Embed Size (px)
Citation preview

SSUUPPRRAATTEENNTTOORRIIAALL DDUURRAAPPLLAASSTTYY WWIITTHH AANN
AABBSSOORRBBAABBLLEE SSYYNNTTHHEETTIICC MMAATTEERRIIAALL::
AANN EEXXPPRRIIMMEENNTTAALL SSTTUUDDYY IINN AA RRAABBBBIITT MMOODDEELL
Dissertation submitted to the Dr. M.G.R. Medical University,Chennai, for the final
M.Ch. Neurosurgery Examination, August 2015

CERTIFICATE
This is to certify that the dissertation titled ―" SUPRATENTORIAL DURAPLASTY WITH
AN ABSORBALE SYNTHETIC MATERIAL: AN EXPRIMENTAL STUDY IN A RABBIT
MODEL" is the bonafide original work of Dr.Brijesh Kumar Tiwari submitted in partial
fulfilment of the rules and regulations, for final M.Ch. Neurosurgery, examination of the Tamil
Nadu Dr. M.G.R. Medical University to be held in August 2015.
Signature of the Guide
Dr. Vivek Joseph
Professor of Neurosurgery
Dept of Neurological Sciences
Christian Medical College, Vellore.
Signature of Head of the Department Signature of the Principal
Dr. Mathew Joseph Dr. Alfred Job Daniel
Professor of Neurosurgery Christian Medical College
Department of Neurological Sciences Vellore
Christian Medical College, Vellore





ACKNOWLEGDEMENTS
I would like to thank to my guide Dr. Vivek Joseph and to my Co-guide Dr.Ranjith K Moorthy
and Dr. Geeta Chacko for all the encouragement, suggestions that helped me write this thesis and
also for the valuable time spent during the observations. They have taught me a lot and it is their
invaluable insight and constant guidance that has made this study possible.
I would like to express my gratitude Dr. Prabha Nair who gave me the concept of this thesis and
Dr. Natesan for his encouragement in this study.
Mr. Antony Raj and the Central Animal Facility have been kind to allow me to use the premises
at all the times of the day knowing that it was impossible to perform this study during the
scheduled working hours .
I am thankful to Dr. Shabari who helped me in making legends.
I thank the Animal Ethics committee and Institutional Review Board (IRB) of Christian Medical
College, Vellore for approving the conduct of this experiment and the Fluid Research grant for
funding this work.
I am thankful to the Almighty for his blessings and grace without which this would not have
been possible.
A special thanks to my parents, brothers and my wife who have been my support throughout this
study.

TABLE OF CONTENTS
SS..NNoo CCoonntteennttss PPaaggee nnoo..
1. List of Tables and Figures 1
2. Introduction 2
3. Literature Review 3
4. Aims & objectives 27
5. Materials & Methods 28
6. Results 35
7. Discussion 50
8. Conclusions 57
9. Bibliography 58
10. Annexure 64

1
LIST OF TABLES AND FIGURES
TABLE No Pg.No
1. Complications with the artificial dural substitutes. 15
2. Infection rates and CSF leaks rates with different artificial dural 24 substitute in the literature.
3. Infection rates and CSF leaks rates with different natural dural 25
substitute in the literature.
4. Post-operative monitoring of the rabbit. 32
5. Macroscopic assessment under magnification on the brain specimen. 34
6. Histological data. 38
7. Macroscopic assesment under magnification: 1 month group rabbit. 39
8. Macroscopic assesment under magnification: 3 month group rabbit. 41
9. List of rabbits sacrificed at 1 month: description of the demographics and 46 surgical outcome.
10. List of rabbits sacrificed at 3 month: description of the demographics and 47
surgical outcome.
11. List of rabbits with mortality as outcome and causes of death 48
12. Operative Outcome in rabbits following duraplasty. 49
FIGURES
Intraoperative images: Fig-1 30
Macroscopic findings under magnification operating microscope Fig 2-5. 37
Microscopic images of the brain and bone sections Fig 6-11a&b. 42

2
IINNTTRROODDUUCCTTIIOONN
Dural substitute is required for dural closure following dural loss as in trauma,
tumor excision and surgery for congenital malformations. The search for an ideal
dural substitute has been on for more than a century. Many materials like rubber and
metal foils were tried initially. These early results were discouraging.
Then, human cadaveric dura and bovine pericardium were used.
Studies suggested that these were good substitutes, but later there were reports of
Creutzfeldt–Jakob disease and slow virus diseases in patients in whom these were
used. Therefore, interest in the artificial dural substitutes was renewed, along with
procuring and processing procedures for disinfecting the naturally derived dura.
The ideal dural substitute should be inexpensive, readily available,
strong, malleable, easily sutured, immunologically inert, nontoxic, of uniform
thickness, form a watertight barrier, unlikely to adhere to the brain or cranium, and
not a source of infectious diseases

3
LITERATURE REVIEW
MORPHOLOGY OF THE DURA MATER
The dura mater is a continuous sheet of collagen surrounding intracranial and
spinal nervous structures.
It is firmly attached to the cranial vault and the skull base and reaches the foramen
magnum, where it divides into 2 layers. The outer layer forms the periosteum of the
spinal canal, and the inner layer forms the meningeal covering of the spinal cord and
the spinal nerve roots.
The dura mater has three layers when assessed by light microscopy.46 The
outer dural border layer, which is two microns thick, is the thinnest layer. It is
composed of fibroblasts with long cellular extensions and collagen and elastic fibres.
The median layer is the “fibrous dura”. It is vascularized and its thickness varies in
the cranial and spinal region. The innermost layer called the dural border cell layer is
eight microns thick and is composed only of cells that adhere to arachnoid trabeculae.
Marina Protasoni et al 47 did electron microscopic analysis of the collagen
architecture of the dura and they found the dura to have five layers. The outermost
layer that is in direct contact with the internal surface of the skull is the bone surface
layer. The median layer, previously identified by anatomists as fibrous dura, was
divided into three layers: the external median layer, vascular median layer, and
internal median layer. The innermost layer directly in contact with dural border cells
was called the arachnoid layer.

4
Collagen fibers in the median layer are variously arranged in three dimensions
forming three different layers: the external, vascular, and internal median layers. The
change in the direction of the collagen fibers is mostly visiblebetween the vascular
and internal median layers. Therefore, this site is subjected to the highest stretching
forces, representing a site of minimal resistance allowing neurosurgeons to
distinguish dura mater into 2 layers.
HEALING OF THE DURA DEFECT:
There is a vast knowledge of healing of the dural defect in experimental
animals, dating from 1938 (Glaser and Thienes 1). The studies have shown that the
neodura starts forming as early as seven days and the defect is completely covered by
a membrane of substantial thickness by 2 – 4 weeks. It has been also noted that the
healing is due to collagen layering by fibroblasts derived from the margins of the dural
defect and the overlying muscle (temporalis).
The usual complication during this healing process was
cerebromeningeal adhesions, which was less common when arachnoid was intact. This
in clinical practice is not always possible. The other interesting observation is that
adhesions are usually common in the early days of healing and gradually decrease over
time.

5
DURAL SUBSTITUTES:
The dural substitutes are of two types: Artificial and the Natural-derived.
artificialdural substitutes are also classified as absorbable and non-absorbable. In the
following paragraphs, the artificial and the natural-derived dural substitutes are discussed in
detail.
ARTIFICIAL DURAL GRAFTS:
Historical:
Abbe2 in 1895 presented to the New York surgical society, the use of Rubber
as a subdural graft. He had done trephining and successfully placed the rubber graft
subdurally over a cortical cicatrix that was causing intractable seizures. The patient
was seizure free after that during the one year and seven months of follow-up. There
was no mention of infection or CSF leak.
Captain Norman 3 experimentally used Tantalum foils as dural substitute in
dogs. Twelve dogs had undergone craniotomy and they had closed the dura with
subdurally placed tantalum foils. The cortex under the graft was damaged to study the
tissue reaction to the graft. They found significant thickening of the dura and
Dural substitute
Natural derived Artificial
Non-Absorbable Absorbable

6
arachnoid, with firm cortico-meningeal adhesions. Hence, they opined that use of
tantalum as a graft over a traumatised cortex was to be avoided.
Brown et al 4 tried polythene sheet as dural graft on animals. They tested it on
seven animals (dogs and monkeys) who were followed-up for variable duration, up to
six months. There were no C SF leaks or infection. The gross and histological
examinations showed a thin, non-adherent, subdural membrane. B ased on t hese
results, they used the polythene as dural graft in eleven patients for supratentorial
surgeries. One of the patients had a localized osteomyelitis and the graft was removed
along with a part of the bone flap. They felt that polythene graft was a good dural
substitute.
Paul Teng5 used Vinyon”N”, a synthetic fabric as dural substitute on e leven
monkeys. The period of observation varied from 21 da ys to 428 da ys. One of the
animals developed epidural abscess over the graft. They observed that there was no
neomembrane formation in all the animals. They also observed that meningocerebral
adhesions occurred only in the cases where edge-to-edge anastomosis of the graft was
done.
In 1961, same authors6 reported the use of the Vinyon”N”( Polyvinyl chloride
fibre polymerised with acrylonnitrile) in thirty-two patients as dural substitutes. They
followed-up the patients from four to fifty two months. In 15 patients, the dural
substitute was recovered at later date. They found no a dhesions. There was a
thickened scar on the outer surface of the graft and the inner surface was covered by a
thin transparent glistening membrane. They concluded Vinyon”N” was a satisfactory
dural substitute.

7
Huertas et al7 used type 81 Orlon ( synthetic acrylic fibre) as dural graft in
seven monkeys. They sacrificed the monkeys at one week to 15 month intervals.
They did not have any infection or CFS leak. The histological analysis showed small
adhesions with no ne omembrane formation. The suture sites had shown tissue
reaction covering the edges. They had used this material on a woman for dural repair
and she was followed-up for three months without any abnormality. They opined that
Orlon seemed to be an ideal material.
NON-ABSORBABLE ARTIFICIAL DURAL GRAFTS:
Sen Yamagata8 used expandable polytetrafluroethylene (ePTFE) in thirty-four
patients. They used it predominantly for cranial surgeries and a few spinal tumours.
Five patients had mild CSF accumulation and none had postoperative meningitis,
CSF rhinorrhea, or complications such as abscess. Six patients underwent re-
craniotomy for various reasons between one to fifteen months and they found the
graft to be thinning gradually. In the first month, few areas were semitransparent, by
4 months entire graft was semitransparent, and even at the end of 15 months the
strength of the graft was preserved. There were no adhesions. At fifteen months, they
also found a thin transparent granulation membrane between the graft and the brain.
They peeled the graft off the brain surface easily; hence, re-surgery was possible
without brain injury. They opined ePTFE was a suitable artificial dura. They also
wanted the ePTFE to be transparent so that they could check for bleeding below the
graft easily.

8
Nakagawa et al9 used ePTFE in eighty-three patients following
decompressive craniotomy for cerebrovascular diseases and traumatic brain injury in
the period of 1995 to 2000. Twenty-seven of them died within sixty days of surgery
and were not included in the study. Of the remaining fifty-six, eight (14.3%) of them
developed severe post-operative infections requiring re-surgery. The duration of
follow-up is not available. The authors had used cadaveric dura for duraplasty prior to
1995. The infection rate in these patients retrospectively was 16%. They had treated
these infections only with antibiotics. The authors concluded that ePTFE was
associated with a high rate of infection when compared to that of cadaveric dural
graft. They also suggested early removal of ePTFE graft, if infection occurs.
It should be noted that the infection rate in Nakagawa series is much higher
compared to other studies with cadaveric human dura, where the infection rate was
about 4%. These studies are discussed in naturally derived dural substitute section.
Messing-Junger et al10, in 2006 r eported a multicentric prospective
study assessing the effectiveness and handling characteristics of a three-layered
polymer dural substitute. The graft was made by sandwiching an elastomeric
fluoropolymer between two layers of ePTFE. They used the graft in 119 patients (102
cranial surgeries and 17 spinal surgeries). One hundred and three patients were
followed-up clinically and with imaging for average time of 15.7 months (range 0.3 –
45.6 months). Eighty-nine of them had imaging of the brain at least nine months after
the surgery. Imaging showed no adhesions in eighty-seven of them and minimal
adhesions in seven (6%) of them.
Twelve patients had developed post-operative complications with eight being
attributable to the graft. Six patients developed postoperative leak (5%), but none

9
needed surgical intervention. Two patients (1.96%) developed infections. One was a
superficial infection, which was treated with antibiotics. The other was bone flap
infection and the graft along with the bone flap was removed even though the graft
was not infected. A patient who had undergone a posterior fossa decompression with
duraplasty for Chiari 1 malformation developed arachnoid fibrosis requiring re-
surgery. Three patients developed extradural hematoma which was treated surgically
without graft removal. Two patients had undergone reoperation for tumour regrowth,
sixteen months after implantation. The removed graft was found to be intact and
thinned out. On histology, there was a thin membrane covering the graft with no
inflammatory or foreign body response to the graft. Hence, they concluded that the
three-layered ePTFE was a safe and effective dural substitute.
Bhatia et al 12 in 1995 reported the use of hydroxyethylmethacrylate (HEMA)
hydrogel sheets in rats and rabbits with no CSF leak or infection developing in either
group. They prepared the plain HEMA sheets from a mixture of ethylene glycol, 2-
HEMA and an aqueous buffer containing Tris-HCl and NaCl. Collagen HEMA sheets
had the same substrate with addition of solubilized rat-tail collagen in the aqueous
buffer.
They used rats and rabbits in the study. The rat study involved twelve animals
divided into three groups of four each. The first group underwent duraplasty with
HEMA sheets, the second group underwent sham-surgery and the third group
consisted of un-operated controls. All the groups had no CSF leak or infection. When
they had used HEMA, the histology of the operative site showed a band of connective
tissue at the edges of the graft extending from the leptomeninges to the overlying
surgical defect. In the sham rats, there was cortical herniation through the dural defect

10
with the histology showing a marked increase in connective tissue and some
thickening of the leptomeninges in all animals. The study with rabbits had five groups
involving craniotomy and duraplasty, laminotomy and duraplasty and control for both
the procedures.
They used thirty-seven rabbits in five different groups and sacrificed them six
or nine weeks after surgery. In a group of four rabbits, duraplasty was done with
collagen-HEMA. In another group of six rabbits, plain HEMA was used. They used a
sandwich of Collagen-HEMA and plain-HEMA in six rabbits. None of the animals
developed CSF leak. One animal in collagen-HEMA group developed wound
dehiscence.
In the control craniotomy-only animals, they noted no adhesions between the
brain and the intact dura. The plain HEMA duraplasty showed no a dhesions on
histology but collagen-HEMA showed excessive fibrosis on the brain surface and this
fibrosis was prevented by placing HEMA between the cortex and collagen-HEMA
graft.
They concluded that poly-HEMA based hydrogels were approaching an ideal
graft, but longer follow-up to exclude neomembrane formation was warranted.
Sakas14 in 1990 r eported Tecoflex EG-85 resin (a medical-grade aliphatic
polyurethane) and L R resin 3320 ( a polysiloxane-carbonate block copolymer) as
dural substitutes in rabbits. They used Tecoflex intracranially and intraspinally. There
were three groups of rabbits in whom the graft was used intracranially - it was placed
epidurally, subdurally or sutured to the dural margin. The graft size was 10 x 10 mm.
Each group consisted of 4 rabbits. A similar procedure was done with L R resin in
three groups, with four rabbits in each group. The graft size was 7 x 7 mm. The

11
Tecoflex was placed intraspinally in 12 animals divided in 2 groups (epidural or
sewn-in).
The rabbits were sacrificed 3, 6 or 9 months later and histological examination
was done of the graft. There was no C SF leak. The Tecoflex did not stimulate
formation of adhesions and pseudo membrane (neomembrane). The resin when
closed watertight or placed subdurally, stimulated formation of pseudo membrane but
without adhesions. They concluded tecoflex was more suitable than L R resin for
neurosurgical use as it was more inert and was biocompatible.
ABSORBABLE ARTIFICIAL DURAL GRAFTS:
Maurer et al15 used an absorbable synthetic Vicryl (Polyglactin 910) as dural
substitute in canines. They studied this on twelve dogs. In nine of them, the contra
lateral side also was operated on. N ative dura (in five), Gelfoam (in two) and
temporalis fascia (in two) were used to cover the defect. There were no CSF leaks or
infections. They did macroscopic observation and histological studies on the site of
dural replacement after sacrificing the dogs at predetermined intervals. The Vicryl
graft was reabsorbed by the 60th day and was replaced by a fibrous neomembrane.
There were no cerebromeningeal adhesions. At the end of twelve months, there was
no chronic inflammatory reaction noted in the Vicryl graft site. Gelfoam elicited the
greatest degree of inflammatory response with some leptomeningeal adhesions and
moderate neovascular invasion. The temporalis fascia graft formed a thick dural graft
with a modest amount of inflammatory response and neovascularity. It also had
occasional zones of leptomeningeal adhesions.

12
They reported another study in 1989 with Vicryl mesh on dogs50. This time
they used more tightly woven Vicryl as the graft. The macroscopic and microscopic
results were similar to the previous observation.
In 1997, Mello et al 16 reported the use biocellulose as a dural graft in canines
(32 dogs). They sacrificed the animals at various periods following implantation,
varying from one month to nine months. There were no CSF leaks or meningitis. Two
of animals developed local infections but the underlying neodura in them were
normal. The study revealed that cellulose when used as graft to cover defects resulted
in formation of a neodura around it (epidural and subdural). There was infiltration of
the cellulose graft by inflammatory cells and formation of collagen. The thickness of
the neodura and cellulose progressively increased in the first 30 days following which
it gradually decreased in the next 240 da ys. There were no a dhesions between the
neodura and the underlying brain irrespective of whether the underlying brain cortex
was injured. The authors concluded that the cellulose film was a suitable graft and a
long-term study was necessary to confirm this.
Yamada15 reported an animal study using composite graft material in 1997.
The composite graft consisted of a p olyglycolic acid (PGA) fabric sandwiched
between two sheets of L-lactic acid-e-caprolactone (50%L-lactic acid, 50% e-
caprolactone) copolymer. They studied the biodegradability by implanting the graft
material on the back of seventy-five rats. The dural substitute was completely
absorbed by end of 24 weeks. They then, they did duraplasty with the graft, in thirty-
one white rabbits, and observed them for periods ranging from two weeks to twenty-
six weeks prior to sacrifice. There were no i nfection, cerebrospinal fluid (CSF)
leakage, and convulsive disorders observed in any rabbit during the follow-up period.

13
After sacrificing the rabbits at the pre-planned period, histopathological
examination of the graft site for adhesions and neomembrane formation was done.
Two weeks post-surgery, a thin connective tissue completely enveloped the dural
substitute without any adhesion between the graft and underlying cortex with a few
inflammatory cells in the connective tissue. F our weeks after the surgery, the
collagenous layer around the dural substitute became thicker and fused with adjacent
dura mater, forming a dura-like tissue with very few inflammatory cells remaining in
the connective tissue. 12 weeks post-surgery histopathological examination revealed a
dura-like tissue fully regenerated in the placed of the dural substitute, which had been
completely reabsorbed, and there were no inflammatory cells remaining in the dura-
like tissue. In rabbits killed 24 weeks after surgery, the dura-like tissue was composed
of a dense network of well-oriented collagen fibers, a few scattered fibroblasts, and
capillary neovascularisation.
In all the experimental animals, they observed no change such as calcification
or significant adhesion between the dura-like tissue and the underlying cortex.
Keisuke Yamada11 (2002) reported the clinical application of a new
bioabsorbable artificial dura mater (GM 672) on fifty-three patients. GM 672 w as
composed of L-lactate- ε- caprolactone (50:50) copolymer film sandwiching PGA
nonwoven fabric. It was 220 micrometres thick.
They used the graft in fifty-three cranial cases, followed up for an average
period of 35.5 m onths (range 15 t o 54 m onths). The authors considered the
intraoperative handling as satisfactory. During the follow-up, fifteen patients had
developed postop subgaleal CSF collection (28.3%), all of whom were managed

14
conservatively. Another patient had poor wound healing leading to subcutaneous
abscess during radiation.
Four of these patients underwent recraniotomy for tumour recurrence. At
seven months after the initial surgery, they found that a neomembrane of varied
thickness with thin fragile areas had replaced the graft. Histology showed that the
neomembrane was composed of two thin layers of collagen fibers and fibroblasts. At
eighteen months, the graft was replaced by a firm collagenous neomembrane with
minimal adhesions. The histological assessment showed the dura-like membrane to
be composed of collagen bands and patent vessels.
The authors felt the GM972 was an ideal dural substitute for patients not
scheduled for elective surgery within a year after the duraplasty.
The above studies with various artificial dural grafts have shown that the
artificial dural substitutes are promising as they are easily available, sterile, pliable
and some are absorbable.
Complications with usage of the artificial dural substitutes for duroplasty:
Many anecdotal case reports of complications with non-absorbable materials
have been reported. The complications reported are delayed inflammatory reactions causing
inflammatory masses; hemorrhage from the inflamed tissue, deep infections and low
virulence infections. These complications occurred from two weeks to as late as 20 years.
(Table 1)

15
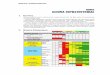
TABLE 1: Complications with the artificial dural substitutes.
NATURAL-DERIVED DURAL SUBSTITUTES:
The homologous or heterologous dural substitutes have been in use for more
than five decades. They were human cadaveric dura, bovine pericardium and porcine
small intestine. The cadaveric dural grafts were sterilized with ethylene oxide and
lyophilized (freeze-dried) for preservation. Lately, the collagen obtained from the
AUTHOR
MATERIAL
COMPLICATIONS
DURATION OF
IMPLANTATION
Adegbite17
Silastic dura
Inflammatory mass with bleed
Seven years
Ongkiko18
Silicon-coated Dacron
Inflammatory mass
Subdural hematoma
Six years
Nine weeks
Gudmundsson19
Collagen coated
Vicryl mesh
Brain abscess and deep infections
eleven days to
four weeks
Siccardi20
Silastic
Inflammatory mass with bleed
Ten years
Thompson21
Silastic
Subarachnoid haemorrhage;
Intracerebral and subdural hematoma
Two months ;
Eleven months
Robertson22
Silastic
Epidural hematoma
Nine to fourteen years
Cohen23
Marlex mesh
Inflammatory fibrosis with calcification
Twenty years
Ekseth24
Silastic
Inflammatory mass with bleed and low
virulent infection with
Propionibacterium acne
Thirteen to eighteen
years

16
bovine pericardium and Achilles’ tendons were used to synthesize the dural
substitute.
Sharkey et al 25 in 1957 reported the use of lyophilized human dura as dural
substitute in twelve patients. It was used for eleven cranial cases and one spinal case.
Three patients died within a month of implantation due to causes unrelated to the
graft. In the remaining nine patients followed for six to sixteen months, one
developed epidural abscess and another developed subdural abscess. The authors felt
the infections were not due to the graft and the lyophilized cadaveric dura was a
satisfactory dural graft.
Rosomoff et al26 studied twelve dogs, with fresh autogenous dura mater, and
lyophilized (ethylene oxide sterilized, freeze-dried) canine and human dura mater as
dural substitute. The craniotomies were done bilaterally allowing twenty-four grafting
sites. The cerebral cortex under the grafting site was injured on alternate animals. The
animals were sacrificed at intervals of 6, 12, 18 and 24 weeks. The histological
appearances of all grafts were described as showing scattered areas of round-cell
inflammation with or without calcification. The human dura mater evoked a more
prominent round cell inflammatory reaction and calcification. There was infiltration
of the grafts by fibroblasts and also evidence of neo-vascularisation. No foreign body
giant cells were seen except for a few talc granuloma. The underlying brain in dogs
without cortical injury showed no untoward reactions. The degree of adhesions in the
cortical-injured dogs did not differ with the type of graft. They concluded that there
was no s ignificant difference between the homologous dural graft and autologous
dura mater.

17
Macfarlane et al27 (1979) reported use of lyophilized human dura mater in
baboons and humans. Their initial experiment with six baboons, showed no cerebro-
meningeal adhesions. Microscopic examination of the lyophilized dura mater showed
fibroblastic infiltration of the dural collagenous framework. There were areas of
vascularization and ossification. They used the lyophilized human dura in one
hundred patients, 21 of whom underwent craniotomies and 79 s pinal or posterior
fossa decompressive procedures. At five months, there were eight CSF leaks (8%)
and five infections [wound infections (1%) and meningitis (2%)]. T hey concluded
the lyophilized dura mater was a good choice for duraplasty.
Parizek et al28 (1989) reported the use of gluteraldehyde treated calf
pericardium as dural graft in 160 p atients (children and adults). Only two of the
patients developed graft related complications (epidural infection in one and
reoperation for dural closure in the other). One of the children had developed multiple
complications following surgery for medulloblastoma, including tumour meningitis,
bacterial meningitis, and pseudomeningocele and eventually he succumbed to the
complications. The histopathological analysis the graft of the child revealed ingrowth
of host tissue into the margins of the graft and into the suture holes.
They analyzed the arrangement of the collagen in the pericardium, fascia lata
and dura. They found the collagen fibres were running parallel in the fascia, forming
laminae with crossing layers in the dura mater, and having a felt-like orientation in
the pericardium. As only two of the one hundred and sixty patients developed
complications, they felt allogeneic dura mater was an optimal substitute.
Laun et al 29 in 1990 r eported a prospective randomized study comparing
lyophilized human dura mater (HDM) and lyophilized bovine pericardium (BP) by

18
using them on 1 02 patients as dural substitutes. Both of them were used on 51
patients each. N one of the patients developed CSF leak in either group during the
unspecified period of follow-up. One patient in BP group developed subgaleal
empyema and one patient in HDM developed meningitis.
Nine patients in the bovine pericardium group underwent reoperation and
histological studies were conducted at the BP graft site. T he histology of the BP
suggested formation of neomembrane on either side of the graft. Most of the BP graft
was gradually absorbed over 24 months. Before implantation, the lyophilized bovine
pericardium consisted of a single layer with a three-dimensional array of slightly
curled collagenous fibers and interstitial spaces. In the four day post- implantation
specimen, there was migration of mainly fibroblasts and histiocytes into the implant
through the natural pores of the graft and along the interstitial spaces. In the three
months post-implantation specimen, the graft was half the thickness as the original,
due to the loss of the thick collagenous bundles. Polarization microscopy showed
newly formed delicate collagenous fibrils which firmly connected the residual graft
with the external and internal layers of the neomembrane. The eleventh month post-
implantation specimen showed a portion with well-preserved collagenous fibres with
continuous transition of collagenous fibres between the graft and the inner layer of
the neomembrane. This was demonstrated using polarization microscope. It also
showed that in the course of time the graft is progressively absorbed and replaced by
the neodura. In the post twenty-four months implantation specimen only a small layer
of the implant remained which was reduced to approximately one tenth of its original

19
thickness. An excellent incorporation into the host membranes was shown by the
polarization microscopy.
They also assessed the intraoperative handling of the grafts and found
the bovine pericardium was more pliable. Based on all these findings, they concluded
that that lyophilized bovine pericardium seems to be better than lyophilized human
dura mater for the repair of dural defects.
Cantore et al30 in 1987 r eported the use of ethanol soaked gamma radiated
cadaveric human dura in 804 pa tients. During the follow-up of the patients for an
unspecified period, 755 (93.9%) had no c omplications. Forty cases (6.0%) had
infections: 28 (3.4%) had wound infections and 22 (3.1%) had meningitis. They felt
that these complications were not due to the graft and the infection rates were in
accordance with similar surgeries without graft at that time in their institution. They
concluded alcohol preserved cadaveric dura was fit for use,
Xu Bang-Zong31 et al in 1988 r eported the use of processed porcine
peritoneum as a dural substitute in dogs and humans. First, the animal study was
carried out in which 20 dogs underwent 43 craniotomies. The postoperative
monitoring duration ranged from 62 to 124 days (average was 102 days) after the first
operation in the original group of 20 do gs. Fifteen of these twenty dogs were re-
operated and followed-up for 210 to 300 days, eight of these fifteen dogs underwent
third surgery and were followed-up for 1 year. They did not report any CSF leak or
meningitis during this time. There were two wound infections.
Histological analysis showed that the bio-membrane consisted mainly of
fibrous connective tissue. Vascularization of the tissue was found in eight cases,
osteotrabeculae in two, and slight infiltration of chronic inflammatory cells in three.

20
A large number of phagocytes were found in the specimens from the two dogs with
incisional infections. The cerebral cortex was normal in 13 do gs and showed mild
infiltration of inflammatory cells with astrocytic proliferation in two dogs.
The electron microscopy of the porcine bio-membrane showed a regularly
arranged collagen and elastic fibres similar to dura mater. There were a f ew
fibroblasts in the dura mater with intact cell membrane, mitochondria and rough
endoplasmic reticulum. Post-implantation graft showed collagenous strands
predominantly regular in arrangement with islands of irregular collagen. There was
evidence of proliferative fibroblasts in the graft.
Based on the encouraging animal study results, they used it in 614 patients for
dural repair. Of these 571 were supra-tentorial surgeries, 41 pos terior fossa and 2
thoracic spine surgeries. Of the cranial surgeries, 393 were following acute head
injury. The follow up p eriod was ranged from 3 months to 5 years. One patient
developed wound infection. There were no CSF leaks. Two other patients underwent
re-craniotomy for secondary lesions, during which graft was assessed and no
significant adhesions were indentified. There were no hi stological studies done.
Electroencephalogram was done pre and post operatively on 613 pa tients and no
abnormality was detected. Thus, the authors concluded that the porcine bio-
membrane (peritoneum) to be an ideal dural substitute.
Laquerrier et al 32(1993) reported the use of bilayered collagen, derived from
human placenta, as dural substitute on canines. They had two types of substitutes, a
collagen bilayered dural substitute made of oxidized type III + I collagen layer,
covered by a type IV oxidized collagen film (collagen dural substitute I) and a
collagen bilayered dural substitute made of oxidized type III + I collagen layer,

21
covered by a type III+ I collagen film (collagen dural substitute II). Both the types
were used on s ix dogs forming two groups, which were sacrificed at predetermined
times.
Post-operatively the animals of either group did not develop wound infection,
CSF leak or meningitis. They sacrificed the animals at 15, 30, 90, 120 and 180 days
after implantation of the graft. The graft along with underlying brain was removed
and analyzed. The histology showed that the neodura started forming by 30 days and
was completed by 90 d ays and the graft was absorbed by that time. One animal
sacrificed at 180 days of the second group had a small adhesion to the cortex.
They concluded that the composition and the structure of the collagen dural
substitute was important to obtain effective healing and repair of dural defects. These
results showed that new biomaterials made of human collagens can be developed for
grafting.
Cormac O Maher et al 33 (2003) reported the use of bovine pericardium
derived acellular collagen matrix as a dural substitute in rabbits. T heir study
consisted of three arms with native group, control group and experimental group. In
control group, they used a conventional gluteraldehyde cross-linked bovine
pericardium–derived dural substitute. The study was done on 46 r abbits with eight
groups. In the native and control dura groups, the rabbits were sacrificed at first and
sixth week. In the experimental group, the rabbits were sacrificed at 1, 2, 4 a nd 6
weeks. They studied the tightness of the closure using Fillipi technique34. They also
studied the graft thickness, adhesions, vascularity and spindle density in the various
groups at the time periods mentioned above.

22
They found that the native dura was very friable and not suitable for suturing.
CSF leaks at 6 weeks were more common than at 1 week (63 and 12%, respectively).
They occurred more frequently in animals in which native dura had been used than in
those receiving the control or experimental grafts. Native dura mater and the control
dura substitute tended to increase in thickness over 6 weeks, the experimental graft
decreased in thickness. Dural thickness was lowest in native dura, followed by control
graft, and finally by the experimental graft at both 1 and 6 weeks. Time did not have a
significant influence on adhesion grades (Park and Tator). 48 Their experimental grafts
never had adhesions covering the entire duraplasty, whereas at 6 weeks they had one
such case among specimens from the native dura group and 42% of the control group
were grade 3. (contiguous adhesions covering the entire duraplasty site)
There was difficulty of removing the craniotomy flap after convalescence
without causing dural tears. These occurred in four of their rabbits, two in the native
dura group at 6 weeks and two in the control graft group at 6 weeks. They recognised
the tears when they removed the bone flap and during the test of leakage pressure.
They felt collagen matrix derived from propylene oxide-treated bovine pericardium
was suitable as graft material for dura mater and further human studies were
necessary to ascertain the usefulness in humans. (Table 2 and 3)
Kadioglu36 (2002) reported a rabbit study with dehydrated human dura and
autologous fascia lata as dural substitutes. They studied ninety rabbits divided into
three groups. They studied the immune response to the dural substitutes. They found
the host inflammatory response to the autogenous fascia lata was more intense than
dehydrated human dura graft, which was characterised by polymorphic leucocytes

23
dominance in the first days. It changed to mononuclear dominance in the course of
the time. The fibroblastic proliferation was assessed and maximum in the dehydrated
dura group. The foreign body reaction was also prominent in the dehydrated dura
group. Cortical adhesions and capsulation of the graft were seen both with autologous
and human graft. The cortical adhesions showed decreasing trend after 60 da ys of
implantation.
Narotam35 (2007) used a collagen-matrix based dural substitute on s eventy-
nine patients. Fifty-seven patients of these underwent a supratentorial procedure and
rest underwent either a posterior fossa surgery or spinal surgery. They were followed-
up after three months with clinical examination and MR imaging with Gadolinium.
Only Sixty-three patients (79.7%) were available for follow-up. 3.8% of the patients
(3 of 79) developed infections. Two of them were superficial and one was deep
infection (osteomyelitic bone flap and brain abscess).
Imaging after three months revealed asymptomatic small pseudomeningoceles
in two (2.5%); a minor subgaleal fluid collection, which resolved spontaneously in
another patient (1.6%). Nonspecific dural enhancement was in seven patients
(11.1%), and asymptomatic spinal epidural enhancement was observed in two of
three patients who had undergone lumbar laminectomy for spinal stenosis. The author
concluded that collagen-matrix based dural graft was a suitable dural substitute.

24
INFECTION AND CSF LEAK RATES:
Table 2: Infection rates and CSF leaks rates with different artificial dural substitutes in
literature.
S.No MATERIAL AUTHOR SUBJECTS INFECTION RATE CSF LEAK
RATE
1. GM972 Yamada15 31 rabbits Nil Nil
2. HEMA hydrogels Sanjiv Bhatia 12 12 rats and 37
rabbits Nil Nil
3. Vicryl Maurer13 12 dogs Nil Nil
4. Tecoflex & LR resin Sakas14 36 rabbits Nil Nil
5. Biocellulose Mello 18 32 dogs 6.25% (superficial) Nil
6. ePTFE Yamagata8 34 humans Nil Nil
7. ePTFE Nakagawa9 56 humans 14.3% (deep) Nil
8. ePTFE Martina10 103 humans 1.94% (superficial
and deep)
5.8%
9. GM 972 Yamada11 53 humans Nil
Nil 28%
Subgaleal
collection

25
Table 3: Infection rates and CSF leaks rates with different natural dural substitute in
the literature:
S.No MATERIAL AUTHOR SUBJECTS INFECTION
RATE
CSF LEAK
RATE
1 Lyophilised Human
Dura (LHD)
Rosomoff 26 12 dogs 8.3% Nil
2 LHD Macfarlane 27 6 baboon Nil Nil
3 Porcine pericardium Xu Bang-Zong 3 20 dogs 10%(superficial) Nil
4 Human placenta based
collagen dura
Laquerrier 32 12 dogs Nil Nil
5 Bovine pericardium
(BP) derived collagen
Cormac 33 46 rabbits Nil Nil
6 Dehydrated human dura Kandioglu 36 90 rabbits Nil Nil
7 LHD Macfarlane 27 100 humans 5%
(1% superficial &
4% deep)
8%
8 Calf pericardium Parizek 28 160 humans 0.62 % (deep) 0.62%
9 LHD
LBP
Laun 29 51 humans
51 humans
2 % (deep)
2 % (deep)
Nil
10 Gamma radiated HD Cantore 30 804 humans 6 % Nil
11 Porcine pericardium Xu Bang-Zong 3 614 humans 0.16% nil
12 LHD Sharkey 25 12 humans 8.3% (deep) Nil

26
The above discussion about natural-derived dural graft shows that xenografts
are generally well tolerated, stimulate formation of neodura and are absorbable.
Though the xenogenic grafts can stimulate some foreign body reaction and aseptic
meningitis, these are close to an ideal dural substitutes.
However, there is a possibility of slow virus infections and prion diseases.
The potential transmission of spongiform encephalopathy through the use of
cadaveric grafts has been reported for more than three decades now (37-45). In 1987,
Prichard37 reported Creutzfeldt-Jakob disease (CJD) in a twenty year woman who had
undergone a duraplasty with processed human dura two years ago. Following this
multiple cases were reported around the world, maximum being from Japan. Centres
for Disease control and prevention (CDC) reported four cases of CJD following
similar implantation in Spain by 1992. An update by CDC in 2003 about Japan stated
97 patients had developed CJD following use of processed human dura. The
estimated minimum risk of CJD within 17 years from the above data is one case per
1,250 grafts.
Though multiple techniques for sterilisation have been used, the fear of these
fatal and disabling diseases does persist. The above-mentioned studies regarding
various artificial and natural dural substitutes show us the wait for the ideal dural
graft continues.

27
AIMS AND OBJECTIVES
Aim of the study: To study the efficacy of an absorbable synthetic material as a
dural substitute.
The parameters to be studied:
- Incidence of post-operative CSF leaks
- Incidence of the wound infections
Macroscopic under magnification
Histological findings
Inflammatory response in the brain and the graft
Adhesions- Between brain and the graft, skull and the graft.
Thickness of the Neodura
Resorption of the graft
.Inclusion criteria: Young healthy rabbits.
Exclusion criteria: None

28
MATERIALS AND METHODS
Study Design:
The experiment was designed to study the benefits of an artificial absorbable
material (polycaprolactone) as a dural substitute. Polycaprolactone is a biodegredable
polyester. This is a descriptive prospective randomised animal study using rabbits as
animal model. Sixteen rabbits (each 7-8 months of age) with one side as control dura
(N) and the other side as experiment dura (P). Each rabbit underwent biparietal single
craniotomy and 1 x 1 c m dura excised on t he P side with onlay graft using
polycaprolactone material while in the N arm, native dura was replaced back without
suturing The rabbits were monitored for signs of infection, CSF leak, wound infection
and graft rejection. Six rabbits each were sacrificed at 30 and 90 days respectively
and brains were harvested with intact dural covering. Four rabbits died due to non-
neurosurgical complications and were not included for analysis. Of the harvested
brains gross assessment for adhesions, resorption of artificial dura and neodura
formation was done under operative microscope.
Operative procedure:
The rabbits were anaesthetized by intramuscular (gluteal or quadricep muscle)
namely, Inj. Ketamine 35mg/kg/ and Inj. Xylazine (10 mg/kg). After the onset of
sedation i.e. after 10 minutes, the rabbit's head was shaved. Over the selected surgical
field, povidone iodine 10%, an antiseptic solution, was applied. Single dose of
prophylactic antibiotic (Ciprofloxacine 7 mg/kg) was given. Single dose of analgesic
(Nimesulide 5 mg/kg) was administered intramuscularly.

29
On the operating table, over a thermal blanket, the animal was
placed in the prone position. With the nasal prong the continuous oxygen was
delivered to the animal. The scalp was drapped. A midline skin incision was made
which extended from the nasal to the parietal region. After reflection of the scalp and
the underlying tissues, the calvarial bones were uncovered. A small burr hole was
created on the frontoparietal suture 2 cm from the midline using a high-speed drill. A
single biparietal craniotomy of 2 x 2 cm was done with the help of 1 mm bone
rongeur (no.1).
Immense care was exercised so as to evade the chances of perforation of the
dura mater and the sagittal sinus. To minimize the thermal damage during the bone
drilling, sterile saline was continuously poured on the surgical field. 1 x 1 cm
duratomy was done on either side with careful preservation of the superior sagittal
sinus.
In the P arm (experiment side) the defect was replaced by synthetic material
polycaprolactone (1x1cm) while in the N arm (control side), the native dura (1x1 cm)
was lifted up leaving it hinged on the medial edge and replaced back without suturing
it.
Haemostasis was achieved. Bone flap was replaced back as well. Without any
drain, wound was also closed in a single layer using 3-0 Ethilon with continuous
suture. Afterwards, using the betadine dressing the wound was completely covered.

30
Intraoperative images: Fig-1

31
Care of the Rabbits:
Pre-operative care
The research was done on sixteen New Zealand white healthy rabbits, both
male and female were chosen; each weighing between 1.5 kg to 3.5 kg. At least two
weeks after receiving the animals, the experiments were started. This was done for the
purpose of proper quarantine and acclimatization of the rabbits. An animal house was
used for keeping them; each rabbit was kept in single perforated cage with unlimited
access to food and water. The room temperature was maintained between 24-28° C.
Before surgery, no preoperative fasting was done and no antibiotic was started.
Post-operative care:
Post operative antibiotics or analgesics were not given. Immediately after
surgery, the rabbits were kept in an open area where they had easy access to food and
water. On the next day after the surgery, examination for neurological deficits was
done after which the rabbits was transferred to their cages.
For a period of 1 week, locomotor activity, convulsions, salivation. general
behavior, urination and defecation were monitored every day. Every week food
consumption and body weight and temperatures were checked. The surgical wound
was examined every day to look for infection or CSF leak. Sutures were removed on
the seventh postoperative day.

32
Macroscopic Gross assessment on the brain specimen:
At the end of pre-determined time, at one month and three months, six rabbits
were sacrificed with intramuscular high dose phenobarbital respectively. After the
confirming the death of the animal, the scalp wound was reopened and the skin flap
was carefully reflected away to expose the craniotomy site.
The craniotomy bone flap along with normal bone margin, underlying dura,
the graft zone and subjacent brain were removed as one specimen and fixed in
formalin. The bone flap was reflected off the brain under operative microscope
(NC4,Carl Zeiss) and the findings were noted. (Table 4)
Table 4: Macroscopic assessment under magnification on the brain specimen
Rabbit S.No: Right side Left side
Bone flap to dura adhesion (Y/N)
Brain to dural adhesions
Dural defect
Graft seen (Y/N)
Comments

33
Gross and microscopic examinations of the bone flap, dura, graft zone and the
underlying brain parenchyma were conducted. The brain was examined grossly
particularly while removing the overlying cranial vault with dura to look for any
visible adhesions. Appropriate photographs were taken with proper labelling. The
area of interest and the right side of the brain were marked.
Serial sectioning of brain (from anterior to posterior) was done and cut surface
was examined. Bone was kept for mild decalcification and processed as described
below. Three tissue bits were taken and processed in small cassettes using Automatic
Tissue processor for 16-18 hours in which the tissue passes through formalin, graded
alcohol, xylene and paraffin wax.
Paraffin embedded tissue blocks were prepared and 5 micron thick sections
were cut using microtome. All the sections were stained with hematoxlyin and eosin.
All the slides were examined and findings were noted in the already set proforma.
(Table 5)

34
Table 5: HISTOLOGICAL DATA
Criteria Control Graft Remark
Adhesion
Inflammatory response in the
brain
(Absent/ Minimal/
Moderate/Severe)
Centre
Inflammatory response grade
(Grade 0;1;2;3)
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response
grade
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response
grade
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Giant cell reaction (Present or
absent)
Edge - 1
Inflammation (present or absent
Giant cell reaction (Present or
absent)
Edge - 2
Inflammation (present or absent)
Giant cell reaction (Present or
absent)
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Neodura Thickness (microns / mm) Thickness of graft (microns / mm)

35
RESULTS
Total of 16 rabbits were being operated.
Mortality
The first 4 rabbits died due to non neurosurgical causes (Table 10) and the
remaining 12 rabbits survived till the date of sacrifice.
Morbidity
One rabbit developed paraparesis (Rabbit No.7) which gradually improved
and the animal was sacrificed at 3 month interval.
CSF Leak and Wound Infection
There were no incidence of infection at the operated site, no cerebrospinal
fluid (CSF) leakage, and convulsive disorders observed in any rabbit during the
follow-up period.
General Behavioural Condition and Wound Healing
There was no fever, weight loss or reduced locomotor activity. The scalp
wound healed well in all the cases within 7 days.

36
Macroscopic Findings under Magnification
On examining the bone flap under operating microscope (NC4,Carl Zeiss) the
following findings were seen. Among the one month group at the graft site (P arm), a
thick coagulum (Fig-2) was seen at the site of the dural defect. A thin layer of the
graft impression was seen ( Fig-3) in three months group. Adhesions were seen
between brain and the graft in two rabbits only (rabbit no 4, Fig-4 and rabbit no 11,
Fig-5). On the N arm side no coagulum or adhesions were seen. (Table 6)
Among the three month group at the graft site (P arm), the graft was
completely absorbed leaving behind a smooth area over the coagulum and there was a
thin coagulum which was completely fused with the normal surrounding dura. On the
N arm it was same as that in the one month group. (Table 7)

37
Macroscopic findings under magnification operating microscope (NC4,Carl
Zeiss 300x)

38
Table 6: Macroscopic assessment under magnification on the brain specimen
1 month group rabbit
Rabbit S.No
Experiment (P/Control N)
Bone flap to dura adhesion (Y/N)
Brain to dural adhesions (Y/N)
Dural defect
Graft seen (Y/N)
Comment
1 P (Left) N N Seen N Thick coagulum seen at the graft site
N (Right) N N
2 P (Right) N N Seen N Thick coagulum seen
N (Left) N N N
3 P (Right) N N Seen N Thick coagulum seen at the graft site
N (Left) N N N
4 P (Right) N Y Seen N Thick coagulum seen at the graft site
N (Left) N N N
5 P (Right) N N Seen N Thick coagulum seen at the graft site
N (Left) N N N
6 P (Right) N N Seen N Thick coagulum seen at the graft site
N (Left) N N N

39
Table 7: Macroscopic assessment under magnification on the brain specimen
: 3 month group rabbit
* This was the first rabbit which was studied and the skull was discarded. In
all the other rabbits the skull was used for macroscopic and histopathological
examination.
Rabbit S.No
Experiment (P/Control N)
Bone flap to dura adhesion (Y/N)
Brain to dural adhesions (Y/N)
Dural defect (Y/N)
Graft seen (Y/N)
Comments
7 P (Left) N *No bone flap available
N (Right) N
8 P (Right) N N N N Flat area present on the coagulum
N (Left) N N N
9 P (Right) N N N N Thin coagulum with flat area seen
N (Left) N N N
10 P (Right) N N N N Thin coagulum with flat area seen
N (Left) N N N
11 P (Right) N Y N N Thin coagulum with flat area seen
N (Left) N N N
12 P (Right) N N N N Thin coagulum with flat area seen
N (Left) N N N

40
Histopathological Findings
One month group: There were no adhesions seen between the graft and the
bone or between graft and the brain parenchyma. There was inflammation seen (n=6)
in the brain of one rabbit on the experimental side (rabbit no.6). There was
fibroblastic proliferation (n=6) seen over the brain surface in 3 rabbits in the
experimental side and 2 in the control side. Foreign body granulomatous
inflammation was seen in all the 6 rabbits at the graft site. There was no neodura
seen. (Table 8)
Three month group: There was no cerebro-graft adhesion, or adhesion
between the graft and the bone. There was inflammatory reaction in the brain on the
experimental side in one rabbit (no. 7) (Fig-6). There was no fibroblast proliferation
(n=6) seen over the brain surface on the experimental side, but two rabbits showed
fibroblast proliferation over the brain surface on the control side. . Foreign body
granulomatous inflammation was seen (n=5) at the graft site. There was no neodura
seen.
Also, there was hyalinised nodule seen in the brain parenchyma of rabbit no-9
(Fig-7) and presence of rarefaction in rabbit no.10 (Fig-8), and foamy macrophages
over the surface of the brain in rabbit no-10. Foreign body granuloma was seen on the
brain surface of the rabbit no-12.( Fig-9) (Table 8)

41
Table 8: Histological Findings
* Bone flap along with the graft was not available for one rabbit in three month group
Criteria 1 Month (n=6) 3 Months (n=6)
Experiment P Control N Experiment P
Control N
Adhesion between bone & graft
0/6 0/6 *0/5 *0/5
Adhesion between graft & brain
0/6 0/6 *0/5 *0/5
Inflammation in the brain
1/6 0/6 1/6 0/6
Inflammation in the graft
6/6 0/6 *5/5 *5/5
Fibroblast proliferation
3/6 2/6 0/6 2/6
Thickness of neodura
Nil Nil Nil Nil
Resorption of graft 6/6 *5/5

42

43

44
There was chronic inflammatory changes seen in the form of foamy cells
and fibrosis of the leptomeninges in eight rabbits (Fig-10). There was no graft seen
either in the one month or the three month group rabbits but there was foreign body
type granulomatous inflammation seen in all rabbits ( Fig-11 a & b)) and there was
no neodura seen

45

46
Table 9: List of rabbits sacrificed at 1 month: description of the demographics
and surgical outcome.
Rabbit
S.No.
Age
(in months)
Weight
(in grams)
Surgical wound
Neurological status
1 11 3500 Healthy No deficits
2 6 2000 Healthy No deficits
3 6 1750 Healthy No deficits
4 6 1700 Healthy No deficits
5 6 1500 Healthy No deficits
6 6 1800 Healthy No deficits

47
Table 10 : List of rabbits sacrificed at 3 month: description of the demographics
and surgical outcome.
Rabbit
S.No.
Age
(in months)
Weight
(in grams)
Surgical wound Neurological status
7 12 2700 Healthy paraparesis
8 9 2800 Healthy No deficits
9 8 2700 Healthy No deficits
10 8 3000 Healthy No deficits
11 6 1600 Healthy No deficits
12 6 1900 Healthy No deficits

48
Table 11: List of rabbits with mortality as outcome and causes of death
Neurological causes considered were operative hemorrhage, post operative
hematoma, seizures and meningitis.
Rabbit no. Day of
death
Cause of death by autopsy Neurological
cause
(Yes / No)
A 0 Unknown No
B On table Anesthesia overdose No
C 3rd Respiratory tract infection
(Pasteurella pneumotropica )
No
D 3rd Septicemia (Heart sample:
NFGNB and Klebsiella sp.
Brain sample : No growth
No

49
Table 12: Operative Outcome in rabbits following duraplasty.
Parameters Number of rabbits
Total number of rabbits 16
Total mortality 4
Morbidity: (of the survived 12 rabbits)
Wound infection 0
Clinical meningitis 0
CSF leak 0
Fever 0
Anorexia 0
Neurological deficits 1

50
DISCUSSION In the literature most of the animal experiments for the dural graft was done on
dog, rat or rabbit with sample size varying fron 12 to 36. The animal ethics committee
allotted a sample size 12, with the experimental and control on either side in the same
rabbit.
Dural Substitutes There are various materials used for the closure of dural defects ,which have
been extensively reviewed. The artificial nonresorbable materials materials such as
metal foils or alloplastic substitutes like Vinyon, Nylon, Dacron, and Silastic have
been used in the past.
These materials have a number of drawbacks as they can remain as permanent
foreign bodies, cause extensive inflammatory reaction, induce the formation of
unusual vascularity with long-term delayed hemorrhage or hematoma, or produce
neural compression by infolding.
Nakagawa et al 9 used ePTFE and concluded that ePTFE was associated with
a high rate of infection ( 4%) when compared to that of cadaveric dural graft.
Though the h omologous or autologous tissue grafts (such as fascia or
pericranium) have been extensively used as effective dural substitutes. The potential
risk of latent virus

51
infection remains the main disadvantage in the with homologous tissue graft. Cantore
et al30 in in a study of 804 patients found 3.4% had wound infections and 3.1% had
meningitis.
Although the autologous grafts like fascia and pericranium are often adequate
as dural substitute tissues but extensive dura loss from neoplastic invasion or trauma
preclude its use.
Absorbable, Dural Substitutes
Completely resorbable material which was used earlier like porcine or
bovine collagens showed granulomatous inflammation around a permanent foreign
body and the resorption time was as long as 6 to 8 m onths and generally led to
fibrosis.
Maurer et al15 used Vicryl (Polyglactin 910) and compared it with Gelfoam
and temporalis fascia. The Vicryl graft was reabsorbed by the 60th day and was
replaced by a fibrous neomembrane and there were no cerebromeningeal adhesions .
The Gelfoam elicited the greatest degree of inflammatory response with some
leptomeningeal adhesions and moderate neovascular invasion. The temporalis fascia
graft formed a thick dural graft with a modest amount of inflammatory response and
neovascularity. It also had occasional zones of leptomeningeal adhesions.

52
Wound infection and postoperative CSF leak:
Mello et al 18found that the infection rate in artificial dural graft with
Biocellulose was 6.25% with nil CSF leak rate in an experimental study on 32 dogs.
Yamada15 used polyglycolic acid (PGA) fabric sandwiched between
two sheets of L-lactic acid-e-caprolactone (50%L-lactic acid, 50% e-caprolactone)
copolymer as dural substitute on 31 rabbits. The results were favourable with no CSF
leak and infection .
However on human experiment in 53 cranial cases the same
material showed postop subgaleal CSF collection (28.3%) and subcutaneous abscess
(1.8%).
Maurer et al 13 who used Vicryl in 12 rats and 37 rabbits found 0%
infection rate and CSF leak ,similar result was obtained by Bhatia et al12 in 12 rats
and 37 rabbits using HEMA as dural substitue. In our study also there was no wound
infection or CSF leak.
Macroscopic under magnification
None of the animal study have used operating microscope to view
the brain and the graft site. We used operating microscope (NC4,Carl Zeiss, 300x)
and found, a thick coagulum at the site of the dural defect in all the rabbits
sacrificed at one month, but there was no adhesion (except rabbit no 4 and 11) which
had adhesion with the brain parenchyma). On the N arm side no coagulum or

53
adhesions were seen. There was reduction in the thickness of the coagulum with
central smooth area seen in 5 of the 6 rabbits sacrificed at three months
Histological findings:
Graft absorption:
In most of the animal studies the absorbable dural substitue absorbes by
90- 180 days , Yamada et al 15 used bioabsorbable PGA fabric and an L-lactic acid- e-
caprolactone copolymer in 31 rabbits found the same. The graft completely dissolved
and was replaced by connective tissue within 6 months.
Neulen et al 51 using bilayered collagen on 34 pigs found only 12.5% graft
absorption at 4 week post implant.
Maurer et al 13 found significant resorption of vicryl mesh on 45 post op day.
Charles et al 50 in a study on 10 dogs sacrificed between 48 hours to 6 months
found that vicryl was almost absorbed after 40 days.
In our study also we found that at one month and the three months group
rabbits there was no histological evidence of graft. There was mild acute
inflammatory reaction in the brain in two rabbits (16.67%) on the side of the graft (no.
6 and no. 7) and there was chronic inflammatory changes seen in the form of foamy
cells and fibroblast proliferation on the brain surface in eight rabbits (66.66%). There
was no neodura seen.

54
Rarefaction:
Bhatia et al 12 used hydroxyethylmethacrylate (HEMA) hydrogel
sheets in 12 rats and 37 rabbits and found variable degree of cortical destruction and
the surrounding tissue and thinning of the cortical layer, increase in the glial cells and
distortion of the neuronal layer II among the rat series, he attributed this to injury
during surgery. In the rabbit group also he found minimal thinning of cortical layer I,
a mild increase in glial cells, and minimal distortion of neurons in layer II
In our study only one rabbit ( rabbit no-10) showed rarefaction of the brain
parenchyma suggestive of neuronal loss. The underlying brain parenchyma was
normal.
Adhesion, fibrotic reaction and foreign body granuloma:
Bhatia et al 12 in an experimental study of 37 rabbits, who observed
postoperatively from 2 to 9 weeks found minimal or no fibrotic reaction or adhesion
among the six rabbits where plain HEMA was used as a dural substitue, fibrotic
reactions were limited to the edge of the graft. Of the four rabbits were collagen -
HEMA was used, showed dense fibrosis and adhesions at the interface between the
gel and the spinal cord and brain.
Neulen et al 51 in an experimental study on 34 pigs who were sacrificed at
4 weeks and 24 weeks using bilayered collagen on experimented injured cortex found
12.5% adhesion of the graft with the leptomeninges and 75 % adhesion of the cortical
lesion with the graft. In 2 of eight cases i,e 25 % had massive lymphocytic infiltrates
and granuloma was seen in 12.5% of animals.

55
Annie et al 32 in an experimental study of bilayered human collagen on 12
dogs who were sacrificed at 15, 30, 90 and 120 days found dense inflammatory
infiltrate and occasional giant cells around the graft at on day 15. The inflammatory
reaction showed a resorbtive granumalatous pattern on day 30. On days 90 and 120
there were no significant changes in the histological findings except for few scattered
fibroblast and there was no inflammation.
Charles et al 50 in a study of vicryl as dural substitute on 10 dogs, sacrificed
between 48 hours to 6 months found no significant adhesion at 4 weeks.
If therefore appears that 3 month is adequate for inflammatory response to
resolve.
Sakas et al14 found no foreign body relation to a biologically inert synthetic
dura (polysiloxane-carbonate film and aliphatic polyurethane) who were sacrificed 3,
6 and 9 months.
None of the animal experiments in the literature have shown persistent foreign
body granulomatous reaction in all the animals sacrificed at various intervals.
However, our study showed a foreign body type granulomatous reaction at the graft
site in all the rabbits (n=11) at 1 month and 3 months seen which was not adherent to
the brain or the overlying bone.

56
In our study on the experimental side there was granuloamtous reaction at the
graft site in all rabbits in both groups (one month and 3 months). There was no
resolution of this inflammation in the three month group compared to the one month
group. The literature suggests that this inflammatory response should resolve by three
months. Therefore the material used (single layer of electro spun polycaprolactone)
is a exciting a persistent foreign body granulamatous reaction which is not resolving
even at 3 months.

57
CONCLUSIONS
This pilot study showed that single layer electrospun polycaprolactone
provided a good seal against a CSF leak as evident by no pseudomeningiocele or CSF
leak in the experimented animals.
There was no cerebro-graft or graft to skull bone adhesion histologically.
The graft material can be cut to any size and shape and was easy to handle and
get absorbed over one month.
However, it showed significant foriegn body type granulomatous reaction at
the dural graft site which did not resolve by 3 months.
Therefore, it does not appear to be suitable as an ideal dural graft. Hence, the
search for an ideal dural substitute continues.

58
BIBLIOGRAPHY
1. Mark Albert Glaser and Clinton H. Thienes. Dural Defects: How Important Is Their Surgical Repair: An Experimental and Clinical Study upon Heteroplastic and Autoplastic Dural Grafts. Cal West Med / 48(3) / 163–166 / March 1938.
2. Abbe, R. Epilepsy from cortical cicatrix; trephining; subdural implantation of rubber-tissue. Ann. Surg., Volume 25 / 95-96 / 1897
3. Captain Norman C. Delarue, Eric A. Linlell , Kenneth G McKenzie An Experimental Study On The Use Of Tantalum In The Sub-Dural Space. J. Neurosurg / Volume 1 / 239-242 /1944
4. Brown MH, Grindlay JH, Craig WM: The use of polythene film as dural substitute. A preliminary report. J Neurosurg / Volume 4 / 505–507 / 1947
5. Paul Teng, Irwin Feigin Vinyon “N” As a dural substitute, An Experimental Study In The Monkey. J Neurosurgery / Volume 12 / 591-599 / 1955
6. Paul Teng, Vinyon “N” as a dural substitute and its use in other neurosurgical conditions. J. Neurol. Neurosurg. Psychiatry 24 / 182-186 / 1961
7. Jorge Huertas. The use of Orlon for dural replacement. J Neurosurgery / 550- 554 / April 1955
8. Sen Yamagata, Kazuo Goto, Yoshifumi Oda et al, Clinical Experience with Expanded Polytetrafluoroethylene Sheet Used as an Artificial Dura Mater Neurologia Medico-Chirurgica 33 (8) / 582-585 / 1993
9. Setsuko Nakagawa, Takashi Hayashi, Shigetaka Anegawa et al, Postoperative Infections after Duraplasty With ePTFE Sheet Neurological Medicine Chirurgiae (Tokyo) 43 / 120-124 / 2003

59
10. Martina Messing-Jünger, Javier Ibanez, Fabio Calbucci et al, Effectiveness and handling characteristics of a three-layer polymer dura substitute: a prospective multicentre clinical studyJ Neurosurg/Volume105 / 853–858/ 2006
11. Keisuke Yamada, Susumu Miyamoto, Motohiro Takayama et al Clinical application of a new bioabsorbable artificial duramater. J. Neurosurg. 96 / 731-735 / April, 2002
12. Sanjiv Bhatia, Peter R. Bergethon , Susan Blease et al A synthetic dural prosthesis constructed from hydroxyethylmethacrylate hydrogels J Neurosurgery / Volume 83 / 897-902 / November,1995
13. Paul Kurt Maurer, Joseph McDonald. Vicryl (Polyglactin 910) mesh as a dural substitute J.Neurosurg / Volume 63 / 448-452 / September 1985
14. Damianos E. Sakas, Komporn Charnvises, Lawrence F. Broges et al Biologically inert synthetic dural substitues: Appraisal of a medical grade aliphatic polyurethane and a polysiloxane carbonate block copolymer. J Neurosurgery / Volume 73 / December 1990
15. Keisuke Yamada, Susuma Miyamoto, Izumi Nagata et al Development of a dural substitute from synthetic bioabsorbable polymers. J Neurosurg / Volume 86 / 1012–1017 / June1997
16. Luis Renato Mello, Leonir T. Feltin, Paulo T. Fontes Neto et al. Duroplasty With Biosynthetic Cellulose: An Experimental Study. J Neurosurg / Volume 86 / 143-150 / January 1997
17. Andrew B. Adegbite, Kenneth W.E Paine, Bohdan Rozdilsky.The role of neomembranes in formation of hematoma around silastic dura substitute. J Neurosurg / Volume 58 / 295-29 / February 1983
18. Carlos M Ongkiko Jr, Jeffrey T. Keller, Frank H. Mayfield et al. An unusual complication of Dura Film as a dural substitute. Report of two cases.J Neurosurg / Volume 60 / 1076-1079 / May 1984

60
19. Gudmundsson and Sogaard. Complications To The Use Of Vicryl-Collagen Dural Substitute. Acta Neurochir (Wien) Volume 132 / 145-147 / 1995
20. Siccardi and Ventimiglia. Fibrotic-Haemorrhagic Reaction To Synthetic Dural Substitute. Acta Neurochir (Wien) Volume 13 / 148-149 / 1995
21. Thompson, Taylor, Hayward Haemorrhage associated with silastic dural substitute. Journal of Neurology, Neurosurgery, and Psychiatry Volume 57 / 646-648 / 1994
22. Robertson, Scott C, Menezes, Arnold H. Hemorrhagic Complications in Association with Silastic Dural Substitute: Pediatric and Adult Case Reports with a Review of the Literature Neurosurgery:January Volume 40 / Issue 1 / 201-206 / 1997 23. Alan R. Cohen, Slobodan Aleksic,Joseph Ransohoff. Inflammatory reaction to synthetic dural substitute J Neurosurg Volume 70 / 633-635 / April 1989
24. Kare Ekseth , Sverre Bostrom. Late complications of Silastic duraplasty: low- virulence infections J Neurosurg Volume 90 / 559-56 / March 1999
25. Paul C. Sharkey, Francis C. Usher, R.C.L Robertson et al. Lyophilized Human Dura Mater as a Dural Substitute. J Neurosurg Volume 15 / No. 2 / 192-198 / Mar 1958,
26. Hubert L. Rosomoff Ethylene oxide sterilized, freeze-dried dura mater for the repair of pachymeningeal defects. J Neurosurg / Volume 16 / 197-208 / 1959
27. M.R. Macfarlane and L Symon. Lyophilised duramater : Experimental neurosurgical use. implantation and extended clinical care. Journal of Neurology Neurosurgury Psychiatry Volume 42 / 854-858 / 1979
28. Jan Parizek, Pavel Mericka, Josef Spacek et al. Xenogeneic pericardium as a dural substitute in reconstruction of suboccipital dura mater in children. J Neurosurg Volume 70 / 905-909 / June 1989

61
29. A.Laun, J C Tonn, C. Jerusalem. Comparative Study Of Lyophilized Human Dura Mater And Lyophilized Bovine Pericardium As Dural Substitutes In Neurosurgery. Acta Neurochir (Wien) Volume 107 / 16-21 / 1990
30. Gaimpaolo Cantore, Beniamino Guidetti, Roberto Delfini. Neurosurgical use of human dura mater sterilized by gamma rays and stored in alcohol: long term results. J Neurosurg Volume 66 / 93-95 / Jannuary 1987
31. Xu Bang-Zong, Pan Hong-Xue, Chen Xi-Jin et al. Study and clinical application of a porcine biomembrane for the repair of dural defects. J Neurosurg Volume 69 / 707-711 / November,1988
32. Annie Laquerriere, Jin Yun, Jerome Tiollier. Experimental evaluation of bilayered human collagen as a dural substitute. J Neurosurg Volume 78 / 487- 491 / March 1993
33. Cormac O. Maher, Robert E. Anderson, Robyn L. Evaluation of a novel propylene oxide treated collagen material as a dural substitute.J Neurosurg Volume 99 / 1070-1076 / 2003
34. Filippi R, Derdilopoulos A, Heimann A et al Tightness of duraplasty in rabbits: a comparative study. Neurosurgery Volume 46 / 1470–1477 / June 2000
35. Pradeep K Narotam, Kesava Reddy, Derek Fewer et al.Collagen matrix duraplasty for clinical and spinal surgery a clinical and imaging study. J Neurosurg Volume 106 / 45-51 / January 2007
36. H H Kadioglu, E Takci, M Arik et al Immune response to dehydrated human dura mater: Evaluation in a rabbit model. Neurology India Volume 50 / September 2002
37. Prichard. Thadani, Kalb et al. Rapidly progressive dementia in a patient who received a cadaveric dura mater graft.MMWR Volume 36 / 49–50 /. February 1987

62
38. Creutzfeldt-Jakob disease in a patient receiving a cadaveric dura mater graft. MMWR Volume 36 / 324–5 / June 5, 1987
39. Creutzfeldt-Jakob Disease in Patients Who Received a Cadaveric Dura Mater Graft —Spain, 1985–1992 MMWR / Vol. 42 / No. 28 / July 23, 1993
40. Creutzfeldt-Jakob Disease Associated with Cadaveric Dura Mater Grafts — Japan, 1979–2003 MMWR / Vol. 52 / No. 48 / December 5, 2003
41. Fiona J Brooke, Alison Boyd, Genevieve M Klug et al Lyodura use and the risk of iatrogenic Creutzfeldt–Jakob disease in Australia eMJA Rapid online publication 14 January 2004
42. C A Heath,R A Barker, T F G Esmonde et al Dura mater-associated Creutzfeldt–Jakob disease: experience from surveillance in the UK J Neurol Neurosurg Psychiatry Volume 77 / 880–882 / 2006
43. Kobayashi, M Asano, S Mohri et al Cross-sequence transmission of sporadic Creutzfeldt-Jakob disease creates a new prion strain. J Biol Chem. Volume 282(41) / 30022-8 / October 2007
44 Creutzfeldt-Jakob Disease Associated with Cadaveric Dura Mater Grafts — Japan, 1979–2003 MMWR / Volume 57(42);1152-1154 / October 24, 2008
45. Tsuyoshi Hamaguchi, M Noguchi-Shinohara, I Nozaki et al Medical Procedures and Risk for Sporadic Creutzfeldt-Jakob Disease, Japan, 1999– 2008 Emerging Infectious Diseases Vol. 15/ No. 2/ February 2009
46. Vandenabeele F, Creemers J, Lambrichts I. Ultrastructure of the human spinal arachnoid mater and dura mater. J Anat Volume 189 /417–430 / 1996
47. Marina Protasoni Simone Sangiorgi, Andrea Cividini, et al The collagenic architecture of human dura mater J Neurosurg Volume 114 / 1723–1730 / June 2011

63
48. Park YK, Taylor C H . Prevention of arachnoiditis and postoperative tethering of the spinal cord with Gore-Tex surgical membrane: an experimental study with rats. Neurosurgery volume 42 / 813 – 824 / 1998
49. Nordstrom MR, Wang TD, Neel HB. Dura mater for soft tissue augmentation: Evaluation in a rabbit model. Arch otolaryngol head neck surg; Volume 119 / 209-214 / 1993;
50. Charles E. Nussbaum, Paul K. Maurer, Maj, MC, and Joseph V. McDonald, Vicryl (Polyglactin 910) mesh as a dural substitute in the presence of pia arachnoid injury. J Neurosurgery / Volume 71/ 124-127/ July 1989
51. Axel Neulen, Anglika Gutenberg, Evaluation of efficacy and biocompatibility of a noval semisynthetic collagen matrix as a dural onlay graft in a large animal model. Acta Neurochirugica / Volume 153/Issue 11/2241-2250/Nov 2011

64
ANNEXURES

65
Histological data: Rabbit Number 1
Criteria Control (Right)
Graft (Left) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent Hyalinised nodule
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or
absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
No No
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

66
Histological data: Rabbit Number:2
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or
absent
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
No Focal fibroblast
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

67
Histological Data-Rabbit 3
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or
absent)
foreign body type granulomatous inflammation
Edge - 2
Inflammation (present or absent
Present
Giant cell reaction (Present or absent)
foreign body type granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Minimal fibroblast
proliferation
No
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

68
Histological Data-Rabbit 4
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or
absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
No
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

69
Histological Data-Rabbit 5
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or
absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Minimal fibroblast
proliferation
Minimal fibroblast
proliferation
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

70
Histological Data-Rabbit 6
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Hemosideropha
ge,lymphocyte
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Minimal fibroblast
proliferation
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

71
Histological Data-Rabbit 7
Criteria Control (Right)
Graft (Left) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Minimal
reaction Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Focal
rarefaction Hemosiderophage,lymphocyte
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Minimal fibroblast
proliferation
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

72
Histological Data-Rabbit 8
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Absent
Absent
Giant cell reaction (Present or absent)
Foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Nil Nil
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

73
Histological Data-Rabbit 9
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Hyalinisation
and hemosiderin
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Macrophages
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Absent
Absent
Giant cell reaction (Present or absent)
Foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Nil Nil
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

74
Histological Data-Rabbit 10
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Hyalinisation Hyalinisation
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent Foamy
macrophage on the graft
side Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Absent
Absent
Giant cell reaction (Present or absent)
Foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Nil Nil
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

75
Histological Data-Rabbit 11
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent
Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent)
Absent
Absent
Giant cell reaction (Present or absent)
Foreign body type
granulomatous inflammation
Edge - 1
Inflammation (present or absent
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type
granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Minimal fibroblast reaction
Nil
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)

76
Histological Data-Rabbit 12
Criteria Control (Left)
Graft (Right) Remark
Adhesion No No
Inflammatory response in the
brain
(Absent/ Minimal/ Moderate/Severe)
Centre
Inflammatory response grade (Grade 0;1;2;3)
Absent Absent
Predominant inflam. cell
Number of Lymphocytes Number of Histiocytes
No. Foreign body giant cells
Edge - 1 Inflammatory response grade Absent Absent
Predominant inflam. cell Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Edge - 2 Inflammatory response grade Absent Absent Foreign body
granuloma seen on
leptomeningis on the control
side Predominant inflam. cell
Number of Lymphocytes
Number of Histiocytes
No. Foreign body giant cells
Inflammatory response in the
graft
Centre
Inflammation (present or absent) Absent
Absent
Giant cell reaction (Present or absent)
Foreign body type granulomatous inflammation
Edge - 1
Inflammation (present or absent Present
Giant cell reaction (Present or absent)
foreign body type granulomatous inflammation
Edge - 2
Inflammation (present or absent)
Present
Giant cell reaction (Present or absent)
foreign body type granulomatous inflammation
Fibroblast proliferation (Minimal - <25%,Moderate 25-50%, Severe->50%)
Nil Nil
Neodura Thickness (microns / mm) No neodura Thickness of graft (microns / mm)