Embed Size (px)
Citation preview

Sudden Cardiac Death in Patients with Left
Ventricular Dysfunction: Focus on Primary Prevention
with ICDsAndrew E. Epstein, MD Professor of Medicine
Division of Cardiovascular DiseaseThe University of Alabama at Birmingham
Birmingham, Alabama

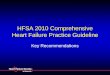
Moss et al. N Engl J Med 2002;346:877-83.
ICD
Conventional
P = 0.007
1.0
0.9
0.8
0.7
0.6
0.0
Probability of Survival
0 1 2 3 4Year
MADIT II: Probability of Survival in ICD vs Conventional Therapy Group
No. At Risk Defibrillator 742 502 (0.91) 274 (0.84) 110 (0.78) 9 Conventional 490 329 (0.90) 170 (0.78) 65 (0.69) 3
• Trial stopped at 20 months • Reduction in death rate with
ICD Rx: 12% at 1 yr, 28% at 2 yrs, 28% at 3 yrs

Comparison of Medical Therapy, Pacing and Defibrillation Therapies in Heart Failure (COMPANION) Trial
• NYHA Class III or IV • NSR, QRS ≥120 ms, PR interval >150 ms • LVEF ≤35%, LVEDD ≥60 mm • Optimal pharmacological therapy (OPT)
• β-blocker (for at least 3 months) • Diuretic, ACEI/ARB, spironolactone (1 month) • Digoxin
• HF hospitalization (or equivalent) in prior 12 months, >1 month prior to enrollment

COMPANION Design
• OPT • CRT w/ ICD Backup
+2
• OPT • CRT
+2
Randomization Stratification
Baseline Implant Follow-up Follow-up Follow-up
Follow-up Follow-up Follow-up
Implant Follow-up Follow-up Follow-up
• OPT
1
<5 Days 0 <2 Working Days One Week One Month Quarterly
Time Post-Randomization
Endpoints Primary: Combined all-cause mortality and all-cause hospitalization Secondary: Morbidity and survival Substudy: QoL

HFSA Late-Breaking Clinical Trials, September 24, 2003. Bristow MR, et al. N Engl J Med 2004;350:2140-2150.
0
20
40
60
80
100
Days from Randomization
Patie
nts
Even
t-fre
e (%
) OPT CRT HR .80 (CI: .68-.94) CRT-D HR .80 (CI: .67-.94)
0 120 240 360 480 600 720 840 960 1,080
12-Month Event Rates OPT: 68% CRT: 55% (AR=13%) CRT-D: 56% (AR=12%)
CRT vs OPT: RR=20%, P=.008 (Critical boundary=.014) CRT-D vs OPT: RR=20%, P=.007 (Critical boundary=.022)
COMPANION: Primary Endpoint: Mortality+Hospitalization

50
60
70
80
90
100
Days from Randomization
OPT CRT HR .76 (CI: .58-1.01) CRT-D HR .64 (CI: .48-.86)
0 120 240 360 480 600 720 840 960 1,080
12-Month Event Rates OPT: 19% CRT: 15% (AR=4%) CRT-D: 12% (AR=7%)
CRT vs OPT: RR=24%, P=.060 (Critical boundary=.014) CRT-D vs OPT: RR=36%, P=.003 (Critical boundary=.022)
Patie
nts
Even
t-fre
e (%
)COMPANION:
Secondary Endpoint: All-Cause Mortality
HFSA Late-Breaking Clinical Trials, September 24, 2003. Bristow MR, et al. N Engl J Med 2004;350:2140-2150.

CRT Improves QoL and NYHA Functional Class
Average Change in QoL Score (MLWHF)
-18
-13,5
-9
-4,5
0
MIR
ACLE
(1)
MUS
TIC
SR (2
)M
USTI
C AF
(3)
CONT
AK C
D (4
)M
IRAC
LE IC
D (5
)
ControlCRT
* * * *
* P<0.05
NYHA: Proportion Improving 1 or More Class
0 %
20 %
40 %
60 %
80 %
MIRACLE (1) MIRACLE ICD (5)
ControlCRT
**
*
1Abraham WT et al. N Engl J Med. 2002;346:1845-1853. 2Cazeau S. N Engl J Med. 2001;344:873-80. 3Leclercq C et al. Eur Heart J. 2002;23:1780-1787.4http://www.fda.gov/cdrh/pdf/P010012b.pdf. Accessed August 2, 2002. 5Young JB et al. JAMA. 2003;289:2685-2694.

Favors CRT Favors No CRT
0.1 0.5 1.0 2.0 3.0
Heart Failure Mortality in Meta Analysis of CRT Trials
Odds Ratio (95% CL)
CONTAK CD (n=490)
InSync ICD (n=554)
MIRACLE (n=532)
MUSTIC (n=58)Overall
Bradley et al. JAMA 2003; 289: 730

Sudden Cardiac Death in Heart Failure Trial: SCD-HeFT
CAD and DCM NYHA II and III
LVEF ≤0.35 No prior VT or VF
Conventional Rx +
Placebo
Conventional Rx +
Amiodarone
Conventional Rx +
ICD
Randomize
Double blind Endpoint: Total Mortality

0
.1
.2
.3
.4
Months of Follow-Up
Mor
talit
y
Amiodarone ICD Therapy Placebo
0 6 12 18 24 30 36 42 48 54 60
HR 97.5% CI P Value Amiodarone vs Placebo 1.06 .86, 1.30 .529 ICD Therapy vs Placebo .77 .62, 0.96 .007
SCD-HeFTMortality by Intention-to-Treat
Bardy GH, et al. N Engl J Med 2005;352:225-237.

CARE-HF Aims
• To assess the effect on morbidity and mortality of adding CRT to optimised pharmacological therapy in patients with moderate and severe HF due to LVSD complicated by cardiac dyssynchrony
• To investigate the mechanisms underlying the observed effect to identify markers predicting success or failure of CRT
Cleland JG, et al. N Engl J Med 2005;352:1539-1549.

CARE-HF Primary Endpoint
(All-cause Mortality or Unplanned Hosp. for Major CVS Event)
348118232292404Medical Therapy768166273323409CRT
Number at risk 0 500 1000 15000.00
0.25
0.50
0.75
1.00
HR 0.63 (95% CI 0.51 to 0.77) P < .0001
Even
t-fre
e Su
rviv
al
Days
CRT
Medical Therapy
Cleland JG, et al. N Engl J Med 2005;352:1539-1549.

CARE-HF All-Cause Mortality
571192321365404Medical Therapy889213351376409CRT
Number at risk 0 500 1000 15000.00
0.25
0.50
0.75
1.00Ev
ent-f
ree
Surv
ival
Days
Medical Therapy
HR 0.64 (95% CI 0.48 to 0.85) P = .0019
CRT
Cleland JG, et al. N Engl J Med 2005;352:1539-1549.

Recovery of LV Function Post MI• 261 patients in HEART (ramipril) trial, all
with reperfusion therapy • Day 1, 9/261 had normal LV function (EF ≥0.55, 3.4%)
• 171/261 (66%) had improvement in EF (0.05 ± 0.10). Final EF 0.57 ± 0.96
• Of 252 patients with EF <0.55: • 13% complete recovery by day 14 • 22% complete recovery by day 90 • Additional 36% had partial recovery by
day 90 ➔ Early dysfunction often improves
Solomon et al. Ann Intern Med 2001;134:451-8

Reasons for Nonresponse• Inappropriate patient selection
• End stage • No dyssynchrony • No correctable dyssynchrony
• Too strict definition of response • Is prevention of disease progression “response”?
• More attention needs to paid to VV timing and AV delays

Procedural Outcomes and Complications in COMPANION Trial
0
3,8
7,5
11,3
15
CRT (n=617) CRT-D (n=595)
%
Implant death
Perforation Any LVlead AE
Lead implant failure
1.3% 1.8% 6.3% 13%0.8% 0.8% 4.7% 9%
Saxon et al. Circulation 2004:110:111.

Cardiac Resynchronization TherapyEntry Criteria Randomized Trials
Study (n) NYHA QRS EF Status
MIRACLE (524#) III, IV ≥130 < 35% Published
MUSTIC SR (58) III >150 < 35% Published
MUSTIC AF (43) III >200* < 35% Published
PATH CHF (42) III, IV ≥120 < 35% Published
CONTAK CD (581¥) III-IV ≥120 < 35% Published
MIRACLE ICD (362^) III-IV ≥130 < 35% Published
PATH CHF II (89) III, IV ≥120 < 35% Published
COMPANION (1520) III, IV ≥120 < 35% Published
CARE HF (800) III, IV ≥120† < 35% Published
MIRACLE ICD II (186) II ≥130 < 35% Presented
PACMAN (328) III ≥150 < 35% Enrolled
VecToR (420) II-IV ≥140 < 35% Enrolling
From WT Abraham
No Randomized Trials Used an Imaging
Dyssynchrony Study

Should all Patients with CHF get a CRT Device?
LBBB QRS >120ms NYHA III,IV EF <35%
NSR Optimal Med Rx
IVCD / RBBB QRS 100-120ms
NYHA II (I) EF 35-40%
AF Optimal Med Rx
Straight Shot Longer Shot
CRT / ICD
ECHO Dyssynchrony
YES No ??Courtesy of Kenneth A. Ellenbogen, MD

Pacemaker and ICD Malfunctions
Maisel WH, et al. JAMA 2006; 295:1901-1906.
Pacemakers n=8834 ICDs n=8489 Devices explanted and malfunction confirmed

• Over 200,000 ICDs are implanted or replaced annually in patients who are at risk for SD.
• In 2005 over 150,000 ICDs were the subject of recalls or safety alerts by their manufacturers.
• A recent Food and Drug Administration study suggested that ICD malfunctions are increasing.
• The Multicenter Registry is funded entirely by a grant from the Minneapolis Heart Institute Foundation, and is supported by the voluntary efforts of its participants.
The Multicenter Registry Investigators American College of Cardiology, 2006
Multicenter Experience With 1,355 Failed and Recalled Implantable Cardioverter Defibrillators

Objective
• The aim of the present study was to examine the failure modes and implant times of contemporary ICD pulse generators in that had failed, or were replaced due to manufacturers recalls.
• We also evaluated the causes and major adverse clinical events associated with ICD failure and replacement.
The Multicenter Registry Investigators American College of Cardiology, 2006
The Multicenter Registry Investigators American College of Cardiology, 2006

Methods
• 9 centers in the U. S. and Canada. • Failure reports entered via Internet since 4/99:
Manufacturer and model Dates of implant and failure Signs of failure and clinical consequence Cause of failure
• A pulse generator failed if it was not performing according to its intended use, or as described in the manufacturer’s published specifications. A normally functioning device that was replaced, removed, or abandoned as the result of a manufacturer’s recall was a failure.
PACE 2001; 24:82-87.

Methods (2)• Categories of ICD pulse generator failure included: Normal battery depletion (ERI)
Premature battery depletion (ERI ≤ 3 yrs) Electronic or housing malfunction Replacement for Recall-Advisory Unknown
• Cause of failure was determined by the reporting center based on clinical and technical evaluations and manufacturers reports.
PACE 2001; 24:82-87.

0
10
20
30
40
50
60
70
80
Normal Battery
Depletion
Recall Advisory
Premature Battery
Depletion
Electronic Housing
Malfunction
Unknown
Perc
ent o
f Pul
se G
ener
ator
s73%
10% 9%6% 2%
Causes of ICD Failure
1,355 Pulse Generators
N= 988 135 122 85 25The Multicenter Registry Investigators American College of Cardiology, 2006

ICD Types and Manufacturers
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
All Single Dual Single-R Dual-R CRT-D
Guidant Medtronic St. Jude
N= 1,355 791 35 93 388 48% = 58% 29%3% 7% 4%100%
All Dual Single Single-R Dual-R CRT-D
The Multicenter Registry Investigators American College of Cardiology, 2006

Causes of Failure for Each ICD Type
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
All Single Dual Single-R Dual-R CRT-D
Normal Battery Depletion
Recall Premature Battery Depletion
Electronic Housing
The Multicenter Registry Investigators American College of Cardiology, 2006

0
1
2
3
4
5
6
Dual Single Dual-R Single-R CRT-D All
Year
s
79135 93388 48 1,355N =
p < 0.001
5.14.8
3.4
2.5
1.9
4.1
Average Implant Time of Failed ICDs
% = 3% 58% 29% 7% 4% 100%The Multicenter Registry Investigators American College of Cardiology, 2006

Average Implant Time of Failed ICDs According to Cause of Failure
0
1
2
3
4
5
6
Years
All Single Dual Single-R Dual-R CRT-D
Normal Battery Depletion
Recall Premature Battery Depletion
Electronic Housing
The Multicenter Registry Investigators American College of Cardiology, 2006

0
10
20
30
40
50
60
70
80
90
100
1 5 9 13 17 21 25 29 33 37 41 45 49 53 57 61 65 69 73 77 81 85 89 93 97 101 105
Years After Implant
Perc
ent F
unct
ioni
ng
1 2 3 4 5 6 7 80
ICDs with and w/o Rate Response
Years After Implantation 0 1 2 3 4 5 6 7 8
Rate Response
No Rate Response
P< 0.001
The Multicenter Registry Investigators American College of Cardiology, 2006

0 10 20 30 40 50 60 70 80 90 100
Percent
CRT-D
Single-R
Dual-R
Dual
Single
AlI
3 years4 years5 years
Proportion of Failed ICDs That Were Functioning 3, 4, & 5 Years After Implant
Percent Functioning
27%
The Multicenter Registry Investigators American College of Cardiology, 2006

Major Adverse Clinical Events• 20 patients had a major adverse clinical event. • 1 patient died due to short-circuiting during shock
delivery. • 1 patient died of a stroke following replacement of a
normally functioning recalled device. • 4 patients were rescued when their devices failed to
treat VT/VF during device testing. • 3 patients experienced syncope due to battery
depletion (2) and electronic component failure. • 11 patients received inappropriate shocks caused by
electronic and housing defects.
The Multicenter Registry Investigators American College of Cardiology, 2006

Limitations• Average implant time may significantly
underestimate device longevity when compared to actuarial survival data.
• The longevity of an ICD pulse generator is the result of a complex interplay between multiple hardware components, the ICD lead, and the individual patient’s needs for therapy, energy requirements for pacing and defibrillation, and diagnostic information including electrograms. We did not evaluate all these variables.
The Multicenter Registry Investigators American College of Cardiology, 2006

Conclusions• Based on this analysis of failed ICDs, the
performance of ICDs, particularly those offering advanced pacing capabilities, has been adversely affected by early battery depletion, electronic or housing failure and recalls.
• A comprehensive, independent national registry is needed to accurately estimate ICD longevity and determine the incidence of unexpected failure modes and adverse clinical events.
The Multicenter Registry Investigators American College of Cardiology, 2006

Complications Associated with ICD Replacement in Response to Advisories:Canadian Heart Rhythm Society Working Group on Device Advisories
• 17 Centers, 2915 recalled devices • 533 (18.3%) replaced
• 66% primary prevention
• Complications in 43 pts (8.1%) • Major requiring reoperation: 31 pts (5.8%) • Death: 2 pts • Minor complications: 12 pts (2.3%) • Of explanted devices, 3 (0.1%) had malfunction (early battery depletion),
none with clinical consequence.
Gould et al. JAMA 2006; 295:1907-1911.

Indications for ICD TherapyClass I • Cardiac arrest due to VF or VT not due to a transient or reversible
cause • Spontaneous sustained VT in association with structural heart disease • Syncope of undetermined origin with clinically relevant,
hemodynamically significant, sustained VT or VF induced at EP study when drug therapy is ineffective, not tolerated, or not preferred
• Nonsustained VT in patients with coronary disease, prior MI, LV dysfunction, and inducible VF or sustained VT at EP study that is not suppressible by a Class I antiarrhythmic drug.
Class II • Patients with LVEF ≤.30, at least 1 month post MI and at least 3 months
post coronary revascularization surgery
Gregoratos G, et al. Circulation. 2002;106:2145-2161.

Class II
• Medically refractory, NYHA Class III or IV heart failure despite optimal medical therapy
• Ischemic or nonischemic cardiomyopathy with
• QRS ≥130 ms
• LVEF ≤0.35
Indications for Resynchronization Therapy
Gregoratos G, et al. Circulation. 2002;106:2145-2161.

Summary• Multiple RCTs have shown that CRT:
• Is safe and well tolerated improves quality of life, functional status, and exercise capacity.
• Improves cardiac structure and function. • Reduces hospitalization and mortality with or without ICD backup.
• Studies needed to risk stratify, identify likely responders, and new groups who may benefit from CRT.
• Reliability/advisory issues recognized and need guidelines for management.