difference with supporting loved ones.
Service accessMaking sure mainstream services were culturally safe and running
support programs for drug users and their families.
Sharing
information
Participants wanted to know more about helpful strategies that work
with Ice users and sharing of best practice models. Participants also
wanted more information about what Ice users need for their journey
to improved health.
Workers’ perspectives on the Victorian alcohol and drug treatment system
In November 2012 VACCHO facilitated a discussion of the proposed Victorian
government AOD treatment system reforms with a combined group of Aboriginal
AOD, mental health and social and emotional wellbeing (SEWB) workersv. The
focus of this discussion was barriers and enablers to effective treatment for Aboriginal
clients. Key themes drawn from this discussion were:
Complexity and breadth of responsibilities – The complexity of the work
required of AOD workers is not well understood or acknowledged
Staff turnover, lack of workforce stability – Participants perceived heavy
workloads and inadequate support for workers dealing with complex issues as
major causes of staff turnover

7
Regional/rural inequity – Disparities in treatment experienced by clients in
rural areas, compared to those living in metropolitan areas, including lack of
treatment facilities and lack of choice in service providers (e.g. the only GP in
town lacks knowledge of drug treatment). The requirement to move clients
from their families, off country to access treatment services was also
considered to be a consequence of the inequitable resourcing of rural/regional
communities
The first two dot points are compounded by a lack of training and supervision.
VACCHO’s most recent AOD and SEWB worker skills survey prepared for the
government identifies an undertrained and unsupported workforce. Among workers
surveyed, less than half (43%) had formal Diploma or Certificate IV level
qualifications in AOD. While 25% were undertaking training (mostly at a Cert IV
level), 32% did not have or were not completing AOD qualifications. In another
VACCHO survey only 20 of 47 AOD workers had an AOD qualification at Certificate
IV-level or higher. Workers also reported low levels of supervision with only 10
workers receiving regular supervision compared to 27 that did not receive supervision
or received inadequate supervision (10 workers were not on site to answer).
5. Victorian Aboriginal people and methamphetamine treatment
Aboriginal-specific programs for healing, detoxification and rehabilitation have
proven effective, with services including:
Wulgunggo Ngalu Learning Place, Gippsland – a 'learning place' for
Indigenous men undertaking community-based orders. A live-in program,
accommodates up to 20 men at one time
Bunjilwarra youth healing service, Hastings – currently closed
Baroona Healing Centre, Echuca – youth focused
Wulgunggo Ngalu Learning Place in Gippsland for Aboriginal men on community
based orders has achieved excellent results that continue to improve. The centre has
been open since 2008, however 66.7% of those referred in 2010/11 successfully

8
completed the program, a figure increasing to 76.6% in 2011/12 and 97.1% in the 11
months to May 2013vi.
The 2011 Bunjilwarra Healing Service evaluation found that young people required
repeated attempts at rehabilitation. Case studies demonstrated the complexities of
each young person’s background and a lack of structures and supports in their early
years. Turning lives around cannot happen in the immediate term. Participating in a
healing framework is only part of this process, but had the potential to be the
important and significant first step. The average length of stay was 69 days, with
some staying a few weeks and others longer. It was common for a young person to
stay for a short period followed by a longer period when they re-entered. The young
people were found to have complex issues and high levels of social disadvantage,
meaning the Healing Service addressed more than just substance abuse by
concurrently addressing broader health and wellbeing issues. The author found a
strength of Bunjilwarra was fostering an environment holding Indigenous culture in
high regard with young people frequently reporting that living in the house helped
them to be proud of their cultural background. For some this was a new experience
and others knew very little about their Indigenous background. The study author
suggests services and programs providing youth residential treatment or youth
detention are ineffective without appropriate aftercarevii.
A NSW study examining the outcomes of Aboriginal and non-Aboriginal people in an
Aboriginal-specific residential substance abuse rehabilitation centre found significant
improvements among participants completing treatment. Outcomes included reduced
psychological distress and increased refusal self-efficacy and empowerment.
Aboriginal people rated cultural components of treatment slightly more helpful than
non-Aboriginal participantsviii.
There is little data on success rates and treatment length in mainstream services.
Aboriginal people also use mainstream services, however their cultural safety has not
been assessed. A study assessing the acceptability and accessibility of mainstream
services for Aboriginal Australians with alcohol or drug use disorders found

9
Aboriginal people were well represented in an urban Area Health Service analysed by
the authors. Representative attendance was attributed to relationships between the
local hospital and the Aboriginal Medical Service (AMS), particularly in
pharmacotherapy dosing and outreach by Aboriginal staff members with the hospital’s
Drugs in Pregnancy Unit. An existing collaboration between the treatment service and
the AMS, including priority appointments for new Aboriginal clients, was also
identified as an influencing factor. Interviews identified increased flexibility of
services, increased outreach services and holistic and human care as the areas needing
improvement, and the importance of Aboriginal staffing was emphasised by clients
and staff membersix.
Evidence from meta-reviews of methamphetamine treatment options show few
proven treatments are availablex,xi,xii,xiii. Evidence from behavioural treatments have led
to reduced methamphetamine dependence, while pharmacotherapy-based treatments
are yet to demonstrate effectiveness in large randomised controlled trials. Behavioural
interventions demonstrating effectiveness include cognitive behavioural therapy
(CBT) and contingency management. Contingency management offers incentives
during treatment such as prizes and money to encourage abstinence. CBT-
Contingency management hybrids such as the Matrix Model have also demonstrated
improved outcomes although it is unclear if improvements are sustained over a longer
periodxiv,xv,xvi.
Outcomes from a Stimulant Treatment Program in NSW where participants received a
stepped-care approach including a median six counselling sessions over a three month
period achieved a reduction in methamphetamine use. While there was no change in
other drug use, crime or HIV risk behaviour, methamphetamine use in the preceding
month fell from 79% at entry to 53% and 55% at three month and six month follow
up. Reduction in use was more common among younger participants, people with no
history of drug treatment, and people without concurrent heroin use. Psychotic
symptoms, hostility and disability associated with poor mental health also reducedxvii.

10
Another NSW study on amphetamine treatment across NSW found regional and rural
areas are disproportionately affected and clients often presented with concurrent
cannabis and/or alcohol problems. Clients were overwhelmingly injecting drug users
with poor socio-demographic characteristics. Counselling was the most common
treatment service provided, followed by detoxification and residential rehabilitation.
Detoxification was usually provided in an in-patient setting, particularly within
metropolitan NSW. Compliance with residential rehabilitation was notably poor. The
authors concluded that interventions for amphetamine use need to consider the
majority of treatment clients will be based in a regional or rural setting, and treatment
for amphetamine users often involves concurrent cannabis and alcohol problemsxviii.
A study analysing barriers to methamphetamine withdrawal treatment in Australia
found current treatment practices are diverse and uncertain and a broad spectrum of
barriers identified. 24 AOD workers (managerial, clinical leadership, and
practitioners) were interviewed across Australia. The authors suggest that AOD
service providers are not clear about the best way to respond to clients seeking
methamphetamine withdrawal treatment and identified general pessimism about
withdrawal treatment for this group. The authors concluded that treatment services
should consider improving withdrawal protocols, educating clinicians and
reconsidering entry criteria to better respond to methamphetamine users who have
made the important first step into withdrawal treatmentxix.
Based on systematic reviews of interventions, the World Health Organization (WHO)
recommends the following related to methamphetamine use:
Dexamphetamine should not be offered for the treatment of stimulant use
disorders in non-specialized settingsxx
Brief interventions, based on motivational principles, should be offered for the
treatment of stimulant use disorders in non-specialist settingsxxi
Patients with stimulant use disorders who do not respond to short duration
psychological treatment may be referred for treatment in a specialist setting, when
availableibid

11
Individuals using cannabis and psychostimulants should be offered brief
intervention, when they are detected in non-specialized health care settings. Brief
intervention should comprise a single session of 5-30 minutes duration,
incorporating individualised feedback and advice on reducing or stopping
cannabis / psychostimulant consumption, and the offer of follow-upxxii
People with ongoing problems related to their cannabis or psychostimulant drug
use who does not respond to brief interventions should be considered for referral
for specialist assessmentibid
An analysis of relapse factors after methamphetamine treatment among people in the
United States found longer time in treatment resulted in improved outcomes. The
analysis also found no difference in relapse between residential and outpatient
treatment. People who had previously been enrolled in methamphetamine treatment
programs were found to have poorer outcomesxxiii.
6. Evidence-based Drug and Alcohol Education Strategies
Knowledge and awareness are generally ineffective for prevention of use of illicit
drugsxxiv. A Cochrane review of non-school based interventions including education
and skills training interventions, family interventions, and multi-component
community interventions found a lack of evidence proving their effectiveness in
preventing or reducing drug use by young peoplexxv. While some studies suggest some
interventions may be effective, small sample sizes, high loss to follow up and other
factors meant the authors could not draw firm conclusions. Similar conclusions were
drawn in a systematic review of primary prevention of cannabis usexxvi.
In a large, systematic review of tobacco and substance abuse prevention programs
interactive programs were found to be more effective than non-interactive programs,
with the latter described at best only marginally effective. Specifically, interactive
programs more effectively reduced, prevented and delayed drug use among
adolescents for tobacco, alcohol, and cannabis. Effectiveness was also linked to
smaller numbers of participantsxxvii.

12
Family-based drug prevention programs have only proven effective when
comprehensively implemented across life-spans and addressed multiple risk factors.
The programs also require content based on proven prevention theory and research,
material that is developmentally appropriate, sensitive to culture and community, of
sufficient length and regularly followed up, interactively taught, includes training for
prevention program providers, and evaluated to understand the effect on
behaviourxxviii. Developing and coordinating such a program state-wide would require
significant and sustained financial and human resources.
In a study of health behaviour modification, the most effective interventions across a
range of health behaviours included physician advice or individual counselling, and
workplace and school-based activitiesxxix. Other interventions to prevent drug use such
as public service announcements on radio, television, print and the Internet have
proven ineffectivexxx,xxxi.
7. Economic cost and the justice system
There has been considerable debate about the cost effectiveness of policies that target
activities to reduce drug supply. A recent review of policies aiming to reduce drug
supply, including those in Australia, found that over the time these policies had been
implemented drugs had become cheaper and of higher quality. The study concluded
that the policies had been ineffective in reducing drug supplyxxxii.

13
The number of Aboriginal prisoners in Victoria has increased 82% since 2006, almost
double the rate of non-Aboriginal prisoners. Aboriginal prisoners account for 7.4% of
Victoria’s prison populationxxxiii,xxxiv. The Koori Prisoner Mental Health and Cognitive
Functioning Study – conducted in a partnership between the Department of Justice,
VACCHO and Monash University – found very high levels of substance abuse
disorders (inclusive of methamphetamines) and mental illness among Victorian
Aboriginal and Torres Strait Islander prisoners. These rates were considerably higher
than for non-Aboriginal prisoners, contributing to increased contact with the justice
systemxxxv.

14
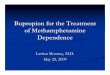
Figure 2: Lifetime prevalence of mental illness among Koori prisoners by gender
Notes: White bars indicate levels found among non-Aboriginal prison population
Source: Ogloff et al. Koori Prisoner Mental Health and Cognitive Function Study. Victorian Department of Justice. 2013
In the five years to September 2012 the number of Aboriginal people in Victorian prisons rose
by 144 peoplexxxvi. This represents an increase in prison expenditure of $45,360 per day in just
five years, or $16.6 million per annum. These figures do not price the consequent economic
costs of imprisonment (e.g. increased health and mental health services as well as losses in
productivity through inability to work) nor the social costs. Using recidivism rates among
Aboriginal prisoners as a yardstick for the effectiveness of imprisonment and prisoner
rehabilitation, the significant increase in prison expenditure has failed: more than half return
to prison within two years, rates are consistently 15 – 20 per cent higher among Aboriginal
prisoners, and despite some variability rates have actually worsened xxxvii.
Drug use is known to become more regular and more dependent once a person has entered
into the justice system.
“…in general, the lifetime drug using and offending career began with the
onset of offending, followed by the onset of illegal drug use, persisting into
regular offending, and finally regular illegal drug use. The first offence was

15
most likely to be minor property offending such as stealing without break-in or
vandalism, and the drug first used was most likely to be cannabis.”
Drugs and crime: a study of incarcerated male offenders,
Australian Institute of Criminology, 2003
The impact of imprisonment extends beyond prison expenditure. Prisoners are more likely to
die or be hospitalised, especially Aboriginal prisoners xxxviii xxxix. Hospitalisation costs (based
on bed days) of Aboriginal prisoners in the first year of release has been costed at $5.4 million
in Western Australia alone, driven predominantly by mental and behavioural disorders and
injuries xl. More than a third of Aboriginal women released from prison were hospitalised xli.
This is just one area of the health system, in one jurisdiction, over a relatively short period.
Aboriginal people are also much more likely to die after they are released from prison, most
commonly through suicide, motor vehicle accidents, circulatory system diseases and drug-
related deaths xlii xliii . These outcomes remain elevated throughout the first year of releasexliv
xlv. Aboriginal prisoners also experience poorer health, with much higher rates of sexually
transmitted infections, blood borne viruses, high blood sugar and diabetes, liver-disease
markers, asthma and more xlvi. These afflictions lead to poor quality of life and premature
death, and engender grief, loss, and trauma among family, friends, and communities.
These imprisonment costs bear a significant economic burden and an unquantifiable social
cost. The period following release from prison represents a significant opportunity to reduce
very high rates of morbidity and mortality and work alongside people to reduce rates of
recidivism. Significant investment at the transition period between prison and the community
could substantially reduce economic and social costs associated with health, mental health,
and re-imprisonment, and has proven effective at significantly improving health service
utilisation in Australia and overseasxlvii,xlviii,xlix,l..

i� Ward et al. Sexual health and relationships in young Aboriginal and Torres Strait Islander people.
Kirby Institute. 2013
ii� Australian Government. Australian Household Drug Survey. 2010
iii� Australian Government. National Aboriginal and Torres Strait Islander Health Survey, 2008
iv� Australian Government. Patterns of use and harms associated with specific populations of
methamphetamine users in Australia - exploratory research. 2008
v� Tunny N Policy Response to New directions for alcohol and other drug services: A roadmap
Worker discussion 1: Warrnambool SEWB forum evaluation report VACCHO Policy Unit 2012
vi� DOJ. Indigenous Offenders and Prisoners: Data Report to the July 2013 AJF. Victorian
Government Department of Justice. 2013
vii� Murphy, B. Final Report of the Koori Youth Alcohol and Drug Healing Service: YSAS &
Ngwala. Youth Research Centre, Melbourne Graduate School of Education, University of
Melbourne. 2011
viii� Berry, S.L. et al. Growth and Empowerment for Indigenous Australians in Substance Abuse
Treatment. International Journal of Mental Health and Addiction Vol 10(6). 2012
ix� Teasdale, K. et al. Improving services for prevention and treatment of substance misuse for
Aboriginal communities in a Sydney Area Health Service. Drug and alcohol review Vol 27(2). 2008
x� Hill, K.P. Treatment for Methamphetamine Dependence: Where Do We Stand? Current
Knowledge and Future Treatment Targets. Psychiatric Times Vol 25(1). 2008
xi� Kay-Lambkin, F.J. Technology and innovation in the psychosocial treatment of
methamphetamine use, risk and dependence. Drug and Alcohol Review Vol 27(3). 2008
xii� Baker A, Lee N.K. A review of psychosocial interventions for amphetamine use. Drug Alcohol
Rev. Vol 22(3). 2003
xiii� Brensilver M, et al. Pharmacotherapy of amphetamine-type stimulant dependence: An update.
Drug Alcohol Rev. 2013
xiv� Rawson R.A. et al. A multi-site comparison of psychosocial approaches for the treatment of
methamphetamine dependence. Addiction. Vol 99(6). 2004

xv� Lee N.K. & Rawson R.A. A systematic review of cognitive and behavioural therapies for
methamphetamine dependence. Drug Alcohol Rev. Vol 27(3). 2008
xvi� Maxwell JC. Emerging research on methamphetamine. Curr Opin Psychiatry. Vol 18(3). 2005
xvii� McKetin, R. et al. Treatment outcomes for methamphetamine users receiving outpatient
counselling from the Stimulant Treatment Program in Australia. Drug and Alcohol Review Vol
32(1). 2013
xviii� McKetin, R. et al. Characteristics of treatment provided for amphetamine use in New South
Wales, Australia. Drug and Alcohol Review Vol 24 (5). 2005
xix� Pennay, A. & Lee, N. Barriers to methamphetamine withdrawal treatment in Australia: Findings
from a survey of AOD service providers. Drug and Alcohol Review Vol 28(6). 2009
xx� WHO. Treatment of psychostimulant dependence [Internet]. [cited 2013 Apr 10]. Available from:
http://www.who.int/mental_health/mhgap/evidence/substance_abuse/q3/en/index.html
xxi� WHO. Psychosocial support for the management of psychostimulant use disorders [Internet]
[cited 2013 Apr 10]. Available from:
http://www.who.int/mental_health/mhgap/evidence/substance_abuse/q5/en/index.html
xxii� WHO. Brief psychosocial interventions [Internet]. [cited 2013 Apr 10]. Available
from:http://www.who.int/mental_health/mhgap/evidence/substance_abuse/q1/en/index.html
xxiii� Brecht M-L et al. Predictors of relapse after treatment for methamphetamine use. J
Psychoactive Drugs. Vol 32(2). 2000
xxiv� Strang, J. et al. Addiction 2: Drug policy and the public good: evidence for effective
interventions. The Lancet Vol 379(9810). 2012
xxv� Gates, S. et al. Interventions for prevention of drug use by young people delivered in non-
school settings (Review), John Wiley & Sons Ltd. 2009
xxvi� Norberg, M. et al. Primary Prevention of Cannabis Use: A Systematic Review of Randomized
Controlled Trials, PLoS ONE 8(1): e53187. 2013
xxvii� Tobler, N.S. et al. School-Based Adolescent Drug Prevention Programs: 1998 Meta-Analysis.
Journal of Primary Prevention Vol 20(4). 2000

xxviii� Dusenbury, L. Family-Based Drug Abuse Prevention Programs: A Review. Journal of Primary
Prevention Vol 20(4). 2000
xxix� Jepson, R.G. et al. The effectiveness of interventions to change six health behaviours: a review
of reviews. BMC Public Health Vol 10(1). 2010
xxx� Werb, D. et al. The effectiveness of anti-illicit-drug public-service announcements: a systematic
review and meta-analysis. Journal of Epidemiology and Community Health Vol 65(10). 2011
xxxi� Jepson, R.G. et al. The effectiveness of interventions to change six health behaviours: a review
of reviews. BMC Public Health Vol 10(1). 2010
xxxii� Werb D, Kerr T, Nosyk B, Strathdee S, Julio Montaner J, Evan Wood E, The temporal
relationship between drug supply indicators: an audit of international government surveillance
systems. BMJ Open 2013;3:e003077 doi:10.1136/bmjopen-2013-003077
xxxiii� DOJ. Statistical Profile of the Victorian prison system 2005-06 to 2009-10. Victorian
Government Department of Justice. 2010
xxxiv� DOJ. Indigenous Offenders and Prisoners: Data Report to the July 2013 AJF. Victorian
Government Department of Justice. 2013
xxxv� Ogloff et al. Koori Prisoner Mental Health and Cognitive Functioning Study. Victorian
Department of Justice. 2013
xxxvi� Shuard J. Department of Justice Data Report to the November 2012 AJF. Echuca; 2012.
xxxvii� Stathis S, Letters P, Doolan I, Fleming R, Heath K, Arnett A, et al. Use of the Massachusetts
Youth Screening Instrument to assess mental health problems in young people within an Australian
youth detention centre. J Paediatr Child Health. 2008 Aug;44(7-8):438–43.
xxxviii� Stewart LM, Henderson CJ, Hobbs MST, Ridout SC, Knuiman MW. Risk of death in
prisoners after release from jail. Australian and New Zealand Journal of Public Health. 2007 Sep
25;28(1):32–6.
xxxix� Kinner SA, Preen DB, Kariminia A, Butler T, Andrews JY, Stoové M, et al. Counting the cost:
estimating the number of deaths among recently released prisoners in Australia. Med. J. Aust. 2011
Jul 18;195(2):64–8

xl� Alan J, Burmas M, Preen D, Pfaff J. Inpatient hospital use in the first year after release from
prison: a Western Australian population-based record linkage study. Australian and New Zealand
Journal of Public Health. 2011;35(3):264–9.
xli� Alan J, Burmas M, Preen D, Pfaff J. Inpatient hospital use in the first year after release from
prison: a Western Australian population-based record linkage study. Australian and New Zealand
Journal of Public Health. 2011;35(3):264–9.
xlii� Stewart LM, Henderson CJ, Hobbs MST, Ridout SC, Knuiman MW. Risk of death in prisoners
after release from jail. Australian and New Zealand Journal of Public Health. 2007 Sep
25;28(1):32–6.
xliii� Kinner SA, Preen DB, Kariminia A, Butler T, Andrews JY, Stoové M, et al. Counting the cost:
estimating the number of deaths among recently released prisoners in Australia. Med. J. Aust. 2011
Jul 18;195(2):64–8
xliv� Stewart LM, Henderson CJ, Hobbs MST, Ridout SC, Knuiman MW. Risk of death in prisoners
after release from jail. Australian and New Zealand Journal of Public Health. 2007 Sep
25;28(1):32–6.
xlv� Kinner SA, Preen DB, Kariminia A, Butler T, Andrews JY, Stoové M, et al. Counting the cost:
estimating the number of deaths among recently released prisoners in Australia. Med. J. Aust. 2011
Jul 18;195(2):64–8
xlvi� Indig D, McEntyre E, Page J, Ross B. 2009 NSW Inmate Health Survey: Aboriginal Health
Report. Sydney: Justice Health; 2010.
xlvii� Kinner SA, Lennox NG, Taylor M. Randomized Controlled Trial of a Post-Release
Intervention for Prisoners With and Without Intellectual Disability. J Dev Disabil. 2009;15(2):72–6
xlviii� Wang EA, Hong CS, Shavit S, Sanders R, Kessell E, Kushel MB. Engaging individuals
recently released from prison into primary care: a randomized trial. Am J Public Health. 2012
Sep;102(9):e22–29
xlix� Wang EA, Hong CS, Samuels L, Shavit S, Sanders R, Kushel M. Transitions Clinic: Creating a
Community-Based Model of Health Care for Recently Released California Prisoners. Public Health
Rep. 2010;125(2):171–7

l� AHRQ. Community-Based Clinic Enhances Access to Medical Care and Reduces Emergency
Department Visits for Chronically Ill Recently Released Prisoners [Internet]. 2011 [cited 2013 Apr
23]. Available from: http://www.innovations.ahrq.gov/content.aspx?id=3195