-
e2
s, CA
f a la ditiontionloorgice bus). L= 0
an 5 years are much more likely to have a pathologic lead point
and early surgical
intussusceptum and guide the aggressiveness
ith this diagnosis from. Patients aged greater
Journal of Pediatric Surgery 50 (2015) 647650
Contents lists available at ScienceDirect
Journal of Pedi
j ourna l homepage: www.e lsecomes so common that surgery is the
best rst step? A classic pediatric with a diagnosis of ileocolic
intussusception were included in the
study. The following data were extracted from electronic medical
re-surgical textbook states that hydrostatic reduction should be
attemptedpathological lead point. In adult patients, pathological
lead points arean expected nding among patients with
intussusception. The questionis: Is there an age at which the
presence of a pathological lead point be-
than 12 years were excluded, because it was felt that they
wouldshare the same characteristics as adult patientswith respect
to this diag-nosis. Hospital charts were reviewed by three
individuals. Only casesrather than a true pathological lead
point.Increasing age is associated with a higher likelihood of
nding a
tion. Electronic medical records of all patients wJanuary 2007
to December 2013 were reviewedmany studies, the success rate with
this approach is very high withthe majority of patients avoiding
the need for laparoscopy or laparoto-my to complete the reduction
[13]. In the occasional patient wherethe intussusception cannot be
reduced, resection is required. Theusual ndings are necrosis due to
prolonged vascular compression,
1. Materials and methods
Hospital records from six regional hospitals within a
singlehealthcare systemwere searched using the diagnosis code
intussuscep- Corresponding author. Tel.: +1 323 783 5500.E-mail
addresses: [email protected] (P. Banapou
(R.M. Sydorak), [email protected] (D. Shaul).1 Tel.: +1 323
783 4857.2 Tel.: +1 323 783 4857; fax: +1 323 783 8747.
http://dx.doi.org/10.1016/j.jpedsurg.2014.09.0780022-3468/ 2015
Elsevier Inc. All rights reserved.of the reduction [1,2]. In
termine how to best manage these patients.
used to determine the presence orYounger children (aged 02
years) with intussusception usually donot have a pathological lead
point. In these cases, resection of the in-volved intestinal
segment is not necessary, provided that the intussus-ception can be
completely reduced, either radiologically or surgically.The
management of intussusception in these younger children is
wellestablished and begins with either hydrostatic or air
reduction, some-times under ultrasound guidance. Ultrasound Doppler
studies are also
absence of blood ow in the
in all patients regardless of age [4]. It was standard training
in the seniorauthors institution to perform surgery on all
pediatric patients with in-tussusception older than 2 years of age.
Similarly, Van der Laan et al.found that all patients older than 2
years of agewith intussusception re-quired laparotomy with the
majority requiring a bowel resection [5].
This study was performed to determine the characteristics of
olderchildren (312 years old) with ileocolic intussusception, to
determinethe incidence of pathological lead points and most
importantly, to de-age group. 2015 Elsevier Inc. All rights
reserved.intervention should be considered. In this study, enema
reduction was safe but minimally benecial in thisdiverticula and 7
others.Conclusion: Children older thSurgical approach to
intussusception in oldlead points
Pooya Banapour , Roman M. Sydorak 1, Donald ShaulKaiser Los
Angeles Medical Center, Department of Surgery, 4760 Sunset Blvd.,
3rd , Los Angele
a b s t r a c ta r t i c l e i n f o
Article history:Received 22 July 2014Received in revised form 2
September 2014Accepted 24 September 2014
Key words:Ileocolic
intussusceptionIntussusceptionPediatricHydrostatic
Background: The likelihood oThis study looks at whetherMethods:
7 year multi-instituResults: Ileocolic intussuscep10612 years,
respectively. Bbined hydrostatic and/or sup b 0.001. Enemas were
saf(15 idiopathic, 14 lead pointand 5/10 aged 612 years (pr),
[email protected] children: Inuence of
90027
ead point as the cause of ileocolic intussusception increases as
children get older.fferent management strategy should be employed
in older patients.al retrospective study of intussusception in
patients aged b12 years.with complete data was found in 153
patients: 109 02 years, 34 35 years, anddy stools occurred in
42/143 of 05 years and 0/10 of 612 years, p b 0.001. Com-al
reduction was successful in 113/143 05 year olds vs 5/10 612 year
olds,t reduced only 1 patient over age 5. Resections were required
in 29 patientsead points were found in 4/109 children under 3
years, in 5/34 aged 35 years.04 vs 35 years and p b0.001 vs 05
years). Lead points consisted of 7Meckels
atric Surgery
v ie r .com/ locate / jpedsurgcords: demographics, date of
birth, age at diagnosis of intussusception,symptoms at presentation
(emesis, grossly bloody stool, fever), lengthof symptoms, and date
of last followup. Feverwas dened as oral or rec-tal temperature
greater than 100.6 F. Radiology reports were reviewedfor the
following information: date of contrast enema, number of con-trast
enema studies, presence of radiologic lead point, level of
-
intussusception at start of enema, level of intussusception at
end ofenema and date(s) of repeat enema(s). Operative notes were
reviewedfor the following: type of operation (laparoscopic,
laparoscopic convert-ed to open, open), presence of pathological
lead point, reduction of in-tussusception and resection. Pathology
reports were reviewed for allndings including the location and
presence of any pathology whichserved as the lead point for the
intussusception. We dened pathologi-cal lead point as the nding of
a pathologic abnormality in the resectedspecimen which served as
the lead point for the intussusception. Thending of ischemia and/or
necrosis without a co-existing lead pointwas not considered a
pathological lead point. Cases involving smallbowel-small bowel
intussusception (n = 10) and patients who had no
clinically, the emergency department physician may have ordered
anabdominal CT scan. In other cases, where the diagnosis of
intussuscep-tion was suspected, an ultrasound or a contrast enema
was obtainedas the initial study. When intussusception was
diagnosed by CT scan,the attending surgeon made a decision on
whether to proceed with anattempt at hydrostatic reduction or
proceed with surgical intervention.If this study suggested a small
bowel to small bowel intussusception thepatient may have been taken
to surgery without an attempt at enemareduction. In some cases,
primarily early in the study period, the lackof an experienced
radiologist may have prompted the surgeon to pro-ceed directly to
the operating room, rather than attempt a hydrostaticreduction.
This was more likely to be true in older patients. Of the 153
esis
mbe
0
648 P. Banapour et al. / Journal of Pediatric Surgery 50 (2015)
647650follow up and/or had insufcient hospital records were
excluded(n = 12). Patients were grouped into the following age
categories: 0,1, 2, 3, 4, 5, 612 years old before statistical
analyses were performed.
The general radiological approach was to use the hydrostatic
enemawith the bag 3 feet above the level of the rectum,
infusingwater solublecontrast up to 3min at a time or until no
further reductionwas evident.Inmost cases the colonwas drained and
the infusionwas repeated up tothree additional times until no
further progress was made.
Analyses of length of symptoms, presence of emesis, bloody
stools,fever at diagnosis, hydrostatic enema reduction attempts,
hydrostaticenema reductions, surgical reductions, surgical
resections and presenceof pathological lead points were performed
based on age groups. UsingGraphPadQuickCalcs Software (2014,
GraphPad Software, Inc, La Jolla,CA), the statistical signicance of
differences between age groups 05and 612 years was calculated.
Fishers exact test was used for categor-ical data and students t
test was used for continuous data. A 5% level ofsignicance was used
for all cases. The study was approved by our re-gional
institutional review board, approval number 10251.
2. Results
A total of 153 cases of ileocolic intussusception were
identiedamong the ages of 012 years from January, 2007 to December,
2013.Of these patients, 55 were age b12 months, 37 were age 1 year,
17were age 2 years, 34 were age 35 years and 10 were age 612
years(Table 1). Examination of the data revealed a natural break
betweenages 5 and 6 years, rather than an anticipated break between
ages 2and 3 years. For this reason, comparisons were made between
groupsaged 05 years and 612 years, respectively. Average length of
symp-toms for the different age groups was 1.9, 2.1, 2.4, 2.2 and
3.3 days, re-spectively. There was a signicant difference in length
of symptomsbetween children of age 612 (3.3 days) and 05 (2.1 days,
p b 0.001).In children aged 05 years, 56% presented with emesis
whereas only40% presented with emesis in children aged 612 years (p
b 0.001).Similarly, 29% of children aged 05 years presented with
bloody stoolswhereas none of the children aged 612 years presented
with bloodystools (p b 0.001). Only 9% of patients aged 05
presented with feverwhereas 30% of patients aged 612 years had a
fever upondiagnosis (p b 0.001).
Inmany cases, the patients initial presentationwas to the
emergen-cy department. If the diagnosis of intussusception was not
suspected
Table 1Patient characteristics.
Em
Age (years) N Average days of Symptoms (mean SD) Nu
0 55 1.9 1.1 451 37 2.1 1.5 242 17 2.4 1.5 1135 34 2.2 1.5
20Total 05 143 2.1 0.2 80612 10 3.3 2.2 4Total 153 2.1 1.2 18
p b 0.001 for 612 vs 05.patientswith intussusception, contrast
enema reductionwas attempted168 times in 130 patients and
successfully reduced the intussusceptionin 67 patients (Table
2).There were 6 patients in whom a CT scanshowed ileocolic
intussusception but the intussusception was sponta-neously reduced
by the time the patient underwent a contrast enemaor surgical
exploration. These cases were counted as spontaneous re-ductions.
There were also 10 patients in whom the CT scan showedsmall bowel
to small bowel intussusception (6 reduced spontaneously,3 underwent
open or laparoscopic reduction, and one patient withPeutzJeghers
syndrome underwent resection of a polyp that hadserved as the lead
point). These patients were excluded from the overallanalysis. The
number of delayed repeated enemas ranged from 0 to 2times per
patient. A total of 80 patients underwent laparoscopic oropen
surgical intervention. Of the surgical cases, 51were reduced
intra-operatively whereas 29 intestinal resections were performed.
Changesconsistent with ischemia and necrosis were seen in 15
patients, noneof which had a pathological lead point, and all of
whom were lessthan three years of age. 14 patients had a
pathological lead point. Specif-ically among the patients aged 6
and above, 10 patients were diagnosedwith ileocolic
intussusception. Hydrostatic reduction was attempted infour
patients and was successful in one. The other 3 went to the
operat-ing room, one was reduced and the other two underwent
resection of apathological lead point. It was the surgeons choice
to take the other 6patients directly to the operating room, without
attempting hydrostaticreduction. Of these 6 patients whowent to the
operating room, one hadreduced spontaneously, two were reduced
surgically without discover-ing a pathological lead point and the
remaining 3 had lead points re-moved. Pathological lead points were
found in 9/143 (6%) ofchildren aged 5 and younger and in 5/10 (50%)
of children aged612 years (p b 0.001).
The pathologic ndings in the patientswith lead points are shown
inTable 3. Of the patients aged 612 years, the lead points included
2 pa-tients with Meckels diverticulum, 1 patient with a metastasis
from aEwings sarcomaprimary, 1 patientwith appendicealmass and
cystic -brosis and 1 patient with a hyperplastic mesenteric lymph
node, whichserved as the lead point. In patients aged 35 years, 11
patients weretaken to the operating room. Lead points were present
in 5 patientsand 5 patients were reduced intraoperatively. The
remaining intussus-ception reduced spontaneously. Of the 8 patients
aged 2 years whowere taken to the operating room, one had a
pathologic lead point. All3 of the resected specimens had
pathologic ndings consistent with
Bloody stools Fever
r Percent Number Percent Number Percent
82 29 53 6 1165 12 32 6 1665 1 6 1 659 6 18 7 2156 42 29 13 940
0 0 3 30
90 33
-
was not helpful, or even harmful. This question has not been
specicallyaddressed in other reports in the literature. This is a
hard question to an-swer given the relatively low prevalence of
intussusception within this
Table 2Therapeutic intervention.
Hydrostatic Enema Operations
Age (years) N Number of patients (%) Number reduced (%) Number
of patients (%) Number reduced (%) Resected (%) Lead Point (% of
N)
0 55 45 (82) 17 (38) 39 (71) 25 (64) 14 (36) 1 (1.8)1 37 34 (92)
20 (59) 13 (35) 11 (85) 2 (15) 2 (5.4)2 17 15 (88) 10 (67) 8 (47) 5
(63) 3 (38) 1 (5.9)35 34 32 (94) 19 (59) 11 (32) 6 (55) 5 (45) 5
(14.7)Total 05 143 126 (88) 66 (52) 71 (50) 47 (69) 24 (34) 9
(6.3)612 10 4 (40) 1 (25) 9 (90) 4 (44) 5 (56) 5 (50)Total 153 130
(85) 67 (52) 80 (52) 51 (51) 29 (36) 14 (18)
p b 0.001 for 612 vs 05.
649P. Banapour et al. / Journal of Pediatric Surgery 50 (2015)
647650ischemia and necrosis while the remaining 5 intussusceptions
were re-duced intraoperatively. There were 2 lead points seen in
the 14 patientsaged 1 yearwhowere taken to the operating room and
12 patients whohad their intussusception reduced intraoperatively.
Although therewere a total of 39 patients aged 012monthswhowere
taken to the op-erating room, only 1 patient had a pathologic lead
point (Meckels diver-ticulum). In total the pathologist identied 4
patients with follicularhyperplasia or lymphoid hyperplasia large
enough to serve as the leadpoint for the intussusception. There may
not be substantial differencesbetween this diagnosis and an
enlarged Peyers patch, which is felt torepresent a potential lead
point in younger children with intussuscep-tion. However, the focus
population in this study is the 612 year oldage group, and lymphoid
hyperplasia was only diagnosed in one ofthese patients.
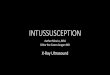
The prevalence of pathological lead points in various age groups
isshown in Fig. 1. The overall prevalence of lead points in the
differentage groups 0, 1, 2, 35 and 612 was 1.8%, 5.4%, 5.9%, 14.7%
and 50%, re-spectively. To determine if any clinical parameters
(other than age)could predict the presence of a pathological lead
point, additional anal-yses were performed. For example, emesis was
present in 50% of pa-tients with a pathological lead point and in
70% of patients without apathological lead point. Similarly, bloody
stools were present in only21% of patients with a pathological lead
point and in 33% of patientswithout a pathological lead point, all
non-signicant. Total follow-upfor this study ranged from 1 to 199
months with a mean of 78 months.months. Patient charts were
reviewed to determine the length of followup while looking for
recurrent intussusception. If present, this wouldhave suggested
that intussusception caused by a pathological leadpoint may have
been reduced. In this specic patient population(reduced
intussusception), follow-up ranged from 1 to 130 months,mean 74
months. Within this time frame, 9 patients were encounteredwho came
back with a recurrent intussusception, however, none werefound to
have a surgically proven pathological lead point.
3. Discussion
The objective of this study was to determine if there is an age
atwhich attempted hydrostatic reduction of an ileocolic
intussusceptionTable 3Pathologic ndings in patients with lead
points.
Age (years) Patients w/leadpoints
Meckelsdiverticulum
LymphoidHyperplasia+
Other
0 1 1 0 01 2 1 1 02 1 0 1 035 5 3 1 1612 5 2 1 2Total 14 7 4
3
+ includes patients with follicular hyperplasia. Pathologic
ndings included raised vascular lesion (35 age group), 2 cm
small
bowel metastasis from primary Ewings sarcoma and inspissated
appendiceal mass(612 age group).older age group. This study
utilizes a patient database with access toover 4 million patients
within a single healthcare system spread outover a seven year
interval. Some of the providers were adult radiologistsand adult
general surgeons, especially for the older patients. Other
pro-viders were pediatric radiologists and pediatric surgeons. As
such, thesuccess rate for hydrostatic reduction was lower than is
generally quot-ed in the pediatric radiology literature. This fact
no doubt inuenced asurgeons decision to either attempt a
hydrostatic reduction or proceeddirectly to surgery. It is
retrospective and there was no specic protocolutilized by the
various facilities. In view of these important limitations,no rm
conclusions can be reached about whether contrast enemasshould be
obtained in older patients. Hydrostatic reduction was onlyattempted
in four patients aged 612 years. One of these was success-fully
reduced. Five of the ten patients in this age group were unable
tohave their intussusceptions surgically reduced and underwent
surgicalresection of a pathological lead point. If hydrostatic
reduction hadbeen attempted in all 10 patients, it is unlikely that
these 5 patientswould have been reduced, giving at most a 50%
success rate. Therefore,only a 50% success rate should be expected,
due to the higher incidenceof pathological lead points in this age
group. This study does suggestthat attempted hydrostatic reduction
appears safe in older patients, asno perforations were observed. It
also showed that a pathological leadpoint is unlikely to be reduced
using standard surgical or radiologicaltechniques. Based upon these
data it is recommended that a therapeuticenema reduction be
attempted in all patients with suspected or provenintussusception
aged 5 years and below, who do not have a contraindi-cation to the
enema. This study can not say that hydrostatic reductionshould not
be performed in older patients, only that it is less likely tobe
successful in this older age group. The decision to attempt a
contrastenemamust bemade by the surgeon based upon the patients
presenta-tion and the skill level of their radiology
department.
6010
0
20
30
40
50
0 yr 1 yr 2 yrs 3 yrs 4 yrs 5 yrs 6-12 yrs
number of patients without lead point
number of patients with lead point
Fig. 1. Pathologic lead points by age group.
-
What this study does clearly show is that pathological lead
points aremore likely at increasing ages, with a cutoff noted at
age 6 years andabove. It was also unable to identify any clinical
parameters (otherthan age) that indicated the high likelihood that
a pathologic leadpoint is present. The exact reason why older
patients (612 years) hadless emesis and bloody stools than their
younger counterparts is notclear. They did tend to present later
than the younger patients. Perhapsthis is because many parents are
more anxious about younger childrenand infantswho are not able to
talk and bring them to the doctor sooner.The higher incidence of
fever in the older children may be due to thehigher likelihood of
compromised intestine and/or a later presentation.
The overall incidence of pathological lead points in children
with in-tussusception has been reported to be 1.5%12% [6]. In this
study, path-ological lead points were found to be more prevalent in
older patients.Pathological lead points occurred in 50% of patients
aged 612 years,but in only 4% of 02 year olds and in 15% of 35 year
olds. Other studiesof intussusception had similar results. In a
study of 1340 children aged3 months to 12 years with recurrent
intussusceptions, 3 of 7 patientswith pathological lead points were
aged greater than 6 years and 1 pa-tient was 4 years old [7].
Saxena and colleagues found 2 pathologicallead points in a study of
over 100 children with intussusception agedup to 16 years; both
lead points were in children greater than 6 yearsold [8]. Many
other studies have shown an increased frequency of path-ological
lead points in children greater than 6 years old [911]. A
radio-logic study of patients aged 014 years with intussusception
found anequal distribution of radiological lead points among age
groups [12].However, these were lead points seen on imaging, not
proven at sur-gery. In this study, every child with a pathological
lead point eventuallyunderwent resection of the pathological lead
point due to failed reduc-
Early in the study period, patients with a possible diagnosis of
intus-susception were evaluated in a variety of ways, and sometimes
withoutthe involvement of a pediatric surgeonuntil after the
diagnosiswasmade.In many cases, CT scans were done, in spite of the
potential radiation ex-posure. Beginning in 2012 a regional
protocolwas established to expeditethe evaluation and treatment of
childrenwith suspected intussusception.It begins with a plain
abdominal X-ray and an abdominal ultrasound, asthis has been shown
to be highly sensitive in diagnosing intussusception[12]. It
discourages the use of CT scans. Once imaging suggesting that
anintussusception is found the patients are transferred to
facilities withon-site pediatric surgeons and radiologists for
denitive management.
References
[1] Digant SM, Rucha S, Eke D. Ultrasound guided reduction of an
ileocolic intussuscep-tion by a hydrostatic method by using normal
saline enema in pediatric patients: astudy of 30 cases. J Clin
Diagn Res 2012;10:17225.
[2] Gonzlez-Spinola J, Pozo GD, Tejedor D, et al.
Intussusception: the accuracy ofultrasound-guided saline enema and
the usefulness of a delayed attempt at reduc-tion. J Pediatr Surg
1999;34:101620.
[3] Lee JH, Choi SH, Jeong YK, et al. Intermittent sonographic
guidance in air enemas forreduction of childhood intussusception. J
Ultrasound Med 2006;25:112530.
[4] Welch KJ, Randolph JG, Ravitch MM. Intussusception. In:
Welch KJ, Randolph JG,Ravitch MM, editors. Pediatric surgery. New
York, NY: Medical Publishers Inc.;1986. p. 86882.
[5] Van der Laan M, Bax NM, Van der Zee DC, et al. The role of
laparoscopy in the man-agement of childhood intussusception. Surg
Endosc 2001;4:3736.
[6] Blakelock RT, Beasley SW. The clinical implications of
non-idiopathic intussuscep-tion. Pediatr Surg Int 1998;14:1637.
[7] Niramis R, Watanatittan S, Kruatrachue A, et al. Management
of recurrent intussus-ception: nonoperative or operative reduction?
J Pediatr Surg 2010;11:217580.
[8] Saxena AK, Hollwarth ME. Factors inuencing management and
comparison of out-comes in pediatric intussusceptions. Acta
Paediatr 2007;96:1199202.
[9] Daneman A, Alton DJ, Lobo E, et al. Patterns of recurrence
of intussusception in chil-dren: a 17-year review. Pediatr Radiol
1998;28:9139.
650 P. Banapour et al. / Journal of Pediatric Surgery 50 (2015)
647650have their intussusception reduced. However, in this study,
no patientwhose intussusception was initially reduced was
subsequently foundto have a pathological lead point. One of the
strengths of this study isthe long-term follow-up of patients who
remain within our system. Itis unlikely that a lead point was
missed given this length of follow up.[10] Eklof DA, Johanson L,
Lohr G. Childhood intussusception: hydrostatic reducibilityand
incidence of leading points in different age groups. Pediatr Radiol
1980;10:836.
[11] Schuh S, Wesson DE. Intussusception in children 2 years of
age or older. Can MedAssoc J 1987;136:26972.
[12] Navarro O, Dugougeat F, Kornecki A, et al. The impact of
imaging in themanagementof intussusception owing to pathologic lead
points in children: a review of 43 cases.Pediatr Radiol
2000;30:594603.tion. It is possible for a patient with a minor
pathological lead point to
Surgical approach to intussusception in older children:
Influence of lead points1. Materials and methods2. Results3.
DiscussionReferences