Embed Size (px)
Citation preview

Surgery Supply Chain - Meeting
Customer Demands While
Managing Costs
William BaileyVice President
September 14, 2015

Magnitude of the Perioperative
Supply Chain Program
1
The surgery program generally represents more than 40% of total hospital supply expenditures One of few departments where supply expenses
usually surpass labour expenses
Inventory value highest of all departments
Standardization is the most difficult – specific product use related to individual surgeon practice
Complicated logistics/distribution systems Expensive inventory, “small job shop” requisitioning
Case carts, specialty carts, backup carts
Special requests, patient-specific items
Copyright © 2015 SHC
Agenda
2
• Roles and Responsibilities
• Product Cost Management and Standardization
• Vendor Relations
• Inventory Management
• Preference / Procedure Cards
• OR Supply Cost - Data Capture
Copyright © 2015 SHC
Roles and Responsibilities
3
The perioperative supply chain requires dedicated, focused management
Copyright © 2015 SHC

Fundamental Roles in the
Perioperative Supply Chain
4
Perioperative Supply Chain Coordinator
OR Inventory Technician(s)
OR Service Line Managers/Coordinators
Copyright © 2015 SHC

Perioperative Supply
Chain Coordinator
– a Critical Program Element
5Copyright © 2015 SHC

The Role of the Perioperative Supply
Chain Coordinator
6
Supply evaluation, selection, procurement
Cost analyses (initiate and support)
Inventory management/minimization
Budget management/support
OR distribution systems
Vendor contact/coordinator
Copyright © 2015 SHC
Roles Supporting the Perioperative
Supply Chain Coordinator
7
OR Inventory Technician(s) Inventory management / restocking
Order placement, tracking
Suite restocking
OR Data Analyst / IT Support Database management
Item file maintenance
Preference card maintenance, utilization reporting
Cost reporting
Copyright © 2015 SHC

The Role of the OR Service Line
Manager / Coordinator
8
Outline of responsibility (supply chain) Trials/evaluations
Back table utilization
Case carts/care plans
Storage design/specialty carts
Scheduling/special requests
Link between clinical and financial program aspects
Primary surgeon interface
Requires dedicated administrative time,
10 to 20% devoted to supply chain!
Copyright © 2015 SHC

Next Level Roles
9
Consignment / implantcoordinator Manage consignment inventory Coordinate invoicing, reimbursement, etc. Coordinate scheduling and receiving of
special requests and loaners
OR Instrument Coordinator / Specialist Organizing backup instrument inventory Super user - instrument tracking system Repair and replacement of
instrumentation Addressing issues related to excessive loss
and repair cost of instruments Managing the loaner instrument process
Copyright © 2015 SHC
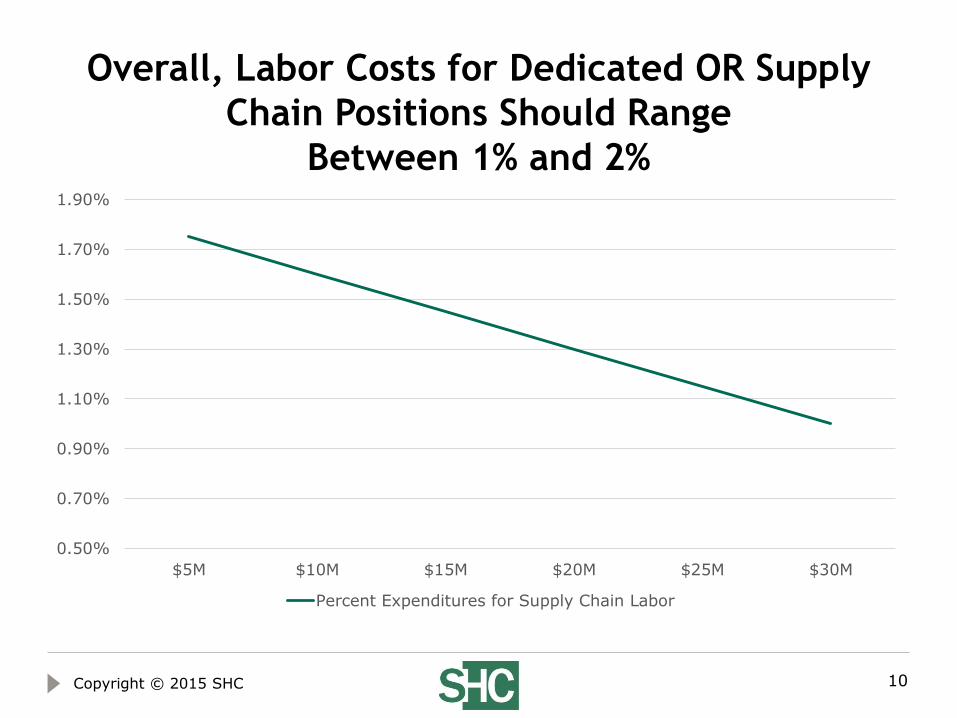
Overall, Labor Costs for Dedicated OR Supply
Chain Positions Should Range
Between 1% and 2%
10
0.50%
0.70%
0.90%
1.10%
1.30%
1.50%
1.70%
1.90%
$5M $10M $15M $20M $25M $30M
Percent Expenditures for Supply Chain Labor
Copyright © 2015 SHC

OR Supply Cost – Data Capture

The single most challenging
aspect of getting cost per case
and item utilization data is the
inability to easily capture all
supplies used on a case!
12
Inaccurate preference / procedure cards
Difficulty in intraoperative documentation
Inability to find the right item!
No scanning capabilities!
Copyright © 2015 SHC

Systems Overlay Technology Is
Available
13
Functionality: Interfaces MM System and OR System
Utilizes RFID and/or bar coding
Transmits supply usage to patient documentation system and inventory system
Consignment management, web-based
Where to acquire? Large suppliers / prime distributors
Inventory management solutions vendors
Home grown systems!
Copyright © 2015 SHC

Intraoperative Supply
Charting Simplified
14
Item is Received and Scanned Into
Inventory – Utilizing Manufacturer’s
Barcode
Bill of Materials Created per Patient Episode
Inventory is Debited, Reorder Points Trigger
Requisitions
P.O.s are Generated, Orders are Placed
Orders are Received and Checked In
Bill of Materials - Charges
Detailed Cost per Case Data
Detailed Preference Card / Supply Utilization
Data
Added Items are Scanned / Assigned to
the Patient Episode
Items are Assigned to Preference Cards
Copyright © 2015 SHC

Practice Variation Identification
15
OR supply cost per case Compare among
providers
Product alternatives / cost variations
Practice differences
Incorporate case time into analysis
Utilization Preference card items
Back table waste
Copyright © 2015 SHC

Preference /
Procedure Card Management
16Copyright © 2015 SHC

Procedure Card Management –
Guiding Principles
17
Procedure file revision is first step 450 – 850 unique procedure descriptions
Procedure card management/changes restricted to clinical leaders
Contents/changes reviewed and approved by surgeons
Content utilization > 85%, returns < 15%
Copyright © 2015 SHC

Example – Procedure Card Utilization
Analysis
18
Item
Procedure
Card Quantity Average Used
Utilization
Percentage
GARMENT COMPRES MED CALF 18IN ANTIEMBOLISM VASOPRE 1 1 100%
GLOVE BIOGEL INDICATOR 7.5 PF BEADED CUFF 1 1 100%
GLOVE SURG 7.5 LATEX BIOGEL OPTIFIT SUPER SENSITI 1 1 100%
CIRCUIT BREATHING ANESTHESIA HIGH POINT ADULT 1 1 100%
SOLUTION SURGICAL SCRUB BETADINE 4OZ 1 1 100%
CATH ROBINSON 14F 94140 1 1 100%
PAD MATERNITY CURITY 1 1 100%
SPONGE SURG 4X4IN 16 PLY BANDED RADIOPAQUE VISTEC 1 1 100%
DRESSING TELFA LATEX FREEA 8X3IN ABSORB NONADHEREN 1 1 100%
PAD ADULT ELECTROSURG GROUNDING STD REM POLYHESIV 1 1 100%
DRAPE SURG 44X40IN UNDER BUTTOCK FLUID COLL POUCH 1 1 100%
ELECTRODE 22FR WHITE CUTTING LOOP BALL TIP ELECTRO 1 0 0%
LOOP ANGLED CUTTING 22FR 8MM SURG 1 0 0%
CANISTER SUCTION PPV 2000ML 1 1 100%
PAD SURG PREP 41X24IN CUFFED NONSTERILE LATEX FREE 1 1 100%
TUBING SUCTION 20FT 3/16IN MEDI-VAC CLEAR NONCONDU 2 2 100%
LEGGINGS SURG 48X31IN CUFF STERILE LATEX FREE DISP 1 1 100%
TUBING IRRIG 81IN .195IN SET TUR Y GRAVITY FLOW RO 1 1 100%
CABLE ELECTROSURG 10FT USA ELITE ACTIVE CORD SYS V 1 1 100%
ELECTRODE USA ELITE SYS 24-26FR BLK ROLLER BALL RE 1 0 0%
ELECTRODE USA ELITE SYS 24FR .012IN YELLOW CUTTING 1 0 0%
Copyright © 2015 SHC

Procedure Card Management
Example
19
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
Jun-13 Jul-13 Aug-13Sep-13 Oct-13 Nov-13Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14Jun-14 Jul-14 Aug-14Sep-14 Oct-14 Nov-14Dec-14
Return Percentage - OR to SPD
Return Percentage
Copyright © 2015 SHC

Product Cost Management
and Standardization

Success of the Perioperative Supply Chain
Program Requires Support From:
21
Administration
OR Governance
OR Management/Service Line Management
Materials Management
Copyright © 2015 SHC

Guiding Principles – Product
Standardization and Practice Change
22
Quality patient care first, best practice identification and standardization
Physician champions
Due diligence in decision making
Copyright © 2015 SHC

Product Procurement
and Standardization
23
OR-specific product evaluation team Right people at the table
Surgeons
Nursing
Purchasing
SPD
Physician chair
Decisions based on bestdemonstrated practice
Impact – efficient process, peer-driven, lower costs, reduced inventory, standardized practices, negotiating leverage
Copyright © 2015 SHC

Product Procurement
and Standardization
24
Two purposes of the OR product evaluation and standardization team: New product selection, introduction, and evaluation
Product standardization Product lines (per management, clinicians)
Contract/GPO compliance (per purchasing)
Goals: All new products used are to be reviewed and approved
using evidence-based information
All factors will be addressed Quality
Cost
Copyright © 2015 SHC

Product Procurement
and Standardization
25
Two correct avenues for non-standard product introduction: New product
Replace current product Totally new product/approach
Patient-specific, special request items Request 5 days notice
Both avenues require review/oversight Require opportunity to assess need and gather all pertinent
information Need Cost Conflict of interest
Sometimes oversight has to happen after the fact, but it should always happen
Copyright © 2015 SHC

Vendor Relations

Interests
27
The hospital’s objectives:
• Quality patient care and service
• Low cost
The surgeon’s objectives:
• Quality patient care and service
• State-of-the-art supplies/equipment
The vendor’s objective:
• $ell, $ell, $ell
Copyright © 2015 SHC

Understanding Vendors
28
The vendor’s desire is to: Sell products
Maximize profit margin
These goals are reached by: Building relationships with
clinicians
Being in the OR suite!
Avoiding hospital protocols
Avoiding duly diligent information processors (purchasing, OR managers, etc.)
Gaining product acceptance prior to pricing discussions (increasing negotiating leverage)
Copyright © 2015 SHC

Vendors Build Relationships
with Clinicians/Decision Makers
29
Ego building
Bypass protocols
Avoiding duly diligent processes/people
Gaining product acceptance prior to pricing discussions
Always in the OR suite
Consulting/research agreements (now under scrutiny)
“Training” and “educational programs”
Problem solver/savior
Vendors are trained to develop relationships to maximize negotiating leverage
Copyright © 2015 SHC

Maximizing Negotiating Leverage
30
Administrative support
Medical director/governance support
Negotiating leverageis only achieved whenthere is a crediblethreat to the vendor’sbusiness
Copyright © 2015 SHC

Vendor Management
31
Utilize vendor tracking / credentialing systems
Define vendor access and conduct expectations
Appointment/granted access only
Badges and colored scrubs
Activities limited to specific, agreed-upon purpose
“While I’m here, try this.” – NO!
Vendors to disclose relationships, conflict-of-interest issues
Put into document, signed by all vendors Expectations/policies
Consequences
Copyright © 2015 SHC

Vendor Relations
32
Consequences of non-compliance: Free product – “Thank you for the generous donation”
First warning – letter to representative’s boss
Second warning – removal of representative (temporary or permanent)
Third warning – prohibit all representatives of a company from visiting hospital
Copyright © 2015 SHC

Inventory Management

Surgical Supplies
34
At least 50% (by dollar) of the items used in the OR are not used anywhere else in the hospital
Supply-related issues account for most of the non-clinical time for OR nurses
Supply 101 is nottaught at nursingschool (nor shouldit be)
Copyright © 2015 SHC

Parameter/Level Setting
35
• Par level – 1.5 to 3 days on handStock item
• Reorder point =(annual usage/250) X order lead time
• Order quantity =(annual usage/250) X days to store
Non-stock item
• Check items at least twice the “days to store” frequency
• Forward review of surgery schedule (nursing, materials coordinator, SPD, etc.)
If manual inventory system:
Copyright © 2015 SHC

Best Practice Concepts – Surgery
Inventory Management
36
Inventory is consolidated to the extent possible Secured/controlled environment (SPD) –
perpetual/automated inventory is possible
Unsecured area (OR core) – manual inventory system required
Exceptions: Omnicell or Pyxis systems
The case cart system is the primary mechanism for getting supplies to the case
Copyright © 2015 SHC

Measuring Inventory Management
Effectiveness
37
Inventory turns =
Annual supply expenditures (all items)Average on-hand inventory value (owned items)
Inclusive of all surgery inventory in OR and SPD
Targets:
University hospital/academic medical center: 6-8
Major medical center: 8-10
Community hospital: 10-12
Ambulatory surgery center: 12-14
Copyright © 2015 SHC

Reducing Inventory
38
Standardization
Product evaluation/selection process
Best practice establishment
Consolidation/ reducing locations Effective case cart system
OR suite/service group design
Inventory management/control
Planning
Level/parameter setting
Consignment
Vendor/distribution options JIT
Prime vendor relationships
Copyright © 2015 SHC

Obsolescence Management
39
Run slow/no moving product lists at least every six months
Categorize by: Commodity type Vendor
Route to OR managementand service line managerscoordinators for review/decision
Get stuff off the shelves! Credit Sell Donate
Copyright © 2015 SHC

Objective of Supply Chain
Cost Management
Identification and standardization to best practice should be the primary goal – shared by all
If you first pursue quality, costs will fall out!
40Copyright © 2015 SHC

Surgery Supply Chain -
Meeting Customer Demands
While
Managing Costs
Discussion











![Re-defining the value chain - KPMG · traditional supply chain models cannot deliver on today's business demands *Survey fielded by [E] BrandConnect, a commercial arm of The Economist](https://img.pdfslide.net/doc/110x75/5f5c16bfbd7bf92e1e53d22b/re-defining-the-value-chain-kpmg-traditional-supply-chain-models-cannot-deliver.jpg)
















