Embed Size (px)
Citation preview

Seminars in Pediatric Surgery (2012) 21, 219-232
Surgical management of portal hypertension in children
Jean de Ville de Goyet, MD, PhD, FRCS, Giuseppe D’Ambrosio, MD,Chiara Grimaldi, MD
From the Department of Paediatric Surgery and Transplantation, Bambino Gesù Children’s Hospital, Rome, Italy.
The management of children with portal hypertension has dramatically changed during the past decade,with an improvement in outcome. This has been achieved by improved efficiency of endoscopic varicealcontrol and the success of liver transplantation. Emergency surgical shunt procedures are rarely required,with acute bleeding episodes generally controlled endoscopically or, occasionally in adults, by interventionalradiological procedures. Portosystemic shunts may be considered as a bridge to transplant in adults but arerarely used in this context in children. Nontransplant surgery or radiological interventions may still beindicated for noncirrhotic portal hypertension when the primary cause can be cured and to allow normal-ization of portal pressure before liver parenchyma is damaged by chronic secondary changes in some specificdiseases. The meso-Rex bypass shunt is used widely but is limited to those with a favorable anatomy andcan even be performed preemptively. Elective portosystemic shunt surgery is reserved for failure to respondto conservative management in the absence of alternative therapies.© 2012 Elsevier Inc. All rights reserved.
KEYWORDSPortal hypertension;Portosystemic shunts;Liver transplantation;Meso-Rex bypass
hbt
it
Normal portal venous pressure is slightly above that ofthe inferior vena cava and ranges from 0 to 11 mm Hg inphysiological conditions.1-3 The pressure gradient betweenboth venous systems is �10 mm Hg and is low because ofthe high compliance and low resistance of the portal veinand sinusoids and the outflow of the large hepatic veins.There is also a negative pump effect resulting from directdrainage into the right atrium and its location at the thora-coabdominal interface with its alternating positive abdom-inal and negative thoracic pressures.
Portal hypertension (PHT) can be defined as pressurethat is higher than normal values, but is rarely measureddirectly. As such, it is usually defined by observation of aseries of pathological changes and complications, such assplenomegaly and hypersplenism, variceal development,portal gastropathy, and accompanying observations of cir-
Address reprint requests and correspondence: Jean de Ville deGoyet, MD, PhD, FRCS, Department of Paediatric Surgery and Transplan-tation Center, Bambino Gesù Children’s Hospital, Piazza San Onofrio 4,00165 Rome, Italy.
cE-mail: [email protected].
1055-8586/$ -see front matter © 2012 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1053/j.sempedsurg.2012.05.005
rhotic changes at ultrasonography, and, even more rarely,the clinical signs of portopulmonary syndromes.
Classification of PHT
PHT can be categorized on the basis of anatomical level ofvascular resistance and histology of liver parenchyma into 3main categories (Table 1) (Figures 1-3).3-5 Arterioportalypertension has a somewhat different mechanism and wille considered now as a separate entity before returning tohe more common causes listed.
Arterioportal hypertension
This is caused by excessive unconstrained arterial inflowinto the portal venous system—a closed vascular systemlimited by volume with a single outflow.6,7 Typically, theres an arterioportal fistula (APF) from a vascular malforma-ion located within the splanchnic area or the liver. The APF
an be “simple,” with a single feeding vessel, or “complex,”
220 Seminars in Pediatric Surgery, Vol 21, No 3, August 2012
involving multiple arteries ending in a common venouschannel or aneurysm (Figures 2 and 3). Although the liverparenchyma is normal initially, it changes with venousbarotrauma and capillaries becoming fibrotic with thicken-ing of the intima. At that point, PHT can be regarded asmixed, with a combination of both increased flow and re-sistance. Managing these patients can be challenging, asthey may ultimately need liver transplantation, which inturn can be compromised because of the damaged wall andreduced flow from the portal vein.
This straightforward classification of PHT plays a keyrole in determination of the correct treatment protocol.
Table 1 Classification of portal hypertension
PrehepaticThrombosis of the portal vein and cavernomatous
transformation (Figure 1)Hepatic
Presinusoidal—due to hepatic fibrosis, for example,schistosomiasis
Sinusoidal—due to cirrhosis, eg, biliary atresia,posthepatitis, etc
Postsinusoidal—eg, venoocclusive diseasePosthepatic, eg, Budd–Chiari syndromeArterioportal hypertension (Figures 2 and 3)
SimpleComplex
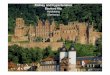
Figure 1 Thrombosis of the portal vein and cavernoma: exam
hepatis.Those who have a relatively normal parenchyma and nor-mal hepatic function will have a different surgical strategycompared with those who have severe parenchymal changesand hepatic dysfunction. Nonetheless, secondary damageand parenchymal fibrosis can develop rapidly in patientswith postsinusoidal PHT (groups 2c and 3) and arterioportalhypertension (group 4), and more slowly in those withpresinusoidal PHT (group 2a). Portal biliopathy changesand secondary biliary cirrhosis can even be seen in patientswith portal vein thrombosis and cavernomatous transforma-tion (group 1). Thus, the distinction between “cirrhotic” and“noncirrhotic” PHT may be evident from the original cause,but it may not always be relevant in terms of managementfor children who are seen at a late stage or who are managedconservatively for too long a period.
Therefore, the surgeon should consider not only the etiol-ogy but also the secondary changes of PHT that have occurredin the parenchyma and how this can affect portal flow, theanatomy of the portal venous system, and the underlying healthof the liver—the hepatic functional reserve.
Strategies for surgery
With prehepatic PHT (group 1), children may have a normalparenchyma and normal liver function for decades, as thereis little, or absent, ongoing damage occurring downstream
owing the variety of cavernomatous transformation of the porta
ples sh
ilrmtid
bccate
(osRv
fi(F
221de Ville de Goyet et al Surgical Management of Portal Hypertension
to the portal blockage.8-10 Such patients may have a patentntrahepatic portal system that is surgically accessible at theevel of the Rex recessus and thus may benefit from aestoration of the continuity of the portal venous system byeso-Rex bypass (MRB)11-18 (Figure 4). We recommend
hat reconstruction is done preemptively when the anatomys favorable, knowing that this can cure the patients’ con-ition and restore normal physiology.18-21 However, chil-
dren with a thrombosed left portal vein within the Rexrecessus who cannot benefit from MRB should be continuedon a conventional endoscopic program and conservativemanagement, as this also provides satisfactory long-termresults by prevention of bleeding.22-26 Such children mightecome candidates for portosystemic shunt surgery whenomplications cannot be managed medically or endoscopi-ally, and our preference is for a “selective” shunt, such asWarren shunt, to preserve some hepatopetal flow through
he cavernoma preserving the hepatotrophic effect of mes-
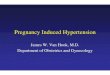
Figure 2 Examples of vascular malformations with arterioportalstulae and portal hypertension (PHT): simple (top) and complexbottom) types (reproduced as drawings 1 and 4, respectively, inigure 3).
nteric blood. Other teams use nonselective H-type shunts
eg, mesocaval and lateral splenorenal) in this scenario andbtain excellent clinical results, possibly because H-typehunts may not cause full diversion of the portal flow.ather, there may be partial diversion by using a longenous interposition graft with a degree of resistance.27-30
We believe that nonshunt surgery should be strictlyavoided, at least as primary surgical therapy, as it has littleeffect on portal pressure and may even seriously worsen thecondition of the abdominal cavity for future surgery.
In PHT groups 2c, 3, and 4, the patient may be amenableto a cure if the diagnosis is made early in the progression ofthe disease, with the liver parenchyma not irreversibly dam-aged. If the liver parenchyma has been irreversibly dam-aged, then patients should be managed as those with cirrho-sis.
Children with venoocclusive disease (group 2c) maybenefit from medical management,31 with resolution of theproblem and normalization of portal pressure and hepaticfunction. Interventional radiology (transjugular intrahepaticportosystemic shunt [TIPSS]) or transplantation is rarelyindicated.
Patients with Budd–Chiari syndrome (group 3) may beamenable to angioplasty and stenting of the hepatic vein andvena cava, which, when combined with anticoagulation,may allow stabilization or recovery of parenchymal damageand normalization of liver function for many years.32 Ulti-mately, there is still a possible need for liver replacement.
Patients with arterioportal hypertension and APF (group4) patients may benefit from embolization if the latter is asimple single tract6,7 (Figures 2 and 3). In more complexarterioportal malformations, radiological interventionsshould be avoided, as they often fail at achieving full devas-cularization and control of the fistula and, more importantly,repeated attempts result in an abnormal arterial network andmay seriously interfere with further surgery. Surgery shouldbe considered if there is either resection of the liver segmentinvolved33 or direct arteriovenous disconnection-devascu-larization (depending on the anatomy).34
Traditionally PHT shunt surgery was reserved for pa-tients in whom the control of variceal bleeding failed ineither the short or long term, with recurrent bleeding epi-sodes. This approach has been relatively successful in adultswith well-compensated cirrhosis. However, in children andespecially in infants, surgery was associated with a rela-tively high rate of anastomotic stricture or thrombosis be-cause of the small diameter of the veins involved. Prolon-gation of a conservative approach, coping medically withrecurrent non–life-threatening bleeding, and postponingsurgery until the child reached adolescence was not anuncommon practice, as it was thought that deferring theshunt procedure led to a higher success rate in the olderadult-sized adolescent. Nowadays, with experience gainedin vascular and transplant surgery and the use of microsur-gical techniques, reasonably good success rates can beachieved even in the smaller age-group by trained teams,
and age should not be a criterion per se for, or indeed
V, live
222 Seminars in Pediatric Surgery, Vol 21, No 3, August 2012
against, shunt surgery.35-43 Although surgeons can nowoffer excellent technical outcomes even in smaller children,the indication for shunt surgery has dropped to very lowfigures, with liver transplantation being offered instead inmany cases.
The choice of shunt procedure itself may vary from teamto team on the basis of the experience of the surgical team.Selective shunts have a relative advantage and should bepreferred in children to preserve them from encephalopathy,although it has been shown that these turn out to be lessselective and more “centralized” with time. Moreover, non-selective H-type shunts do provide excellent clinical results.It is perhaps more important that the surgical team is expertand confident with one technique that in their hands pro-vides good success rates. It is also crucial that a multidis-ciplinary team is involved who can propose a wide range oftherapeutic options (medical, surgical, radiological, andtransplant) to individualize treatment.
Any therapeutic algorithm must take into considerationthe possibility of liver replacement in the medium to longterm. Its use may be jeopardized by previous abdominaloperations and portosystemic shunt surgery. The indications
Figure 3 Schematic representations of vascular malformations w(CA, celiac trunk; CHA, common hepatic artery; LHA, left hepahepatic artery; RPV, right portal vein; L, left portal vein; II-III, -
for shunt surgery in children with chronic liver disease are
few because of the successful results of liver replacement.These may include those with well-compensated disease(Pediatric End-stage Liver Disease [PELD] �10), such asthose with PHT group 2a causes (ie, congenital hepaticfibrosis) and, less commonly, groups 2c and 3, with well-preserved liver function but symptomatic variceal bleed-ing.3,5,23,24,44 Nonsurgical interventional options such asTIPSS may be more appropriate and should be discussedwith the transplant team. This alternative preserves the in-tact abdomen, and stents can be removed at the time oftransplantation. It may even improve the patient’s conditionwhen used as a bridge to transplant by its effect on ascitesand PHT.
Hypersplenism is rarely a major issue in children anddoes not cause clinical concern in most cases, even in thosewith long-lasting PHT and major splenomegaly (Figure 5).Rarely, a selective portosystemic shunt (distal splenorenalshunt or “Warren shunt”) may be used because it providesregional decompression and effective venous drainage ofthe spleen with reduction in size and improvements inthrombocytopenia and leukopenia. Reported results havebeen mixed,36,45,46 and a lot depends on the quality of the
erioportal fistulae and PHT: complex (A-C) and simple (D) typesery; RAHA, right accessory hepatic artery; DHA, diaphragmaticr segments II-III and IV).
ith arttic art
flow through the shunt. The option for isolated splenectomy

s (R,
223de Ville de Goyet et al Surgical Management of Portal Hypertension
must be discussed carefully, and it is rare in clinical prac-tice. It may be indicated for those with recurrent gastroin-testinal bleeding and extensive thrombosis of the portalsystem, including the splenic vein where options for per-forming a portosystemic shunt are few or nil. Portal pressuredoes drop for some time after splenectomy. A further indi-cation, at least in our opinion, is the difficult teenager with
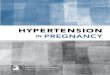
Figure 4 Retrograde portogram (top) and conventional angiogramscan be ignored on standard imaging and best delineated on portogram
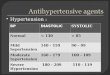
Figure 5 Huge splenomegaly of idiopathic origin in
longstanding prehepatic PHT (group 1) not amenable to anMRB, presenting with huge splenomegaly, who starts re-fusing medical therapy, medical assessments, and having alifestyle that puts him/her at risk of difficult-to-managebleeding either from splenic rupture caused by hazardoussporting practice, or gastrointestinal bleeding far from med-ical support. These patients may benefit from preemptive
m) in 2 patients (left and right) showing that intrahepatic portal veinsRex recessus; RL, Right liver; SMV, superior mesenteric vein).
(botto
a teenager with longstanding extrahepatic PHT.

cnsbd
ficaatatavsca
gbqiglpscrbgsifrtr
224 Seminars in Pediatric Surgery, Vol 21, No 3, August 2012
splenectomy (after an adequate vaccination program), witha central splenorenal shunt being performed at the sameoperation (to avoid loss of the splenic vein by thrombosis)or a spleno-Rex bypass if the left portal vein in the Rexrecessus is patent in a child who was not referred previouslyfor MRB surgery (Figure 5).
In rare cases, the occurrence of a portopulmonary syn-drome (hypoxia and hepatopulmonary syndrome, or pulmo-nary arterial hypertension, as a complication related to PHTand portosystemic shunting) is an indication for liver trans-plantation.47 Again, in a patient with PHT caused by portalavernomatous change, having a patent Rex, and who wasot referred for MRB previously, MRB may also be con-idered to treat Portopulmonary syndrome, as it can resolveoth portal hypertension and the hepato-pulmonary syn-rome.
Assessment of the surgical patient
Preliminary assessment must establish the cause of PHT,hepatic function, and “reserve,” with appropriate histologyand any existing complications of PHT.
Appropriate preoperative assessment includes coagula-tion profile, delineation of the portal venous system, Dopp-ler ultrasonography of the neck.
Coagulation profile
Thrombocytopenia and a slightly prolonged internationalnormalized ratio are common, but other anomalies may beidentified.48-58 These are rarely important for those goingor liver transplantation, as the new liver will correct exist-ng anomalies, but can be important when performing vas-ular nontransplant surgery. Coagulopathy is a risk for intra-nd postoperative hemorrhage, and conversely a hyperco-gulable state can be associated with an increased risk ofhrombosis. Minor changes may be relevant; a deficit inntithrombin III makes the patient insensitive to heparinreatment, and MTHFR-C667T homozygotic children haven increased risk of thrombosis.58 Those with a history ofenous thrombosis (portal vein or otherwise) should becreened to detect the small proportion with a true geneticoagulation disorder and to offer adequate perioperativentithrombotic prophylaxis.
Delineation of the portal venous system (Dopplerultrasonography and contrast-enhanced computedtomography or magnetic resonance angiography)
Correct identification of the anatomy of the major veins isimperative and includes the portal vein, superior mesentericvein, splenic vein, left renal vein, and inferior vena cava.The distance between the splenic vein and left renal vein(for a splenorenal shunt) or between the mesenteric vein and
vena cava (for a mesocaval shunt) can be estimated. Rarely,conventional angiography may be useful, for example, be-fore the surgical approach to a complex arterioportal mal-formation.
Doppler ultrasonography of the neck
This is to confirm patency and caliber of both internaljugular veins if this is being considered for bypass. Mostconsider it as the best available material,28 as it is autolo-ous, grows with the child, and mimics the characteristics ofoth diameter and length of the portal vein, ensuring ade-uate flow and low thrombosis rates (certainly by compar-son with smaller diameter veins such as the saphenous veinraft). Using 1 of the 2 patent internal jugular veins has aow morbidity, which is not the case when iliac veins arerocured or when the vena cava is divided for creation of ahunt (Auvert shunt). The internal jugular vein can be pro-ured as long as 6-8 cm in length and easily matcheselatively long gaps needed in mesocaval and meso-Rexypasses. Neither does it need much in the way of complexraft preparation as, for example, when preparing a spiralaphenous vein graft. In those cases of significant differencen diameter between left and right internal jugular veins,urther assessment of the venous anatomy of the brain isecommended to check whether intracranial left/right anas-omoses are present and, if so, are large. Lack of this is aelative contraindication for procuring 1 vein.
Feasibility of MRB
Wedged hepatic venous portography via the transjugularapproach is safe and efficient where this shunt is beingconsidered59-65 (Figure 4). Patency of the left portal branchand Rex recessus is the key observation to success.59,60
Nowadays, direct percutaneous portography is not recom-mended, as the portal radicals are small in caliber and thechance of opacification is lowered.
Shunt surgery
Portosystemic shunts are nonphysiological routes created todivert the portal and mesenteric blood flow into the systemiccirculation. A variety of techniques are available, and withrelatively simple technical modifications (side-to-side anas-tomosis vs H-type, caliber of the bypass, length of the graft,use of prosthetic material, site of drainage), the surgeon hasplenty of choices for achieving a partial, rather than a full,portal flow diversion. The drop in portal pressure is vari-able, depending on how much flow is diverted,28-30,37 andvaries according to the diameter of the anastomosis, thediameter and length of the interposition graft, and the loca-tion of the site chosen for portal blood diversion.27
Portosystemic shunts may be either “selective” or “non-selective.”23,24 Selective shunts divert selectively a region
of the abdomen, for example, the stomach and spleen, to
tvpm�
dr
tcatosoiHTltsfvcnG
225de Ville de Goyet et al Surgical Management of Portal Hypertension
decompress esophagogastric varices. Blood is predomi-nantly shunted into the low-pressure systemic venous cir-culation, and the varices then flow at a lower pressure withno residual risk of bleeding.
Selective shunts
Distal splenorenal shunt (“Warren” shunt)This involves division of the splenic vein and anasto-
mosing the distal stump into the left renal vein, therebypreserving portal and mesenteric blood flow to theliver.36,45,46,66 However, with the complex collateralizationand networking of the splanchnic venous system, somecommunications always persists, and it has been shown thatthis “selective” shunt progressively “centralizes” with time.This option decreases spleen size, improves hypersplenism,and normalizes platelet and leukocyte counts.36,45,46 Selec-ive shunts have been used with success to treat bleedingarices and hypersplenism and have been shown to reduceostoperative encephalopathy with equivalent long-termortality and rebleeding rates. Long-term patency rates90% have been reported.
Nonselective shunts
These create a direct communication between the portalsystem and the systemic circulation, and depending on theflow, a full diversion can be achieved, with a consequent fallin the portal pressure. All these shunts have been associatedwith a significant risk of hepatic encephalopathy (comparedwith selective shunts). Nonselective shunting should beavoided when possible, as preservation of neurocognitivefunction is particularly important in children. In children,learning disorders or behavioral abnormalities can also bemanifestations of encephalopathy.
End-to-side portocaval shuntIn this operation, the portal vein is divided close to the
liver and end-to-side anastomosis of the lower stump to theinferior vena cava (IVC) is performed.
Proximal splenorenal shuntThe splenic vein is divided and the spleen is removed.
End-to-side anastomosis of the splenic vein stump to the leftrenal vein is performed.38
Mesocaval shuntAlthough it is possible to create a side-to-side mesocaval
shunt after mobilization of both the superior mesenteric vein(SMV) and IVC (without the interposition of a graft), theusual mesocaval shunt is an “H type” with the interpositionof a prosthetic conduit (Dacron/GoreTex) (Drapanasshunt)27 or autologous vein graft. In children, mesocavalshunting with an interposed jugular vein has been preferredby many teams and has been used with acceptable re-
sults.28,29,37 The Auvert shunt is a mesocaval shunt fash-ioned after division of the iliac veins and mobilization of theIVC, which is then anastomosed onto the SMV.41 Theisadvantage is a high rate of late venous complicationselated to interruption of both iliac veins.
Some nonselective shunts are performed to try to limithe hemodynamic effects of the flow diversion either byalibration or by some sort of hemodynamic balance in anttempt to both avoid full rerouting of blood flow away fromhe liver and reduce the risk of encephalopathy. In return,ne expects a reduced effect on the portal pressure, hyper-plenism, and possibly a higher risk of thrombosis orcclusion in the long term. Examples of this approachnclude the Sarfeh and the Mitra shunts. The former is an-type portocaval shunt using an 8-mm-diameter Gore-ex graft and is usually done with extensive collateral
igation. The latter, first described by Denton Cooley inhe 1960s, is a nonselective side-to-side splenorenalhunt.30 In this, the spleen is preserved, and the shunt isashioned between the splenic vein and the left renalein. It is said to reduce the risk of encephalopathyompared with other nonselective shunts because it doesot completely steal portal flow away from the liver.ood results have been reported with this shunt.30,41
TIPSS as (nonsurgical) shunt interventionAn intrahepatic metallic stent is inserted between the
intrahepatic portions of the portal vein and the hepatic vein,which creates a (nonselective) portocaval shunt. Calibrationcan be achieved in some, with a direct pressure gradientmeasurement during the procedure to allow limited flowdiversion, but hepatic encephalopathy can still occur. Theadvantages of avoiding a major abdominal intervention andpreserving the abdomen intact for possible transplantation isbalanced by potential complications such as shunt stenosis/thrombosis, bleeding, portal vein thrombosis, and migrationof the stent into the right atrium.
Experience in children remains limited to case reportsbecause it is more difficult in small patients.67 Nonetheless,it should be considered if a surgical shunt is indicated,whether as a bridge to transplant or not. Patients withwell-preserved liver function and severe chronic PHT aregood indications (ie, children with hepatic fibrosis or cysticfibrosis).
Portal vein thrombosis and the MRB
Prehepatic PHT, and specifically portal vein thrombosis, isthe commonest cause of PHT in children. Most have noobvious etiologic cause in their history and are thought of asidiopathic, perhaps even congenital, cases. Direct damage tothe portal vein in about 25% of cases can be inferred with ahistory of umbilical vein catheterization (UVC) during theneonatal period. Less commonly, portal vein thrombosismay be caused by trauma, tumors, or secondary to perito-
nitis.
dspttiitb
tigpRpipwIiti
(msmrapi
pbwcpimcgBcaliilaa
rcoW
226 Seminars in Pediatric Surgery, Vol 21, No 3, August 2012
The etiologic role of thrombophilic states and/or of sin-gle prothrombotic factor remains controversial. Most stud-ies have shown that coagulation abnormalities demonstrablein portal vein thrombosis are secondary, rather than pri-mary, disorders.48-51 In posthepatic venous thrombosis inadults, the reverse is probably true.52 Primary coagulationisorders have been reported but remain uncommon.53-55 Iteems more likely that coagulation disorders may predis-ose to thrombosis when associated with other risk fac-ors.56,57 Pietrobattista et al58 observed a correlation be-ween minor thrombophilias (eg, MTHFR-C667T mutation)n a series of 31 children with portal vein thrombosis thatncluded many with a history of UVC. It should be notedhat UVC, if appropriately performed, is rarely complicatedy portal vein thrombosis.68,69 In general, genetic prothrom-
botic risk factors seem to have only a minor role in prehe-patic PHT, with a few exceptions confirming the rule. Dif-fuse thrombosis of the splanchnic venous system may alsobe an exception to this general rule.70
Children with portal vein thrombosis should have nounderlying liver disease, and their liver function is expectedto remain normal throughout life. Some, however, maydevelop a portal biliopathy caused by extrinsic compressionof the extrahepatic bile ducts, which worsens with time andmay cause progressive cholestasis after a few decades.71
Such cholestatic change may be inferred by minor dilatationof the intrahepatic bile ducts and an association with biliarysludge or even stones. Portal vein thrombosis may extendvariably into splanchnic system, although usually the portalvein trunk has disappeared. Extension upstream into thesplenic vein or mesenteric veins is rare, leaving these ves-sels available as anastomotic sites. Even in those childrenwith large cavernomas (Figure 1), thrombosis may not ex-tend into the intrahepatic portal venous system. Usually thelatter is patent, although hypoplastic with small-diameter(3-4 mm) veins. These may not be visible on conventionalimaging (eg, Doppler ultrasonography, angio computed to-mography, and angio magnetic resonance imaging, or evenconventional angiography) (Figure 4), but it should be pos-sible to image them adequately using retrograde portogra-phy. Direct catheter insertion into the reopened umbilicalvein can be done intraoperatively but has the disadvantageof needing a laparotomy and the risk of finding a throm-bosed left portal vein, therefore making MRB unfeasible.
Consideration should be given to perform a liver biopsyto confirm normal liver histology in older children, thosewith abnormal portogram findings (eg, partial thrombosis,wall irregularities, and poorly defined portogram findingsthat may indicate associated hepatoportal sclerosis), andthose who have undergone transplant because fibrotic liversdue to chronic graft dysfunction or cholestasis may com-promise flow.
MRB (also known as mesenterico-left portal bypass or,more simply, the Rex shunt) was first used for portal veinthrombosis after transplantation before being applied to
those with idiopathic prehepatic PHT (group 1).11-18 Ana- pomically, the umbilical fissure is a natural place for enter-ng the liver outside the porta hepatis, and has relativelyood access to the portal system. Ideally, outflow is by aatent umbilical portion of the left portal vein within theex recessus, and flow should be from left to right within aatent intrahepatic portal venous system. The easiest inflows from a patent SMV immediately below the edge of theancreas; however, alternative sites have been proposedith success, such as the coronary vein, the splenic vein, the
MV, or even a large gastroduodenal vein. The conduit itselfs preferably an autologous vein of adequate diameter, andhe best results have been described in children in whom thenternal jugular vein has been used.12,13,17,18 Other alterna-
tives are more complex (eg, spiraled saphenous vein) andassociated with less favorable outcomes (eg, recanalizedumbilical vein, cryopreserved allogeneic vein, or prostheticGoreTex).
Portosystemic collaterals tend to close spontaneouslyafter the procedure when the bypass is patent, with adequateflow redirected into the liver and hepatopetal flow re-stored11-18 (Figure 6). Restoration of normal physiologyFigure 7) also corrects the secondary coagulation abnor-alities, improves neurocognitive ability, and may correct
ubclinical encephalopathy.72 It improves growth and bodyass index if the child has failed to thrive, and isolated
eports suggest it reverts hepatopulmonary syndrome anddenomatous transformation of the liver.73-77 Moreover, therocedure has not been associated with significant morbid-ty, and no mortality has been reported.
More recently, MRB has been proposed as the optimalrocedure for this condition, with a suggestion that it shoulde performed earlier in the course of the disease. Childrenith portal vein thrombosis have been usually managed
onservatively, under the assumption that by having goodarenchymal liver function they are not at risk and thatntermittent bleeding is relatively well tolerated. Further-ore, it has been often stated that complications are less
ommon both in frequency and in severity as the childrows into adulthood. The report from a workshop inaveno, Italy, stated that the common outcome in thesehildren includes a “relatively low” risk of bleeding (onverage, 1.3 episodes/year), and the risk of rebleeding in theong term after obliteration of varices is low, but there is anncreased risk of hepatic dysfunction, hepatitis B and Cnfection (repeated transfusions), severe hypersplenism re-ated to massive splenomegaly, and progressive symptom-tic portal biliopathy with prepubertal growth retardation inbout half of all cases.78 Of course, such patients do much
better compared with a comparable cohort of patients withcirrhosis, but they have a diminished quality of life com-pared with healthy children.78,79 Although a 90% survivalate has been reported in long-term follow-up studies withonservative management, similar or even better overallutcomes can be achieved when MRB is done early in life.e believe MRB should be proposed as early as reasonably
ossible after diagnosis.18 The operation is rather standard-

Phd
shapstdgenepa
F(
swfiaiopldO
227de Ville de Goyet et al Surgical Management of Portal Hypertension
ized and in trained hands can achieve excellent results inchildren from any age and any weight: the best weight/veindiameter balance is from about 10 kg of weight upward.Here the Rex fossa is easy to approach; the mesenteric veinis of a good diameter; and the jugular vein has an optimallength/diameter ratio. The lower limit is difficult to define,but infants of approximately 4 kg have successfully under-gone surgery.13 In older children and in adults, longstanding
HT and the development of numerous collaterals and auge cavernoma may render the operation technically moreemanding.
Overall, we believe that MRB should be performedooner rather than later, perhaps as soon as the diagnosisas been confirmed in children, even if there is completebsence of complications. Only children in whom the leftortal vein can be shown to be thrombosed or damagedhould the procedure be postponed and a more conven-ional strategy pursued. The management of some chil-ren with intermediate conditions (eg, abnormal porto-ram, difficult access to the portal system because ofxtensive thrombosis, no autologous material available)eeds to be individualized. Liver transplantation remainsxceptional, and most reported cases are adults withortal vein thrombosis complicated by cirrhosis second-ry to portal biliopathy.
Role of portal stenting for prehepatic PHT
Several authors have reported attempts at percutaneoustranshepatic angioplasty/stenting of a thrombosed portalvein. Gauthier80 reported a series of 10 patients in Bicêtre,
rance, with success in only 1 case with medium-term
Figure 6 Meso-Rex bypass: percutaneous angioplasty of a stenosplenic and gastric routes and feeding the esophageal varices and rinto the liver. (1, superior mesenteric vein; 2, splenic vein; 3, vacatheter).
4-year) follow-up. Similarly, Cwikiel et al81 reported a
uccessful experience in a single case of the 5 in which itas attempted. It appears that such cases were different
rom common idiopathic prehepatic PHT cases in that thentrahepatic portal system was large enough in diameter tollow transhepatic access and intravascular maneuvers. Thiss made clear by Cwikiel et al81 in their report, where theybserved that although transjugular puncture of the intrahe-atic portal vein was possible in 4 of 5 cases, full recana-ization of the portal trunk was possible in only 1, withifficulties attributable to the small caliber of veins. Semiz-ysu et al82 confirmed the technical difficulties and prob-
lems in children. As so few stents have been inserted, it isdifficult to predict the long-term outcome, and there must bethe possibility of revision because of growth.
Interventional radiological attempts should probably bekept in reserve for patients with an identifiable intrahepaticportal system and those with a limited (short in length)portal vein thrombosis, or better, those with limited stric-tures of the portal vein.
Nonshunt surgical options
A variety of nonshunt surgical procedures have beenproposed over the years. Although some of these proce-dures are rather simple and easy to perform, others arecomplex and aggressive. The simplicity of the formerdoes not imply that they have a role today or are preferredto other treatments. Many were conceived in a time whenalternative more modern strategies were not available, orwere proposed to manage complex, sometimes last-chance, clinical conditions. Most probably, they now
pass showing that the mesenteric venous flow is diverted into theritoneal collaterals. After plasty of the bypass, the flow is rerouted4, bypass; 5, left portal vein; 6, right portal vein; c, transhepatic
tic byetroperices;
have no place, particularly in children.83-87

td
with th
228 Seminars in Pediatric Surgery, Vol 21, No 3, August 2012
Surgical ligation of varices and esophagealtransection
Direct ligation of the varices via a thoracic or transgastricroute is historically the “ancestor” of endoscopic varicealeradication, although the latter has proved much more effi-cient at a less invasive cost. Transection of the esophagus orthe upper stomach, with direct reanastomosis (Sugiura pro-cedure and others), interrupts the intramural vein andvariceal network, immediately separating esophageal vari-ces from the splanchnic venous system and minimizingbleeding. It was originally proposed as an alternative toshunt procedures in adults.83 A number of modifications ofhe Sugiura operation have been proposed for chil-ren,84,86,87 and its use has been reported largely from
developing countries with limited surgical and medicalmanagement options and no access to liver transplanta-tion.84,87,88 Although satisfactory long-term results are re-ported, these have been mostly in patients with prehepaticPHT. The procedure is palliative and has a high incidence ofrecurrence in the medium term; it also creates numerousadhesions that make further abdominal surgery more diffi-
Figure 7 Portal flow patterns in the normal patient (transhepathrombosis with cavernoma (partial diversion and PHT), compared
cult.
Splenectomy and splenic embolization
Splenectomy or splenic artery embolization may be advo-cated in some rare cases of severe hypersplenism.89-92 Itdoes reduce the arterial inflow to the portal venous systemand PHT, and therefore may reduce the frequency of bleed-ing esophageal varices. This is usually regarded as tempo-rary, and recurrence is the rule. Additionally, there are othercomplications, such as postsplenectomy sepsis and intra-peritoneal adhesions, together with propagation of throm-bosis in the splenic vein into the portal venous system,exacerbating PHT and rendering further shunt surgery lim-ited or hazardous. Splenectomy must be considered a lastresort in children and should not be proposed if other man-agement options are available. If splenectomy is to be per-formed in a child with PHT, the surgeon should also con-sider performing a proximal splenorenal shunt at the sametime to achieve portal decompression and retain splenic veinpatency.
Partial splenectomy has been proposed recently withpreservation of some splenic flow combined with an omen-topexy. This seems a reasonable alternative, as this helps
te) and in patients with normal liver and prehepatic portal veine latter patient after mesocaval shunt, and after meso-Rex bypass.
tic rou
preserve the splenic vein without performing a portosys-

ccutpai
cppirsp
229de Ville de Goyet et al Surgical Management of Portal Hypertension
temic shunt.92,93 Partial splenic embolization is a similarompromise, but the effects on PHT are limited, although itan have a significant effect on hypersplenism. It should besed with caution, as a significant embolization (necessaryo obtain a clinical effect) correlates with increasing com-lications, such as pain, necrosis, and abscess formation,nd again may make further regional surgery more demand-ng.89-91,94
The ultimate shunt procedure: Livertransplantation
Management has dramatically changed during the past 2decades for children with cirrhotic PHT. This has beenbecause of the efficiency of endoscopic variceal control inthe chronically ill, but stable, patient, and the wide use andsuccess of liver transplantation in those who deteriorate.Children with poor synthetic liver reserve and PHT areprimarily candidates for liver transplant. In these, the highrate of complications after shunt surgery outweighs its po-tential short-term benefits. One-year patient survival afterliver transplant approaches 95% in experienced centers, andthe procedure is curative for the primary disease; this hasinfluenced the strategy of a no-shunt choice for the stablepatient by many teams.
The role of portosystemic shunting in children with adiseased liver is reduced to highly selected cases withvery good residual hepatic function that is likely to per-sist unchanged for a long period and may typically in-clude cases of hepatic fibrosis and cystic fibrosis. Evenhere, the role of surgical shunting has probably beendisplaced by comparison with a TIPSS procedure, as thisis easy to follow, revise, tailor, and even remove whennecessary (transplantation).
Figure 8 Liver adenoma in a patient with cavernomatous transformati
Complications and outcome after shunt andbypass
Successful shunt surgery achieves relief of PHT and cor-rection of most of its complications. When performed byskilled surgeons, it is an efficient and safe procedure. Highlong-term patency rates, ranging from 89% to 97%, havebeen reported.28,29,35-39 Failure to achieve satisfactory out-omes is mostly related to unfavorable anatomy of theortal venous system and diffuse thrombosis. Along withrevention of gastrointestinal hemorrhage, other benefitsnclude correction of splenomegaly and hypersplenism, cor-ection of biliary anomalies (ie, portal biliopathy), and tran-ient acceleration of growth leading to a significant im-rovement in quality of life.95
Shunt thrombosis is a serious problem, more frequentwhen using a conduit, and can be related to technical prob-lems, such as compression and kinking, or a hypercoagula-ble state. Experienced centers report low rates of shuntthrombosis (�5%). Doppler ultrasonographic assessmentshould be done during the first week to detect early prob-lems. Postoperative prophylaxis is recommended, with low-dose heparin during the first week, followed by antiplateletagents (aspirin and dipyridamole) for 3-6 months. In casesof shunt thrombosis, the shunt may be salvageable either bysurgical revision (preferably if early thrombosis), or byradiological intervention to attempt percutaneous recanali-zation and/or balloon angioplasty. Such procedures weresuccessful in 9 of 10 cases in the Bicêtre series.95
Chylous ascites owing to disruption of retroperitoneallymphatic channels by surgery are uncommon after a suc-cessful shunt operation that allows good portal decompres-sion. Persistence may imply an insufficient drop in portalvenous pressure, maintaining high pressure and flow in thelymphatic system.
Encephalopathy is a problem after conventional shuntsurgery in patients with cirrhosis, yet occurs infrequently in
on of the portal vein, extrahepatic PHT, and major splenomegaly.

230 Seminars in Pediatric Surgery, Vol 21, No 3, August 2012
those without parenchymal disease.95-97 Nonetheless, thisaffirmation may have to be reviewed in light of recentreports suggesting that subclinical encephalopathy is muchmore common than thought even in those with preservedliver function, and further studies are necessary.72,98-100
Portopulmonary syndrome (hepatopulmonary syndromeand pulmonary hypertension) is rare in children and can beobserved in those with either cirrhotic or noncirrhoticPHT.95,101 French research suggests a rate of 1 case ofpulmonary arterial hypertension among more than 100 chil-dren with portosystemic shunts for prehepatic PHT.47,80,95
These complications may occur late after shunt surgery, andlong-term cardiopulmonary follow-up is recommended (eg,echocardiography, resting and stressed O2 saturation mea-surements).
Liver nodules (liver cell adenomas, focal nodular hyper-plasia) may develop in the long term in some postshuntpatients, but the risk appears to be modest. It is seen mostlyin those patients with prolonged survival who have notrequired transplantation. Ultrasonography-based screeningover the long term is suggested102 (Figure 8).
Conclusions
The management of children with PHT has changed dra-matically in the past decade with an improved outcomepartly based on the efficiency of endoscopic variceal controlin the acute scenario and the success of liver transplantation.
Emergency shunt procedures should now be extremelyrare, with acute bleeding generally controlled endoscopi-cally or, less commonly in the older child, by a TIPSSprocedure. The concept of a short-term surgical shunt as abridge to transplant is rarely considered in children.
Surgery is indicated for complicated cases with noncir-rhotic PHT, with MRB proposed, even preemptively, forthose with favorable anatomy.
References
1. Vargas HE, Gerber D, Abu-Elmagd K. Management of portal hyper-tension-related bleeding. Surg Clin North Am 1999;79:1-22.
2. Garcia-Tsao G, Groszmann RJ, Fisher RL, et al. Portal pressure,presence of gastroesophageal varices and variceal bleeding. Hepatol-ogy 1985;5:419-24.
3. Whitington P. Portal hypertension in children. Pediatr Ann 1995;14:494-9.
4. Howard ER. Etiology of portal hypertension and congenital anoma-lies of the portal venous system. In: Howard ER, Stringer MD,Colombani PM, eds. Surgery of the Liver, Bile Ducts and Pancreas inChildren. London: Arnold; 2002:287-95.
5. Maksoud JG, Gonçalves ME. Treatment of portal hypertension inchildren. World J Surg 1994;18:251-8.
6. Kumar N, de Ville de Goyet J, Sharif K, et al. Congenital, solitary,large, intrahepatic arterioportal fistula in a child: Management and
review of the literature. Pediatr Radiol 2003;33:20-3.7. Norton SP, Jacobson K, Moroz SP, et al. The congenital intrahepaticarterioportal fistula syndrome: Elucidation and proposed classifica-tion. J Pediatr Gastroenterol Nutr 2006;43:248-55.
8. Lykavieris P, Gauthier F, Hadchouel P, et al. Risk of gastrointestinalbleeding during adolescence and early adulthood in children withportal vein obstruction. J Pediatr 2000;136:805-9.
9. Weiss B, Shteyer E, Vivante A, et al. Etiology and long-term out-come of extrahepatic portal vein obstruction in children. World JGastroenterol 2010;16:4968-7.
10. Webb LJ, Sherlock S. The aetiology, presentation and natural historyof extrahepatic portal venous obstruction. Q J Med 1979;192:627-39.
11. de Ville de Goyet J, Clapuyt P, Otte JB. Extrahilar mesenterico-leftportal shunt to relieve extrahepatic portal hypertension after partialliver transplant. Transplantation 1992;53:231-2.
12. de Ville de Goyet J, Gibbs P, Clapuyt P, et al. Original extrahilarapproach for hepatic portal revascularization and relief of extrahe-patic portal hypertension related to later portal vein thrombosis afterpediatric liver transplantation. Long term results. Transplantation1996;62:71-4.
13. de Ville de Goyet J, Alberti D, Clapuyt P, et al. Direct bypassing ofextrahepatic portal venous obstruction in children: A new techniquefor combined hepatic portal revascularization and treatment of extra-hepatic portal hypertension. J Pediatr Surg 1998;33:597-60.
14. de Ville de Goyet J, Alberti D, Falchetti D, et al. Treatment ofextrahepatic portal hypertension in children with mesenteric-to-leftportal vein bypass: A new physiological procedure. Eur J Surg1999;165:777-81.
15. Superina R, Bambini DA, Lokar J, et al. Correction of extrahepaticportal vein thrombosis by the mesenteric to left portal vein bypass.Ann Surg 2006;243:515-8.
16. Dasgupta R, Roberts E, Superina RA, et al. Effectiveness of Rexshunt in the treatment of portal hypertension. J Pediatr Surg 2006;41:108-11.
17. Krebs-Schmitt D, Briem-Richter A, Grabhorn E, et al. Effectivenessof Rex shunt in children with portal hypertension following livertransplant or with primary portal hypertension. Pediatr Transplant2009;13:540-4.
18. Sharif K, McKiernan P, de Ville de Goyet J, et al. Mesoportal bypassfor extrahepatic portal vein obstruction in children: Close to a cure formost! J Pediatr Surg 2010;45:272-6.
19. Schneider B, Emre S, Groszmann R, et al. Expert pediatric opinion onthe report of the Baveno IV consensus workshop on methodology ofdiagnosis and therapy in portal hypertension. Pediatr Transplant2006;10:893-907.
20. Superina R, Shneider B, Emre S, et al. Surgical guidelines for themanagement of extra-hepatic portal vein obstruction. Pediatr Trans-plant 2006;10:908-13.
21. Gauthier F. Recent concepts regarding extra-hepatic portal hyperten-sion. Semin Pediatr Surg 2005;14:216-25.
22. Maksoud-Filho JG, Gonçalves MEP, Cardoso SR, et al. Long-termfollow-up of children with extrahepatic portal vein obstruction: Im-pact of an endoscopic sclerotherapy program on bleeding episodes,hepatic function, hypersplenism, and mortality. J Pediatr Surg 2009;44:1877-83.
23. Mileti E, Rosenthal P. Management of portal hypertension in chil-dren. Curr Gastroenterol Rep 2011;13:10-6.
24. Scholz S, Sharif K. Surgery for portal hypertension in children. CurrGastroenterol Rep 2011;13:279-85.
25. Sarin SK, Gupta N, Kumar S, et al. Equal efficacy of endoscopicvariceal ligation and propranolol in preventing variceal bleeding inpatients with noncirrhotic portal hypertension. Gastroenterologist2010;139:1238-45.
26. Lay CS, Tsai YT, Lee FY, et al. Endoscopic variceal ligation versuspropranolol in prophylaxis of first variceal bleeding in patients withcirrhosis. J Gastroenterol Hepatol 2006;21:413-9.
27. Drapanas T, LoCicero J, Dowling B. Hemodynamics of the interpo-
sition mesocaval shunt. Ann Surg 1975;181:523-31.
231de Ville de Goyet et al Surgical Management of Portal Hypertension
28. Gauthier F, De Dreuzy O, Valayer J, et al. H-type shunt with anautologous venous graft for treatment of portal hypertension in chil-dren. J Pediatr Surg 1989;24:1041-3.
29. Altman RP. Portal decompression by interposition mesocaval shuntin patients with biliary atresia. J Pediatr Surg 1976;11:809-14.
30. Mitra SK, Mukherjee B, Prasad GR, et al. Extrahepatic portal ob-struction in children—Experience with side-to-side lienorenal shuntwithout splenectomy. Indian J Pediatr 1983;50:55-60.
31. Corbacioglu S, Greil J, Peters C, et al. Defibrotide in the treatment ofchildren with veno-occlusive disease: A retrospective multicentrestudy demonstrates therapeutic efficacy upon early intervention.Bone Marrow Transplant 2004;33:189-95.
32. Valla DC. Prognosis in Budd Chiari syndrome after re-establishinghepatic venous drainage. Gut 2008;57:1469-147.
33. Billing JS, Jamieson NV. Hepatic arterioportal fistula: A curablecause of portal hypertension in infancy. HPB Surgery 1997;10:311-4.
34. Heaton ND, Davenport M, Karani J, et al. Congenital hepatoportalarteriovenous fistula. Surgery 1995;117:170-4.
35. Superina RA, Alonso EM. Medical and surgical management ofportal hypertension in children. Curr Treat Options Gastroenterol2006;9:432-43.
36. Botha JF, Campos BD, Grant WJ, et al. Portosystemic shunts inchildren: A 15-year experience. J Am Coll Surg 2004;199:179-85.
37. Bismuth H, Franco D. Portal diversion for portal hypertension inearly childhood. Ann Surg 1976;183:439-46.
38. Prasad AS, Gupta S, Kohli V, et al. Proximal splenorenal shunts forextrahepatic portal venous obstruction in children. Ann Surg 1994;219:193-6.
39. Orloff MJ, Orloff MS, Girard B, et al. Bleeding esophagogastricvarices from extrahepatic portal hypertension: 40 years’ experiencewith portal-systemic shunt. J Am Coll Surg 2002;194:717-30.
40. Grace ND, Conn HO, Resnick RH, et al. Distal splenorenal vs.portal-systemic shunts after hemorrhage from varices: A randomizedcontrolled trial. Hepatology 1988;8:1475-81.
41. Rypins EB, Sarfeh IJ. Partial portal decompression: Two approachesto the management of portal hypertension. Hepatology 1990;12:370-2.
42. Kheradpir MH. Late results of a modified new surgical procedure for thetreatment of portal hypertension. Eur J Pediatr Surg 2007;17:17-22.
43. Rao KL, Goyal A, Menon P, et al. Extrahepatic portal hypertensionin children: Observations on three surgical procedures. Pediatr SurgInt 2004;20:679-84.
44. Brems JJ, Hiatt JR, Klein AS, et al. Effect of a prior portasystemicshunt on subsequent liver transplantation. Ann Surg 1989;209:51-6.
45. Shilyansky J, Roberts EA, Superina RA. Distal splenorenal shunts forthe treatment of severe thrombocytopenia from portal hypertension inchildren. J Gastrointest Surg 1999;3:167-72.
46. Eizaguirre I, Tovar JA, Orcolaga R, et al. Warren’s shunt in thetreatment of portal hypertension in children [in Spanish]. Cir Pediátr1991;4:134-9.
47. Barbé T, Losay J, Grimon G, et al. Pulmonary arteriovenous shuntingin children with liver disease. J Pediatr 1995;126:571-9.
48. Dubuisson C, Boyer-Neumann C, Wolf M, et al. Protein C, protein Sand antithrombin III in children with portal vein obstruction. J Hepa-tol 1997;27:132-5.
49. Seixas CA, Hessel G, Ribeiro CC, et al. Factor V Leyden is notcommon in children with portal thrombosis. Thromb Haemost 1997;77:258-61.
50. Mahmoud AE, Elias E, Beauchamp N, et al. Prevalence of the factorV Leyden mutation in hepatic and portal vein thrombosis. Gut 1997;40:798-800.
51. Pinto RB, Silveira TR, Rosling R, et al. Thrombophilic disorders inchildren and adolescents with portal vein thrombosis [in Portuguese].J Pediatr (Rio J) 2003;79:165-72.
52. Bhattacharyya M, Makharia G, Kannan M, et al. Inherited prothrom-botic defects in Budd-Chiari syndrome and portal vein thrombosis: A
study from North India. Am J Clin Pathol 2004;121:844-7.53. Pati HP, Srivastava A, Sahni P. Extra hepatic portal vein thrombosisin a child associated with lupus anticoagulant. J Trop Pediatr 2003;49:191-2.
54. Arav-Boger R, Reif S, Bujanover Y. Portal vein thrombosis causedby protein C and protein S deficiency associated with cytomegalovi-rus infection. J Pediatr 1995;126:586-8.
55. Ettingshausen CE, Saguer IM, Kreuz W. Portal vein thrombosis in apatient with severe haemophilia A and F V G1691A mutation duringcontinuous infusion of F VIII after intramural jejunal bleeding—Successful thrombolysis under heparin therapy. Eur J Pediatr 1999;158(Suppl 3):S180-2.
56. Uttenreuther-Fischer MM, Vetter B, Hellmann C, et al. Paediatricthrombo-embolism: The influence of non-genetic factors and the roleof activated protein C resistance and protein C deficiency. Eur J Pe-diatr 1997;156:277-81.
57. Heller C, Schobess R, Kurnik K, et al. Abdominal venous thrombosisin neonates and infants: Role of prothrombotic risk factors—A mul-ticentre case-control study. For the Childhood Thrombophilia StudyGroup. Br J Haematol 2000;111:534-9.
58. Pietrobattista A, Luciani M, Abraldes JG, et al. Extrahepatic portalvein thrombosis in children and adolescents: Influence of geneticthrombophilic disorders. World J Gastroenterol 2010;16:6123-7.
59. Kwan SW, Fidelman N, Durack JC, et al. Rex shunt preoperativeimaging: Diagnostic capability of imaging modalities. PLoS One2011;6:e22222.
60. Chaves IJ, Rigsby CK, Schoeneman SE, et al. Pre- and postoperativeimaging and interventions for the meso-Rex bypass in children andyoung adults. Pediatr Radiol 2012;42:220-32.
61. Martinez-Cuesta A, Elduayen B, Vivas I, et al. CO2 wedged hepaticvenography: technical considerations and comparison with direct andindirect portography with iodinated contrast. Abdom Imaging 2000;25:576-8.
62. Puppala S, Patel J, Woodley H, et al. Preoperative imaging of leftportal vein at the Rex recess for Rex shunt formation using wedgedhepatic vein carbon dioxide portography. J Pediatr Surg 2009;44:2043-7.
63. Lawson AJ, Rischbieter P, Numanoglu A, et al. Imaging the Rex veinpreoperatively using wedged hepatic venous portography. PediatrRadiol 2011;41:1246-9.
64. Maleux G, Nevens F, Heye S, et al. The use of carbon dioxidewedged hepatic venography to identify the portal vein: Comparisonwith direct catheter portography with iodinated contrast medium andanalysis of predictive factors influencing level of opacification. JVasc Interv Radiol 2006;17:177-9.
65. Debernardi-Venon W, Bandi JC, García-Pagán JC, et al. CO2 wedgedhepatic venography in the evaluation of portal hypertension. Gut2000;46:856-86.
66. Warren WD, Millikan WJ, Smith RB, et al. Noncirrhotic portal veinthrombosis. Physiology before and after shunts. Ann Surg 1980;192:341-8.
67. Heyman MB, LaBerge JM, Somberg KA, et al. Transjugular intra-hepatic portosystemic shunts (TIPS) in children. J Pediatr 1997;131:914-9.
68. Schwartz DS, Gettner PA, Konstantino MM, et al. Umbilical venouscatheterization and the risk of portal vein thrombosis. J Pediatr1997;131:760-2.
69. Kim JH, Lee YS, Kim SH, et al. Does umbilical vein catheterizationlead to portal venous thrombosis? Prospective US evaluation in 100neonates. Radiology 2001;219:645-50.
70. Stringer MD, Heaton ND, Karani J, et al. Patterns of portal vein occlu-sion and their aetiological significance. Br J Surg 1994;81:1328-31.
71. Agarwal AK, Sharma D, Singh S, et al. Portal biliopathy: A study of39 surgically treated patients. HPB (Oxford) 2011;13:33-9.
72. Goel A, Yadav S, Saraswat V, et al. Cerebral oedema in minimalhepatic encephalopathy due to extrahepatic portal venous obstruction.
Liver Int 2010;30:1143-51.
232 Seminars in Pediatric Surgery, Vol 21, No 3, August 2012
73. Lautz TB, Sundaram SS, Whitington PF, et al. Growth impairment inchildren with extrahepatic portal vein obstruction is improved bymesenterico-left portal vein bypass. J Pediatr Surg 2009;44:2067-70.
74. Mack CL, Zelko FA, Lokar J, et al. Surgically restoring portal bloodflow to the liver in children with primary extrahepatic portal veinthrombosis improves fluid neurocognitive ability. Pediatrics 2006;117:e405-12.
75. Stringer MD. Improved body mass index after mesenterico-portalbypass. Pediatr Surg Int 2007;23:539-43.
76. Chiu B, Superina RA. Encephalopathy caused by a splenorenal shuntcan be reversed by performing a mesenteric-to-left portal vein by-pass. J Pediatr Surg 2006;41:1177-9.
77. Mack CL, Superina RA, Whitington PF. Surgical restoration of portalflow corrects procoagulant and anticoagulant deficiencies associatedwith extrahepatic portal hypertension. J Pediatr 2003;142:197-9.
78. Bellomo-Brandao MA, Morcillo AM, Hessel G, et al. Growth assess-ment in children with extra-hepatic portal vein obstruction and portalhypertension. Arq Gastroenterol 2003;40:247-50.
79. van der Plas SM, Hansen BE, de Boer JB, et al. Generic and disease-specific health related quality of life in non-cirrhotic, cirrhotic andtransplanted liver patients: A cross-sectional study. BMC Gastroen-terol 2003;3:33. Available at: http://www.biomedcentral.com/1471-230X/3/33.
80. Gauthier F. Recent concepts regarding extra-hepatic portal hyperten-sion. Semin Pediatr Surg 2005;14:216-25.
81. Cwikiel W, Keussen I, Larsson L, et al. Interventional treatment ofchildren with portal hypertension secondary to portal vein occlusion.Eur J Pediatr Surg 2003;13:312-8.
82. Semiz-Oysu A, Keussen I, Cwikiel W. Interventional radiologicalmanagement of prehepatic obstruction of the splanchnic venous sys-tem. Cardiovasc Intervent Radiol 2007;30:688-95.
83. Sugiura M, Futagawa S. A new technique for treating esophagealvarices. J Thorac Cardiovasc Surg 1973;66:677-85.
84. Sharma D, Agrawal S, Saxena A, et al. A modified technique ofdevascularization for surgical management of portal hypertension inchildren. Trop Doct 2001;31:93-5.
85. Faruk S, Yes E, Emir H, et al. Sugiura procedure in portal hyperten-sive children. J Hepato Biliary Pancreat Surg 2001;8:245-9.
86. Superina RA, Weber JL, Shandling B. A modified Sugiura operationfor bleeding varices in children. J Pediatr Surg 1983;18:794-9.
87. Uchiyama M, Iwafuchi M, Ohsawa Y, et al. Long-term results afternonshunt operations for esophageal varices in children. J Pediatr Surg1994;29:1429-33.
88. Abouna GM, Baissony H, Al-Nakib BM, et al. The place of Sugiuraoperation for portal hypertension and bleeding esophageal varices.
Surgery 1987;101:91-8.89. Shah R, Mahour GH, Ford EG, et al. Partial splenic embolization. Aneffective alternative to splenectomy for hypersplenism. Am Surg1990;56:774-7.
90. Koconis KG, Singh H, Soares G. Partial splenic embolization in thetreatment of patients with portal hypertension: A review of the Eng-lish language literature. J Vasc Interv Radiol 2007;18:463-81.
91. Madoff DC, Denys A, Wallace MJ, et al. Splenic arterial interven-tions: Anatomy, indications, technical considerations, and potentialcomplications. Radiographics 2005;25:S191-211.
92. Subhasis RC, Rajiv C, Akshay S, et al. Surgical treatment of massivesplenomegaly and severe hypersplenism secondary to extrahepaticportal venous obstruction in children. Surg Today 2007;37:19-23.
93. Xu RY, Liu B, Lin N. Therapeutic effects of endoscopic varicealligation combined with partial splenic embolization for portal hyper-tension. World J Gastroenterol 2004;10:1072-4.
94. Aslanidou E, Fotoulaki M, Tsitouridis I, et al. Partial splenic embo-lization: Successful treatment of hypersplenism, secondary to biliarycirrhosis and portal hypertension in cystic fibrosis. J Cyst Fibros2007;6:212-4.
95. Valayer J, Branchereau S. Portal hypertension: Portosystemic shunts.In: Stringer MD, Oldham KT, Mouriquand PDE, et al, eds. PediatricSurgery and Urology: Long-Term Outcomes. Philadelphia, PA,Saunders, 1998, pp 439-46.
96. Alagille D, Carlier JC, Chiva M, et al. Long-term neuropsychologicaloutcome in children undergoing portal-systemic shunts for portal veinobstruction without liver disease. J Pediatr Gastroenterol Nutr 1986;5:861-6.
97. Mohapatra MK, Mohapatra AK, Acharya SK, et al. Encephalopathyin patients with extrahepatic obstruction after lienorenal shunts. Br JSurg 1992;79:1103-5.
98. Rovira A, Alonso J, Cordoba J. MR imaging findings in hepaticencephalopathy. Am J Neuroradiol 2008;29:1612-21.
99. Srivastava A, Yadav SK, Lal R, et al. Effect of surgical portosystemicshunt on prevalence of minimal hepatic encephalopathy in childrenwith extrahepatic portal venous obstruction: Assessment by magneticresonance imaging and psychometry. J Pediatr Gastroenterol Nutr2010;51:766-72.
100. Yadav SK, Srivastava A, Srivastava A, et al. Encephalopathy assessmentin children with extra-hepatic portal vein obstruction with MR, psy-chometry and critical flicker frequency. J Hepatol 2010;52:348-54.
101. Kumar S, Kumar A, Sharma BC, et al. Systemic and pulmonaryhemodynamics in patients with extrahepatic portal vein obstruc-tion is similar to compensated cirrhotic patients. Hepatol Int2009;3:384-91.
102. Guérin F, Porras J, Fabre M, et al. Liver nodules after portal systemicshunt surgery for extrahepatic portal vein obstruction in children.
J Pediatr Surg 2009;44:1337-43.