Embed Size (px)
Citation preview
Implementing the Key Action Statements: AnAlgorithm and Explanation for Process of Care for theEvaluation, Diagnosis, Treatment, and Monitoring ofADHD in Children and Adolescents
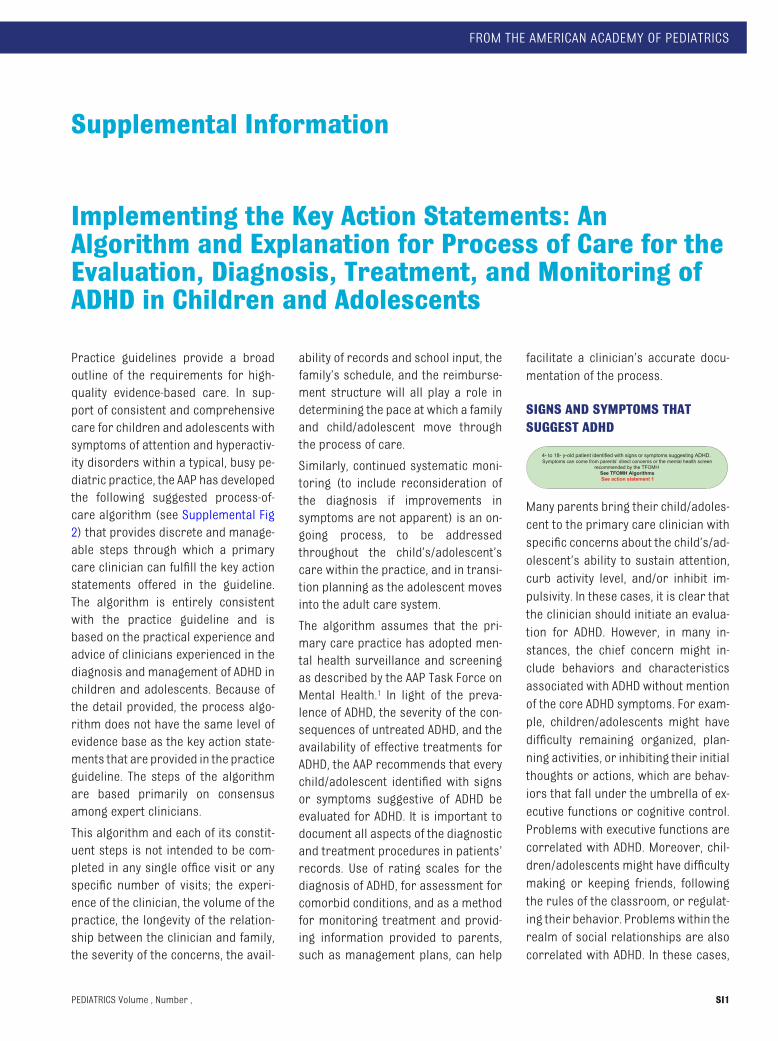
Practice guidelines provide a broadoutline of the requirements for high-quality evidence-based care. In sup-port of consistent and comprehensivecare for children and adolescents withsymptoms of attention and hyperactiv-ity disorders within a typical, busy pe-diatric practice, the AAP has developedthe following suggested process-of-care algorithm (see Supplemental Fig2) that provides discrete and manage-able steps through which a primarycare clinician can fulfill the key actionstatements offered in the guideline.The algorithm is entirely consistentwith the practice guideline and isbased on the practical experience andadvice of clinicians experienced in thediagnosis and management of ADHD inchildren and adolescents. Because ofthe detail provided, the process algo-rithm does not have the same level ofevidence base as the key action state-ments that are provided in the practiceguideline. The steps of the algorithmare based primarily on consensusamong expert clinicians.
This algorithm and each of its constit-uent steps is not intended to be com-pleted in any single office visit or anyspecific number of visits; the experi-ence of the clinician, the volume of thepractice, the longevity of the relation-ship between the clinician and family,the severity of the concerns, the avail-
ability of records and school input, thefamily’s schedule, and the reimburse-ment structure will all play a role indetermining the pace at which a familyand child/adolescent move throughthe process of care.
Similarly, continued systematic moni-toring (to include reconsideration ofthe diagnosis if improvements insymptoms are not apparent) is an on-going process, to be addressedthroughout the child’s/adolescent’scare within the practice, and in transi-tion planning as the adolescent movesinto the adult care system.
The algorithm assumes that the pri-mary care practice has adopted men-tal health surveillance and screeningas described by the AAP Task Force onMental Health.1 In light of the preva-lence of ADHD, the severity of the con-sequences of untreated ADHD, and theavailability of effective treatments forADHD, the AAP recommends that everychild/adolescent identified with signsor symptoms suggestive of ADHD beevaluated for ADHD. It is important todocument all aspects of the diagnosticand treatment procedures in patients’records. Use of rating scales for thediagnosis of ADHD, for assessment forcomorbid conditions, and as a methodfor monitoring treatment and provid-ing information provided to parents,such as management plans, can help
facilitate a clinician’s accurate docu-mentation of the process.
SIGNS AND SYMPTOMS THATSUGGEST ADHD
4- to 18- y-old patient identified with signs or symptoms suggesting ADHD. Symptoms can come from parents’ direct concerns or the mental health screen
recommended by the TFOMHSee TFOMH Algorithms See action statement 1
Many parents bring their child/adoles-cent to the primary care clinician withspecific concerns about the child’s/ad-olescent’s ability to sustain attention,curb activity level, and/or inhibit im-pulsivity. In these cases, it is clear thatthe clinician should initiate an evalua-tion for ADHD. However, in many in-stances, the chief concern might in-clude behaviors and characteristicsassociated with ADHD without mentionof the core ADHD symptoms. For exam-ple, children/adolescents might havedifficulty remaining organized, plan-ning activities, or inhibiting their initialthoughts or actions, which are behav-iors that fall under the umbrella of ex-ecutive functions or cognitive control.Problems with executive functions arecorrelated with ADHD. Moreover, chil-dren/adolescents might have difficultymaking or keeping friends, followingthe rules of the classroom, or regulat-ing their behavior. Problemswithin therealm of social relationships are alsocorrelated with ADHD. In these cases,
FROM THE AMERICAN ACADEMY OF PEDIATRICS
Supplemental Information
PEDIATRICS Volume , Number , SI1
Assess impact on treatment plan
Further evaluation/referral as needed
Exit this guideline.Evaluate or refer, as
appropriate.Iden�fy the child as
CYSHCN if appropriate.
Inattention and/or hyperactivity/impulsivity
problems not rising to DSM-IV diagnosisProvide educa�on of family and child
re: concerns (eg, triggers for ina�en�on or hyperac�vity) and behavior
management strategies or school-based strategies
Enhanced Surveillance
Coexisting disorders preclude primary care
management?
Follow-up and establish co-
management planSee TFOMH Algorithms
4- to 18- y-old patient identified with signs or symptoms suggesting ADHD. Symptoms can come from parents’ direct concerns or the mental health screen
recommended by the TFOMHSee TFOMH Algorithms See action statement 1
Yes
1
2
4
6 7
5
Overview of the ADHD Care Process
See action statement 3
Provide educa�on to family and child re: concerns (eg, triggers for
ina�en�on or hyperac�vity) and behavior-management strategies or
school-based strategies
Provide educa�on addressing concern (eg,
expecta�ons for a�en�on as a func�on of age)
Enhanced Surveillance
No
Yes
8
9
10
12
DSM-IVdiagnosis of
ADHD?
Legend = Start
= Continued care
= Decision
= Action/process
Yes
13
Op�on: Medica�on(ADHD only and past medical or family history of cardiovascular
disease considered) Ini�ate treatment
Titrate to maximum benefit, minimum adverse effectsMonitor target outcomes
Op�on: Behavior management (developmental varia�on,
problem or ADHD)
Iden�fy service or approach
Monitor target outcomes
Op�on: Collaborate with school to enhance supports
and services (developmental varia�on, problem, or ADHD)
Iden�fy changes
Monitor target outcomes
See action statement 5
See action statement 6
BEGIN TREATMENT
Coexisting conditions?
14
15
16Do
symptoms improve?
Reevaluate to confirm diagnosis and/or provide education to improve
adherence.
Reconsider treatment plan including changing of the medication or dose, adding a medication approved for
adjuvant therapy, and/or changing behavioral therapy.
Yes
No
Follow-up for chronic care
management at least 2x/year for
ADHD issues
3
Perform Diagnostic Evaluation for ADHD and Evaluate or Screen for Other/Coexisting Conditions:
Family(parents, guardian, other frequent caregivers):
Chief concerns
History of symptoms (eg, age of onset and course over �me)
Family history
Past medical history
Psychosocial history
Review of systems
Validated ADHD instrument
Evalua�on of coexis�ng condi�ons
Report of func�on, both strengths and weaknesses
School (and important community informants):
Concerns
Validated ADHD instrument
Evalua�on of coexis�ng condi�ons
Report on how well pa�ents func�on in academic, work, and social interac�ons
Academic records (eg, report cards, standardized tes�ng, psychoeduca�onal evalua�ons)
Administra�ve reports (eg, disciplinary ac�ons)
Child/adolescent (as appropriate for child’s age and developmental status):
Interview, including concerns regarding behavior, family rela�onships, peers, school
For adolescents: validated self-report instrument of ADHD and coexis�ng condi�ons
Report of child’s self-iden�fied impression of func�on, both strengths and weaknesses
Clinician’s observa�ons of child’s behavior
Physical and neurologic examina�on
See action statements 2–3
No
Other condition?
Yes
No
Apparently typical or
developmental variation?
Yes
No
No
11
17
18
ESTABLISH MANAGEMENT TEAM
Identify child as CYSHCN
Establish team including
coordination plan
Collaborate with family, school,
and child to identify target
goals.
See action statement 4
SUPPLEMENTAL APPENDIX FIGURE 2ADHD process-of-care algorithm. TFOMH indicates Task Force on Mental Health; CYSHCN, child/youth with special health care needs.1
SI2 FROM THE AMERICAN ACADEMY OF PEDIATRICS
initiating the diagnostic evaluationmight be appropriate.
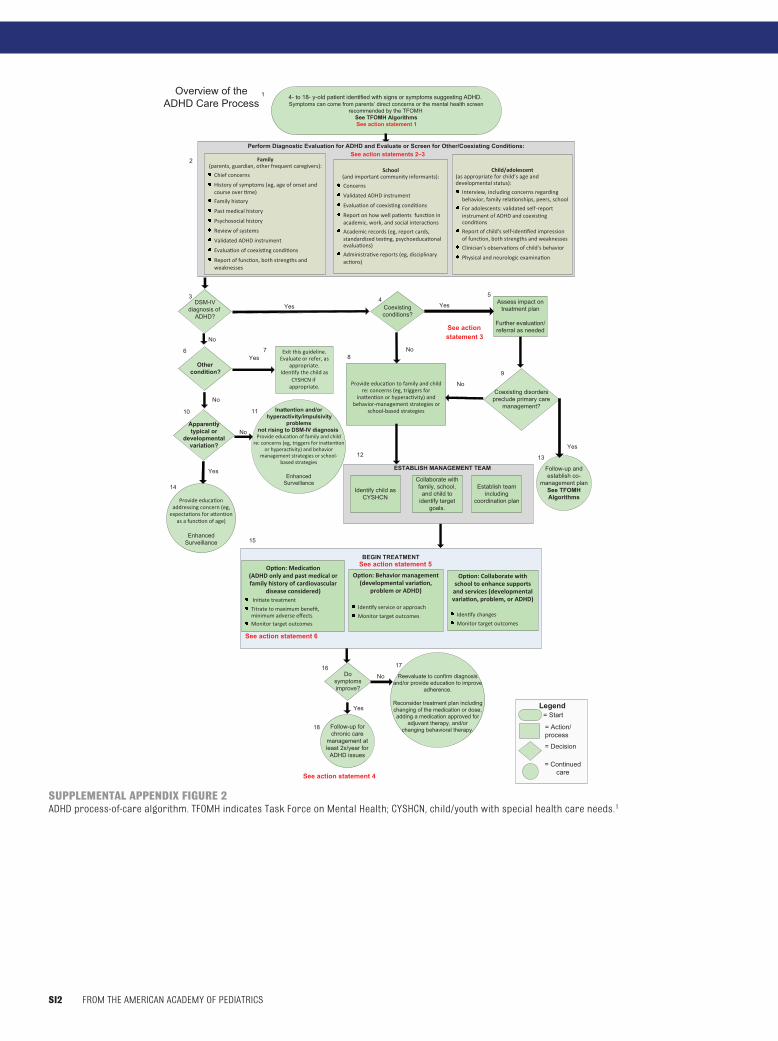
Perform Diagnostic Evaluation forADHD and Evaluate or Screen for
Coexisting Disorders
Ideally, the primary care office staffcan ask the assistance of the parent(s)in obtaining information on the pur-pose of a visit at the time of scheduling.If possible, an extended visit is oftendesirable for the evaluation of ADHD.As a general approach to the initialevaluation, data on the child’s/adoles-cent’s symptoms and functioning (eg,home or school questionnaires)should be gathered from parents,school personnel, and other sources,preferably before the visit. This strat-egy allows the primary care pediatri-cian to focus on pertinent issues forthat child/adolescent and family at thetime of the visit. Parental consent toauthorize the release of school data to
pediatric providers is important to ob-tain. The process might be facilitated ifthe family is given the responsibility toprovide other informants with thequestionnaires or data-collection
forms to be used and to request otherrecords and reports.
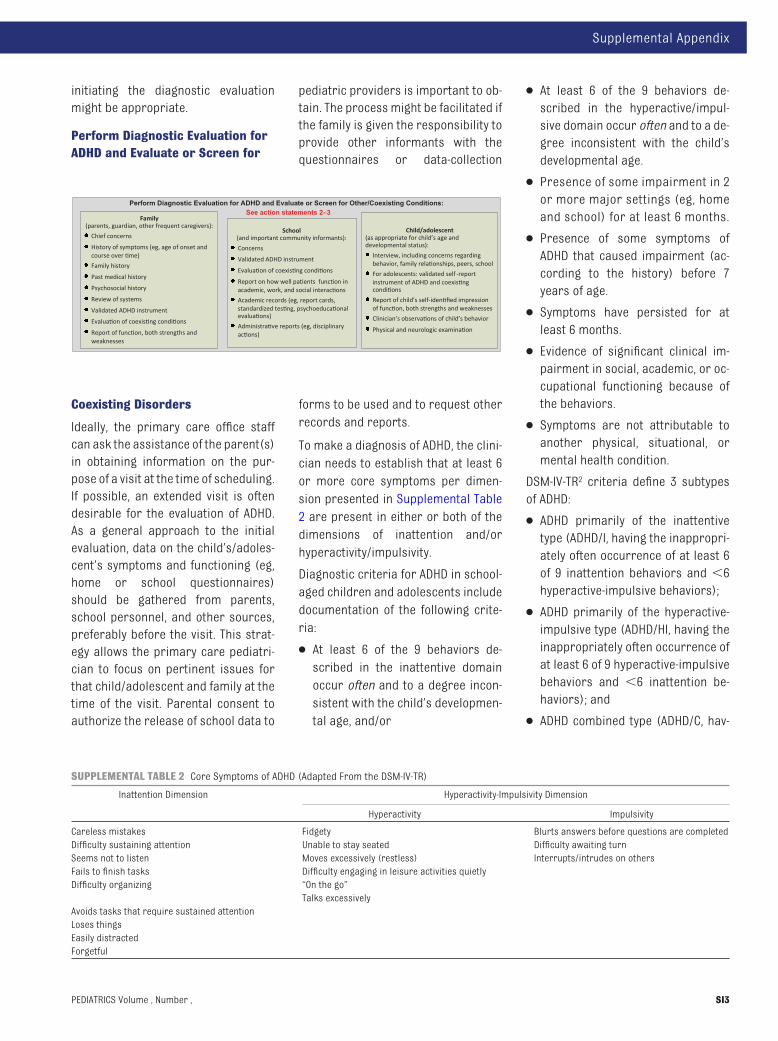
To make a diagnosis of ADHD, the clini-cian needs to establish that at least 6or more core symptoms per dimen-sion presented in Supplemental Table2 are present in either or both of thedimensions of inattention and/orhyperactivity/impulsivity.
Diagnostic criteria for ADHD in school-aged children and adolescents includedocumentation of the following crite-ria:
● At least 6 of the 9 behaviors de-scribed in the inattentive domainoccur often and to a degree incon-sistent with the child’s developmen-tal age, and/or
● At least 6 of the 9 behaviors de-scribed in the hyperactive/impul-sive domain occur often and to a de-gree inconsistent with the child’sdevelopmental age.
● Presence of some impairment in 2or more major settings (eg, homeand school) for at least 6 months.
● Presence of some symptoms ofADHD that caused impairment (ac-cording to the history) before 7years of age.
● Symptoms have persisted for atleast 6 months.
● Evidence of significant clinical im-pairment in social, academic, or oc-cupational functioning because ofthe behaviors.
● Symptoms are not attributable toanother physical, situational, ormental health condition.
DSM-IV-TR2 criteria define 3 subtypesof ADHD:
● ADHD primarily of the inattentivetype (ADHD/I, having the inappropri-ately often occurrence of at least 6of 9 inattention behaviors and �6hyperactive-impulsive behaviors);
● ADHD primarily of the hyperactive-impulsive type (ADHD/HI, having theinappropriately often occurrence ofat least 6 of 9 hyperactive-impulsivebehaviors and �6 inattention be-haviors); and
● ADHD combined type (ADHD/C, hav-
Perform Diagnostic Evaluation for ADHD and Evaluate or Screen for Other/Coexisting Conditions:
Family(parents, guardian, other frequent caregivers):
Chief concerns
History of symptoms (eg, age of onset and course over �me)
Family history
Past medical history
Psychosocial history
Review of systems
Validated ADHD instrument
Evalua�on of coexis�ng condi�ons
Report of func�on, both strengths and weaknesses
School (and important community informants):
Concerns
Validated ADHD instrument
Evalua�on of coexis�ng condi�ons
Report on how well pa�ents func�on in academic, work, and social interac�ons
Academic records (eg, report cards, standardized tes�ng, psychoeduca�onal evalua�ons)
Administra�ve reports (eg, disciplinary ac�ons)
Child/adolescent (as appropriate for child’s age and developmental status):
Interview, including concerns regarding behavior, family rela�onships, peers, school
For adolescents: validated self -report instrument of ADHD and coexis�ng condi�ons
Report of child’s self-iden�fied impression of func�on, both strengths and weaknesses
Clinician’s observa�ons of child’s behavior
Physical and neurologic examina�on
See action statements 2–3
SUPPLEMENTAL TABLE 2 Core Symptoms of ADHD (Adapted From the DSM-IV-TR)
Inattention Dimension Hyperactivity-Impulsivity Dimension
Hyperactivity Impulsivity
Careless mistakes Fidgety Blurts answers before questions are completedDifficulty sustaining attention Unable to stay seated Difficulty awaiting turnSeems not to listen Moves excessively (restless) Interrupts/intrudes on othersFails to finish tasks Difficulty engaging in leisure activities quietlyDifficulty organizing “On the go”
Talks excessivelyAvoids tasks that require sustained attentionLoses thingsEasily distractedForgetful
Supplemental Appendix
PEDIATRICS Volume , Number , SI3

ing the inappropriately often occur-rence of at least 6 of 9 behaviors inboth the inattention andhyperactive-impulsive dimensions).
There is also evidence that the criteriaare appropriate for preschool-agedchildren3 and adolescents.4 The use ofspecific DSM-IV-TR criteria decreasesvariation among clinicians in how thediagnosis is made and will facilitatecommunication among professionalsand patients.
DSM-IV-TR criteria require evidence ofimpairing symptoms before 7 years ofage. In some cases, the symptoms ofADHD might not be recognized by par-ents or teachers until the child is olderthan 7 years, when school tasks be-comemore challenging. In children forwhom the problems are identified af-ter 7 years of age, history can oftenidentify an earlier age of onset of someof the symptoms. Delayed recognitionmight be seen more often in the inat-tentive subtype of ADHD.5
If symptoms arise suddenly, withoutprevious history, primary care clini-cians should consider other condi-tions including head trauma, physicalor sexual abuse, neurodegenerativedisorders, mood or anxiety disorders,substance abuse, or a major psycho-logical stress in the family or school.
The requirements that a child musthave significant impairment in func-tion and some impairment in at least 2settings are the most challenging as-pects of the DSM-IV-TR criteria for theclinician to obtain accurate informa-tion. The presence of functional im-pairments is often the most troublingissue for children, families, and teach-ers and is a central requirement inmaking the diagnosis of ADHD6 (alsosee Behavior Management”).
As was determined in the previousguideline, parent and teacher ratingscales that use DSM-IV-TR criteria forADHD are helpful in obtaining the infor-
mation required to make a diagnosison the basis of the DSM-IV-TR criteria.Broad-band rating scales that assessmental health functioning in generaldo not provide reliable and valid indi-cations of ADHD diagnoses but mighthelp in screening for co-occurring be-havioral conditions.7
No current instruments routinely usedin primary care practice reliably as-sess the nature or degree of functionalimpairment in children with ADHD, al-though parent-report instrumentsmight help. Some measures that areavailable are limited, because theymostly provide only a global rating (eg,the Strengths and Difficulties Ques-tionnaire [SDQ] Impact Scale8 and theChildren’s Global Assessment Scale[CGAS]9) or have more limited valida-tion (eg, the performance componentof the Vanderbilt Scales10,11). Review ofdocuments, such as report cards andresults of standardized testing, and ev-idence of detention, suspensions, orexpulsions from school can also serveas evidence of functional impairment.With information obtained from theparent and school, the clinician willneed to make a clinical judgmentabout the effect of the core and asso-ciated symptoms of ADHD on academicachievement, classroom performance,family and social relationships, inde-pendent functioning and safety/acci-dental injuries, self-perception, leisureactivities, and self-care (such as bath-ing, toileting, dressing, and eating). Ad-ditional guidance regarding functionalassessment is available through theAAP ADHD toolkit and the Task Force onMental Health.15,16
In the absence of other concerns andfindings on medical history, family andsocial history, and physical examina-tion of the child, no further diagnostictestingwill help to reach the diagnosis.Compared with clinical interviews,standardized psychological tests, suchas computerized tests of attention,
have not been found to reliably differ-entiate between youth with and with-out ADHD.14,15 Appropriate further as-sessment is indicated if an underlyingetiology is suspected. Assessmentssuch as screening for high lead levels,low iron or ferritin levels or abnormalthyroid hormone levels or imagingstudies should be pursued only if otherhistoric or physical information sug-gests their presence. Conditions suchas sleep disorders, such as apnea, ab-sence seizures, hyperthyroidism, ormood or anxiety disorders might pres-ent with ADHD symptoms and might berelieved when the primary condition istreated.
Current criteria do not describe gen-der or developmental differences, al-though numerous studies have foundthat the frequency of symptomatic be-haviors varies significantly acrossgender and age groups (for a review,see Barkley16). Compared with othergirls, girls with ADHD experience moredepression, anxiety, distress, poorteacher relationships, stress, externallocus of control, and impaired aca-demics. Compared with boys withADHD, girls with ADHD experiencemore impairment in self-reported anx-iety, distress, depression, and externallocus of control. Furthermore, the be-havioral characteristics specified inthe DSM-IV-TR, despite efforts to stan-dardize them, remain subjective, to agreat extent, and may be interpreteddifferently by different observers. Cul-tural norms and expectations of par-ents or teachers may influence theperspectives of various informants.The rates of ADHD and its treatmenthave been found to be different fordifferent racial/ethnic groups.17,18 Theclinician must remain sensitive to cul-tural differences in the appropriate-ness of behaviors and perceptions ofmental health conditions. Other fac-tors, such as poverty and access tocare, likely contribute to the cultural
SI4 FROM THE AMERICAN ACADEMY OF PEDIATRICS

differences. These complexities in thediagnosis mean that clinicians whouse DSM-IV-TR criteria must applythem in the context of sound clinicaljudgment.
The DSM-IV-TR does include a categoryof “ADHD not otherwise specified.” Thiscategory is meant for children whomeet many but not the full criteria forADHD, such as children who meet allthe symptom and impairment criteriabut whose age of onset is later than 7years or children who have clinicallysignificant impairment but do notmeet all the symptom requirements.Clinically significant impairment is re-quired in diagnosing a child with ADHD.Children with inattentive or hyperac-tive/impulsive symptoms but less thansignificant impairment are character-ized as having “problems.”
FAMILY
A comprehensive diagnostic evalua-tion typically begins with identifyingthe family’s chief concerns. The clini-cian also needs to have the familymembers complete a validated ADHDinstrument. Family members shouldbe asked to provide a history of signsand symptoms. This history includesdetermining the onset, frequency, andduration of problem behaviors, situa-tions in which they increase or de-crease, previous treatments and theirresults, and the family’s understand-ing of the issues. The family historyshould include any medical syn-dromes, developmental delays, cogni-tive limitations, learning disorders, ormental illness in family members, in-cluding ADHD and mood, anxiety, andbipolar disorders. In addition, parentaltobacco and substance use is relevantto risk factors for ADHD.17 Family mem-bers might not have been formally di-agnosed with ADHD; asking about fam-ily members’ school experience andproblems similar to those of the pa-
tient might suggest undiagnosedcases of ADHD.
Updating the medical history can fo-cus on factors associated with ADHD,such as preterm delivery, neonatalproblems, congenital infections, andhead trauma. The psychosocial his-tory should include environmental fac-tors, such as family stress and prob-lematic relationships that mightcontribute to the child’s/adolescent’soverall functioning.
It is important to obtain history of con-ditions that might mimic ADHD symp-toms or might co-occur with the condi-tion. Co-occurring conditions arediscussed later in the process algo-rithm. Several available question-naires also provide a screen for coex-isting conditions and a report offunction. It is important to obtain ahistory that would suggest lead expo-sure, absence seizures, or other men-tal illnesses such as anxiety or mooddisorders and Tourette disorder. A fullreview of systems might also revealother symptoms, such as sleep distur-bances, that may assist in formulatinga differential diagnosis and/or may beconsidered in the development of man-agement plans. The patient should alsobe screened for hearing and/or visualproblems.
Primary sleep disorders, such as ob-structive sleep apnea syndrome andrestless-leg syndrome/periodic limb-movement disorder, might presentwith symptoms of inattention, hyper-activity, and impulsivity or are fre-quently associated with ADHD.18–21 Allchildren being evaluated for ADHDshould be systematically screened forsymptoms of (ie, frequent snoring, ob-served breathing pauses; restlesssleep, urge to move their legs at night;daytime sleepiness) and risk factorsfor (ie, adenotonsillar hypertrophy,asthma/allergies, obesity; family his-tory of restless-leg syndrome/periodiclimb-movement disorder, iron defi-
ciency) primary sleep disorders.22
Sleep-assessment measures that havebeen shown to be useful in the pediat-ric primary care practice setting in-clude brief screening tools25 andparent-report surveys.26,27 Overnightpolysomnography should be stronglyconsidered for children with symp-toms suggestive of and/or risk factorsfor obstructive sleep apnea syndromeand restless-leg syndrome/periodiclimb-movement disorder.28
In addition, even in the absence of pri-mary sleep disorders, modest reduc-tions in sleep duration, such as thoseassociated with environmentally re-lated insufficient sleep, might be asso-ciated with detectable deterioration invigilance and attention in childrenwithADHD and should be evaluated and ad-dressed.29 Common clinical presenta-tions of insomnia in children withADHD include bedtime resistance, de-layed sleep onset, night wakings, andearly-morning awakening. Both a base-line assessment (ie, before initiatingtreatment) and ongoing periodicscreening for sleep problems shouldbe included in the management of allchildren with ADHD. Sleep diaries areuseful adjuncts in quantifying sleep-onset latency and night wakings andassessing variability in sleep pat-terns.30 The differential diagnosis of in-somnia in childrenwith ADHD includes:
● ADHD medication (stimulant andnonstimulant) effects:
● Direct effects on sleep architec-ture (ie, prolonged sleep-onset la-tency and decreased sleep dura-tion, increased night wakings)31–
33; and
● Indirect effects such as inade-quate control of ADHD symptomsin the evening and medicationwithdrawal or reboundsymptoms.23,34
● Sleep problems associated with co-existing psychiatric conditions (ie,
Supplemental Appendix
PEDIATRICS Volume , Number , SI5

anxiety andmood disorders, disrup-tive behavior disorders).34,35
● Circadian-based phase delay insleep-wake patterns, which havebeen shown to occur in some chil-dren with ADHD, which results inboth prolonged sleep onset and dif-ficulty waking in the morning.36
● Inadequate sleep hygiene (ie, incon-sistent bedtimes and wake times,absence of a bedtime routine, elec-tronics in the bedroom, caffeineuse).37
● Intrinsic deficit associated withADHD. Numerous studies have foundthat nonmedicated children withADHD and no comorbidmood or anx-iety disorders have significantlygreater bedtime resistance, moresleep-onset difficulties, and morefrequent night awakenings whencompared with typically developingcontrol children.38 In addition, somechildren with ADHD seem to have ev-idence of increased daytime sleepi-ness even in the absence of a pri-mary sleep disorder.39,40
A sound assessment of functioning inmajor areas can then be used to con-struct an educational and behavioralprofile including not only concerns butalso strengths or talents. The mostcommon areas of functioning affectedby ADHD include academic achieve-ment; peer, parent, sibling, and adultauthority-figure relationships; partici-pation in recreation such as sports;and behavior and emotional regula-tion, including risky behavior. One sys-tematic approach to the assessment offunction can use the framework of theInternational Classification of Func-tioning, Disability, and Health.6,41
Suggestions and recommendationsfor scales such as the modified PatientHealth Questionnaire-9 Modified forAdolescents (PHQ-A)42 and Screen forChild Anxiety Related Emotional Disor-ders (SCARED)43 have been developed
by the AAP Task Force on MentalHealth.13 The situation might be morecomplicated when parents disagree,particularly in divorce situations whenparents with shared custody perceivethe child’s problems and strengths dif-ferently. Under such circumstances,the clinician must use communicationskills to find a consensus on the diag-nosis and plan. Eliciting informationfrom extended family members mighthelp clarify some of the differences.
SCHOOL AND/OR OTHERCOMMUNITY INFORMANTS
Multiple informants are required forclinicians to determine the natureand severity of symptoms, impact ofthe symptoms on function in 2 ormore settings, and whether thechild/adolescent meets DSM-IV-TRcriteria for the diagnosis of ADHD. Inmost cases, the teacher providesthose reports. The reports of parentsand teachers are often sufficient forthe ADHD diagnosis, but informationfrom the patient is essential for iden-tifying the internalizing conditions ofmood and anxiety disorders. Ratingscales recommended by the TaskForce on Mental Health may be help-ful. In some circumstances, it mightbe desirable to solicit informationfrom additional sources. School re-ports, for example, might be moredifficult to obtain—or less compre-hensive—in cases that involvepreschool-aged children and adoles-cents. Other adults who are active inthe life of an adolescent, such ascoaches, pastors, or scout leaders,can be asked to complete ratingscales to develop a full profile of theadolescent, although the accuracy oftheir reporting has not been studied
Teachers might indicate their majorconcerns by using questionnairesor verbal input by telephone orthrough direct conversation. An ap-propriate school representative
should be asked to complete a vali-dated ADHD instrument or behav-ior scale based on DSM-IV-TR criteriafor ADHD and provide observationsthat might suggest coexisting or al-ternative conditions, including dis-ruptive behavior disorders, depres-sion and anxiety disorders, tics, orlearning disabilities. Report offunction, both strengths and weak-nesses, might be gleaned by ques-tionnaires or academic recordsthat can include report cards; stan-dardized testing in reading, mathe-matics, and written expression; vali-dated functional assessment toolsmentioned previously44; and previ-ous psychoeducational evaluations.These records can help establish achild’s/adolescent’s profile of aca-demic and behavioral performancein school, the presence of a learningdisability, difficulty in followingschool rules, the quality of peer in-teractions, and the extent of schoolabsences.
If the records indicate that the childis having difficulty learning aca-demic skills, the physician should de-termine if the child has been as-sessed for a potential learningproblem by the school, becausethere is a high comorbidity betweenlearning disabilities and ADHD. Theschool assessment might use aresponse-to-intervention model aspart of the diagnostic process inwhich learning problems are evalu-ated on the basis of the child’s re-sponse to evidence-based academicinterventions, or a multidisciplinaryteam evaluation might be conductedby the school. If the child has an Indi-vidualized Education Program, thisdocument should be reviewed by theclinician.
If the child continues to struggle de-spite the school’s interventions andtreatment for ADHD, further psychoe-ducational or neuropsychological as-
SI6 FROM THE AMERICAN ACADEMY OF PEDIATRICS

sessment is necessary. The clinicianmight want to recommend that theevaluations be performed by an inde-pendent psychologist or neuropsy-chologist. Despite the importance ofthe psychological assessments, in-surance coverage is quite variable,and families should be encouragedto investigate their coverage whenpursuing independent psychologicalevaluations. Financing community-based evaluations has been ad-dressed in a previous AAP state-ment.45 Children with intellectual orother developmental disabilitiesmight also have ADHD, but the as-sessment in these cases is morecomplicated, because one must en-sure that the academic expectationsare matched to the child’s academicabilities and the level of ADHD symp-toms exceeds what would be ex-pected for a child’s developmentallevel. Primary care physicians in-volved in assessing ADHD in childrenwith intellectual disabilities willneed to collaborate closely with aschool psychologist or independentpsychologist.
In addition to the academic informa-tion, information should be re-quested that characterizes thechild’s/adolescent’s level of func-tioning with regards to peer,teacher, and other authority figurerelationships; ability to follow direc-tions; organizational skills; history ofclassroom disruption; and assign-ment completion. Administrativereports of disciplinary action, suchas suspensions and expulsions, anddescriptions of behavior at schoolreflect social function and behav-ioral regulation and suggest the pos-sibility of coexisting conditions.
For adolescents who have multipleteachers, it is desirable to obtain be-havior and impairment ratings from atleast 2 teachers in academic subjects(eg, math and English teachers or, for
children/adolescents with learningdisabilities, a teacher in the area ofstrong function and a teacher in thearea of weak function). The ADHD tool-kit13 providesmaterials relevant to thisschool data collection.
Teacher and parent reports frequentlydisagree,46 and there alsomight be dis-agreement between parents. These ob-servations might not be inaccurate,because parents and teachers ob-serve the children under different cir-cumstances. When there is disagree-ment, it is helpful to obtain moreinformation such as the circumstanceunder which the individuals observedthe child, the demands on the childduring those observations, the observ-ers’ understanding of the behaviorsand how to deal with them, and the ob-servers’ understanding of ADHD andhow it is treated as well as the rolethey play with the child. As noted pre-viously, obtaining information from ad-ditional sources, such as grandpar-ents, coaches, or Sunday schoolteachers, can be helpful. The clini-cian’s decision about the diagnosis is aclinical judgment made on the basis ofall the information that is available.
CHILD/ADOLESCENT
The clinician should conduct an age-appropriate interview, including thechild’s/adolescent’s concern regardinghis or her own behavior, and regardingfamily relationships, peers, andschool. Itis important to include a discussion ofhis or her strengths, goals, and difficul-ties. Along with the interview, the use ofan appropriate validated self-reportinstrument of ADHD and co-existingconditions, primarily for adolescents,canaid in theassessmentof riskof ADHDand anxiety and mood disorders. It isalso important to ask about delusionalthinking and suicidal thoughts or ac-tions. This evaluation should also pro-vide a baseline of the child’s/adoles-cent’s self-identified report of function
at home, in school, at work, and amongpeers as well as validated functional as-sessment tools.44 Whenever possible, theindividual child’s or youth’s own view ofwhat heor shewould like to see changedshould be considered primary targetsfor intervention, because these goalsmight at times differ widely from parentor school concerns.
The clinician must keep in mind thetendency of many children/adoles-cents to underreport their ADHD andother disruptive behavior symptoms.However, the baseline impressions ofthe child/adolescent can then be usedas the basis for shaping the patient’sunderstanding of ADHD and coexistingsymptoms as well as monitoring func-tion in social, behavioral, and aca-demic domains. Active involvement ofthe children/adolescents might beuseful to empower them to under-stand and participate in their own di-agnostic formulation and, later, to ob-tain “buy in” to their treatment planand improve adherence to treatment.Recommendations of the AAP TaskForce on Mental Health and the Guide-lines for Adolescent Depression in Pri-mary Care (GLAD-PC)47,48 include usingvalidated diagnostic rating scales foradolescent mood and anxiety disor-ders for clinicians whowish to use thisformat. In addition, the CRAFFT (car, re-lax, alone, forget, friends, trouble) isan available screen for substanceabuse.49
Clinical observations of the patientshould be recorded and include his orher level of attention, activity, and im-pulsivity during the encounter. An im-portant caveat is that the findings seenin other settings, including core symp-toms, are often not observed duringoffice visits.50
Special attention should be paid to lan-guage skills in preschool-aged andyoung school-aged children, becausedifficulties with language can be asymptom of a language disorder and
Supplemental Appendix
PEDIATRICS Volume , Number , SI7
predictor of subsequent reading prob-lems; such language disorders mightpresent as problems with attentionand impulsivity. Likewise, social inter-actions should be noted during the ex-amination, because they are anotherpossible area of deficiency.
The physical and neurologic exami-nation must be comprehensive. Aphysical and neurologic examinationshould be conducted to determine iffurther medical or developmental as-sessments are indicated. Baselineheight, weight, blood pressure, andpulse measurements should be taken.Among the signs to note are hearingand visual acuity and cardiovascularstatus. Dysmorphic features shouldalso be noted, because ADHD might beassociated with genetic syndromes(eg, fetal alcohol syndrome and fragileX). The neurologic evaluation shouldinclude developmental andmental sta-tus observations including affect; com-munication skills, including speechand language; tics; and gross and finemotor coordination. Many childrenwith ADHD will have poor coordination,which might be severe enough to war-rant a diagnosis of developmental co-ordination disorder. The findings canaffect how well the child can performin competitive sports and can also ad-versely affect his or her writing skills.Through history and examination ofthe child’s fine and gross motor skills,the clinician can identify these deficitsand address them in the managementplan.
DSM-IVdiagnosis of
ADHD?
As a result of the diagnostic evalua-tion, a primary care clinician should beable to answer the following ques-tions:
● How many inattentive and hyperac-tive/impulsive behavior criteria forADHD does the child/adolescent
meet across the major settings ofhis or her life?
● Have these criteria been present for6 months or longer?
● Was the onset of these or similarbehaviors present before the age of7 years?
● What functional impairments, if any,are caused by these behaviors?
● Could any other condition be a bet-ter explanation for the behaviors?
● Is there evidence of coexisting prob-lems or disorders?
On the basis of this information, theclinician should be able to arrive at apreliminary diagnosis.
OTHER DISORDERS
If symptoms arise suddenly, with-out any previous history, primarycare clinicians should considerother conditions, including headtrauma, physical or sexual abuse,neurodegenerative disorders,mood and anxiety disorders, sub-stance abuse, or a major psycho-logical stress in the family or inschool, such as bullying.
Exit this guideline.Evaluate or refer, as
appropriate.
appropriate.
Iden�fy the child as CYSHCN if
YesOther
condition?
If the evaluation identifies or sug-gests that another disorder is thecause of the concerning signs andsymptoms, then it is appropriate toexit this algorithm. The approach inthat case is dictated by the results ofthe evaluation. If a referral is made,the primary care clinician shouldframe the referral questions clearlyand expect these referral questionsto be answered in a manner that willensure that a comanagement planthat addresses the families’ andchild’s/adolescent’s ongoing needsfor education and general and spe-cialty health care is established. Re-
sources from the AAP Task Force onMental Health might be helpful.
TYPICAL OR DEVELOPMENTALVARIATION:
Provide educa�on addressing concern (eg,
expecta�ons for a�en�on as a func�on of age)
Enhanced Surveillance
Apparently typical or
developmental variation?
Yes
Evaluation might reveal that thechild’s/adolescent’s inattention, ac-tivity level, and impulsivity are withinthe normal range of development;mildly or inconsistently elevated incomparison to peers; or not associ-ated with any functional impairmentin behavior, academics, social skills,or other domains. It is important forthe clinician to probe further to de-termine if the parental concerns re-garding the child/adolescent are at-tributable to other issues in thefamily, such as parental tension ordrug abuse in another family mem-ber; whether they are caused byother issues in school, such as socialpressures or bullying; or whetherthey are within the spectrum of typi-cal development. Parent educationabout contributions to their con-cerns and to the spectrum of devel-opmental variation might be helpful.Education about the range of typicaldevelopment and strategies for im-proving a child’s/adolescent’s be-haviors when they are problematicmight be helpful. A schedule of en-hanced surveillance absolves thefamily of the need to reinitiate con-tact if the situation deteriorates. If arecommendation for continued rou-tine systematic surveillance is made,then assurance that ongoing con-
SI8 FROM THE AMERICAN ACADEMY OF PEDIATRICS
cerns can be revisited in future pri-mary care visits would be important.
INATTENTION, HYPERACTIVITY, AND/OR IMPULSIVITY (PROBLEM LEVEL):
Children/adolescents whose symptomsdo not meet the criteria for diagnosis ofADHDmight still encounter difficulties orimpairment in some settings, as de-scribed in the DSM-PC Child and Adoles-cent Version.51
Professional consensus is that medica-tion is not an appropriate treatment forchildren/adolescents with inattention,hyperactivity, and/or impulsivity prob-lems that do not meet the DSM-IV-TR cri-teria for ADHD. Children/adolescentswith these problems and their familiesmight benefit from education, includingidentifying and eliminating triggers thatprompt inattention, hyperactivity, or im-
pulsivity; behavior-management options,including a behavior-therapy or parent-ing program; strategies for improvingschoolperformanceorbehavior; and therecommendations provided in the inat-tention and hyperactivity/impulsivitycluster guidance in the Task Force onMental Health ADHD toolkit.13
ATTENTION-DEFICIT/HYPERACTIVITYDISORDER:
If the child/adolescent is found to meetthe DSM-IV-TR criteria for ADHD, includ-ing commensurate functional disabili-ties, suchdiagnosis shouldbemade, andprogress through theprocess-of-careal-gorithm continues as shown.
Provide Education to the Family andChild/Adolescent
Education for the family and child/adolescent about ADHD is an impor-tant element in the care plan whenADHD is diagnosed or inattention, hy-peractivity, and/or impulsivity (prob-lem level) is identified. Family educa-tion continues throughout thecourse of treatment. It includes an-ticipatory guidance in such areas astransitions (eg, from elementary tomiddle and middle to high schoolsand from high school to college oremployment) and working withschools and developmental chal-lenges that might be affected byADHD, including driving, gender, anddrugs.
Family education includes all mem-bers of the family, including develop-mentally age-appropriate informationfor the affected child/adolescent andany siblings. Topics include the disor-der; the symptoms; the assessmentprocess; commonly coexisting disor-ders; treatment choices and their ap-plication, likely effects, and outcomes;long-term implications; impact onschool performance; and socialparticipation.
A critical piece of the treatment planis to empower children/adolescentsto understand their condition andthe degree of impairment that it hason their daily life, including strate-gies for addressing symptoms andimpairments. At every stage, this ed-ucation must continue in a mannerconsistent with the child’s/adoles-cent’s own level of understanding. Inaddition, it is helpful for a child/ado-lescent with ADHD to know the nameof any medication that he or she willbe using as well as common adverseeffects.
The issue of how the patient thinks ofhimself or herself is another area toaddress; it should be clarified thatthe condition does not mean that he
Inattention and/or hyperactivity/impulsivity
problems not rising to DSM-IV DiagnosisProvide educa�on of family and child
re: concerns (eg, triggers for ina�en�on or hyperac�vity) and behavior
management strategies or schoolbased strategies
Enhanced Surveillance
Apparently typical or
developmental variation?
No
Provide educa�on to family and child re: concerns (eg, triggers for
ina�en�on or hyperac�vity) and behavior-management strategies or
based strategies
DSM-IVdiagnosis of
ADHD?Coexisting conditions?
No
Yes
Supplemental Appendix
PEDIATRICS Volume , Number , SI9
or she is less smart than other chil-dren/adolescents. It can also behelpful to identify and support areasof strength and help the child/ado-lescent with ADHD to learn how toidentify when he or she needs helpand how to procure it.
Education for parents should includeproactive strategies that can helpmake the home environment morefacilitative for their child/adolescentwith ADHD. For example, making ad-aptations and providing structurethat enables the child/adolescent tobest use his or her strengths andcompensate for deficits can be help-ful to parents. Such strategies in-clude providing greater consistencyin the parents’ behavior toward theirchild/adolescent with ADHD, formingdaily routines and schedules, anddisplaying house rules in prominentplaces as visual reminders. It mayhelp parents to communicate abouttheir child’s/adolescent’s behaviorand each parent’s response as wellas the parental division of labor. It isalso important to check on the par-ents’ well-being, because parents ofchildren/adolescents with ADHD fre-quently are under stress and mightnot take into consideration their ownwell-being or that of other familymembers. These concerns are par-ticularly relevant when a parent alsohas ADHD or associated conditions.
Parents will likely benefit if they learnabout optimal ways to partner withschools such that teachers can be-come part of the educational and inter-vention teams. Parents will benefitfrom being informed about school ser-vices that are available to addresstheir child’s/adolescent’s needs, in-cluding the Individuals With Disabili-ties Education Act (IDEA) and the Reha-bilitation Act (504) services providedby their state, and the eligibility re-quirements for them. With a parent’spermission, the clinician can provide
the school with information from theevaluation that will help the school de-termine eligibility for special educa-tion services and develop appropriateadaptations. Advocacy and supportgroups such as CHADD (Children andAdults With Attention-Deficit/Hyperac-tivity Disorder) can also provide infor-mation and support to families.
The ADHD toolkit13 provides lists of ed-ucational resources including Web-based resources, organizations, andbooks that might be useful to parentsand students.
COEXISTING CONDITIONS:
If other disorders are suspected or de-tected during the diagnostic evalua-tion, an assessment of the urgency ofthese conditions and their impact onthe ADHD treatment plan needs to bemade.
Urgent conditions, such as suicidalthoughts or acts or other behaviorswith the potential to severely injurethe child/adolescent or other peo-ple, such as severe temper out-bursts or child abuse, should be ad-dressed immediately with servicescapable of handling crisissituations.
The evidence shows that coexistingconditions, such as oppositionality andanxiety, might improve with treatment
of ADHD.51 For example, children withADHD and coexisting anxiety disordersmight find that ADHD medications de-crease anxiety symptoms as well asADHD behaviors. In the cases of severelearning disorders or oppositional de-fiant disorder, a trial of treatment forADHD might indicate whether the ap-parent coexisting condition can bemodulated with treatment of the ADHD.Other patients might require addi-tional therapeutic treatments, such ascognitive behavioral therapy or a dif-ferent or additional medication, to ad-equately treat the ADHD and coexistingcondition.
Untreated substance use disorderneeds to be addressed first beforefully addressing the patient’s ADHDtreatments.
If the primary care clinician requiresthe advice of another subspecialist,then the clinician should considercarefully when to initiate treatment forADHD. In some cases, it might be advis-able to delay the start of medicationuntil the role of each member of thetreatment team is established. For ex-ample, with some coexisting psychiat-ric disorders, such as severe anxiety,depression, and bipolar disorder, a co-managing developmental behavioralpediatrician or psychiatrist might take
Assess impact on treatment plan
Further evaluation/referral as needed
Coexisting disorders preclude primary care
Follow-up and establish co-
management planSee TFOMH Algorithms
Yes
Provide educa�on to family and child re: concerns (eg, triggers for
ina�en�on or hyperac�vity) and behavior-management strategies or
No
Yes
DSM-IVdiagnosis of
ADHD?Coexisting conditions?
Yes
SI10 FROM THE AMERICAN ACADEMY OF PEDIATRICS
responsibility for treatment of boththe ADHD and the coexisting illness.
At other times, such as in the case of achild or adolescent with coexistingmild depression or obsessive-compulsive disorder, a mental healthclinician, developmental-behavioralpediatrician, neurodevelopmental dis-ability clinician, or child neurologistmay treat the coexisting conditionwhile the primary care clinician over-sees the treatment for ADHD, or theconsulting physician may advise theprimary care physician about thetreatment of the coexisting conditionto the extent that the primary care phy-sician is comfortable treating both theADHD and coexisting problems.
ESTABLISH MANAGEMENT TEAM
Identify child as CYSHCN
Establish team including
coordination plan
Collaborate with family, school,
and child to identify target
goals.
IDENTIFY AS A CHILD/YOUTH WITHSPECIAL HEALTH CARE NEEDS:
Any child who meets the criteria forADHD should be considered a child/youth with special health care needs.The AAP encourages clinicians to de-velop systems that ensure that themedical home needs of all children/youth with chronic illnesses are met.These needs—and strategies formeeting them—are discussed in fur-ther detail elsewhere in this guidelineand in other AAP resources such asThe Building Your Medical Home Tool-kit and Addressing Mental Health Con-cerns in Primary Care: A Clinician’sToolkit.43,53
Management Issues
Questions that are important to con-sider in developing a managementplan include the following:
● Does the family need further assis-tance in understanding the coresymptoms of ADHD and their child’s/adolescent’s target symptoms andcoexisting conditions?
● Does the family need support inlearning how to establish, measure,and monitor target goals?
● Have the family’s goals been identi-fied and addressed in the care plan?
● Does the family have an understand-ing of effective behavior-management techniques for re-sponding to tantrums, oppositionalbehavior, or poor compliance to re-quests and commands?
● Is help needed for normalizing peerand family relationships?
● Does the child/adolescent need helpin academic areas? If so, has a for-mal evaluation been performed andreviewed to distinguish work pro-duction problems secondary toADHD from coexisting learning orlanguage disabilities?
● Does the child/adolescent need helpin achieving independence in self-help or schoolwork production?
● Does the child/adolescent or familyrequire help with optimizing, orga-nizing, planning, or managingschoolwork flow?
● Does the family need help in recog-nition, understanding, or manage-ment of coexisting conditions?
● Is there a plan in place to systemat-ically educate the child/adolescentabout ADHD and its treatment aswell as the child’s/adolescent’s ownstrengths and weaknesses?
● Is there a plan in place to empowerthe child/adolescent with the knowl-edge and understanding that will in-crease his or her adherence totreatments, and has that begun asearly as possible and been ad-dressed at the child’s/adolescent’sdevelopmental level?
● Does the family have a copy of a careplan that summarizes findings andtreatment recommendations thatcan be updated and used in schoolsettings and other professional set-
tings so that the history and treat-ment plan does not need to be con-stantly reinvented?
● Is the follow-up plan sufficient toprovide comprehensive, coordi-nated, family-centered, culturallycompetent, ongoing care?
COLLABORATE WITH THE FAMILY,SCHOOL, AND CHILD/ADOLESCENT TOIDENTIFY TARGET GOALS:
Whereas an initial stimulant medica-tion trial might focus on normalizingcore symptoms of ADHD, a longer-termcomprehensive plan should focus onidentifying and addressing individual-ized and specific behavioral, academic,and social target goals and treat-ments. The clinician should assist par-ents, teachers, other informants, andthe child/adolescent in developing tar-get goals in the areas of function mostcommonly affected by ADHD: academ-ics; peer, parent, or sibling relation-ships; and safety in the community.Other goals might be identified by us-ing the International Classification ofFunction (ICF) analysis conducted inthe diagnostic phase of the clinicalpathway.6
It is not necessary to develop goals inevery area all at once. Families mightbe encouraged to identify up to 3 of themost impairing areas on which theywill initially work; parents and thechild/adolescent can then add othertargets as indicated by their relativeimportance. Such an exercisewill facil-itate greater understanding of the ef-fects of the disorder on each memberof the family and might lead to an im-proved collaboration in the develop-ment of a few specific and measurableoutcomes. It is helpful to incorporatethe child’s/adolescent’s strengths andresilient factors in considering targetgoals and in generating a treatmentplan. Goals for the school require inputfrom the teachers in terms of bothidentification and measurement.
Supplemental Appendix
PEDIATRICS Volume , Number , SI11

Establishing measurable goals in in-terpersonal domains and behavior inunstructured settings might be partic-ularly important. Whenever possible, itis important to make progress “count-able.” For behaviors such as “fre-quency of yelling” or frequency ofmissing assignments, charts may besuggested as strategies for recordingthe event so that parents, teachers, thechild/adolescent, and clinicians can allagree on howmuch progress has beenmade. In this way, successes can bebuilt on in a systematic way. Suchstrategies can help a family accuratelyassess and see progress of behaviorchanges. A daily single-page reportcard can be used to identify and moni-tor 4 or 5 behaviors that affect functionat school, and these reports can beshared with the parents. Other strate-gies and tools are available to clini-cians in the AAP ADHD toolkit13 and toparents in the book ADHD: What EveryParent Needs to Know.52
As treatment proceeds, in addition tousing a DSM-IV-TR–based ADHD ratingscale to monitor core symptomchanges, formal and informal queriescan be made in the areas of functionmost commonly affected by ADHD (eg,academic achievement; peer, parent,or sibling relationships; and safety inthe community). Progress can also bemonitored by determining progress onthe target goals. At every visit, it ishelpful to gradually empower chil-dren/adolescents to become full part-ners in their treatment plan by adoles-cence. Information from the school,including ADHD symptoms (ratingscale completed by the teacher),grades, and any other formal testingresults, are also helpful at these visits.
ESTABLISH TEAM ANDCOORDINATION PLAN:
It is best for the treatment team to in-clude everyone involved in the care ofthe child/adolescent: the child/adoles-
cent, parents, teachers, the primarycare clinician, therapists, subspecial-ists, and other adults (such as coachesor religious leaders) who will be ac-tively engaged in supporting and mon-itoring the treatment of ADHD. It ishelpful for the primary care clinicianor an assigned “care coordinator” toensure that each team member isaware of his or her role and that bothroutine and as-needed communicationstrategies and expectations for re-ports (frequency, scope) are clear. Col-laboration with the school goes be-yond the initial report of diagnosis andis best facilitated by agreement on astandardized, reliable system for ex-changing communications.
TREATMENT:
Medication
This treatment option is restricted tochildren/adolescents who meet the di-agnostic criteria for ADHD.
Although it is a rare occurrence55
and more evidence is required toidentify whether it is an increasedrisk, it is important to obtain acareful history of cardiac symp-toms; a cardiac family history, par-ticularly of arrhythmias, suddendeath, and death at a young agefrom cardiac conditions; and vitalsigns, cardiac physical examina-tion, and further evaluation on thebasis of clinical judgment.
Stimulant medications and severalnonstimulant medications are nowavailable, as outlined in SupplementalTable 3. The presence of a tic disordermight affect the decision about which
medication to initiate for ADHD ther-apy. With the greater availability ofmedications approved by the FDA forchildren/adolescents with ADHD, it hasbecome increasingly unlikely that clini-cians need to consider the off-label useof othermedications. The choice of for-mulation depends on factors such asthe efficacy of each agent for a givenchild/adolescent, the preferred lengthof coverage time, whether a child canswallow pills or capsules, and ex-pense. The extended-release formula-tions are generally more expensivethan the immediate-release formula-tions but might be preferred by manyfamilies and children/adolescents, be-cause they provide the benefits of con-sistent and sustained coverage withfewer administrations per day. Long-acting formulations usually precludethe need for school-based administra-tion of ADHD medication. Better cover-age with fewer administrations leadsto greater convenience for the familyand, therefore, might also lead to bet-ter adherence to the medication man-agement plan. Some patients, particu-larly some adolescents, might requiremore than 12 hours of coverage to en-sure adequate focus and concentra-tion during evening study time anddriving; in these cases, a short-actingpreparation might be used in additionto a long-acting preparation.
The ease with which preparations canbe administered and the minimizationof adverse effects are important forthe quality-of-life concerns that chil-dren, youth, and parents expressaround the decision to usemedication.
Op�on: Medica�on(ADHD only and past medical or family history of cardiovascular
disease considered) Ini�ate treatment
Titrate to maximum benefit, minimum adverse effectsMonitor target outcomes
Op�on: Behavior management (developmental varia�on,
problem or ADHD)
Iden�fy service or approach
Monitor target outcomes
Op�on: Collaborate with school to enhance supports
and services (developmental varia�on, problem, or ADHD)
Iden�fy changes
Monitor target outcomes
See action statement 5
See action statement 6
BEGIN TREATMENT
SI12 FROM THE AMERICAN ACADEMY OF PEDIATRICS
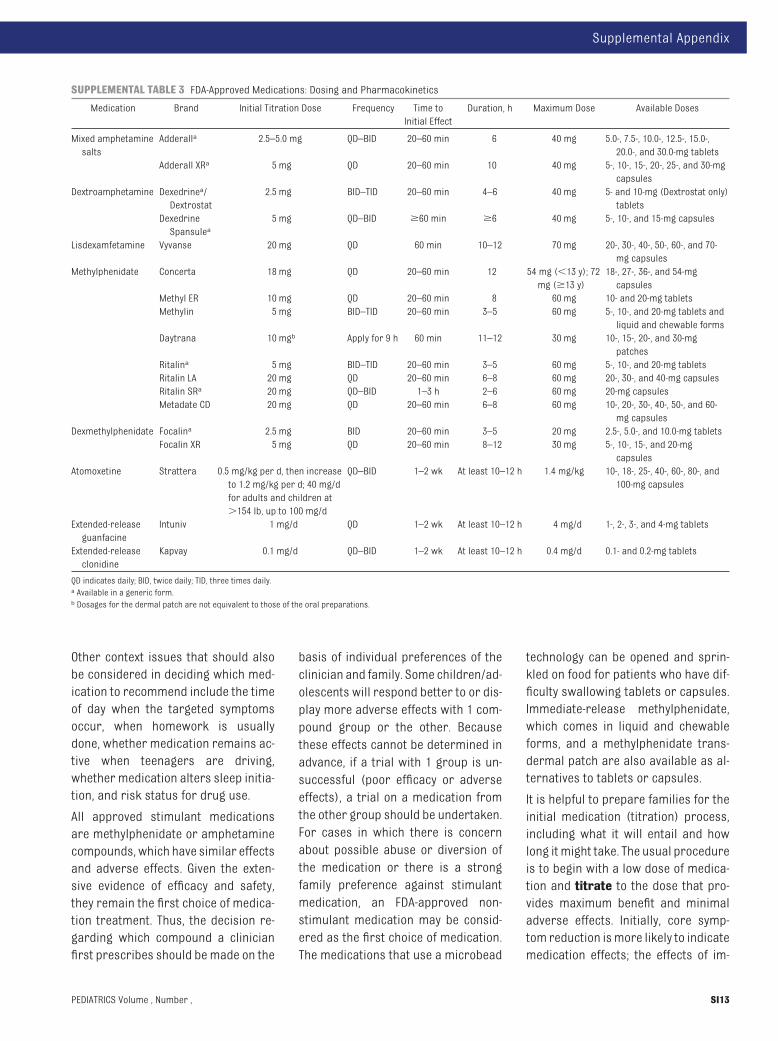
Other context issues that should alsobe considered in deciding which med-ication to recommend include the timeof day when the targeted symptomsoccur, when homework is usuallydone, whether medication remains ac-tive when teenagers are driving,whether medication alters sleep initia-tion, and risk status for drug use.
All approved stimulant medicationsare methylphenidate or amphetaminecompounds, which have similar effectsand adverse effects. Given the exten-sive evidence of efficacy and safety,they remain the first choice of medica-tion treatment. Thus, the decision re-garding which compound a clinicianfirst prescribes should bemade on the
basis of individual preferences of theclinician and family. Some children/ad-olescents will respond better to or dis-play more adverse effects with 1 com-pound group or the other. Becausethese effects cannot be determined inadvance, if a trial with 1 group is un-successful (poor efficacy or adverseeffects), a trial on a medication fromthe other group should be undertaken.For cases in which there is concernabout possible abuse or diversion ofthe medication or there is a strongfamily preference against stimulantmedication, an FDA-approved non-stimulant medication may be consid-ered as the first choice of medication.The medications that use a microbead
technology can be opened and sprin-kled on food for patients who have dif-ficulty swallowing tablets or capsules.Immediate-release methylphenidate,which comes in liquid and chewableforms, and a methylphenidate trans-dermal patch are also available as al-ternatives to tablets or capsules.
It is helpful to prepare families for theinitial medication (titration) process,including what it will entail and howlong itmight take. The usual procedureis to begin with a low dose of medica-tion and titrate to the dose that pro-vides maximum benefit and minimaladverse effects. Initially, core symp-tom reduction ismore likely to indicatemedication effects; the effects of im-
SUPPLEMENTAL TABLE 3 FDA-Approved Medications: Dosing and Pharmacokinetics
Medication Brand Initial Titration Dose Frequency Time toInitial Effect
Duration, h Maximum Dose Available Doses
Mixed amphetaminesalts
Adderalla 2.5–5.0 mg QD–BID 20–60 min 6 40 mg 5.0-, 7.5-, 10.0-, 12.5-, 15.0-,20.0-, and 30.0-mg tablets
Adderall XRa 5 mg QD 20–60 min 10 40 mg 5-, 10-, 15-, 20-, 25-, and 30-mgcapsules
Dextroamphetamine Dexedrinea/Dextrostat
2.5 mg BID–TID 20–60 min 4–6 40 mg 5- and 10-mg (Dextrostat only)tablets
DexedrineSpansulea
5 mg QD–BID �60 min �6 40 mg 5-, 10-, and 15-mg capsules
Lisdexamfetamine Vyvanse 20 mg QD 60 min 10–12 70 mg 20-, 30-, 40-, 50-, 60-, and 70-mg capsules
Methylphenidate Concerta 18 mg QD 20–60 min 12 54 mg (�13 y); 72mg (�13 y)
18-, 27-, 36-, and 54-mgcapsules
Methyl ER 10 mg QD 20–60 min 8 60 mg 10- and 20-mg tabletsMethylin 5 mg BID–TID 20–60 min 3–5 60 mg 5-, 10-, and 20-mg tablets and
liquid and chewable formsDaytrana 10 mgb Apply for 9 h 60 min 11–12 30 mg 10-, 15-, 20-, and 30-mg
patchesRitalina 5 mg BID–TID 20–60 min 3–5 60 mg 5-, 10-, and 20-mg tabletsRitalin LA 20 mg QD 20–60 min 6–8 60 mg 20-, 30-, and 40-mg capsulesRitalin SRa 20 mg QD–BID 1–3 h 2–6 60 mg 20-mg capsulesMetadate CD 20 mg QD 20–60 min 6–8 60 mg 10-, 20-, 30-, 40-, 50-, and 60-
mg capsulesDexmethylphenidate Focalina 2.5 mg BID 20–60 min 3–5 20 mg 2.5-, 5.0-, and 10.0-mg tablets
Focalin XR 5 mg QD 20–60 min 8–12 30 mg 5-, 10-, 15-, and 20-mgcapsules
Atomoxetine Strattera 0.5 mg/kg per d, then increaseto 1.2 mg/kg per d; 40 mg/dfor adults and children at�154 lb, up to 100 mg/d
QD–BID 1–2 wk At least 10–12 h 1.4 mg/kg 10-, 18-, 25-, 40-, 60-, 80-, and100-mg capsules
Extended-releaseguanfacine
Intuniv 1 mg/d QD 1–2 wk At least 10–12 h 4 mg/d 1-, 2-, 3-, and 4-mg tablets
Extended-releaseclonidine
Kapvay 0.1 mg/d QD–BID 1–2 wk At least 10–12 h 0.4 mg/d 0.1- and 0.2-mg tablets
QD indicates daily; BID, twice daily; TID, three times daily.a Available in a generic form.b Dosages for the dermal patch are not equivalent to those of the oral preparations.
Supplemental Appendix
PEDIATRICS Volume , Number , SI13

provement in function require a moreextended time period. Stimulant medi-cations can be effectively titrated on a3- to 7-day basis. During the firstmonthof treatment, medication dose may betitrated with a weekly or biweekly tele-phone call to the family. The increasingdoses can be provided either by pre-scriptions that allow dose adjust-ments upward or, for some of themed-ications, by 1 prescription of tablets/capsules of the same strength withinstructions to administer progres-sively higher amounts by doubling ortripling the initial dose. Another ap-proach similar to that used in the MTAstudy56 is for parents to be directed toadminister different doses of the samepreparation, each for 1 week at a time(eg, Saturday through Friday). At theend of each week, teacher and parentfeedback and/or DSM-IV-TR–basedADHD rating scales can be completedthrough a telephone interview, fax, orsecure electronic system. In additionto the ADHD rating scale, parents andteachers should be asked to review ad-verse effects and target goals.
A face-to face follow-up visit is recom-mended by the fourth week of medica-tion, during which clinicians reviewthe responses to the varying doses andmonitor adverse effects, pulse, bloodpressure, and weight. To ensure thatprogress in symptom control is beingmaintained, clinicians should continueto monitor levels of core symptomsand improvement in specified targetgoals. A general guide for visits to theprimary care clinician is for the face toface visits to occur initially on amonthly basis, until there is a consis-tent optimal response, and then every3 months in the first year of treatment.Subsequent visits will depend on theresponse but should occur at least 2times per year, until it is clear that tar-get goals are progressing and stable,and then periodically as determined bythe family and the clinician. Recent re-
sults from the MTA study indicate thatthere are a number of children/adoles-cents who, by 3 years after startingmedication, continue to improve evenif the medication has been discontin-ued.57 The findings suggest that chil-dren/adolescents who are stable intheir improvement of ADHD symptomsmay be given a trial off medication af-ter several years to determine if med-ication is still needed. This process isbest undertakenwith closemonitoringof the child’s/adolescent’s core symp-toms and function at home, in school,and in the community.
Whenever possible, improvements incore symptoms and target goalsshould be monitored in an objectiveway (eg, going from 60% to 20%miss-ing assignments per week [see theADHD toolkit13]), and the core symp-toms can be monitored by use of oneof the DSM-IV-TR–based ADHD ratingscales such as the Vanderbilt ADHDfollow-up scales. Clinicians are en-couraged to educate parents that al-though medication can be effectivein facilitating schoolwork produc-tion, it has not been shown to be ef-fective in addressing learning dis-abilities. A child/adolescent whocontinues to experience academicunderachievement after attainingsome control of ADHD behavioralsymptoms should be assessed for acoexisting condition, including learn-ing and language disabilities, othermental health disorders, or otherpsychosocial stressors. Noncompli-ance with the treatment plan shouldalso be assessed.
If the maximum dose of a stimulantpreparation is reached and less-than-satisfactory results have beenachieved or intolerable adverse ef-fects occur before adequate efficacywith a medication from one of thestimulant groups (methylphenidateor amphetamine), a medication fromthe other stimulant group should be
recommended with a similar titra-tion plan. At least half of the chil-dren/adolescents whose symptomsfail to respond to 1 stimulant medi-cation may have a positive responseto the alternative medication.56
Families concerned about the use ofstimulants or with concerns aboutabuse or diversion may choose tostart with atomoxetine or extended-release guanfacine or extended-release clonidine. In addition, thosewhose symptoms do not respond toeither stimulant group might still re-spond to atomoxetine or extended-release guanfacine or extended-release clonidine. Extended releaseguanfacine or extended release clo-nidine also may be added as an ad-junctive therapy in children who par-tially respond to stimulantmedication.
There is a block-box warning onatomoxetine of the possibility ofsuicidal ideation when initiatingmedication management. Earlysymptoms of suicidal ideationmight include thinking about self-harm and increasing agitation. Ifthere are any concerns about sui-cidal ideation in children pre-scribed atomoxetine, further evalu-ation, reconsideration about theuse of atomoxetine, and more fre-quent monitoring should be consid-ered, and if necessary, referral to amental health clinician should bemade.
Atomoxetine is a selectivenorepinephrine-reuptake inhibitorand might result in maximum re-sponse only after approximately 4 to 6weeks. Extended-release guanfacineand extended-release clonidine are�2A-adrenergic agonists and might re-sult in maximum response in approxi-mately 2 to 4 weeks. Parents may beencouraged to complete weekly symp-tom and adverse-effect monitoring, as
SI14 FROM THE AMERICAN ACADEMY OF PEDIATRICS

described previously, as an objectivemeasure to monitor efficacy. Becausesymptom change is more gradual withatomoxetine and �2A-adrenergic ago-nists than with stimulant medications,families who have had previous expe-rience with stimulants should bemadeaware of this fact. In some patients, amodest effect of atomoxetine might beseen in 1 week. Atomoxetine mightcause gastrointestinal tract symptomsand sedation early in treatment, so it isrecommended to prescribe half thetreatment dose (0.5 mg/kg) for thefirst week. Appetite suppression canalso occur. Both �2A agonists cancause the adverse effect of somno-lence. In addition, it is recommendedthat the medications be tapered whendiscontinued to prevent a possible re-bound in blood pressure.
Special Circumstances: Preschool-Aged Children
Clinicians should initiate ADHD treat-ment of preschool-aged children(4 –5 years of age) with behaviortherapy and should also assess forother developmental problems, es-pecially with language. If children donot experience adequate symptomand functional improvement with be-havior therapy (most programs are10–14 weeks long, but the clinicianshould check with the therapistsabout their usual length of interven-tion), the clinician should first evalu-ate the adequacy and parental ac-ceptance of the therapy. If thesymptoms and/or functioning havenot improved and the child is at sig-nificant behavioral or developmentalrisk because of ADHD, medicationcan be prescribed, as described pre-viously. It must be noted that, cur-rently, the FDA has only approveddextroamphetamine for ADHD in chil-dren in this age group, althoughthere is little evidence to support itssafety and efficacy. There is, how-ever, evidence that methylphenidate
is safe and efficacious for children inthis age group.58 Evidence58 suggeststhat the rate of metabolizing methyl-phenidate is slower in children 4 and5 years of age, so they should bestarted at a lower dose that is in-creased in smaller increments. In ad-dition, the preschool-aged childrenstudied in the multisite study58 hadmore severe dysfunction, whichshould be considered in the decisionto try treatment with methylpheni-date. The additional criteria for de-fining moderate-to-severe impair-ment include symptoms present forat least 9 months and clear impair-ment in both the home and day care/preschool settings that has not re-sponded to an appropriatebehavioral intervention. Limited evi-dence59 and no FDA approval for chil-dren in this age group are availablefor atomoxetine, and no evidence orapproval for extended-release guan-facine or extended-release clonidineare available.
Special Circumstances: Adolescents
Clinicians should assess adolescentpatients with ADHD for symptoms ofsubstance use or abuse before begin-ning medication treatment. If sub-stance abuse is revealed, they shouldhave the patient stop the use, and theyshould provide treatment or refer fortreatment for substance abuse beforebeginning treatment for ADHD. Clini-cians are also encouraged to monitorsymptoms and prescription refills forsigns of misuse or diversion of ADHDmedication.
Special concern should be taken toprovide medication coverage forADHD symptom control while driving.Longer-acting or late-afternoon/short-acting medications might behelpful in this regard. Counseling foradolescents around medication is-sues should include dealing with re-sistance to treatment and empower-
ing children/adolescents to takecharge of and own their medicationmanagement as much as possible.Techniques of motivational inter-viewing might be useful in improvingadherence.60
Special Circumstances: Families andChildren/Adolescents Who DeclineMedication
The decision about what is the mostacceptable treatment for their child/adolescent rests with the family, andthe clinician must respect that deci-sion. The clinician should, however, ad-dress any misinformation or concernsabout medication shared by the family,encourage all other dimensions oftreatment, and provide appropriatemonitoring.
Special Circumstances: Inattention orHyperactivity/Impulsivity (ProblemLevel)
Medication is not appropriate for chil-dren/adolescents whose symptoms donot meet DSM-IV-TR criteria for diagno-sis of ADHD.
Behavior Management
Evidence-based parent training typi-cally begins with 7 to 12 weekly groupsessions with a trained therapist orcertified instructor. The focus is onparent education about ADHD, thechild’s/adolescent’s behavior prob-lems, and difficulties in family relation-ships. A typical program aims to im-prove the parents’/caregivers’understanding of the child’s/adoles-cent’s behavior and to teach themskills to help the child/adolescent toreduce the behavioral difficultiesposed by ADHD.
Programs offer specific techniques forreinforcing adaptive and positive be-haviors and decreasing or eliminatinginappropriate behaviors, both ofwhich alter the motivation of the child/adolescent to control attention, activ-ity, and impulsivity. These programs
Supplemental Appendix
PEDIATRICS Volume , Number , SI15

emphasize establishing positive inter-actions between parents and children;learning how to shape children’s be-haviors through combinations ofpraising and ignoring; how to give suc-cessful commands; how to reinforcepositive behaviors; how to extinguishinappropriate behaviors through ig-noring; how to identify which behav-iors are handled most appropriatelythrough punishment; and determininghow to carry punishments out in a re-sponsible way. These programs all em-phasize teaching self-control andbuilding positive family relationships.If parents strongly disagree about be-havior management or have conten-tious relationships, parenting pro-grams will likely be unsuccessful.
Other strategies, such as changing thephysical environment to reduce stim-uli to overactivity, are also effective bychanging the stimuli that trigger prob-lem behaviors. Depending on the se-verity of the child’s/adolescent’s be-haviors and the capabilities of theparents, group or individual trainingprograms will be required. Programstypically include support for mainte-nance and relapse prevention.
Behavior therapy should be differenti-ated from psychological interventionsdirected to the child/adolescent anddesigned to change the child’s/adoles-cent’s emotional status (eg, play ther-apy) or thought patterns (eg, interper-sonal talk therapy). Thesepsychological interventions do nothave a demonstrated efficacy for theADHD core symptoms, and gainsachieved in the treatment setting usu-ally do not transfer into the classroomor home. By contrast, parent trainingin behavior therapy and classroom be-havior interventions have successfullychanged the behavior of children/ado-lescents with ADHD.61 Behavior therapyis also applicable for children/adoles-cents who have problems in the do-mains of inattention or hypersensitivi-
ty/impulsivity but do notmeet the DSM-IV-TR criteria and for those children/adolescents with a developmentalvariation.
Unless primary care clinicians arespecifically trained, have trained staffor a colocated therapist, or dedicatemany visits to providing the ongoingtreatment, they might not be effectivein providing behavior therapy.62 Clini-cians might also have difficulties de-termining the skills of behavior thera-pists listed in the behavioral healthinsurance plan. This determination isimportant, because many therapistsfocus on a play or interpersonal-talktherapy that has not been shown to beeffective in treating the core symp-toms of ADHD. Telephone inquiries oftherapists, agencies, and mentalhealth clinicians regarding their ap-proach to behavior therapy might al-low clinicians to develop a resourcelist for parents. Clinicians might alsorequest references from other par-ents of children/adolescents withADHD, professional organizations(eg, Association for Behavior andCognitive Therapies), and ADHD advo-cacy organizations (eg, CHADD). Par-ents who have read authoritativelywritten books about behavior thera-py/behavior parent training might bein a better position to know whatthey are looking for in a therapistand ask the salient questions whenseeking appropriate therapists.Some of these resources are avail-able in the ADHD toolkit13 and thebook ADHD: What Every Parent Needsto Know.54
Classroom behavior management alsofocuses on shaping the child’s/adoles-cent’s behaviors and may be inte-grated into classroom routines for allstudents or targeted for a selectedchild/adolescent in the classroom.Classroom management often beginswith increasing the structure of activi-ties. Token economy refers to using
points or tokens that are given for pos-itive behaviors, and response cost re-fers to points or tokens subtracted forinappropriate behaviors. The tokensor points can then be cashed in after adefined period for rewards or privi-leges. Systematic rewards (eg, use of atoken economy) are included to in-crease appropriate behavior and elim-inate inappropriate behavior. A peri-odic (often daily) behavior report cardcan record the child’s/adolescent’sprogress or performance with regardto goals and communicate the child’s/adolescent’s progress to the parents,who then provide reinforcers or con-sequences based on that day’s perfor-mance. Such programs are also usefulfor the purpose of monitoring medica-tion effects.
COLLABORATE WITH THE SCHOOL TOENHANCE SUPPORTS AND SERVICES
Many teachers and schools have effec-tive strategies for supporting andserving children/adolescents withADHD. Schools can implementbehavior-management programs thatdirectly target ADHD symptoms as wellas interventions to enhance academicand social functioning. Schools mayalso use strategies (eg, daily behaviorreport cards) to enhance communica-tion with families. All schools shouldhave specialists (eg, school psycholo-gists, counselors, special educators)who observe the child/adolescent,identify triggers and reinforcers, andsupport teachers in changing the cir-cumstances of the classroom andmaking accommodations to addressADHD symptoms, such as written-output bypass strategies, untimedtesting, testing in less distracting envi-ronments, preferential seating, androutine reminders.
Clinicians should be aware of the eligi-bility criteria for the 504 RehabilitationAct and the IndividualsWith DisabilitiesEducation Act supports in their state
SI16 FROM THE AMERICAN ACADEMY OF PEDIATRICS

and local school district(s)63 andshould understand the process for re-ferral as well as the individuals withwhom the physician or parent shouldmake contact. This information can beprovided to parents to support theirefforts to request classroom adapta-tions for their child/adolescent withADHD, including the use of empiricallysupported academic interventions toaddress achievement difficulties asso-ciated with ADHD symptoms.
Do symptoms improve?
In providing a medical home, primarycare clinicians should regularly moni-tor all aspects of ADHD treatment, toinclude:
● systematic reassessment of coresymptoms and function;
● regular reassessment of targetgoals;
● assurance that the family is satis-fied with the care they are receiv-ing from other clinicians and thera-pists, if applicable;
● provision of anticipatory guid-ance, further child/adolescentand family education, and transi-tion planning as needed andappropriate;
● assurance that care coordinationis occurring and meeting the needsof the child/adolescent and family;
● confirmation of adherence to anyprescribed medication regimen,with adjustments made as needed;
● heart rate, blood pressure, height,and weight monitoring; and
● continuing to form a therapeutic re-lationship with the child/adolescentand empower families and chil-dren/adolescents to be strong, in-formed advocates.
Some treatment monitoring can occurduring general health care visits if theclinician inquires about progress to-
ward target goals, adherence to medi-cation and behavior therapy, con-cerns, or changes.
Monitoring of children/adolescentswith inattention or hyperactivity/im-pulsivity problems can help to ensureprompt treatment, should their symp-toms worsen to the extent that a diag-nosis of ADHD is warranted.
Reevaluate to confirm diagnosis and/or provide education to improve
adherence.
Reconsider treatment plan including changing of the medication or dose, adding a medication approved for
adjuvant therapy, and/or changing behavioral therapy.
No
ADHD treatment failuremight be a signof incorrect or incomplete diagnosis.Clinicians are advised to repeat the fulldiagnostic evaluation and pay in-creased attention to the possibility ofcoexisting conditions that mimic orare associated with ADHD, such assleep disorders, Asperger syndrome,or epilepsy (eg, absence epilepsy orpartial seizures). A coexisting learningdisordermight also cause an apparenttreatment failure. In the case of achild/adolescent previously diagnosedwith problem-level inattention or hy-peractivity, repeating the diagnosticevaluation might result in a diagnosisof ADHD, which would allow for in-creased school supports and the inclu-sion of medication in the treatmentplan.
Treatment failure could also signalpoor adherence to the treatment plan.Increased monitoring and education,especially by including the patientearly in his or her treatment, might in-crease treatment adherence. It is help-ful to try to identify the issues that re-strict adherence.
Yes
Follow-up for chronic care
management at least 2x/year for
ADHD issues
In the early stages of treatment, after asuccessful titration period, the fre-quency of follow-up visits will dependon adherence, coexisting conditions,and persistence of symptoms. Asnoted previously, a general guide forvisits to the primary care clinician isfor these visits to occur initially on amonthly basis, then every 3 months inthe first year of treatment. More fre-quent visits might be necessary if co-morbid conditions are present. Visitsshould then be held at least twice eachyear with additional telephone moni-toring at the time of medication-refillrequests. Ongoing communicationwith the school regarding medicationand services is also needed.
It should be noted that at this point,there is little evidence to establish theoptimal, yet practical, follow-up regi-men. It is likely that the regimen willneed to be tailored to the individualchild/adolescent and family needs onthe basis of clinical judgment.
PREPARING THE PRACTICE
Specific office practice proceduresthat facilitate the optimal and efficientdiagnosis and treatment process arecritical for successful management ofchildren/adolescents with ADHD. Moredetail can also be found in the report ofthe AAP Task Force on Mental Health.1
The office process can include:
● developing a packet of ADHD ques-tionnaires and rating scales for par-ents and teachers to complete be-fore a scheduled visit;
● allotting adequate time for ADHD-related visits;
● determining appropriate billing,documentation, and monitoring ofinsurance payments to ensure thatthey adequately cover the servicesrendered;
● implementing methods to track and
Supplemental Appendix
PEDIATRICS Volume , Number , SI17

follow-up patients (refer to medicalhome procedures for more detail);
● asking questions during all clinicalencounters and placing brochuresand posters in the office to alert par-ents and children/adolescents thatbehavior and school problems andADHD are appropriate issues to dis-cuss with the clinician;
● developing an office system formonitoring and titrating medication(a follow-up system should includethe clinician’s assessment of familyorganization, telephone access, andparent-teacher communication ef-fectiveness); and
● collaborating with schools andother involved community providersand resources that can enhance theprocess for ADHD diagnosis andmanagement, which can beachieved on a case-by-case basisthrough coordination of the diagno-sis and treatment plan amongschool staff, the clinician, parents,and other involved professionals(note that this less-systematic ap-proach carries significant chal-lenges, including ensuring consis-tent care for all children/adolescents with ADHD).
A community-level system that reflectsconsensus among district school staffand local primary care clinicians forkey elements of diagnosis, interven-tions, and ongoing communication canhelp to ensure consistent, well-coordinated, and cost-effective care. Acommunity-based systemwith schoolsrelieves the individual primary careclinician from negotiating with eachschool about care and communicationregarding each patient. Offices thathave incorporated medical home prin-ciples are ideal for establishing thiskind of community-level system. Thekey elements for a community-basedcollaborative system include consen-sus on:
● a clear and organized process bywhich an evaluation can be initiatedwhen concerns are identified by ei-ther parents or school personnel;
● a packet of information completedby parents and a teacher abouteach child/adolescent referred tothe primary care clinician;
● a contact person at the practice toreceive information from parentsand teachers at the time of evalua-tion and during follow-up;
● an assessment process to investi-gate coexisting conditions;
● a directory of evidence-based inter-ventions available in thecommunity;
● an ongoing process for follow-upvisits, telephone calls, teacher re-ports, and medication refills;
● availability of forms for collectingand exchanging information; and
● a plan for keeping school staff andprimary care clinicians up-to-dateon the process.
The clinician might face challenges todeveloping such a collaborative pro-cess. As examples, the primary careprovider might be caring for children/adolescents from more than 1 schoolsystem; a school systemmight be quitelarge and not easily accessed; schoolsmight have limited staff and resourcesto complete assessments; or it mightbe difficult for the physician andteacher or other school personnel tocommunicate by telephone becausetheir schedules differ. There are work-able strategies for addressing each ofthese challenges.
In the case of multiple or large schoolsystems in a community, the primarycare clinician might want to begin with1 school psychologist or principal, orseveral practices can initiate contactcollectively with a community schoolsystem. Agreement among the clini-cians on the components of a good
evaluation process facilitates cooper-ation and communication with theschool toward common goals. For ex-ample, agreement on the behavior rat-ing scales used can facilitate comple-tion by school personnel. Standardcommunication forms that monitorprogress and specific interventionscan be faxed between the school andthe pediatric office to shareinformation.
Collaborative systems also extend toother providers who may comanagecare with the primary care clinician.Providers may include a mental healthprofessional who sees the child/ado-lescent for psychosocial interventionsor a specialist who addresses difficultcases, such as a developmental-behavioral pediatrician, child psychia-trist, child neurologist, neurodevelop-mental disability physician, orpsychologist. Agreed-on processes forroutine communication can also beused in these relationships. The AAPTask Force onMental Health provides afull discussion of collaborative rela-tionships with mental health profes-sionals, including colocation and inte-grated models, in its Chapter ActionKit64 and Pedialink Module.
It is important to note that good carefrequently requires activities that cur-rently are not reimbursed. These activ-ities include contacts with teachersand mental health consultants andnon–face-to-face contact with parentsand patients. It would be helpful for cli-nicians to document the nonreim-bursed efforts and for the nationalAAP, state chapters, and clinicians tocontinue to try tomake third-party pay-ers understand the need for these ef-forts and provide compensation forthis appropriate care.
COMPLEMENTARY AND UNPROVENTHERAPIES
Families of children/adolescents withADHD increasingly ask about comple-
SI18 FROM THE AMERICAN ACADEMY OF PEDIATRICS

mentary and alternative therapies forADHD. Such therapies might includelarge doses of vitamins, essential fattyacids, and other dietary alterations;chelation; and electroencephalo-graphic (EEG) biofeedback.65 To date,there is insufficient evidence to deter-mine whether these therapies lead tochanges in core symptoms of ADHD orfunction, and for many of them, thereis limited information about theirsafety. For these reasons, these thera-pies cannot be recommended. Sometherapies, chelation, and megavita-mins have been proven to cause someadverse effects and arecontraindicated.
Physicians can play a constructive rolein helping families make thoughtfultreatment choices by reviewing thestated goals or effects claimed for agiven treatment; the state of evidenceto support or discourage use of thetreatment; and known or potential ad-verse effects. Physicians should en-courage families that wish to pursuethese treatments to try 1 interventionat a time, choose target goals they willuse, monitor core symptoms to mea-
sure efficacy, and choose a time framein which they anticipate the changes tooccur. Families should also be stronglyencouraged to continue to use themore evidence-based interventions atthe same time that they are exploringcomplementary and alternativetreatments.
Clinicians should respect families’ in-terests and preferences while they ad-dress and answer questions aboutcomplementary and unproven thera-pies to preserve and enhance the clini-cian/family relationship. In addition,primary care clinicians should knowabout additional therapies that fami-lies might be administering to ade-quately monitor for drug interactions.Parents and children/adolescents whodo not feel that their choices in healthcare are respected by their primarycare clinician might be less likely tocommunicate about complementaryor alternative therapies.
Further information about comple-mentary and other therapies pro-moted for the treatment of ADHD canbe found in a chapter on this topic inDevelopmental-Behavioral Pediatrics:
Evidence and Practice65 or in an articlein the Journal of Developmental andBehavioral Pediatrics.52
CONCLUSION
ADHD is the most common neurobio-logical disorder of children/adoles-cents; untreated, ADHD can have far-reaching and serious consequenceson their health and well-being. Fortu-nately, effective treatments are avail-able, as are methods for assessingand diagnosing children/adolescentswith ADHD. The AAP is committed tosupporting primary care physicians inproviding quality care to children/ado-lescents with ADHD and their families.
The algorithm presented here repre-sents a portion of that commitment. Itis an effort to assist primary care cli-nicians in delivering care that meetsthe quality standards of the practiceguideline. Additional support and guid-ance can be obtained through theADHD toolkit12 and the work and publi-cations of the AAP Task Force on Men-tal Health.13
REFERENCES
1. Foy JM; American Academy of PediatricsTask Force on Mental Health. Enhancing pe-diatric mental health care: algorithms forprimary care. Pediatrics . 2010;125(3suppl)S109–S125
2. American Psychiatric Association. Diagnos-tic and Statistical Manual of Mental Disor-ders, 4th ed, Text Revision (DSM-IV-TR).Washington, DC: American PsychiatricAssociation; 2000:382–397
3. Egger HL, Kondo D, Angold A. The epidemiol-ogy and diagnostic issues in preschoolattention-deficit/hyperactivity disorder. In-fant Young Child. 2006;19(2):109–122
4. Wolraich ML, Wibbelsman CJ, Brown TE, etal. Attention-deficit/hyperactivity disorderamong adolescents: a review of the diagno-sis, treatment, and clinical implications. Pe-diatrics. 2005;115(6):1734–1746
5. Lahey BB, Carlson CL. Attention deficit disor-der without hyperactivity: a review of re-search relevant to DSM-IV. In: Widiger TA,Frances AJ, Pincus HA, Davis W, First
MDSM-IV Sourcebook. Washington, DC:American Psychiatric Press; 1994:163–188
6. Lollar DJ, Simeonsson RJ. Diagnosis tofunction: classification for children andyouths. J Dev Behav Pediatr. 2005;26(4):323–330
7. Brown R, Freeman WS, Perrin JM, et al.Prevalence and assessment of attention-deficit/hyperactivity disorder in primarycare settings. Pediatrics. 2001;107(3). Avail-able at: www.pediatrics.org/cgi/content/full/107/3/e43
8. Goodman R. The extended version of theStrengths and Difficulties Questionnaire asa guide to child psychiatric caseness andconsequent burden. J Child Psychol Psychi-atry. 1999;40(5):791–801
9. Shaffer D, Gould MS, Brasic J, et al. A chil-dren’s global assessment scale (CGAS).Arch Gen Psychiatry . 1983 ;40(11) :1228–1231
10. WolraichML, Feurer ID,HannahJN,BaumgaertelA, Pinnock TY. Obtaining systematic teacher re-
port of disruptive behavior disorders utilizingDSM-IV. J Abnorm Child Psychol. 1998;26(2):141–152
11. WolraichML, Lambert EW, Worley KA, DoffingMA, Simmons T, Bickman L. Psychometricproperties of the Vanderbilt ADHD Diagnos-tic Parent Rating Scale in a referred popu-lation. J Pediatr Psychol. 2003;28(8):559–568
12. American Academy of Pediatrics. AttentionDeficit Hyperactivity Disorder ToolkitElkGrove Village, IL: American Academy ofPediatrics; 2011
13. American Academy of Pediatrics, TaskForce on Mental Health. Addressing MentalHealth Concerns in Primary Care: A Clini-cian’s ToolkitElk Grove Village, IL: AmericanAcademy of Pediatrics; 2010
14. Gordon M, Barkley RA, Lovett B. Tests andobservational measures. In: BarkleyRAAttention-Deficit Hyperactivity Disorder:A Handbook for Diagnosis and Treatment.
Supplemental Appendix
PEDIATRICS Volume , Number , SI19

3rd ed. New York, NY: Guilford Press; 2005:369–388
15. Edwards M, Gardner ES, Chelonis JJ, SchulzEG, Flake RA, Diaz PF. Estimates of the valid-ity and utility of the Conners’ ContinuousPerformance Test in the assessment of in-attentive and/or hyperactive-impulsive be-haviors in children. J Abnorm Child Psychol.2007;35(3):393–404
16. Barkley R. Attention-Deficit HyperactivityDisorder: A Handbook for Diagnosis andTreatment. 3rd ed. New York, NY: GuilfordPress; 2006
17. Angold A, Erkanli A, Egger HL, Costello EJ.Stimulant treatment for children: a commu-nity perspective. J Am Acad Child AdolescPsychiatry. 2000;39(8):975–998
18. Rowland AS, Lesesne CA, Abramowitz AJ.The epidemiology of attention-deficit/hyperactivity disorder (ADHD): a publichealth view. Ment Retard Dev Disabil ResRev. 2002;8(3):162–170
19. Chronis AM, Lahey BB, Pelham WE Jr, KippHL, Baumann BL, Lee SS. Psychopathologyand substance abuse in parents of youngchildren with attention-deficit/hyperactivitydisorder. J Am Acad Child Adolesc Psychia-try. 2003;42(12):1424–1432
20. Konofal E, Lecendreux M, Cortese S. Sleepand ADHD ; Sleep Med. 2010;11(7):652–658
21. Gozal D, Kheirandish-Gozal L. Neurocogni-tive and behavioral morbidity in childrenwith sleep disorders. Curr Opin Pulm Med.2007;13(6):505–509
22. Capdevila OS, Kheirandish-Gozal L, Dayyat E,Gozal D. Pediatric obstructive sleep apnea:complications, management, and long-termoutcomes. Proc Am Thorac Soc. 2008;5(2):274–282
23. Cortese S, Konofal E, Lecendreux M, et al.Restless legs syndrome and attention-deficit/hyperactivity disorder: a review ofthe literature. Sleep. 2005;28(8):1007–1013
24. Owens JA. A clinical overview of sleep andattention-deficit/hyperactivity disorder inchildren and adolescents. J Can Acad ChildAdolesc Psychiatry. 2009;18(2):92–102
25. Owens J, Dalzell V. Use of the “BEARS” sleepscreening tool in a pediatric residents’ con-tinuity clinic: a pilot study. Sleep Med. 2005;6(1):63–69
26. Chervin RD, Hedger K, Dillon JE, Pituch KJ.Pediatric Sleep Questionnaire (PSQ): valid-ity and reliability of scales for sleep-disordered breathing, snoring, sleepiness,and behavioral problems. Sleep Med. 2000;1(1):21–32
27. Owens J, Nobile C, McGuinn M, Spirito A. TheChildren’s Sleep Habits Questionnaire: con-struction and validation of a sleep survey
for school-aged children. Sleep. 2000;23(8):1043–1051
28. Sadeh A, Pergamin L, Bar-Haim Y. Sleep inchildren with attention-deficit hyperactivitydisorder: a meta-analysis of polysomno-graphic studies. Sleep Med Rev. 2006;10(6):381–398
29. Gruber R, Wiebe S, Montecalvo L, Brunetti B,Amsel R, Carrier J. Impact of sleep restric-tion on neurobehavioral functioning of chil-dren with attention-deficit hyperactivity dis-order. Sleep. 2011;34(3):315–323
30. Gruber R, Sadeh A, Raviv A. Instability ofsleep patterns in children with attention-deficit/hyperactivity disorder. J Am AcadChild Adolesc Psychiatry. 2000;39(4):495–501
31. SteinMA, Sarampote CS, Waldman ID, et al. Adose-response study of OROS methylpheni-date in children and adolescents with ADHD.Pediatrics. 2003;112(5). Available at: www.pediatrics.org/cgi/content/full/112/5/e404
32. Corkum P, Panton R, Ironside S, Macpher-son M, Williams T. Acute impact of immedi-ate release methylphenidate administeredthree times a day on sleep in children withattention-deficit/hyperactivity disorder. JPediatr Psychol. 2008;33(4):368–379
33. O’Brien LM, Ivanenko A, Crabtree VM, et al.The effect of stimulants on sleep character-istics in children with attention deficit/hyperactivity disorder. Sleep Med. 2003;4(4):309–316
34. Owens J, Sangal RB, Sutton VK, Bakken R,Allen AJ, Kelsey D. Subjective and objectivemeasures of sleep in children withattention-deficit/hyperactivity disorder.Sleep Med. 2009;10(4):446–456
35. Mick E, Biederman J, Jetton J, Faraone SV.Sleep disturbances associated with ADHD:the impact of psychiatric comorbidity andpharmacotherapy. J Child Adolesc Psycho-pharmacol. 2000;10(3):223–231
36. van der Heijden KB, Smits MG, van SomerenEJ, Boudewijn Gunning W. Prediction of mel-atonin efficacy by pretreatment dim lightmelatonin onset in children with idiopathicchronic sleep onset insomnia. J Sleep Res.2005;14(2):187–194
37. Weiss MD, Wasdell MB, Bomben MM, Rea KJ,Freeman RD. Sleep hygiene and melatonintreatment for children and adolescentswith ADHD and initial insomnia. J Am AcadChild Adolesc Psychiatry. 2006;45(5):512–519
38. Cortese S, Faraone S, Konofal E, LecendreuxM. Sleep in children with attention-deficit/hyperactivity disorder: meta-analysis ofsubjective and objective studies. J Am Acad
Child Adolesc Psychiatry. 2009;48(9):894–908
39. Golan N, Shahar E, Ravid S, Pillar G. Sleepdisorders and daytime sleepiness in chil-dren with attention-deficit/hyperactive dis-order. Sleep. 2004;27(2):261–266
40. Lecendreux M, Konofal E, Bouvard M, Falis-sard B, Mouren-Simeoni MC. Sleep andalertness in children with ADHD. J Child Psy-chol Psychiatry. 2000;41(6):803–812
41. Ustün TB. Using the International Classifica-tion of Functioning, Disability and Health inattention-deficit/hyperactivity disorder:separating disease from its epiphenomena.Ambul Pediatr. 2007;7(1 suppl):132–139
42. Johnson JG, Harris ES, Spitzer RL, WilliamsJB. The patient health questionnaire foradolescents: validation of an instrument forthe assessment of mental disorders amongadolescent primary care patients. J AdolescHealth. 2002;30(3):196–204
43. Birmaher B, Khetarpal S, Brent D, et al. TheScreen for Child Anxiety Related EmotionalDisorders (SCARED): scale construction andpsychometric characteristics. J Am AcadChild Adolesc Psychiatry. 1997;36(4):545–553
44. Fabiano GA, Pelham WE, Waschbusch DA, etal. A practical measure of impairment: psy-chometric properties of the impairmentrating scale in samples of children with at-tention deficit hyperactivity disorder andtwo school-based samples. J Clin Child Ado-lesc Psychol. 2006;35(3):369–385
45. American Academy of Pediatrics, TaskForce on Mental Health; American Academyof Child and Adolescent Psychiatry, Commit-tee on Health Care Access and Economics.Improving mental health services in pri-mary care: reducing administrative and fi-nancial barriers to access and collabora-tion [published correction appears inPediatrics. 2009;123(6):1611]. Pediatrics.2009;123(4):1248–1251
46. Wolraich ML, Lambert EW, Bickman L, Sim-mons T, Doffing MA, Worley KA. Assessingthe impact of parent and teacher agree-ment on diagnosing ADHD. J Dev Behav Pe-diatr. 2004;25(1):41–47
47. Zuckerbrot R, Cheung AH, Jensen PS, SteinRE, Laraque D; GLAD-PC Steering Group.Guidelines for Adolescent Depression in Pri-mary Care (GLAD-PC): I. Identification, as-sessment, and initial management. Pediat-rics. 2007;120(5). Available at: www.pediatrics.org/cgi/content/full/120/5/e1299
48. Cheung A, Zuckerbrot RA, Jensen PS, GhalibK, Laraque D, Stein RE; GLAD-PC SteeringGroup. Guidelines for Adolescent Depres-sion in Primary Care (GLAD-PC): II. Treat-
SI20 FROM THE AMERICAN ACADEMY OF PEDIATRICS

ment and ongoing management [publishedcorrection appears in Pediatrics. 2008;121(1):227]. Pediatrics. 2007;120(5). Avail-able at: www.pediatrics.org/cgi/content/full/120/5/e1313
49. Center for Adolescent Substance Abuse Re-search, Children’s Hospital Boston. CRAFFT:Screening Adolescents for Alcohol andDrugs. Boston, MA: Children’s HospitalBoston ; 2001 . Ava i lab le at : www.childrenshospital.org/views/february09/images/CRAFFT.pdf. Accessed June 29, 2011
50. Sleator EK, Ullman RK. Can the physician di-agnose hyperactivity in the office? Pediat-rics. 1981;67(1):13–17
51. Wolraich ML, Felice ME, Drotar DD. The Clas-sification of Child and Adolescent Mental Con-ditions inPrimaryCare: Diagnostic andStatis-ticalManual for Primary Care (DSM-PC), Childand Adolescent Version. Elk Grove, IL: Ameri-can Academy of Pediatrics; 1996
52. Jensen P, Hinshaw SP, Swanson JM, et al.Findings from the NIMH multimodal treat-ment study of ADHD (MTA): implications andapplications for primary care providers. JDev Behav Pediatr. 2001;22(1):60–73
52. American Academy of Pediatrics, NationalCenter for Medical Home Implementation.Building Your Medical Home [toolkit]. Avail-able at: http://www.pediatricmedhome.org.Accessed September 28, 2011
54. Reiff M. ADHD: What Every Parent Needs toKnow. 2nd ed. Elk Grove Village, IL: AmericanAcademy of Pediatrics; 2011
55. Perrin JM, Friedman RA, Knilans TK, et al;American Academy of Pediatrics, Black BoxWorking Group, Section on Cardiology andCardiac Surgery. Cardiovascular monitor-ing and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics.2008;122(2):451–453
56. Greenhill LL, Abikoff HB, Arnold E, et al. Med-ication treatment strategies in the MTAstudy: relevance to clinicians and research-ers. J Am Acad Child Adolesc Psychiatry.1996;35(10):1304–1313
57. Molina BS, Hinshaw SP, Swanson JM, et al.The MTA at 8 years: prospective follow-up ofchildren treated for combined type ADHD inthe multisite study. J Am Acad Child AdolescPsychiatry. 2009;48(5):484–500
58. Greenhill L, Kollins S, Abikoff H, McCrackenJ, Riddle M, Swanson J. Efficacy and safetyof immediate-release methylphenidatetreatment for preschoolerswith ADHD. J AmAcad Child Adolesc Psychiatry. 2006;45(11):1284–1293
59. Kratochvil CJ, Vaughan VS, Stoner JA, et al. Adouble-blind-placebo controlled study ofatomoxetine in young children with ADHD.Pediatrics. 2011;127(4). Available at: www.pediatrics.org/cgi/content/full/127/4/e862
60. Charach A, Volpe T, Boydell KM, Gearing RE. Atheoretical approach to medication adher-ence for children and youthwith psychiatricdisorders. Harv Rev Psychiatry. 2008;16(2):126–135
61. Charach A, Dashti B, Carson PAttention Def-
icit Hyperactivity Disorder: Effectiveness ofTreatment in At-risk Preschoolers; Long-term Effectiveness in All Ages; and Variabil-ity in Prevalence, Diagnosis, and Treatment.Rockville, MD: Agency for Healthcare Re-search and Quality; 2011.In press
62. Sonuga-Barke E, Thompson M, Daley D,Laver-Bradbury C. Parent training for atten-tion deficit/hyperactivity disorder: is it aseffective when delivered as routine ratherthan as specialist care? Br J Clin Psychol.2004;43(pt 4):449–457
63. Davila RR, Williams ML, MacDonald JT.Memorandum on clarification of policy toaddress the needs of children with atten-tion deficit disorders within generaland/or special education. In: ParkerHCThe ADD Hyperactivity Handbook forSchools. Plantation, FL: Impact Publica-tions Inc; 1991:261–268
64. American Academy of Pediatrics, TaskForce on Mental Health. Strategies for Sys-tem Change in Children’s Mental Health: AChapter Action Kit. Elk Grove Village, IL:American Academy of Pediatrics; 2007.Ava i lab le a t : h t tp : / /www.aap .org/commpeds/dochs/mentalhealth/cak/finalcak.pdf. Accessed September 28, 2011
65. Chan E. Complementary and alternativemedicine in developmental-behavioral pedi-atrics. In: Wolraich ML, Drotar DD, DworkinPH, Perrin ECDevelopmental-BehavioralPediatrics: Evidence and Practice. Philadel-phia, PA: Mosby Elsevier; 2008:259–280
Supplemental Appendix
PEDIATRICS Volume , Number , SI21










![Supplemental Information for the IDSA/SHEA Guideline … · Supplemental Information for the IDSA/SHEA Guideline on Implementing an Antibiotic Stewardship Program ... OR "Endophthalmitis"[Majr]](https://img.pdfslide.net/doc/110x75/5b8193097f8b9aad638c9b62/supplemental-information-for-the-idsashea-guideline-supplemental-information.jpg)