Embed Size (px)
Citation preview

Surface-attached cells, biofilms and biocide susceptibility: Implications for hospital
cleaning and disinfection
Authors: J.A. Otter, K. Vickery, J.T. Walker, E. deLancey Pulcini, P. Stoodley, S.D. Goldenberg, J.A.G. Salkeld, J. Chewins, S. Yezli, & J.D. Edgeworth
NOTICE: this is the author’s version of a work that was accepted for publication in Journal of Hospital Infection. Changes resulting from the publishing process, such as peer review, editing, corrections, structural formatting, and other quality control mechanisms may not be reflected in this document. Changes may have been made to this work since it was submitted for publication. A definitive version was subsequently published in Journal of Hospital Infection, VOL# 89, ISSUE# 1, (January 2015) DOI# 10.1016/j.jhin.2014.09.008
Otter JA, Vickery K, Walker JT, de Lancey Pulcini E, Stoodley P, Goldenberg SD, Salkeld JA, Chewins J, Yezli S, Edgeworth JD, "Surface-attached cells, biofilms and biocide susceptibility: Implications for hospital cleaning and disinfection," Journal of Hospital Infection. January 2015 89(1):16–27.
Made available through Montana State University’s ScholarWorks scholarworks.montana.edu

ls, biofilms and biocide
Surface-attached cel susceptibility: implications for hospitalcleaning and disinfection
J.A. Otter a, b, *, K. Vickery c, J.T. Walker d, E. deLancey Pulcini e, P. Stoodley f, g,S.D. Goldenberg a, J.A.G. Salkeld b, J. Chewins b, S. Yezli b, J.D. Edgeworth a
aCentre for Clinical Infection and Diagnostics Research, Department of Infectious Diseases, King’s College London and Guy’s andSt. Thomas’ NHS Foundation Trust, London, UKbBioquell (UK) Ltd., Andover, UKcAustralian School of Advanced Medicine, Macquarie University, Nth Ryde, Australiad Public Health England MSD, Porton Down, Salisbury, UKeCenter for Biofilm Engineering, Montana State University, Bozeman, MT, USAfDepartments of Microbial Infection and Immunity and Orthopedics, Ohio State University, Columbus, OH, USAgNational Centre for Advanced Tribology, University of Southampton, Southampton, UK
ach toBiofilvices
a desospites, ain howattemlationns ann detere i
Microbes tend to atthealthcare settings. indwelling medical deextended periods in discovered on dry hsusceptible to biocidformation may explamore), interfere with mixed bacterial popudetergent formula-tiounrec-ognized role itesting standards. Th
Summary
microbes on dry hospital will inform new approachreduce microbial attachmactivity of biocides agains
tegiee of m
available surfaces and readily form biofilms, which is prob-lematic in ms are traditionally associated with wet or damp surfaces such as and tubing on medical equipment. However, microbes can survive for iccated state on dry hospital surfaces, and biofilms have recently been al surfaces. Microbes attached to surfaces and in biofilms are less ntibiotics and physical stress. Thus, surface attachment and/or biofilm
vegetative bacteria can survive on surfaces for weeks to months (or pts to recover microbes through environmental sampling, and provide a for the horizontal transfer of resistance genes. The capacity of existing d disinfectants to disrupt biofilms may have an important and previously ermining their effectiveness in the field, which should be reflected in s a need for further research to elucidate the nature and physiology of surfaces, specifically the prevalence and compo-sition of biofilms. This es to hospital cleaning and disinfection, including novel surfaces that ent and improve microbial detachment, and methods to augment the t surface-attached microbes such as bacteriophages and antimicrobial
peptides. Future straconsider the presenc
s to address environmental contamination on hospital surfaces should icrobes attached to surfaces, including biofilms.

Introduction survival is not surprising for the metabolically inert bacterialendospores, survival of some vegetative bacteria that is
Microbes tend to attach to available surfaces and formbiofilms readily.1e3 Biofilms are problematic in healthcaresettings, where they are thought to be involved in 65% ofnosocomial infections, and are usually reported in relation toindwelling medical devices and prostheses, water lines andtubing on endoscopes, and on wounds.1e3 In these settings,biofilm persistence can be prolonged, periodically ‘sloughingoff’ and releasing planktonic bacteria that may act as a sourceof infection. Biofilms are a common problem on liquidehardsurface interfaces, and in areas of a hospital that are usuallywet or damp, such as taps and sink drains.4 The recent prob-lems caused by Pseudomonas aeruginosa in water supplied tointensive care units, which resulted in changes to UK nationalguidance, illustrates this problem.4
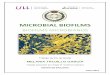
A biofilm is a community of micro-organisms attached to asubstrate producing extracellular polymeric substances (EPS)and exhibiting an altered phenotype compared with corre-sponding planktonic cells, especially regarding growth, genetranscription, protein production and intercellular inter-action.1e3,5,6 Biofilms comprising various micro-organisms,including bacteria, viruses, fungi and other micro-organisms,can form on almost any biological or inanimate surface, andhave been identified in various industrial and clinical set-tings.1,7 Not all microbes attached to surfaces meet the defi-nition of a biofilm, and the transition from a planktonic culturethrough surface attachment to an established biofilm is likelyto be a continuum rather than a stepwise process (Figure 1).1e3
Microbes including bacterial spores, vegetative bacteria,fungi and viruses can also survive on dry surfaces for extendedperiods.8e10 Contaminated environmental surfaces are anincreasingly recognized reservoir in the transmission of certainhealthcare-associated pathogens.11e13 Whilst this extended
Planktonic c
Surface attachment
Biofilm develand matura
Up to 10x less susceptible
Figure 1. Schematic of surface attachment, biofilm formation and bfaces, development and maturation of biofilms, and implications for miillustrates EPS. The biofilm development and maturation process is a cothe reduced biocide susceptibility associated with surface attachmentthe biocide, microbe and testing conditions, bacteria in mature biosurfaces, often by several orders of magnitude.18e20
measured in years rather than days challenges our under-standing of bacterial physiology.10,14 The structural and phys-iological state of microbes dried on to hospital surfaces has notbeen studied in detail, but it seems likely that bacteria attachto surfaces to some degree, and may form biofilms. Indeed, arecent study from Australia by Vickery et al.15 ‘destructivelysampled’ (i.e. cut the materials out of the hospital environ-ment and undertook laboratory analysis) several hospital sur-faces after cleaning and bleach disinfection. Scanning electronmicroscopy was used to examine the surfaces for biofilms,which were identified on five of six surfaces. Furthermore,viable meticillin-resistant Staphylococcus aureus (MRSA) wasidentified in the biofilm on three of the surfaces.
This article will review in-vitro studies that explore thestructure, physiology and biocide susceptibility of microbesdried on to hard surfaces in the context of surface attachmentand biofilm establishment, and discuss the potential implica-tions for hospital cleaning and disinfection.16
Search strategy
Pubmed was searched with no date restrictions using thesearch terms ‘biofilm and biocide’, ‘biofilm and reduced sus-ceptibility’, ‘biofilm and [MRSA, VRE, C. difficile, Acineto-bacter, E. coli, Pseudomonas]’ and ‘susceptibility planktonicbiofilm biocide’ (see Figure 1). The reference lists of articlesidentified via the Pubmed searches were hand searched toidentify other relevant literature.
Resistance and reduced susceptibility
Biofilms constitute a protected mode of growth, allowingbacteria to survive in hostile environments and conferring
ells
Mature biofilm
opment tion
Up to 1000x less susceptible
iocide susceptibility. This illustrates bacterial attachment to sur-crobial susceptibility. The grey shading around the mature biofilmsmplex step-wise process, simplified here as a single step.2,3 Whilstand biofilms will be determined by a number of factors, not leastfilms are consistently less susceptible than biofilms attached to

reduced susceptibility to dehydration, phagocytosis, metaltoxicity, acid exposure, antibiotics and biocides.1,7,17 Microbesattached to surfaces that have not formed an establishedbiofilm appear to represent an intermediate step, with reducedsusceptibility to biocides compared with planktonic cells, butincreased susceptibility relative to biofilms (Figure 1).18e20
Mechanisms of reduced susceptibilityCauses of reduced susceptibility to antimicrobial agents in
biofilms are multi-factorial, including reduced penetration(particularly due to changes in cell density and the productionof EPS), slow growth (and subsequent reduced metabolism ofantimicrobial agents), modulation of the stress response andother metabolic processes, and changes in quorumsensing.5,21e23 It seems likely that these mechanisms alsoexplain reduced biocide susceptibility in surface-attached cellsthat have not yet formed biofilms.
Biocide susceptibilityMany studies have evaluated the impact of established
biofilms on biocide susceptibility, and fewer studies haveevaluated the susceptibility of surface-attached cells that havenot yet formed established biofilms (Figure 1). Table I sum-marizes studies that have investigated organisms and biocidesrelevant to disinfection in healthcare settings that include datacomparing susceptibility in planktonic culture with surface-attached cells and/or biofilms. Studies have evaluated arange of organisms (both alone and in combination), varioussuspending media, and several methods of attaching cells tosurfaces and producing biofilms on different substrates; all ofthese factors are likely to influence biocide susceptibility. Oneimportant factor is the maturation of the microbes tested,which ranges from cells attached to surfaces for hours tosamples extracted from continuously fed biofilm reactors thatare weeks old.24,25 Furthermore, few studies have controlledfor cell density in attached cells or biofilms compared withplanktonic culture.26 Thus, although several studies have sug-gested that cell density alone does not explain the reducedsusceptibility of biofilms to biocides, it is difficult to be certainof the impact of the biofilm phenotype independent of celldensity in many studies.20,27e29 A number of different ap-proaches have been taken to quantify growth, including bothdirect microbial culture and indirect measures, such as live/dead viability assays.20,30e32 Finally, different approaches tocompare susceptibility in planktonic culture and biofilms haveincluded measuring the amount of biocide required to inhibitgrowth [minimum inhibitory concentration (MIC)] or kill cells[minimum bactericidal concentration (MBC)],7,18,20,33 ormeasuring the survival time at a given concentration ofbiocide;20,32,34,35 this makes comparison of studies difficult.
Notwithstanding difficulties in comparing studies, the phaseof the surface-attached cells influences biocide susceptibility.In general, bacteria in planktonic culture are more susceptiblethan attached cells, which are, in turn, more susceptible thanestablished biofilms (Figure 1).18e20 Meanwhile, detachedbiofilm cells revert to the susceptible phenotypic state.19,36,37
Similarly, growth phase affects biocide susceptibility ofplanktonic culture.38e40 Reduced susceptibility in surface-attached cells ranges widely from two-fold to >1000-fold.26,41 For example, clinical isolates of MRSA andP. aeruginosa were grown as biofilms on discs of common ma-terials in the hospital environment, and treated with three
commonly used hospital biocides: benzalkonium chloride (1%w/v), chlorhexidine gluconate (4% w/v) and triclosan (1% w/v).7 The MBCs of all biocides for planktonic cultures of bothorganisms were considerably less than the concentrationsrecommended for use by the manufacturer. However, whenisolates were grown as biofilms, the biocides were ineffectiveat killing bacteria at the concentrations recommended for use.The MBCs of all three biocides were found to be 10e1000-foldhigher than the same isolates grown in planktonic culture forMRSA and P. aeruginosa. Following biocide treatment, up to11% of cells in MRSA biofilms survived, and up to 80% of cells inP. aeruginosa biofilms survived. Another study evaluated thesusceptibility of four Candida spp. and two Escherichia colistrains to sodium hypochlorite, ethanol, hydrogen peroxide andiodine.20 Strains were tested in planktonic culture, as attachedcells and as biofilms in microtitre plates. Whilst susceptibilityvaried by organism and biocide, biofilms were less susceptiblethan attached cells, which were less susceptible than plank-tonic cells. MICs for biofilms were up to >10-fold higher for 5-min and 24-h exposures compared with planktonic cells. Thesestudies suggest that although biocides may be effective againstplanktonic populations of bacteria, some biocides currentlyused in hospitals may be ineffective against nosocomial path-ogens when attached to surfaces or in biofilms, and thus fail tocontrol this reservoir for hospital-acquired infection.7
However, whilst surface-attached microbes and biofilms aregenerally less susceptible to biocides than bacteria in plank-tonic culture, the degree of reduced susceptibility is not al-ways this stark. For example, a study reported no differencebetween planktonic culture and biofilms of Klebsiella pneu-moniae exposed to sodium hypochlorite and monochlor-amine.42 Other studies have not identified reducedsusceptibility for all biocides or organisms tested.20,24,43,44 It isdifficult to determine the relative importance of organism,biocide and testing conditions in these studies that found littleor no reduced biocide susceptibility associated with biofilms.
The composition of the biofilm also influences susceptibility.For example, high-nutrient, high-density biofilms are less sus-ceptible to biocides than low-nutrient, low-density bio-films.18,31,45 This seems particularly important in the context ofbiofilms thatmaybepresent onhospital surfaces,which are likelyto be low-nutrient, low-density biofilms in most cases. However,gross contamination with body fluids could provide an environ-ment in which high-nutrient, high-density biofilms could form onhospital surfaces. Indeed, three-quarters of thebiofilms reportedbyVickeryetal.had very thick EPSdespite having a lowdensity ofmicrobes inmost cases, perhaps in response todesiccation.15,46,47
The microbial ecology of the biofilm is another factorinfluencing susceptibility. Biofilms composed of multiple spe-cies are less susceptible than single-species biofilms, althoughthis is not always the case with the corresponding planktoniccultures.19,36,37,48
Some biocides are more effective than others at inactivatingbacteria in biofilms, although conflicting data have been re-ported, which may be explained by differences in experimentalconditions.20,24,35,49,50 In one study, susceptibility varied byphase, organism and biocide.20 In another study, the oxidizingagents sodium hypochlorite and peroxygens were more effec-tive than a range of other chemicals (including alcohols,biguanides, halogens, phenols and quaternary ammoniumcompounds) for inactivating P. aeruginosa and S. aureus bio-films.35 In other studies, sodium hypochlorite was more

Table I
Biocide susceptibility of planktonic vs surface-attached and/or biofilm mode
Author Organisms(N isolates)
Biocides Methods Findings
Condell 201218 Salmonellaenterica (189)
Seven common foodcontact surfacebiocides
Tested in planktonicculture, dried on surfacesand as established high-nutrient (2-day) or low-nutrient (7-day) biofilms onmicrotitre plates
Susceptibility rank: high-nutrientbiofilm < low-nutrientbiofilm < surface dried < planktonic
Behnke 201237 Pseudomonasaeruginosa (1);Burkholderiacepacia (1)
Chlorine dioxide Tested in single- andbinary-species planktonicculture, attached (4-day)and detached biofilm
Susceptibility rank: attachedbiofilm < detachedbiofilm ¼ planktonic cells. Binarycultures were less susceptible thansingle-species cultures
Xing 201249 Staphylococcusaureus (13)
Chlorhexidine andharmaline
Tested in planktonicculture and in 2-daybiofilms on microtitreplates
Biofilms were 10 to >100 times lesssusceptible to chlorhexidine and >2times less susceptible to harmaline.Synergy noted for most strains
Leung 201220 Candida spp. (4);Escherichia coli (2)
Sodium hypochlorite,ethanol, hydrogenperoxide and iodine
Tested in planktonicculture (low- and high-titre), attached cells(90 min) and 1-day biofilmin microtitre plates; 24-hand 5-min contact timescompared
Susceptibility rank:biofilm < attached cells < high-titreplanktonic cells � low-titreplanktonic cells. MICs for biofilm vsplanktonic cells up to >10-foldhigher for 5-min and 24-h exposures
Behnke 201136 P. aeruginosa (1);B. cepacia (1)
Sodium hypochlorite Tested in single- andbinary-species planktoniccultures, attached (4-day)and detached biofilms
Susceptibility rank: attachedbiofilm < detachedbiofilm ¼ planktonic cells. Binary-species cultures were lesssusceptible than single-speciescultures for attached and detachedbiofilms, but the reverse was true forplanktonic cells
Xu 201134 Neisseriagonorrhoeae (3)
Atmosphericpressure non-equilibrium plasma
Tested dried on glasssurfaces or 4-day biofilm onglass
Bacteria in biofilm survivedapproximately twice as long asbacteria dried on surfaces
Wong 201044 S. enterica (1) Six biocides Tested in planktonicculture or 3-day biofilm onmicrotitre plates
Bacteria in biofilm were lesssusceptible than planktonic cells forall but sodium hypochlorite
Tote 201035 S. aureus (1);P. aeruginosa (1)
12 biocides Tested in planktonicculture or in 1-day(P. aeruginosa) or 3-day(S. aureus) biofilm onmicrotitre plates
Most disinfectants tested did noteliminate bacteria in the biofilmafter 60-min contact. Only hydrogenperoxide and chlorine had an impacton the biofilm matrix
Lee 200924 Meticillin-resistantS. aureus (2)
Three denture-cleaning biocides
Tested in planktonicculture, sessile biofilm(4 h), established biofilm(24 h) or mature biofilm(120 h) on resin
Two of three biocides were lesseffective for the inactivation ofbacteria in biofilm. NaOCl was themost effective against biofilm
Hendry2009103
S. aureus (1);meticillin-resistantS. aureus (1);P. aeruginosa (1);E. coli (1); Candidaalbicans (1)
Eucalyptus oil,’1,8-cineole’ andchlorhexidine
Tested in planktonicculture or 2-day biofilm onmicrotitre plates
Biofilm MICs and MBCs were 10 to>100 times less susceptible thanplanktonic culture. Synergy betweenchlorhexidine and the other agentswas noted against some organisms
Smith 20087 Meticillin-resistantS. aureus (8);P. aeruginosa (8)
Benzalkoniumchloride, triclosanand chlorhexidine
Tested in planktonicculture or 1-day biofilms onmetal or plastic discs
MBCs for MRSA biofilms were 100 to1000 times greater than forplanktonic cells; MBCs forP. aeruginosa biofilm were 10 to 100timesgreater than for planktonic cells
(continued on next page)

Table I (continued )
Author Organisms(N isolates)
Biocides Methods Findings
Brandle 200819 Enterococcusfaecalis (1);Streptococcussobrinus (1);C. albicans (1);Actinomyces.naeslundii (1),Fusobacteriumnucleatum (1)
Calcium hydroxide Tested in planktonicculture, adherent cells,single-species 5-day biofilmand mixed-species 5-daybiofilm on dentin anddetached biofilm
Susceptibility rank: mixed speciesbiofilm < single-species biofilm <
adherent < planktonic ¼ detachedbiofilm
Nett 200826 C. albicans (2);Candida parapsilosis(2); Candidaglabrata (1)
Ethanol, hydrogenperoxide and sodiumdodecyl sulphate
Tested in planktonicculture, planktonic culturewith adjustment to matchthe cell density of thebiofilm and 1-day biofilm onmicrotitre plates
Concentrations required to inhibitgrowth in biofilm were 2- to 10-foldhigher; lower concentrations ofhydrogen peroxide preventedbiofilm formation than the otheragents tested
Karpanen2008102
Staphylococcusepidermidis (2)
Chlorhexidinegluconate, tea treeoil, eucalyptus oiland thymol
Tested in planktonicculture or 3-day biofilm onmicrotitre plates
MICs/MBCs were elevated up to 16-fold for biofilm; synergy was notedbetween chlorhexidine andeucalyptus oil
Bjarnsholt2007104
P. aeruginosa (1) Silver Tested in planktonicculture or 4-day biofilm
Biofilm was 10e100 times lesssusceptible than planktonic cells
Tabak 200740 Salmonellatyphimurium (3)
Triclosan Tested in planktonic (logand stationary phase)culture and in 1-day biofilmon microtitre plates
Susceptibility rank:biofilm < stationary phaseplanktonic < log phase planktonic.8-log difference in bacteria survivingin biofilm vs planktonic log phase
Surdeau2006105
E. coli (1);Enterococcus hirae(1); P. aeruginosa(1); S. aureus (1)
Novel disinfectant(Oxsil 320N)
Tested in planktonicculture and 1-day biofilmon stainless steel
Disinfectant concentration requiredto achieve a 5-log reduction wasapproximately 10 times more forbiofilm vs planktonic culture
Theraud200430
Five fungi frompatient (3) andenvironment (3)
Five antiseptics,three disinfectantsand UVC
Tested in single- andmixed-species planktonicculture, and single- andmixed-species 1-daybiofilms on microtitreplates
UVC and 3% hydrogen peroxide werenot fungicidal in initial suspensiontests. Agents were less effectiveagainst mixed suspensions. Onlychlorhexidine was effective againstbiofilms
Simoes2003106
Pseudomonasflourescens (1)
Ortho-phthalaldehyde
Tested in planktonicculture and 6-day biofilmon glass
Biofilm was less susceptible thanplanktonic cells based on respiratoryactivity
Bardouniotis200333
Mycobacteriumfortuitum (1);Mycobacteriummarinum (1)
Seven biocides Tested in planktonicculture and biofilm onmicrotitre plate assessedover 14 days
MBECs were up to 40-fold higherthan MBCs for M. fortuitum, but notfor M. marinum
Elvers 2002107 Alcaligenesdenitrificans (1);Pseudomonasalcaligenes (1);Stenotrophomonasmaltophilia (1);Flavobacteriumindologenes (1);Fusarium oxysporum(1); Fusobacteriumsolani (1);Rhodotorulaglutinis (1)
One biocide(isothiazolonecompound)
Tested in single-speciesplanktonic culture, andsingle- and mixed-species1-day biofilms on glass
Biofilms were less susceptible thanplanktonic cells. Mixed-speciesbiofilm, particularly for the bacterialspecies, offered greater protection

Table I (continued )
Author Organisms(N isolates)
Biocides Methods Findings
Peng 200231 Bacillus cereus (1) Sodium hypochloriteand quaternaryammoniumcompounds
Tested in planktonicculture, attached tostainless steel chips (4 h)and 8-day biofilm onstainless steel with orwithout milk
Susceptibility rank: milk biofilm< biofilm < attached < planktonic.5-log difference between planktoniccells and milk biofilm
Bardouniotis2001108
Mycobacteriumphlei (1)
Seven biocides Tested in planktonicculture and 5-day biofilmon microtitre plate
MBECs were higher than MBCs after30-min and 120-min exposure tomost agents tested
Joseph 200132 Salmonella spp. (2) Chlorine and iodine Tested in planktonicculture and 10-day biofilmson plastic, cement andstainless steel
Biofilms were less susceptible toboth disinfectants; survival time nomore than 10 min in suspensionvs > 25 min in biofilm
Cochran200029
P. aeruginosa (1) Monochloramine andhydrogen peroxide
Tested in planktonicculture and 3-h to 3-daybiofilms on alginate beadsand glass slides
Biofilms were less susceptible toboth disinfectants. Reduceddiffusion of biocide in biofilm did notexplain reduced susceptibility
Elasri 199953 P. aeruginosa (1) UVA, UVB and UVC Strain tested in planktonicculture or biofilm inalginate beads assessedover 1 day
Biofilm transmitted only a smallamount of UV radiation (13% of UVC,31% of UVB and 33% of UVA),meaning biofilm was less susceptiblethan planktonic cells
Das 199843 S. epidermidis (1);E. coli (1)
Five biocides Tested in planktonicculture and 6e24-h biofilmson microtitre plates
Biofilms were up to 33-fold lesssusceptible to the disinfectantstested, apart from chloroxylenol andcetrimide (E. coli only)
Stewart199845
Enterobacteraerogenes (1)
Four biocides Tested in planktonicculture and high- and low-density biofilms on alginatebeads assessed over 5 h
Susceptibility rank: high-densitybiofilm < low-densitybiofilm < planktonic
Yu 199342 Klebsiellapneumoniae (1)
Sodium hypochloriteand monochloramine
Tested in planktonicculture and biofilm onstainless steel discs
No difference identified betweenplanktonic and biofilm cells
Eginton 199856 S. epidermidis (1);P. aeruginosa (1)
Sodium hypochloriteand dodigen; SDS andTween-80
Tested in planktonicculture and 16-h biofilmson glass and stainless steel
Biofilms were up to >1000-fold lesssusceptible than planktonic cells;attachment to the surfaces wasloosened
LeChevallier198825
Pseudomonaspicketti,PseudomonaspaucimobilisMoraxellaa;K. pneumoniae (1)
Hypochlorous acid,hypochlorite,chlorine dioxide andmonochloramine
Tested in planktonicculture and 3-week biofilmson granular activatedcarbon, metal or glass
Biofilms were 150 to 3000 times lesssusceptible to hypochlorous acid,and 2- to 100-fold less susceptible tomonochloramine
MBC, minimum bactericidal concentration; MIC, minimum inhibitory concentration; MBEC, minimal biofilm eradicating concentration; UV,ultraviolet.Search strategy: Pubmed search for ‘susceptibility planktonic biofilm biocide’ performed on 15th November 2013. Of 44 results, 35 wereselected for review and 21 were included. A further 10 articles were included following review of the reference lists. Articles were included ifthey tested organisms and biocides relevant to disinfection in healthcare facilities, and included data comparing planktonic with surface-attached and/or biofilm mode susceptibility.a Population from de-ionized water system: composition 70% P. picketti; 18% Moraxella spp.; 12% P. paucimobilis.
effective than chlorhexidine for inactivating Enterococcusfaecium and MRSA in biofilms,24,50 whereas chlorhexidine wasfound to be effective against yeast biofilms when sodium hy-pochlorite was not effective.30 In general, oxidizing agentstarget multiple biofilm components and microbial targets,whereas other biocides such as chlorhexidine only target cell
wall components; thus, oxidizing agents tend to have a higherlevel of efficacy against biofilms.20,24,35,49,50 The variations inperformance of biocides under different experimental condi-tions may have implications for practice, where the samebiocide could have a different impact on biofilms in differentsettings.

Comparing biocides may be further confounded by the‘doseeresponse’ type relationship that has been shown be-tween biofilm susceptibility and biocide concentration.35,51,52
For example, one study showed that 10% hydrogen peroxidewas considerably more effective for inactivating bacteria inbiofilms compared with 6% hydrogen peroxide.51 Biofilms havealso been shown to reduce the susceptibility of microbes tophysical processes such as exposure to ultraviolet (UV) radia-tion, most likely due to poor penetration of UV into the bio-film.53 This may have implications for automated roomdisinfection systems using UV radiation.54 To the authors’knowledge, no studies have evaluated the impact of hydrogen-peroxide-based automated room disinfection systems againstbiofilms, although emerging data suggest that liquid hydrogenperoxide, as an oxidizing agent, targets both the biofilm matrixand microbes in the biofilm.35
Aside from the inactivation of microbes attached to sur-faces, the chemical properties of biocides also seem to beimportant in terms of preventing, promoting or dismantlingbiofilms.26,35,55 One study showed that only sodium hypochlo-rite and hydrogen peroxide damaged both the bacteria withinthe biofilm and the biofilm matrix itself.35 Also, hydrogenperoxide was more effective than other agents at preventingCandida spp. biofilm formation.26 In another study, exposure tochlorhexidine and benzalkonium chloride inhibited biofilmformation for E. coli, K. pneumoniae and P. aeruginosa, butpromoted biofilm formation in Staphylococcus epidermidis,suggesting that microbial factors are important.55 It is possible,therefore, that one microbe in a biofilm may be inactivated bya biocide, but another less susceptible microbe may surviveand then grow to replace the microbe that was inactivated.
Antibiotic susceptibilityBacteria in biofilms are usually less susceptible to antibiotics
than bacteria in planktonic culture, and many of the mecha-nisms for reduced susceptibility to biocides and antibiotics areshared.5,6 Furthermore, bacteria acquired from surfaces inbiofilm mode with reduced biocide susceptibility may retainreduced susceptibility to antibiotics.
Physical removalThe protected mode of growth offers physical protection to
cells within biofilms, and makes the physical breakdown ofbiofilms challenging.5 Although biofilm attachment appears tobe loosened by some biocides,35,56 several studies have illus-trated how difficult it can be to remove bacteria in biofilmsthrough cleaning and/or inactivation through disinfection. Forexample, regular and extended detergent cleaning did notremove a Bacillus cereus biofilm in vitro; a modified procedureincluding heating to 70
�C was required.31 Clearly, heating to
70�C is not feasible for the cleaning and disinfection of hospital
surfaces in clinical areas. Similarly, attached, viable Pseudo-monas fragiwere detected on stainless steel surfaces after twocleaning and disinfection procedures were tested under ‘worst-case’ conditions at 50% in-use disinfectant concentrations.57
An acid-detergent-based method was more effective atremoving attached cells than an alkaline-detergent-basedmethod. However, these studies were performed usingmature biofilms which may not be representative of the bio-films present on hospital surfaces.
Surface-attached cells and biofilms are clearly not the onlyreason for failures in hospital disinfection, given the difficulty
in achieving adequate distribution and contact time usingmanual methods.11,13,54,58 However, both reduced biocidesusceptibility (Table I) and increasing resilience to physicalremoval by cleaning are likely to contribute to failures inhospital cleaning. This could partly explain why disinfectantsthat are effective for the inactivation of planktonic bacteria inlaboratory tests are not effective for the eradication of aconsiderably lower load of the same bacterial species fromhospital surfaces.11,13,58e60 In support of this, it is noteworthythat the biofilms identified by Vickery et al. were on surfacesthat had been cleaned with detergent and then disinfectedusing 500 ppm chlorine.15 These findings may have implicationsfor infection control practices within hospitals, and on thechoice of appropriate disinfectants used to decontaminatesurfaces.11,13,54
The presence of biofilms on dry hospital surfaces could alsointerfere with attempts to recover microbes through environ-mental sampling.15,61e63 This could mean that an environ-mental reservoir of a pathogen remains undetected, or theconcentration of contamination and degree of associated risk isunderestimated.
PersistenceVegetative bacteria dried on to surfaces can survive for
weeks to months (or more) in vitro, despite the lack of anutrient source or water (aside from ambient humidity).8,9
Biofilms may explain this surprising propensity of vegetativebacteria.8e10 This is supported by a recent study which foundthat biofilm-forming strains of Acinetobacter baumannii sur-vived for longer on dry surfaces than non-biofilm-formingstrains (36 vs 15 days; P < 0.001).64 In-vitro studies evalu-ating the persistence of dried inocula did not supply any wateror nutrients.8e10,14,65 However, in the hospital environment,daily and terminal cleaning or disinfection does provide asupply of water, and some bacteria may be able to metabolizesome constituent parts of detergents and even disinfectants,providing a nutrient source for the growth in biofilms.66e69
Transfer of plasmids and development ofantimicrobial resistance
Biofilms are suited for horizontal gene disseminationbecause they are a mixed population at high bacterial density,which facilitates metabolic activity in the harshest environ-ments, albeit at a reduced rate. Horizontal transfer of plasmidsdoes occur through conjugation, as illustrated by the transferof extended-spectrum b-lactamase (CTX-M-15) and carbape-nemase (NDM-1) plasmids between Enterobacteriaceae whendried on surfaces.70,71 Furthermore, the mutation rate (therate at which DNA replication mistakes occur during cell divi-sion) of bacteria in biofilms is increased.6,72 Thus, both hori-zontal transfer of resistance determinants such as plasmids andincreased mutation rates could result in the acquisition or de-novo development of reduced susceptibility to antimicrobialagents and other important microbial capabilities, such asincreased virulence.
Tackling surface-attached cells and biofilms
Surface-attached cells, especially established biofilms, pre-sent a difficult challenge to hospital cleaning and disinfection,

combining protection from physical removal with reduced sus-ceptibility to biocides (Table I).31,57 A number of different ap-proaches are available to tackle surface-attached cells andbiofilms. Using physical methods to dislodge detached bacteria,which can be aided by the use of a detergent, can be effective inremoving established biofilms and preventing the developmentof biofilms.5,56,73 However, detergent cleaning alonemay not besufficient to remove biofilms.5,15,31,56,61,73 Tackling themicrobesin the biofilm alone (e.g. using some disinfectants or attempts tointerfere with quorum sensing) can be effective, but may notreach microbes protected deep in the biofilm matrix. Tacklingthe biofilm matrix alone (e.g. using enzymatic digestion) willhelp to reach microbes protected within the biofilm matrix andinterrupt persistenceof thebiofilm, butwill not necessarily havedirect microbicidal activity. Thus, tackling both the microbes inthe biofilm and the biofilm matrix simultaneously (usingoxidizing disinfectants or combination approaches) offers thepotential to reach microbes protected deep in the matrix andinterrupt the persistence of the biofilm. In addition, some bio-cides have the ability to reduce biofilm formation, which can beassisted by choosing surface materials that do not readily sup-port biofilm formation.
Biocides and biocide adjuvants
Differences between biocides appear to influence their ac-tivity against bacteria attached to surfaces and may also pro-mote, prevent or dismantle biofilms. Thus, biocides with thehighest activity against bacteria attached to surfaces, andideally those with the ability to prevent biofilm formation anddismantle existing biofilms, should be selected. Emerging dataindicate that oxidizing agents may possess more of theseproperties than other agents.35 Similarly, detergent formula-tions that are better at physical removal should be selected,although there is a paucity of data on the capacity of currentlyavailable detergents to address surface-attached cells.73
Several novel approaches also warrant consideration as po-tential additives to hospital detergents or disinfectants toaugment their effectiveness against biofilms. Firstly, certainenzymes such as DNase and dispersinB have been shown todissolve the biofilm matrix.73e78 For example, detergents sup-plemented with high concentrations of enzymes were effectiveagainst hydrated biofilms, whereas detergents supplementedwith low concentrations of enzymes were not.73 Secondly,quorum-sensing inhibitors have proven successful in increasingantimicrobial susceptibility.79e81 In one study, drimendiol, aquorum-sensing inhibitor, was found to enhance the effects ofcopper sulphate on biofilms of Pseudomonas syringae.81 Thirdly,recently discovered human antimicrobial peptides also haveantibiofilm activities.82e84 For example, a range of antimicro-bial peptides tested against multi-drug-resistant A. baumanniidemonstrated direct antimicrobial activity, and enhanced theactivity of a range of other antimicrobial agents.82
However, the addition of enzymes, quorum-sensing in-hibitors or antimicrobial peptides into a cleaning or disinfectionsolution would result in chemical residues on surfaces withassociated health and safety implications, so are not recom-mended without further study. Another approach is the inclu-sion of bacteriophages, which have been found to disruptbiofilms.85,86 For example, Streptococcus pyogenes biofilmswere degraded by PlyC, a bacteriophage-encoded endolysin,which also acted synergistically with a range of antimicrobial
agents.86 However, the therapeutic use of bacteriophages inhuman medicine and, by implication, in the clinical environ-ment is controversial due topotential for the rapid developmentof resistance and the risk that the introduced bacteriophagesmay play an unintended role in horizontal gene transfer.85,87
Surface modification to prevent biofilm formation
Some surface materials are more prone to biofilm formationthan others.71,88 A recent study reviewed attempts to modifythe chemical or physical surface properties of medical devicesto inhibit or prevent microbial adhesion.88 These include‘liquid glass’ (silicon dioxide), Sharklet pattern,89,90 advancedpolymer coatings [e.g. polyethylene glycol (PEG), super-hydrophobic/philic and zwitterionic]91�94 and diamond-likecarbon films.95 Whilst these technologies have the potentialto reduce biofilm deposition on hospital surfaces, they are atan early stage of development. The feasibility and cost-effectiveness of scaling up these technologies for use on hos-pital surfaces needs to be evaluated.
Another approach is the implementation of antimicrobialsurfaces. Options include metals such as copper and silver, orchemicals such as organosilanes with quaternary ammoniumgroups and light-activated antimicrobials.12,71,96 Copper is themost-studied candidate for antimicrobial surfaces, and hasbeen shown to inactivate microbes and DNA deposited on sur-faces and may reduce the transmission of pathogens in thehospital setting.12,71,97 However, the presence of a condition-ing film can greatly reduce the efficacy of antimicrobialsurfaces.98e100 Thus, an antimicrobial surface that combinesreduced biofilm formation with direct antimicrobial activity isa promising area for future research. Another challenge indeveloping an antimicrobial surface for hospitals is therequirement for multiple different surface types (from fabricto hard surfaces) with a range of required functions. Thus,there is unlikely to be a single agent or surface structure that issuitable for all applications.
Implications for susceptibility testing
Surface-attached cells and biofilms are a more accuratereflection of the occurrence of bacteria in nature than plank-tonic cells.1,101 However, planktonic culture remains the cur-rent model for many microbiological studies and testingstandards including susceptibility testing.1,101 Although quan-titative surface tests for evaluation of the bactericidal activityof chemical disinfectants do exist (e.g. BS EN 13697:2001),none have been published for EPS-producing biofilms. Futuretesting should specify the use of surface-attached cells andconsider the use of biofilm models to ensure that the disin-fectants tested are as effective in the ‘real world’ as in labo-ratory tests.1 It seems likely that low-nutrient, low-densitysurface-attached cells would be more appropriate than high-nutrient, high-density established biofilms. Most in-vitrostudies measured growth over a 24-h period to evaluate theimpact of a chemical biocide to determine the MIC or MBC,using methodology often used to test antibiotic susceptibility(Table I).7,20,102 One study compared the MICs of four commonbiocides for E. coil and various Candida spp. with a ‘contacttime’ of 5 min and 24 h.20 Unsurprisingly, the concentrationrequired to inhibit growth within 5 min was considerablygreater than the concentration required to inhibit growth over

24 h. Thus, as biocides are only applied for a short period inpractice, evaluating the impact of a biocide over a short con-tact time as per most published biocide testing standards ismore suitable for in-vitro biocide studies than measuring theMIC or MBC when microbes are grown in varying concentrationsof biocide.
Further research is required to evaluate the prevalence andcomposition of biofilms in situ on hard and soft hospital sur-faces, to develop in-vitro models that are representative ofthose likely to be found on hospital surfaces, and to optimizemethods to tackle biofilms on hospital surfaces, which mayinclude new cleaning and disinfection agents and adjuvants,new technologies (such as microfibre or automated roomdisinfection technology), and surface modification.15
Conclusion
Surface-attached cells are likely to be common on dry hos-pital surfaces, and there is evidence that they also harbourestablished biofilms. The variety of methods used to create andevaluate in-vitro biofilms makes it difficult to compare studiesevaluating antibiofilm biocide activity. Nonetheless, microbesattached to surfaces, especially established biofilms, are lesssusceptible to chemical biocides, UV radiation and antibioticsthan their corresponding planktonic bacteria. The phase of thesurface-attached microbes influences susceptibility: attachedcells are more susceptible to biocides than established bio-films; low-density, nutrient-limited biofilms make less of animpact on biocide susceptibility than high-density, high-nutrient biofilms; and biocides are less effective for inacti-vating bacteria in mixed-species biofilms than in single-speciesbiofilms. Biocide-specific issues also influence susceptibility interms of activity against bacteria in biofilms, and the preven-tion, promotion and dismantling of biofilms. Reduced suscep-tibility to biocides combined with protection from physicalremoval through cleaning is likely to contribute to failures inhospital cleaning and disinfection.
Biofilms may explain why vegetative bacteria can survive forunusually long periods (weeks to months) on dry hospital sur-faces. Also, the presence of surface-attached bacteria and bio-films is likely to interferewith attempts to recover bacteria fromhospital surfaces, and may lead to underestimation of both theprevalence of contamination with pathogens and the number ofbacteria that are on surfaces. This has important implications,particularly for hospital outbreak investigation. Biofilms providea mixed bacterial community where the horizontal transfer ofresistance genes may occur. Attempts to tackle surface-attached microbes and biofilms on hospital surfaces shouldinclude: identification and selection of biocide and detergentswith the best all-round performance, including the ability toinactivate surface-attached cells and biofilms; ensuring that in-vitro tests are developed to model surface-attached microbeslikely to be encountered in the field; harnessing surface scienceto develop a hospital environment that reduces the chance ofbiofilm formation; and further research to develop novel ap-proaches to augment the activity of biocides against surface-attached microbes, including established biofilms.
Conflict of interest statementJAO is employed part-time by Bioquell, and JAGS, JC and SYare employed by Bioquell. All other authors have no con-flicts of interest to declare.
Funding sourceNone.
References
1. Lindsay D, von Holy A. Bacterial biofilms within the clinicalsetting: what healthcare professionals should know. J Hosp Infect2006;64:313e325.
2. Hall-Stoodley L, Stoodley P. Biofilm formation and dispersal and thetransmission of human pathogens. Trends Microbiol 2005;13:7e10.
3. Hall-Stoodley L, Costerton JW, Stoodley P. Bacterial biofilms:from the natural environment to infectious diseases. Nat RevMicrobiol 2004;2:95e108.
4. Loveday HP, Wilson J, Kerr K, Pitchers R, Walker JT, Browne J.Pseudomonas infection and healthcare water systems e a rapidsystematic review. J Hosp Infect 2014;86:7e15.
5. Mah TF, O’Toole GA. Mechanisms of biofilm resistance to anti-microbial agents. Trends Microbiol 2001;9:34e39.
6. Hoiby N, Bjarnsholt T, Givskov M, Molin S, Ciofu O. Antibioticresistance of bacterial biofilms. Int J Antimicrob Agents2010;35:322e332.
7. Smith K, Hunter IS. Efficacy of common hospital biocides withbiofilms of multi-drug resistant clinical isolates. J Med Microbiol2008;57:966e973.
8. Otter JA, French GL. Survival of nosocomial bacteria and sporeson surfaces and inactivation by hydrogen peroxide vapor. J ClinMicrobiol 2009;47:205e207.
9. Kramer A, Schwebke I, Kampf G. How long do nosocomial path-ogens persist on inanimate surfaces? A systematic review. BMCInfect Dis 2006;6:130.
10. Wagenvoort JH, De Brauwer EI, Penders RJ, Willems RJ, Top J,Bonten MJ. Environmental survival of vancomycin-resistantEnterococcus faecium. J Hosp Infect 2011;77:282e283.
11. Otter JA, Yezli S, French GL. The role played by contaminatedsurfaces in the transmission of nosocomial pathogens. InfectControl Hosp Epidemiol 2011;32:687e699.
12. Salgado CD, Sepkowitz KA, John JF, et al. Copper surfaces reducethe rate of healthcare-acquired infections in the intensive careunit. Infect Control Hosp Epidemiol 2013;34:479e486.
13. Donskey CJ. Does improving surface cleaning and disinfectionreduce health care-associated infections? Am J Infect Control2013;41:S12eS19.
14. Wagenvoort JH, Joosten EJ. An outbreak Acinetobacter bau-mannii that mimics MRSA in its environmental longevity. J HospInfect 2002;52:226e227.
15. Vickery K, Deva A, Jacombs A, Allan J, Valente P, Gosbell IB.Presence of biofilm containing viable multiresistant organismsdespite terminal cleaning on clinical surfaces in an intensive careunit. J Hosp Infect 2012;80:52e55.
16. Yezli S, Otter JA. Does the discovery of biofilms on dry hospitalenvironmental surfaces change the way we think about hospitaldisinfection? J Hosp Infect 2012;81:293e294.
17. Smith K, Perez A, Ramage G, Gemmell CG, Lang S. Comparison ofbiofilm-associated cell survival following in vitro exposure ofmeticillin-resistant Staphylococcus aureus biofilms to the anti-biotics clindamycin, daptomycin, linezolid, tigecycline and van-comycin. Int J Antimicrob Agents 2009;33:374e378.
18. Condell O, IversenC,Cooney S, et al. Efficacy of biocides used in themodern food industry to control Salmonella enterica, and links be-tween biocide tolerance and resistance to clinically relevant anti-microbial compounds. Appl Environ Microbiol 2012;78:3087e3097.
19. Brandle N, Zehnder M, Weiger R, Waltimo T. Impact of growthconditions on susceptibility of five microbial species to alkalinestress. J Endod 2008;34:579e582.
20. Leung CY, Chan YC, Samaranayake LP, Seneviratne CJ. Biocideresistance of Candida and Escherichia coli biofilms is associatedwith higher antioxidative capacities. JHosp Infect 2012;81:79e86.

21. Parsek MR, Greenberg EP. Sociomicrobiology: the connectionsbetween quorum sensing and biofilms. Trends Microbiol2005;13:27e33.
22. Stewart PS. Diffusion in biofilms. J Bacteriol 2003;185:1485e1491.23. Keren I, Kaldalu N, Spoering A, Wang Y, Lewis K. Persister cells
and tolerance to antimicrobials. FEMS Microbiol Lett2004;230:13e18.
24. Lee D, Howlett J, Pratten J, et al. Susceptibility of MRSA biofilmsto denture-cleansing agents. FEMS Microbiol Lett2009;291:241e246.
25. LeChevallier MW, Cawthon CD, Lee RG. Inactivation of biofilmbacteria. Appl Environ Microbiol 1988;54:2492e2499.
26. Nett JE, Guite KM, Ringeisen A, Holoyda KA, Andes DR. Reducedbiocide susceptibility in Candida albicans biofilms. AntimicrobAgents Chemother 2008;52:3411e3413.
27. Watamoto T, Samaranayake LP, Egusa H, Yatani H,Samaranayke YH, Seneviratne CJ. Susceptibility of Candidaalbicans filamentation-defective mutants to clinical biocides.J Hosp Infect 2010;74:189e191.
28. Seneviratne CJ, Jin LJ, Samaranayake YH, Samaranayake LP. Celldensity and cell aging as factors modulating antifungal resistanceof Candida albicans biofilms. Antimicrob Agents Chemother2008;52:3259e3266.
29. Cochran WL, McFeters GA, Stewart PS. Reduced susceptibility ofthin Pseudomonas aeruginosa biofilms to hydrogen peroxide andmonochloramine. J Appl Microbiol 2000;88:22e30.
30. Theraud M, Bedouin Y, Guiguen C, Gangneux JP. Efficacy of an-tiseptics and disinfectants on clinical and environmental yeastisolates in planktonic and biofilm conditions. J Med Microbiol2004;53:1013e1018.
31. Peng JS, Tsai WC, Chou CC. Inactivation and removal of Bacilluscereus by sanitizer and detergent. Int J Food Microbiol2002;77:11e18.
32. Joseph B, Otta SK, Karunasagar I, Karunasagar I. Biofilm forma-tion by Salmonella spp. on food contact surfaces and theirsensitivity to sanitizers. Int J Food Microbiol 2001;64:367e372.
33. Bardouniotis E, Ceri H, Olson ME. Biofilm formation and biocidesusceptibility testing of Mycobacterium fortuitum and Mycobac-terium marinum. Curr Microbiol 2003;46:28e32.
34. Xu L, Tu Y, Yu Y, Tan M, Li J, Chen H. Augmented survival ofNeisseria gonorrhoeae within biofilms: exposure to atmosphericpressure non-thermal plasmas. Eur J Clin Microbiol Infect Dis2011;30:25e31.
35. Tote K, Horemans T, Vanden Berghe D, Maes L, Cos P. Inhibitoryeffect of biocides on the viable masses and matrices of Staphy-lococcus aureus and Pseudomonas aeruginosa biofilms. Appl En-viron Microbiol 2010;76:3135e3142.
36. Behnke S, Parker AE, Woodall D, Camper AK. Comparing thechlorine disinfection of detached biofilm clusters with those ofsessile biofilms and planktonic cells in single- and dual-speciescultures. Appl Environ Microbiol 2011;77:7176e7184.
37. Behnke S, Camper AK. Chlorine dioxide disinfection of single anddual species biofilms, detached biofilm and planktonic cells.Biofouling 2012;28:635e647.
38. Bjergbaek LA, Haagensen JA, Molin S, Roslev P. Effect of oxygenlimitation and starvation on the benzalkonium chloride suscepti-bility of Escherichia coli. J Appl Microbiol 2008;105:1310e1317.
39. Field TR, White A, Elborn JS, Tunney MM. Effect of oxygen limi-tation on the in vitro antimicrobial susceptibility of clinical iso-lates of Pseudomonas aeruginosa grown planktonically and asbiofilms. Eur J Clin Microbiol Infect Dis 2005;24:677e687.
40. Tabak M, Scher K, Hartog E, et al. Effect of triclosan on Salmo-nella typhimurium at different growth stages and in biofilms.FEMS Microbiol Lett 2007;267:200e206.
41. Smith K, Gemmell CG, Hunter IS. The association betweenbiocide tolerance and the presence or absence of qac genesamong hospital-acquired and community-acquired MRSA isolates.J Antimicrob Chemother 2008;61:78e84.
42. Yu FP, Pyle BH, McFeters GA. A direct viable count method forthe enumeration of attached bacteria and assessment of biofilmdisinfection. J Microbiol Methods 1993;17:167e180.
43. Das JR, Bhakoo M, Jones MV, Gilbert P. Changes in the biocidesusceptibility of Staphylococcus epidermidis and Escherichia colicells associated with rapid attachment to plastic surfaces. J ApplMicrobiol 1998;84:852e858.
44. Wong HS, Townsend KM, Fenwick SG, Trengove RD,O’Handley RM. Comparative susceptibility of planktonic and 3-day-old Salmonella typhimurium biofilms to disinfectants.J Appl Microbiol 2010;108:2222e2228.
45. Stewart PS, Grab L, Diemer JA. Analysis of biocide transportlimitation in an artificial biofilm system. J Appl Microbiol1998;85:495e500.
46. van de Mortel M, Halverson LJ. Cell envelope componentscontributing to biofilm growth and survival of Pseudomonas putidain low-water-content habitats. Mol Microbiol 2004;52:735e750.
47. Flemming HC, Wingender J. The biofilm matrix. Nat Rev Micro-biol 2010;8:623e633.
48. Bridier A, Sanchez-Vizuete Mdel P, Le Coq D, et al. Biofilms of aBacillus subtilis hospital isolate protect Staphylococcus aureusfrom biocide action. PLoS One 2012;7:e44506.
49. Xing M, Shen F, Liu L, et al. Antimicrobial efficacy of the alkaloidharmaline alone and in combinationwith chlorhexidine digluconateagainst clinical isolates of Staphylococcus aureus grown in plank-tonic and biofilm cultures. Lett Appl Microbiol 2012;54:475e482.
50. Williamson AE, Cardon JW, Drake DR. Antimicrobial susceptibilityof monoculture biofilms of a clinical isolate of Enterococcusfaecalis. J Endod 2009;35:95e97.
51. Yun HS, Kim Y, Oh S, Jeon WM, Frank JF, Kim SH. Susceptibility ofListeria monocytogenes biofilms and planktonic cultures tohydrogen peroxide in food processing environments. Biosci Bio-technol Biochem 2012;76:2008e2013.
52. Peeters E, Nelis HJ, Coenye T. Evaluation of the efficacy ofdisinfection procedures against Burkholderia cenocepacia bio-films. J Hosp Infect 2008;70:361e368.
53. Elasri MO, Miller RV. Study of the response of a biofilm bacterialcommunity to UV radiation. Appl Environ Microbiol1999;65:2025e2031.
54. Otter JA, Yezli S, Perl TM, Barbut F, French GL. Is there a role for‘no-touch’ automated room disinfection systems in infectionprevention and control? J Hosp Infect 2013;83:1e13.
55. Houari A, Di Martino P. Effect of chlorhexidine and benzalkoniumchloride on bacterial biofilm formation. Lett Appl Microbiol2007;45:652e656.
56. Eginton PJ, Holah J, Allison DG, Handley PS, Gilbert P. Changes inthe strength of attachment of micro-organisms to surfacesfollowing treatment with disinfectants and cleansing agents. LettAppl Microbiol 1998;27:101e105.
57. Stone LS, Zottola EA. Effect of cleaning and sanitizing on theattachment of Pseudomonas fragi to stainless steel. J Food Sci1985;50:951e956.
58. Manian FA, Griesenauer S, Senkel D, et al. Isolation of Acineto-bacter baumannii complex and methicillin-resistant Staphylo-coccus aureus from hospital rooms following terminal cleaningand disinfection: can we do better? Infect Control Hosp Epi-demiol 2011;32:667e672.
59. Goodman ER, Platt R, Bass R, Onderdonk AB, Yokoe DS, Huang SS.Impact of an environmental cleaning intervention on the pres-ence of methicillin-resistant Staphylococcus aureus andvancomycin-resistant enterococci on surfaces in intensive careunit rooms. Infect Control Hosp Epidemiol 2008;29:593e599.
60. Wilcox MH, Fawley WN, Wigglesworth N, Parnell P, Verity P,Freeman J. Comparison of the effect of detergent versus hypo-chlorite cleaning on environmental contamination and incidenceof Clostridium difficile infection. J Hosp Infect 2003;54:109e114.
61. French GL, Otter JA, Shannon KP, Adams NM, Watling D,Parks MJ. Tackling contamination of the hospital environment by

methicillin-resistant Staphylococcus aureus (MRSA): a comparisonbetween conventional terminal cleaning and hydrogen peroxidevapour decontamination. J Hosp Infect 2004;57:31e37.
62. Zanetti G, Blanc DS, Federli I, et al. Importation of Acinetobacterbaumannii into a burn unit: a recurrent outbreak of infectionassociated with widespread environmental contamination. InfectControl Hosp Epidemiol 2007;28:723e725.
63. Boyce JM, Havill NL, Havill HL, Mangione E, Dumigan DG,Moore BA. Comparison of fluorescent marker systems with 2quantitative methods of assessing terminal cleaning practices.Infect Control Hosp Epidemiol 2011;32:1187e1193.
64. Espinal P, Marti S, Vila J. Effect of biofilm formation on thesurvival of Acinetobacter baumannii on dry surfaces. J HospInfect 2012;80:56e60.
65. Wagenvoort JH, Sluijsmans W, Penders RJ. Better environmentalsurvival of outbreak vs. sporadic MRSA isolates. J Hosp Infect2000;45:231e234.
66. Weber DJ, Rutala WA, Sickbert-Bennett EE. Outbreaks associatedwith contaminated antiseptics and disinfectants. AntimicrobAgents Chemother 2007;51:4217e4224.
67. BasuA,Dixit SS, Phale PS.Metabolismof benzyl alcohol via catecholortho-pathway in methylnaphthalene-degrading Pseudomonasputida CSV86. Appl Microbiol Biotechnol 2003;62:579e585.
68. Gottsching A, Schmidt S. Productive degradation of the biocidebenzylbenzoate by Acinetobacter sp. strain AG1 isolated fromthe River Elbe. Res Microbiol 2007;158:251e257.
69. Ying GG. Fate, behavior and effects of surfactants and their degra-dation products in the environment. Environ Int 2006;32:417e431.
70. Molin S, Tolker-Nielsen T. Gene transfer occurs with enhancedefficiency in biofilms and induces enhanced stabilisation of thebiofilm structure. Curr Opin Biotechnol 2003;14:255e261.
71. Warnes SL, Highmore CJ, Keevil CW. Horizontal transfer ofantibiotic resistance genes on abiotic touch surfaces: implica-tions for public health. MBio 2012;3:e00489ee00512.
72. Driffield K, Miller K, Bostock JM, O’Neill AJ, Chopra I. Increasedmutability of Pseudomonas aeruginosa in biofilms. J AntimicrobChemother 2008;61:1053e1056.
73. Vickery K, Pajkos A, Cossart Y. Removal of biofilm from endo-scopes: evaluation of detergent efficiency. Am J Infect Control2004;32:170e176.
74. Brindle ER, Miller DA, Stewart PS. Hydrodynamic deformation andremoval of Staphylococcus epidermidis biofilms treated withurea, chlorhexidine, iron chloride, or DispersinB. BiotechnolBioeng 2011;108:2968e2977.
75. Kaplan JB, LoVetri K, Cardona ST, et al. Recombinant humanDNase I decreases biofilm and increases antimicrobial suscepti-bility in staphylococci. J Antibiot (Tokyo) 2012;65:73e77.
76. Li W, Liu H, Xu Q. Extracellular dextran and DNA affect the for-mation of Enterococcus faecalis biofilms and their susceptibilityto 2% chlorhexidine. J Endod 2012;38:894e898.
77. Latimer J, Forbes S, McBain AJ. Attenuated virulence and bio-film formation in Staphylococcus aureus following sublethalexposure to triclosan. Antimicrob Agents Chemother2012;56:3092e3100.
78. Alipour M, Suntres ZE, Omri A. Importance of DNase and alginatelyase for enhancing free and liposome encapsulated amino-glycoside activity against Pseudomonas aeruginosa. J AntimicrobChemother 2009;64:317e325.
79. Liaqat I, Bachmann RT, Sabri AN, Edyvean RG, Biggs CA. Inves-tigating the effect of patulin, penicillic acid and EDTA on biofilmformation of isolates from dental unit water lines. Appl MicrobiolBiotechnol 2008;81:349e358.
80. Bjarnsholt T, Jensen PO, Rasmussen TB, et al. Garlic blocks quorumsensing and promotes rapid clearing of pulmonary Pseudomonasaeruginosa infections. Microbiology 2005;151:3873e3880.
81. Paza C, Carcamo G, Silva M, Becerra J, Urrutia H, Sossa K. Dri-mendiol, a drimane sesquiterpene with quorum sensing inhibitionactivity. Nat Prod Commun 2013;8:147e148.
82. Gopal R, Kim YG, Lee JH, et al. Synergistic effects and antibiofilmproperties of chimeric peptides against multidrug-resistant Aci-netobacter baumannii strains. Antimicrob Agents Chemother2014;58:1622e1629.
83. Feng X, Sambanthamoorthy K, Palys T, Paranavitana C. The hu-man antimicrobial peptide LL-37 and its fragments possess bothantimicrobial and antibiofilm activities against multidrug-resistant Acinetobacter baumannii. Peptides 2013;49:131e137.
84. Forbes S, McBain AJ, Felton-Smith S, Jowitt TA, Birchenough HL,Dobson CB. Comparative surface antimicrobial properties ofsynthetic biocides and novel human apolipoprotein E derivedantimicrobial peptides. Biomaterials 2013;34:5453e5464.
85. Sillankorva S, Azeredo J. Bacteriophage attack as an anti-biofilmstrategy. Methods Mol Biol 2014;1147:277e285.
86. Shen Y, Koller T, Kreikemeyer B, Nelson DC. Rapid degradation ofStreptococcus pyogenes biofilms by PlyC, a bacteriophage-encoded endolysin. J Antimicrob Chemother 2013;68:1818e1824.
87. Lu TK, Koeris MS. The next generation of bacteriophage therapy.Curr Opin Microbiol 2011;14:524e531.
88. Desrousseaux C, Sautou V, Descamps S, Traore O. Modification ofthe surfaces of medical devices to prevent microbial adhesionand biofilm formation. J Hosp Infect 2013;85:87e93.
89. Chung KK, Schumacher JF, Sampson EM, Burne RA, Antonelli PJ,Brennan AB. Impact of engineered surface microtopography onbiofilm formation of Staphylococcus aureus. Biointerphases2007;2:89e94.
90. Reddy ST, Chung KK, McDaniel CJ, Darouiche RO, Landman J,Brennan AB. Micropatterned surfaces for reducing the risk ofcatheter-associated urinary tract infection: an in vitro study onthe effect of Sharklet micropatterned surfaces to inhibit bacte-rial colonization and migration of uropathogenic Escherichia coli.J Endourol 2011;25:1547e1552.
91. Park KD, Kim YS, Han DK, et al. Bacterial adhesion on PEGmodified polyurethane surfaces. Biomaterials 1998;19:851e859.
92. Hou S, Burton EA, Simon KA, Blodgett D, Luk YY, Ren D. Inhibitionof Escherichia coli biofilm formation by self-assembled mono-layers of functional alkanethiols on gold. Appl Environ Microbiol2007;73:4300e4307.
93. Hirota K, Murakami K, Nemoto K, Miyake Y. Coating of a surfacewith 2-methacryloyloxyethyl phosphorylcholine (MPC) co-polymer significantly reduces retention of human pathogenicmicroorganisms. FEMS Microbiol Lett 2005;248:37e45.
94. Cheng G, Zhang Z, Chen S, Bryers JD, Jiang S. Inhibition of bac-terial adhesion and biofilm formation on zwitterionic surfaces.Biomaterials 2007;28:4192e4199.
95. Liu C, Zhao Q, Liu Y, Wang S, Abel EW. Reduction of bacterialadhesion on modified DLC coatings. Colloids Surf B Biointerfaces2008;61:182e187.
96. Humphreys H. Self-disinfecting and microbiocide-impregnatedsurfaces and fabrics: what potential in interrupting the spread ofhealthcare-associated infection? Clin Infect Dis 2014;58:848e853.
97. Grass G, Rensing C, Solioz M. Metallic copper as an antimicrobialsurface. Appl Environ Microbiol 2011;77:1541e1547.
98. Ojeil M, Jermann C, Holah J, Denyer SP, Maillard JY. Evaluation ofnew in vitro efficacy test for antimicrobial surface activityreflecting UK hospital conditions. J Hosp Infect 2013;85:274e281.
99. O’Gorman J, Humphreys H. Application of copper to prevent andcontrol infection. Where are we now? J Hosp Infect2012;81:217e223.
100. Airey P, Verran J. Potential use of copper as a hygienic surface;problems associated with cumulative soiling and cleaning. J HospInfect 2007;67:271e277.
101. Parsek MR, Fuqua C. Biofilms 2003: emerging themes and chal-lenges in studies of surface-associated microbial life. J Bacteriol2004;186:4427e4440.
102. Karpanen TJ, Worthington T, Hendry ER, Conway BR,Lambert PA. Antimicrobial efficacy of chlorhexidine digluconatealone and in combination with eucalyptus oil, tea tree oil and

thymol against planktonic and biofilm cultures of Staphylococcusepidermidis. J Antimicrob Chemother 2008;62:1031e1036.
103. Hendry ER, Worthington T, Conway BR, Lambert PA. Antimicro-bial efficacy of eucalyptus oil and 1,8-cineole alone and incombination with chlorhexidine digluconate against microor-ganisms grown in planktonic and biofilm cultures. J AntimicrobChemother 2009;64:1219e1225.
104. Bjarnsholt T, Kirketerp-Moller K, Kristiansen S, et al. Silver againstPseudomonas aeruginosa biofilms. APMIS 2007;115:921e928.
105. Surdeau N, Laurent-Maquin D, Bouthors S, Gelle MP. Sensitivity ofbacterial biofilms and planktonic cells to a new antimicrobialagent, Oxsil 320N. J Hosp Infect 2006;62:487e493.
106. Simoes M, Carvalho H, Pereira MO, Vieira MJ. Studies on thebehaviour of Pseudomonas fluorescens biofilms after ortho-phthalaldehyde treatment. Biofouling 2003;19:151e157.
107. Elvers KT, Leeming K, Lappin-Scott HM. Binary and mixed popu-lation biofilms: time-lapse image analysis and disinfection withbiocides. J Ind Microbiol Biotechnol 2002;29:331e338.
108. Bardouniotis E, Huddleston W, Ceri H, Olson ME. Characterizationof biofilm growth and biocide susceptibility testing of Mycobac-terium phlei using the MBEC assay system. FEMS Microbiol Lett2001;203:263e267.