Embed Size (px)
Citation preview

CentralBringing Excellence in Open Access
Journal of Cardiology & Clinical Research
Cite this article: Pavri BB, Wong KL, Ho RT, Kocovic DZ (2014) Autonomic Modulation during Stable and Unstable Ventricular Tachycardia. J Cardiol Clin Res 2(4): 1039.
*Corresponding authorBehzad B Pavri, Thomas Jefferson University Hospital, 925 Chestnut Street, Philadelphia, PA 19107, USA, Tel: 215-955-8882; Fax: 215-503-3976; Email:
Submitted: 16 October 2014
Accepted: 18 Novemebr 2014
Published: 20 Novemebr 2014
ISSN: 2333-6676
Copyright© 2014 Pavri et al.
OPEN ACCESS
Keywords•Ventricular tachycardia•Electrophysiology•Monomorphic•Blood pressure
Research Article
Autonomic Modulation during Stable and Unstable Ventricular TachycardiaBehzad B Pavri1*, Kar-Lai Wong2, Reginald T Ho1 and Dusan Z Kocovic2
1Thomas Jefferson University Hospital, USA2Lankenau Hospital, USA
Abstract
Objective: This study was designed to study the role of autonomic function in hemodynamic stability during Ventricular Tachycardia (VT).
Background: Sustained VT may be hemodynamically tolerated or may result in syncope. Autonomic modulation may play an important role in the hemodynamic consequences of VT.
Methods: The study was performed in two parts: (1) A retrospective review of electrophysiology studies with induced VT with ventriculo-atrial dissociation; and (2) Prospective performance of three standardized tests of autonomic function (isometric handgrip, Valsalva maneuver, deep breath test) in 45 patients with inducible VT. Sinus Cycle Length (SCL) was measured for the first 20 seconds during VT from the high right atrial electrogram, and compared in patients with stable and unstable VT with ventriculo-atrial dissociation.
Results: SCL shortened in patients with stable VT (from 778 ms at VT onset to 664 ms at 20 s, p<0.001), whereas SCL did not change in patients with unstable VT (803 ms to 790 ms, p=0.8). Stable VT patients were more likely to have normal results on standardized autonomic tests as compared to patients with unstable VT. Both groups had comparable LV function and medication use, although VT rate was faster in the unstable group.
Conclusion: Sinus acceleration during VT, preserved autonomic function, and slower VT rate were associated with hemodynamic stability. Standardized autonomic test results correlated with hemodynamic behavior during VT. Based upon these data, we conclude that in addition to VT rate, the ability of the autonomic nervous system to respond to abrupt-onset tachycardia may influence hemodynamic stability during VT.
INTRODUCTIONThe hemodynamic response to sustained monomorphic
Ventricular Tachycardia (VT) is of clinical importance. Patients presenting with tolerated (non-syncopal) VT are more likely to have tolerated recurrences and a better prognosis as compared to patients who present with syncope [1-6]. Although the determinants of hemodynamic stability are not fully understood, VT rate is clearly an important factor. Other factors that likely contribute to hemodynamic stability include the initial response and subsequent changes in sympathovagal balance that attempt to compensate for the sudden drop in Blood Pressure (BP) that accompanies the VT onset.
The goals of this study were to examine the differences in autonomic response in patients with hemodynamically stable and unstable VT, both during VT and during sinus rhythm based on autonomic responses to standardized tests of
autonomic function. The study was performed in two phases: a retrospective analysis of previously acquired electrograms during VT induced in the Electrophysiology (EP) laboratory, and a prospective study where patients with inducible VT underwent additional non-invasive assessment of the autonomic nervous system. The purpose of the prospective study was to correlate autonomic tone as assessed by standardized non-invasive testing to hemodynamic stability of the induced VT episode. We hypothesized that patients with hemodynamically tolerated VT would exhibit preserved autonomic reflexes, as compared to patients with poorly tolerated VT.
METHODS
Retrospective study
Patient selection: Consecutive patients who had inducible sustained monomorphic VT with Ventriculo-Atrial (VA)

CentralBringing Excellence in Open Access
Pavri et al. (2014)Email:
J Cardiol Clin Res 2(4): 1039 (2014) 2/6
dissociation at the time of diagnostic EP study were included. Informed consent was obtained from all patients. If a patient had multiple episodes of VT induced during the EP study, the first sustained episode was selected for analysis, in order to eliminate any confounding influences from hemodynamic or autonomic perturbations resulting from prior VT episodes.
Exclusion criteria: Patients with ectopic atrial tachycardia, atrial fibrillation or flutter within 48 hours of the study were excluded. Patients with clinically evident sinus node dysfunction (clinical history suggestive of chronotropic incompetence or corrected sinus node recovery times > 550 ms) were excluded. Patients with frequent premature atrial complexes were excluded, since frequent ectopy confounded assessment of sinus node behavior. Finally, patient with any degree of VA conduction during VT were excluded.
Electrophysiology study: EP studies were performed in the post-absorptive state. Three 6 French quadripolar catheters were positioned in the High Right Atrium (HRA), the His bundle region and the Right Ventricular (RV) apex. The RV apex catheter was moved later to the RV outflow tract. A 5-French vascular sheath was placed in the right femoral artery for BP monitoring. Programmed ventricular stimulation was performed using squared stimuli of 2 ms duration delivered at twice diastolic threshold. Programmed ventricular stimulation was performed using up to triple extrastimuli at 2 drive cycle lengths (600 and 400 ms) from the RV apex and the RV outflow tract. Coupling intervals of extrastimuli were reduced by 10 ms decrements until ventricular refractoriness was reached or until sustained VT was induced. When monomorphic VT was induced, the arrhythmia was allowed to continue for at least 30 seconds unless the patient experienced hemodynamic collapse. Termination was achieved by over-drive burst pacing or external cardioversion. Patients were not electrically cardioverted unless they were unconscious. The nurses and physicians involved in the study assessed level of consciousness by direct evaluation of the patient, seeking response to verbal and tactile stimuli.
Measurements: Sinus cycle length: The HRA catheter recording was used to study sinus node behavior during VT episodes. The sinus cycle length was measured as consecutive atrial-atrial intervals from the HRA catheter Electrogram (EGM.) Occasional premature atrial complexes and the subsequent cycle were excluded. The sinus cycle length was measured at VT induction (T0), at 10 (T10) and 20 seconds (T20) into VT. The percentage change in SCL at Tn was calculated as {SCL(Tn) – SCL (T0)}/SCL (T0).
Hemodynamic definitions: Unstable VT was defined as VT requiring termination within 30 seconds by overdrive pacing or external cardioversion due to impending or actual loss of consciousness. Patients were designated as having stable VT if they did not require urgent termination of the arrhythmia.
Prospective study
Patient selection: All consenting patients with sustained clinical VT or syncope who had inducible VT at diagnostic EP study were included. The same exclusion criteria described in the retrospective study were used to screen the prospective cohort. However, VA dissociation was not a requirement for inclusion,
since the purpose of the prospective study was to correlate autonomic tone as assessed by standardized non-invasive testing to hemodynamic stability of the induced VT episode.
Sinus node behavior: In patients who had VA dissociation during VT, the behavior of the atrial cycle length was assessed as in the retrospective study.
Autonomic function testing: Each patient underwent standardized non-invasive autonomic function testing within 48 hours of EP study. The institutional review board approved the consent form for autonomic function testing. All patients were categorized into either stable or unstable groups, based on the above definitions, prior to performance of the following autonomic function tests:
Isometric hand grip: Patients were asked to squeeze a hand dynamometer (JAMARTM, Jackson, MI) at 30% of their voluntary maximal contraction for as long as possible or a maximum of 5 minutes. BP was monitored continuously with a non-invasive radial artery tonometer (Colin 7000 TM). The test was repeated 3 times with adequate rest periods between trials. The average maximal rise in diastolic BP was calculated by averaging the maximal diastolic BP from each trial. A rise in diastolic BP by 15mmHg or greater (over baseline diastolic BP) was considered a normal response. A blunted rise (<15mmHg) was considered to be a marker of decreased sympathetic activity [7,8].
Valsalva maneuver: Patients were asked to blow into the barrel of a 20cc syringe with the plunger removed, and with a small puncture made in the barrel wall to allow an air leak. The syringe was attached to a sphygmomanometer, and the patient was instructed to blow into the barrel to raise the column of mercury to 40mmHg with a single breath. The air leak provided by the puncture ensured that the glottis stayed open during the entire maneuver. After a training run, the patient performed 3 Valsalva maneuvers with a 5 minute rest period between trials. The ECG was continuously recorded at 50 mm/sec paper speed and 20 mm/mV amplification for 1 minute prior to, and during each trial. A “tachycardia ratio” was calculated as the ratio of the minimal RR interval during the strain phase to the maximal RR interval prior to the onset of the maneuver. The average tachycardia ratio of 3 trials was calculated. An abnormal Valsalva test was defined as a tachycardia ratio of >0.85, and was considered to be a marker of decreased sympathetic modulation [9,10].
Deep breath test: Patients were asked to inhale slowly and deeply over 5 seconds and to exhale over 5 seconds, thus breathing at 6 breaths per minute, for a total of 8 breaths. This respiratory rate has been shown to produce maximal heart rate variability in normal subjects [11]. Continuous 3 lead ECG was recorded at 50mm/sec paper speed and 20mm/mV amplification. The difference in the maximum heart rate during inspiration and the minimum heart rate during expiration was calculated for each breath. Five of 8 breaths with the largest heart rate difference were averaged to provide an index of respirophasic parasympathetic modulation. An abnormal deep breath test was defined as a heart rate variation of less than 15 bpm during deep breathing, and was indicative of abnormal vagal modulation [9].

CentralBringing Excellence in Open Access
Pavri et al. (2014)Email:
J Cardiol Clin Res 2(4): 1039 (2014) 3/6
Statistical methods
The paired Students’ t test was used to compare changes in sinus cycle length during VT. The unpaired Students’ t test was used to compare sinus cycle length and continuous variables of autonomic function testing between the groups with stable and unstable VT. Dichotomous variables of autonomic function testing (normal or abnormal) were analyzed using the Chi square test. The data are expressed as mean values ± SD.
RESULTSThere were 20 patients in the retrospective group, and 45
patients in the prospective group.
Patient characteristics
The patient characteristics of the prospective (n=45) group of patients are shown in Table 1. There was no difference in left ventricular ejection fraction or NYHA class in patients with stable and unstable VT, although patients with unstable VT tended to be older (p=0.05). Syncope was more commonly the presenting symptom in patients in the unstable group (p<0.001). Patients with unstable VT were more likely to have a history of coronary artery disease (p=0.04) and be on amiodarone therapy (p=0.02).
Sinus node behavior and VT cycle length
There was no difference in sinus node behavior in the retrospective and prospective portions of the study, and hence the combined data were analyzed collectively (Table 2). Patients with unstable VT had shorter VT cycle lengths than patients with stable VT (266 vs.384ms, p=0.02). In 38 patients with stable VT, the sinus cycle length shortened from VT onset (mean SCL at T0=778 ms), to 10 seconds (mean SCL at T10=674 ms) and further at 20 seconds (mean SCL at T20=654 ms) into VT (p<0.001 for all comparisons). In 27 patients with unstable VT, there was no significant change in sinus cycle length at 10 or 20 seconds into VT (mean CL at T0=803 ms, at T10=787 ms, and at T20=790 ms, all p=NS). The percentage change in sinus cycle length at 10 and 20 seconds was significantly different between the stable and unstable groups (p<0.001 at T10 and p=0.004 at T20).
Autonomic function testing (figure)
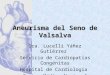
Of 45 enrolled patients, 37 underwent standardized autonomic function testing. Three patients refused, 1 patient was unable to follow instructions regarding the deep breath test, and 4 patients were discharged from the hospital before autonomic testing could be performed. The results of autonomic function tests are shown in Tables 3 and 4. The isometric handgrip test was the best discriminator between the patients with stable and unstable VT. All patients in the stable VT group had a normal response to handgrip, compared to only 27% in the unstable group. The results of the Valsalva maneuver were also significantly different between the two groups (p<0.001), but the results of the deep breath test were not (p=0.15).
DISCUSSION
Previous studies
The response of the autonomic nervous system to tachycardia has been assessed in animal and human studies. Welch et al [12]
Clinical Characteristic Stable VT Unstable VT p value
Number of patients 26 19
Age 61.1±14.8 69.1±11 0.02
Gender (number male) 26 17 0.64
Left ventricular ejection fraction 0.32±0.16 0.28±0.14 0.45
NYHA class 2.0±1.0 2.2±0.98 0.49
Coronary artery disease 21 18 0.09
Diabetes mellitus 4 6 0.16
Amiodarone use 5 10 0.02
Beta blocker use 15 8 0.30
Ace-inhibitor use 21 12 0.19
Table 1: Clinical characteristics of patients in the prospective group.
Stable Unstable p value
Number of VT episodes 38 27 -Baseline mean sinus cycle length
(ms) 778±169 799±195 0.65
Cycle length of induced VT (ms) 384±313 266±44 0.02
Systolic BP in VT at T10 (mmHg) 80±26 40±11 <0.001
Mean sinus cycle length at T10 (ms) 674±134 787±185 0.01
Percentage change in SCL at T10 -12.5±10.1 -1.3±8.6 <0.001
Systolic BP in VT at T20 (mmHg) 93±25 40±6 <0.001
Mean sinus cycle length at T20 (ms) 654±131 790±193 0.01
Percentage change in SCL at T20 -14.6±12.2 -3.5±12.7 0.004
Table 2: Sinus node behavior (retrospective and prospective groups combined).
Autonomic Function Test Stable(n=23)
Unstable(n=15) p value
Change in diastolic BP with isometric handgrip (mmHg) 26±9 9±6 <0.001
Number (%) of patients who passed isometric handgrip test
23 (100%) 4 (27%) <0.001
Mean tachycardia ratio during Valsalva maneuver 0.79 0.88 0.003
Number (%) of patients who passed Valsalva maneuver test 16 (73%) 2 (13%) <0.001
Mean heart rate change during deep breath test (breaths/m) 11±8 7±5 0.06
Number (%) of patients who passed deep breath test 5 (25%) 1 (7%) 0.15
Table 3: Results of autonomic function testing in the prospective group.
Autonomic Function Test Sensitivity Specificity PPV NPV
Isometric Handgrip Test 73 100 100 85
Valsalva Maneuver 87 70 65 89
Deep Breath Test 93 22 44 83
Table 4: Sensitivity, Specificity, Negative and Positive Predictive Values for autonomic function tests in predicting hemodynamics during VT. All values are percentages.
Abbreviations: PPV: Positive Predictive Value; NPV: Negative Predictive Value

CentralBringing Excellence in Open Access
Pavri et al. (2014)Email:
J Cardiol Clin Res 2(4): 1039 (2014) 4/6
reported that sympathetic nerve traffic increased following single Ventricular Premature Depolarizations (VPDs), and was suppressed immediately following VPDs. They noted that the degree of sympathetic activation was proportional to the prematurity of the VPD. Waxman et al [13] studied hemodynamics during right atrial pacing at 200 bpm. They noted a dramatic fall in BP, followed by a brisk overshoot with coincidental reflex sinus bradycardia after termination of pacing. Significant improvement in initial hypotension was noted with continued pacing. These observations confirmed the role of sympathetic activation in response to BP fall during tachycardia.
Smith et al [14] found that autonomic changes within the first 10 seconds of VT predicted hemodynamics at 1 minute
into VT. With stepwise regression, systolic BP at 1 minute was best predicted by VT rate (R2=0.52, p=0.0005) the sympathetic response at 10 seconds (R2=0.65, p=0.0002) and left ventricular ejection fraction (R2=0.7, p=0.0001.) Further, sympathetic nerve activity increased 92% at 10 seconds into VT in direct proportion to fall in BP, and remained 83% above pre-VT levels at 1 minute. Morady et al [15] studied 13 patients with unstable VT induced during EP study. They measured arterial plasma epinephrine and nor-epinephrine levels before, during, and at 1, 3, 5, 10 & 15 minute intervals after VT. VT required terminated by external counter shock in an average time of 18 seconds due to hemodynamic collapse. The mean VT cycle length was 187 ms (>300 bpm), and all patients lost consciousness with a mean blood pressure of 28
0
5
10
15
20
25
30
Change in Diastolic BP with Isometric Handgrip
00.10.20.30.40.50.60.70.80.9
1
Mean Tachycardia Ratio During Valsalva
0102030405060708090
100
% of patients who passed isometric handgrip test
0102030405060708090
100
% of patients who passed Valsalva Maneuver
0
10
20
30
40
50
60
70
80
90
100
% of patients who passed Deep Breathing
0
2
4
6
8
10
12
14
16
18
20
Mean HR Change during Deep Breathing
Figure 1 Autonomic function test results.

CentralBringing Excellence in Open Access
Pavri et al. (2014)Email:
J Cardiol Clin Res 2(4): 1039 (2014) 5/6
mm Hg. Both epinephrine and nor-epinephrine levels did not change during unstable VT, but increased by more than 3 fold 1 minute after the defibrillation shock. Thus non-neural responses to unstable VT are slow to occur. The same group of investigators also reported on 22 patients with stable VT during EP study [16]. They measured arterial plasma epinephrine and nor-epinephrine levels before, during, and 15-30 s after VT. The mean VT cycle length was 328 ms (180 bpm) and no patient lost consciousness, with a mean BP=76 mm Hg during VT. Epinephrine levels did not change during or after VT, whereas nor-epinephrine levels increased both during and after VT.
Huikuri et al [17] studied sinus node behavior in 32 patients with inducible VT and VA dissociation during 32 episodes of stable VT and 21 episodes of unstable VT. The atrial cycle length was measured before and every 5 seconds into VT. Patients with unstable VT had significantly shorter VT cycle length. (235 ms vs. 320 ms; p<0.05.) During stable VT, the sinus rate accelerated during VT. In unstable VT, sinus rate accelerated initially but then decelerated 10 seconds into VT, resulting in slower sinus rate at VT termination than at VT initiation. Intravenous propranolol was infused in 6 patients with unstable VT and 4 with stable VT. In patients with stable VT, the initial sinus acceleration was unchanged but was followed by a decrease in sinus rate 20 sec into VT. Two patients with initially stable VT became unstable requiring cardioversion. In patients with unstable VT, there were no significant changes in sinus node behavior after propranolol infusion. The authors concluded that the lack of effect of propranolol on initial sinus acceleration suggested that vagal withdrawal, rather than sympathetic activation, played a greater role in determining initial sinus node behavior at the onset of VT. The sinus acceleration that occurred later during sustained stable VT may be due to subsequent sympathetic activation. They postulated that the mechanism(s) for sinus slowing during unstable VT may include compromised sinus node response to autonomic control due to decreased sinus node perfusion, or there may be a failure of baroreceptor compensation.
Finally, preserved baroreflex sensitivity post-myocardial infarction has been associated with hemodynamic stability during sustained monomorphic VT. Landolina et al [18] observed that baroreflexes were impaired in 13 patients with unstable VT, as compared to 11 patients with hemodynamically unstable VT, although the groups were comparable in age, left ventricular function and VT rate.
Present study
Sinus node behavior: The results of the current study confirm the observations of Huikuri et al [17]. Sinus node behavior during VT with VA dissociation was consistently different in patients with stable and unstable VT. Episodes of stable VT were associated with sinus node acceleration, whereas unstable VT episodes were accompanied by lack of sinus acceleration, and sometimes sinus slowing. One might have expected the contrary, since a greater fall in BP (as seen during unstable VT episodes) might be expected to trigger a greater sympathetic response and result in greater sinus acceleration. The results of this and previous studies suggest that the behavior of the sinus node is not simply a response to the hypotension seen during unstable VT, but a marker of ongoing autonomic modulation.
(a) The mechanism(s) underlying these different patterns of autonomic modulation during stable and unstable VT are unknown, but one may postulate the following:The observed differences in the stable and unstable VT groups may relate to the demonstrated differences in baseline autonomic function, as demonstrated by the results of standardized testing in this study. Patients with abnormal autonomic function at baseline may demonstrate abnormal autonomic modulation during VT, contributing to hemodynamic instability.
(b) It may also be postulated that the mechanical deformation of the ventricles during unstable VT episodes may trigger vagal afferent (mechanoreceptor) nerve endings in the myocardium that result in an inappropriate vagal activation, resulting in peripheral vasodilatation, sinus slowing and unstable hemodynamics. This would be akin to the Bezold-Jarisch reflex that is postulated to occur during vasovagal syncope and during acute inferior wall infarction. Such activation of vagal afferents may not occur during stable VT episodes, thereby allowing peripheral vasoconstriction and sinus acceleration, resulting in stable hemodynamics.
(c) In the authors’ opinion, sinus node ischemia is a less plausible explanation; the lack of sinus acceleration was evident within 5-10 seconds of VT onset, which was probably not sufficient time to cause significant sinus node ischemia. The sinus node artery is disproportionately large considering the extent of the area it supplies [19,20] and up to 10% of patients can have a dual arterial supply [21]. Therefore the sinus node would be unlikely to develop acute ischemic dysfunction within 5-10 seconds related to a drop in perfusion pressure.
Autonomic function testing (Table 4 and figure): This is the first study showing remarkable correlation between results of standardized non-invasive autonomic function tests and the hemodynamic response during VT. These simple bedside tests were able to separate, as groups, patients with stable and unstable VT. Patients with unstable VT were more likely to have abnormal autonomic responses during standardized autonomic function tests. The isometric handgrip test had the best results in distinguishing patients with stable (100% had normal results) and unstable VT (27% had normal results). The superior performance of the isometric handgrip test may suggest that the ability to activate sympathetic tone is crucial to hemodynamic stability.
The importance of VT rate in hemodynamic stability cannot be disputed; however, there was a clear difference in the autonomic profiles of patients with stable and unstable VT. We paired 7 patients with stable VT with 7 patients with unstable VT, using the criterion of similar VT rates (VT cycle lengths less than 10ms apart, mean VT CL=240ms, range 220-340ms, Table 5). Although VT cycle lengths were similar, the results of autonomic function testing, especially the isometric handgrip test, were significantly different. All patients with stable VT had normal results with isometric handgrip, as compared to 17% with unstable VT (p<0.001). The respective values for Valsalva testing were 67% and 14% (p=0.01), and for deep breath test were 17% and 0% (p<0.001). Thus, in spite of comparable VT cycle lengths during VT, patients with stable VT were more likely to have normal autonomic function, as compared to patients with unstable VT.

CentralBringing Excellence in Open Access
Pavri et al. (2014)Email:
J Cardiol Clin Res 2(4): 1039 (2014) 6/6
Possible Clinical Significance: Aside from providing mechanistic insight into hemodynamic adaptation during VT, the results of this study may provide an opportunity to test novel algorithms for dual chamber defibrillators. For example, in patients with VA dissociation during VT, anti-tachycardia pacing may be attempted for a longer time as long as the atrial rate is accelerating. However, if the atrial cycle length is not accelerating, the defibrillator could be programmed to abandon anti-tachycardia pacing sooner, and proceed with cardioversion shock therapy. Stored data from dual chamber defibrillator may be analyzed to determine whether patients showing atrial rate acceleration during spontaneous VT episodes have better prognosis as compared to patients showing lack of atrial rate acceleration.
CONCLUSIONBased upon these results, we conclude that sinus node
behavior is different in patients with stable and unstable VT, with clear sinus acceleration occurring in the stable group. This behavior is not simply a reflex response to the hypotension that accompanies the onset of VT, but rather a marker of on-going autonomic modulation that influences hemodynamic stability during VT. This is the first study showing that patients with stable VT are more likely to have normal results during simple, non-invasive tests of autonomic function. These findings are best explained by postulating an underlying difference in the ability of the autonomic nervous system to respond to abrupt tachycardia, especially prompt sympathetic activation in patients with stable VT.
REFERENCES1. Hamer AW, Rubin SA, Peter T, Mandel WJ. Factors that predict
syncope during ventricular tachycardia in patients. Am Heart J. 1984; 107: 997-1005.
2. Kadish AH, Buxton AE, Waxman HL, Flores B, Josephson ME, Marchlinski FE. Usefulness of electrophysiologic study to determine the clinical tolerance of arrhythmia recurrences during amiodarone therapy. J Am CollCardiol. 1987; 10: 90-96.
3. Gottlieb CD, Berger MD, Miller JM, Lesh MD, Rosenthal ME, Marchlinski FE, et al. What is an acceptable risk for cardiac arrest patients treated with amiodarone? Circ. 1988; 78.
4. Brugada P, Talajic M, Smeets J, Mulleneers R, Wellens HJ. The value of the clinical history to assess prognosis of patients with ventricular tachycardia or ventricular fibrillation after myocardial infarction. Eur Heart J. 1989; 10: 747-752.
5. Saxon LA, Uretz EF, Denes P. Significance of the clinical presentation in ventricular tachycardia/fibrillation. Am Heart J. 1989; 118: 695-701.
6. Sarter BH, Finkle JK, Gerszten RE, Buxton AE. What is the risk of sudden cardiac death in patients presenting with hemodynamically stable sustained ventricular tachycardia after myocardial infarction? J Am Coll Cardiol. 1996; 28: 122-129.
7. Ewing DJ, Irving JB, Kerr F, Wildsmith JA, Clarke BF. Cardiovascular responses to sustained handgrip in normal subjects and in patients with diabetes mellitus: a test of autonomic function. Clin Sci Mol Med. 1974; 46: 295-306.
8. McAllister RG Jr. Effect of adrenergic receptor blockade on the responses to isometric handgrip: studies in normal and hypertensive subjects. J Cardiovasc Pharmacol. 1979; 1: 253-263.
9. Ziegler D, Laux G, Dannehl K, Spuler M, Muhlen H, Mayer P, et al. Assessment of cardiovascular autonomic function: age related normal ranges and reproducibility of spectral analysis, vector analysis, and standard tests of heart rate variation and blood pressure responses. Diabet Med. 1992; 9: 166-175.
10. Levin AB. A simple test of cardiac function based upon the heart rate changes induced by the Valsalva maneuver. Am J Cardiol. 1966; 18: 90-99.
11. Mackay JD. Respiratory sinus arrhythmia in diabetic neuropathy. Diabetologia. 1983; 24: 253-256.
12. Welch WJ, Smith ML, Rea RF, Bauernfeind RA, Eckberg DL. Enhancement of sympathetic nerve activity by single premature ventricular beats in humans. J Am Coll Cardiol. 1989; 13: 69-75.
13. Waxman MB, Cameron DA. The reflex effects of tachycardias on autonomic tone. Ann N Y Acad Sci. 1990; 601: 378-393.
14. Smith ML, Ellenbogen KA, Beightol LA, Eckberg DL. Sympathetic neural responses to induced ventricular tachycardia. J Am Coll Cardiol. 1991; 18: 1015-1024.
15. Morady F, DiCarlo LA Jr, Halter JB, de Buitleir M, Krol RB, Baerman JM. The plasma catecholamine response to ventricular tachycardia induction and external countershock during electrophysiologic testing. J Am CollCardiol. 1986; 8: 584-591.
16. Morady F, Halter JB, DiCarlo LA Jr, Baerman JM, de Buitleir M. The interplay between endogenous catecholamines and induced ventricular tachycardia during electrophysiologic testing. Am Heart J. 1987; 113: 227-233.
17. Huikuri HV, Zaman L, Castellanos A, Kessler KM, Cox M, Glicksman F, et al. Changes in spontaneous sinus node rate as an estimate of cardiac autonomic tone during stable and unstable ventricular tachycardia. J Am Coll Cardiol. 1989; 13: 646-652.
18. Landolina M, Mantica M, Pessano P, Manfredini R, Foresti A, Schwartz PJ, et al. Impaired baroreflex sensitivity is correlated with hemodynamic deterioration of sustained ventricular tachycardia. J Am Coll Cardiol. 1997; 29: 568-575.
19. James TN, Nadeau RA. Sinus bradycardia during injections directly into the sinus node artery. Am J Physiol. 1963; 204: 9-15.
20. James TN. Pulse and impulse formation in the sinus node. Henry Ford Hosp Med J. 1967; 15: 275-280.
21. Vieweg WV, Alpert JS, Hagan AD. Origin of the sinoatrial node and atrioventricular node arteries in right, mixed, and left inferior emphasis systems. Cathet Cardiovasc Diagn. 1975; 1: 361-373.
Pavri BB, Wong KL, Ho RT, Kocovic DZ (2014) Autonomic Modulation during Stable and Unstable Ventricular Tachycardia. J Cardiol Clin Res 2(4): 1039.
Cite this article