Embed Size (px)
Citation preview

SURGICAL GRAND ROUNDSDavid H. Harpole, Jr., M.D.New Options for Achieving
Individualized Approaches to Non-small Cell Lung Cancer Management
SPONSORED BY THE VANDERBILT SCHOOL OF MEDICINEDEPARTMENT OF SURGERYDEPARTMENT OF THORACIC SURGERY
Dr. Harpole has financial relationships with the following companies:
GlaxoSmithKline – ConsultantGlaxoSmithKline – spouse, Shareholder
**To be determined following presentation review: ** Vanderbilt CME has determined there is no conflict of interest.

New Options for Achieving Individualized Approaches to Non-Small Cell Lung Cancer
(NSCLC) Management
David H. Harpole Jr, MDProfessor of Surgery
Division of Thoracic SurgeryDepartment of Surgery
Associate Professor of PathologyDepartment of Pathology
Duke Institute for Genome Science and PolicyDuke University Medical Center
Durham, North Carolina

• List barriers that hinder optimal care for NSCLC patients and establish methods to achieve improved outcomes
• Define strategies to better include patients and their families in a shared decision making process for the management of their NSCLC
• Assess the latest data from newer oncologic therapies to determine future strategies for improving the significant failure rate seen among current approaches for NSCLC management
• Determine individualized NSCLC patient scenarios where novel targeted therapies may apply and assess how these options may integrate into existing regimens, taking into account potential safety issues
• Examine the potential role of biomarkers in the individualized management of NSCLC patient and identify new knowledge and skill sets required for their incorporation into clinical practice
Educational Activity Learning Objectives

> 85% of Lung Cancer is Caused by Cigarette Smoking
• Decrease in risk seen 5 years after stopping, never reaches baseline • Cessation after diagnosis improves treatment tolerance and outcome
Videtic GM, et al. J Clin Oncol. 2003;21(8):1544-1549.Fox JL, et al. Lung Cancer. 2004;44(3):287-293.

Non-small Cell Lung Cancer (NSCLC)
• NSCLC accounts for ~135,000 cases of lung cancer annually
• Approximately 30–40% of these patients will have metastatic disease
• Untreated patients have a median survival of ~4–5 months

Jemal A, et al. CA Cancer J Clin. 2009;59(4):225-249.
Estimated New Cancer Cases United States, 2009
Males Females

Estimated Cancer Deaths United States, 2009
Jemal A, et al. CA Cancer J Clin. 2009;59(4):225-249.
Males Females

Survival by Clinical and Pathologic StageProposed IASLC Stage Groupings
Detterbeck FC, et al. Chest. 2009;136:260-271.Goldstraw P, et al. J Thorac Oncol. 2007;2:706-714.
Clinical Pathological

Lung Cancer: Symptoms
• Related to Primary Lesion
• Related to Spread within Chest
• Related to Distant Metastasis
• Cough, often dry• Shortness of breath• Hemoptysis• Wheezing
• Shortness of breath• Hoarseness• Superior vena cava syndrome• Horner’s syndrome
• Brain• Bone• Liver• Adrenal glands

Lung Cancer Assessment
• History and Physical Exam: – Assess weight loss and – Performance status
• Labs: CBC, comprehensive metabolic panel• Smoking cessation counseling • CXR• CT Chest with IV contrast (includes liver and adrenal
glands)• Biopsy:
– Bronchoscopy– CT guided– Mediastinoscopy– Endoscopic Ultrasonography (EUS-FNA, EBUS-FNA)– Thoracentesis
• +/- FDG-PET scan or PET/CT• +/- MRI Brain/Spine (Suggestive Symptoms)

Overview of NSCLC Treatment
Stage I Surgery (Poor risk: RFA, SBRT)
Surgery or RadiationWith Chemotherapy
ChemotherapyTargeted Therapy
Stage IVor
Recurrent Disease
Stage II Adjuvant Chemotherapy
Stage III

Therapy in Stage IV DiseaseGoals
• Palliative– Improve symptoms– Improve quality of life– Control disease
• Improve progression free survival• Improve overall survival

Non-Small Cell Lung Cancer:Stage IV Disease
GENERAL PRINCIPLES:• Baseline factors predict survival
– Age– Weight loss– Gender– Performance status
• Age does not predict worse outcome– Elderly patients with a good performance status should be offered
systemic treatment– Older patients are more susceptible to toxic side effects of
chemotherapy

Common Chemotherapy for Stage IV NSCLC
• Platinum– Cisplatin– Carboplatin
• Taxanes– Paclitaxel– Docetaxel
• Gemcitabine• Vinca Alkaloids
– Vinorelbine– Vinblastine
• Pemetrexed• Mitomycin

Non-Small Cell Lung Cancer:Chemotherapy Side Effects
• Neutropenia • Neutropenic fevers• Anemia • Thrombocytopenia• Hair loss • Fatigue• Nausea & vomiting • Diarrhea/constipation• Mouth sores • Allergic reaction• Loss of appetite • Rash• Neuropathy • Muscle aches• Hearing loss • Edema• Renal failure • Eye tearing• Death

Survival After 1, 2, or 3 Cytotoxic Chemotherapies
Delbaldo C, et al. JAMA. 2004;292:470-484.
2 drugs are better than 1

Survival After 1, 2, or 3 Cytotoxic Chemotherapies
3 cytotoxic drugs are not better than 2
Delbaldo C, et al. JAMA. 2004;292:470-484.

What Treatment? Chemotherapy Individualization
Schiller et al., New Engl J Med 346: 92, 2002
Balance agent toxicity with tumor sensitivity

Recent Advances: Cis /Gem vs Cis /Pem
Cisplatin 75 mg/m2 day 1 +Pemetrexed 500 mg/m2 day 1
(n = 862)
RandomizationFactors • Stage • Performance status • Gender • Histologic vs cytologic
diagnosis• History of brain
metastases
Cisplatin 75 mg/m2 day 1 +Gemcitabine 1250 mg/m2 days 1,8
(n = 863)
Vitamin B12 , folate, and dexamethasone given in both arms
Each cycle repeated q 3 wk up to 6 cycles
Scagliotti GV, et al. J Clin Oncol. 2008;26:3543-3551.
RANDOMI
ZATION
Primary EndpointOverall Survival

Recent Advances: Cis /Gem vs Cis /Pem: Survival
Scagliotti GV, et al. J Clin Oncol. 2008;26:3543-3551.
1.00.90.80.70.60.50.40.30.20.10.0
0 6 12 18 24 30
Surv
ival
Pro
babi
lity
Survival Time, mo
Median (95% CI)Cisplatin/pemetrexed 10.3 (9.8-11.2)Cisplatin/gemcitabine 10.3 (9.6-10.9)CP vs CG Adjusted HR (95% CI)
0.94 (0.84-1.05)

Recent Advances: Pemetrexed/Cisplatin
vs Gemcitabine/Cisplatin: Results
HR = 1.3P = 0.0510.849.36
Median OS, mos(squamous cell carcinoma)
HR = 0.81 (0.70-0.94)P = 0.0310.4 11.8
Median OS, mos(adeno or large cell carcinoma)
HR = 1.04 (0.94-1.15)5.1 4.8 Median PFS, mos
HR = 0.94 (0.84-1.05)10.3 10.3 Median OS, mos
HR = 0.90 (0.79-1.02)4.7 5.3 Median PFS, mos(adeno or large cell carcinoma)
P = 0.1985.09 4.50 DOR, mos28.2%
Gem/Cisplatin
P = 0.31230.6%ORR
P Value or HR (95% CI)Pem/CisplatinEndpoint
Scagliotti GV, et al. Eur J Cancer. 2009;45(13):2298-2303.

• Continuing the same combination therapy • Crossing over to a different combination regimen• Continuing a “targeted agent” after 4-6 cycles of
chemotherapy• Instituting early second-line • Continuing “one” of the 2 agents administered
as front-line combination• Instituting a non-cross resistant agent after
initial chemotherapy
Maintenance Therapy

• Stage IIIB/IV NSCLC• ECOG PS 0-1• 4 prior cycles of
gem, doce, or tax+
cis or carbo, with CR, PR, or SD
Maintenance Pemetrexed vs Placebo
Primary Endpoint = PFS2:1
Randomization
Pemetrexed + BSC (N = 441)*
Placebo (d1, q21d) + BSC (N = 222)*
Ciuleanu T, et al. Lancet. 2009;374(9699):1432-1440.

Pemetrexed 4.0 mos
Placebo 2.0 mos
Progression-free SurvivalPF
S P
roba
bilit
y
Time (months)
HR = 0.60 (95% CI: 0.49–0.73)P < 0.00001
Ciuleanu T, et al. Lancet 2009;374(9699):1432-1440.
0 3 6 9 12 15 18 21 240.00.10.20.30.40.50.60.70.80.91.0

Overall Survival (ITT)
Pemetrexed 13.4 mos
Placebo 10.6 mos
Surv
ival
Pro
babi
lity
Time (months)
HR = 0.79 (95% CI: 0.65–0.95)P = 0.012
Ciuleanu T, et al. Lancet 2009;374(9699):1432-1440.
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 480.0
0.1
0.20.3
0.4
0.5
0.6
0.70.8
0.9
1.0

Overall SurvivalAdenocarcinoma vs Squamous
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 480.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 480.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pemetrexed 15.5 mos Pemetrexed 9.9 mos
Placebo 10.3 mos
Placebo 10.8 mos
Adenocarcinoma (n = 481)Adenocarcinoma (n = 481) Squamous (n = 182)Squamous (n = 182)
HR = 0.70 (95% CI: 0.56-0.88)P = 0.002
HR = 1.07 (95% CI: 0.49–1.73)P = 0.678
Surv
ival
Pro
babi
lity
Time (months) Time (months)
Ciuleanu T, et al. Lancet 2009;374(9699):1432-1440.

Maintenance Chemotherapy
• To be considered maintenance chemotherapy, patient must not have had progressive disease on first line therapy
PFS benefit
OS benefit 1st line bevacizumab
combo?
1st line pemetrexed?
Histology
Pemetrexed Yes Yes No No Non-squam
Docetaxel Yes No No No All
Erlotinib Yes No No All
Erlotinib + bevacizumab
Yes Yes No Non-squam
(bevacizumab) ? ? Yes No Non-squam

Second Line Chemotherapy
• To be considered second (or third line) chemotherapy, patient must have had progressive disease during or after first line therapy
• Previously there were no studies as few patients responded to first line therapy.
• Several agents have FDA approval for second line

Initial second line trial TAX 317: Docetaxel vs. Supportive Care
for Salvage Therapy in Adv NSCLC Schema
R A N D O M I Z E
Docetaxel 100 mg/m2 IV q 3 wk
Docetaxel 75 mg/m2 IV q 3 wk
Best Supportive Care (no chemo)
Stage IIIB/IV> 1 prior
platinum-based Rx
No paclitaxelPS 0-2N = 204
(protocol amendment)
Shepherd, JCO 18: 2095-2103, 2000.
Shepherd FA et al. J ClinOncol 2000: 18; 2095-2103

Shepherd FA et al. J ClinOncol 2000: 18; 2095-2103
Response(%)Median survival (months)
1-year-survival (%)
p = 0.01 (log rank)
Docetaxel 75 mg/m2 (n = 55)Best supportive care (n = 49)
0 3 6 9 12 15 18 21
Cumulative probability
0.0
0.2
0.4
0.6
0.8
1.0
Doc 6.0 7.5 37
BSC
4.6 12
Survival time (months)
Second-line Docetaxel in Advanced NSCLC

Comparing to other agents: TAX 320: Second-Line Docetaxel
Monotherapy for Advanced NSCLC
Fossella FV, et al. J Clin Oncol. 2000;18:2354-2362.
Stage III or IV locally advanced or
metastatic NSCLC
Stratified by:Response to previous
platinum-based therapyPS
N = 373
Docetaxel 75 mg/m2 q3w n = 125
Control q3wVinorelbine 30 mg/m2 days 1, 8, 15
or ifosfamide 2 mg/m2 days 1-3n = 123
R A N D O M I Z E
End PointsPrimary: overall survivalSecondary: overall response rate, duration of response, TTP, safety, quality of life

Months
% S
urvi
val
100
80
60
40
20
00 3 6 9 12 15 18 21
Second-Line Docetaxel Monotherapy for Advanced NSCLC: Survival
Median Survival
(mo)1-y Survival
(%)Docetaxel 75 mg/m2 5.7 32Vinorelbine or ifosfamide
5.6 19
P = NS P = 0.025
Fossella FV, et al. J Clin Oncol. 2000;18:2354-2362.

Second Agent approved: Pemetrexed vs. Docetaxel in 2nd-line NSCLC
Pemetrexed 500 mg/m2 i.v. q3wks (n = 2 83)(folic acid 350-1,000 µg daily + vitamin B12 1,000 µg q 9wks; dexamethasone 4mg bid on d-1,d0,d+1)
Docetaxel 75 mg/m2 i.v. q3wks (n = 288)(dexamethasone 8 mg bid on d-1,d0,d+1)
R A N D O MIZ ED
Stratified by:
• ECOG PS 0/1 vs. 2• Stage III vs. IV• # of prior chemo• Best response to prior
chemo• Time since last chemo • Prior platinum• Prior taxane• Homocysteine level • Center
Powered for equivalencyHanna N, et al. J Clin Oncol. 2004;22:1589-1597.

Second Line Therapy of Pemetrexed vs. Docetaxel Survival (ITT); Hanna, ASCO, 2003
Pemetrexed (n = 283)Docetaxel (n = 288)
Surv
ival
Dis
trib
utio
n Fu
nctio
n
MonthsITT = intent to treatHR = hazard ratioCI = confidence intervalMST = median survival time
0.00
0.25
0.50
0.75
1.00
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0 22.5
MST 8.3 mos1-yr OS: 29.7%
HR 0.9995% CI of HR (0.82, 1.20)
MST 7.9 mos1-yr OS: 29.7%
Hanna N, et al. J Clin Oncol. 2004;22:1589-1597.

Hematological Toxicities (Grade ¾ - % Patient)
Pemetrexed Docetaxel(n = 265) (n = 276) p-value
Neutropenia 5.3 40.2 < 0.001Febrile Neutropenia 1.9 12.7 < 0.001Infection w/ gr 3/4 Neutropenia 0.0 3.3 0.004
Anemia 4.2 4.3 0.99Thrombocytopenia 1.9 < 1.0 0.116
Hanna N, et al. J Clin Oncol. 2004;22:1589-1597.

Hospitalizations, Transfusions & Growth Factors
Pemetrexed Docetaxel (n = 276) (n = 265) p-value
Patients with > 1 hosp 31.7% 40.6% 0.032due to an adverse event
Total hospitalizations 1.5% 13.4% < 0.001 due to febrile neutropenia
G-CSF/GM-CSF 2.6% 19.2% < 0.001
Erythropoietin 6.8% 10.1% 0.169
Red blood cell 16.6% 11.6% 0.085Transfusions
Hanna N, et al. J Clin Oncol. 2004;22:1589-1597.

Phase III Trial of Pemetrexed Vs. Docetaxel in Pretreated NSCLC:
Efficacy by Histology
Non- Squamous*
Squamous Hazard Ratio:Non-Squam Treated with Pem Vs. Other
P - Value
Pemn = 176
Doc n = 173
Pem n = 78
Doc n = 94
OS 9.2m 8.2m 6.2m 7.4m 0.48 0.001
PFS 3.4m 3.0m 2.3m 2.7m 0.56 0.004
Peterson et al., IASLC 2007, abstract P2-328
*Adeno/Large Cell

Overall Survival (months)
50
100
Perc
ent S
urvi
ving
0
Non-squamous: Median = 9.2
Squamous: Median = 6.2
Pemetrexed in 2nd line NSCLCPeterson et al, Eur J Ca 2007 (suppl 4):363
Peterson et al., IASLC 2007, abstract P2-328

Patients Randomized to Docetaxel Overall Survival (months)
50
100
Perc
ent S
urvi
ving
Overall Survival (months)
Non-squamous: Median = 8.2
Squamous:Median = 7.4
0
Peterson et al., IASLC 2007, abstract P2-328

Why might pemetrexed be more effective in non-squamous NSCLC?
• Primary target of pemetrexed is thymidylate synthase (TS)
• TS expression is significantly higher in squamous cell vs adenocarcinoma– Ceppi et al 2006;107(7):1589-96
• Pemetrexed is more active in tumors with low levels of TS, DHFR, GARFT– Hanauske et al 2007;25(5):417-23
Hanna, ASCO, 2008

BR.21: Erlotinib vs. Placebo in 2nd or 3rd Line NSCLC
• Primary endpoint: improvement in overall survival of 33%• Secondary endpoints include progression-free survival, overall response rate,
duration of response, quality of life, and safety2:1 randomization to the experimental arm.
Eligibility• Locally advanced or metastatic NSCLC
• 1 or 2 prior chemotherapy regimen(s) failed
Stratification• Center• PS (0/1 vs 2/3)• Response to prior
therapy• Prior regimens • Prior platinum
Erlotinib: 150 mg/d+ best supportive care
n = 488
Placebo+ best supportive care
n = 243
N = 731
RANDOMIZE
Shephard FA, et al. N Engl J Med. 2005;353:123-132.

BR.21: Selected Patient Characteristics
% of Patients
CharacteristicErlotinib (n = 488) Placebo (n = 243)
≥
65 years of age 39 37Female 35 34PS 0/1 13/52 14/54 PS 2/3 26/9 23/9Adenocarcinoma 50 49Prior regimens 1/2/3 50/49/1 50/49/1Current or ex-smoker 73 77
• Patient characteristics were balanced between the arms of the study
Shephard FA, et al. N Engl J Med. 2005;353:123-132.

*From Cox regression model.†From 2-sided log-rank test.CI=confidence interval; HR=hazard ratio.
BR.21: Erlotinib Significantly Improved Overall Survival
Surv
ival
Dis
trib
utio
n Fu
nctio
n
HR (OS) = 0.70 (95% CI, 0.58-0.85)* P < 0.001†
ErlotinibPlacebo
Months0 6 12 18 24 30
1.00
0.75
0.50
0.25
0
Erlotinib 150 mg/day (n = 488)
Placebo (n = 243)
Median Survival 6.7 mo 4.7 mo1-Year Survival 31.2% 21.5%
Shepherd FA, et al. J Clin Oncol. 2004;22(suppl):14S. Abstract 7022 and oral presentation; Shepherd et al. N
Engl J Med. 2005;353:123.

Toxicity of Small Molecular Agents1. Cavitation and/or bleeding common (VEGF)
– Clearly a class effect– Seems limited to primary lung cancer
2. Hypertension– Due to INOS effect– Usually treatable with medications
3. Other unique toxicities (especially with the multitargeted agents)
– Rash– Hand-foot syndrome– Fatigue– Slightly increased neutropenia (effect of VEGF on
lymphoid cells)

Targeted Therapy in Oncology
Target• Present in tumor tissue• Critical for tumor growth/progression• Druggable• Dispensable or absent in normal cells
Agent• Targets tumor cells• Spares normal cells• Decreased toxicity
Drug Discovery and Development

Agents Targeting the VEGF Pathway
VEGFR-2VEGFR-1PPP
PPPP
P
Endothelial cell
Small-molecule VEGFR inhibitors– Vatalanib (PTK 787)– Sunitinib (SU11248)– Sorafenib (Bay 43-9006)– ZD6474
Anti-VEGFR antibodies(IMC-1121b)
VEGFAnti-VEGF antibodies
(bevacizumab)Soluble
VEGFRs(VEGF-Trap)
Podar K, Anderson K. Blood. 2005;105:1383-1395.

Phase III Trial of Bevacizumab in Non-Squamous NSCLC: ECOG 4599
N = 855 (eligible)
(PC)Paclitaxel 200 mg/m2
Carboplatin AUC = 6(q 3 weeks) x 6 cycles
(PCB)PC x 6 cycles
+Bevacizumab
(15 mg/kg q 3 wks) to PD
Eligibility:• Non-squamous NSCLC• No Hx of hemoptysis• No CNS metastases
No crossover to Bevacizumab permitted
Stratification Variables:• RT vs no RT• Stage IIIB or IV vs recurrent• Wt loss < 5% vs ≥
5%• Measurable vs non-measurable
Sandler A, et al. New Engl J Med. 2006;355:2542-2550.

Carboplatin/Paclitaxel +/- Bevacizumab: Key Clinical Outcomes
Sandler A, et al. N Engl J Med. 2006;355:2542-2550. Sandler A, et al. J Clin Oncol. 2005;23(16S):4.
HR = hazard ratio; OS = overall survival; PFS = progression-free survivalResponse rate = carboplatin/paclitaxel – 15%; carboplatin/paclitaxel + bevacizumab – 35%; P < 0.001
0 6 12 18 24 30 36
0
20
40
60
80
100
Months
P = 0.003; HR = 0.79 Median OS: 12.3 months vs
10.3 months1-Year OS: 51% vs 44%2-Year OS: 23% vs 15%
Patie
nts
Surv
ivin
g (%
)
Overall Survival
0
20
40
60
80
100
Patie
nts
With
PFS
(%)
0 6 12 18 24 30 36Months
P < 0.001; HR = 0.66 Median PFS: 6.2 months vs
4.5 months6-Month PFS: 55% vs 33%1-Year PFS: 15% vs 6%
Progression-Free SurvivalCarboplatin/paclitaxelCarboplatin/paclitaxel + bevacizumab
Carboplatin/paclitaxelCarboplatin/paclitaxel + bevacizumab

Grade 3–5 Non-Hematologic ToxicityCP
(N = 441)BvCP
(N = 427)P
ValueHemorrhage 1.1 4.7 0.001
Hemoptysis 0.5% 2.1%
CNS 0.2% 0.7%
GI 0.5% 1.2%
Other† 0.2% 1.2%
Hypertension 0.7% 7.7% < 0.001
Proteinuria --- 3.1% < 0.001
Venous thromb 3.2% 5.6%
Arterial thromb 1.6% 2.8%
Sandler A, et al. New Engl J Med. 2006;355:2542-2550.

AVAiL Trial Study Design
Reck M, et al. J Clin Oncol. 2009;27(8):1227-1234. CG: cisplatin-gemcitabine
Bevacizumab
Previously untreated, stage
IIIb, IV or recurrent non-squamous
NSCLC
RANDOMIZE
PD
Bevacizumab15 mg/kg + CG
PD
PDBevacizumab
Bevacizumab7.5 mg/kg + CG
Placebo 7.5 + CGPlacebo 15 + CG
2
1
2
1
Stratification factors: disease stage, ECOG, PS, region, gender

AVAiL Primary Endpoint: PFS
Toxicity was similar to that of E4599
Reck M, et al. J Clin Oncol. 2009;27(8):1227-1234. CG: cisplatin-gemcitabine
Bevacizumab 7.5 mg Group Bevacizumab 15 mg Group

AVAiL: Overall Survival (secondary endpoint)
1.0
0.8
0.6
0.4
0.2
0
Prob
abili
ty o
f OS
Time (months)0 6 12 18 24 30 36
347 272 182 100 36 3 0345 286 182 107 34 3 0351 264 177 92 33 2 0
Placebo + CGBev 7.5 mg/kg + CG
No. at risk
Bev 15 mg/kg + CG
*ITT (intent-to-treat) population
Placebo + CG
Bev 7.5 mg/kg
+ CG
Bev 15 mg/kg
+ CGHR (95% CI)
0.93 (0.78–1.11)
1.03 (0.86–1.23)
P value 0.42 0.76Median OS (months) 13.1 13.6 13.4
Reck M, et al. Ann Oncol. 2010 Feb 11. [Epub ahead of print]CG: cisplatin-gemcitabine

Oral VEGF-TKIs
Agent Target/MOA Company
ZD6474 VEGFR-2, EGFR AstraZeneca
Sunitinib VEGFR-1/2, PDGFR, Kit, FLT-3 Sugen/Pfizer Inc
Sorafenib VEGFR-2/3, FLT-3, Kit Onyx/Bayer
Vatalanib VEGFR-1/2/3, PDGFR, Kit Novartis
AG013736 VEGFR-1/2, PDGFR, Kit Pfizer Inc
AMG 706 VEGFR, PDGFR, Kit, Ret Amgen
AEE-788 VEGFR, EGFR, erb Novartis

Molecular Subtypes
KRAS
Adenocarcinoma
Pending
EGFR
BRAFPIK3CA
EML4-ALKFGFR4
HER2
MEK

Epidermal Growth Factor Receptor (EGFR) as a Target
• Expression in many cancers; NSCLC (> 80%)
• EGFR expression is associated with tumor growth, metastasis and poor prognosis
• Blocking EGFR has the potential to improve outcome in NSCLC

EGFR Signaling
Adapted from Ciardiello F, Tortora G. N Engl J Med. 2008;358:1160-1174.
gefitiniberlotinib

EGFR Mutations
• Found in 350 of 2105 patients with advanced NSCLC(16.6%)
• Mutation distribution – Women > men (70% vs 30%)– Never smokers > smoking history (67% vs 33%)– Those with adenocarcinomas (80.9%) (P < 0.001 for all
comparisons). • Deletions in exon 19 (62.2%) and L858R (37.8%)• Adverse events
– Mild rashes– Diarrhea– Grade 3 cutaneous toxic effects in 16 patients (7.4%) – Grade 3 diarrhea in 8 patients (3.7%)
Rosell R, et al; Spanish Lung Cancer Group. N Engl J Med. 2009;361(10):958-967.

EGFR Mutations
Rosell R, et al; Spanish Lung Cancer Group. N Engl J Med. 2009;361(10):958-967.

IPASS Study Design
Gefitinib (250 mg/day)
Carboplatin (AUC 5 or 6) / paclitaxel (200 mg/m2) 3 weekly#
1:1 randomisation
Primary• Progression-free survival
(non-inferiority)
Secondary• Objective response rate• Overall survival
Exploratory• EGFR mutation
EndpointsPatients• Chemonaïve
• Age ≥
18 years
• Adenocarcinoma histology
• Never or light ex- smokers
• Life expectancy ≥
12 weeks
• PS 0-2
• Measurable stage IIIB/ IV disease
Mok TS, et al. N Engl J Med. 2009;361(10):947-957.

First-line Gefitinib vs Carboplatin- Paclitaxel
Mok TS, et al. N Engl J Med. 2009;361(10):947-957.

First-line Gefitinib vs Carboplatin- Paclitaxel
Mok TS, et al. N Engl J Med. 2009;361(10):947-957.
Systemic Chemotherapy AdvantageGefitinib Advantage

A Phase II, Multicenter, Randomized Clinical Trial to Evaluate the Efficacy and Safety of Bevacizumab in Combination With Either
Chemotherapy (Docetaxel Or Pemetrexed) or Erlotinib Hydrochloride Compared With Chemotherapy Alone for Treatment
of Recurrent or Refractory Non-Small Cell Lung Cancer
Herbst RS, et al. J Clin Oncol. 2007;25(30):4743-4750.

Efficacy and Safety SummaryEFFICACY SUMMARY
SAFETY SUMMARY
*Proteomics pendingHerbst RS, et al. J Clin Oncol. 2007;25(30):4743-4750.

Hainsworth J, Herbst R. IASLC Chicago IL. Nov. 13-15, 2008.
Bevacizumab + Erlotinib for Advanced NSCLC After Failure of Standard First-line Chemotherapy
Patients (N = 636) randomized 1:1 Bevacizumab (15 mg/kg IV Q3 weeks) + Erlotinib (150 mg daily) orPlacebo + Erlotinib (150 mg daily)Responses assessed every 6 weeks to week 24; then every 12 weeks
Bevacizumab + Erlotinib
Placebo + Erlotinib P Value
Median Overall Survival (months) 9.3 9.20.75
HR = 0.97 (95% CI: 0.80-1.18)
Median Progression Free Survival (months) 3.4 1.7
< 0.0001HR = 0.62
(95% CI: 0.52-0.75)
Objective Response Rate 12.6 6.2 0.006

EML4-ALK Fusion Product in NSCLC • A receptor tyrosine kinase (anaplastic lymphoma kinase [ALK] fuses
to the echinoderm microtubule-associated protein-like 4 (EML-4)• Multiple variants of the translocation have been identified• Oncogenic (transforms cell lines and transgenic mice develop lung
cancer)• EML4–ALK fusion transcript was detected in 6.7% (5 out of 75) of
NSCLC patients examined
Soda M, et al. Nature. 2007;448(7153):561-566.

Frequency of EML4/ALK translocationsAuthor Total
NumberPos % Notes
Shaw ASCO 2009
141 19 13% More likely in adenocarcinoma, light or never smokers, didn’t overlap with EGFR or KRAS, younger patients
Inamura, JTO 2008
149 5 3% No overlap with EGFR or KRAS
Takeuchi, CCR 2008
253 11 4%
Koivuner, CCR 2008
305 8 3% More common in never or light smokers
Wong, Cancer 2009
266 13 5% Mostly adenocarcinoma, never smokers, younger
Takahashi, ASO 2009
313 5 1.6% Only looked at surgical cases. No overlap with EGFR, KRAS, HER2, 4 never smokers, 1 <1py smoker, all adenocarcinomas.

Is the EML4-ALK Transcript Specific for NSCLC?
• PCR in 120 NSCLC specimens1
• Controls: Non-neoplastic lung tissues • ALK protein levels assayed from 662 NSCLC specimens • Results
– EML4-ALK transcripts (variants 1 and 3) detected in 9/120 NSCLC samples • Also found in noncancerous lung tissues• No transcripts were detected in matching tumor samples from these
patients– Analysis of EML4-ALK+ cases
• Only a minority of cells harbored the EML4-ALK gene (FISH)• None of these cases was found to express the EML4-ALK protein
• Conclusion: EML4-ALK transcript cannot be regarded as a specific diagnostic tool for NSCLC
• Findings challenged by Mano et al2
Martelli MP, et al. Am J Pathol. 2009;174:661-670.Mano H, Takeuchi K. Am J Pathol. 2010 Jan 14. [Epub ahead of print]

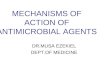
Kwak EL, et al. ASCO. 2009.
Tumor Responses to PF-02341066 for NSCLC Evaluable Patients With ALK Fusions
Tumor Size Change Duration of Response (Weeks)

Molecular Analysis and NSCLC
Bepler G, et al. Cancer Control. 2008;15(2):130-138.
ERCC1 (excision repair cross complementation)↑Expression prognostic for improved survival↑Expression predictive of reduced response to platinum-based therapy
RRM1 (regulatory subunit of ribonucleotide reductase)↑Expression prognostic for improved survival↑Expression predictive of reduced response to gemcitabine therapy
BRCA1 (breast cancer 1)Low level of expression prognostic for long survivalLow level of expression may be predictive of good platinum efficacy and poor taxane efficacy
EGFR (epidermal growth factor receptor)EGFR mutations and gene copy number prognostic of survivalPredictive for EGFR tyrosine kinase inhibitor efficacy
Oligonucleotide-based Gene Expression ProfilesPromising strategy for risk assessment and prediction of therapeutic efficacy

NSCLC Management Guidelines 1
• Recommendations for the treatment of patients with stage IV NSCLC, based on 162 publications
• Chemotherapy and biologicals• Strategies that improve overall survival • First-line therapy
– Patients with performance status of 0 or 1Platinum-based two-drug combination of cytotoxic drugs is recommended Nonplatinum cytotoxic doublets are acceptable for patients with contraindications
– For patients with performance status of 2, single cytotoxic drug is sufficient
Azzoli CG, et al. J Clin Oncol. 2009;27:6251-6266.

NSCLC Management Guidelines 2• Stop first-line cytotoxic chemotherapy at disease progression
or after 4 cycles in patients who are not responding to treatment
• Stop two-drug cytotoxic chemotherapy at 6 cycles in all patients
• EGFR mutations – First-line gefitinib may be recommended for patients with
known mutation– Otherwise, cytotoxic chemotherapy is preferred – Cetuximab is recommended with cisplatin-vinorelbine for
patients with EGFR-positive tumors by IHC • Bevacizumab is generally recommended with carboplatin-
paclitaxel
Azzoli CG, et al. J Clin Oncol. 2009;27:6251-6266.

NSCLC Management Guidelines 2
• Second-line therapy – Docetaxel – Erlotinib – Gefitinib or– Pemetrexed
• Third-line therapy – Erlotinib for erlotinib or gefitinib naive patients– Data are insufficient to recommend the routine third-
line use of cytotoxic drugs• Data are insufficient to recommend routine use of
molecular markers to select chemotherapy

Nursing Considerations
• Assessment– Geriatric Patient
• Planning– Histology, Stage, Intervention
• Patient Education– Knowledge base
• Caregiver Support• Resources

Multidisciplinary Patient Management
• Medical Oncology• Thoracic Surgery• Pulmonology• Radiation Therapy• Pathology• Nursing• Pharmacy• Medical Director• Case Manager• Clinical Research Team

Communication With Patients Goals
• Compliance (especially with po medications)• Smoking cessation• Patient self evaluation and reporting • Manage disease symptoms, disease burden,
and treatment side effects• Offer Web resources

• 55-year-old person with Stage IV NSCLC– Adenocarcinoma histology– Good performance status– Hemoptysis on 3 occasions, total ~15 cc blood
• What is the most appropriate chemotherapy ?A. Cisplatin and gemcitabineB. Cisplatin and pemetrexedC. Carboplatin, paclitaxel, bevacizumabD. Carboplatin and paclitaxelE. Cisplatin, vinorelbine, cetuximab
Case Scenario 1

• 55-year-old woman with Stage IV NSCLC– Adenocarcinoma – Good performance status– EGFR exon 19 deletion
• What is the optimal chemotherapy?A. Carboplatin, paclitaxel, bevacizumabB. Carboplatin, paclitaxelC. Cisplatin, pemetrexed, bevacizumabD. Erlotinib
Case Scenario 2

• 55-year-old woman with Stage IV adenocarcinoma of the lung, completes 6 cycles of cisplatin, paclitaxel, and bevacizumab with stable disease, grade 1 neuropathy, and continues to work full time
• What is the most appropriate next step?A. Continue cisplatin, paclitaxel, and bevacizumab until
progressionB. Continue paclitaxel and bevacizumab until progressionC. Begin docetaxel until progressionD. Begin pemetrexed until progressionE. Discontinue therapy and monitor until progressive
disease
Case Scenario 3

• 55-year-old man with Stage IV squamous cell carcinoma completes 6 cycles of cisplatin and vinorelbine with stable disease, grade 1 neuropathy, and continues to work full time
• What is the most appropriate next step?A. Continue cisplatin and vinorelbine until progressionB. Start cetuximab and continue until progressionC. Start docetaxel and continue until progressionD. Start pemetrexed until progressionE. Discontinue therapy and monitor until progressive
disease
Case Scenario 4

Summary• Chemotherapy
– Two agents > one – Three agents no better than two – Role for maintenance therapy?
Still under evaluation
• Targeted Therapy– Agents targeting the EGFR and VEGF pathways have proved
successful– Further study will include
Earlier stage NSCLC– The small molecule VEGF inhibitors appear promising in phase
II trials and are being studied in phase III trials– Combining targeted agents appears promising– Targeting the insulin-like growth factor pathway
Promising candidates in development

Lung Cancer: Conclusions
• Smoking remains primary cause of lung cancer• Screening remains controversial• Staging helps determine treatment• Clinical trial participation may be attractive• Multiple options in non-small cell lung cancer• The future: Treat lung cancer based on
molecular characteristics of tumors

Please take post-test now and complete the evaluation form