Embed Size (px)
Citation preview
Surgery for Cerebrovascular Surgery for Cerebrovascular Diseases(CVDs)Diseases(CVDs)
Jian-min Zhang Dept. of Neurosurgery 2nd Affiliated Hospital
Zhejiang University College of Medicine
• Cerebral vascular diseases (CVDs) are series of diseases with high mortality, which have loaded a heavy burden to the society.
• Classification : Hemorrhagic and Occlusive
• Treatment : medicine and surgery• With the development of basic science,
microneurosurgery and endovascular techniques, more and more CVDs can be treated by means of surgery.
introductionintroduction
1. Hemorrhagic CVDs intracranial aneurysmcerebral vascular malformation hypertensive hemorrhage

(1). intracranial aneurysm(1). intracranial aneurysm
general knowledge
• incidence: 0.2-7.9% in autopsy; 6-8/105/year for ruptured aneurysms. It is the third common CVDs and the incidence is increasing.
• Most common in 40-60 years old• Morphology: abnormal dilation of intracraniaarteries----saccular,
fusiform and dissecting• Often diagnosed when ruptured and cause subarachnoid hemorrh
age(SAH). • Mortality decreased with the improvement of diagnose and mana
gement.
EtiologyEtiology
•Congenital
•Acquired:
Infectious
Traumatic
Caused by angiosclerosis
Caused by disecting of blood vessels
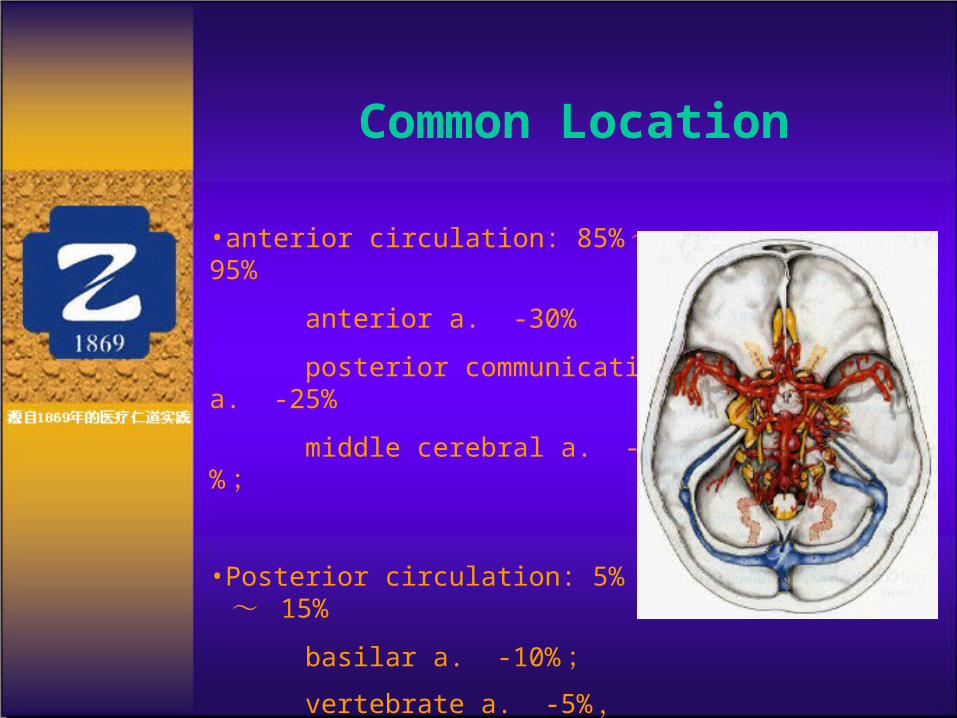
Common Location
•anterior circulation: 85%~ 95%
anterior a. -30%
posterior communicating a. -25%
middle cerebral a. -20% ;
•Posterior circulation: 5% ~ 15%
basilar a. -10% ; vertebrate a. -5% ,

Risk factors
•age
•Genetic background
•Homodynamic factors•Defects in medial layer of blood vessels
•Hypertension
Natural history
•Ruptured :7% die on the spot,7% misdiagnosed
•Re-bleeding: peak at 7-10th days
Pathology
•SAH
•Intracranial hemorrhage
•hydrocephalus
•Cerebral vasospasm
Symptoms
•bleeding : headache, nausea and consciousness disturbance
•Local neurological symptoms
•Systematic symptoms

动脉瘤破裂出血 .avi
Hunt-Hess scale
I Asymptomatic or minimal headache and slight nuchal rigidity
II Moderate to severe headache, nuchal rigidity, no neurological deficit other than cranial nerve palsy
III Drowsiness, confusion, or mild focal deficit IV Stupor, moderate to severe hemiparesis, possible ea
rly decerebrate rigidity and vegetative disturbances V Deep coma, decerebrate rigidity, moribund appeara
nce
diagnosis•Lumbar pucture
•CT/MRI
•DSA ,CTA , MRA
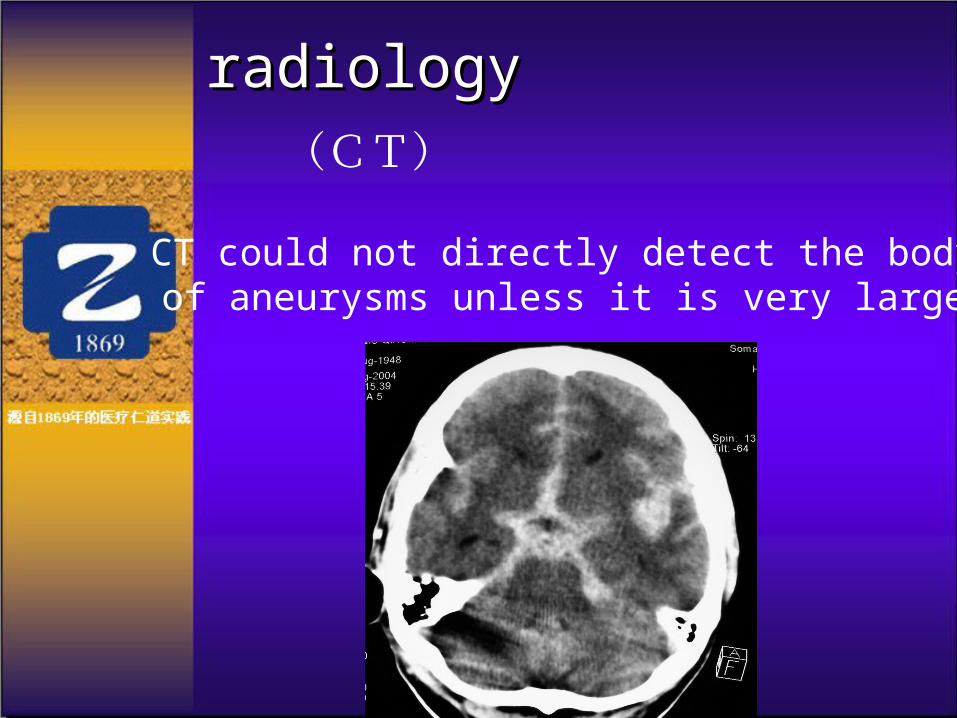
(CT)
CT could not directly detect the body of aneurysms unless it is very large
radiologyradiology

managements•medical
•surgical
•endovascular

1 .medical•Lying in bed for more than 4 weeks •Avoiding agitation or excertion
•haemostatic
•Dehydration to reduce intracranial pressure
•Anti-vasospasm
•external ventricular drainage
•Controlling the blood pressure
•Symptomatic treatment

2 .surgical
•history : 1885,Horsley ligation of internal carotid a.
1927 cerebral angiography
1931 encapsulate the aneurysms with muscles
1937 aneurysm clipping ( by Dandy) and trapping
1942 ligation of the neck of the aneurysms
•Purpose of the operation : avoiding re-rupture and re-bleeding, keep the aneurysm-bearing arteries open and controlling vasospasm
•Operation: direct—clipping, ligation or trapping
Indirect: ligation of carotid artery or blocking the aneurysm-bearing atery
Trapping (preoperative tests)
indication
• age < 75 ;• Hunt-Hess scale: I - III
• Hunt-Hess scale IV-V should be operated when the pati
ents recover to I-III
• In acute phase: with intracerebral hemorrhage or large v
olume of SAH
• Infectious aneurysm
Operation time
• Immediate operation for Hunt-Hess I -II ;• Patients with recurrent bleeding ;• Patients with vasospasm should be operated on
after 14-21 days from the initial bleeding;
• Patient >50 years should avoid operation with in 1 week from the last bleeding ;
• Patients with giant aneurysms, wide base aneurysms should wait for the retraction of the brain edema, for the operations are difficult.
Open surgery for aneurysm clipping
•approach•By microsurgery and special instruments•Endoscope-assisting operation •Close the neck of the aneurysms keep the aneurysms-bearing artery open and protect the nearby blood vessels and nerves
Pros of the aneurysm clipping
•For the reconstruction of endomembrane of the blood vessels, which is the most important against the pressure of the blood flow.
•Anatomically “cure”: better durance, less incidence of recurrence
•Can remove the haematoma in the subarachnoid space and in the cerebral tissue, reduce the intracranial pressure and alleviate the vasospasm.
•Require skilled neurosurgeons
•Invasive, with many complications: retracting the brain tissues and cranial nerves, poor tolerance by severe, aged patients or patients with systematic co-morbidities
•High risk for posterior circulation aneurysms
Cons of the aneurysm clipping

3 .endovascular treatment
history
1974: Self made latex balloon
1988: mechanic detachable coil system
1991: Guglielmi detachable coil, GDC
recent development : Trufill DCS Orbit ; Hydrocoil
Matrix coil
stent assisted coil
Onyx glue emblization

Endovascular treatment is best suitable for the aneurysms located between posterior cerebral artery and anterior inferior cerebelar artery on the basilar artery.
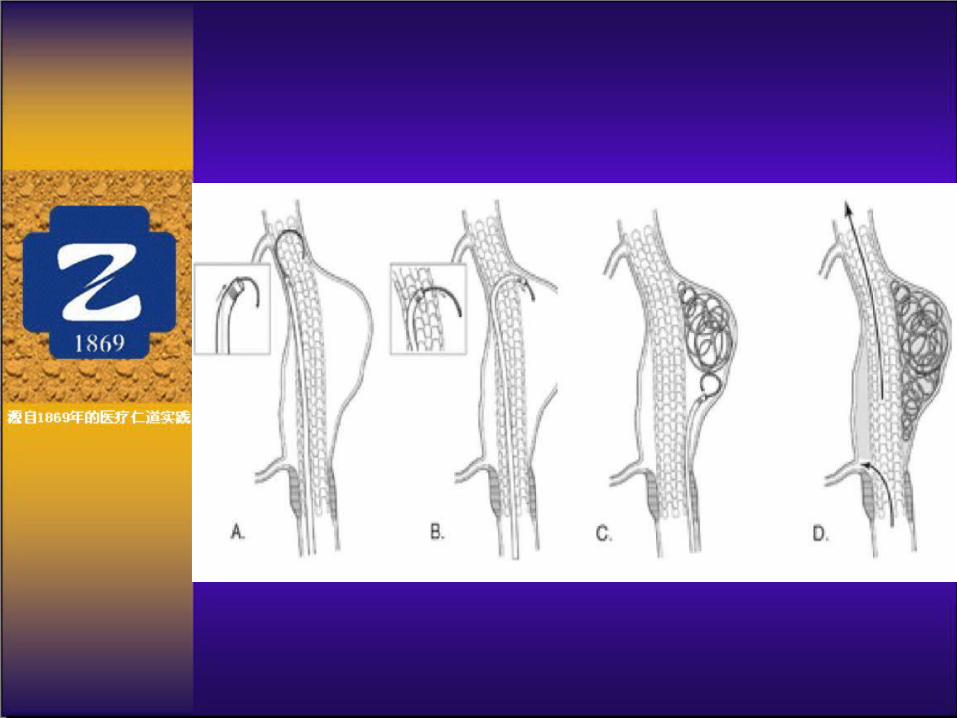
broad neck aneurysms are difficult to treat by endovascular techniques. Endovascular stent could be placed inside the aneurysm-bearing arteries to constrain the coil. The stent assisted coiling is broadly applied in intracranial broad neck aneurysm, giant aneurysm, dissecting aneurysm, pseudoaneurysm, fusiform aneurysm.
The intracranial stent is necessary for the re-construction of the arteries, and for reducing the pressure to the artery wall. It is also helpful to the embolization inside the aneurysms and to the formation of the endomembrane of the arteries to closed the neck of the aneurysms 。
•Stent assisted coiling
Indication of endovascular treatment
endovascular treatment is suitable for more than 90% aneurysms, except for the infectious aneurysms or aneurysms with large haematoma.
Pros of endovascular treatment
• Avoid open surgery, less invasive, no retraction of the brain, less complications ;
• Do not limited by the operation approaches ;
• Less in-hospital time, faster recovery

Cons of endovascular treatment
• Not suitable for the reconstruction of the endomenbrane of the arteries.
• More cases with incomplete embolization, higher rate of re-rupture and need for further treatment;
• Higher rate of cerebral infarction and vasospasm.
• Higher cost in China (but more inexpensive in some countries).

(2).Vascular malformation(2).Vascular malformation

Classification
•Arteriovenou malformation
•cavernous hemangioma
•telangiectasis
•Venous maformation

(( 11 )) Arteriovenous malformation,AVMArteriovenous malformation,AVM
• AVM is the direct communication of arteries and veins in the brain. The blood in the arteries directly goes in to veins without passing through capillaries
• this pathophysiology cause a series of homodynamic disturbance.
Clinical manifestation
1. bleeding: 68% of the AVM patients2. Epilepsy seizures: 17%-47% of the patients
begin with epilepsy seizures, which is caused by the lack of blood supply resulting from the steal phenomenon, the incidence of the seizures is associated with the size, locations and the type of AVM
3. headaches (not a specific symptoms) 15%-24% of the patients begin with headache

diagnosis
•Clinical manifestations
•CT 、 MRI/MRA 、 DSA

Treatment
•Surgical
•endovascular
•Stereotaxic radial therapy
•Combined therapies
Operation
Remove the AVM, improve the blood supply, control the seizures

Endovascular therapy
•Only simple AVM can be controlled by endovascular therapy, any residual will lead to recurrence •The improvement of endovascular therapy will reduce the rate of incomplete embolization and recurrence
•Gamma knife and x-knife•Indicated for minor AVM (<3cm in diameter, high risk for operation, small residual after operation or embolization, lesions in functional areas or patients that can not tolerant open surgery.•It often take 2-3 years for the closure of the AVM. About 20% cases failed. Less than 25% cases are suitable for stereotaxic RT.
Stereotaxic radial therapy
Combined therapy
•For most of the AVM patients, combined therapies
of the 3 treatments are the optimal therapies.•Open surgery, endovascular embolization and
stereotaxic radial therapy will not replace each
other.
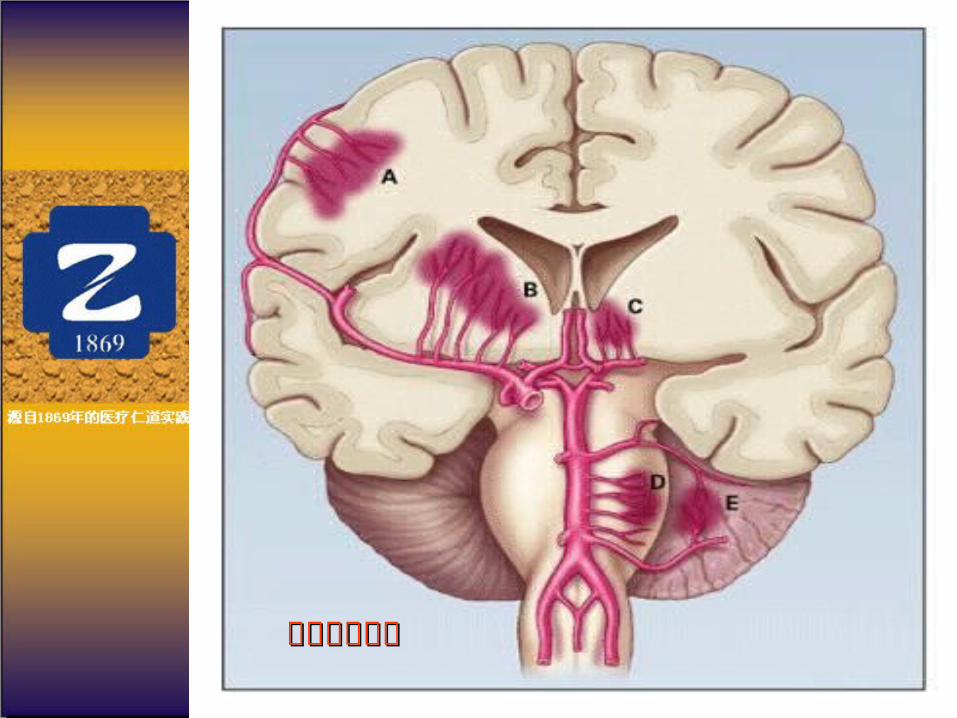
(( 22 )) Cavernous angiomaCavernous angioma

20-40 years old epilepsy seizures, repeated bleeding or neurological deficittreatment: operation (microsurgery, with navigation) stereotaxic observe

(3).(3).Hypertensive hemorrhage
高血压脑出血高血压脑出血
•Open procedure to reduce intracranial pressure•Stereotaxic respiration combine with urokinase
2.Occlusive cerebral vascular 2.Occlusive cerebral vascular diseasesdiseases
• Stenosis of carotid artery or vertebral-basilar artery
• Acute embolization
(1).Carotid Artery Stenosis(1).Carotid Artery Stenosis
•Ischemic stroke claims for 85% of the stroke patients. The world wide incidence is 200/105. the most common cause of ischemic stroke is the carotid stenosis caused by Atherosclerotic thrombosis. The narrower the carotid artery, the more incidence of the stroke.
•The plaque in carotid artery is composed of cholesterol cellulose and platelets. In severe narrowed carotid artery, the micro-thrombi are flushed by the unsteady blood flow and detach from the endomembrane, causing transient ischemic attack (TIA) or cerebral infarction. Timely intervention of the sclerotic stenosis of the carotid artery is crucial for the prevention of the transformation of TIA or reversible ischemic neurological deficit (RIND) to complete infarction.

Treatment
•Carotid endarterectomy
•Endovascular therapy
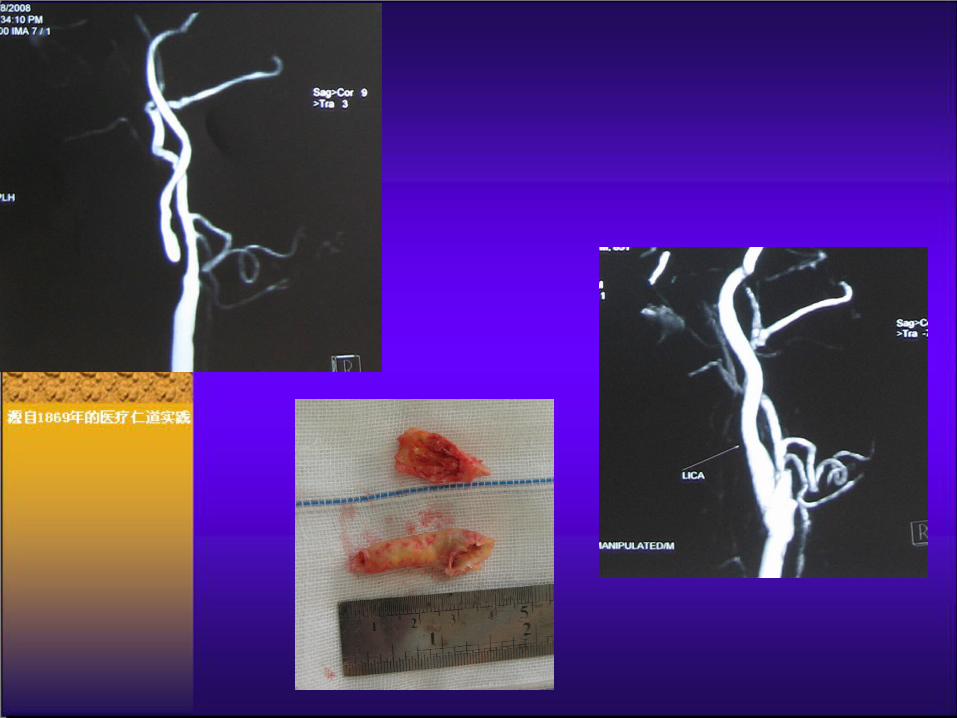
Surgical treatment of carotid stenosis
• Firstly performed in 1954, Carotid endarterectomy CEA have become an effective method to alleviate carotid stenosis. According to a study, 9% patients with carotid stenosis about 70%-90% that receive CEA have ipsilateral ischemic stroke, while 26% patients that received optimal medical treatment have ipsilateral stroke.

CEA剪辑.mpg
Interventional therapy
• PTAS have become one of the most commonly used methods to treat carotid stenosis. This method restored the diameter of the narrowed carotid artery, improve the blood flow to the brain by placing a stent in the locus of the stenosis. The stent also help to avoid the detachment of the atherosclerotic plaque. Effect rate of PTAS is 89.7-100%, restenosis incidence is 4%.
• Main purpose of stenting is to improve the blood flow to the brain.
• In recent 5 years, better catheter, sheath and stent and better protection of the distal arteries make the interventional therapy become more and more interested by neurological doctors.

(2) Moyamoya Dieases
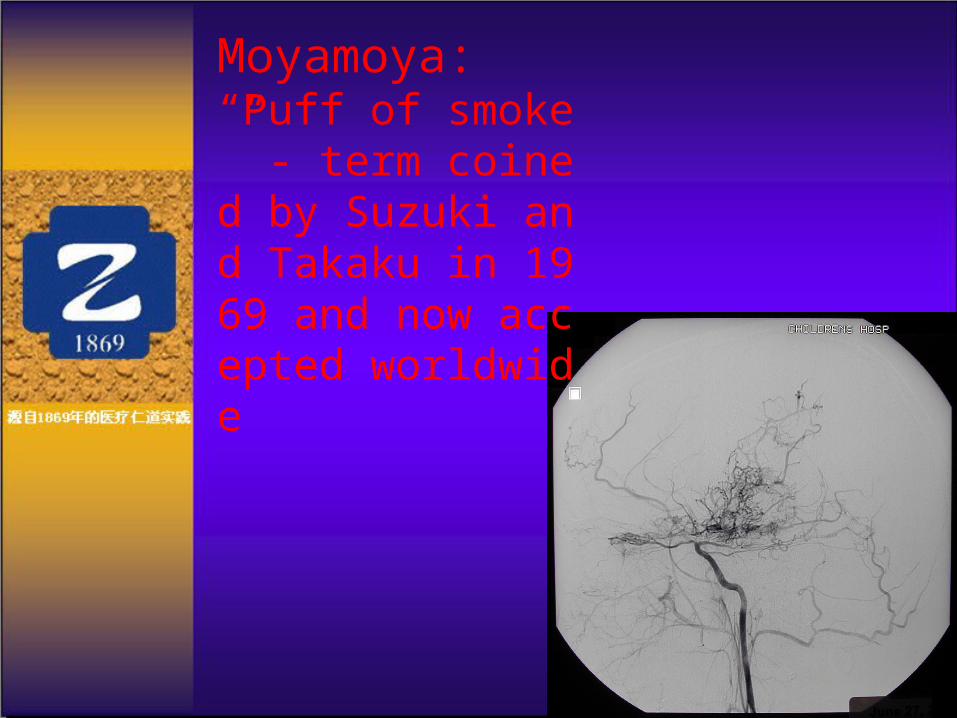
Moyamoya:“Puff of smoke” - term coined by Suzuki and Takaku in 1969 and now accepted worldwide
TrendsTrends
•With the development of microsurgical devices, interventional materials and clinical techniques, the surgery treatment of cerebral vascular diseases will be more widely applied •Time is brain, time is important in both hemorrhagic and ischemic CVDs. Early transport to clinical center of CVDs, early diagnosis and early treatment will bring about good recovery .