Embed Size (px)
Citation preview

Supercharging the blood: How GPs can help preoperative blood management Dr Michael Leahy Haematology Royal Perth Hospital

Discussion topics
Anaemia the problem Patient Blood Management Preoperative assessment Management

Prevalence of preoperative anaemia in elective surgery
Non-cardiac 30-40% Orthopaedic 20-44% Cardiac surgery 25-54% Colorectal surgery 25-70% Major gynaecological 17%
(Browning 2012) Vascular
33% Auerbach M. et al. Transfusion (2008) Beattie et al: Anesthesiology (2009) 110:574 Bierbaum B.E. et al. J Bone Joint Surg (1999) 81:2 Carson J et al: JAMA. (1998) 279:199-205 Dunkelgrun et al: Am J Cardiol (2008)101:1196 Gombotz H. et al: Tranfusion (2007) 47:1468 Karkouti K. et al. Circulation (2008) 117: 478 Hung et al. Anaesthesia (2011)66:812 Kulier A. et al. Circulation (2007) 116: 471 Sahleh et al: Br J Anaesth. (2007) 99:801.
71% males and 56% females for cardiac & orthopaedic surgery were anaemic on admission. Grey et al. Vox Sang 2011

Krishnasivam et al Transfusion 2018
Prevalence of anaemia in patients admitted to RPH over 2010-2015

Patient Blood Management : definition
“Patient blood management is an evidence-based bundle of care that optimizes medical and surgical patient outcomes by clinically managing and preserving a patient’s blood” Leahy et al Transfusion 2017 Consensus definition developed at the International Foundation for Patient Blood Management International PBM Summit Melbourne Australia 2016

Optimise patient’s
own blood
Minimise blood loss
& Bleeding
Harness & optimise physio-logical
tolerance of anaemia
1st Pillar
2nd Pillar
3rd Pillar
9/2011 PBM FHHS Hofmann: The Oncologist 2011

Fremantle Hospital workshops in 2012 assist GPs to optimise patients for surgery

..likely significant blood loss ? orthopaedic, GIT, gynaecology preoperative assessment ? ….history ? …basic investigations ? Anaemia, iron deficiency, renal failure ?
Questions to ask when referring patients for surgery ?

History
Tiredness, fatigue G I Tract symptons and signs Menorrhagia Cardiac disease Haematuria or haemoglobinuria

Examination
Pallor Koilonychia Cardiac murmurs Abdominal masses Splenomegaly Telangiectases

Co-morbidities
Chronic inflammation Renal dysfunction Liver dysfunction Cardiac failure B12 and/or folate deficiency Iron deficiency

Clinical consequences of iron deficiency
IDA correlates with reduced health-related QoL, treating IDA improves QoL hair loss
Significant economic-burden on the individual and the whole population
Tachycardia Dyspnoea
Restless legs
Nausea Chronic fatigue
Impaired cognitive function
Headache
Increased susceptibility to
infection
Abnormal nail findings and hair loss
Gasche C., et al., Gut, 2004, 53: 1190–1197. Bruner AB., et al., Lancet, 1996, 348: 992–996. Ebinger M., et al., J Gastroenterol Hepatol., 2004, 19: 192–199. Ershler WB., et al., Value Health, 2005, 8: 629–638.
Gasche C., et al., Inflamm Bowel Dis., 2007, 13: 1545-1553. Pizzi LT., et al., Inflamm Bowel Dis., 2006, 12: 47–52. Wells CW., et al., Inflamm Bowel Dis., 2006, 12: 123–130.

TYPES OF IRON DEFICIENCY True iron deficiency Low hepcidin state
Functional iron deficiency – anaemia of chronic disease High or “relatively high” hepcidin state

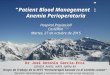
Hepcidin Regulation of Iron Uptake and Release
Copyright 2013, Irwin Gross M.D.


Criteria for diagnosis of iron deficiency in routine practice.
Aapro M et al. Ann Oncol 2012;annonc.mds112
© The Author 2012. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: [email protected]

Is the patient anaemic? Hb <130 g/L (male) or Hb <120 g/L (female)
Recommended screening to accompany GP referral (results from ≤ 3 months prior to referral): • Full blood count & reticulocyte count – single cost when ordered together • Iron studies2 including Ferritin • CRP and Creatinine – single cost when ordered together • U&Es and LFTs • Vitamin B12 & Folate if indicated – single cost when ordered together • Other investigations as appropriate depending on comorbidity
Preoperative GP Management : using the wait time to investigate anaemia and iron deficiency and to optimise haemoglobin and iron stores
This template1 is for patients referred to RPH undergoing procedures in which substantial blood loss is anticipated such as major orthopaedic, vascular, cardiac, urological and general surgery or for surgery for patients that are typically anaemic such as orthopaedic surgery.
Ferritin <30 mcg/L2,3
No Yes
Ferritin >100 mcg/L
Possible anaemia of chronic disease or inflammation, or other cause5
•Consider clinical context •Review renal function, MCV/MCH and blood film •Check B12/folate levels & reticulocyte count •Check liver and thyroid function •Seek haematology advice or, in the presence of chronic kidney disease, renal advice
Possible iron deficiency •Consider clinical context •Consider haematology advice or, in the presence of chronic kidney disease, renal advice •Discuss with gastroenterologist regarding GI investigations and their timing in relation to surgery3
•Commence iron therapy#
Iron deficiency anaemia •Evaluate possible causes based on clinical findings •Discuss with gastroenterologist regarding GI investigations and their timing in relation to surgery3
•Commence iron therapy#
•Consider iron therapy# if anticipated postoperative Hb decrease is ≥30 g/L •Determine cause and need for GI investigations if Ferritin is suggestive of iron deficiency <30 mcg/L2,3
Raised Normal
CRP4
Ferritin 30–100 mcg/L2,3
Reduced likelihood of anaemia / iron deficiency delays to patient being wait listed for surgery
‘Fit for Surgery’ (anaemia and iron deficiency specific)
For clinical advice ring haematology registrar or haematologist on call
Is Ferritin < 100mcg/L?
No Yes
PTO

Recommended screening to accompany GP surgery referral (results from ≤ 3 months prior to referral):
Full blood count & reticulocyte count – single cost when ordered together Iron studies including Ferritin CRP and Creatinine – single cost when ordered together U&Es and LFTs Vitamin B12 & Folate if indicated – single cost when ordered together Other investigations as appropriate depending on comorbidity

Ferritin <30 mcg/L Iron deficiency +/-anaemia • Evaluate possible causes based on clinical
findings • Discuss with gastroenterologist regarding GI
investigations and their timing in relation to surgery
• Commence iron therapy

Possible iron deficiency Ferritin 30-100mcg/L
•Consider clinical context •Consider haematology advice or, in the presence of chronic kidney disease, renal advice
•Discuss with gastroenterologist regarding GI investigations and their timing in relation to surgery3
•Commence iron therapy
•Transferrin Saturation <20% either absolute or functional iron deficiency

If Ferritin is 30 - 100mcg/L
Consider iron therapy if anticipated postoperative blood loss is >2-3 units RBC
i.e. Hb loss >30g/L Determine cause and need for GI
investigations if Ferritin is suggestive of iron deficiency <30 mcg/L

Possible anaemia of chronic disease or inflammation, or other cause: Ferritin >100mcg/L
•Consider clinical context •Review renal function, MCV/MCH and blood film •Check B12/folate levels & reticulocyte count •Check liver and thyroid function •Seek haematology advice or, in the presence of chronic kidney disease, renal advice
•TSAT <20% consider absolute or functional iron deficiency

Treatment of iron deficiency
Oral: if 3+ months to surgery and no significant comorbidities
Intravenous: <3 months to surgery or if comorbidities

x x


Maltofer iron polymaltose better tolerated?
100mg elemental iron in each tablet
100mg elemental iron per tablet

CLINICAL EXAMPLE OF MUCOSAL BLOCK of oral iron
Over a course of 1800mg (30 doses of 60 mg orally)
Hb increases by more than 7g/L on alternate day dosing compared with daily dosing
Alternate day dosing less side effects and more effective Stoffel et al Lancet Haematol 2017;4:524-33

IV Iron in Australia Intravenous Iron Iron Polymaltose (iron dextrin – Ferrum H/Ferrosig) $4.00 per 100 mg suitable for TDI up to 2500 mg over 5-6 hours (or
accelerated infusion) Iron Sucrose (Venofer) $13.00 per 100mg multiple 100-200 mg doses or larger 500mg* dose (no
more than 1000mg in one week before being reassessed) licensed and PBS listed for renal dialysis setting
(Australia only)

Ferric Carboxymaltose Iron carboxymaltose 2010 PBS $309 per 1000mg Up to 1000mg can be administered in 15 minutes

Dosing IV iron Gazoni formula for iron deficit in mg: [body weight in kg x (target Hb - actual Hb in g/dL) x 0.24 + 500]

Follow-up Adequate response assess at 4 weeks Hb increase by 20g/L after 3 weeks and to normal in 6-8 weeks Poor response
Ferritin >100 mcg delays response Helicobacter and Coeliac disease, vitamin C,D ? Drugs: H2 antagonists proton pump inhibitors
Once iron corrected re-assess every 3 months for 1 year, then 6-12 monthly Substitute iron again if Ferritin <100 mcg/L, Hb below normal

Case Study One…. Mrs Robson is a 42 year old mother of 7 children (aged between 18 months and 12 years). She has been short of breath on exertion for a few months and presents to the emergency department (ED) with chest
pain. She has a low grade fever, productive cough with yellow sputum and chest pain on coughing, reproduced with chest wall
pressure. Other vital signs are within normal limits and ECG and chest XRAY unremarkable. As she is being prepared for discharge home for a chest infection her FBC result came back at follows:
Hb 84 (115-155g/L) WCC 11.8 (4 – 11 a 10/9/L) Platelets 439 (150 – 400 x 10/9/L) MCV 60.1 ( 80 – 98fl) MCH 16.4 (27 – 33pg) RDW 19.2 (11.5 – 15.5 %) RCC 2.2 (3.5 - 5 x1012/L)
Differential diagnosis?
Iron studies Transferrin Saturation 6% (15-45) Ferritin 2 ug/l (15-45)
Management ? Investigation ?
-

Case Study 2: Mrs S. a 65 yr old woman arrives at pre admission clinic prior to a TKR (Total Knee Replacement) and
has an FBC, U&E, Fe studies. History of rheumatoid arthritis controlled with weekly methotrexate.
Hb 95g/L (135-180) WCC 5.3 x 10 9/L (4-11) Platelet 361 x 109/L (150 – 400)
RCC 2.1 x1012 /L (3.5-5.5) MCV 77 fl (80 – 100) MCH 26 pg (27 – 32.0) RDW 16.6 (9-15)
Ferritin 120 ug/L (30 – 620) Transferrin Sat 14 % (20 – 45%)
Creatinine 160 umol/L (60 – 110) eGFR 53 (>60 ml/min 1.73 per m2)
How would you proceed?

Case study 3 67 yr male with NIDDM presents with SOBE and chest pain prior to hip surgery. He is pale and has a yellowish complexion Hb 59g/L MCV 120 fl (80-100) RBC 1.8 x1012 (3.7-5.5) WBC 3.2 /nl ( 4-11) platelets 120/nl (150-400) Reticulocytes 2% (2-4) 50/nl (90-140) TSAT 60 % (15-45) Ferritin 700 ug/L (30-350) Bilirubin 30 umol/l (12-22) ALT 50 U/L (45-150) Alk Phosphatase 49 U/L (30-150) LDH 800 U/L (<250) Differential Diagnosis? Confirmation?

Hb 110 (135-180g/L) HCT 0.45 (0.4-0.5) WCC 7.8 (4 – 11 a 10/9/L) Platelets 389 (150 – 400 x 10/9/L) MCV 69 .0 ( 80 – 98fl) MCH 22.4 (27 – 33pg) RDW 19.2 (11.5 – 15.5 %) RCC 6.5 (3.5 - 5 x1012/L) Iron studies Transferrin Saturation 48% (15-45) Ferritin 250ug/l (30-300) What is differential diagnosis? Confirmation?
25 yr male with tiredness Case Study 4