Embed Size (px)
Citation preview

Successful prevention of syphilis infection with azithromycin in both
HIV-negative and HIV-positive individuals, San Francisco, 1999-2003.
J. D. Klausner,1,2 K. Steiner,1 R. Kohn1
1San Francisco Dept Public Health, San Francisco, CA 2University of California, San Francisco, San Francisco, CA.

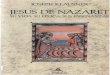
Background: Syphilis trends in San Francisco
EARLY LATENTPRIMARY & SECONDARY
Rep
orte
d ca
ses
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
2,200
19
55
19
56
19
57
19
58
19
59
19
60
19
61
19
62
19
63
19
64
19
65
19
66
19
67
19
68
19
69
19
70
19
71
19
72
19
73
19
74
19
75
19
76
19
77
19
78
19
79
19
80
19
81
19
82
19
83
19
84
19
85
19
86
19
87
19
88
19
89
19
90
19
91
19
92
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02

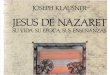
Background: Current syphilis epidemic in San Francisco
0
20
40
60
80
100
120
140
160
180
1999
Q1
1999
Q2
1999
Q3
1999
Q4
2000
Q1
2000
Q2
2000
Q3
2000
Q4
2001
Q1
2001
Q2
2001
Q3
2001
Q4
2002
Q1
2002
Q2
2002
Q3
2002
Q4
2003
Q1
2003
Q2
2003
Q3
2003
Q4
Quarter
Cases
GAY/BI MALE + TG
MALE UNK
HETERO MALE
FEMALE

Background:Previous studies on azithromycin and syphilis
• Hook EW, Stephens J, Ennis DM, Ann Intern Med, 1999– randomized trial of 1 gram azithromycin vs. 2.4 mu
benzathine penicillin for incubating disease– no reactive FTA-ABS at 3 months in either group
• Hook EW et al., Sex Trans Dis, 2001– RCT of azithromycin vs. benzathine penicillin for
syphilis cases– 2 grams of azithromycin as effective as benzathine
penicillin for treating disease

Background:Syphilis treatment in San Francisco
• Contacts: new cases versus “epi treatment”– 2.4 mu benzathine penicillin G I.M. (“bicillin”) – 100 mg doxycycline P.O. BID for 14 days– 1 gram azithromycin P.O.
• Field-delivered therapy with Azithromycin began March, 1999

Objective
• Compare observed success in treating incubating syphilis using azithromycin to success with other treatments in order to justify continued use of azithromycin

Methods:San Francisco STD Registry
• STD clinic medical record data
• Reported morbidity and reactive STS
• Interview data and field activity
• Screening data

Methods: Sample
• Data from 1999 through 2003
• Non-reactive RPR or VDRL with any syphilis treatment (n=3812)
• Follow-up titer between 30 and 90 days after initial titer (n=151)

Methods: Measurements
• Outcome: any reactive titer defines treatment failure
• Biological false positives excluded from analysis
• HIV status measured from multiple sources, including self-reported status

Results:All patients
confidence limitsTreated Failures Percent lower upper
TreatmentArithromycin 1G 0.5% 6.8%Doxycycline 5 0 0.0% 0.0% 52.2%Bicillin 18 1 5.6% 0.1% 27.3%(Multiple) 2 0 0.0% 0.0% 84.2%All 151 4 2.6% 0.7% 6.6%
Treatment outcome
126 3 2.4%

Results: By HIV Status
Treated Failures Percent Treated Failures PercentTreatmentArithromycin 1GDoxycycline 4 0 0.0% none none noneBicillin 11 1 9.1% 6 0 0.0%(Multiple) 2 0 0.0% none none noneAll 103 3 2.9% 22 0 0.0%
HIV-negative HIV-positive
0 0.0%86 2 2.3% 16

Conclusions
• Failure rate for azithromycin was not significantly greater than rate for bicillin
• Since no resistance to bicillin has been documented, apparent treatment failures likely indicate re-exposure
• Success in treatment did not vary between HIV-negative and HIV-positive clients

Limitations
• No way to distinguish treatment failure from re-exposure
• Not all exposed will develop disease• No randomization
– penicillin allergies– field versus clinic
• Small number of follow-up titers• Wide confidence limits for negative results

Limitations
• No power to assess temporal trends– Azithromycin epi-treatment failures:
• November 2002
• April 2003
• July 2003
– Bicillin epi-treatment failure:• April 1999

Further research
• Another randomized trial of azithromycin vs. bicillin– HIV-positive clients only– San Francisco & Los Angeles– Five years later than 1999 study by Hook

Thank you ...