Embed Size (px)
Citation preview

Surgical AirwaySurgical AirwaySybile Val, MD
SUNY Downstate Medical CenterCenter
August 6, 2009
www.downstatesurgery.org

Case PresentationCase Presentation• HPI • MedsHPI
– 42 YOF presented to ED on 4/18 with
Meds– Singulair– Advair
dyspnea• PMH
A th
– Albuteral– Sensipar
– Asthma– ESRD on HD
• PSH
• Allergies– NKDA
• PSH– RUE fistula
creation
www.downstatesurgery.org

Case PresentationCase Presentation
• In EDIn ED– Afebrile, BP 97/66 HR 109 RR 22 Sat
96%96%– On Exam
• Mild respiratory distressMild respiratory distress• No JVD• Rales in lower 1/3 of b/l lung fields, no
wheezing• No Peripheral edema
www.downstatesurgery.org

Case PresentationCase Presentationwww.downstatesurgery.org

Case PresentationCase Presentation
• LabsLabs– Unremarkable
• Plan• Plan– Admit to Medicine w/ Dx of CHF
exacerbationexacerbation– Renal for HD
O th i iti t d– Oxygen therapy initiated
www.downstatesurgery.org

Case PresentationCase Presentation
• Post DialysisPost Dialysis– No improvement in SOB
Alterations in mental status– Alterations in mental status– ABG: 7.17/94/237/36/100%
BiPAP initiated– BiPAP initiated– MICU consult called
R d tiRecommendations:Intubate the patient
www.downstatesurgery.org

Case PresentationCase Presentation• Anesthesia consultedest es a co su ted
– Using accessory muscles– Obtunded with saturation of 91-96%– Attempts at intubation with fiberoptic
scope x 2Gastric contents regurgitated– Gastric contents regurgitated
• Surgery consultedCricothryoidotomy attempted @ bedside– Cricothryoidotomy attempted @ bedside
– Pt taken to OR for revision and control of bleeding
www.downstatesurgery.org

Case PresentationH it l CHospital Course
• POD#1 • POD#39– ENT consulted
• Cricoid cartilage palpable below stoma
• POD#2
– New onset A. fib w/ RVR
– Cardioverted– Started on heparin and
– Tracheostomy revision • POD#6
– Weaned from ventilator
Started on heparin and amniodarone
• POD#45– Will watching TV,
bright red blood noted • POD#9– Trach downsized – on HD
POD#15
bright red blood noted from trach
– Desaturated to 38%– Excessive blood in
• POD#15– Cleared for discharge
• POD#26Developed Vfib while on
oropharynx– Coded, ACLS initiated– Pt pronounced @7pm
Autopsy declined– Developed Vfib while on HD
– Autopsy declined
www.downstatesurgery.org

Questions??
www.downstatesurgery.org

Surgical AirwaySurgical Airwaywww.downstatesurgery.org

Indications f I t b tifor Intubation
PHYSIOLOGIC• Persistent hypoxemia with oxygen
supplementation• PACO2 >55, Ph <7.25• Vital capacity <15ml/kg with NM d/o
www.downstatesurgery.org

Indications f I t b tifor Intubation
CLINICAL• Altered mental status
R i t di t ith HD i t bilit• Respiratory distress with HD instability• Upper airway obstruction
– Angioedema– Trauma– Infection– Bleeding– Tumor– Tracheomalacia– Tracheal Stenosis
• Copious secretion requiring frequent s ctioningsuctioning
www.downstatesurgery.org

Indications f S i l Aifor Surgical Airway
• Upper Airway pp yObstruction
• Prolonged intubation• Chronic respiratory
insuff.• Neuromuscular Neuromuscular
disorders
www.downstatesurgery.org

Surgical AirwaySurgical Airway• Historically • TypesHistorically
– Acute or impending airway
Types– Cricothyrotomy– Standard
obstruction• Now…
Ai t l i
tracheostomy– Percutaneous
dilatation – Airway control in conjunction with prolonged usage
dilatation tracheostomy
p g gof mechanical ventilation
www.downstatesurgery.org

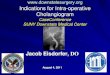
AnatomyAnatomy
CMAJ • April 22, 2008 • 178(9)
www.downstatesurgery.org

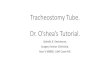
CricothyrotomyCricothyrotomywww.downstatesurgery.org

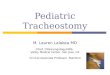
Standard TracheostomyStandard Tracheostomywww.downstatesurgery.org

Standard TracheostomyStandard Tracheostomywww.downstatesurgery.org

Standard TracheostomyStandard Tracheostomywww.downstatesurgery.org

Standard TracheostomyStandard Tracheostomywww.downstatesurgery.org

Standard TracheostomyStandard Tracheostomywww.downstatesurgery.org

ComplicationsComplicationsEarly Latey
• False passage• Decannulation
• Granulation• Tracheomalacia
• Pneumomediastinum• Pneumothorax• Bleeding
• Stenosis• Tracheoinnominate
fistula• Bleeding • Infection• Mucous Plug
fistula• Tracheoesophageal
fistulaMucous Plug• Negative Pressure
Pulm Edema
www.downstatesurgery.org

Could we have done somethingCould we have done something different in this case??
www.downstatesurgery.org

• Retrospective study atRetrospective study at Cook County
• Between August 2001 gto October 2003
• 197 subjects in study j ywith 244 day follow up– 107 standard trach
– 90 using awake technique
www.downstatesurgery.org

• Awake Technique:Awake Technique:– Semirecumbent position
– No general anesthetic
– Subcutaneous lidocaine
– Wide incision and use of i id h kcricoid hook
– Direct laryngoscopy if neededneeded
– Availability of GA and OR
www.downstatesurgery.org

This group had a more significant set of complicationsThis group had a more significant set of complications
www.downstatesurgery.org

C l i• Conclusion:Awake tracheostomy should be considered in any
patient with impending or ongoing airway
obstruction or potentially difficult intubation
www.downstatesurgery.org

When is the best time to offer a tracheostomy?tracheostomy?
www.downstatesurgery.org

ReferencesReferences
• ACS Surgeryg y• Sabiston• Altman et al.: Urgent Surgical Airway Intervention. Laryngoscope 2005; 115:2101‐2104
• Freeman et al.: Relationship between tracheostomy timing and duration of mechanicaltracheostomy timing and duration of mechanical ventilation in critically ill patient. Crit Care Med 2005;33:2513‐2520
• Bourjeily et al.: Review of Tracheostomy Usage: Types and Indications Clin Pulm Med 2002;9(5):267‐2722002;9(5):267 272
www.downstatesurgery.org