Embed Size (px)
Citation preview

FEAT
UR
EA
RT
ICLES
CASE REPORTS
Successful TransapicalImplantation of an Edwards SapienValve Within an Insufficient AorticCoreValve Prosthesis: An InitialExperienceSimone Schleger, MD,* Markus Kasel, MD,*Jayshree Vogel, MS, Michael Lieber, MD,Dietmar Antoni, MD, Ellen Hoffmann, MD, PhD, andWalter B. Eichinger, MD, PhD
Department of Cardiac Surgery, Hospital Bogenhausen;Department of Cardiology, Hospital Bogenhausen; and Departmentof Cardiology, German Heart Center Munich, Munich, Germany
Transcatheter aortic valve implantation (TAVI) has be-come an emerging alternative for high-risk patients withaortic stenosis unsuitable for surgical intervention. Wereport the case of a 26-mm Edwards Sapien valve (Ed-wards Lifesciences, Irvine, CA) implanted into an insuf-ficient 29-mm CoreValve prosthesis (Medtronic Inc, Min-neapolis, MN) 1 year after implantation using thetransapical approach in a 59-year-old man. Transesopha-geal echocardiography showed severe paravalvular re-gurgitation and computed tomography revealed the Cor-eValve to be located slightly below the aortic annuluswith evidence of underdeployment. The balloon-expand-able Sapien system caused a better expansion of theunderdeployed CoreValve and the pericardial skirt ade-quately covered the leakage. The paravalvular regurgita-tion disappeared and the patient recovered.
(Ann Thorac Surg 2013;95:1070–2)© 2013 by The Society of Thoracic Surgeons
Paravalvular regurgitation is 1 of the major complica-tions of transcatheter aortic valve implantation
(TAVI) [1] and occurs or might occur when (1) the valveis misplaced and implanted either below or above theaortic annulus, leading to incomplete coverage bythe prosthetic skirt [2]; (2) the valve, although placed inthe correct position at first, migrates toward the ventricleover time [3]; or (3) the radial force of the self-expandingCoreValve prosthesis (Medtronic, Inc, Minneapolis, MN)is not strong enough to dilate a heavily calcified nativeaortic valve, and the stiffness of the calcific nature of thenative valve leads to deformation of the round geometryof the CoreValve frame [4].
Previous cases of aortic insufficiency have been treatedwith CoreValve-in-CoreValve as well as Edwards Sa-pien–in-CoreValve implantations [5–7]. In all of thesecases, the valve-in-valve implantation took place eitherimmediately or within a few days after the first procedurethrough the transfemoral approach.
Accepted for publication June 8, 2012.
*Drs Schleger and Kasel shared first authorship.
Address correspondence to Dr Schleger, Klinikum Bogenhausen,
Englschalkingerstrasse 77, 81925 Munich, Germany; e-mail: [email protected].© 2013 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
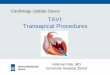
A 59-year-old male patient was rehospitalized with con-gestive heart failure due to severe aortic insufficiency.One year previously, critical aortic valve stenosis wastreated with a transfemoral 29-mm CoreValve biopros-thesis (CoreValve, Inc, Irvine, CA) because of his severecomorbidities and a previous cardiac bypass operation. Apercutaneous procedure was chosen because the periop-erative risk was regarded as significantly increased, witha calculated logistic EuroSCORE of 24% and a Society ofThoracic Surgeons risk score of 13%. After the transfemo-ral implantation procedure, the mean aortic valve pres-sure gradient decreased from 34 to 8 mm Hg and thepatient’s clinical symptoms improved at first. However,aortic insufficiency (II) remained, presumably resultingfrom either deep implantation or migration of theCoreValve over time, or both, and the patient was read-mitted to the hospital several times within the first yearafter implantation. Intentions to control his clinicalsymptoms with medications showed no benefit. He wassuffering from dyspnea and had congestive heart failure(New York Heart Association class IV). Transesophagealechocardiography revealed severe regurgitation of theCoreValve prosthesis (Fig 1), a normal aortic valve meangradient (11 mm Hg), a moderately reduced left ventric-ular ejection fraction of 40%, as well as secondary pul-monary hypertension.
Computed tomography (CT) showed the CoreValveprosthesis to be located slightly below the aortic annuluswith evidence of underdeployment, thus creating severeaortic insufficiency (III) (Fig 2).
Because of the patient’s history and ingrowths of theCoreValve, surgical treatment was denied and a sec-ond TAVI procedure was considered. Computed to-mography was performed to evaluate the diameter ofthe previously implanted CoreValve and showed aninner waist diameter of 24 mm and an annulus diam-eter of 21.5 mm � 25 mm (Fig 2 inset). Signs of valveunderdeployment could be identified, with the Cor-eValve being fairly oval instead of round. Because of ashorter access route and more precise valve placement,as well as a lesser amount of contrast medium requiredand taking into consideration the patient’s renal fail-ure, the transapical approach was chosen as themethod of implantation. It offers optimal control inplacing the second prosthesis in the exact positioncoming from below the CoreValve prosthesis withouthaving to pass the abdominal aorta as well as the aorticarch, thus making the whole procedure more manage-able than with the transfemoral approach. Accordingto the obtained measurements, a 26-mm EdwardsSapien valve was chosen, aiming to cover the annuluswith the Edwards Sapien skirt to achieve better valvedeployment. The risk of underdeployment in an Ed-wards Sapien valve is minimal compared with that in aCoreValve prosthesis because of the balloon-
Drs Schleger and Kasel disclose that they have finan-cial relationships with Edwards Lifesciences.
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2012.06.029
1071Ann Thorac Surg CASE REPORT SCHLEGER ET AL2013;95:1070–2 TRANSAPICAL IMPLANTATION OF EDWARDS SAPIEN VALVE
FEA
TU
RE
AR
TIC
LES
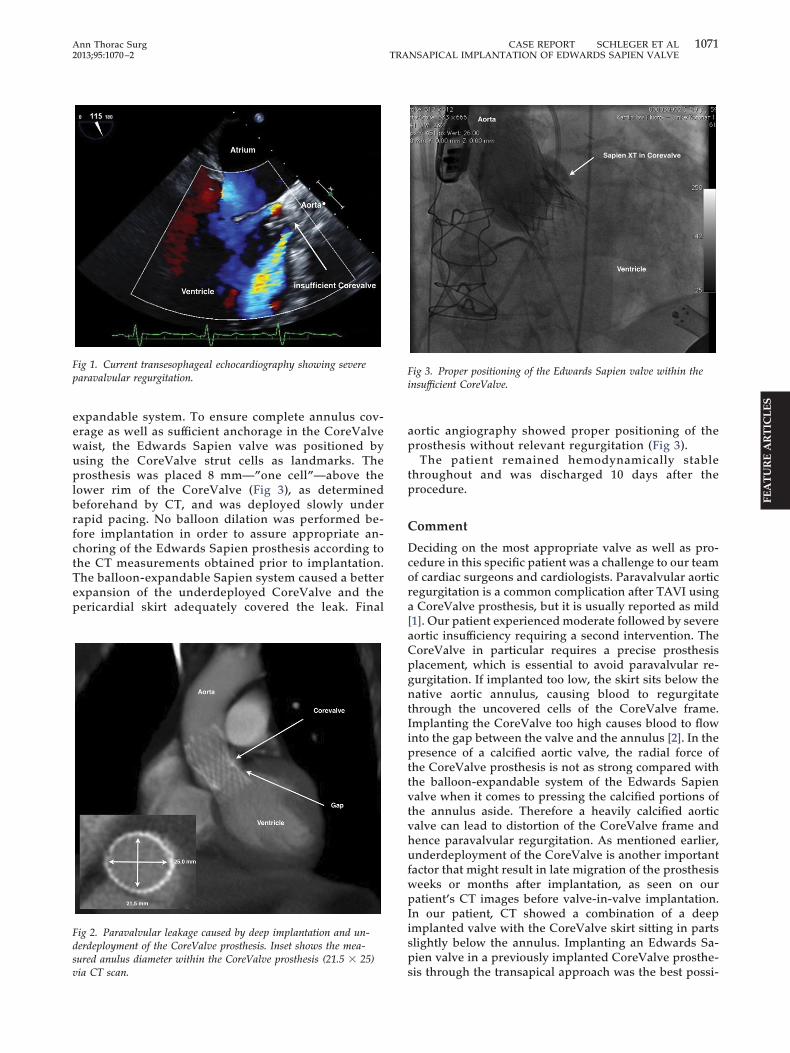
expandable system. To ensure complete annulus cov-erage as well as sufficient anchorage in the CoreValvewaist, the Edwards Sapien valve was positioned byusing the CoreValve strut cells as landmarks. Theprosthesis was placed 8 mm—”one cell”—above thelower rim of the CoreValve (Fig 3), as determinedbeforehand by CT, and was deployed slowly underrapid pacing. No balloon dilation was performed be-fore implantation in order to assure appropriate an-choring of the Edwards Sapien prosthesis according tothe CT measurements obtained prior to implantation.The balloon-expandable Sapien system caused a betterexpansion of the underdeployed CoreValve and thepericardial skirt adequately covered the leak. Final
Fig 1. Current transesophageal echocardiography showing severeparavalvular regurgitation.
Fig 2. Paravalvular leakage caused by deep implantation and un-derdeployment of the CoreValve prosthesis. Inset shows the mea-sured anulus diameter within the CoreValve prosthesis (21.5 � 25)
via CT scan.aortic angiography showed proper positioning of theprosthesis without relevant regurgitation (Fig 3).
The patient remained hemodynamically stablethroughout and was discharged 10 days after theprocedure.
Comment
Deciding on the most appropriate valve as well as pro-cedure in this specific patient was a challenge to our teamof cardiac surgeons and cardiologists. Paravalvular aorticregurgitation is a common complication after TAVI usinga CoreValve prosthesis, but it is usually reported as mild[1]. Our patient experienced moderate followed by severeaortic insufficiency requiring a second intervention. TheCoreValve in particular requires a precise prosthesisplacement, which is essential to avoid paravalvular re-gurgitation. If implanted too low, the skirt sits below thenative aortic annulus, causing blood to regurgitatethrough the uncovered cells of the CoreValve frame.Implanting the CoreValve too high causes blood to flowinto the gap between the valve and the annulus [2]. In thepresence of a calcified aortic valve, the radial force ofthe CoreValve prosthesis is not as strong compared withthe balloon-expandable system of the Edwards Sapienvalve when it comes to pressing the calcified portions ofthe annulus aside. Therefore a heavily calcified aorticvalve can lead to distortion of the CoreValve frame andhence paravalvular regurgitation. As mentioned earlier,underdeployment of the CoreValve is another importantfactor that might result in late migration of the prosthesisweeks or months after implantation, as seen on ourpatient’s CT images before valve-in-valve implantation.In our patient, CT showed a combination of a deepimplanted valve with the CoreValve skirt sitting in partsslightly below the annulus. Implanting an Edwards Sa-pien valve in a previously implanted CoreValve prosthe-
Fig 3. Proper positioning of the Edwards Sapien valve within theinsufficient CoreValve.
sis through the transapical approach was the best possi-

1072 CASE REPORT KIMURA ET AL Ann Thorac SurgRESECTION OF GIANT INTERVENTRICULAR FIBROMA 2013;95:1072–4
FEAT
UR
EA
RT
ICLES
ble treatment option for our patient, who had highsurgical risk because of various comorbidities. It is afeasible procedure and can rather easily be done as abailout procedure in patients with severe aortic regurgi-tation unsuitable for surgical intervention.
References
1. Sherif MA, Abdel-Wahab M, Stöcker B, et al. Anatomic andprocedural predictors of paravalvular aortic regurgitationafter implantation of the Medtronic CoreValve bioprosthesis.J Am Coll Cardiol 2010;56:1623–29.
2. Jilaihawi H, Chin D, Spyt T, et al. Prosthesis-patient mismatch aftertranscatheter aortic valve implantation with the Medtronic Cor-eValve bioprosthesis. Eur Heart J 2010;31:857–64.
3. Pang PY, Chiam PT, Chua YL, Sin YK. A survivor of lateprosthesis migration and rotation following percutaneoustranscatheter aortic valve implantation. Eur J CardiothoracSurg 2012;41:1195–6. Epub 2012 Jan 6.
4. Grube E, Schuler G, Buellesfeld L, et al. Percutaneous aorticvalve replacement for severe aortic stenosis in high-riskpatients using the second- and current third-generation self-expanding CoreValve prosthesis: device success and 30-dayclinical outcome. J Am Coll Cardiol 2007;50:69–76.
5. Taramasso M, Sharp A, Maisano F. First-in-man case reportof the Use of an Edwards-Sapien Valve to treat a regurgitantCoreValve aortic valve prosthesis. Catheter Cardiovasc Interv2010;75:51–5.
6. Ussia GP, Mulè M, Tamburino C. The valve-in-valve tech-nique: transcatheter treatment of aortic bioprosthesis malpo-sition. Catheter Cardiovasc Interv 2009,73:713–6.
7. Piazza N, Schultz C, de Jaequre PP, Serruys PW. Implantation oftwo self-expanding aortic bioprosthetic valves during the sameprocedures—insights into valve-in-valve implantation (‘Russiandoll concept’). Catheter Cardiovasc Interv 2009;73:530–9.
Successful Surgical Removal of aGiant Interventricular Fibroma:Surgical Approach WithoutVentriculotomyNaritaka Kimura, MD, Muneaki Matsubara, MD,Naotaka Atsumi, MD, and Masatsugu Terada, MD
Department of Cardiovascular Surgery, Tokyo MetropolitanChildren’s Medical Center, Tokyo, Japan
A 14-month-old boy was transported to our hospital byambulance because of cardiopulmonary arrest after thesudden onset of convulsions. He was resuscitated andtransthoracic echocardiography showed a giant inter-ventricular tumor. The cause of this episode wasthought to be ventricular arrhythmias induced by thetumor. At operation, an incision line was confirmed bydirect ultrasonography. The heart was incised directlyon the interventricular septum. The tumor was care-fully dissected and completely removed without enter-ing the ventricular cavity. Histologic analysis revealeda fibroma. The patient’s postoperative course was
Accepted for publication Aug 1, 2012.
Address correspondence to Dr Kimura, 2-8-29 Musashidai, Fuchu-shi,
Tokyo 183-8561, Japan; e-mail: [email protected].© 2013 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
uneventful, and he remains well without episodes ofheart failure or ventricular arrhythmia.
(Ann Thorac Surg 2013;95:1072– 4)© 2013 by The Society of Thoracic Surgeons
Cardiac fibroma is a rare lesion that typically arisesfrom the ventricular free wall or interventricular
septum. Although it is a benign tumor, surgical interven-tion is recommended when children experience second-ary clinical symptoms [1]. Cho and colleagues [2] re-ported that most ventricular fibromas can be completelyor almost completely resected with good results. In casereports, tumors were removed or resected by entering 1or both ventricular cavities, and the septum was recon-structed directly or with a patch. This report describes acase of a large interventricular fibroma that was success-fully removed without ventriculotomy.
A 14-month-old boy with no significant medical historyhad a sudden onset of convulsions at his home followedby cardiopulmonary arrest. Cardiopulmonary resuscita-tion was initiated immediately, and normal sinus rhythmwas restored within 20 minutes. He was admitted to theintensive care unit of our hospital. Transthoracic echo-cardiography showed a large hypoechoic mass in theinterventricular septum, consistent with cardiac tumor(Fig 1A). Cardiac magnetic resonance imaging showed awell-defined large tumor in the interventricular septum,with tumor signal low in the early phase and tumorsignal rapidly enhanced in the late phase (Fig 1B). Car-diac fibroma was highly suspected based on these find-ings. Cardiac catheterization revealed normal pressureand good cardiac function without significant inflow oroutflow obstruction. Amiodarone therapy was initiated,but the patient experienced 2 additional episodes ofconvulsions, and electrocardiographic monitoring dem-onstrated simultaneous onset of nonsustained ventricu-lar tachycardia for about 1 minute. Fortunately, his he-modynamic status was not severely compromised, andthe convulsions remitted spontaneously. He was referredfor surgical intervention to prevent a potentially lethaloutcome related to malignant ventricular arrhythmia.
The operation was performed when the patient was 17months old. Through a median sternotomy, he wasplaced on cardiopulmonary bypass, and an ultrasonog-raphy probe was placed directly on the surface of theheart to confirm the incisional line needed to reach thetumor without entering the ventricles. The aorta wasthen cross-clamped, and cardioplegic arrest was induced.The heart was incised directly on the interventricularseptum along the left anterior descending artery, and agray-white tumor was found at a depth of 5 mm. Thetumor was carefully dissected, and complete excision wasachieved without entry into the ventricular cavity (Fig2A). The tumor was 60 � 35 � 18 mm and weighed 13 g(Fig 2B). Hemostasis was established, and the spaceoccupied by the tumor in the interventricular septum wasclosed by running sutures to minimize the dead space.
The heart incision was then closed. The aortic cross-0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2012.08.028