Embed Size (px)
Citation preview

TRIGEMINAL AUTONOMIC CEPHALALGIAS (M MATHARU, SECTION EDITOR)
Supraorbital and Supratrochlear Stimulation for TrigeminalAutonomic Cephalalgias
Julien Vaisman & Edrick Lopez & Nicholas K. Muraoka
# Springer Science+Business Media New York 2014
Abstract Trigeminal autonomic cephalalgias (TAC) is a rareprimary headache disorder with challenging and limited treat-ment options for those unfortunate patients with severe andrefractory pain. This article will review the conventional phar-macologic treatments as well as the new neuromodulationtechniques designed to offer alternative and less invasivetreatments. These techniques have evolved from the treatmentof migraine headache, a much more common headache syn-drome, and expanded towards application in patients withTAC. Specifically, the article will discuss the targeting of thesupratrochlear and supraorbital nerves, both terminal branchesof the trigeminal nerve.
Keywords Cluster headache . Chronic cluster headache .
Migraine headache . Neuromodulation . Occipital nerve .
Pain . Peripheral nerve . Sphenopalatine ganglion .
Supraorbital nerve . Supratrochlear nerve . Stimulation .
Transcutaneous nerve stimulation . Trigeminal autonomiccephalalgia
Introduction
Trigeminal autonomic cephalalgias (TAC) is a group of pri-mary headache conditions of relatively short duration associ-ated with cranial autonomic symptoms. The term TAC en-compasses several disabling neurovascular syndromes, themost common being cluster headaches (CH), short-lastingunilateral neuralgiform headache with conjunctival injectionand tearing (SUNCT), and short-lasting unilateralneuralgiform headache with cranial autonomic features syn-drome (SUNA) [1].
Although TAC is a relatively rare disorder, the humantoll for the headaches sufferers remains very high, manypatients displaying a high suicidal ideation rate along withdecreased productivity because of job loss or disabilities[2]. As a result, there is an increased need for earlydetection, assuring an effective, safe, and evidence-basedtreatment.
Over the past 2 decades, the neuromodulation field haswitnessed a robust growth and has expanded from its originalapplication for the treatment of the failed back syndrome toother various intractable painful neuropathic conditions suchas chronic regional pain syndrome, postherpetic neuralgia,and headaches.
For the treatment of severe, intractable headache condi-tions, a number of peripheral nerves including the occipital,supraorbital, and supratrochlear nerves became the target ofstimulation at their location in the epifascial and subcutaneoustissue. The modality has gained popularity since 1999, whenWeiner and Reed described their technique for occipital stim-ulation in a number of patients with occipital neuralgia [3].Thus, the greater and the lesser occipital nerves became acommon target for the treatment of various drug-resistant,refractory headaches such as occipital neuralgia, chronic mi-graine, hemicrania continua, chronic CH, and hypnicheadache [4, 5].
This article is part of the Topical Collection on Trigeminal AutonomicCephalalgias
J. Vaisman : E. Lopez :N. K. MuraokaDepartment of Physical Medicine and Rehabilitation, HarvardMedical School, Boston, MA, USA
E. Lopez :N. K. MuraokaSpaulding Rehabilitation Hospital, 300 First Avenue, Charlestown,MA 02129, USA
J. Vaisman (*)Pain andWellness Center, 10Centennial Drive, Peabody,MA 01960,USAe-mail: [email protected]
Curr Pain Headache Rep (2014) 18:409DOI 10.1007/s11916-014-0409-4

As an alternative to the stimulation of the occipital nerves,the 2 terminal branches of the trigeminal nerve, the supraor-bital and supratrochlear nerves, became a target for the treat-ment of intractable TAC, giving the presumed involvement ofthe trigemino-vascular axis and the frontal localization of thepain.
The present article will discuss the application ofneuromodulation techniques for various headache conditions,focusing on the supraorbital and supratrochlear stimulation,various treatment options, and the technical challenges relatedto the actual implantation process.
Classification and Treatment of the TrigeminalAutonomic Cephalalgias
The trigeminal autonomic cephalalgias are a group of primaryheadache conditions accompanied by cranial autonomicsymptoms such as lacrimation, conjunctival injection, nasalcongestion, and rhinorrhea. Interestingly, these are the samesymptoms elicited by stimulating the ophthalmic/V1 branchof the trigeminal nerve in healthy patients [6].
Cluster Headaches
Cluster headaches are the most common of the trigeminalautonomic cephalalgia subtypes; they classically presentperiorbital or in the eye and are strictly unilateral during eachepisode, but attacks can affect the contralateral side about20 % of the time [7]. Men are affected more frequently thanfemales at a ratio of 5:1. Attacks typically last 30–60 min andoccur at a frequency from once every other day to 8 times aday. During active periods, the attacks may be provoked byalcohol, histamine, or nitroglycerin [1]. The quality of the painis described as severe, throbbing, and lancinating causing theindividual to be restless, in contrast to the person suffering amigraine, who prefers to be still. Prodrome symptoms arereported almost universally and vary from twinges to pressureto a pulsating feeling in the area that becomes painful duringthe attack [8]. Chronic CH (CCH) occurs over the interval ofmore than 1 year without remission or with remissions lastingless than 1 month [1]. The chronic form accounts for up to10 % of patients with CH.
CH are best treated acutely with supplemental oxygen [9]and subcutaneous [10] or intranasal [11] Sumatriptan. Oraltriptans have not been shown to be effective as acute treatmentof cluster headache and are associated with medication over-use headaches [12]. Preventative treatments include prednis-olone and methysergide for episodic cluster headaches; andverapamil, topiramate, gabapentin, lithium, melatonin, andgreater occipital nerve blocks for CCH [13].
Paroxysmal Hemicrania
Paroxysmal hemicrania typically affects unilaterally the tem-poral, peri-auricular, peri-orbital, and maxillary areas. Painreferral to the neck, shoulder, and arm can be common.Attacks last an average of 13–29 min [14]. Compared withcluster headaches, paroxysmal hemicrania occur more fre-quently, from 8 to 30 attacks per day. Paroxysmal hemicraniadoes not appear to affect either gender more frequently [15].
One of the diagnostic criteria of paroxysmal hemicrania isthat it is responsive to indomethacin, so this NSAID is thefirst-line treatment of paroxysmal hemicrania symptoms [16].In individuals with contraindications to indomethacin intake,there are case reports of topiramate being used as successfulprophylactic treatment for paroxysmal hemicrania [17].
SUNCT and SUNA
In SUNCT, both conjunctival injection and tearing are present.SUNCT can be viewed as a subtype of SUNA, where SUNAcan have any of the cranial autonomic symptoms in additionto conjunctival injection and tearing, such as nasal stuffiness,rhinorrhea, ptosis, and sweating. SUNCTand SUNA are bothprimary headache syndromes characterized by a high frequen-cy of symptoms of short duration. Average duration ofSUNCT attacks are 1 min, with maximum length of 2 min;in comparison, SUNA attacks can last as long as 10 min.SUNCT attacks can come as frequently as 200 per day [1].Prevention of these TAC varieties is with oral Lamotrigine.Intravenous lidocaine infusions can be used as a transition tooral Lamotrigine [18]. Subcutaneous infusion of lidocaineproved to be effective as abortive treatment on 78% occasionsin patients with SUNCT and SUNA [19].
Despite optimal medical management of headache symp-toms, up to 20 % of patients with chronic cluster headachesare refractory to these treatments [20]. Headaches are consid-ered intractable if there are persistent symptoms or intolerableside-effects after an adequate trial (appropriate dose andlength of treatment) of medications [21].
A variety of invasive procedures have emerged to addressthese intractable headaches. There are case reports of surgicalinterventions targeting various structures including: the tri-geminal nerve and its branches, the Gasserian ganglion (sen-sory ganglion of the trigeminal nerve located in Meckel’scave) and the sphenopalatine ganglion. These procedurescarry their associated risk of morbidity and experience is thatthere is recurrence of symptoms in as little as 6 months,necessitating repeat procedures [22].
Partial sectioning of the main trigeminal sensory root and/or the nervus intermedius has been a treatment for refractorycluster headaches, however, in a case series of 13 patients, allbut 1 had a return of symptoms by 2 years postprocedure [23].Microvascular decompression of the trigeminal nerve has
409, Page 2 of 7 Curr Pain Headache Rep (2014) 18:409

been reported in medically intractable SUNCT and SUNApatients. Although 12 of the 19 patients (63 %) were pain-free at median follow-up of 14 months, the remaining patientsdid not experience any benefit and 2 patients had persistentcomplications such as ataxia and hearing impairment [18].
Neurolysis of the Gasserian ganglion, which is the sensoryganglion of the trigeminal nerve, is done with the idea thatsymptoms of TACs affect the sensory distribution of thetrigeminal nerve. There has been chemical neurolysis withglycerol, however, 63 % of the treated patients had persistentheadaches at 1-year follow-up [22]. Radiofrequency ablationof the Gasserian ganglion has been attempted as well, withpotentially debilitating side effects including abducens nervepalsy [24], facial anesthesia dolorosa and corneal anesthesia,which can lead to blindness [25].
Percutaneous radiofrequency ablation of the sphenopalatineganglion, which is located in the pterygopalatine fossa, hasshown some benefits in episodic CH, but the procedure seemsto be less effective in patients with chronic CH [26]. Gammaknife surgery of the sphenopalatine ganglion with or withouttargeting the ipsilateral trigeminal nerve has been done forchronic cluster headaches in patients with symptoms refractoryto medications and even other surgical procedures. Satisfactorypain relief was only seen in 59 % of the patients at 34-monthfollow-up with half of the group developing facial sensoryimpairments after the procedure [27]. Microvascular decom-pression of the sphenopalatine ganglion has been attempted forrefractory cluster headache, however, a small case series failedto show a significant difference in presurgical vs postsurgicalpain scores, attack frequency, or quality of life [28].
Neuromodulation for pain is a growing field that is receiv-ing much interest and has shown promise. For this reason, it isfelt that destructive surgical options should not be included inmodern treatment options for the trigeminal autonomiccephalalgias [13].
Neuromodulation – Evolving Therapy (other than for HA)
The first concept for the application of neurostimulation inmodernmedicine was 1965, whenMelzak andWall publishedtheir gate control theory of pain in Science: selective stimula-tion of large diameter myelinated fibers causes inhibition ofthe small fiber pathway that transmit pain and temperaturesensation [29]. Norman Shealy is credited with the first clin-ical application of neuromodulation when he placed an elec-tric lead attached to an external cardiac generator over thedorsal column of the spinal cord in the intrathecal space totreat intractable pain in a terminally ill cancer patient [30].
Hosobuchi and colleagues developed an invasive approachof deep brain stimulation in 1973 by implanting leads into thethalamus of individuals with facial anesthesia dolorosa [31].
Tsubokawa et al used motor cortex stimulation to alleviatecentral pain originating in the thalamus [32].
Peripheral nerve stimulators are used to manage pain bytargeting a specific peripheral nerve. Peripheral nerve fieldstimulation (PNfS) is another technique to induce paresthesiaover an area of pain that overlaps several cutaneous nervedistributions and not confined to a single peripheral nervedistribution [33]. The mechanism of PNfS is also suggestedto work via the gate control theory of pain. The subcutaneouslayer of the skin has a high density of A beta terminal sensoryfibers and electrodes are placed under the skin in the region ofpain [34]. A recent randomized control study looking at PNfSfor chronic axial low back pain refractory to medications,interventions, and surgery found 24 of 32 patients (80 %)who had a trial system placed responded to the trial andunderwent implantation of permanent device. At 1-yearfollow-up, 70 % had good to excellent pain relief with anadditional 17 % reporting fair relief in symptoms [35].
Specifically related to the trigeminal autonomiccephalalgias, there have been attempts at targeting variousstructures for neurostimulation. The most invasive is deepbrain hypothalamic stimulation. The rationale for this is basedon PET scan results of nitrous-oxide induced symptoms inindividuals with chronic cluster headaches suggesting in-creased blood flow in the diencephalon, specifically the hy-pothalamus [36]. Experience with this in 58 patients hasshown success in 60% of the treated group, however, becauseof the invasive nature of the procedure, there is a small but realrisk of brain hemorrhage [37]. Another target has been theoccipital nerve, which has been effective in about two-thirdsof the treated group [38].
Stimulation as Treatment for Headaches
The supratrochlear and supraorbital nerves are branches of thefrontal nerve, which is the largest branch of the ophthalmicdivision of the trigeminal nerve. The supratrochlear nerveascends medially under the corrugator and frontal belly ofthe occipitofrontalis muscles to supply the innervation of theskin above the orbital area. The supraorbital nerve passes viathe supraorbital foramen and then ascends just lateral to thesupratrochlear nerve to finally divide into a smaller medial anda larger lateral branch. Both branches are situated in the frontalbelly of the occipitofrontalis muscle and then pierce the mus-cle and the epicranial aponeurosis. Therefore, they are ame-nable to stimulation as they emerge from the orbit and furtherdivide into their terminal branches, which supply the skin ofthe forehead. Hence, it makes sense to attempt stimulatingboth nerves in the supraorbital area for the treatment of TAC.
Building on this theory Vaisman et al performed an obser-vational, open-label, retrospective case series of 5 patientswith intractable trigeminal autonomic cephalalgia who were
Curr Pain Headache Rep (2014) 18:409 Page 3 of 7, 409

implanted with a supraorbital/supratrochlear neuromodulationsystem [39••]. Trial stimulation led to implantation of all 5patients. All patients reported improvement in their activitiesof daily living. The follow-up of the patients ranged between18 months and 36 months, with a mean of 25.2 months.Following the implant, the Visual Analog Scale score wasreduced to a mean of 1.6 from an initial mean score of 8.9.Three patients were completely weaned off opioid medica-tions, while 2 patients continued to take opioid at a lowerdosage. All patients experienced a decrease of the adjuvantneuropathic drugs. The authors found that supraorbital/supratrochlear peripheral nerve stimulation appears to be afairly safe and potentially effective therapeutic modality forpatients with intractable TAC. It was found that similar tooccipital nerve stimulation, the supraorbital nerve blocks donot accurately predict who will respond to a trial ofsupraorbital/supratrochlear nerve stimulation [40].
A few cases of supraorbital nerve stimulation for othertypes of headaches have been reported. In 1 retrospective caseseries, 10 patients had permanent implantation of a supraor-bital nerve stimulator for the treatment of chronic, intractablefrontal, and frontotemporal neuritis unresponsive to medica-tion [41]. Permanent implantation resulted in significant re-ductions in pain and use of opioids. Adverse events wereminor, limited to 3 patients who had lead migrations and 1with a minor scalp infection. Reed et al reported on 7 patientswho were successfully treated for intractable chronic migrainewith dual stimulation of both the occipital and supraorbitalnerves [42]. These patients were followed for a period rangingfrom 1 to 35 months. The authors concluded that this combi-nation led to a substantial better outcome than occipital nervestimulation alone. Slavin et al reported on 5 patients undergo-ing supraorbital nerve stimulation for craniofacial pain [40]. Inaddition, a single case report of supraorbital nerve stimulationfor supraorbital neuralgia was also published [43]. Prior to theaforementioned Vaisman et al study [39••] only 1 report usingstrictly supraorbital stimulation for the treatment of chronicCH had been published [44]. Goadsby reported 50 % successin treating 2 CH patients with occipital nerve stimulation [45]In a review of neurostimulation for primary headache disor-ders in 2009, Schwedt recommended that “further studies arerequired to determine the safety and efficacy of supraorbitalnerve stimulation for treating headache disorders” [46].
Not surprisingly, other anatomic targets, such as cervicalposterior epidural space, cervical medial branch nerves, andthe sphenopalatine ganglion were found to be valuable targetsfor neuromodulation. For example, high epidural spinal cordstimulation was reported successful in 7 patients suffering fromintractable CH [47]. One case of intractable episodic CH treatedsuccessfully with percutaneous cervical zygapophyseal radio-frequency ablation has been reported [48].
The sphenopalatine ganglion can be amenable to electricalstimulation using the classical infrazygomatic approach
during an acute episode of CH and the relief of pain occursafter several minutes of stimulation [49, 50]. Recently,Schoenen et al showed that stimulation of the SPG could bean effective novel therapy for chronic cluster headache suf-ferers, with dual beneficial effects, acute pain relief and ob-served attack prevention, and has an acceptable safety profilecompared with similar surgical procedures [51•]. Theirs was amulticenter, multiple CH attack study in patients sufferingfrom refractory CCH. Each CH attack was randomly treatedwith full, sub-perception, or sham stimulation. Pain relief at15 min following SPG stimulation and device- or procedure-related serious adverse events were evaluated. Nineteen of 28(68 %) patients experienced a clinically significant improve-ment. Pain relief was achieved in 67.1 % of full stimulation-treated attacks compared with 7.4 % of sham-treated and7.3 % of sub-perception-treated attacks. Five serious adverseevents occurred (3 lead revisions and 2 explantations) andmost patients (81 %) experienced transient, mild/moderateloss of sensation within distinct maxillary nerve regions butmost resolved within 3 months. Mueller et al followed 10CCH patients implanted with occipital nerve stimulators overa 12 month period. The authors found that the frequency,duration, and severity of the cluster attacks were reduced in90 % of patients [52].
Burns et al published a large study [53] that included 14patients with intractable CCH treated with occipital nervestimulation. A total of 6 patients reported meaningful im-provement of the pain. Improvement evolved over weeks ormonths, although attacks returned in a few days when thedevice malfunctioned due to battery depletion. Magis et al[54] followed a total of 8 patients with intractable CCH afteroccipital nerve implantation. Again the results appeared to befavorable. Interestingly, the authors found a delay of at least2 months between implantation and significant clinical im-provement, suggesting that the procedure acts via a slowneuromodulation process at the level of the upper brain stemor diencephalic centers. The general impression from the fewstudies using occipital stimulation for patients with intractableCH is that relief occurred slowly over time while autonomicphenomena appeared to persist [55].
Other studies found supraorbital nerve stimulation effectivein relieving neuropathic facial pain including ophthalmicpostherpetic neuralgia [56–58]. The mechanism of pain relieffor patients undergoing peripheral nerve stimulation remainselusive, despite some prevailing theories, including increasedblood flow, increased serotonin and dopamine at the spinalcord level, inhibition of nociceptive responses of wide-dynamic range neurons, and a possible alteration of paininhibitory circuits [59–61].
There is a building body of solid literature indicating thatperipheral nerve stimulation is a potentially promising therapyfor patients suffering from chronic migraine (CM). Serra et al[62] recently published a prospective, randomized cross-over
409, Page 4 of 7 Curr Pain Headache Rep (2014) 18:409

trial looking at occipital nerve stimulation for the treatment ofchronic migraine and medication overuse headache. Theyfound that occipital nerve stimulation appeared to be safe andeffective in reducing headache intensity and frequency, improv-ing quality of life, and reducing medication use in patientssuffering from chronic migraine or medication overuse head-ache. Adding to the evidence, Silberstein et al [63] published arandomized, controlled multicenter study, in which patientsdiagnosed with CM were implanted with a neurostimulationdevice near the occipital nerves and randomized 2:1 to active orsham stimulation. The primary endpoint was a difference in thepercentage of responders (defined as patients that achieved a50 % reduction in mean daily visual analog scale scores) ineach group at 12 weeks. They did not find significant differencein the percentage of responders in the active group comparedwith the control group. Nonetheless, although this study failedto meet its primary endpoint, this is the first large-scale study ofperipheral nerve stimulation of the occipital nerves in chronicmigraine patients that showed significant reductions in pain,headache days, and migraine-related disability.
In addition, Schoenen et al [64] published in 2013 adouble-blinded, randomized, sham-controlled trial looking atsupraorbital transcutaneous nerve stimulation (TNS) as atreatment for migraine. They concluded that treatment with asupraorbital TNS is effective and safe as a preventive therapyfor migraine.
Intractable chronic CH has been shown to be responsive todeep brain stimulation [65–67], but it is more invasive and canalso lead to much more severe complications such as intrace-rebral hemorrhage and/or death [68]. For those patients withintractable TACwho do not respond to suboccipital peripheralnerve stimulation, or who might not be candidates for DBS,another option is stimulation of the trigeminal nerve branches.Clearly, direct stimulation of a peripheral nerve is less invasiveand a safer procedure than deep brain stimulation [69].
Considering that CH arises unilaterally in the first andsecond trigeminal nerve distribution [70], it makes sense tostimulate peripheral nerves which, in fact, are branches of thetrigeminal nerve. Also, because central sensitization mecha-nisms appear to play a significant role in the pathophysiologyof CH [71], it makes more sense to seek a neuromodulationtechnique for the treatment of this condition.
Device Implantation and Technical Considerations
As the intracranial trigeminal location is not easily amenableto stimulation, the peripheral branches of the trigeminal nervebecome an appealing target for neuromodulation. Similar tothe model of spinal cord stimulation, a trial of stimulation isinitially performed in order to identify the best candidates withthe general goal that the stimulation will be felt over the skinabove the corresponding orbit.
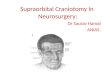
The trial 8-contact lead is placed in the operating roomunder sterile conditions. Light sedation is provided so thepatient can verify adequate coverage of the painful region. Acurved Tuohy needle is navigated just above the supraorbitalmargin of the frontal bone and directed medially towards theglabella. As a landmark, the supraorbital notch is usuallyeasily palpated along the supraorbital prominence, on thesame line with the pupil. The lead is placed through the needlefollowing which the needle is removed and the lead is an-chored to the skin. Fluoroscopy is used to confirm the finallead placement (Fig. 1). Once the intraoperative test is deemedsatisfactory, the patient is discharged home with appropriateinstructions on how to use the device. Typically the trial isextended for a period of 10–14 days. During the trial thepatients carry on with their normal daily activities. The triallead is exiting the temporal area of the skin where it is coveredby a sterile dressing and is connected to a handheld program-mer, usually similar in size to a cellular phone. The patientsreceive a few programs and are welcome to use the trialstimulation as much as they deem necessary during the trialin order to hopefully achieve satisfactory pain relief.
A positive response to the stimulator trial is a 50 % reduc-tion in pain from the baseline visual analog score and apermanent implant would be considered in these individuals.Those patients who pass the trial stimulation are brought backto the operating room where the actual implant takes place.General anesthesia is induced and typically the proceduretakes up to 2.5 h. A small incision is made above the zygo-matic process of the frontal bone and the lead is placed in asimilar manner and anchored to the underlying superficialfascia with a nonabsorbable suture. The next step is thetunneling of the lead and its extension to the internal pulsegenerator, which is placed in a superficial pocket in thesubclavicular area just above the pectoralis muscle.
Fig. 1 An octrode lead was implanted above the superior orbital margin(arrow)
Curr Pain Headache Rep (2014) 18:409 Page 5 of 7, 409

In the retrospective case series of 5 patients the maincomplication was skin erosion and secondary skin infection,which occurred in 2 patients [39••]. Interestingly, the skininfection occurred 1 year after the implant and required a leadrevision; however, the stimulation was successfully regained.
Extrapolating the supraorbital and supratrochlear implan-tation to the occipital nerve implantation, where many moreimplants have been performed, it is conceivable that othercomplications could arise if indeed this procedure gains morepopularity. These complications may include: lead migration,device malfunction with disconnection and lead fracture, painat the site of the lead or internal pulse generator, infections andallergic reactions to surgical material. (63).
Conclusions
Neuromodulation appears to become a frontline therapy forthose rare patients with TAC and intractable pain. Supraorbitaland supratrochlear stimulation should be considered alone orin combination with other extra cranial targets such as theoccipital nerve or the sphenopalatine ganglion.
Compliance with Ethics Guidelines
Conflict of Interest Julien Vaisman declares that he has no conflict ofinterest. Edrick Lopez declares that he has no conflict of interest. NicholasK. Muraoka declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Headache Classification Subcommittee of the InternationalHeadache Society. The international classification of headachedisorders: 2nd edition. Cephalalgia. 2004;24:9–160.
2. Rozen TD, Fishman RS. Cluster headache in the United States ofAmerica: demographics, clinical characteristic, triggers, suicidality,and personal burden. Headache. 2012;52:99–113.
3. Weiner RL, Reed KL. Peripheral neurostimulation for control ofintractable occipital neuralgia. Neuromodulation. 1999;2:217–21.
4. Son BC, Yang SH, Hong JT, Lee SW. Occipital nerve stimulationfor medically refractory hypnic headache. Neuromodulation.2012;15:381–6.
5. Bartsch T, Pameleire K, Goadsby PJ. Neurostimulation approachesto primary headache disorders. Curr Opin Neurol. 2009;22:262–8.
6. Frese A, Evers S, May A. Autonomic activation in experimentaltrigeminal pain. Cephalalgia. 2003;23:67–8.
7. Dodick DW, Rozen TD, Goadsby PJ, Silberstein SD. Clusterheadache. Cephalalgia. 2000;20:787–803.
8. Torelli P, Manzoni GC. Pain and behaviour in cluster headache. Aprospective study and review of the literature. Funct Neurol.2003;18:205–10.
9. Cohen AS, Burns B, Goadsby PJ. High-flow oxygen for treatmentof cluster headache: a randomized trial. JAMA. 2009;302:2451–7.
10. Treatment of acute cluster headache with sumatriptan. TheSumatriptan Cluster Headache. Study Group. N Engl J Med.1991;325:322–6.
11. van Vliet JA, Bahra A, Martin V, et al. Intranasal sumatriptan incluster headache: randomized placebo-controlled double-blindstudy. Neurology. 2003;60:630–3.
12. Abrams BM. Medication overuse headaches. Med Clin N Am.2013;97:337–52.
13. Goadsby PJ. Trigeminal autonomic cephalalgias. Continuum.2012;18:883–95.
14. Boes CJ, Dodick DW. Refining the clinical spectrum of chronicparoxysmal hemicrania: a review of 74 patients. Headache.2002;42:699–708.
15. Boes CJ, Vincent M, Russell D. Chronic paroxysmal hemicrania.In: Olesen J, Goadsby PJ, Ramadan NM, et al., editors. The head-aches. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2006.p. 815–22.
16. Silberstein SD, Vodovskaia N. Trigeminal autonomic cephalalgiasother than cluster headache. Med Clin N Am. 2013;97:321–8.
17. Cohen AS, Goadsby PJ. Paroxysmal hemicrania responding totopiramate. J Neurol Neurosurg Psychiatry. 2007;78:96–7.
18. Lambru G, Matharu MS. SUNCTand SUNA: medical and surgicaltreatments. Neurol Sci. 2013;34 Suppl 1:75–81.
19. Williams MH, Broadley SA. SUNCT and SUNA: clinical featuresand medical treatment. J Clin Neurosci. 2008;15:526–34.
20. Sillay KA, Sani S, Starr PA. Deep brain stimulation for medicallyintractable cluster headaches. Neurobiol Dis. 2010;38:361–8.
21. Goadsby PJ, Schoenen J, Ferrari MD, Silberstein SD, Dodick D.Towards a definition of intractable headache for use in clinicalpractice and trials. Cephalalgia. 2006;26:1168–70.
22. Hassenbusch SJ, Kunkel RS, Kosmorsky GS, Covington EC, PillayPK. Trigeminal cisternal injection of glycerol for treatment of chronicintractable cluster headaches. Neurosurgery. 1991;29:504–8.
23. Morgenlander JC, Wilkins RH. Surgical treatment of cluster head-ache. J Neurosurg. 1990;72:866–71.
24. Chatterjee N, Chatterjee S, Roy C. Abducens nerve palsy afterpercutaneous radiofrequency ablation of gasserian ganglion. JNeurosurg Anesthesiol. 2013.
25. Pieper DR, Dickerson J, Hassenbusch SJ. Percutaneousretrogasserian glycerol rhizolysis for treatment of chronic intracta-ble cluster headaches: long-term results. Neurosurgery. 2000;46:363–8. discussion 368–70.
26. Narouze SN. Role of sphenopalatine ganglion neuroablation in themanagement of cluster headache. Curr Pain Headache Rep.2010;14:160–3.
27. Kano H, Kondziolka D, Mathieu D, et al. Stereotactic radiosurgeryfor intractable cluster headache: an initial report from the NorthAmerican Gamma Knife Consortium. J Neurosurg. 2011;114:1736–43.
28. Oomen K, Wijck AV, Hordijk G, Ru JD. Microvascular decom-pression of the pterygopalatine ganglion in patients with refractorycluster headache. Cephalalgia. 2011;31:1236–9.
29. Melzack R, Wall PD. Pain mechanisms: a new theory. Science.1965;150:971–9.
30. Shealy CN, Mortimer JT, Hagfors NR. Dorsal columnelectroanalgesia. J Neurosurg. 1970;32:560–4.
31. Hosobuchi Y, Adams JE, Rutkin B. Chronic thalamic stimulationfor the control of facial anesthesia dolorosa. Arch Neurol. 1973;29:158–61.
409, Page 6 of 7 Curr Pain Headache Rep (2014) 18:409

32. Tsubokawa T, Katayama Y, Yamamoto T, Hirayama T, Koyama S.Treatment of thalamic pain by chronic motor cortex stimulation.Pacing Clin Electrophysiol. 1991;14:131–4.
33. AbejonD,Deer T, Verrills P. Subcutaneous stimulation: how to assessoptimal implantation depth. Neuromodulation. 2011;14:343–8.
34. Cairns KD, McRoberts WP, Deer T. Peripheral nerve stimulationfor the treatment of truncal pain. In: Slavin KV, editors. Peripheralnerve stimulation. Vol. 24. Progress in Neurological Surgery. Basel:Karger; 2011; p. 58–69.
35. McRoberts WP, Wolkowitz R, Meyer DJ, et al. Peripheral nervefield stimulation for the management of localized chronic intracta-ble back pain: results from a randomized controlled study.Neuromodulation. 2013.
36. May A, Bahra A, Büchel C, Frackowiak RS, Goadsby PJ.Hypothalamic activation in cluster headache attacks. Lancet.1998;352:275–8.
37. May A, Leone M, Boecker H, et al. Hypothalamic deep brainstimulation in positron emission tomography. J Neurosci.2006;26:3589–93.
38. Burns B,Watkins L, Goadsby PJ. Successful treatment ofmedicallyintractable cluster headache using occipital nerve stimulation.Lancet. 2007;369:1099–106.
39.•• Vaisman J, Markley H, Ordia J, Deer T. The treatment of medicallyintractable trigeminal autonomic cephalalgia. With supraorbital/supratrochlear stimulation: a retrospective case series.Neuromodulation. 2012;15:374–80. This gathers the largest groupof patients with TAC, treated with supra orbital/supratrochlearstimulation.
40. Slavin KV, Colpan ME, Munawar N, Wess C, Nersesyan H.Trigeminal and occipital peripheral nerve stimulation for craniofa-cial pain: a single-institution experience and review of the literature.Neurosurg Focus. 2006;21:E5.
41. Amin S, Buvanendran A, Park KS, Kroin JS, Moric M. Peripheralnerve stimulator for the treatment of supraorbital neuralgia: a retro-spective case series. Cephalalgia. 2008;28:355–9.
42. Reed KL, Black SB, Banta II CJ, Will KR. Combined occipital andsupraorbital neurostimulation for the treatment of chronic migraineheadaches: initial experience. Cephalalgia. 2010;30:260–71.
43. Asensio-Samper JM, Villanueva VL, Perez AV, et al. Peripheralneurostimulation in supraorbital neuralgia refractory to convention-al therapy. Pain Prat. 2008;8:120–4.
44. Narouze SN, Kapural L. Supraorbital nerve electric stimulation forthe treatment of intractable chronic cluster headache: a case report.Headache. 2007;47:1100–2.
45. Goadsby PJ. Neurostimulation in primary headache syndromes.Expert Rev Neurother. 2007;7:1785–9.
46. Schwedt TJ. Neurostimulation for primary headache disorders.Curr Neurol Neurosci Rep. 2009;9:101–7.
47. Wolter T, Kaube H, Mohadjer M. High cervical epiduralneurostimulation for cluster headache: case report and review ofthe literature. Cephalalgia. 2008;28:1091–4.
48. Vaisman J, Nimgade A. Refractory episodic cluster headache re-sponsive to percutaneous cervical zygapophyseal radiofrequencyablation: a case report. Headache. 2003;43:279–81.
49. Ansarinia M, Rezai A, Tepper SJ, et al. Electrical stimulation ofsphenopalatine ganglion for acute treatment of cluster headaches.Headache. 2010;50:1164–74.
50. Oluigbo CO, Makonnen G, Narouze S, Rezai AR. Sphenopalatineganglion interventions: technical aspects and application. ProgNeurol Surg. 2011;24:171–9.
51.• Schoenen J, Jensen R, Lanteri-Minet M. Stimulation of thesphenopalatine ganglion (SPG) for cluster headache treatment.Pathway CH-1: a randomized, sham-controlled study.Cephalalgia. 2013;33:816–30. This brings a unique and novel idea
to stimulate to sphenopalatine ganglion as a target for the treatmentof TAC.
52. Mueller OM, Gaul C, Katsarava Z, et al. Occipital nervestimulation for the treatment of chronic cluster headache—lessonslearned from 18 months experience. Cent Eur Neurosurg. 2011;72:84–9.
53. Burns B, Watkins L, Goadsby PJ. Treatment of intractable chroniccluster headache by occipital nerve stimulation in 14 patients.Neurology. 2009;72:341–5.
54. Magis D, Allena M, Bolla M, et al. Occipital nerve stimulation fordrug-resistant chronic cluster headache: a prospective pilot study.Lancet Neurol. 2007;6:314–21.
55. Jasper JF, Hayek SM. Implanted occipital nerve stimulators. PlainPhysician. 2008;11:187–200.
56. Dunteman E. Peripheral nerve stimulation for unremitting ophthal-mic postherpetic neuralgia. Neuromodulation. 2002;5:32–7.
57. Slavin K, Wess C. Trigeminal branch stimulation for intrac-table neuropathic pain: technical note. Neuromodulation.2005;8:7–13.
58. Johnson MD, Burchiel KJ. Peripheral stimulation for treatment oftrigeminal post-herpetic neuralgia and trigeminal posttraumaticneuropathic pain: a pilot study. Neurosurgery. 2004;55:135–41.discussion 141–132.
59. Aderjan D, Stankewitz A, May A. Neuronal mechanisms duringrepetitive trigemino-nociceptive stimulation in migraine patients.Pain. 2010;151:97–103.
60. Ordia J, Vaisman J. Subcutaneous peripheral nerve stimulation withpaddle lead for the treatment of low back pain: case report.Neuromodulation. 2009;12:205–9.
61. Popeney CA, Alo KM. Peripheral neurostimulation for the treat-ment of chronic, disabling transformed migraine. Headache.2003;43:369–75.
62. Serra G, Marchioretto F. Randomized trial occipital nerve stimula-tion for chronic migraine: a randomized trial. Plain Physician.2012;15:245–53.
63. Silberstein S, Dodick D, Saper J, et al. Safety and efficacyof peripheral nerve stimulation of the occipital nerves for themanagement of chronic migraine: results from a randomized,multicenter, double-blinded, controlled study. Cephalalgia.2012;16:1165–79.
64. Schoenen J, Vandersmissen B, Jeangette S, et al. Migraine preven-tion with a supraorbital transcutaneous stimulator : a randomizedcontrolled trial. Neurology. 2013;80:697. [Epub February 6, 2013].
65. Fontaine D, Lazorthes Y, Mertens P, et al. Safety and efficacy ofdeep brain stimulation in refractory cluster headache: a randomizedplacebo-controlled double-blind trial followed by a 1-year openextension. J Headache Pain. 2010;11:23–31.
66. Leone M, Franzini A, Broggi G, Bussone G. Hypothalamic stimu-lation for intractable cluster headache: long-term experience.Neurology. 2006;67:150–52.
67. Leone M, May A, Franzini A, et al. Deep brain stimulation forintractable chronic cluster headache: proposals for patient selection.Cephalalgia. 2004;24:934–7.
68. Schoenen J, Di Clemente L, Vandenheede M, et al. Hypothalamicstimulation in chronic cluster headache: a pilot study of efficacy andmode of action. Brain. 2005;128:940–7.
69. Schoenen J, Allena M, Magis D. Neurostimulation therapy inintractable headaches. Handb Clin Neurol. 2010;97:443–50.
70. May A. Cluster headache: pathogenesis, diagnosis, and manage-ment. Lancet. 2005;366:843–55.
71. Fernandez-de-Las-Penas C, Ortega-Santiago R, Cuadrado ML,Lopez-de-Silanes C, Pareja JA. Bilateral widespread mechanicalpain hypersensitivity as sign of central sensitization in patients withcluster headache. Headache. 2011;51:384–91.
Curr Pain Headache Rep (2014) 18:409 Page 7 of 7, 409


![Scravani - Facial Pain [Read-Only] · 13.4 – Superior laryngeal neuralgia 13.5 – Nasociliary neuralgia 13.6 – Supraorbital neuralgia 13.7 – Other terminal branch neuralgias](https://img.pdfslide.net/doc/110x75/5e9b9e94e532ce0d9f31854b/scravani-facial-pain-read-only-134-a-superior-laryngeal-neuralgia-135-a.jpg)











![Case Report Supraorbital Blowin Fracture Presenting as an ...downloads.hindawi.com/journals/crid/2013/574146.pdf · Journal of Oral and Maxillofacial Surgery ,vol., no., pp. [] M](https://img.pdfslide.net/doc/110x75/5f70896bea774871053a442d/case-report-supraorbital-blowin-fracture-presenting-as-an-journal-of-oral-and.jpg)