Embed Size (px)
Citation preview
Abstract Case Report – Four Days Posttreatment Discussion
Objective: To present a rare case report of a teenager who developed sudden bilateral moderately-severe sensorineural hearing loss following a night of polysubstance abuse that resolved with pentoxifylline therapy. Presentation, audiologic findings, associated co-morbidities, treatment options, and potential etiologies are discussed.Study Design: Case report and review of literature.Methods: Chart review of an 18-year-old female who presented two days after a binge of polysubstance abuse with sudden-onset bilateral hearing loss. Workup included MRI / CT brain imaging, lumbar puncture, and infectious disease / autoimmune screening. Results: The patient admitted to using heroin, benzodiazepines and cocaine one night prior to developing bilateral moderately-severe sensorineural hearing loss (60 dB SRT/ 60% discrimination). The hearing loss was initially treated with high-dose oral prednisone and antiviral therapy without resolution, followed by a ten month course of pentoxifylline with subsequent hearing improvement no longer requiring hearing-aid amplification (normal speech audiometry, 15dB SRT / 90% discrimination) and only residual high-frequency sensorineural hearing loss (3-8 kHz). Conclusion: This case report highlights the importance of recreational drug abuse history when evaluating patients with sudden onset hearing loss. Several cases have been reported in the literature with sudden hearing loss requiring cochlear implantation following hydrocodone / acetaminophen abuse. Potential etiologies include altered pharmacokinetics, vascular spasm / ischemia, encephalopathy, acute intralabyrinthine injury and genetic polymorphisms of drug metabolizing enzymes.
• Six days following the onset of hearing loss, the patient presented to our office for a second opinion.
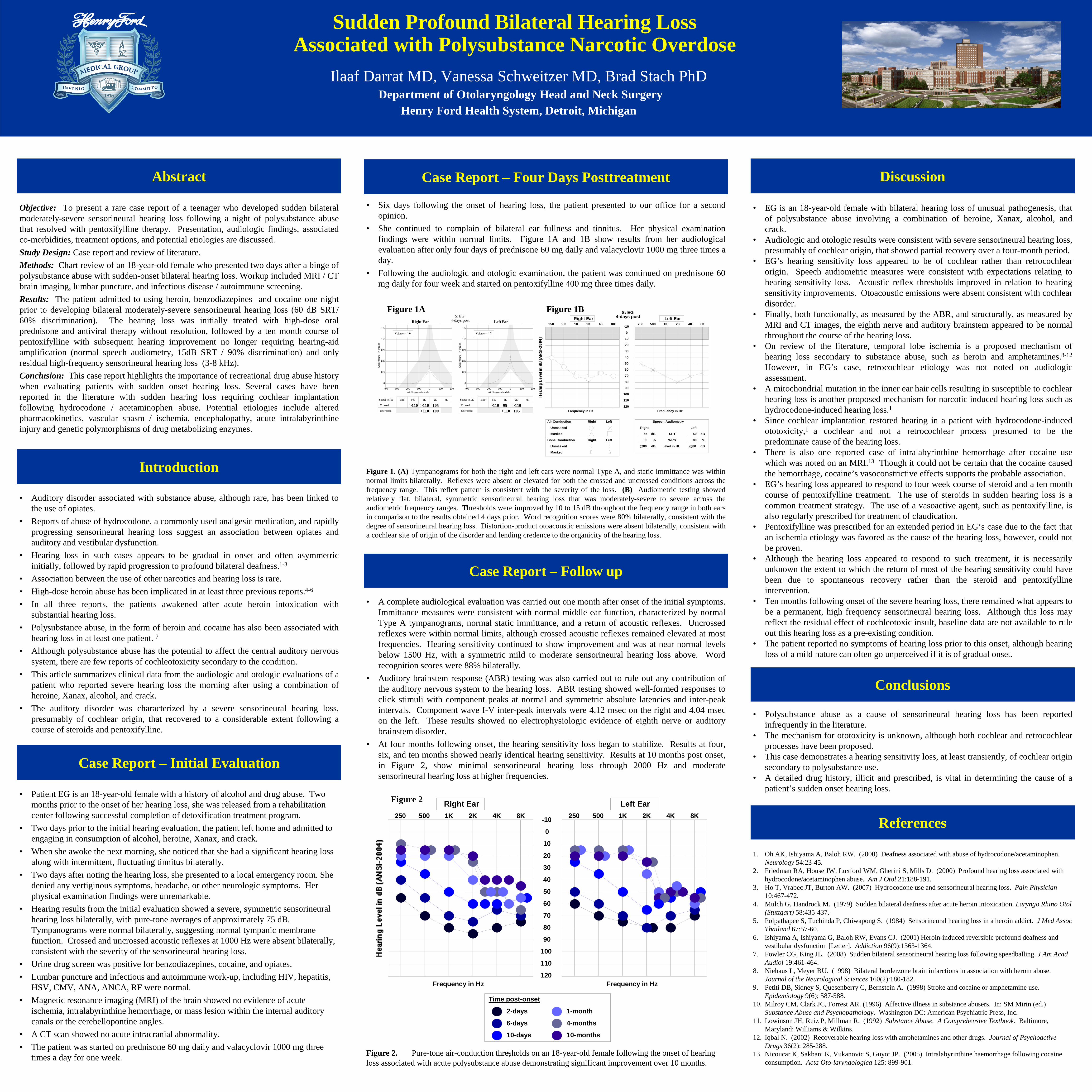
• She continued to complain of bilateral ear fullness and tinnitus. Her physical examination findings were within normal limits. Figure 1A and 1B show results from her audiological evaluation after only four days of prednisone 60 mg daily and valacyclovir 1000 mg three times a day.
• Following the audiologic and otologic examination, the patient was continued on prednisone 60 mg daily for four week and started on pentoxifylline 400 mg three times daily.
• A complete audiological evaluation was carried out one month after onset of the initial symptoms. Immittance measures were consistent with normal middle ear function, characterized by normal Type A tympanograms, normal static immittance, and a return of acoustic reflexes. Uncrossed reflexes were within normal limits, although crossed acoustic reflexes remained elevated at most frequencies. Hearing sensitivity continued to show improvement and was at near normal levels below 1500 Hz, with a symmetric mild to moderate sensorineural hearing loss above. Word recognition scores were 88% bilaterally.
• Auditory brainstem response (ABR) testing was also carried out to rule out any contribution of the auditory nervous system to the hearing loss. ABR testing showed well-formed responses to click stimuli with component peaks at normal and symmetric absolute latencies and inter-peak intervals. Component wave I-V inter-peak intervals were 4.12 msec on the right and 4.04 msec on the left. These results showed no electrophysiologic evidence of eighth nerve or auditory brainstem disorder.
• At four months following onset, the hearing sensitivity loss began to stabilize. Results at four, six, and ten months showed nearly identical hearing sensitivity. Results at 10 months post onset, in Figure 2, show minimal sensorineural hearing loss through 2000 Hz and moderate sensorineural hearing loss at higher frequencies.
• EG is an 18-year-old female with bilateral hearing loss of unusual pathogenesis, that of polysubstance abuse involving a combination of heroine, Xanax, alcohol, and crack.
• Audiologic and otologic results were consistent with severe sensorineural hearing loss, presumably of cochlear origin, that showed partial recovery over a four-month period.
• EG’s hearing sensitivity loss appeared to be of cochlear rather than retrocochlear origin. Speech audiometric measures were consistent with expectations relating to hearing sensitivity loss. Acoustic reflex thresholds improved in relation to hearing sensitivity improvements. Otoacoustic emissions were absent consistent with cochlear disorder.
• Finally, both functionally, as measured by the ABR, and structurally, as measured by MRI and CT images, the eighth nerve and auditory brainstem appeared to be normal throughout the course of the hearing loss.
• On review of the literature, temporal lobe ischemia is a proposed mechanism of hearing loss secondary to substance abuse, such as heroin and amphetamines.8-12
However, in EG’s case, retrocochlear etiology was not noted on audiologic assessment.
• A mitochondrial mutation in the inner ear hair cells resulting in susceptible to cochlear hearing loss is another proposed mechanism for narcotic induced hearing loss such as hydrocodone-induced hearing loss.1
• Since cochlear implantation restored hearing in a patient with hydrocodone-induced ototoxicity,1 a cochlear and not a retrocochlear process presumed to be the predominate cause of the hearing loss.
• There is also one reported case of intralabyrinthine hemorrhage after cocaine use which was noted on an MRI.13 Though it could not be certain that the cocaine caused the hemorrhage, cocaine’s vasoconstrictive effects supports the probable association.
• EG’s hearing loss appeared to respond to four week course of steroid and a ten month course of pentoxifylline treatment. The use of steroids in sudden hearing loss is a common treatment strategy. The use of a vasoactive agent, such as pentoxifylline, is also regularly prescribed for treatment of claudication.
• Pentoxifylline was prescribed for an extended period in EG’s case due to the fact that an ischemia etiology was favored as the cause of the hearing loss, however, could not be proven.
• Although the hearing loss appeared to respond to such treatment, it is necessarily unknown the extent to which the return of most of the hearing sensitivity could have been due to spontaneous recovery rather than the steroid and pentoxifylline intervention.
• Ten months following onset of the severe hearing loss, there remained what appears to be a permanent, high frequency sensorineural hearing loss. Although this loss may reflect the residual effect of cochleotoxic insult, baseline data are not available to rule out this hearing loss as a pre-existing condition.
• The patient reported no symptoms of hearing loss prior to this onset, although hearing loss of a mild nature can often go unperceived if it is of gradual onset.
Introduction
Case Report – Follow up
• Auditory disorder associated with substance abuse, although rare, has been linked to the use of opiates.
• Reports of abuse of hydrocodone, a commonly used analgesic medication, and rapidly progressing sensorineural hearing loss suggest an association between opiates and auditory and vestibular dysfunction.
• Hearing loss in such cases appears to be gradual in onset and often asymmetric initially, followed by rapid progression to profound bilateral deafness.1-3
• Association between the use of other narcotics and hearing loss is rare. • High-dose heroin abuse has been implicated in at least three previous reports.4-6
• In all three reports, the patients awakened after acute heroin intoxication with substantial hearing loss.
• Polysubstance abuse, in the form of heroin and cocaine has also been associated with hearing loss in at least one patient. 7
• Although polysubstance abuse has the potential to affect the central auditory nervous system, there are few reports of cochleotoxicity secondary to the condition.
• This article summarizes clinical data from the audiologic and otologic evaluations of a patient who reported severe hearing loss the morning after using a combination of heroine, Xanax, alcohol, and crack.
• The auditory disorder was characterized by a severe sensorineural hearing loss, presumably of cochlear origin, that recovered to a considerable extent following a course of steroids and pentoxifylline.
Case Report – Initial Evaluation
References
1. Oh AK, Ishiyama A, Baloh RW. (2000) Deafness associated with abuse of hydrocodone/acetaminophen. Neurology 54:23-45.
2. Friedman RA, House JW, Luxford WM, Gherini S, Mills D. (2000) Profound hearing loss associated with hydrocodone/acetaminophen abuse. Am J Otol 21:188-191.
3. Ho T, Vrabec JT, Burton AW. (2007) Hydrocodone use and sensorineural hearing loss. Pain Physician10:467-472.
4. Mulch G, Handrock M. (1979) Sudden bilateral deafness after acute heroin intoxication. Laryngo Rhino Otol (Stuttgart) 58:435-437.
5. Polpathapee S, Tuchinda P, Chiwapong S. (1984) Sensorineural hearing loss in a heroin addict. J Med Assoc Thailand 67:57-60.
6. Ishiyama A, Ishiyama G, Baloh RW, Evans CJ. (2001) Heroin-induced reversible profound deafness and vestibular dysfunction [Letter]. Addiction 96(9):1363-1364.
7. Fowler CG, King JL. (2008) Sudden bilateral sensorineural hearing loss following speedballing. J Am Acad Audiol 19:461-464.
8. Niehaus L, Meyer BU. (1998) Bilateral borderzone brain infarctions in association with heroin abuse. Journal of the Neurological Sciences 160(2):180-182.
9. Petiti DB, Sidney S, Quesenberry C, Bernstein A. (1998) Stroke and cocaine or amphetamine use. Epidemiology 9(6); 587-588.
10. Milroy CM, Clark JC, Forrest AR. (1996) Affective illness in substance abusers. In: SM Mirin (ed.) Substance Abuse and Psychopathology. Washington DC: American Psychiatric Press, Inc.
11. Lowinson JH, Ruiz P, Millman R. (1992) Substance Abuse. A Comprehensive Textbook. Baltimore, Maryland: Williams & Wilkins.
12. Iqbal N. (2002) Recoverable hearing loss with amphetamines and other drugs. Journal of Psychoactive Drugs 36(2): 285-288.
13. Nicoucar K, Sakbani K, Vukanovic S, Guyot JP. (2005) Intralabyrinthine haemorrhage following cocaine consumption. Acta Oto-laryngologica 125: 899-901.
• Patient EG is an 18-year-old female with a history of alcohol and drug abuse. Two months prior to the onset of her hearing loss, she was released from a rehabilitation center following successful completion of detoxification treatment program.
• Two days prior to the initial hearing evaluation, the patient left home and admitted to engaging in consumption of alcohol, heroine, Xanax, and crack.
• When she awoke the next morning, she noticed that she had a significant hearing loss along with intermittent, fluctuating tinnitus bilaterally.
• Two days after noting the hearing loss, she presented to a local emergency room. She denied any vertiginous symptoms, headache, or other neurologic symptoms. Her physical examination findings were unremarkable.
• Hearing results from the initial evaluation showed a severe, symmetric sensorineural hearing loss bilaterally, with pure-tone averages of approximately 75 dB. Tympanograms were normal bilaterally, suggesting normal tympanic membrane function. Crossed and uncrossed acoustic reflexes at 1000 Hz were absent bilaterally, consistent with the severity of the sensorineural hearing loss.
• Urine drug screen was positive for benzodiazepines, cocaine, and opiates. • Lumbar puncture and infectious and autoimmune work-up, including HIV, hepatitis,
HSV, CMV, ANA, ANCA, RF were normal.• Magnetic resonance imaging (MRI) of the brain showed no evidence of acute
ischemia, intralabyrinthine hemorrhage, or mass lesion within the internal auditory canals or the cerebellopontine angles.
• A CT scan showed no acute intracranial abnormality.• The patient was started on prednisone 60 mg daily and valacyclovir 1000 mg three
times a day for one week. \
Sudden Profound Bilateral Hearing Loss Associated with Polysubstance Narcotic Overdose
Ilaaf Darrat MD, Vanessa Schweitzer MD, Brad Stach PhDDepartment of Otolaryngology Head and Neck Surgery
Henry Ford Health System, Detroit, Michigan
Right Ear
Signal to RE BBN 500 1K 2K 4K
Crossed
Uncrossed
>110 105 100
-400 -300 -200 -100 0 100 200 Air Pressure in daPa
1.5
1.2
0.9
0.6
0.3
0
LeftEar
Signal to LE BBN 500 1K 2K 4K
Crossed
Uncrossed
95 105
-400 -300 -200 -100 0 100 200 Air Pressure in daPa
1.5
1.2
0.9
0.6
0.3
0
S: EG4-days post
Volume = 1.0 Volume = 1.2
>110>110 >110
>110>110
250 500 1K 2K 4K 8K
Frequency in Hz
250 500 1K 2K 4K 8K
Frequency in Hz
110
120
100
80
60
40
20
0
-10
10
30
50
70
90
Right Ear Left Ear
Right Left
Unmasked
Right Left
Masked
Unmasked
Masked
Air Conduction
Bone Conduction
Speech Audiometry
Right Left
SRT
WRS
Level in HL
dB
%
dB
%
55 50
80
@80
80
@80dB dB
S: EG4-days post
Figure 1A Figure 1B
Figure 1. (A) Tympanograms for both the right and left ears were normal Type A, and static immittance was within normal limits bilaterally. Reflexes were absent or elevated for both the crossed and uncrossed conditions across the frequency range. This reflex pattern is consistent with the severity of the loss. (B) Audiometric testing showed relatively flat, bilateral, symmetric sensorineural hearing loss that was moderately-severe to severe across the audiometric frequency ranges. Thresholds were improved by 10 to 15 dB throughout the frequency range in both ears in comparison to the results obtained 4 days prior. Word recognition scores were 80% bilaterally, consistent with the degree of sensorineural hearing loss. Distortion-product otoacoustic emissions were absent bilaterally, consistent with a cochlear site of origin of the disorder and lending credence to the organicity of the hearing loss.
Figure 2
Figure 2. Pure-tone air-conduction thresholds on an 18-year-old female following the onset of hearing loss associated with acute polysubstance abuse demonstrating significant improvement over 10 months.
250 500 1K 2K 4K 8K
Frequency in Hz
250 500 1K 2K 4K 8K
Frequency in Hz
110
120
100
80
60
40
20
0
-10
10
30
50
70
90
Right Ear Left Ear
2-days
6-days
10-days
1-month
4-months
10-months
Time post-onset
Conclusions
• Polysubstance abuse as a cause of sensorineural hearing loss has been reported infrequently in the literature.
• The mechanism for ototoxicity is unknown, although both cochlear and retrocochlear processes have been proposed.
• This case demonstrates a hearing sensitivity loss, at least transiently, of cochlear origin secondary to polysubstance use.
• A detailed drug history, illicit and prescribed, is vital in determining the cause of a patient’s sudden onset hearing loss.


















![Oliver Strange - Sudden Westerns 06 - Sudden Gold-Seeker(1937)[1]](https://img.pdfslide.net/doc/110x75/54fae2e44a7959575b8b4b9b/oliver-strange-sudden-westerns-06-sudden-gold-seeker19371.jpg)









