Embed Size (px)
Citation preview

Surgical management in differentiated thyroid cancer
1
Surgical management in differentiated thyroid cancer นพ. วงศกร เชาวชาญกจ
อ.นพ. สมฤทธ( มหธโนมล ภาควชาศลยศาสตร คณะแพทยศาสตร
มหาวทยาลยสงขลานครนทร จากขอมลของ GLOBOCAN ป 2012 ผปวยมะเรงทFงหมด 7 พนลานคน เปนผชายและผหญงอยางละ 3.5 พนลานคนพบวาอบตการณของมะเรงไทรอยดในเพศชายรอยละ 0.9 เพศหญงรอยละ 3.5(1) ในประเทศสหรฐอเมรกามผปวยประมาณ 58,629 คนทVถกวนจฉยวาเปนมะเรงไทรอยดตFงแตป 2008-2012 โดยรอยละ 89 เปน papillary, รอยละ 5.1 เปน follicular, รอยละ 2.2 เปน Hurthle cell, รอยละ 1.7 เปน medullary และรอยละ 0.8 เปน anaplastic(2) จากขอมลของ Cancer in Thailand ตFงแตป 2010-2012อบตการณของมะเรงไทรอยด พบในผหญงมากกวาผชายประมาณ 3.4เทา(3)เปนมะเรงทVพบบอยเปนอนดบเจดในผหญง (5.1 รายตอแสน) สาหรบขอมลของโรงพยาบาลสงขลานครนทร ประจาป 2014 จานวนผปวยมะเรงรายใหมทFงหมด 5,320 คน พบมะเรงไทรอยดในเพศชาย 50 คนคดเปนรอยละ 2 และเพศหญง 214 คนคดเปนรอยละ 8โดยแบงเปน papillary รอยละ 77, follicular รอยละ 13(4)
ในบทความนFจะกลาวถงคาแนะนาตาม American Thyroid Association (ATA) 2015 ในสวนทVเกVยวของกบผาตดรกษาผปวย differentiated thyroid cancer ชนด papillary thyroid cancer (PTC)และ follicular thyroid cancer (FTC)ทFงกอน ระหวางและหลงผาตด Preoperativeinvestigation and care
1. Neck imaging – ultrasound (US) a. การทา preoperative neck US ของตอมนFาเหลองทVคอ (central and lateral neck compartment) แนะนาให
ทาในผปวยทกรายทVจะทา thyroidectomy ทVมลกษณะทาง cytologyทVสงสยหรอเปน malignant หรอลกษณะจากทาง molecular
b. US-guided FNA ใหทาในผปวยทVมตอมนFาเหลองทVมขนาด≥8-10 มลลเมตร ทVมลกษณะทาง อลตราซาวดทVสงสยวาเปน malignancy

Surgical management in differentiated thyroid cancer
2
ใน Differentiated thyroid carcinoma โดยเฉพาะ papillary carcinoma จะมการแพรกระจายไปยงตอมนFาเหลองรอยละ 20-50(5)และอาจจะพบไดตFงแตมะเรงยงอยในตอมไทรอยดและมขนาดเลกการตรวจพบ micrometastases (<2 mm) อาจพบไดถงรอยละ90 ขFนอยกบวธการตรวจ(6)อยางไรกตามความสาคญของ micrometastases ยงนอยกวา macrometastases มาก
ลกษณะทางอลตราซาวดทVบงบอกถง metastatic lymph nodes ไดแก enlargement, loss of the fatty hilum, rounded rather than oval shape, hyperechogenicity, cystic change, calcifications and peripheral vascularity มการศกษา(7)พบวาลกษณะทVม sensitivity สงสดคอ absence of a hilum (100%) แตม low specificity (29%) สวน microcalcifications ม specificity สงสด (100%)
ตาแหนงของตอมนFาเหลองมความสาคญmalignant lymph nodes มกพบทV levels III, IV และ VI มากกวา IIอาจจะไมเสมอไปใน PTC ทV upper pole ซV งมกจะพบทV levels III และ II(7)
นอกจาการด cytology แลวการตรวจ US-guided FNA with thyroglobulin (Tg) in FNA washout fluid measurement เปนการชวยเพVมการวนจฉย metastatic lymph node ในกลมทVม 1 หรอ 2 ขอของ suspicious US feature ซV งในการศกษาของ Pak et al.(8)แนะนาคา cutoff ของ FNA-Tg ทV 32 ng/mL
2. Neck imaging – CT/MRI/PET
a. การใช CT, MRI with intravenous contrast แนะนาในผปวยทVสงสย advanced disease ไดแก invasive primary tumor, multiple or bulky lymph node involvement
b. Routine preoperative 18FDG-PET scanning ไมเปนทVแนะนา เนVองจากการทา US เปน operator dependent และไมสามารถประเมนอวยวะทVอยลกได นอกจากนFการทVม
กระดกหรอลมจะทาใหมขอจากดของการทา US สาหรบใน locally invasive primary tumors (Progressive dysphagia, respiratory compromise, hemoptysis,
rapid tumor enlargement, significant voice change or finding of vocal cord paralysis, mass fixation to airway or neck, sonographic features of extrathyroidal extension (posterior or mediastinum) ซV งในกลมผปวยเหลานFการทา CT/MRI with IV contrast จะไดประโยชนเพVอวางแผนการรกษาตอไป แตการทVผปวยไดรบ iodine โดยทVวไปแลวจะถกกาจดหมดภายใน 4-8 สปดาห ซV งการทา imaging with contrast อาจทาใหผปวยไดรบการรกษาลาชาขFน ถาวางแผนรกษาRAI หลงการผาตด(9)

Surgical management in differentiated thyroid cancer
3
3. การวด Serum Tg และ anti-Tg antibodies สาหรบการตรวจ serum Tg หรอ anti-Tg antibodies ไมแนะนาใหตรวจ ซV งจาก systemetic review และ
meta-analysis พบวา การตรวจพบ serum Tg ทVสงกอนการผาตดอาจจะบอกความไว (sensitivity) ของการตดตามโรคดวย serum Tg ไดดขFนหลงการผาตด จากการศกษา cross-sectional analysis จากผปวย 1,770 คน ทVมการตรวจ anti-Tg antibodies ในชวง perioperation จาก National Thyroid Cancer Treatment Cooperative Study ระหวางป 1987 ถง 2011 พบวา คา serum anti-Tg antibody ไมไดมความสมพนธกบระยะของโรคหรอ disease-free รวมทFง overall survival(10)
4. Preoperative care communication กอนการผาตด ศลยแพทยควรจะแนะนาผปวยเกVยวกบความเสVยงของการผาตดรวมถง การบาดเจบตอ
เสนประสาทและตอมพาราไทรอยด(11) 1. Preoperative voice assessment ผปวยทกคนทVเขารบการผาตดไทรอยดควรจะมการประเมนการเสยงโดยให
ผปวยบอกการ เปลVยนแปลงของเสยงรวมกบแพทยในการประเมนเสยงของผปวย 2. Preoperative voice assessment
a. Preoperative voice abnormalities b. History of cervical or upper chest surgery (RLN or vagus nerve at risk) c. Known thyroid cancer with posterior extrathyroidal extension or extensive central nodal
metastases การเปลVยนแปลงของเสยงเปนภาวะแทรกซอนทVสาคญของการผาตดไทรอยด ซV งสงผลตอการใชชวต การ
ประเมนกอนการผาตดจงมความจาเปนซVงหากพบวาม preoperative vocal cord paralysis หรอ paresis อาจบอกไดวาเปน invasive thyroid malignancy และมความสาคญในการวางแผนการผาตดและการประเมนทางเดนหายใจ(12) การบาดเจบตอ contralateral nerve ขณะผาตดเปนสาเหตของการเกด bilateral cord paralysis ได ซV งการประเมนควรถามถงการเปลVยนแปลงหรอความผดปกตของเสยงทFงจากผปวยและแพทย ซV งตองลงบนทกไวในเวชระเบยน
การทางานของเสยงและกลองเสยงอาจจะประเมนโดย laryngoscopy ซV งการประเมนจากเสยงอยางเดยวอาจจะไมเพยงพอ พบวา อตราของpreoperative vocal cord paresis ในผปวยทVเปน benign thyroid disease จาก laryngoscopy พบไดรอยละ 0-3.5 และมากถงรอยละ 8 ในผปวยมะเรงไทรอยด(13)รอยละ 10-15 ของผปวยทVเปนมะเรงไทรอยดทVมาดวย extrathyroidal extension อวยวะทVมกจะเกVยวของไดแก strap muscle (53%), RLN (47%), trachea (30%), esophagus (21%) และ larynx (12%)(14)

Surgical management in differentiated thyroid cancer
การตรวจกลองเสยงควรจะไดรบการตรวจแมวาผปกบ RLN (thyroid หรอ parathyroid) anterior approach to cervical spine) ละ 1.5-30 ในผปวยหลงผาตดโดยไมมอาการประมาณ มะเรงไทรอยดทVม gross extrathyroidal extension เสยงปกต(15)
ระยะของโรค (Tumor staging)(16)
agement in differentiated thyroid cancer
การตรวจกลองเสยงควรจะไดรบการตรวจแมวาผปวยจะมเสยงปกต ถามประวตการผาตดทVคอ ทVparathyroid) หรอ vagus nerve (carotid endarterectomy, cervical esophagectomy
anterior approach to cervical spine) หรอมประวตของการฉายแสงทVคอ ซV ง vocal cord paralysis ไมมอาการประมาณ 1 ใน 3 นอกจากนF การตรวจกลองเสยงแ
gross extrathyroidal extension ไปทางดาน posterior หรอม extensive nodal involvement
(16)
4
วยจะมเสยงปกต ถามประวตการผาตดทVคอ ทVเกVยวของvagus nerve (carotid endarterectomy, cervical esophagectomy และ
ocal cord paralysis อาจจะพบไดรอยการตรวจกลองเสยงแนะนาใหผปวย
extensive nodal involvement แมวา

Surgical management in differentiated thyroid cancer
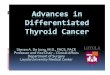
รปทV 1 AJCC 7th edition/TNM classification system for differentiated thyroid carcinoma
2. การผาตดรกษามะเรงไทรอยดชนด
การรกษามเปาหมายหลก ไดแก
1. เพVมอตราการรอดชวตทFงหมดและจากตวโรค 2. ลดความเสVยงของการเกด 3. การประเมนระยะของโรคทVถกตองและหลกเลVยงการรกษาทVเกนความจาเปน
สาหรบเปาหมายจาเพาะของการผาตด คอ
1. การผาตดเอา primary tumor:ขณะทVการม residual metastatic lymph nodes
2. การลดความเสVยงของการกลบเปนซF าและการแพรกระจายของตวโรคการรกษาโรค ขณะทVการรกษาโดยใช (adjuvants roles)(18)
agement in differentiated thyroid cancer
edition/TNM classification system for differentiated thyroid carcinoma
การผาตดรกษามะเรงไทรอยดชนด Papillary และ Follicular
เพVมอตราการรอดชวตทFงหมดและจากตวโรค (overall and disease-specific survival)ลดความเสVยงของการเกด persistent/recurrent disease และภาวะแทรกซอน การประเมนระยะของโรคทVถกตองและหลกเลVยงการรกษาทVเกนความจาเปน
ของการผาตด คอ
primary tumor:การทา completeness of surgical resection มความสาคญตอresidual metastatic lymph nodes เปนสาเหตทVพบไดบอยทVเกด persistence/recurrence
การลดความเสVยงของการกลบเปนซF าและการแพรกระจายของตวโรค: การผาตดเปนสVงทVสาคญทVสดในะทVการรกษาโดยใช RAI, TSH suppression และการรกษาอVนๆเปนการรกษาเสรม
5
edition/TNM classification system for differentiated thyroid carcinoma
specific survival)
มความสาคญตอ ผลการรกษา persistence/recurrence(17)
การผาตดเปนสVงทVสาคญทVสดในและการรกษาอVนๆเปนการรกษาเสรม

Surgical management in differentiated thyroid cancer
6
3. การให postoperative RAI:สาหรบผปวยทVได RAI remnant ablation หรอการรกษาดวย RAI หรอใหในกลมของ residual หรอ metastatic disease การผาตดเอาตอมไทรอยดออกไดทFงหมดเปนองคประกอบทVสาคญของการรกษา(19)
4. การประเมนระยะและความเสVยงของตวโรคอยางแมนยา:ระยะและความเสVยงของการเปนโรคถกใชเพVอวางแนวทางการพยากรณโรคเบFองตน แนวทางการรกษา การตดตามผลการรกษา ซV งมความสาคญในการรกษาโรค(20)
5. เพVอการตดตามโรคอยางแมนยาในระยะยาวเพVอดการกลบเปนซF าของโรค 6. ลดอนตรายจากการรกษา:โดยวธการผาตดและประสบการณของศลยแพทยเปนสVงสาคญในการลด
ภาวะแทรกซอนจากการผาตด การผาตดตอมไทรอยด(11)
a. สาหรบผปวยมะเรงไทรอยดทVมขนาด > 4 cm, gross extrathyroidal extension (cT4), metastatic lymph nodes (cN1), distant metastases (cM1) การรกษาเรVมตนคอ การทา near-total or total thyroidectomy and gross removal of all primary tumorถาไมมขอหาม
b. สาหรบผปวยมะเรงไทรอยดทVมขนาด > 1 cmแต < 4 cm ทVไมม extrathyroidal extension หรอ metastatic lymph nodesการรกษาเรVมตนคอ การทา near-total or total thyroidectomy หรอ lobectomyซV งการทา thyroid lobectomy เพยงอยางเดยวเพยงพอสาหรบการรกษา low-risk papillary and follicular carcinoma อยางไรกตามทมการรกษาอาจเลอก total thyroidectomy เพVอรกษาดวย RAI ตอไดและสามารถตดตามโรคได ซV งขFนอยกบผปวยและลกษณะของโรค
c. สาหรบผปวยมะเรงไทรอยดทVมขนาด < 1 cmทVไมม extrathyroidal extension หรอ metastatic lymph nodes การรกษาเรVมตนคอ การทา lobectomyถาไมมขอบงชFของการผาตด contralateral lobe ชดเจน ซV งการทา lobectomy เพยงพอใน small, unifocal, intrathyroidal carcinoma ในผปวยทVไมเคยฉายแสงทVศรษะและคอหรอไมม familial thyroid carcinoma
การเลอกวธการผาตดนFน ขFนอยกบHigh risk features ไดแก cN1, RLN involvement, grossly invasive
disease, experienced surgeons และ complication rates แนวทางการรกษาในอดต แนะนาการทา total thyroidectomy เปนการรกษาหลกในผปวยทVเปน DTC > 1
cm แมวาจะมหรอไมม loco-regional หรอ distant metastases(21)ซV งจาก retrospective data พบวาการทา bilateral surgical procedure จะเพVมอตราการรอดชวต, ลดอตราการกลบเปนซF า, งายตอการใช RAI remnant ablation และสามารถตดตามการกลบเปนซF า/persistent ของโรคไดงาย(22) อยางไรกตาม ขอมลในปจจบนพบวา ถาเลอกผปวยทV

Surgical management in differentiated thyroid cancer
7
เหมาะสม การผาตดแบบ unilateral หรอ bilateral thyroid surgery มผลลพธเหมอนกน(23-25)นอกจากนF เนVองจากการใช RAI ablation เปนอกหนVงเหตผลของการสนบสนนการทา total thyroidectomy ใน low to intermediate risk แตในปจจบน การเลอกให RAI ablation อาจพจารณาในบางรายและบางรายไมจาเปนตองไดรบ RAI ablation ตอ ซV งเปรยบเทยบกบการทVผปวยเหลอเนFอไทรอยดปกตไวซV งลด ความจาเปนของ exogenous thyroid hormone ได นอกจากนF การตดตามโรคหลงจากการผาตดลดการใช whole body RAI scanning มาเปนการทา neck ultrasound และวด serum Tg level กนมากขFน ในการศกษาผปวย PTC 52,173 คน ระหวางป 1985-1998 จาก National Cancer Data Base (43,227 คนไดรบการทา total thyroidectomy, 8,946 คนไดรบการทา lobectomy)(22)พบวา อตราการรอดชวตทV 10 ปของ total thyroidectomy สงกวา lobectomy เลกนอย (98.4% vs 97.1% ตามลาดบ p<0.05) และอตราการกลบเปนซF าใน 10 ปนอยกวาเลกนอย (7.7% vs. 9.8% ตามลาดบ p<0.05) เมVอวเคราะหถงขนาดของกอนเนFอพบวามความแตกตางอยางมนยสาคญทางสถตในเรVองของการรอดชวตและการกลบเปนซF า เมVอขนาดกอนมากกวา 1 cm อยางไรกตาม ขอมลดาน extrathyroid extension, completeness of resection และ comorbid condition ไมไดนามาวเคราะหวามผลตอการรอดชวตและการกลบเปนซF าซV งพบวาการทา lobectomy จะมผลลพธทVแยกวาซV งอาจเปนจากการทVผปวยทVทา lobectomy ม high risk feature รวมดวย การศกษาของ Haigh และคณะ(24)วเคราะหผปวยทVเปน PTC5,432 คนจาก SEER database (4,612 คนไดรบการทา total thyroidectomy และ 820 คนไดรบการทา lobectomy) ไมพบความแตกตางกนในเรVองของอตราการรอดชวต 10 ประหวาง 2 กลม ซV งพบวาผปวยทVไดรบการทา thyroid lobectomy พบ extrathyroidal extension รอยละ 7, distant metastasis รอยละ 1 และ primary tumor > 5cm รอยละ 5
ขอมลลาสดจากการศกษา 2 การศกษาใน SEER databaseซV งไมพบความแตกตางอยางมนยสาคญทางสถตในเรVองอตราการรอดชวตระหวางการทา total thyroidectomy และ lobectomy(23, 26)การศกษาของ Barney และคณะ(23)ผปวย DTC ทFงหมด 23,605 คน ในป 1983 ถง 2002 ทVทา total thyroidectomy 12,598 คน และ 3,266 คนไดรบการทา lobectomy ไมพบความแตกตางอยางมนยสาคญทางสถตในดานอตราการรอดชวต 10 ป (90.4% ใน total thyroidectomy และ 90.8% ใน lobectomy) นอกเหนอจากนFพบวา อาย, ระยะของโรค, เพศ, ปทVวนจฉยโรค, การให RAI ไมความแตกตางกนใน ดานอตรารอดชวตทFงหมดหรอเฉพาะตวโรคและการศกษาของ Mendelsohn(26)วเคราะหผปวย PTC ทFงหมด 22,724 คน ระหวางป 1998-2001 (16,760 คนรบการผาตด total thyroidectomy และ 5,964 คนรบการผาตด lobectomy) ไมพบความแตกตางกนในทFงสองกลม โดยพบวาผปวยทVทา lobectomy มรอยละ 1.6 ทVไดรบ external beam radiation therapy, รอยละ 16 ม extrathyroidal extension, รอยละ 9 กอนมากกวา 4 cm, รอยละ 20 ไดรบ RAI ablation

Surgical management in differentiated thyroid cancer
8
นอกจากนFผปวยทVเปน PTC มกจะเปน multifocal ซV งจากการศกษาหลายการศกษาพบวา อตราการกลบเปนซF าจะนอยลงเมVอผปวยไดรบการทา total thyroidectomy เทยบกบ lobectomy(5)อยางไรกตาม การเลอกผปวยอยางเหมาะสม local-regional recurrence rate นอยกวารอยละ 1-4 และอตราการทา completion thyroidectomy ตาม thyroid lobectomy นอยกวารอยละ 10(25)นอกจากนFการกลบเปนซF าจะพบเมVอตดตามไปเปนระยะเวลานานและไมมผลตออตราการรอดชวตเพราะฉะนFนการทา lobectomy อาจเหมาะในผปวยทVเปน low to intermediate risk (unifocal tumor < 4cm, ไมม extrathyroidal invasion, ไมมการกระจายไปยงตอมนFาเหลอง) ซV งอตราการกลบเปนซF าคอนขางตVาในผปวยเหลานFผลการรกษา ใกลเคยงกบผปวยทVทา total thyroidectomy แตการทา salvage therapy อาจมประสทธภาพในผปวยทVม การกลบเปนซF าหลงจากการทา lobectomy รวมทFงการทV neck US และการตดตาม serum Tg เพVอดการกลบเปนซF าของโรคมประสทธภาพทVดขFนและการให RAI therapy ในผปวยบางรายเทานFน สามารถลดการทา total thyroidectomy ใน low และ intermediate risk ผปวยได อยางไรกตามการทา near-total หรอ total thyroidectomy จาเปนถาตองไดรบการรกษาหลงผาตดดวย RAI therapy ซV งแนะนาวาตองใหในผปวยทVมขนาดกอน > 4 cm, ม gross extrathyroidal extension หรอม regional หรอ distant metastases
สาหรบกอนขนาด 1-4 cm อาจเลอกไดทFง bilateral thyroidectomy หรอ unilateral procedure ผปวยทVอาย > 45 ป, contralateral thyroid nodule, มประวตฉายแสงทVศรษะและคอ, มประวตครอบครวเปน DTC แนะนาbilateral procedure เพVอวางแผนการให RAItherapy ตอไปและงายตอการตดตาม(25)
ในการศกษาผปวยทVทาการผาตด thyroidectomy โดยเกบขอมลจาก Health Care Utilization Project Nationwide Inpatient Sample (HCUP-NIS) แบงศลยแพทยเปน low (6,072 คนทVทาการผาตด < 10 คน/ป), intermediate (11,544 คนทVทาการผาตด 10-100 คน/ป) และ high volume (4,009 คนทVทาการ ผาตด >100 คน/ป)(27)โดยพบวาศลยแพทยกลม high volume มภาวะแทรกซอนจากการผาตดนอยทVสด รอยละ 7.5 สวน intermediate และ low volume คดเปนรอยละ 13.4 และ 18.9 (p<0.001) ตามลาดบนอกจากนFในกลม high volume thyroid surgeon พบภาวะแทรกซอนรอยละ 7.6 เมVอทา lobectomy แตจะเพVมขFนเปนรอยละ 14.5 ใน total thyroidectomy สวน low volume surgeon พบภาวะแทรกซอนรอยละ 11.8 และ 24.1 ตามลาดบ ดงนFนผปวยควรไดรบการประเมนถงประโยชนและความเสVยงของการทา total thyroidectomy และ thyroid lobectomy แมวาจะไดรบการผาตดโดยhigh volume surgeon
การผาตดเลาะตอมนSาเหลอง
a. การทา Therapeutic central-compartment (level VI) neck dissection ในผปวยทV clinically involved central nodes ควรทา total thyroidectomy รวมกบการผาตด central neck node

Surgical management in differentiated thyroid cancer
b. Prophylactic central-compartment neck dissection clinically involved lateral neck node (cN1b)
c. การทา Thyroidectomy without prophylactic central neck dissection noninvasive, clinically node
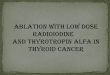
รปทV 2แสดงตาแหนงตอมนFาเหลองบรเวณลาคอ สวนการทา therapeutic lateral neck compartment lymph node dissection
proven metastatic lateral cervical lymphadenopathyการแพรกระจายไปยงตอมนF าเหลองตFงแตตอนวนจฉยพบไดบอยในผปวยทVเปน
carcinoma และพบไดนอยกวาใน follicular carcinomaรายงานวาไมไดมผลลพธทVสาคญในผปวย การม lymph node metastases, อาย รอดชวตอยางมนยสาคญทางสถต(29
metastases เปนรอยละ 82 และเปนรอยละ cervical lymph node metastases เปนปจจยเสVยงของการลดอตราการรอดชวตแตพบในผปวยทVเปน ทVอายมากกวา 45 ปเทานFน(30)แตในขอมลลาสดจาก เสVยงของการเสยชวตอยางมนยสาคญทางสถตmetastatic lymph nodes ตFงแต 6 ตอมขFนไปจะเพVมอตราการเสยชวตmetastases กอนผาตดเพVอการประเมนและพยากรณโรคไดแมนยา
agement in differentiated thyroid cancer
compartment neck dissection ควรทาในผปวยทVเปน PTC with T3 clinically involved lateral neck node (cN1b) หรอเพVอขอมลการวางแผนตอไป
Thyroidectomy without prophylactic central neck dissection เหมาะสมในผปวยทVเปน noninvasive, clinically node-negative PTC (cN0) และ most follicular cancer
แสดงตาแหนงตอมนFาเหลองบรเวณลาคอ
therapeutic lateral neck compartment lymph node dissection ควรทาในผปวยทVเปน proven metastatic lateral cervical lymphadenopathy
การแพรกระจายไปยงตอมนF าเหลองตFงแตตอนวนจฉยพบไดบอยในผปวยทVเปน follicular carcinoma(28)แมวาการพบการกระจายไปยงตอมนFา
ทVสาคญในผปวย low risk แตการศกษาใน SEER database ในผปวย อาย > 45 ป, distant metastases และกอนเนFองอกใหญเปนตวบงชF เกVยวกบอตราการ
29)นอกจากนFอตราการรอดชวตทV 14 ปของผปวยทVเปน และเปนรอยละ 79 ถาม nodal metastases (p<0.05) จากการศกษา
เปนปจจยเสVยงของการลดอตราการรอดชวตแตพบในผปวยทVเปน แตในขอมลลาสดจาก National Cancer Data Base และ SEER
งมนยสาคญทางสถตในผปวยทVม lymph node metastasis ทVอายนอยกวา ตอมขFนไปจะเพVมอตราการเสยชวต(31)ซV งการศกษานF เนนการตรวจ
เพVอการประเมนและพยากรณโรคไดแมนยา
9
PTC with T3 or T4, cN0 หรอหรอเพVอขอมลการวางแผนตอไป
เหมาะสมในผปวยทVเปน T1 or T2, cancer
ควรทาในผปวยทVเปน biopsy-
การแพรกระจายไปยงตอมนF าเหลองตFงแตตอนวนจฉยพบไดบอยในผปวยทVเปน papillary thyroid แมวาการพบการกระจายไปยงตอมนFาเหลองใน PTC
ในผปวย PTC 9,904 คน พบวา และกอนเนFองอกใหญเปนตวบงชF เกVยวกบอตราการ
ปของผปวยทVเปน PTC without lymph node จากการศกษา SEER สรปวา การม
เปนปจจยเสVยงของการลดอตราการรอดชวตแตพบในผปวยทVเปน FTC และ PTC SEER พบวามการเพVมความ
ทVอายนอยกวา 45 ปและการทVม ซV งการศกษานF เนนการตรวจ nodal

Surgical management in differentiated thyroid cancer
10
ตาแหนงของตอมนFาเหลองทVคอมกพบการกระจายไปยง central neck (VI) การทา therapeutic lymph node dissection แนะนาใหทาใน cN1 เทานFน อยางไรกตาม การทา prophylactic level VI neck dissection ใน cN0 ยงไมมขอบงชFชดเจน ซV งในเรVองของการทา prophylactic dissection วาสามารถเพVม disease-specific survival, ลด local recurrence และ post treatment Tg level ได ยงมขอมลทVจากด(32)
การทา prophylactic central neck dissection อาจใชเพVอเปนขอมลในการใช adjuvant RAI(17, 32)และเพVมความแมนยาในการประเมนความเสVยงขอการกลบเปนซF าอยางไรกตามหลายการศกษา ไมพบวาการทา prophylactic dissection จะเพVม long term outcome ขณะทVเพVมความเสVยงของการเกด temporary hypocalcaemiaแมวาprophylactic dissection อาจจะลดความจาเปนของการให RAI(33)
สาหรบเหตผลของการเลอกวาจะทา prophylactic dissection หรอไมอาจตองดปจจยของความเสVยงในการเกด metastasis หรอ recurrence (older or very young age, larger tumor size, multifocal disease, extrathyroidal extension, known lateral node metastases) หรออกกลมคอ ผปวยทVไดรบการทา bilateral thyroidectomy แลวการทา nodal staging เพVอขอมลในการให adjuvant therapy ตอไป(34) ซV งการใชขอมลจากการทา prophylactic central neck dissection ตองระวงในการแปลระยะของโรค ซV งมกพบ microscopic nodal positivity ไดบอย ซV งจะเพVมระยะของโรคจาก cN0 เปน pN1a และเพVมจากระยะทV 1 เปนระยะทV 3 ในผปวยทVอายมากกวา 45 ป(32) อยางไรกตามการพบ microscopic nodal positivity ไมเพVมความเสVยงของการกลบเปนซF าเทากบ macroscopic disease ซV งการเพVมระยะของโรคอาจนาไปสการให RAI ทVเกนความจาเปน(35)
การศกษาพบวา การมBRAFV600E mutation มความสมพนธกบการม nodal disease(36)แตการพบ BRAFV600Emutation ยงมขอจากดในการบอกการกลบเปนซF าและยงไมมผลตอการตดสนใจในการทา prophylactic central neck dissection
ตอมนFาเหลองทV lateral neck (II-V), level VII (anterior mediastinum) และ level I (rarely) อาจจะมการแพรกระจายจากมะเรงไทรอยดไดสาหรบผปวยทVม nodal disease จากการ peroperative US และไดรบการทา nodal FNA cytology หรอ Tg washout แลวการผาตดโดยการทา compartmental node dissection อาจจะลดความเสVยงของการกลบเปนซF าและการเสยชวต(37) การทา completion thyroidectomy(11)
a. การทา completion thyroidectomy แนะนาใหทาในผปวยทกรายทVมขอบงชFของการทา bilateral thyroidectomy และทาtherapeutic central neck lymph node dissection ถาตอมนFาเหลองคอโต
b. ไมแนะนาการทา RAI ablation ในเพVอทดแทน completion thyroidectomy การทา completion thyroidectomy จาเปนทVตองทาหลงจากการทา lobectomy ในผปวยเปน indeterminate
ขFนไป ผปวยทVเปน multicentric disease และตองไดรบ RAI ตอจากการผาตดตองไดรบการทา completion

Surgical management in differentiated thyroid cancer
11
thyroidectomy อยางไรกตามเนVองจาก intrathyroid PTC หรอ low-risk FTC สามารถรกษาโดยการทา lobectomy ได โดยไมจาเปนตองทา completion thyroidectomy ความเสVยงของกาผาตด two stage thyroidectomy (lobectomy แลวตามดวย completion thyroidectomy) เทากบการทา near-total หรอ total thyroidectomy(38) Intraoperative voice and parathyroid management
a. Visual identification of RLN during dissection and external branch of superior laryngeal nerve b. Intraoperative neural stimulation อาจจะพจารณา c. ตอมพาราไทรอยดและหลอดเลอดทVมาเลFยงควรจะรกษาไวระหวางการผาตด อตราการบาดเจบตอ RLN จะตVาเมVอมการหา RLN เมVอเทยบกบการทVไมสามารถหาRLN ไดสวนEBSLN
ควรจะรกษาไวแตถาไมสามารถหาได ควรจะหลกเลVยงการบาดเจบตอ EBSLN โดยการผาตดใหใกล thyroid capsule ทV superior pole และใกลกบเสนเลอดบรเวณนFนใหมากทVสด
สาหรบการใช intraoperative nerve monitoring ชวยทาใหการผาตดทาไดงายขFน(15)การศกษาพบวาการมหรอไมม intraoperative nerve monitoring ใหผลลพธไมแตกตางกนจาก systematic meta-analysis จาก 20 RCT พบวา ไมความแตกตางอยางมนยสาคญทางสถตในเรVองประโยชนของ intraoperative neuromonitoring เมVอเปรยบเทยบกบการหาเสนประสาทได ไมวาจะเปนดานผลลพธ, การบาดเจบตอ RLN ทFงชVวคราวและถาวร(39)หลายการศกษาพบวา intraoperative nerve monitoring มกถกใชโดย higher volume surgeons ทVจะชวยในการผาตดและพบวาทาใหอตราของ nerve paralysis ดขFนเมVอใชในการผาตดทVเปน reoperation หรอมความซบซอน การทา neural stimulation ในผปวยทVตองทา completion of lobectomy สามารถทดสอบเพVอความปลอดภยระหวางการทาcontralateral surgery และหลกเลVยงการเกด bilateral vocal cord paralysis(40)
โดยปกตแลว การรกษาตอมพาราไทรอยดสามารถทาโดยการผาตดอยางระมดระวงในการหาตอม พาราไทรอยด(41)ถาไมสามารถระบตาแหนงของตอมพาราไทรอยดได ศลยแพทยควรจะพยายามเลาะ thyroid capsule และผก inferior thyroid artery ใหใกลกบ thyroid มากทVสด เนVองจากตอมพาราไทรอยด รบเลอดมาจาก inferior thyroid artery แตถาเกดหลกเลVยงไมไดทVจะตองเอาตอมพาราไทรอยดออก เชน เปน intrathyroidal หรอถกตดออกระหวางเลาะตอมนFาเหลองทVคอหรอขาดเลอด ควรสงยนยนวา ไมมมะเรงทVตอมพาราไทรอยดกอนการทาauto transplantationเขาสกลามเนFอstrap หรอกลามเนFอsternocleidomastoidและมความสาคญในการดชFนเนFอ thyroidectomy และตอมนFาเหลองทVคอเมVอผาตดเสรจและกอนนาสงเพVอตรวจทางพยาธวทยาวามตอมพาราไทรอยดอยดวยหรอไม

Surgical management in differentiated thyroid cancer
12
3. Postoperative care
ถามเสยงทVผดปกตควรไดรบการตรวจ laryngeal examinationการประเมนเสยงควรทาหลงการผาตดและขFนอยกบการประเมนของผปวยและแพทย โดยปกตแลวการประเมนสามารถทาไดตFงแต 2 สปดาหถง 2 เดอนหลงจากการผาตด การตรวจพบความผดปกตของการเคลVอนไหวของเสนเสยงตองไดรบการรกษาทนทซV งมผลตอผลลพธทVดและลดโอกาสของการทา open thyroplasty repair โดยการทา laryngeal exam สาหรบการรกษา RLN paralysis มหลากหลาย เชน การทา voice therapy, vocal cord injection หรอ open vocal cord medicalization(42)
บทสรป มะเรงไทรอยดชนด PTC และ FTC เปนชนดทVพบไดเปนสวนใหญของมะเรงไทรอยด โดยการผาตดถอเปนวธหลกในการรกษา สาหรบแนวทางในการดแลรกษาทVเกVยวของกบการผาตด ทFงกอน ระหวางและหลงผาตด โดยยดตามระดบความนาเชVอถอของหลกฐานและคาแนะนาตาม ATA 2015 สามารถสรปไดดงตารางทV 1 และ 2 ตารางทU 1 การแปลผลระดบคาแนะนาและการนาไปใช(11)
คาแนะนา หลกฐานสนนสนน การแปลผล
Strong recommendation
High-quality evidence Moderate-quality evidence Low-quality evidence
RCT without important limitations or overwhelming evidence from observational studies RCT with important limitations or strong evidence from observational studies Observational studies/case studies
Can apply to most patients in most circumstances without reservation Can apply to most patients in most circumstances without reservation May change when higher-quality evidence becomes available
Weak recommendation
High-quality evidence Moderate-quality evidence
RCT without important limitations or overwhelming evidence from observational studies RCT with important limitationsor strong evidence
Best action may differ based on circumstances or patients’ values Best action may differ based on circumstances or patients’ values

Surgical management in differentiated thyroid cancer
13
Low-quality evidence
from observational studies Observational studies/case studies
Other alternatives may be equally reasonable
Insufficient Evidence is conflicting, of poor quality, or lacking
Insufficient evidence to recommend for or against
ตารางทU 2 สรปคาแนะนาของ ATA 2015 ในการผาตดรกษาผปวย differentiated thyroid cancer(11)
คาแนะนา Level of recommendation
Level of evidence
Preoperative management
Preoperative investigation 1. อลตราซาวดทVคอ
(A) การทาอลตราซาวดทVคอกอนการผาตดเพVอประเมน ตอมนFาเหลองทVคอ (central and especially lateral neck compartments) แนะนาใหทาในผปวยทกรายทVตองทา thyroidectomy ทVมผลทางเซลลวทยาหรอ molecular ทVเปนมะเรงหรอสงสยมะเรง (B) การทา US-guided FNAของตอมนFาเหลองแนะนาในผปวยทVมลกษณะอลตราซาวดสงสยทVมขนาดตFงแต 8-10 มลลเมตร เพVอยนยนวาเปนมะเรงหรอไม (C) สาหรบการตรวจ FNA-Tg washout ของตอมนFาเหลองทVคอเหมาะสมในผปวยบางรายแตการแปลผลอาจจะทาไดยากในผปวยทVกอนตดกบตอมไทรอยด
2. การทา cross-sectional imaging studies (CT, MRI) with intravenous (IV) contrast แนะนาเปนการตรวจเพVมเตมจากอลตราซาวดสาหรบผปวยทVสงสย advanced disease ไดแก invasive primary tumor หรอมตอมนFาเหลองทVคอโต
3. การทา Routine preoperative 18FDG-PET scanning ไมแนะนา
Strong
Strong
Weak
Strong
Strong
Moderate-
quality
Moderate-
quality
Low-quality
Low-quality
Low-quality

Surgical management in differentiated thyroid cancer
14
4. การตรวจ Routine preoperative measurement of serum Tg or anti-Tg antibodies ไมแนะนา
Preoperative care communication 1. กอนการผาตด ศลยแพทยควรจะอธบายถงความเสVยงของการ ผาตดในการบาดเจบตอเสนประสาทและตอมพาราไทรอยดแกผปวยรวมทFงการอนญาตการผาตดรวมทFงการสVอสารกบวสญญแพทยและความผดปกตทVตรวจพบกอนการผาตด
Preoperative voice assessment 1. ผปวยทFงหมดทVเขารบการผาตดไทรอยดควรจะมการประเมน เสยงกอนการผาตดโดยการใหผปวยบอกการเปลVยนแปลงของ เสยงรวมกบการประเมนของแพทยรวมดวย
2. การ laryngeal exam กอนการผาตดควรทาในผปวยดงตอไปนF
(A) ความผดปกตของเสยงกอนการผาตด (B) มประวตการผาตดทVบรเวณคอหรอหนาอกชวงบนทVม ความเสVยงตอการบาดเจบของ Recurrent laryngeal nerve (RLN) หรอ vagus nerve (C) มะเรงไทรอยดทVม posterior extrathyroidal extension หรอม extensive central nodal metastases
Weak
Strong
Strong
Strong
Strong
Strong
Low-quality
Moderate-
quality
Moderate-
quality
Moderate
Moderate-
quality
Low-quality
Intraoperative management
แนวทางรกษาเมVอผลชFนเนFอเปน follicular cell–derived malignancy 1. สาหรบผปวยทVเปนมะเรงไทรอยดขนาด > 4 cm, gross
extrathyroidal extension (cT4), clinically apparent metastatic disease to nodes (cN1), distant sites (cM1) การผาตดทVแนะนา คอ near-total หรอ total thyroidectomyโดยทV gross primary tumor ออก ถาไมมขอหามของการผาตด
2. สาหรบผปวยทVเปนมะเรงไทรอยดขนาด 1 cm และ<4 cm โดยทVไมม extrathyroidal extension และไมกระจายไป ตอมนFาเหลอง (cN0) การผาตดทVแนะนาสามารถทาไดทFงbilateral
Strong
Strong
Moderate-
quality
Moderate-
quality

Surgical management in differentiated thyroid cancer
15
procedure (near total or total thyroidectomy) หรอ unilateral procedure (lobectomy)การทา Thyroid lobectomy อาจจะเพยงพอสาหรบ low-risk papillary and follicular carcinomas อยางไรกตามอาจเลอกเปน total thyroidectomyซVงสามารถให RAI therapy หรอเพVมการตดตามโรคได ซV งทFงหมดนFขFนกบตวโรคและความตองการของผปวย
3. ถาการผาตดถกเลอกสาหรบผปวยทVเปนมะเรงไทรอยด<1 cm โดยไมม extrathyroidal extension และ cN0 การผาตดทVแนะนา คอ lobectomy ถาไมมขอบงชF ทVชดเจนของการผาตด contralateral lobe การผาตด Thyroid lobectomyเปนการรกษาทVเหมาะสมกบ small, unifocal, intrathyroidal carcinomasทVไมเคยฉายแสงทVศรษะและคอมากอน, ไมเปน familial thyroid carcinoma หรอไมมตอมนFาเหลองทVคอ
การผาตดเลาะตอมนFาเหลองทVคอ 1. Central neck
(A) Therapeutic central-compartment (level VI) neck dissection แนะนาในผปวยทVมกอนตอมนFาเหลองทV central neck โต รวมกบ total thyroidectomy เพVอกาจดโรคจาก central neck (B) Prophylactic central-compartment neck dissection (Ipsilateral or bilateral) ควรพจารณาในผปวยทVเปน Papillary thyroid carcinoma ทVไมม central neck lymph nodes (cN0) ทV primary tumorsเปน T3 or T4 หรอตรวจพบวาม Lateral neck nodes (cN1b) หรอเพVมเปนขอมลทVนาไปใชเพVอ วางแผนการรกษาตอ (C) Thyroidectomy without prophylactic central neck Dissection เหมาะสมสาหรบ small (T1 or T2), noninvasive, clinically node-negative PTC (cN0) และ most
Strong
Strong
Weak
Strong
Moderate-
quality
Moderate-
quality
Low-quality
Moderate-
quality

Surgical management in differentiated thyroid cancer
16
Follicular cancers 2. Therapeutic lateral neck compartmental lymph node
dissection ควรทาในผปวยทVมผลชFนเนFอพสจนวาเปน metastatic lateral cervical lymphadenopathy
Completion thyroidectomy (A) Completion thyroidectomyควรจะแนะนาใหผปวยทVควร ไดรบการทา bilateral thyroidectomy ตFงแตการเรVมตนรกษา สวนการทาTherapeutic central neck lymph node dissectionควรจะทาดวยถามตอมนFาเหลองโต การทา thyroid lobetomy อาจเพยงพอสาหรบlow-risk papillary/follicular carcinoma (B) การให RAI ablation เพVอแทนการทา completion thyroidectomy ไมแนะนา อยางไรกตามอาจจะใชทาลายเนFอเยVอในผปวยบางรายได
Intraoperative voice and parathyroid management 1. เสนประสาท
(A) การทVสามารถระบ RLN ไดดวยการมองเหนระหวาง การผาตดจาเปนตองทาในผปวยทกราย นอกจากนFควรจะ รกษา external branch of the superior laryngeal nerve (EBSLN) ระหวางการผาตดบรเวณ superior pole ของตอมไทรอยด (B) Intraoperative neural stimulation (with or without monitoring) อาจจะชวยในการระบเสนประสาทและยนยน การทางานของเสนประสาท
2.ตอมพาราไทรอยดและเสนเลอดทVมาเลFยงควรจะรกษาระหวาง การผาตดไทรอยด
Strong
Strong
Weak
Strong
Weak
Strong
Moderate-
quality
Moderate-
quality
Low-quality
Moderate-
quality
Low-quality
Moderate-
quality
Postoperative management
1. ผปวยควรมการประเมนเสยงหลงการผาตด สวนการทา laryngeal exam ควรทาถาเสยงผดปกต
2. รายละเอยดและการดแลหลงการผาตดควรจะอธบายใหแกผปวยและผทVเกVยวของในการดแลผปวยหลงการผาตด
Strong
Strong
Moderate-
quality
Low-quality

Surgical management in differentiated thyroid cancer
17
References
1. Ferlay J SI, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray, F. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. International Agency for Research on Cancer. 2013.
2. Howlader N NA, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2012, based on November 2014 SEER data submission, posted to the SEER web site, April 2015. Bethesda, MD. National Cancer Institute. 2015.
3. W. Imsamran AC, S. Wiangnon, D. Pongnikorn, K. Suwanrungrung, S. Sangrajrang RB. Cancer in Thailand 2010-2012. National Cancer Institute Thailand. 2015;8:76.
4. Prechawittayakul P. Hospital-based tumor registry Songklanagarind hospital annual report 2014 Faculty of medicine, Prince of Songkla University2016 [cited 2016]. Available from: http://medinfo2.psu.ac.th/cancer/data/tumor_registry_2014.pdf.
5. Grebe SK HI. Thyroid cancer nodal metastases: biologic significance and therapeutic considerations. Surg Oncol Clin N Am. 1996;5:43-63.
6. Qubain SW NS, Baba M, Takao S, Aikou T Distribution of lymph node micrometastasis in pN0 well-differentiated thyroid carcinoma. Surgery. 2002;131:249-56.
7. Kuna SK BI, Tesic V, Kuna K, Herceg GH, Dodig D Ultrasonographic differentiation of benign from malignant neck lymphadenopathy in thyroid cancer. J Ultrasound Med 2006;25:1531-7.
8. Pak K SS, Hong H, Cheon GJ, Hahn SK, Kang KW, Kim EE, Lee DS, Chung JK Diagnostic values of thyroglobulin measurement in fine-needle aspiration of lymph nodes in patients with thyroid cancer. Endocrine. 2015;49:70-7.
9. Padovani RP KT, Nakabashi CC, Camacho CP, Andreoni DM, Malouf EZ, Marone MM, Maciel RM, Biscolla RP One month is sufficient for urinary iodine to return to its baseline value after the use of water-soluble iodinated contrast agents in post- thyroidectomy patients requiring radioiodine therapy. Thyroid. 2012;22:926-30.
10. McLeod DS CD, Ladenson PW, Ain KB, Brierley JD, Fein HG, Haugen BR, Jonklaas J, Magner J, Ross DS, Skarulis MC, Steward DL, Maxon HR, Sherman SI. Prognosis of differentiated thyroid cancer in relation to serum thyrotropin and thyroglobulin antibody status at time of diagnosis. Thyroid 2014;24(35-42).

Surgical management in differentiated thyroid cancer
18
11. Bryan R. Haugen EKA, Keith C. Bible,Gerard M. Doherty, Susan J. Mandel. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1-92.
12. Roh JL YY, Park CI. Recurrent laryngeal nerve paralysis in patients with papillary thyroid carcinomas: evaluation and management of resulting vocal dysfunction. am J Surg. 2009;197:459-65.
13. Cheng SP LJ, Liu TP, Lee KS, Liu CL Pre-operative ultrasonography assessment of vocal cord movement during thyroid and parathyroid surgery. World J Surg. 2012;36:2509-15.
14. Shindo ML CS, Kandil E, McCaffrey JC, Orloff L, Porterfield JR, Randolph G, Shaha A, Shin J, Terris D Management of invasive well-differentiated thyroid cancer an American Head and Neck Society consensus statement. Head Neck. 2014;36:1379-90.
15. Rosenthal LH BM, Deeb RH. Vocal fold immobility: a longitudinal analysis of etiology over 20 years. Laryngoscope. 2007;117:1864-70.
16. Robert I. Haddad WML, Lindsay Bischoff, Naifa Lamki Busaidy. Thyroid carcinoma. NCCN clinical practice guideline in oncology. 2016;1.
17. Wang TS DS, Sznyter LA, Heller KS Incidence of metastatic well-differentiated thyroid cancer in cervical lymph nodes. Arch Otolaryngol Head Neck Surg 2004;130:110-3.
18. Cooper DS SB, Ho M, Sperling M, Ladenson PW, Ross DS, Ain KB, Bigos ST, Brierley JD, Haugen BR, Klein I, Robbins J, Sherman SI, Taylor T, Maxon HR III Thyrotropin suppression and disease progression in patients with differentiated thyroid cancer: results from the National Thyroid Cancer Treatment Cooperative Registry. Thyroid. 1998;8:737-44.
19. Lin JD CT, Huang MJ, Weng HF, Tzen KY Use of radioactive iodine for thyroid remnant ablation in well-differentiated thyroid carcinoma to replace thyroid reoperation. Am J Clin Oncol. 1998;21:77-81.
20. Brierley JD PT, Tsang RW, Gospodarowicz MK, O’Sullivan B A comparison of different staging systems predictability of patient outcome. Thyroid carcinoma as an example. Cancer. 1997;79:2414-23.
21. Cooper DS DG, Haugen BR. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167-214.
22. Bilimoria KY BD, Ko CY, et al. Extent of surgery affects survival for papillary thyroid cancer. Ann Surg. 2007;246:375-81.

Surgical management in differentiated thyroid cancer
19
23. Barney BM HY, Sharma P, Shrieve DC, Tward JD Overall and cause-specific survival for patients undergoing lobectomy, near-total, or total thyroidectomy for differentiated thyroid cancer. Head Neck. 2011;33:645-9.
24. Haigh PI UD, Rotstein LE. Extent of thyroidectomy is not a major determinant of survival in low- or high-risk papillary thyroid cancer. Ann Surg Oncol 2005;12:81-9.
25. Nixon IJ GI, Patel SG, Palmer FL, Whitcher MM, Tuttle RM, Shaha A, Shah JP Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. Surgery. 2012;151:571-9.
26. Mendelsohn AH ED, Abemayor E, St John MA Surgery for papillary thyroid carcinoma: is lobectomy enough? Arch Otolaryngol Head Neck Surg. 2010;136:1055-61.
27. Kandil E NS, Abbas A, Tufano RP. The impact of surgical volume on patient outcomes following thyroid surgery. Surgery. 2013;154:1346-52.
28. Hughes DT WM, Miller BS, Gauger PG, Burney RE, Doherty GM. Influence of prophylactic central lymph node dissection on postoperative thyroglobulin levels and radioiodine treatment in papillary thyroid cancer. Surgery. 2010;148:1100-6.
29. Podnos YD SD, Wagman LD, Ellenhorn JD The implication of lymph node metastasis on survival in patients with well-differentiated thyroid cancer. Am Surg. 2005;71:731-4.
30. Zaydfudim V FI, Griffin MR, Phay JE . Surgery 144:1070–1077. The impact of lymph node involvement on survival in patients with papillary and follicular thyroid carcinoma. Surgery. 2008;144:1070-7.
31. Adam MA PJ, Goffredo P, Dinan MA, Reed SD, Scheri RP, Hyslop T, Roman SA, Sosa JA. Presence and number of lymph node metastases are associated with compromised survival for patients younger than age 45 years with papillary thyroid cancer. J Clin Oncol. 2015;33:2370-5.
32. Hartl DM ME, Borget I, Leboulleux S, Mirghani H, Schlumberger M Influence of prophylactic neck dissection on rate of retreatment for papillary thyroid carcinoma. World J Surg 2013;37:1951-8.
33. Viola D MG, Valerio L, Molinaro E, Agate L, Faviana P, Seccia V, Sensi E, Romei C, Piaggi P, Tor- regrossa L, Sellari-Franceschini S, Basolo F, Vitti P, Elisei R, Miccoli P. Prophylactic central compartment lymph node dissection in papillary thyroid carcinoma: clinical implications derived from the first prospective randomized controlled single institution study. J Clin Endocrinol Metab. 2015;100:1316-24.

Surgical management in differentiated thyroid cancer
20
34. Laird AM GP, Miller BS, Doherty GM Evaluation of postoperative radioactive iodine scans in patients who underwent prophylactic central lymph node dissection. World J Surg. 2012;36:1268-73.
35. Randolph GW DQ, Heller KS, et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid. 2012;18:170-2.
36. Kim TH PY, Lim JA, Ahn HY, Lee EK, Lee YJ, Kim KW, Hahn SK, Youn YK, Kim KH, Cho BY, Park do J The association of the BRAF(V600E) mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer: a meta-analysis. Cancer. 2012;118:1764-73.
37. Ito Y MA, Inoue H, et al. . An observational trial for papillary thyroid microcarcinoma in Japanese patients. . World J Surg 2010;34:28-35.
38. Untch BR PF, Ganly I, Patel SG, Michael TR, Shah JP, Shaha AA Oncologic outcomes after completion thyroidectomy for patients with well- differentiated thyroid carcinoma. Ann Surg Oncol. 2014;21:1374-8.
39. Pisanu A PG, Podda M, Cois A, Uccheddu A Systematic review with meta-analysis of studies comparing intraoperative neuromonitoring of recurrent laryngeal nerves versus visualization alone during thyroidectomy. J Surg Res. 2014;188:152-61.
40. Musholt TJ CT, Dralle H, Frilling A, Goretzki PE, Hermann MM, Kussmann J, Lorenz K, Nies C, Schab- ram J, Schabram P, Scheuba C, Simon D, Steinmuller T, Trupka AW, Wahl RA, Zielke A, Bockisch A, Karges W, Luster M, Schmid KW. German Association of Endocrine Surgeons practice guidelines for the surgical treatment of benign thyroid disease. Langenbecks Arch Surg. 2011;396:639-49.
41. Randolph GW CO. Principles in thyroid surgery. In: Randolph GW (ed) Surgery of the Thyroid and Parathyroid Glands. 2, editor. Philadelphia2013. 273-93 p.
42. Yung KC LI, Courey MS Effect of temporary vocal fold injection medialization on the rate of permanent medialization laryngoplasty in unilateral vocal fold paralysis patients. Laryngoscope. 2011;121:2191-4.