Embed Size (px)
DESCRIPTION
Now, with more than 15 years of fingernail testing under our belts, and a three year dataset with more than 10,000 samples, USDTL has the data to back up the claim: fingernail testing is a suitable alternative to hair testing. (“Hard Evidence”, page 4) The full dataset and results will be published in the September special issue of the Journal of Analytical Toxicology, but in this issue we have a preview of the positivity rates from that dataset. We think you’ll find them illuminating, and reason enough to trust fingernails as the new gold standard of drug and alcohol testing.
Citation preview

Substance
4New reporting of a large dataset of fingernail testing results.
8Fingernail testing as an alternative to hair specimens.
17Heroin use reaches a new high, nationally.
Clarity in Toxicology | v.6 i.2
Nailing theGold Standard
A wealth of new data brings
fingernail testing to the
forefront of toxicology.
Spring/Summer
2015

2 Spring/Summer 2015 Substance
Letter from the editor
TOXICOLOGY MOVES FORWARD
Once an alternative specimen for drug and alcohol testing, fingernails are quickly becoming the norm and the new gold standard.
The crux of drug testing is this: Trust. How much do you trust the results you get from your lab? How much do you trust the methodology being used to generate those results? It’s a tough call, and there are many factors to be weighed. One of the most important factors is which testing specimen to use.
In 1986, when President Ronald Reagan signed the Drug Free Federal Workplace law, instituting drug testing for over 20 million federal employees, urine testing was seen as the gold standard in this industry. Over the years, however, the limitations of urine testing - limited window of detection, ease of sample adulteration, lack of utility in child exposure testing - were often demonstrated by research. Alternatives were soon needed.
Hair testing was quickly discovered as a superior alternative to urine testing and remains a powerful tool in the drug and alcohol testing toolbox. Yet, hair has its limitations. Research has demonstrated conclusively that hair testing suffers from two separate testing biases. The retention of certain drugs and their metabolites in hair specimens varies greatly depending on the amount of pigment in the hair sample. For example, cocaine has been shown to accumulate at higher concentrations in darker pigmented hair than light hair. Other studies have shown that certain cosmetic treatments and hair bleaching can strip analytes out of hair samples. With these limitations, a certain level of mistrust crept in.
And then, along came fingernail testing. No pigment bias. Stable retention of drug and alcohol biomarkers. The longest window of detection for any drug testing specimen. Nails provided an alternative to hair testing that couldn’t be beat. It has taken quite some time, however, for the drug testing industry to accept nails as that alternative, with many professionals asking for “more data” to convince them.
Now, with more than 15 years of fingernail testing under our belts, and a three year dataset with more than 10,000 samples, USDTL has the data to back up the claim: fingernail testing is a suitable alternative to hair testing. (“Hard Evidence”, page 4)
The full dataset and results will be published in the September special issue of the Journal of Analytical Toxicology, but in this issue we have a preview of the positivity rates from that dataset. We think you’ll find them illuminating, and reason enough to trust fingernails as the new gold standard of drug and alcohol testing.
Thanks for reading,Michelle Lach, Editor-in-Chief
Correction: Some copies of the Winter 2015 issue of Substance contained an error on page 9, erroneously showing that the direct alchol biomarker EtS is detected in nail and hair samples. This is not the case. Only EtG is detected in nail and hair. We apologize for any confusion this may have caused.

3USDTL
SubstanceSpring/Summer 2015volume 6issue 2
Michelle Lach, MSIMCEditor-in-Chief
Joseph Salerno, MSManaging & Design Editor
Dru Wagner, MAGraphic Designer
Substance is a quarterly news magazine of toxicology science, data, and news. It is our mission to distil the technical world of toxicology, drug testing, and addiction science into plain words. If you have suggestions for topics you would like to know more about, let us know.
© 2015 USDTL, Inc. All Rights Reserved.
1700 S. Mount Prospect Rd.Des Plaines, IL, [email protected]
USDTL.com
Table of Contents
4
HARD EVIDENCE | Adam Negrusz, Ph.D., F-ABFT
Fingernail testing is often cited as an alternative specimen to hair. Now, three years and more than 10,000 data points later, fingernails are taking their place as the go-to specimen for long-term alcohol and drug testing.
8
Nailing Drug Testing | Joseph Salerno, MS
Fingernail testing has many similarities to hair testing, as well as some advantages including ease of collection, stability, and a longer window of detection.
16
RISING STAR
Irene Shu, Ph.D. DABCC, USDTL Assistant Laboratory Director awarded the 2015 Lemuel J. Bowie Young Investigator Award.
17
DATA IN ACTION
CESAR FAX: Percentage of National Treatment Admissions for Heroin at Highest Level; Admissions for Other Opiates May Be Leveling Off.
18
NATIONAL POSITIVITY RATES
Quarterly positivity results for drug and alcohol testing in fingernail and hair specimens.
Cover illustration by Joseph Salerno.

4 Spring/Summer 2015 Substance
HARD EVIDENCE
Fingernail testing is often cited as an alternative specimen to hair. Now, three years and more than 10,000 data points later, fingernails are taking their place as the go-to specimen for long-term alcohol and drug testing.
by Adam Negrusz, Ph.D., F-ABFT
During the last few decades both fingernails and toenails have become very useful specimens for the detection of drug use and abuse.1,2 Nails are made of a fibrous structural protein known as keratin. The average growth rate for fingernails is 3 mm per month2. Toenails grow 30-50% slower than fingernails and are much more susceptible to drug contamination from sweat.1,2 As the nail grows, chemicals (illicit substances, drugs, alcohol biomarkers, etc.) incorporate into the keratin fibers where they are trapped for long periods (3-5 months in fingernails, and 8-14 months in toenails).2
The mechanisms of drug incorporation in nails have not been extensively studied. In two recently published reports, the mechanisms of incorporation of the sleep aid zolpidem after a single oral dose were investigated.3,4 The results indicated three mechanisms of drug incorporation to nails:
1) Contamination from sweat, detectable 24 hours after drug use,
2) Incorporation from the nail bed (vertical growth), detected after 2 weeks, and
3) Incorporation from the germinal matrix (horizontal growth), where concentration is the highest approximately 3 months after drug administration. The studies showed that the concentration of zolpidem was higher in toenails than in fingernails, and the incorporation from sweat was not reversed by daily hygiene.3,4 An extensive review of the application of nail testing in
drug treatment programs, identification of in utero exposure to drugs, therapeutic drug monitoring, forensic toxicology - including postmortem applications and drug facilitated sexual assault - was recently published by Cappelle et al.1
Both hair and nails are keratinized specimens, however, there are a few differences between nails and hair that impact their usefulness in drug testing. Firstly, both fingernails and toenails grow continuously and do not have the growth cycle that is characteristic for hair.1,2 In addition, nails do not contain the color pigment melanin, and so are free of hair-color bias. Physicochemical properties of drugs can play an important role in drug accumulation in nails. Specifically, substances lacking a nitrogen atom may accumulate in nails at higher concentrations than in hair.1 For example, the concentrations of the direct alcohol biomarker ethyl glucuronide (EtG) and 11-nor-Δ9-tetrahydrocannabinol-9-carboxylic acid (THCA, the metabolite of tetrahydrocannabinol [THC], the psychoactive ingredient in marijuana) in nails are 3 times and 4.9 times higher, respectively, than in matching hair samples.5,6
Here at USDTL we have been offering alcohol and drug testing in fingernail and toenail specimens as an alternate to hair testing since 1999. We are excited to be one of the first labs to report the resulting positivity data for more than 10,000 nail specimens tested over a three year span.

USDTL 5USDTL
Collecting Fingernail DataA total of 10,349 nail samples were tested for
52 drugs, drug metabolites, and EtG. The samples were collected from high risk populations between January 1, 2012 and December 31, 2014. Sample sources included drug courts, child advocacy centers, drug treatment facilities, drunk driving programs, reference laboratories, physicians/health professionals’ programs, lawyers, and others. Approximately 3 mm clippings (about 100 mg) from all ten nails were submitted to the laboratory for each nail specimen. Samples were analyzed by validated analytical procedures.
We also examined differences in concentrations of drugs in fingernails and toenails. We started systematically recording the type of nail (fingernail vs. toenail) in May of 2014. Figure 3 (page 15) includes only results where the type of specimen was clearly indicated. As such, sample numbers as well as concentration ranges for the fingernail-toenail comparison may differ from those seen for the total data set.
One of the most fundamental principles of forensic toxicology is that in order to report any given specimen positive for a substance, at least two different analytical techniques have to be used on two separate aliquots from a specimen. In this study, the initial testing of nails was performed using either enzyme linked immunoassay (ELISA), or by liquid chromatography-tandem mass spectrometry (LC-MS-MS). Presumptive positive samples were then subjected to confirmatory testing for targeted analytes. LC-MS-MS was used for confirmatory analysis for the majority of drug classes, except for phencyclidine,
barbiturates, tramadol, and normeperidine. For the latter, gas chromatography-mass spectrometry (GC-MS) was employed. The presence of THCA in nails was confirmed by super sensitive GC-GC-MS-MS.
AmphetaminesA total of 7,799 samples were analyzed for
amphetamines (amphetamine, methamphetamine, MDMA, MDA, and MDEA; Figure 1); 14.4% of the samples were positive for amphetamine, and 13.7% were positive for methamphetamine. The samples we collected did not show obvious
AM
PHET
AM
INE
14.
4%
MET
HA
MPH
ETA
MIN
E 1
3.7%
MD
MA
0.3
%
MD
A 0
.09%
MD
EA 0
.05%
Figure 1. Amphetamine drug class positivity rates in fingernail specimens. 3 year dataset.

concentration differences between fingernails and toenails for amphetamine and methamphetamine (Figure 3), however, previous studies with more limited numbers of samples have shown higher concentrations of the compounds in toenails than in fingernails.1
There were only 22 samples found positive for MDMA (0.3%), 7 for MDA (0.09%), and 4 for MDEA (0.05%). The data set in our study was too limited to compare MDA, MDMA, and MDEA concentrations between fingernails and toenails. A previous study looking at ketamine in fingernail clippings was only able to discover it at the concentration of 0.314 ng/mg (below the limit of quantitation).7 In our study ketamine was found in 2 nail samples at concentrations of 3,772 and 12,632 pg/mg. Ketamine metabolite (norketamine) was found in one sample only at 201 pg/mg.
Cocaine7,787 total specimens were tested for cocaine and cocaine
metabolites. Cocaine, benzoylecgonine, norcocaine, and cocaethylene were found in 5.3%, 5.2%, 2.6%, and 1.2% of nail samples, respectively. (Figure 2) Cocaine was present in both fingernails and toenails in higher concentrations than benzoylecgonine, and higher concentrations of cocaine and benzoylecgonine were observed in fingernails than in toenails. (Figure 3) Previous studies have found higher concentrations of benzoylecgonine than cocaine in postmortem toenails from subjects of unspecified drug use history.8
Figure 2. Parent drug and metabolite positivity rates in fingernail specimens. 3 year dataset.
ETH
YL
GLU
CU
RON
IDE
(Et
G)
24.
9%
TH
CA
18.
1%
CO
CA
INE
5.3
%
BEN
ZO
YLE
CG
ON
INE
5.2
%
NO
RC
OC
AIN
E 2
.6%
CO
CA
ETH
YLE
NE
1.2
%
CO
DEI
NE
1.9
%
MO
RPH
INE
3.6
%
HY
DRO
MO
RPH
ON
E 2
.2%
HY
DRO
CO
DO
NE
11.4
%
6 Spring/Summer 2015 Substance

Opiates and OpioidsPositivity rates of selected opioids (morphine, codeine, 6-MAM [heroin
metabolite], hydrocodone, hydromorphone) in nail samples are presented in Figure 2. The most prevalent of the above five opioids was hydrocodone. It was detected in 11.4% of 7,779 tested nail samples, compared to 1.5-3.6% for the other four tested opioids. 6-MAM was present in 115 samples out of 7,779. (Editor’s note: This paragraph was edited on 8/26/2015 to correct a mistake.)
Other opioids including methadone, EDDP (methadone metabolite), oxycodone, and oxymorphone were found in 1.2%, 1.0%, 15.1%, and 2.6%, respectively, of approximately 3,400 samples analyzed. Methadone and EDDP were found in 44 and 35 samples, respectively, out of 3,567 submitted for analysis for these analytes (Figure 2).
Very limited information is available on the presence of other opioids (and opioid antagonists) such as buprenorphine, norbuprenorphine, naltrexone, naloxone, 6-ß-naltrexol, nalbuphine, or butorphanol in nails. Buprenorphine and norbuprenorphine were found in 15 and 12 nail samples, respectively, out of 40 samples submitted for buprenorphine analysis. We did not receive nail samples with a request for simultaneous testing for both buprenorphine/norbuprenorphine and naloxone. In fact, naloxone was not detected in any nail sample. On the other hand, naltrexone was found in only 2 nail samples (73 and 71 pg/mg), and 6-ß-naltrexol, naltrexone metabolite, was present in 9 out of 18 samples received. To our knowledge, this is the first
study reporting naltrexone (used in alcohol dependence treatment) and its metabolite tested in nails.
Marijuana TestingThe detection of THCA is very
important to differentiate between marijuana ingestion (intentional and/or passive inhalation) and external contamination.1
In our study the overall positivity rate for THCA was 18.1%. (Figure 1) Mean concentration in toenails were roughly the same as in fingernails (15 pg/mg and 13.2 pg/mg, respectively; Figure 3). The concentration ranges were also very similar suggesting that both specimens are equally useful in
Continued on page 14, Data
OX
YC
OD
ON
E 1
5.1%
OX
YM
OR
PHO
NE
2.6
%
6-M
AM
(H
ERO
IN M
ETA
BOLI
TE)
1.5
%
MET
HA
DO
NE
1.2
%
EDD
P (
MET
HA
DO
NE
MET
ABO
LIT
E) 1
.0%
7USDTL

8 Spring/Summer 2015 Substance
NAILING DRUG &
ALCOHOL TESTING
Fingernail testing has many similarities to hair testing, as well as some advantages including ease of collection, stability, and a longer window of detection.
by Joseph Salerno, MS
This article was originally published in DATIA Focus Magazine, Summer 2014, vol. 7, iss. 3.
Substance abuse in the 21st century is an ever-evolving and sophisticated animal. Through the Internet, new drugs—both illicit and prescription—are available in dizzying arrays. Along with the new drugs being abused are new methods to avoid detection. Labs must maintain constant research and development to meet the needs of the ever-changing market. Thankfully, the old adage ‘you are what you eat’ still rings true.
Hair testing has caught on as a popular sample to detect substances of abuse and so has the ability of the abuser to Google ways to offset drug tests. In an effort to remain ahead of the curve in this complex market, researchers have turned to other sample types to go beyond the limits of hair testing. Fingernails are composed of keratin, the same protein matrix found in hair. Fingernail testing has many similarities to hair testing, as well as some advantages including ease of collection, stability, and a longer window of detection. The detection of substances in fingernails provides a powerful tool for the drug and alcohol testing industry.
Incorporation of Drug and Alcohol Biomarkers in Nail Samples
Fingernail keratin is four times thicker than that
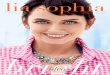
found in hair. While hair grows only in length from the hair root, nail keratin grows in two directions. From the germinal matrix, fingernails grow in length as they emerge from the nail root. As they elongate, fingernails also grow in thickness with new keratin being added to the underside of the fingernail along the nail bed (Figure 1, page 10).
It was previously thought that substances could only enter the fingernail from the germinal matrix, but research on therapeutic drug monitoring has debunked this model of drug capture.3,4 Blood vessels in the nail bed continuously feed the growing fingernail. As a result, drug and alcohol biomarkers are trapped in the keratin matrix over the entire fingernail as it grows in length.
Fingernails are a reservoir matrix made up of a tight weave of keratin fibers that are also porous. This tight but porous nature means that nails are a superb matrix for catching and trapping drug and alcohol biomarkers.5 Chronic drug or alcohol use causes a continuous build-up of biomarkers along the entire fingernail as it grows.
Detecting Drugs in FingernailsAmphetamine and methamphetamine were
the first illicit substances to be detected in nail samples in 1984.1 The role of nails in other uses like environmental exposure analysis, forensics, poison investigation, and others extends as far back as the

9USDTL
1800s.2 Much of what is known about the drugs in fingernails comes from drug therapy monitoring, most notably early studies into the antifungal treatment of toenails.3 Despite gaining acceptance as a tool for alcohol and substance abuse detection in recent decades, the body of evidence supporting fingernail testing spans nearly two centuries.
Drug and alcohol use can be detected in fingernail samples 1–2 weeks following use. In that time, the leading edge of the fingernail can grow out to a length that gives sufficient quantity for testing. The window of detection for drugs in fingernails is from three months up to six months after use, depending on several factors. The rate of fingernail growth can vary from person to person and can be affected by age (slower growth in older persons), disease state, and even weather (fingernails may grow slower in colder weather).3,6 Some drugs may wash out of fingernails as quickly as three months after use; yet, other drugs can have a much longer retention time. Despite this variability, research has shown that the window of detection for drug use in fingernails is at least equivalent to that of hair, and for many drugs the look-back is much longer than for hair.3
The same drugs that can be detected in hair samples can also be detected in fingernails. In some cases, fingernails may capture more of a drug than is typically found in hair samples. For example, a 2013 study found that fingernail samples positive for carboxy-THC (a marijuana metabolite) captured five times more of the biomarker than positive hair samples.7 Fingernails are able to remove the variation in results caused by hair pigment for some drugs. For instance, the same dose of amphetamine may give a 30-fold difference in the amount detected in blonde hair versus black hair. This is due to variation in test results for some drugs
caused by differences in hair pigment. Fingernail testing removes this variation. Research comparing fingernails and hair for other drugs has shown the two sample types to be equivalent, although the comparison has not been made for all potential substances of abuse. These various studies suggest that fingernail testing is a suitable, and in some cases superior, alternative to hair testing.
Fingernails are a reservoir matrix made up of a tight weave of keratin fibers that are also porous. This tight but porous nature means that nails are a superb matrix for catching and trapping drug and alcohol biomarkers.

GerminalMatrix
Free Edge
Nail Plate
Nail Bed
Nail Cross Section
Scalp
Hair Root
Hair Cross Section
As nail grows in thickness and length, biomarkers build up in the nail at the germinal matrix and
along the nail bed, collecting the full history of drug use.
100 microns
400 microns 100 microns
100 microns
100 microns
100 microns
Nail keratin is 4X thicker than hair.Nail often captures more of a biomarker than hair.
THC
THC
THCTHC
EtGEtG
EtG
Drug and alcohol biomarkers are trapped in the keratin fibers of the fingernail.Hair is also made of keratin fibers, but biomarkers may be washed out of hair by common cosmetic treatments, a problem that doesn’t exist when testing nails.
Direct Alcohol Biomarker testing is not available in toenail. Fingernail and toenail cannot be mixed.
Figure 1
The Benefits of Fingernail Testing
Non-intrusive, donor collected sample.
Minimal impact on the donor’s appearance.
We confirm all presumptive positives on state-of-the-art instruments.
Nail and hair samples capture the same drugs. 1:1
A 2-3 mm clipping, the width of a quarter, from each fingernail
Nails provide 3-6 months of drug and alcohol use history.
10 Spring/Summer 2015 Substance

GerminalMatrix
Free Edge
Nail Plate
Nail Bed
Nail Cross Section
Scalp
Hair Root
Hair Cross Section
As nail grows in thickness and length, biomarkers build up in the nail at the germinal matrix and
along the nail bed, collecting the full history of drug use.
100 microns
400 microns 100 microns
100 microns
100 microns
100 microns
Nail keratin is 4X thicker than hair.Nail often captures more of a biomarker than hair.
THC
THC
THCTHC
EtGEtG
EtG
Drug and alcohol biomarkers are trapped in the keratin fibers of the fingernail.Hair is also made of keratin fibers, but biomarkers may be washed out of hair by common cosmetic treatments, a problem that doesn’t exist when testing nails.
Direct Alcohol Biomarker testing is not available in toenail. Fingernail and toenail cannot be mixed.
Figure 1
The Benefits of Fingernail Testing
Non-intrusive, donor collected sample.
Minimal impact on the donor’s appearance.
We confirm all presumptive positives on state-of-the-art instruments.
Nail and hair samples capture the same drugs. 1:1
A 2-3 mm clipping, the width of a quarter, from each fingernail
Nails provide 3-6 months of drug and alcohol use history.
11USDTL

12 Spring/Summer 2015 Substance
If a donor’s fingernails are not of sufficient length, waiting 7–10 days will allow enough fingernail growth to give the ideal sample size. Because a donor’s drug and alcohol use impacts the entire length and width of the fingernail, this new growth will still capture a 3–6 month history
of drug use. In contrast, a three-month window of detection in hair can only be achieved if the donor already has at least 1.5 inches of hair on the head. Any new hair growth will not contain any history of previous drug or alcohol use.
Alcohol Testing in FingernailsAlcohol testing in fingernails, as in hair, is
done through the analysis of ethyl glucuronide (EtG), a direct alcohol biomarker. EtG is known as a direct biomarker, because it is only produced by the body when ethanol is present. This is in
contrast to indirect biomarkers such as aspartate aminotransferase (AST), gamma glutamyl transferase (GGT), or carbohydrate deficient transferrin (CDT), among others. Indirect markers measure the effects of ethanol consumption on the health of the body. Other conditions may confound
indirect biomarkers, such as age or certain diseases. Ethanol is converted to EtG in the liver and then deposited in fingernails primarily from the nail bed capillaries.
The use of fingernail samples for EtG testing may be a preferred sample type over hair for two reasons. First, EtG accumulates at higher concentrations in fingernail samples. EtG testing in fingernails eliminates a possible bias seen in hair EtG testing as well. A 2012 study compared EtG levels in paired fingernail and hair samples taken from 606 college students. EtG levels in positive fingernail samples were 2.5 times higher than those detected in positive hair samples.8
The college student data also suggested a possible bias for EtG testing in hair samples; fingernail
and hair samples taken from male subjects showed strong agreement in their positivity rate. However, there was very little agreement between the two sample types for female subjects. Earlier research from 2010 demonstrated that EtG in hair could be broken down as a result of some cosmetic hair treatments, such as hair bleaching and dyeing, which may account for the difference between the two sample groups9 (Figure 2 and 3).
Sample CollectionFingernail testing offers several
advantages in sample collection. Fingernail samples are clipped from the leading edge of the growing nail and are the least intrusive of any testing sample. Fingernails
can be collected by the donor themselves
Fingernails offer a drug and alcohol testing sample that is a useful, and in many ways superior alternative to hair testing.
The rate of growth of fingernails, coupled with the stability of drugs in the nail keratin matrix, provides the longest
window of detection of any drug testing sample.
Figure 2. Comparison of results of EtG testing in male hair and nails.

13USDTL
in front of a trained observer, as opposed to hair samples which need to be taken by a trained collector. Additionally, the collection of fingernails has very low impact on the personal appearance of the donor, which is not always true when hair samples are collected. Fingernails are almost universally available, which may not be true for donors experiencing hair loss and thinning.
An ideal sample size for screening and confirmation of positive results is 100 mg of fingernails. A 2–3 mm clipping—about the width of the edge of a U.S. Quarter— from all ten fingernails will give the optimal sample size.
ConclusionSubstance abuse in the 21st century is
complicated. Detection methods must be open to alternative samples to keep up. Fingernails offer a drug and alcohol testing sample that is a useful, and in many ways superior alternative to hair testing. The rate of growth of fingernails, coupled with the stability of drugs in the nail keratin matrix, provides the longest window of detection of any drug testing sample. Because they grow in both length and thickness, fingernails preserve their window of detection in a greater surface area, and allow for greatest accessibility to drug and alcohol use history. Well-researched and long-used for various forensic applications, fingernails are a powerful tool to be included in the drug and alcohol testing professional’s toolbox.
References1. Suzuki, O., Hattori, H., & Asano, M. (1984). Nails
as useful materials for detection of methamphetamine
or amphetamine abuse. Forensic Science International, 24,
9-16.
2. Lander, H., Hodge, P.R., & Crisp, C.S. (1965).
Arsenic in the hair and nails. Its significance in acute
arsenical poisoning. Journal of Forensic Medicine, 12, 52-67.
3. Palmeri, A., Pichini, S., Pacifici, R., Zuccaro, P.,
& Lopez, A. (2000). Drugs in nails: Physiology,
pharmacokinetics, and forensic toxicology. Clinical
Pharmacokinetics, 38, 95-110.
4. Shuster, S., & Munro, C.S. (1992). Single dose
treatment of fungal nail disease [letter]. Lancet, 339,
1066.
5. Walters, K.A., & Flynn, G.L. (1983). Permeability
characteristics of the human nail plate. International
Journal of Cosmetic Science, 5, 231-246.
6. Bean, W.B. (1953). A note on fingernail growth.
Journal of Investigative Dermatology, 20, 27-31.
7. Jones, J., Jones, M., Plate, C., & Lewis, D. (2013).
The Detection of THCA using 2-dimensional gas
chromatographytandem mass spectrometry in human
fingernail clippings: method validation and comparison
with head hair. American Journal of Analytical Chemistry,
4, 1-8.
8. Jones, J., Jones, M., Plate, C., Lewis, D., Fendrich,
M., Berger, L., & Fuhrmann, D. (20120). Liquid
chromatographytandem mass spectrometry assay
to detect ethyl glucuronide in human fingernail:
comparison to hair and gender differences. American
Journal of Analytical Chemistry, 3, 83-91.
9. Morini, L., Zucchella, A., Polettini, A., Lucia, P.,
& Groppi, A. (2010). Effect of bleaching on ethyl
glucuronide in hair: An in vitro experiment. Forensic
Science International, 198, 23-27.
Figure 3. Comparison of results of EtG testing in female hair and nails.

Data, continued from page 7.
revealing cannabis use. Comparing matched hair and nail specimens Jones et al.5 developed a highly sensitive GC-GC-MS-MS method for the quantification of THCA in keratinized specimens with the limit of detection and quantification of 10 and 20 fg/mg, respectively. The mean THCA concentration in nails was 1.8 pg/mg in Jones et al., lower that the mean concentration in this study (13.7 pg/mg). 7,797 nail samples were analyzed for THCA concentrations in our study.
Alcohol UseOut of 3,039 samples submitted for EtG analysis,
24.9% were positive, with a concentration range from 20-3,754 pg/mg (median 88, mean 177; Figure 2).
In another study by Jones et al.,6 the reported EtG mean concentration was 29.1 pg/mg, and it was 3 times higher than in corresponding hair samples of college students (age 18-26 years). The mean concentration was significantly lower than in this report where subjects expressed risky alcohol drinking behavior. Morini et al.9 found a correlation between EtG concentration in fingernails and self-reported alcohol consumption. The highest EtG concentration was 92.6 pg/mg for a person consuming >60 g of alcohol per day. In a
separate study, Berger et al.10 also found that EtG in fingernails at 30 pg/mg has 100% sensitivity to identify high-risk drinking behavior (≥30 standard drinks per week), and 100% specificity to rule out abstinence, compared to hair EtG at 30 pg/mg. In both studies, the highest EtG concentration in fingernails was 397.08 pg/mg. Both studies concluded that the detection of EtG in nails is a better alcohol use biomarker than in hair.
Other DrugsExamples of other drugs and metabolites found
in nails include barbiturates, benzodiazepines, normeperidine, phencyclidine, tramadol, and norpropoxyphene. The positivity rate for benzodiazepines in nails was below 1%, except for alprazolam which showed a positivity rate of 1.6%.
SummaryIn summary, this data demonstrates nails are
a very useful matrix for the detection of drugs and illicit substances, and may be a superior alternative specimen type to hair samples. Nail sample preparation is relatively simple and the advancement in analytical instrument technology allows for accurate measurements of extremely low quantities (femtograms) of parent compounds as well as their metabolites. Most parent drugs are present at greater concentrations than their metabolites. Naltrexone is an exceptional case where its metabolite, 6-ß-naltrexone, is the predominant form present in nails. It is worth pointing out that the concentrations of substances found antemortem in our study are largely comparable with concentrations reported in postmortem cases, whether or not the causes or manners of death were drug-related. More research is necessary to better understand and interpret these analytical findings.
References1. Cappelle, D., Yegles, M.,
Neels, H., van Nuijs, A.L.N.,
De Doncker, M., Maudens, K.,
Covaci, A., Crunelle, C.L. (2015)
Nail analysis for the detection
of drugs of abuse and pharmaceuticals: a review. Forensic
Toxicology, 33, 12-36.
2. Baumgartner, M.R. (2014) Nails: an adequate
alternative matrix in forensic toxicology for drug analysis?
Bioanalysis, 6, 2189-2191.
3. Hang, C., Ping, X., Min, S. (2013) Long-term follow-
up analysis of zolpidem in fingernails after a single
oral dose. Analytical and Bioanalytical Chemistry, 405,
7281-7289.
One of the most fundamental principles of forensic toxicology is that in order to report any given specimen positive for a substance, at least two different analytical techniques have to be used on two separate aliquots...
14 Spring/Summer 2015 Substance

4. Madry, M.M., Steuer, A.E., Binz, T.M., Baumgartner,
M.R., Kreamer, T. (2014) Systematic investigation of the
incorporation mechanism of zolpidem in fingernails.
Drug Testing and Analysis, 6, 533-541.
5. Jones, J., Jones, M., Plate, C., Lewis, D. (2013)
The detection of THCA using 2-dimensional gas
chromatography-tandem mass spectrometry in human
fingernail clippings: method validation and comparison
with head hair. American Journal of Analytical Chemistry,
4, 1-8.
6. Jones, J., Jones, M., Plate, C., Lewis, D., Fendrich, M.,
Berger, L., Fuhrmann, D. (2012) Liquid chromatography-
tandem mass spectrometry assay to detect ethyl
glucuronide in human fingernail: comparison to hair
and gender differences. American Journal of Analytical
Chemistry, 3, 83-91.
7. Cirimele, V., Kintz, P., Mangin, P. (1995) Detection
of amphetamines in fingernails: an alternative to hair
analysis. Archives of Toxicology, 70, 68-69.
8. Engelhart, D.A., Lavins, E.S., Sutheimer, C.A. (1998)
Detection of drugs of abuse in nails. Journal of Analytical
Toxicology, 22, 314-318.
9. Morini, L., Calucci, M., Ruberto M.G., Groppi, A.
(2012) Determination of ethyl glucuronide in nails by
liquid chromatography tandem mass spectrometry as a
potential new biomarker for chronic alcohol abuse and
binge drinking behavior. Analytical and Bioanalytical
Chemistry, 402, 1865-1870.
10. Berger, L., Fendrich, M., Jones, J., Fuhrmann, D.,
Plate, C., Lewis, D. (2014) Ethyl glucuronide in hair and
fingernails as a long-term alcohol biomarker. Addiction,
109, 425-431.
Figure 3. Comparison of fingernail and toenail results.
AmphetamineMethamphetamine
MDMACocaine
BenzoylecgonineNorcocaine
Cocaethylene6-MAMCodeineMorphine
HydromorphoneHydrocodoneOxycodone
OxymorphoneMethadone
EDDPBuprenorphine
NorbuprenorphineCarboxy-THC
AlprazolamDiazepam
NordiazepamEthyl Glucuronide
13.7%12.3%0.3%5.5%5.3%2.5%1.4%1.9%2.0%3.7%2.7%8.7%
17.7%4.1%1.0%1.0%
35.7%28.6%16.6%2.6%1.0%1.1%
24.2%
18.0%13.3%0.2%2.9%2.9%0.5%0.4%1.1%2.0%2.7%2.2%8.0%13.6%2.3%0.4%0.4%33.3%33.3%20.0%0.7%0.7%0.7%24.2%
FINGERNAILS ANALYTES TOENAILS
15USDTL

Dr. Irene Shu, Assistant Laboratory Director for USDTL, was selected as the 2015 winner of the Lemuel J. Bowie Young Investigator Award by the Chicago Section of the American Association of Clinical Chemistry (AACC).
Irene Shu, Ph.D., DABCC, joined USDTL, Inc. in 2013 and received her Bachelor of Science degree in Chemistry with a minor in Life Science from National Tsing-Hua University in Hsinchu,
Taiwan in 2006. She then received her Ph.D. degree in Chemistry from University of Washington in Seattle, WA in 2011. She pursued Clinical Chemistry Post-doctoral Fellowship training program in Houston, TX at Houston Methodist Hospital accredited by the Commission on Accreditation in Clinical Chemistry (COMACC).
During the Clinical Chemistry training program in 2011-2013, she evaluated a wide range of clinical
assays, particularly focusing on toxicology testing. She developed and validated the first LC-MSMS assays to expand the clinical toxicology service of the laboratory, and generated a track record of peer-reviewed journal articles and abstracts presented at scientific conferences. She received American Board of Clinical Chemistry certificates in clinical chemistry in 2013 and in toxicological chemistry in 2014.
“The Chicago Section’s Young Investigator Award is named in honor of Lemuel J. Bowie, Ph.D. Dr. Bowie was a long time active member of AACC and the Chicago Section. He served many positions within the Chicago section including Chair and went on to actively participate in AACC at a national and international level culminating in his election as President of AACC in 1993.”1 Dr. Bowie passed away in 1998, in Evanston, IL, and is survived by his wife Cheryl, and their children Kwame and Shani.
References1. Retrieved from: https://www.aacc.org/
community/local-sections/chicago/awards/lemuel-bowie-young.
RISING STAR
Dr. Irene Shu, Ph.D. DABCC, awarded the 2015 Lemuel J. Bowie Young Investigator Award.
Dr. Irene Shu (left) receives the Lemuel J. Bowie Young Investigator’s Award from Cheryl Bowie (right), widow of Dr. Bowie.
16 Spring/Summer 2015 Substance

DATA IN ACTION
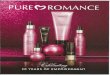
CESAR FAX: Percentage of National Treatment Admissions for Heroin at Highest Level; Admissions for Other Opiates May Be Leveling Off.
The percentage of admissions to state-funded substance abuse treatment facilities citing heroin as a primary substance of abuse has reached the highest level since data collection began in 1992, according to data from the national Treatment Episode Data Set (TEDS). After six years of stability, heroin admissions increased from 14%
in 2010 to 16% in 2012 (the most recent year for which data are available). In contrast, admissions for the primary abuse of other opiates*, which had increased steadily since the late 1990s, remained at around 10% in 2011 (10.1%) and 2012 (9.7%). Cocaine admissions continued to decline, reaching a new low of 7% in 2012 (data not shown).
NOTES: TEDS data are of admissions to treatment ages 12 and older for abuse of alcohol and/or drugs in facilities that report to State administrative data systems. Data include records for admissions that were received and processed through 10/17/13.TEDS admissions do not represent individuals; an individual admitted to treatment twice within a calendar year would be counted as two admissions. Admissions can report up to three substances of abuse that led to the treatment episode.
*The category Other Opiates includes non-prescription methadone, buprenorphine, codeine, hydrocodone, hydromorphone, meperidine, morphine, opium, oxycodone, pentazocine, propoxyphene, tramadol, and any other drug with morphine-like effects.
†While the focus of this analysis is on treatment admissions for drugs other than alcohol, it should be noted that alcohol remains the most frequently mentioned primary substance of abuse—despite the fact that the percentage of admissions for alcohol decreased from 59% in 1992 to 39% in 2012.
SOURCE: Adapted by CESAR from the Center for Behavioral Health Statistics and Quality, SAMHSA, Treatment Episode Data Set (TEDS): 2002-2012. National Admissions to Substance Abuse Treatment Services, 2014. Available online at http://www.samhsa.gov/data/client-level-data-teds/reports?tab=18.
Percentage of All
Admissions
Primary Substance of Abuse (Other Than Alcohol†) at Admission to U.S. State Licensed or Certified Substance Abuse Treatment Facilities, Ages 12 and
Older, 1992 to 2012
0%
1992 1996 2000 2004 2008 2012
4%
8%
12%
16%
20%
Heroin
Other Opiates
17USDTL

USDTL NATIONAL POSITIVITY RATES*
Fingernail Specimens Amphetamines | 16.6%
Cocaine | 5.8%
Opiates | 9.7%
Cannabinoids | 19.3%
Benzodiazepines | 3.1%
Oxycodone | 4.8%
Tramadol | 4.4%
Fentanyl | 0.0%
Buprenorphine | 34.8%
Ketamine | 0.0%
Ethyl Glucuronide | 19.4%
Barbiturates | 0.0%
Methadone | 1.7%
10 02040
Not shown: Meperidine 0.0%, Phencyclidine 0.2%, Propoxyphene 0.0%
18 Spring/Summer 2015 Substance

Ketamine | 0.0%
Quarterly report date range: January 1, 2015 – March 31, 2015* These data report national positivity rates for forensic toxicology tests conducted by USDTL on behalf of external clients and are not reflective of systematic research results.
Hair SpecimensAmphetamines | 14.9%
Cocaine | 6.9%
Opiates | 14.8%
Cannabinoids | 10.4%
Oxycodone | 11.1%
Tramadol | 4.3%
Fentanyl | 0.6%
Buprenorphine | 47.8%
Ketamine | 4.8%
Barbiturates | 0.5%
Methadone | 2.4%
20 50100
Not shown: Meperidine 0.2%, Phencyclidine 0.1%, Propoxyphene 0.1%
Benzodiazepines | 2.4%
Ethyl Glucuronide | 16.8%
19USDTL

EVENTS & EXHIBITS
• August 25-27 – The 38th National Child Welfare, Juvenile, and Family Law Conference – Monterey, CA
• September 23-26 – Substance Abuse Program Administrators Association 2015 Annual Conference – Houston, TX
• October 8-9 – Illinois Association of Problem-Solving Courts 2015 Conference – Springfield, IL
• October 9-13 – The Association for Addiction Professionals Annual Conference – Washington, DC
• October 21-24 – California Society of Addiction Medicine Synapse to Society: Addiction Medicine State of the Art 2015 – San Francisco, CA
• October 31 - November 4 – American Public Health Association Annual Meeting – Chicago, IL
1700 S. Mount Prospect Rd. | Des Plaines, IL 60018 | 800.235.2367 | www.USDTL.com
United States Drug Testing Laboratories, Inc.1700 S. Mount Prospect Road|Des Plaines, IL|60018Main: 847.375.0770|www.USDTL.com|Fax: 847.375.0775
®
Like what we have to share? Follow us
for more!
®
20 Spring/Summer 2015 Substance