-
ft-
ettM.
oad
KEYWORDS:Left-sided gallbladder;Preoperative diagnosis;Bile duct
injury;Intrahepatic portal;Venous and biliarysystems;
uncommon anomaly. The first published account of sinis-1
tography. Although laparoscopic cholecystectomy for
patic portal venous and biliary systems associated with
nperforming any form of partial hepatectomy, including
2,68
A retrospective review was performed on patients with
possible, appropriate radiographs were retrieved and ana-lyzed,
together with intraoperative photographs whentaken. The
preoperative diagnosis of left-sided gallbladderwas assessed. The
details of the operative procedure were
---* Corresponding author. Tel.:161-7-3176-2111;
fax:161-7-3176-7011.
The American Journal of Surgery (2013) -, --E-mail address:
[email protected] gallbladders can be
performed safely,4,5 it wouldappear from the literature that bile
duct injury at cholecys-tectomy is not unusual.2,6 Because of the
anomalous intrahe-
left-sided gallbladder who were managed by the PrincessAlexandra
Hospital hepatobiliary surgeons since 1996. Thepatients were
identified by way of unit log books. Whentroposition of the
gallbladder was in 1886, and fewer than150 cases have been reported
in the literature.2 However,the condition may not be as rare as
generally believed,3
and the diagnosis is frequently missed even with
ultraso-nography and endoscopic retrograde cholangiopancrea-
4
reduced-size and living-donor liver transplantation.
Patients and MethodsLeft-sided gallbladder is considered to be a
very sinistroposition, the implications are considerable wheHepatic
resectionManuscript received July 10, 2012; r
2012
0002-9610/$ - see front matter
2013http://dx.doi.org/10.1016/j.amjsurg.20AbstractBACKGROUND: A
left-sided gallbladder in a normally positioned liver is considered
to be a very
uncommon anomaly. Laparoscopic cholecystectomy can be performed
safely, but bile duct injury isnot unusual. It is associated with
anomalous intrahepatic portal and biliary systems which impactsany
form of partial hepatectomy.
METHODS: We performed a retrospective review of patients with
left-sided gallbladder who weremanaged by the hepatobiliary
surgeons at our institution since 1996.
RESULTS: Nineteen patients with left-sided gallbladder underwent
a hepatobiliary procedure. Of the13 patients with gallstones, only
1 was diagnosed before cholecystectomy. Nine operations
werecompleted laparoscopically, whereas 4 required an open
procedure. Two patients were referred withbile duct injuries. There
was 1 liver resection for a colorectal metastasis. Left-sided
gallbladders in3 deceased organ donors resulted in major
implications in the performance of liver transplantation.
CONCLUSIONS: Left-sided gallbladders are probably more common
than generally believed but arerarely diagnosed before
cholecystectomy. Associated bile duct injury appears to be not
infrequent.Because of the aberrant vasculobiliary anatomy, any form
of liver resection requires careful planning. 2013 Elsevier Inc.
All rights reserved.Surgical implications of a le
Russell W. Strong, M.D.*, Jonathan FawcPeter Hodgkinson, M.D.,
Stephen Lynch,Kellee Slater, M.D., Shinn Yeung, M.D.
Hepatobiliary Unit, Princess Alexandra Hospital, Ipswich Revised
manuscript September 10,
Elsevier Inc. All rights reserved.
12.10.035, Woolloongabba, Queensland 4102, Australiasided
gallbladder
, M.D., Michael Hatzifotis, M.D.,D., Thomas ORourke,
M.D.,scrutinized, and particular attention was paid to the methodof
gallbladder removal, either laparoscopically or as an
-
open operation. In those patients with left-sided gallbladderin
whom partial hepatectomy, including reduced-size
livertransplantation, was performed or planned, the conse-quences
related to the anomalous portal venous and biliarysystems were
assessed.
Results
veins between the liver and the inferior vena cava (IVC),
2There were 19 patients with left-sided gallbladders
whounderwent surgical procedures (Table 1). Thirteen
patientspresented with typical biliary-type pain, and
gallstoneswere diagnosed by ultrasonography. However, only1 patient
was diagnosed preoperatively as having a left-sided gallbladder,
and this was as a result of computedtomography performed for
another reason.
Of the 13 patients undergoing cholecystectomy, 9 pro-cedures
were successfully performed laparoscopically;1 procedure was
converted to an open operation tocomplete exploration and remove a
stone in the commonbile duct. Three procedures were converted to
openoperations to complete the cholecystectomy. One patientwho had
gallstones diagnosed by ultrasonography wasreferred by a surgeon
who could not find the gallbladder atopen operation. At reoperation
by one of our surgeons(S.L.), the gallbladder could not be found
extrahepati-cally, but a hard lump was palpable intrahepatically
insegment 3. Opening the liver identified the
intrahepaticgallbladder, which was then removed. However, therewere
5 bile ducts draining directly into the gallbladder,and a
challenging Roux-en-Y biliary reconstruction of the5 ducts ensued.
The patient was well with normal liverfunction 4 years later.
There were 2 patients who sustained bile duct injuryduring
cholecystectomy of a left-sided gallbladder at otherinstitutions.
They were immediately referred to the hep-atobiliary unit at
Princess Alexandra Hospital, and 1 of thesurgeons (J.F.) traveled
to these hospitals to perform biliaryreconstruction. The patients
have been well since that time.
There was 1 patient with a colorectal liver metastasis,which was
originally thought to be in the left hemiliver, butidentification
of a left-sided gallbladder led to the realiza-tion that there was
an absent segment 4, and a left-sidedresection would necessitate
extension into segments 5and 8. This was achieved without any
problems.
There were 3 deceased organ donors with left-sidedgallbladders.
All donor operations were performed by 1 ofour surgeons (R.S.). The
first was in 1997 and was from an
Table 1 Patients with left-sided gallbladder
undergoinghepatobiliary surgical procedure
Cholecystectomy 13Biliary reconstruction after bile duct injury
elsewhere 2Liver resection for colorectal metastasis 1Donor liver
for transplantation 3
Total 19and the major hepatic veins bypassing the IVC
andconnected directly to the right atrium. It was decided notto use
the liver for transplantation.
Comments
The finding of a left-sided gallbladder signifies a
devel-opmental aberration, which may have major consequenceswhen
performing cholecystectomy or any form of hepatec-tomy. The vast
majority of publications on the subject haveemanated from Asian
countries, especially Japan, butwhether the incidence is greater
there or is just identifiedwith greater frequency is not known. The
reportedincidence of the condition ranges from 0.2% to 1.1%.6 Ina
recent publication from the University of Tokyo Hospital,a
3-dimensional reconstruction of the vascular structures ofthe liver
among 8,050 consecutive image readings by 1 radi-ologist over a
7-year period found 35 patients (0.4%) whowere incidentally
diagnosed.3 Moo-Young et al2 estimatedthat in the United States,
between 70 and 100 cases ofleft-sided gallbladder will be seen at
laparoscopic cholecys-tectomy each year.
So, how does a left-sided gallbladder come about? Thereis a
difference of opinion about origin as well as nomen-clature. Uesaka
et al,7 in reporting on 2 patients withleft-sided gallbladders,
showed intrahepatic portal venousanomalies. In the fetal period,
the intrahepatic portalvenous system develops from the pair of
umbilical veins.During development, the left umbilical vein becomes
1 ofadult donor. The intention was to harvest a reduced-sizegraft
for a child who was in desperate need of livertransplantation. The
intrahepatic vasculobiliary anatomywas confusing, and the procedure
would have been aban-doned except for the relative urgency. Within
48 hours oftransplantation, portal vein thrombosis had
occurred,necessitating urgent repeated transplantation.
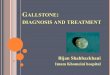
The second donor liver with sinistroposition of thegallbladder
was intended to be used as a split liverdtheright side for an adult
recipient and the left side for a child.On finding a left-sided
gallbladder, the proposition wasabandoned, the surgeon being very
aware of the previousexperience. The liver was used purely as a
whole liver graftfor an adult. A cholangiogram after
transplantation showedthe biliary anatomy, (Fig. 1) which in itself
would havemade split liver transplantation extremely difficult, but
to-gether with the likely aberrations of the intrahepatic portaland
hepatic venous systems,7,8 it was virtually impossible.
The third donor with a left-sided gallbladder was a12-year-old
girl who had cardiac arrest outside a majorprovincial hospital. She
was resuscitated but became braindead and was an organ donor. She
had previously had openheart surgery. At the donor operation, she
was found tohave a left-sided gallbladder; a preduodenal portal
vein,hepatic artery, and common bile duct; no short hepatic
The American Journal of Surgery, Vol -, No -, - 2013the afferent
vessels to the liver, whereas the right umbilical
-
laddvein atrophies. After obstruction of the left umbilical
veinand ductus venosus, the typical umbilical portion to theleft
main portal vein is formed. Atrophy of the left umbil-ical vein,
with persistence of the right umbilical vein, prob-ably accounts
for the anomaly. It can be associated withother anomalies,
including a preduodenal portal vein, asidentified in 1 of the liver
donors in this series, or azygoscontinuation of the IVC. On
occasion, all of these anoma-lies are considered to accompany
developmental failureof other intra-abdominal vascular
systems.8,9
Nagai et al8 from Japan do not regard it as a
left-sidedgallbladder but as a right-sided round ligament, which is
as-sociated with abnormal intrahepatic venous branching andhas
significant implications during liver resection. Thisconcept is
supported by Shindoh et al,3 who concluded
Figure 1 The biliary anatomy.R.W. Strong et al. Surgical
implications of left-sided gallbthat it was a right-sided round
ligament with anomalousconnection to the right paramedian portal
pedicle, wasnot a malposition of the gallbladder, and its origin
wascaused by a persistence of the right umbilical vein.
In contrast, Savier et al6 in Paris believe that it is
bestunderstood as a failure of development of the medial seg-ment
of the left hemiliver, ie, segment 4, and fusion ofthe midplane and
left intersectional plane. Further, in a laterstudy using
multidetector-row computed tomography with3-dimensional volume
rendering reconstruction, the sameauthors were firm in their belief
that the abnormality isnot a consequence of the persistence of the
right umbilicalvein but the result of defective development of the
medialsection of the left hemiliver during embryonic life
and,therefore, fusion of the planes.10
Implications for cholecystectomy
This is all somewhat academic for the surgeon who isabout to
perform a cholecystectomy and is unexpectedlyfaced with a
left-sided gallbladder. Both in the presentseries and from reports
in the literature, the preoperativediagnosis of a left-sided
gallbladder is rare.2,4,5,11 It is asso-ciated with anomalies of
the cystic duct and artery.2,4,12 Thecystic artery originates from
the right hepatic artery, whichlies to the right of the common
hepatic duct (CHD), alwayspassing from right to left across in
front of the CHD to thegallbladder.4 The cystic duct most commonly
curls aroundthe CHD to enter it on the right side but may enter the
CHDon its left side or, as in 1 case in the present series, enter
theleft hepatic duct. The possibility of an anomaly of the
bileducts should always be considered when a left-sided
gall-bladder is encountered.2
There is no doubt that patients with left-sided gallblad-der can
have it successfully removed laparoscopically as inthe present
series and as reported in the literature.4,5,13
Although cholecystectomy can be performed with the stan-dard
port sites, the best arrangement consists of medial po-sitioning of
the gallbladder retracting ports Fig. 2A andplacement of the
right-hand operating port well to the leftof the midline. According
to Idu et al,4 the most useful sim-ple procedure for improving
exposure is the falciform lift,which lifts the central portion of
the liver and moves theligament off the operative field Fig.
2B.
It would seem most prudent to perform a retrogradedissection,
fundus down, whether laparoscopically or as anopen procedure Fig.
2C. During laparoscopic cholecystec-tomy, the main problem seems to
be surgical exposure be-cause of the vicinity of several bile ducts
in a limited spaceunder the round ligament, including the
hepatoduodenalligament just behind the neck of the gallbladderFig.
2D,E. A cautious laparoscopic approach would seemreasonable, taking
into account other local conditionssuch as inflammation,
remembering that bile duct injurywould appear to be more likely to
occur with a left-sidedgallbladder.2,6 In addition, there is a
variable degree towhich the gallbladder is embedded within the
liver paren-chyma, which in itself causes technical difficulties.
Theextreme end of the spectrum was manifested in 1 case inthis
series.
There should be a strong tendency to convert to anopen procedure
when there is anatomic uncertainty,particularly when there is
marked inflammation. Thegallbladder obscures the hepatoduodenal
ligament struc-tures. The inability to dissect and reveal the
Calottriangle, as in cholecystectomy of a gallbladder in thenormal
position, is almost certainly a contributing factortoward an
increased propensity to cause bile duct injury,and awareness of
such issues should help avoid this.Perception and orientation are
extremely important insurgery, and especially in minimal access
surgery, aspointed out in a recent article by Sodergren et al.14
Wayet al,15 in an analysis of 252 cases of laparoscopic bileduct
injuries, found the primary error in 97% of caseswas a visual
perceptual illusion, leading to operator diso-rientation, and
Hugh16 suggested that misidentification ofbiliary anatomy with
inadequate extrabiliary reference
er 3points led to disorientation and was a major cause of
-
4bile duct injury during laparoscopic cholecystectomy. Ifthese
parameters are instrumental in such problems dur-ing so-called
routine laparoscopic cholecystectomy, thinkof how much more likely
bile duct injury is to occur whendealing with a left-sided
gallbladder.
Implications for hepatic resection and livertransplantation
Although detailed vascular and biliary anatomy is notnecessary
before performing a cholecystectomy, it is abso-lutely essential
before performing a partial hepatectomy,including the use of
reduced-size grafts for liver transplan-tation. In addition,
routine intraoperative confirmation ofthe vascular structures using
ultrasonography or a testclamp before ligation of prominent vessels
may reducethe risk of anatomic misinterpretation and
subsequentsurgical complications.3 Close attention must be paid
tothe abnormal branching of the intrahepatic portal vein.When
performing a right hemihepatectomy, only the portal
Figure 2 (AE) Laparoscopic cholecysThe American Journal of
Surgery, Vol -, No -, - 2013branches that arise from the right
umbilical vein and courseto the right should be divided. Ligation
of the right portalvein itself results in interruption of portal
flow to a portionof the left hemiliver.7,8
What about the use of partial livers for transplantationfrom
donors with left-sided gallbladders? There have beensuccessful
living donor transplantations, mainly adult tochild, using the left
side, but even in these cases technicalmodifications were required,
and considerable preoperativeimaging and preparation was
necessary.1719 In the settingof deceased donors, who are the main
source of organs inWestern societies, this imaging and preparation
is not pos-sible, and it would seem most appropriate to use the
wholeliver in these circumstances.
Conclusions
In conclusion, left-sided gallbladders are probably morecommon
than generally believed. They are rarely diagnosedbefore
cholecystectomy. Itwould appear that cholecystectomy
tectomy of a left-sided gallbladder.
-
is associated with a higher rate of bile duct injury with
left-sided gallbladders than when the gallbladder is in its
normalposition. Because of the aberrant intrahepatic
vasculobiliaryanatomy, any form of liver resection is complex and
requirescareful planning.
References
1. Hochstetter F. Anomalien der Pfortader and der Nabelvene in
Verbin-
dung mit Defect oder Linkslage der Gallenblase. Arch Anat
Entwick;
1886:36984.
2. Moo-Young T, Picus D, Teefey S, et al. Common bile duct
injury fol-
lowing laparoscopic cholecystectomy in the setting of
sinistroposition
of the gallbladder and biliary confluence: a case report. J
Gastrointest
Surg 2010;14:16070.
3. Shindoh J, Akahane M, Satou S, et al. Vascular architecture
in anom-
alous right-sided ligamentum teres: three dimensional analyses
in
35 patients. HPB (Oxford) 2012;14:3241.
4. Idu M, Jakimowicz H, Iuppa A, et al. Hepatobiliary anatomy
in
patients with transposition of the gallbladder: implications for
safe
laparoscopic cholecystectomy. Br J Surg 1996;83:14423.
5. Mulvey J, Laura S, Kelly T. Laparoscopic removal of the
left-sided
gallbladder. ANZ J Surg 2004;74:3901.
6. Savier E, Taboury J, Lucidarme O, et al. Fusion of the planes
of the
liver: an anatomic entity merging the midplane and the left
intersec-
tional plane. J Am Coll Surg 2005;200:7119.
7. Uesaka K, Yasui K, Morimoto T, et al. Left -sided gallbladder
with in-
trahepatic portal venous anomalies. J Hepatobiliary Pancreat
Surg
1995;2:42530.
8. Nagai M, Kubota K, Kawasaki S, et al. Are left-sided
gallbladders
really located on the left side? Ann Surg 1997;225:27480.
9. Matsusue S, Kashihara S, Koizumi S. Pancreatectomy for
carcinoma
of the head of the pancreas associated with multiple anomalies
includ-
ing preduodenal portal vein. Jpn J Surg 1984;14:3948.
10. Lucidarme O, Taboury J, Savier E, et al. Fusion of the
midplane with
the left intersectional plane: a liver anatomical variation
revisited with
multidetector-row CT. Eur Radiol 2006;16:1699708.
11. Wong L, Rusby J, Ismail T. Left-sided gallbladder: a
diagnostic and
surgical challenge. ANZ J Surg 2001;71:5578.
12. Wu T, Lee R, Chiang J, et al. Reappraisal of left-sided
gallbladder and
its accompanying anomalies: a report of two cases and
literature
review. Acta Radiol 2005;46:2336.
13. Reddy P, Subramanian R, Yuvaraja S. Laparoscopic
cholecystectomy
for left-sided gallbladder. JSLS 2005;9:3567.
14. Sodergren M, Yang GZ, Lord Darzi A. Perception and
orientation in
minimally invasive surgery. Arch Surg 2012;147:2101.
15. Way LW, Stewart L, Gantert W, et al. Causes and prevention
of lapa-
roscopic bile duct injuries: analysis of 252 cases from a human
factors
and cognitive psychology perspective. Ann Surg
2003;237:4609.
16. Hugh TB. New strategies to prevent laparoscopic bile duct
injury: sur-
geons can learn from pilots. Surgery 2002;132:82635.
17. Maetani Y, Itoh K, Kojima N, et al. Portal vein anomaly
associated
with deviation of the ligamentum teres to the right and
malposition
of the gallbladder. Radiology 1998;207:7238.
18. Rocca J, Rodriguez-Davalos M, Burke-Davis M, et al. Living-
donor
hepatectomy in right-sided round ligament liver: importance of
map-
ping the anatomy to the left medial segment. J Hepatobiliary
Pancreat
Surg 2006;13:4547.
19. Hwang S, Lee SG, Park KM, et al. Hepatectomy of living
donors with
a left-sided gallbladder and multiple combined anomalies for
adult-to-
adult living donor liver transplantation. Liver Transpl
2004;10:1416.
R.W. Strong et al. Surgical implications of left-sided
gallbladder 5
Surgical implications of a left-sided gallbladderPatients and
MethodsResultsCommentsImplications for cholecystectomyImplications
for hepatic resection and liver transplantation
ConclusionsReferences

















![Surgical Management of Cholangiocarcinoma1].2... · ectable biliary cancerectable biliary cancer py prior to surgical exploration (HC = 59%, GB = 82%) nts with gallbladder cancer](https://img.pdfslide.net/doc/110x75/5f4dc0a6f6e64a3565033521/surgical-management-of-c-12-ectable-biliary-cancerectable-biliary-cancer.jpg)