Embed Size (px)
Citation preview

Review: Surgery for Transposition of the Great Arteriesin the First Year of Life
CLAUDIO ZAVANELLA, M.D.,* S. SUBRAMANIAN, M.D., F.R.C.S.,
Elective intracardiac repair by the Mustard operation isrecommended in patients with transposition of the greatarteries and intact ventricular septum in the first year of life(Fig. 1). In patients with associated ventricular septal defectin the first three months of life, early banding followed byearly debanding before the first year of life is recommended.When the left ventricular outflow tract obstruction is discreteat valvular or subvalvular level, Mustard operation, closureof the ventricular septal defect and direct relief of out-flow obstruction is acceptable, but in patients with an unfavor-able left ventricular outflow tract anatomy, a preliminary shuntfollowed by a Rastelli operation after the age of four years willprobably result in a greater salvage. The utilization ofsurface induced profound hypothermia and circulatory arrestallows for more precise and rapid surgery and is shown to bea definite advantage in the very young infant.
TRANSPOSITION OF THE great arteries account forabout 20% of cardiac deaths in newborns. In a
group of 240 cases of transposition of the greatarteries studied by Shaher,30 63% had intact ventricularseptum and 70% of these infants died in the first monthsof life. It is not surprising, therefore, that this lesionhas been of great interest to cardiologists and surgeonssince Albert proposed his first experimental model forintracardiac correction of the transposition of thegreat arteries.2 Other surgical efforts in this directionwere made by Merendino,23 Senning,29 Barnard,5 butMustard26 was the first to report in 1964 a successfulapproach to this relatively simple defect using anintracardiac baffle of pericardium. This procedure wascarried out successfully by Mustard in patients andsubsequently reproduced very satisfactorily by numer-ous centers.1,9,10,17,21,31,36,43Timing of the corrective procedure for transposition,
however, continued to be the subject of controversy.McGoon,21 Rashkind,28 Mustard25 recommended thatthe corrective procedure should be delayed till thechild was two years old. The early reluctance tocorrect infants with transposition of the great arteries
* Fellow, Department of Cardiovascular Surgery.t Chief, Division of Cardiovascular Surgery, Professor of Surgery,
State University of New York at Buffalo.Submitted for publication: May 2, 1977.
From the Department of Cardiovascular Surgery,Children's Hospital, Buffalo, New York
was presumably related to the alleged high mortalityof the pump oxygenator.'9'43 In view of the reportedhigh mortality for primary correction of transpositionof the great arteries in infancy,14 the two stage ap-proach to the surgical treatment in transposition con-tinued to be in vogue until early 1971.
Palliative Procedures
Rashkind's balloon atrial septostomy (BAS) haschanged the outlook of these severely hypoxic new-borns. Results at the Buffalo Children's Hospitalindicate that the mortality of 84% has decreased to28% with the introduction of balloon septostomy.4'Similar results have been reported by Neches.27 Theprocedure of balloon septostomy is occasionally insuf-ficient to control the severe hypoxia and it does notprevent cerebrovascular accidents. Furthermore, theballoon-created defects have not consistently been longlasting. Measurement at autopsy or at surgical correc-tion showed that three-quarters had defects as largeas the fossa ovale. The larger defects were observedin children over the age of two years. With regard tothe smaller defects, serial cardiac catheterization sug-gested that in two instances it constricted over aperiod of months. In two other patients, the Rashkindtechnic failed to fracture the atrial septum. TheRashkind technic is effective in creating adequateseptostomy in most but not in all patients. In spite ofa good balloon septostomy, there are a number ofpatients who continue to have poor mixing, as wasseen in eight patients with poor clinical results. Asurgical septectomy would not have contributed furtherdue to the adequate size of the balloon created defect.We feel that if the initial Rashkind septostomy istechnically unsatisfactory, a repeat septostomy is con-traindicated and could be hazardous to life. An analysisof the long term results of balloon atrial septostomy
0003-4932-78-0200-0143-0085 C J. B. Lippincott Company
143
ZAVANELLA AND SUBRAMANIAN
% ~~~~~~N=427.
staged approach was clearly unacceptable. Bonchekand Starr10 utilizing extracorporeal circulation reporteda series of ten patients below the age of two yearswith two deaths and indicated the possibility and needfor early correction. Encouraged by our early ex-periences utilizing surface induced profound hypother-mia and circulatory arrest as advocated by the Kyotogroup24 and Barratt-Boyes,8 we began offering primaryintracardiac correction to all patients with transpositionof the great arteries both simple and complex.37'38
Materials
Our total experience at the Children's Hospitalbetween November 1967 and November 1976 with
I; & , intracardiac surgery for transposition of the great01-I I Yrs. i arteries consists of 170 patients. Of these, 82 were
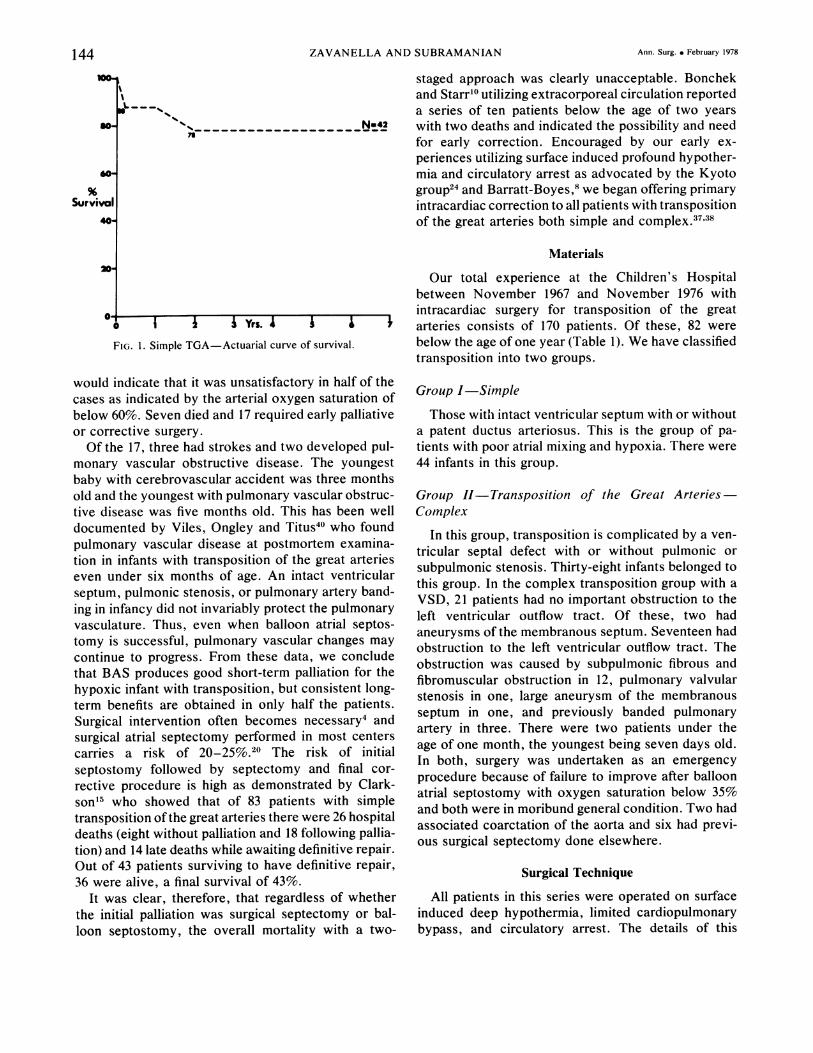
FIG. 1. Simple TGA-Actuarial curve of survival. below the age of one year (Table 1). We have classified
transposition into two groups.
would indicate that it was unsatisfactory in half of thecases as indicated by the arterial oxygen saturation ofbelow 60%. Seven died and 17 required early palliativeor corrective surgery.
Of the 17, three had strokes and two developed pul-monary vascular obstructive disease. The youngestbaby with cerebrovascular accident was three monthsold and the youngest with pulmonary vascular obstruc-tive disease was five months old. This has been welldocumented by Viles, Ongley and Titus40 who foundpulmonary vascular disease at postmortem examina-tion in infants with transposition of the great arterieseven under six months of age. An intact ventricularseptum, pulmonic stenosis, or pulmonary artery band-ing in infancy did not invariably protect the pulmonaryvasculature. Thus, even when balloon atrial septos-tomy is successful, pulmonary vascular changes may
continue to progress. From these data, we concludethat BAS produces good short-term palliation for thehypoxic infant with transposition, but consistent long-term benefits are obtained in only half the patients.Surgical intervention often becomes necessary4 andsurgical atrial septectomy performed in most centerscarries a risk of 20-25%.20 The risk of initialseptostomy followed by septectomy and final cor-
rective procedure is high as demonstrated by Clark-son15 who showed that of 83 patients with simpletransposition of the great arteries there were 26 hospitaldeaths (eight without palliation and 18 following pallia-tion) and 14 late deaths while awaiting definitive repair.Out of 43 patients surviving to have definitive repair,36 were alive, a final survival of 43%.
It was clear, therefore, that regardless of whetherthe initial palliation was surgical septectomy or bal-loon septostomy, the overall mortality with a two-
Group I-Simple
Those with intact ventricular septum with or withouta patent ductus arteriosus. This is the group of pa-
tients with poor atrial mixing and hypoxia. There were
44 infants in this group.
Group II-Transposition of the Great Arteries-Complex
In this group, transposition is complicated by a ven-
tricular septal defect with or without pulmonic or
subpulmonic stenosis. Thirty-eight infants belonged tothis group. In the complex transposition group with a
VSD, 21 patients had no important obstruction to theleft ventricular outflow tract. Of these, two hadaneurysms of the membranous septum. Seventeen hadobstruction to the left ventricular outflow tract. Theobstruction was caused by subpulmonic fibrous andfibromuscular obstruction in 12, pulmonary valvularstenosis in one, large aneurysm of the membranousseptum in one, and previously banded pulmonaryartery in three. There were two patients under theage of one month, the youngest being seven days old.In both, surgery was undertaken as an emergency
procedure because of failure to improve after balloonatrial septostomy with oxygen saturation below 35%and both were in moribund general condition. Two hadassociated coarctation of the aorta and six had previ-ous surgical septectomy done elsewhere.
Surgical Technique
All patients in this series were operated on surfaceinduced deep hypothermia, limited cardiopulmonarybypass, and circulatory arrest. The details of this
so-
60-
Survival40
144 Ann. Surg. e February 1978
SURGERY FOR ARTERY TRANSPOSITION
technique have been described by us elsewhere.3228Anesthesia is induced and maintained with Halothaneand the patients is paralyzed with intermittent suc-cinylcholine or curare. Early in our experience, thepatient was packed with crushed ice bags but thistechnique has now been superseded by placing theinfant during cooling in a "Hypothermia Chamber"*which has been developed by US.39 The chamber con-sists of two parts. The lower half is a powerfulrefrigerating unit with a blower fan which circulatescold air into the upper chamber which is a transparentplexiglass box. The ambient temperature in thechamber is recorded on a chart paper and theesophageal and rectal temperatures are displayed onthe console. The chamber is hinged for easy entry andexit and all monitoring and anesthesia lines are broughtout through a porthole. The refrigerator is capable oflowering the ambient temperature down to - 100and usually 0 to -5° is adequate. The infant isadditionally placed on a circulating water blanket tocool the back. The cooling time using this chamber isless than the older methods of ice bags or the waterbed. An average four kilogram infant can be cooledfrom 370 to 250 in 36 minutes with the chambercompared to 60 minutes with the water bed as against56 minutes with the ice bags.33
At an esophageal temperature of 250, the infant isremoved from the chamber and placed on the operatingtable and thoracotomy is performed. Cardiopulmonarybypass is established with a single atrial catheter andthe arterial return is to the ascending aorta. ABentley-Temptrolt infant oxygenator is used and theintegral heat exchanger in this unit has been found tobe adequate for cooling and rewarming. The initialprime consists of equal quantities of fresh frozenplasma and 5% dextrose with added mannitol andpotassium. Following total hemodilution perfusion toachieve an esophageal temperature to 18-20°, cardio-circulatory arrest is obtained and the patient is ex-sanguinated into the reservoir of the oxygenator. Thisinitial prime is now discarded and replaced with plate-let depleted red cells. On completion of the intra-cardiac procedure, the left atrium is cannulated, thepatient is transfused to the extent that he was ex-sanguinated earlier and cardiopulmonary bypass is re-established and rewarming carried out to 34-36°esophageal depending on the adequacy of the cardiacoutput.The atrial incision is oblique and directed towards
the junction of the superior and inferior pulmonaryveins and in the lower half of the atrial wall to avoid
injury to the sinus node. The atrial septum is com-pletely excised leaving a fringe of atrial tissue nearthe tricuspid valve to protect the middle internodaltract. The raw surface of the endocardium is notresutured routinely as recommended by Mustard.26Early in the series, the coronary sinus was cut backinto the left atrium, but subsequently, this maneuverwas omitted in order to prevent any possible injuryto the tail of the A-V node. For some time we believedthat this change in technique might have an influencein the preservation of postoperative normal sinusrhythm and in a lesser incidence of arrhythmia, butthis impression has not been substantiated by data.
Because of our satisfactory early experience withpericardium as the material for the baffle with noclinical obstructive complications related to it, we havecontinued to use pericardium exclusively as theintra-atrial baffle in patients with transposition of thegreat arteries. Such a uniformly satisfactory experiencewould indicate that the nature of the material is un-likely to be the influencing factor in producing stenoticcomplications. The shape, size, and the manner oftailoring the baffle inside the atrium are probably thedeterminants. Even in those patients who had had apericardiotomy during the previous surgical septec-tomy, it was possible to get an adequate piece ofpericardium. The pericardium is roughly rectangular,slightly broader at the superior vena caval end and alittle bit larger than required. After performance of theposterior suture line around the pulmonary venousorifice, the width of the pericardium at its waist isdetermined where it is sutured to the residue of theatrial septum near the tricuspid valve. The excesswidth of the pericardium at this point is cut back andtrimmed off towards the superior and inferior venaecavae leaving two rectangular extensions towards thesestructures. This shape of the pericardium is somewhatsimilar to the trouser-leg patch advocated by Brom3,"'in that it insures that there is an adequate pericardialwall to the new left and right atria. Care is alsotaken to ensure that there is an adequate superiorvena caval inlet (12mm diameter in the infant group asmeasured by a Hegar dilator). The superior vena cavalextension of the patch is little more redundant than theinferior caval extension since in our experience, itis almost impossible to produce obstruction to theinferior vena cava. In half the patients, the coronarysinus blood was returned with with caval blood to theleft side and in the rest, the coronary sinus bloodreturned to the right ventricle along with the pulmonaryvenous drainage. In half the infants, the right atriumwas not enlarged but closed by direct suture and inthe other half, the right atrium was enlarged either bypericardium or a woven Dacron vascular prosthesis in
*Manufactured by Thermo-Temp, Buffalo, New York.tBentley Laboratories, Inc., Santa Ana, California.
Vol. 187 * No. 2 145

ZAVANELLA AND SUBRAMANIAN
TABLE 1. Transpositioni ol the Great Arteries
Simple Complex
Total Deaths Total Deaths
<i mos. 2 2 0 01-3 mos. 8 1 8 33-6 mos. 12 1 9 36-12 mos. 22 0 21 4
Total 44 4 38 10
order to provide a larger reservoir capacity for thenew left atrium. The value of such right atrial en-
largement has been debated by Berman9 and Kirklint8but there are no firm data to indicate whether thisimproves the postoperative cardiac performance. Thismanuever permits us to use a more redundantpericardial baffle than one would normally dare. Uponcompletion of the procedure, saline is instilled intothe left atrium through the appendage to distend thebaffle, detect any leaks, and to assess the size of thebaffle. Should it appear to be redundant, it is reefedwith horizontal mattress sutures at appropriate pointsto avoid pulmonary venous obstruction. This techniqueof intraoperative assessment gives a good three dimen-sional visualization of the contour of the baffle.A right ventriculotomy was not used for the closure
of the ventricular septal defect in any of these pa-tients. In two, muscular defects were approachedthrough an apical left ventriculotomy. In two, theventricular defect was closed through the root of theaorta and in two others through the pulmonary artery.Upon completion of the intracardiac procedure, theleft atrium is cannulated and the patient rewarmed on
bypass to 35°. Thermodilution cardiac output catheteris inserted through the right atrium and advancedinto the aorttc root for postoperative management; rightand left atrial catheters are also inserted and pacemakerwires, both atrial and ventricular, are sutured to theheart.The postoperative care of these patients is no dif-
ferent from other seriously ill infants who undergocardiac surgery, and the techniques of managementhave been described by us elsewhere.34'35
Results
Table 1 illustrates the operative mortality in. allgroups of patients undergoing surgery for transpositionof the great arteries in the first year of life.
Group I
Of the 44 patients with intact ventricular septum,there were four deaths, a mortality of 9%. Of these,
two were under one month of age; one died of renalfailure, the other due to digitalis intoxication. A six-week-old infant was severely hypoxic, dehydrated dueto gastroenteritis, and moribund prior to surgery, andthe wisdom of choosing primary intracardiac surgery inthis patient is questionable. The five-month-old childdied following reoperation for postoperative hemor-rhage.
Group II
In the complex transposition group, death was due torenal failure in two, respiratory insufficiency two daysafter surgery in one, severe intravascular hemolysisand hematuria in one patient. Error in postoperativemanagement resulted in death of one patient who wasextubated 24 hours following surgery and subsequentlydeveloped respiratory distress, and an unrelieved ob-structing mucous plug in the trachea caused his death.Low cardiac output secondary to inadequately relievedobstruction to the left ventricular outflow tract wasthe cause of death in the remaining five. The mortalityin this group was ten out of 38 patients (26%).The high mortality (6 out of 12) in the group with
ventricular septal defect and left ventricular outflowtract obstruction was due to our inability to relievethe long fibromuscular obstruction of the left ventricu-lar outflow tract. The poor result in this group hasled us to review our policy of primary intracardiaccorrection in this age group and we currently recom-mend initial shunting followed by an external valvedconduit operation after four years of age.
Late Results
In addition to the operative mortality, there werefour late deaths. One infant had an excellent clinicalresult and was sent home in junctional rhythm but wasadmitted to another hospital six months after surgerywith cardiac arrest and, presumably, this was relatedto his arrhythmia. The third patient died of pneumoniaand the cause of death could not be determined inthe fourth. The other late death was related to poorlyfunctioning right ventricle associated with rightventricular myocardiopathy and heart failure. Two pa-tients underwent reoperation. The first, a two-month-old infant who had undergone surgery for transposi-tion with intact ventricular septum, showed evidence ofleft ventricular outflow tract obstruction at postopera-tive follow-up and was restudied and found to havea small gradient across the left ventricular outflowtract. She was restudied four years later and thisgradient was found to have increased and she had clini-cal symptoms of severe pulmonary outflow obstructionwith syncopal episodes. At surgery, no discrete ob-
146 Ann. Surg. o February 1978
SURGERY FOR ARTERY TRANSPOSITION 147
struction was found underneath the pulmonary valveand a left ventricular outflow tract myotomy wascarried out with impressive clinical improvement.The second patient developed right ventricular myo-
cardiopathy and tricuspid regurgitation and underwentsuccessful tricuspid valve replacement. There were no
reoperations for vena caval or pulmonary venous ob-structions and none for important intracardiac shunts.Of the 64 long-term survivors, clinical follow-up isavailable in 46 patients and 27 patients have beenrestudied with cardiac catheterization and angiocardio-grams.
Follow-up
Clinical and electrocardiographic follow-up is avail-able in 63 long-term survivors, and hemodynamicstudies and angiocardiograms are available in 27 pa-tients. The follow-up status of all the patients has beengraded excellent, good, or poor depending upon thefindings. These findings are summarized in Table 2.
Late clinical follow-up is available in only 41 patientsand, of these, 39 were considered to be a good resultand two were poor results. Postoperative electro-cardiograms were reviewed in these 41 patients and inan additional 22 whose last cardiogram was at the timeof discharge from the hospital. Details of the post-operative rhythm for all 63 patients are provided inTable 3. Forty-seven patients were in normal sinusrhythm and were, therefore, considered to have ex-
cellent results (75%). An additional two patients hadsinus rhythm with occasional episodes of junctionalrhythm. The patients with 2:1 block, trifascicularblock, and supraventricular arrhythmia are consideredto be poor results. Of the 27 patients restudied withcardiac catheterization and angiocardiograms, 10 didnot live in the immediate area and so were catheterizedprior to discharge from the hospital; 17 were studiedelectively as late follow-ups ranging from one to fiveyears. Of the total 27 patients, seven showed excellentresults with no hemodynamic or angiographic abnor-malities; 18 patients were considered good resultseven if they had minor residue not requiring furtherintervention; and, two patients who had pulmonaryartery hypertension prior to surgery continued to have
TABLE 2. Assessmnent at Follow-up
Excellent Good Poor
Clinical-late 39 2ECG 47 12 4Cardiac cath 7 18 2All of the above 5 20 2*
* Reoperated.
TABLE 3. Postoperative RhYthmn
Sinus 47 (75%)Sinus with occasional junctional 2Supraventricular 2Sick sinus 2Junctional 7Trifascicular block 12:1 block 2
moderately elevated pulmonary artery pressure andvascular resistances. These latter two patients werealso considered good results since pulmonary arteryhypertension did not progress after surgery. Thecardiac catheterization abnormalities are listed inTable 4.When all three studies-clinical, electrocardio-
graphic, and hemodynamic-were taken into con-sideration in evaluating the patients, five patientscould be considered as excellent results, 20 as good,and two as poor. The two patients overall who wereconsidered poor results underwent reoperation, one forsubpulmonic obstruction and the other for tricuspidvalve regurgitation. It is interesting to note that thisgood and excellent follow-up in 90% of the patients issuperior to the results in the older age group in whomonly 80% of the patients were found to be in thegood category. It further reinforces our plea for earlycorrection of transposition in the first year of life.
Discussion
It is now abundantly clear from the literature thatsurgical results obtained with simple transposition ofthe great arteries are excellent. The mortality has beenconsistently below 10% in most reported series. Theresults have been good even in very small infants overone month of age and similar good results have beenreported by others. 10"13,17,31 The need for early correc-tion of simple transposition of the great arteries isexemplified by the data presented here and also by the
TABLE 4. Postoperative Cardiac Cath
SVC obstruction mild-4severe- I
Subpulmonic obstruction mild-ilsevere-I *
Baffle holes trivial-9
Tricuspid regurgitation mild-Isevere-I *
Pulmonary hypertension 2t
RV dysfunction I
* Reoperated.t Present before surgery no progression after surgery.
VOl. 187.oNO. 2
ZAVANELLA AND SUBRAMANIAN Ann. Surg. * February 1978
,-f-_._-- N 42
434
44
4
47t~~~~
- _ _2,
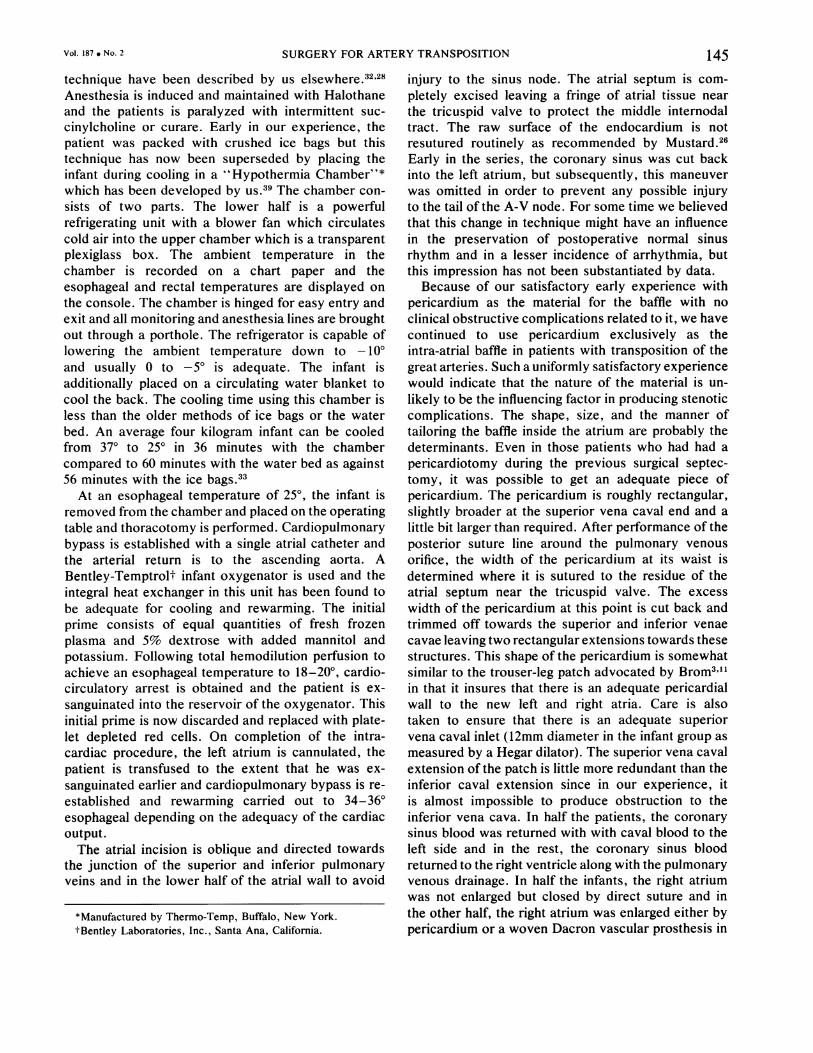
FIG. 2. Simple TGA-The actuarial curve for un-treated patients with simpleTGA was constructed datapublished by Liebman et al.(Circulation 40:237, 1969).Both curves of survivalfollowing the Mustard op-eration should be viewedin the perspective given bydifferent start points in thenatural history curve mod-ified by balloon atrial sep-tostomy.
VWl lo2 3 4 Glvi 21^ 2
----10 HNATURAL HISTORY
- MODIFICATION BY A.S.
------ JMUSTARD OPERATION <1 YR.
MUSTARD OPRATION >1 YR.
data from Clarkson'5 who showed that overall mortalityrates are 63% and 23% when corrective surgery was
undertaken at the average ages of 37 months and 13months respectively. However, when early correctiopwas carried out at 3-6 months of age, the same
group reported a mortality of 8.5%. The mortality rateof 9% reported in this series is comparable6 to mostpublished series and confirms our policy of early cor-
rection in cases of failure of balloon septostomy and
V
3-6_
6-12_sOESAW0COI"C
MCAT^H C_EC WNE1
4mnINEEIwHI
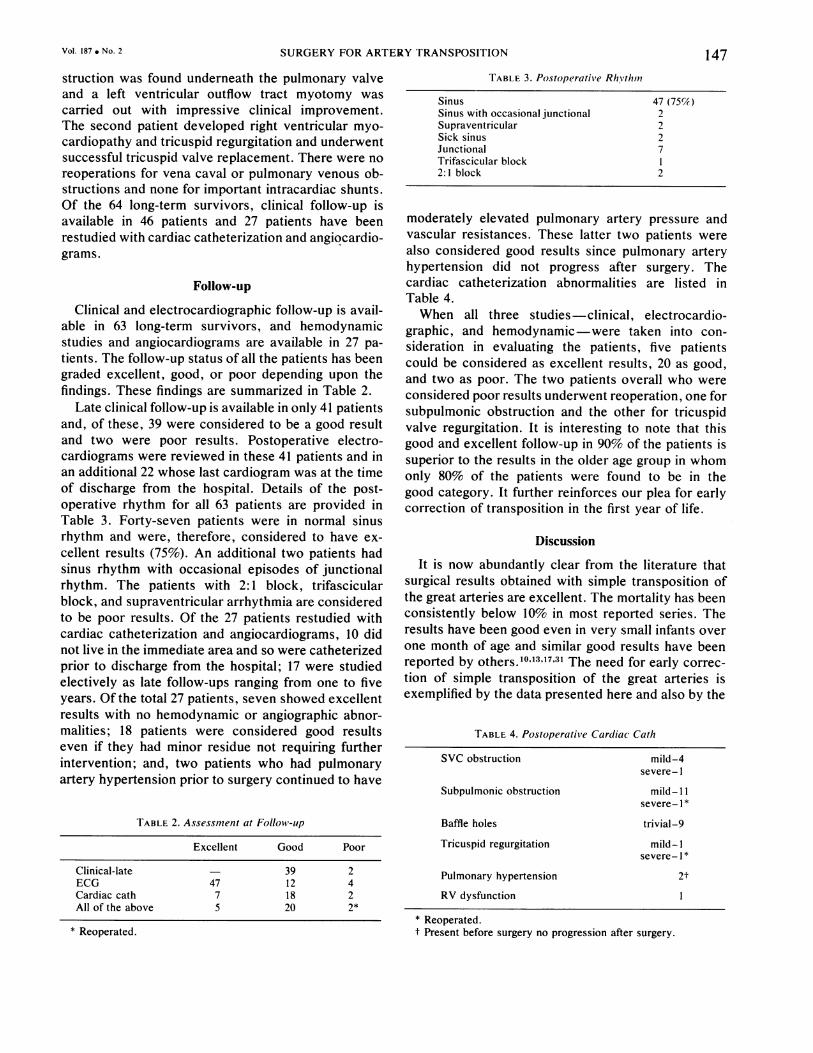
FIG. 3. TGA protocol.
early elective repair after three months to preventcerebrovascular accidents or pulmonary vascular ob-structive disease (Figs. 2 and 3). Early correctionestablishes normal growth and physical development ofthe child and relieves the family of financial andpsychological trauma of multiple staged procedures.The surgical results in the complex transposition
group are less encouraging and this is due to thehigh mortality in the group with left ventricularoutflow tract obstruction. The risk of surgery in TGAwith ventricular septal defect and pulmonary arteryhypertension in the very young sick infant is alsohigh and this leads one to speculate as to the pos-
sible virtures of early banding of infants underthree months with uncontrolled heart failure with a
view to early debanding and complete correction.Current data for early banding of the pulmonaryartery in this group of complex transposition are notavailable but it is advocated by Barratt-Boyes7 even
though Castaneda12 has shown that complete correc-
tion can be carried out in the very young infantwith an acceptable mortality. The three infants in thisgroup with previous pulmonary artery banding under-went surgery without any undue complications andeven though we do not have data to support our
policy, we recommend banding of the pulmonaryartery in this group in the first three months of lifeand early debanding before they are one year of age.
148
3 6 9
Vol. 187 * No. 2 SURGERY FOR ARTERY TRANSPOSITION 149
By early debanding, we can avoid reconstruction ofthe posteriorly placed pulmonary artery.
Dissatisfied with the long term result of palliationobtained in patients with transposition of the greatarteries and left ventricular outflow tract obstructionwith palliative procedures, we had earlier advocatedone stage primary correction in these infants. Analy-sis of the results in this group indicates that thisapproach is suitable for patients with discrete pul-monary valvular or fibrous or membranous subpul-monic obstruction, but the mortality obtained in thegroup of patients with fibromuscular long narrow leftventricular outflow tract obstruction is high. Excel-lent operative results reported by McGoon22 obtainedin children over the age of five undergoing Rastellioperation for TGA, VSD, and LVOT would indicatethat, if one is willing to accept the initial mortalityof the palliative procedure and the attrition whileawaiting corrective surgery, this staged approach inthis complex group may be superior. We have, there-fore, now retreated from our earlier support of primaryintracardiac repair in infants with left ventricular out-flow tract obstruction in transposition and favor atwo stage approach, initial shunt followed at age fouryears by a valved external conduit operation (Rastelliprocedure).
Recently Jatene16 proposed a spectacular new ap-proach to transposition of the great arteries withventricular septal defect and pulmonary artery hyper-tension. This consists of transplanting the coronaryostia to the posterior great artery and transecting thetwo great arteries and "switching" them over. Hisfirst case was a small infant who did extremely well,and postoperative studies and angiograms supportedthe validity of this approach. Since then, however,47 such operations have been carried out in the worldwith only seven survivors. Contrary to our expecta-tions, this method of complete correction of transposi-tion has carried a very high mortality possibly relatedto unfavorable selection of patients. Until such time aswe can demonstrate that the current method of treat-ment of transposition; namely, Mustard operation andventricular septal defect closure, is either unacceptablein terms of mortality or late mordibity, the Jateneoperation will continue to be experimental.
Pericardium has been used exclusively by us as abaffle and to date, we do not have any instances ofpulmonary venous obstruction and patients who areshown to have superior vena caval narrowing at re-study were suspected to have some degree of obstruc-tion in the postoperative period. Late caval and pul-monary venous obstruction has been attributed toshrinkage of pericardium by some and to the choiceof the material, namely, Dacron, by others. We at-
tribute our satisfactory results to the technique ofplacement of the patch and the method of tailoringit and also to our technique of testing the patch atthe time of surgery to prevent too much laxity ortightness. We believe that the technique of placementof the baffle rather than the material itself is re-sponsible for the minimal complications in our series.
Postoperative hemodynamic studies reported byWagner indicate that patients repaired in the firstyear of life all ended up with normal ejection frac-tions of the right ventricle. In patients repaired at alater age, contractility may have suffered by the de-layed repair. Although age at surgery is not the onlydeterminant ofcardiac performance, the data presentedby Wagner would favor early repair.42To enlarge the right atrium or not is a question that
has not yet been determined by postoperative studies.Theoretically, it would be an advantage to provide alarger reservoir capacity of the new functional leftatrium, but postoperative studies in patients in whomthe atrium had not been enlarged show that in bothatria the V waves were dominant but generallyhigher in the "new" left atrium which feeds thesystemic right ventricle. The pressure curves wererepresentative of underlying ventricular performanceand not of atrial size. The data show that the featuresof the new atrial curves indicate that the surgery hasachieved functional as well as anatomical corrections.Typical abnormal contours are expressive of right andleft ventrical performance problems. Kirklin's specula-tion that increasing the right atrial cavity may decreaseeffectiveness of the atrial contraction in the post-operative period is a valid one. The main advantageof enlarging the right atrium lies in our ability toplace a redundant intracardiac patch without fear ofobstructing the pulmonary venous return.
References
1. Aberdeen, E., Waterston, D. J., Carr, I., et al.: SuccessfulCorrection of Transposed Great Arteries by Mustard'sOperation. Lancet, 1:1233, 1965.
2. Albert, H. M.: Surgical Correction of Transposition of theGreat Arteries. Surg. Forum, 5:74, 1954.
3. Amato, J. J., Rheinlander, H. F. and Cleveland, R. J.: AMethod for Rapid Tailoring of the Intraatrial Baffle inTransposition of the Great Arteries. Ann. Thorac. Surg.20:586, 1975.
4. Baker, F., Baker, L., Zoltun, R. and Zuberbuhler, J. R.:Effectiveness of the Rashkind Procedure in Transposition ofthe Great Arteries in Infants. Circulation, XLIII (Suppl. 1),I-1, 1971.
5. Barnard, C. N., Schrire, V. and Beck, W.: Complete Trans-position of the Great Vessels: A Successful Complete Cor-rection. J. Thorac. Cardiovasc. Surg. 43:768, 1962.
6. Barratt-Boyes, B. G.: Cardiac Surgery in Neonates and Infants.Circulation, 44:924, 1971.
7. Barratt-Boyes, B. G.: personal communication.8. Barratt-Boyes, B. G., Simpson, M. and Neutze, J. M.: Intra-

150 ZAVANELLA AND SUBRAMANIAN Ann. Surg. i February 1978
cardiac Surgery in Neonates and Infants Using DeepHypothermia with Surface Cooling and Limited Cardiopul-monary Bypass. Circulation, 43: 44:25, (Suppl. 1), 1971.
9. Berman, M. A., Talner, N. S. and Stansel, H. C. Jr.: Ex-perience with Mustard's Operation in Infants Less Than OneYear of Age: Emphasis on Late Complications IncludingPatch Stenosis. Surgery, 43:133, 1973.
10. Bonchek, L. I. and Starr, A.: Total Correction of Trans-position of the Great Arteries in Infancy on Initial SurgicalManagement. Ann. Thorac. Surg., 14:376, 1972.
11. Brom, G.: Various Types of Patch Used in Venous Reversalto Correction Transposition of the Great Arteries. Pre-sented-Bilboa, Spain, 1976.
12. Castaneda, A. R., Lamberti, J., Sade, R. M., et al.: OpenHeart Surgery During the First Three Months of Life. J.Thorac. Cardiovasc. Surg. 68:719, 1974.
13. Champsaur, G. L., Sokol, D. M., Trusler, G. A. and Mustard,W. T.: Repair of Transposition of the Great Arteries in 123Pediatric Patients. Circulation, XLVII: 1032, 1973.
14. Ching, E., DuShane, J. W., McGoon, D. C. and Danielson,G. K.: Total Correction of Cardiac Anomalies in InfancyUsing Extracorporeal Circulation. J. Thorac. Cardiovasc.Surg., 62:117, 1971.
15. Clarkson, P. M., Barratt-Boyes, B. G., Neutze, J. M. andLowe, J. B.: Results Over a Ten Year Period of Pal-liation Followed by Corrective Surgery for Complete Trans-position of the Great Arteries. Circulation, XLV: 1251, 1972.
16. Jatene, A. D., Fontes, V. F., Paulista, P. P. et al.: SuccessfulAnatomic Correction of Transposition of the Great Vessels.A Preliminary Report. Separata Arqu. bras. Card., 28: August1975.
17. Kilman, J. W., Williams, T. E., Jr., Kakos, G. S., et al.:Surgical Correction of Transposition Complex in Infancy. J.Thorac. Cardiovasc. Surg., 66:387, 1973.
18. Kirklin, J. W.: Letter to the Editor: Surgery 73:800, 1973(Berman, M. A., Talner, N. S., Stansel, H. C., Jr.:Experience with Mustard's Operation in Infants Less ThanOne Year of Age: Emphasis on Late Complications IncludingPatch Stenosis. Surgery, 73:133, 1973).
19. Lindesmith, G. G., Stiles, Q. R., Tucker, B. L., et al.: TheMustard Operation as a Palliative Procedure. J. Thorac.Cardiovasc. Surg., 63:75, 1972.
20. Litwin, S. B., Plauth, W. H., Jones, J. E. and Bernhard,W. F.: Appraisal of Surgical Septostomy for Transposi-tion of the Great Arteries. Circulation, 43 (Suppl. 1):7, 1971.
21. McGoon, D. C.: Surgery for Transposition of the GreatArteries. Circulation, XLV:June 1972.
22. McGoon, D. C., Wallace, R. B. and Danielson, G. K.: TheRastelli Operation. Its Indications and Results. J. Thorac.Cardiovasc. Surg., 65:65, 1973.
23. Merendino, K. A., Jesseph, J. E., Herron, P. W., et al.:Interatrial Venous Transposition. Surgery, 42: 898, 1957.
24. Mori, A., Muraoka, R., Yokota, Y., Okamoto, Y., et al.:I3eep-phtmia combined with cardiopulmonary bypas forcardiac surgery in enonates and infants. J. Thorac. Cardio-vasc. Surg. 63:422, 1972.
25. Mustard, W. T.: Recent Experiences with Surgical Managementof the Great Arteries. J. Thorac. Cardiovasc. Surg., 9:532,1968.
26. Mustard, W. T., Keith, J. D., Trusler, G. A., et al.: The
Surgical Management of Transposition of the Great Arteries.J. Thorac. Cardiovasc. Surg., 48:953, 1964.
27. Neches, W. H., Mullins, C. E. and McNamara, D. G.: TheInfant with Transposition of the Great Arteries. TI-Resultsof Balloon Atrial Septostomy. Am. Heart J., 84:603, 1972.
28. Rashkind, W. J.: Palliative Procedures for Transposition of theGreat Arteries. Br. Heart J., 33 (Suppl. 1):69, 1971.
29. Senning, A.: Surgical Correction for Transposition of the GreatVessels. Surgery, 45:966, 1959.
30. Shaher, R. M. as quoted by Mustard, W. T.: Transposition ofthe great arteries. In Siurgery of the Chest, Gibbon, J.,Sabison, D., Spencer, F. (eds.) 2nd edition, Philadelphia,W. B. Saunders.
31. Stark, J.: Primary definitive intracardiac operations in infants:Transposition of the great arteries. In Advances in Cardio-vascular Surgery Kirklin, J. W. (ed.), New York, Grune &Stratton, 1973.
32. Subramanian, S.: Hypothermic circulatory Arrest. In PediatricSurgerv; Ravitch, M. M., Welch, K. J., Benson, C. D.,Aberdeen, E., Randolph, J.; Yearbook Medical Publishers,Chicago, Illinois,-in press.
33. Subramanian, S.: The Sick Infant-Advances in MedicalManagement-Deep Hypothermia. Johns Hopkins Med. J.,in press.
34. Subramanian, S.: Early Correction of Congenital CardiacDefects Using.Profound Hypothermia and Circulatory Arrest.Ann. R. Coll.- gfrg. Engl., 54:176, 1974.
35. Subramanian, S&Z Techniques in Operative and PostoperativeManagemertii of Infants Undergoing Open Heart Surgery.Postgraduate Course, Cardiovascular Surgery, AmericanCollege of Surgeons-Miami, Fla., 1974. ASC ClinitapesSeries #C74-PG4 #1.
36. Subramanian, S. and Wagner, H.: Correction ofTransposition ofthe Great Arteries in Infants Under Surface Induced DeepHypothermia. Ann. Thorac. Surg., 16:391, 1973.
37. Subramanian, S., Wagner, H., Vlad, P. and Lambert, E.: Sur-face Induced Deep Hypothermia in Cardiac Surgery. J.Pediatric Surg., 6:612, 1971.
38. Venugopal,;P., Olszowka, J., Wagner, H., et al.: Early Correc-tion of Congenital Heart Disease with Surface Induced DeepHypotherm-ia and Circulatory Arrest. J. Thorac. Cardiovasc.Surg., 66:375, 1973.
39. Vidne, B. A. and Subramanian, S.: Surface Induced ProfoundHypothermia in Infant Cardiac Surgery: A New System. Ann.Thorac. Surg., 22:572, 1976.
40. Viles, P. H., Ongley, P. A. and Titus. C. O.: The Spectrumof Pulmonary Vascular Disease in Transposition of the GreatArteries. Circulation, 42: (Suppl. 1):116, 1970.
41. Vlad, P. and Lambert, E. C.: Experiences with Balloonseptostomy for transposition ofthe great arteries. In Advancesin Cardiovascular Surgery. Kirklin, J. W. (ed.) New York,Grune & Stratton.
42. Wagner, H. R., Teske, D. W.: Transposition of the greatarteries: Problems of ventricular function before and afterMustard procedure. In The Child with Congenital HeartDisease after Surgery, Kidd, B. S., Rowe, R. D.; Futura,Mount Kisco, New York- 1976.
43. Waldhausen, J. A., Pierce, W. S., Park, D., et al.: PhysiologicCorrection ofTransposition ofthe Great Arteries. Circulation,XLIII:738, 1971.

![Developing Country of Pakistan Great Arteries in a ... · congenitally corrected transposition of the great arteries (CCTGA) [1]. CCTGA is a defect whereby the right atrium is connected](https://img.pdfslide.net/doc/110x75/5cace22d88c99376788cec5d/developing-country-of-pakistan-great-arteries-in-a-congenitally-corrected.jpg)

















![Diagnosis of Transposition of the Great Arteries in the Fetus · Transposition of the great arteries (TGA) was first described by Mathew Baillie in 1797 [1]. The term transposition](https://img.pdfslide.net/doc/110x75/5cace22d88c99376788cec55/diagnosis-of-transposition-of-the-great-arteries-in-the-fetus-transposition.jpg)








