Embed Size (px)
Citation preview

Surgical Management of Sphenoid Wing Meningiomas
Mohamed Emara MD, Alaa Farag MD, Walid Badawy MD, Hosam Maaty MD, Fathy Elnos MD
Department of Neurosurgery, Banha University
ABSTRACTBackground: Sphenoidal meningiomas constitute 18% of intracranial masses.
Sphenoid wing meningiomas still present a difficult surgical challenge especially when they are large in size and involve neurovascular structures. Objective: The aim of the study is to shed light on the management of sphenoid wing meningioma, study the outcome of microsurgical resection and factors affecting its resectability. Patients and Methods: In this prospective study, thirty cases were included thirteen outer and / or middle sphenoid wing, thirteen clinoidal and four meningiomas en plaque. In each case diagnosis was made clinically and confirmed radiologically and histo-pathologically. Results: Between March 2011 and June 2014, thirty patients with meningiomas primarily originating from sphenoid ridge were operated, 22 (73.3%) patients were females and 8(26.7%) were males. In seventeen cases total resection was achieved, and subtotal resection in thirteen cases. In this study mortality was recorded in two case and morbidity in nine cases. Eight cases has excellent outcome fourteen were good and six were fair and two died. Conclusion: The surgical treatment of sphenoid wing meningiomas still represents a challenge for neurosurgeons. Surgery for sphenoid wing meningiomas poses a variety of problems reflecting the complex anatomy of the sphenoid region.
Key Words: Meningioma, sphenoid wing,surgical treatment Correspondence to Alaa A Farag. Department of Neurosurgery Banha University, Egypt. email: [email protected] Tel. +2/01287518299
INTRODUCTIONMeningiomas are among the
most common primary intracranial tumors. They are slow growing tumors originating from the arachnoidal cap cells and may occur anywhere that arachnoid cells are found(8).
Meningioma account for 14.3-19% of primary intracranial neoplasms
with a reported incidence 4.4 per 100000 person-year. Female : male ratio is 2:1. The true prevelance is likely even greater, as incidental meningiomas have been reported in 2.3% of autopsy examinations. Most commonly diagnosed in middle-aged and eldery patients. Cranial meningiomas are roughly 10 fold
- 1 -
more common than spinal meningiomas(9)
Deletion of the neurofibro-matosis type 2(NF2) gene, ionizing radiation and head truma are associ-ated with an increase risk, while the role of sex hormones in meningioma development is still uncertain(8)
Sphenoid wing meningioma account for about 11.9% of intracranial meningiomas, they are classified into lateral sphenoid wing (or pterional) which are usually similar to convexity meningioma, middle (or alar) and medial (or clinoidal). The medial type tends to encase the internal carotid artery (ICA) and middle cerebral artery (MCA) as well as cranial nerves(1)(2)(14).
The clinical presentation of sphenoid wing meningiomas is manifestation of increased intracranial tension. Clinical features unique to this group of meningiomas include: exophtalmous, transient diplopia due to occlumotor nerve dysfunction, periorbital pain or numbness in the territory of the V1 branch, progressive visual loss, and seizures(6)(13).
Contrasted - enhansed cranial CT and MR imaging are the predominant imaging techniques used in the diagnosis and management of meningiomas; however, in selected cases, MR spectroscopy, MR angiography and Positron emission tomography may be useful(7).
The most appropriate surgical treatment of lateral and middle sphenoid wing meningioma is total removal. Complete removal implies total removal of the tumor, including the dural attachment and bone that is involved with the tumor(9)
Clinoidal meningiomas consid-ered a major neurosurgical challenge due to involvement of important neuron-vascular structures, cranial base techniques can be used for surgical removal of these tumors with good results(10).
Sterotactic radiosurgery can be used as an alternative treatment to surgery. For incomplety resected or recurrent tumors conventional radio-therapy is beneficial. When the lesion is considered unresectable or all other treatments have failed; hormonal therapy or chemotherapy should be considered(15).
Future therapies will include combination of targeted molecular agents, and this will most likely be accomplished through continued progress in the understanding of the genetics and biological changes associated with meningioma.(15)
The aim of the study is to shed light on the management of sphenoid wing meningioma, study the outcome of microsurgical resection and factors affecting its resectability.
- 2 -
PATIENTS AND METHODSBetween March 2011 and June
2014, a prospective study including 30 patients with meningiomas primarily originating from sphenoid ridge was done. The meningioma extended along the anterior and middle cranial fossae. All patients were admitted to the Neurosurgery department in Banha University Hospital and Nasser Institute hospital.
In this study, the patients were subjected to thorough neurological examination. Computerized tomo-graphy as well as Magnetic resonance imaging, with and without contrast enhancement, were done for all cases preoperatively. MRA or CT angiographies were also done when the relation of tumor to vessels need to be delinned. All these patients were submitted to surgery. Postoperative CT and MRI was done as a routine.
Tumors were classified according to size into small (less than 3cm in maximum dimention), large (more than 3 and less than 5cm in maximum dimention) and giant (more than 5cm in maximum dimention).
Operative Management:Surgery was performed with
general anaesthesia, with the aid of an operating microscope and micro-surgical instrumentation in all cases.
The choice of surgical approach for these meningiomas depended on the location of the tumor and extent of
its dural attachment. The aim of surgery was either total or subtotal excision depending on the preoperative imaging study. Pterional and fronto – orbito - zygomatic approaches were used.
Intra-operatively, the aim was complete microsurgical removal of the tumor aiming to cure the patients unless the tumor was encasing vessels or nervous tissue. The plan of tumor removal included infilterated dura and bone.
A carefully planned craniotomy was done exposing the tumor and also any part of the dura invaded by the meningioma. The dura was coagulated, to provide early control of the tumor blood supply. The dura was incised in circumferential manner.
Removal of the tumor was started with internal decompression depending on understanding of the bony and neurovascular anatomy of the middle cranial fossa, sellar and parasellar region.
Parts of the tumor adherent to middle cerebral artery or internal carotid artery or infilterating the cavernous sinus (CS) were not removed. Infilterated dura and bone was removed. Hemostasis was done with the aid of surgicell. Watertight dural closure was done using pericranial flap or fascia lata graft. The wound was closed in anatomical layers
- 3 -
The grading for meningioma resection is conventional Simpson grading. In the resection of sphenoidal meningiomas, sometimes it is difficult for the surgeon to ascertain that the entire area of dural involvement or attachment has been exposed, resected, or coagulated. Therefore, we choose to define "Gross total resection" in this series as Simpson grade I and II and "subtotal" for other grades.
Cases with histological evidence of malignancy or with residual lesions were sent for conventional radiotherapy or gamma knife.
Follow up of cases was conducted in the Neurosurgical outpatient clinic. Evaluation was done both clinically and radiologically by the help of CT and MRI with contrast, to detect any residual of the excised tumor.
In this study, the outcome was considered to be:
Excellent: Total tumor removal with improvement of clinical condition with no deficit.
Good: Total tumor removal without improvement of clinical condition or with development of new treatable deficit or In complete tumor removal done with improve-ement of the clinical condition.
Fair: Incomplete tumor removal without clinical improvement
or Total removal with development of new untreatable deficit or deterioration of previous deficit.
Poor: Incomplete tumor removal with development of a new untreatable deficit
RESULTS:Thirty patients with
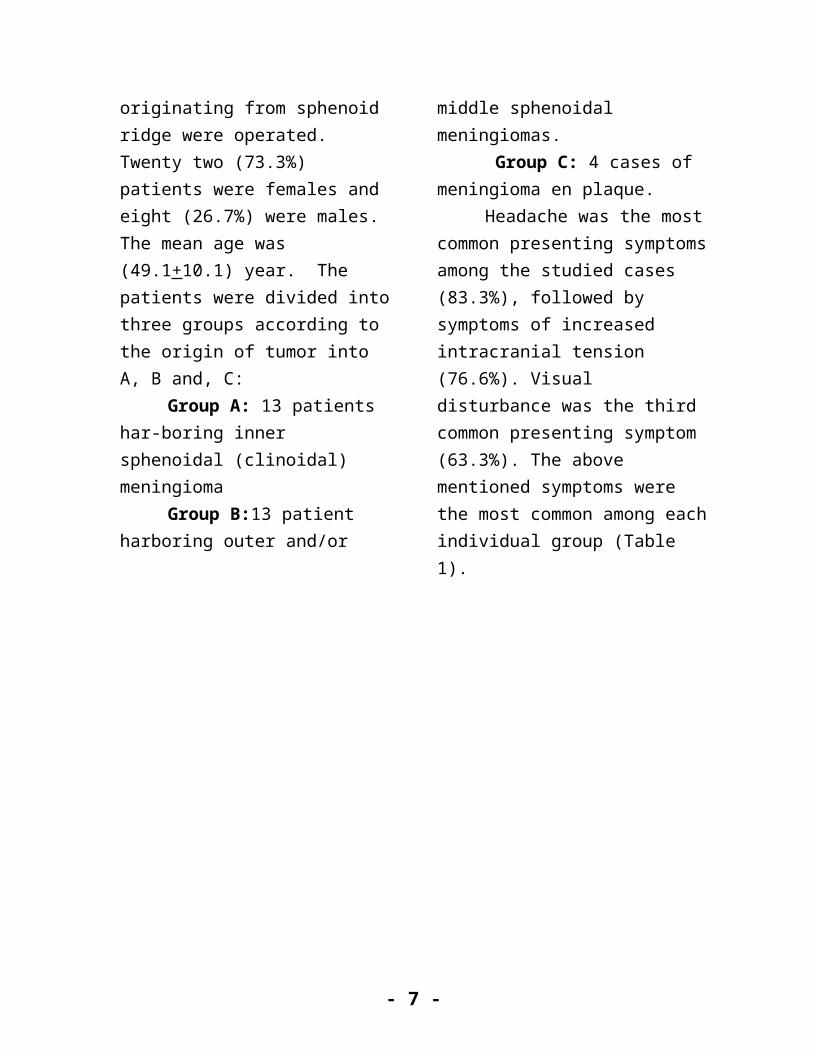
meningiomas primarily originating from sphenoid ridge were operated. Twenty two (73.3%) patients were females and eight (26.7%) were males. The mean age was (49.1+10.1) year. The patients were divided into three groups according to the origin of tumor into A, B and, C:
Group A: 13 patients har-boring inner sphenoidal (clinoidal) meningioma
Group B:13 patient harboring outer and/or middle sphenoidal meningiomas.
Group C: 4 cases of meningioma en plaque.
Headache was the most common presenting symptoms among the studied cases (83.3%), followed by symptoms of increased intracranial tension (76.6%). Visual disturbance was the third common presenting symptom (63.3%). The above mentioned symptoms were the most common among each individual group (Table 1).
- 4 -
- 5 -
Table (1): Presenting symptoms among studied groups
Symptom
Group A
INNER
NO=13
Group B
OUTER&
MIDDLE
No = 13
Group C
EN-PLAQUE
NO=4
Total
No=30
NO % NO % NO % NO %
Headache 10 76.9 11 84.6 4 100 25 83.3
Visual disturbance 12 92.3 5 38.5 2 50 19 63.3
Increased intracranial tension 9 69.2 10 76,9 4 100 23 76.6
Seizures 5 38.5 5 38.5 1 25 11 36.6
Proptosis 0 0 0 0 3 75 3 10
Diplopia 3 23.1 1 7.7 0 0 4 10.3
Motor weakness 2 15.4 4 31.2 0 0 6 20
Impaired consciousness 2 15.4 1 7.7 0 0 3 10
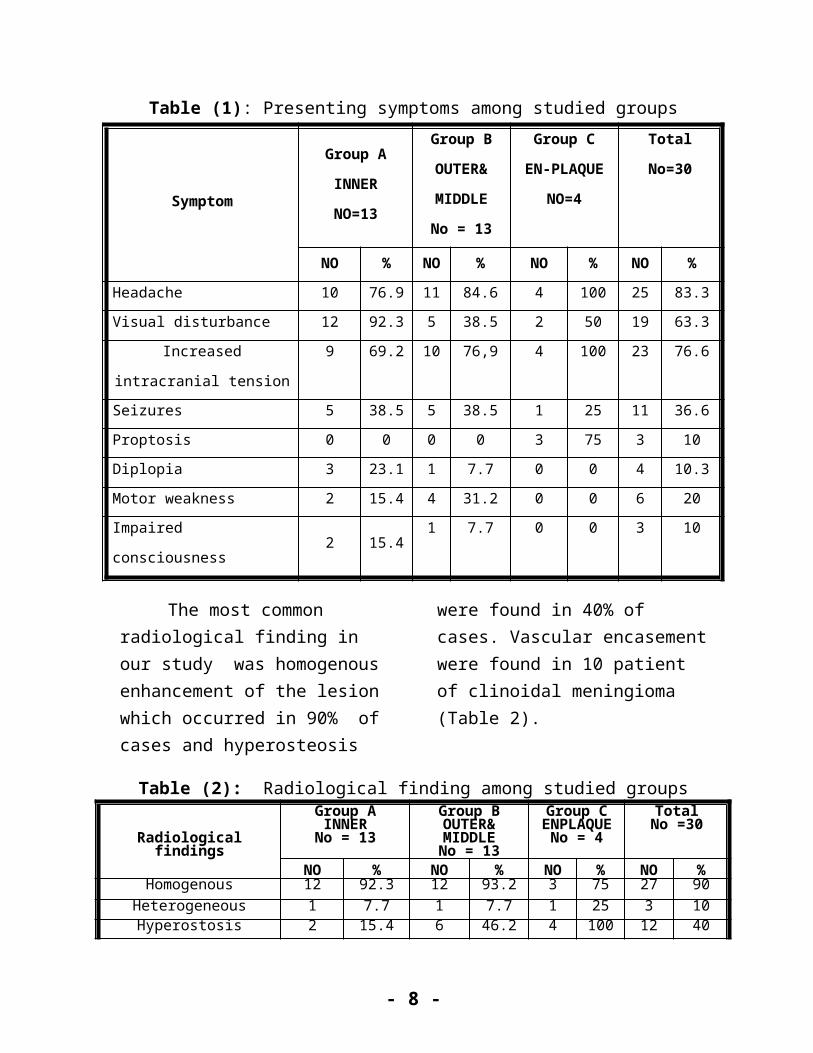
The most common radiological finding in our study was homogenous enhancement of the lesion which occurred in 90% of cases and
hyperosteosis were found in 40% of cases. Vascular encasement were found in 10 patient of clinoidal meningioma (Table 2).
Table (2): Radiological finding among studied groups
Radiological findings
Group AINNERNo = 13
Group BOUTER& MIDDLENo = 13
Group CENPLAQUE
No = 4
TotalNo =30
NO % NO % NO % NO %Homogenous 12 92.3 12 93.2 3 75 27 90
Heterogeneous 1 7.7 1 7.7 1 25 3 10Hyperostosis 2 15.4 6 46.2 4 100 12 40
Edema 5 38.5 7 53.8 2 50 14 46.6Calcification 3 23.1 5 38.5 1 25 9 30
Vessels 10 76.9 1 7.7 0 0 11 36.6
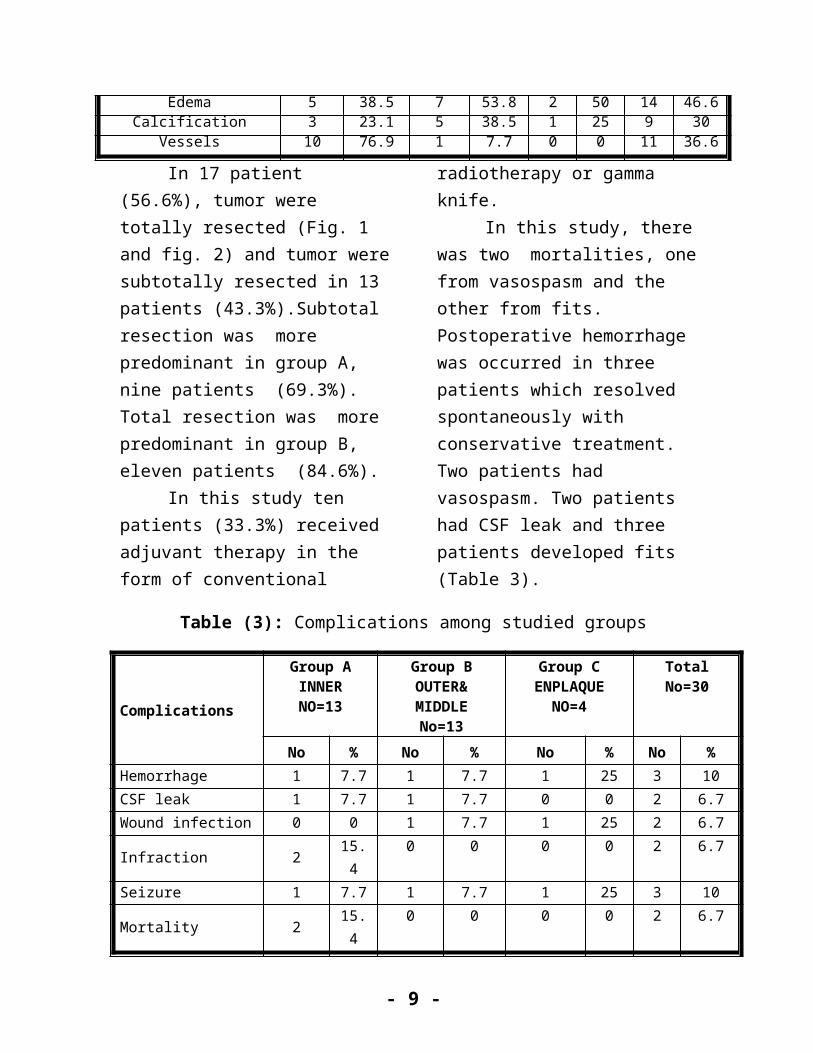
In 17 patient (56.6%), tumor were totally resected (Fig. 1 and fig. 2) and tumor were subtotally resected in 13 patients (43.3%).Subtotal resection was more predominant in group A, nine patients (69.3%). Total resection
was more predominant in group B, eleven patients (84.6%).
In this study ten patients (33.3%) received adjuvant therapy in the form of conventional radiotherapy or gamma knife.
- 6 -
In this study, there was two mortalities, one from vasospasm and the other from fits. Postoperative hemorrhage was occurred in three patients which resolved spontaneously
with conservative treatment. Two patients had vasospasm. Two patients had CSF leak and three patients developed fits (Table 3).
Table (3): Complications among studied groups
Complications
Group AINNERNO=13
Group BOUTER& MIDDLE
No=13
Group CENPLAQUE
NO=4
TotalNo=30
No % No % No % No %Hemorrhage 1 7.7 1 7.7 1 25 3 10CSF leak 1 7.7 1 7.7 0 0 2 6.7Wound infection 0 0 1 7.7 1 25 2 6.7Infraction 2 15.4 0 0 0 0 2 6.7Seizure 1 7.7 1 7.7 1 25 3 10Mortality 2 15.4 0 0 0 0 2 6.7
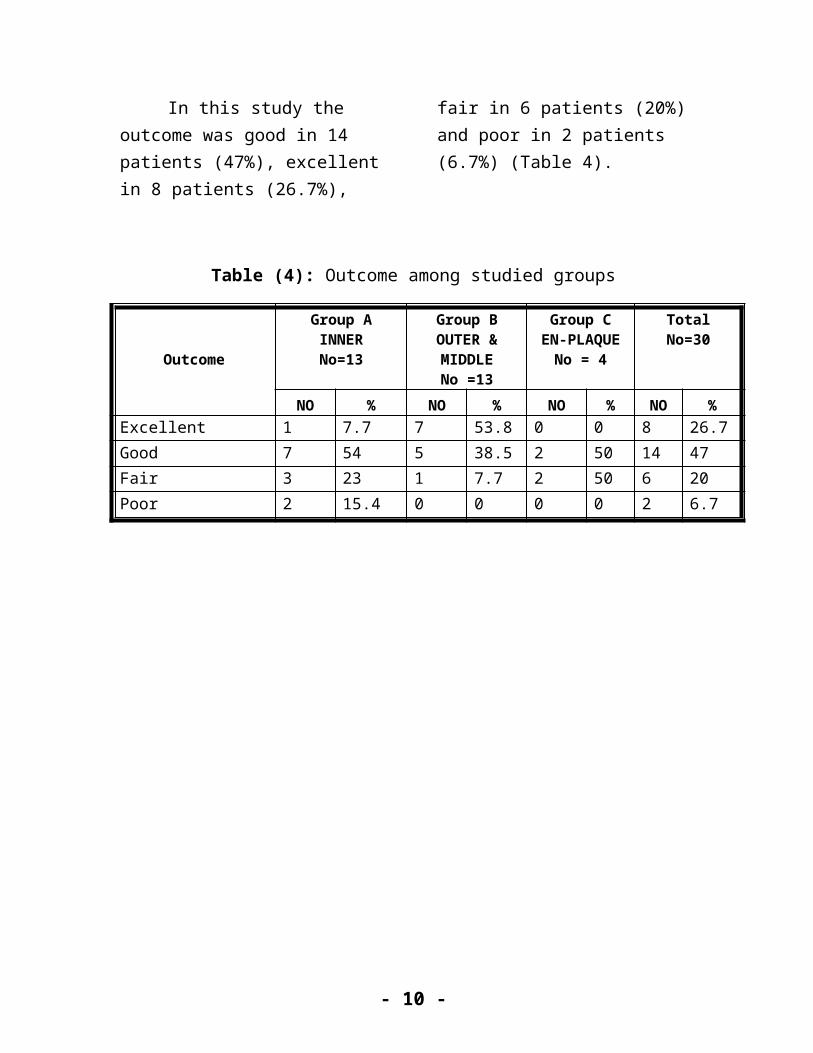
In this study the outcome was good in 14 patients (47%), excellent in 8 patients (26.7%), fair in 6 patients
(20%) and poor in 2 patients (6.7%) (Table 4).
Table (4): Outcome among studied groups
Outcome
Group AINNERNo=13
Group BOUTER & MIDDLE
No =13
Group CEN-PLAQUE
No = 4
TotalNo=30
NO % NO % NO % NO %Excellent 1 7.7 7 53.8 0 0 8 26.7Good 7 54 5 38.5 2 50 14 47Fair 3 23 1 7.7 2 50 6 20Poor 2 15.4 0 0 0 0 2 6.7
- 7 -
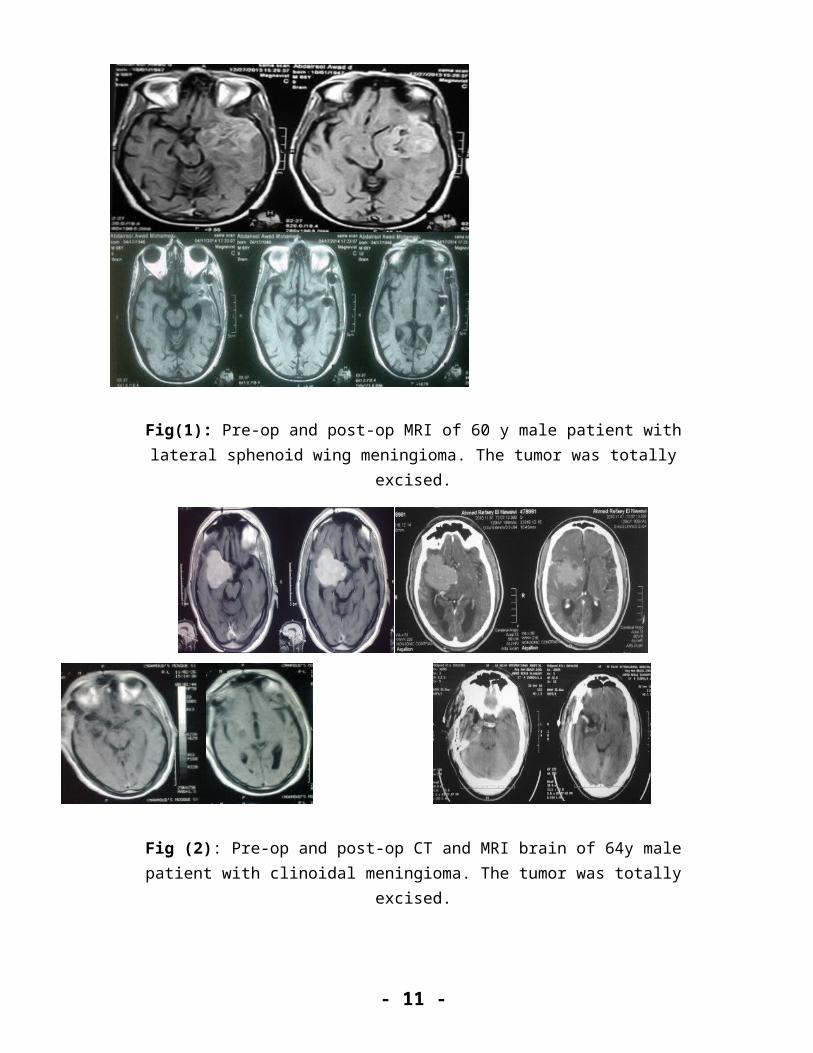
Fig(1): Pre-op and post-op MRI of 60 y male patient with lateral sphenoid wing meningioma. The tumor was totally excised.
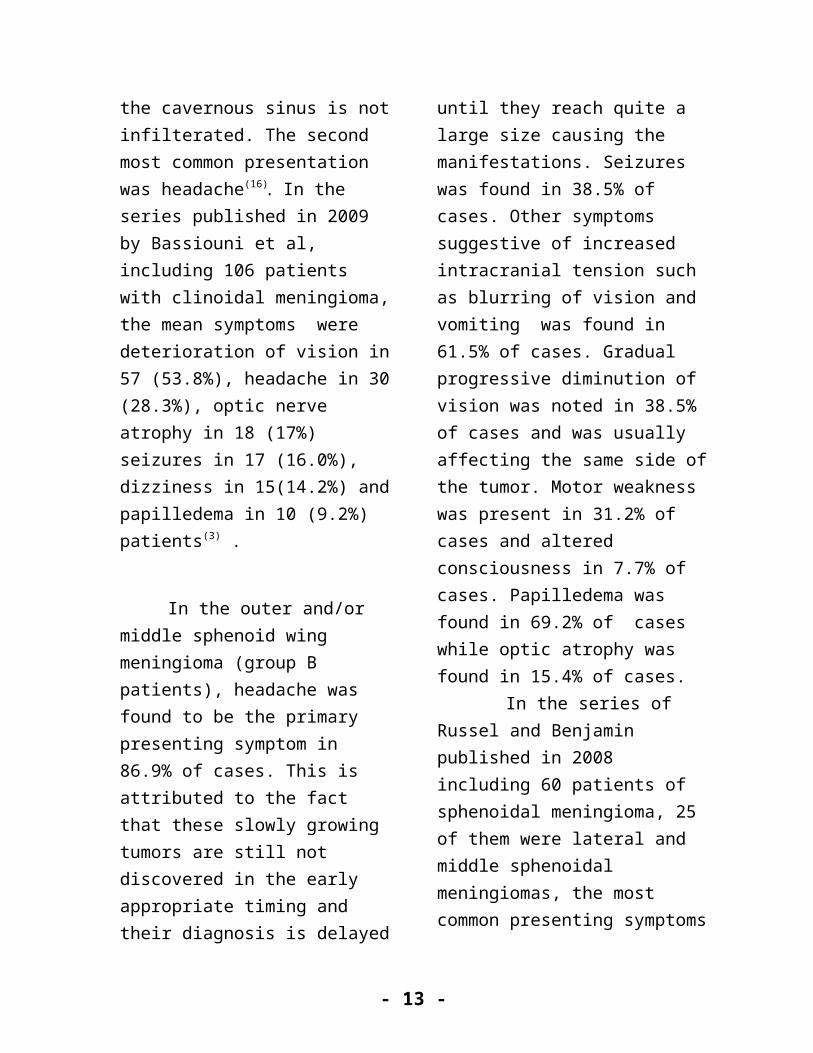
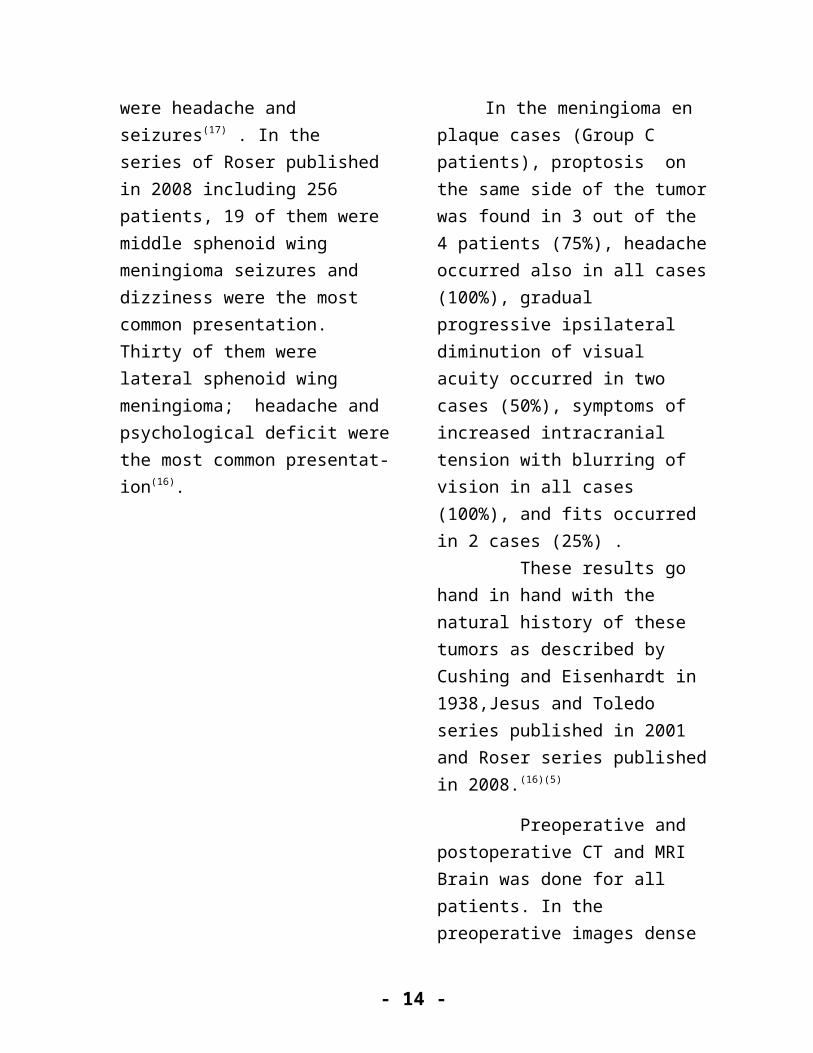
Fig (2): Pre-op and post-op CT and MRI brain of 64y male patient with clinoidal meningioma. The tumor was totally excised.
DISCUSSION
Sphenoid wing is the most common location for skull base meningiomas. Meningiomas involving the sphenoid wing are mostly
histopathologically benign(6). With the advancements in neuroradiological studies, one can better appreciate how difficult these meningiomas are to cure. Surgical management of these cases becomes increasingly
- 8 -
challenging as the site moves inwards from the pterion to the clinoid(8)
In the medial or clinoidal menengioma (Group A patients), progressive visual deterioration was found to be the primary presenting symptom in 92.3% of cases. This visual deterioration was gradual, progressive and asymmetrical, always affecting first the ipsilateral side. Headache also occurred in 76.9% of cases of this group. This headache was gradual progressive and usually radiated frontally or temporally .Other symptoms of group A included, blurring of vision, vomiting, seizures and motor weakness. Fundus abnormalities, papilledema was found in 38.4% of cases and optic atrophy was found in 53.% of cases .
Those results were similar to those of other series where visual deterioration was the most frequent presentation. In the series of Roser published in 2008 including 256 patients, 174 of them were medial sphenoid wing meningioma. Visual disturbance was the most common presentation account for 66.7% if the cavernous sinus is infilterated and 60.9% if the cavernous sinus is not infilterated. The second most common presentation was headache(16). In the series published in 2009 by Bassiouni et al, including 106 patients with clinoidal meningioma, the mean
symptoms were deterioration of vision in 57 (53.8%), headache in 30 (28.3%), optic nerve atrophy in 18 (17%) seizures in 17 (16.0%), dizziness in 15(14.2%) and papilledema in 10 (9.2%) patients(3) .
In the outer and/or middle sphenoid wing meningioma (group B patients), headache was found to be the primary presenting symptom in 86.9% of cases. This is attributed to the fact that these slowly growing tumors are still not discovered in the early appropriate timing and their diagnosis is delayed until they reach quite a large size causing the manifestations. Seizures was found in 38.5% of cases. Other symptoms suggestive of increased intracranial tension such as blurring of vision and vomiting was found in 61.5% of cases. Gradual progressive diminution of vision was noted in 38.5% of cases and was usually affecting the same side of the tumor. Motor weakness was present in 31.2% of cases and altered consciousness in 7.7% of cases. Papilledema was found in 69.2% of cases while optic atrophy was found in 15.4% of cases.
In the series of Russel and Benjamin published in 2008 including 60 patients of sphenoidal meningioma, 25 of them were lateral and middle sphenoidal meningiomas, the most common presenting symptoms were
- 9 -
headache and seizures(17) . In the series of Roser published in 2008 including 256 patients, 19 of them were middle sphenoid wing meningioma seizures and dizziness were the most common presentation. Thirty of them were lateral sphenoid wing meningioma; headache and psychological deficit were the most common presentat-ion(16).
In the meningioma en plaque cases (Group C patients), proptosis on the same side of the tumor was found in 3 out of the 4 patients (75%), headache occurred also in all cases (100%), gradual progressive ipsilateral diminution of visual acuity occurred in two cases (50%), symptoms of increased intracranial tension with blurring of vision in all cases (100%), and fits occurred in 2 cases (25%) . These results go hand in hand with the natural history of these tumors as described by Cushing and Eisenhardt in 1938,Jesus and Toledo series published in 2001 and Roser series published in 2008.(16)(5)
Preoperative and postoperative CT and MRI Brain was done for all patients. In the preoperative images dense enhancement was found in 27 patients (90%) and was caused by the lack of blood brain barrier in these extra-axial tumors. The margins of the enhancing mass are sharply demarcated, with broad base against
bone of the sphenoid ridge and a creeping dural tail, the latter of which is highly suggestive and specific(7). In our study we couldn’t find a direct correlation between the dense enhancement and the vascularity of the meningioma. Some of the densely enhancing masses were not found as hypervascular as expected. This support the fact that enhancement depend mainly on lack of blood brain barrier.
Pterional approach was the most common approach used in this study, used in 26 pateints representing 86,7%. This was due to that this approach offers several advantages. It permited a direct approach to the dural attachment of the tumor along the sphenoid ridge and thereby allows for early devascularization. Wide opening of the sylvian fissure improves surgical access and optimizes visualization of all critical neurovascular structures (the MCA, ACA, ICA, and anterior optic pathways). Intradural or extradural removal of hyperostotic bone of the sphenoid wing including the anterior clinoid process could be performed. Good relaxation of the brain was achieved by opening the basal cisterns and releasing the CSF. This maneuver avoided application of self-retaining spatulas in many cases(9). This was also the opinion of Pamir et al in the series published in 2008 and Bassiouni et al in 2009.(12),(3)
- 10 -
The size of the tumor was calculated on the maximum diameter of tumor obtained from CT scans or MR images. In Group A (the clinoidal variety), from the 13 cases studied, the tumor was small in three, large in eight and giant in two cases. Concerning Group B, from the 13 cases harboring an outer or middle or whole sphenoid masses one was small, 7 were large and the remaining 5 masses were giant. In Group C, the en plaque variety, 2 cases were large, one was small and one was giant. In this study, we found a significant negative correlation between degree of resection and tumour location (as degree of resection decreases in more medial tumors). Also, there was significant negative correlation between degree of resection and vascular encasement, as more resection can be achived in less vascular encasement of the tumors.
In Group A (the clinoidal variety), 13 cases were operated in the study. Total resection was achieved in 4 cases (30.7%) and subtotal resection was done in 9 patients (69.3%). The prognosis was excellent in 1 case (7.7%), good in 7 cases (54%), fair in 3 cases (23%) and poor in 2 cases (15.4%). Two patients died post operatively one from vasospasm and the other from post operative fits. Post operative hemorrhage was recorded in one patients (7.7%). He was managed conservatively. Two patients (15.4%) developed infarction (vasospasm) one of them died and the other had hemiplegia. CSF leak occurred in one patient (7.7%). It stopped with the use of lumbar drain. One patient had fits. He needed mechanical ventilation and died later.
The extent of resection of clinoidal meningiomas varies in different series. The rates of total resection vary between 43 and 91%. Table (5) shows the different reported series of clinoidal meningiomas.(9)
- 11 -
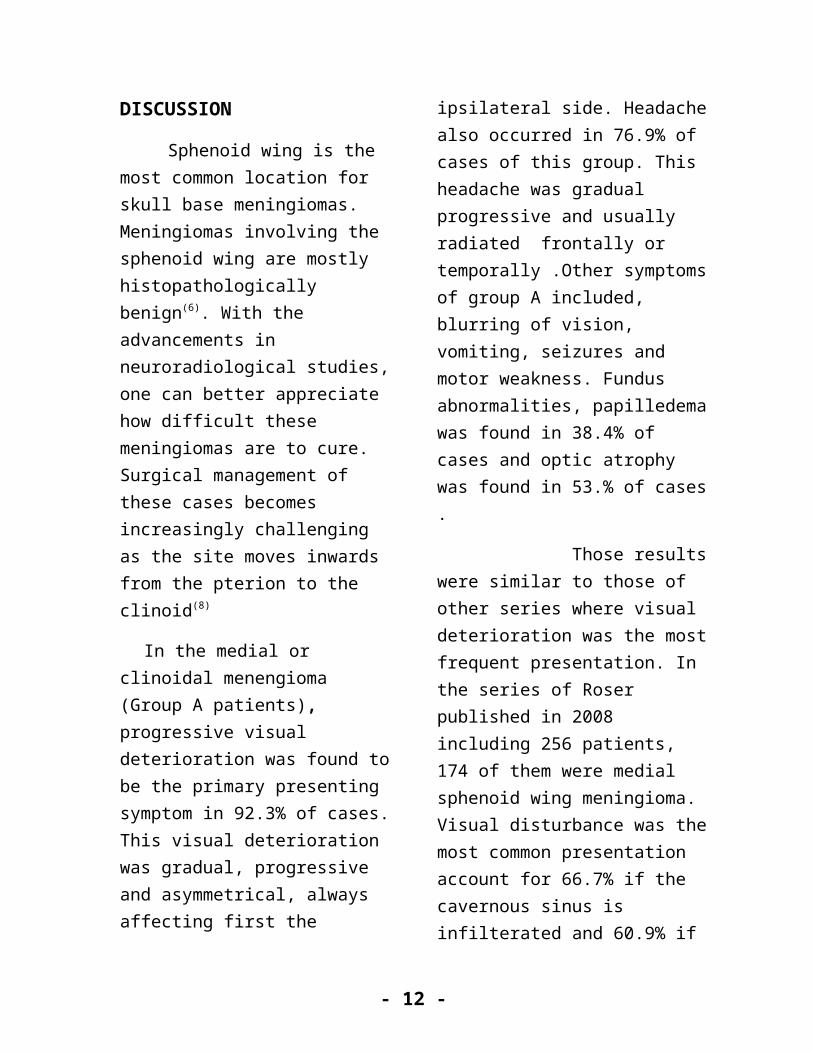
Table (4): Different reported series of clinoidal meningiomas(9)
Recurrence/progression
-%
Mean follow
up
Major morbidity-%
Extent of resection-%
Improvement of vision %
Cs involvement
Mortality-%
No of patients
Series
457 m8Gross total 83838824Almefty, 1990
2653 m12Gross total54.539.41533Puzzilli et al, 1999
03 m0Gross total66.610006Day,2000
226 m12Gross total 7023560Goel et al,2000
037 m0Gross total 877514016Lee et al,2001
042 m11.5Gross total 777123026Tobias et al,2003
236.5 y7.4Gross total 43640108Nakamura et al,2006
9.339 m18.6Gross total 91852043Russel et al,2008
912.8 y18Gross total 696331035Pamir et al,2008
6.917Gross total 5940291.9106Bassiouni et al,2009
In this study, lateral and/or middle sphenoidal meningioma group, aggressive bony removal was performed to the hyperostotic bone. At the end of the procedures, the dural attachment was coagulated. Gross total resection was achieved in 11patients (84.6%), while in 2 patients (15.4%) subtotal resection was performed. In the latter two cases, total removal was not achieved as the MCA or one of its branches was encased by the tumor. The outcome was excellent in 7 patients (53.8%), good in 5 patients (38.5%), and fair in 1 patient (7.7%). Post operative hemorrhage was recorded in one patient (7.7%). It did not need surgical intervention. Post operative fits
occured in one patient (7.7%) and also wound infection occurred in one patients (7.7%). CSF leak occurred in one patient (7.7%) and stopped with repeated dressing. Brotchi and Bonnal in 2006 reported the same results with nine patients(4). In the series of Morokkoff et al published in 2008 including 163 cases, there was no mortality, they had complication rate of 9.4% and 1.7% developed new neurological deficit of their cases(11).
In this study, four cases with meningioma en plaque were operated. Two of them were totally excised (50%) and two patients were subtotally excised. The surgical outcome was fair in 2 cases and good in 2 cases. There was no mortality,
- 12 -
one patient complicated with hemorrhage post operatively resolved with serial follow up, and another one patient complicated with fits. Superficial wound infection occurred in one patient. It resolved with repeated dressing. Proptosis improved partially in all patients. In the series of Roser published in 2008, including 86 patients, gross total resection was achived in 38% of cases with recurrence rate 32%. In his series 5 patients (7.1%) had hygroma, 5 patients had hydrocephalus, infarction occurred in 2 patients and hemorrhage occurred in 2 patients. One patient died from pulmonary embolism(16)
CONCLUSION:
The surgical decision for these tumors should depends primarily on the clinical finding of the patient and radiological finding of the tumor. Location of the meningioma is an important factor determining the degree of tumor resectability.
Encasement of ICA and / or MCA and their branches together with CS invasion and extension into superior orbital fissure are limiting factors for radical removal.
Tumors of the outer third of the sphenoid ridge and many small middle wing tumors are essentially convexity meningiomas with regard to clinical presentation and surgical treatment.
The objective in every procedure, should be total removal of the meningioma.
In the clinoidal variety, clinoidal masses not attached to the carotid artery branches, total resection is recommended. For clinoidal masses attached to the carotid or cavernous sinus subtotal resection is recommended.
For en plaque variety, an extensive resection of tumor, dura and bone will lead to good tumor control with minimal morbidity, good cosmetic and functional results.
Radiotherapy and radiosurgery play an increasing role in controlling residual or progressive disease
REFERENCES:
1-Al-Mefty O, ed. Meningiomas. New York: Raven Press Ltd., Krisht A F. Clinoidal Meningiomas. In: DeMonte F, McDermot M W, Al-Mefty O, eds. AL – Meftys, Meningiomas. Second edition. Pheladelphia, thieme; 24, pp. 228-256, 1991
2-Al-Mefty O.Clinoidal meningiomas. Neurosurg; 73 (6): 840 – 849, 1990
3-Bassiouni H, Asgari S, Sandalcioglu IE, Seifert V, Stolke D and Marquardt G. Anterior clinoidal meningiomas: functional outcome after microsurgical resection in a consecutive series of 106 patients: clinical article. J Neurosurg; 111(5): 1078-1090, 2009.
4-Brotchi J and Pirotte B. Sphenoid wing meningiomas. In: Sekhar LN. Fessler
- 13 -
RG, eds. Atlas of Neurosurgical Techniques: Brain. New York, NY: Thieme; pp 623-632, 2006.
5-De Jesus O and Toledo M M. Surgical Management of Meningioma en Plaque of the Sphenoid Ridge. Surg Neurology; 55: 265–9, 2001.
6- Delfini R. Management of Tumours of Middle Fossa , In: Sindou M: Practical Handbook of neurosurgery. 1sted, New York: Springer Wien; vol2 , 6:95-111, 2009.
7-Dillon WP and Uzelac A. Modern Imaging Techniques for Meningiomas. In: De Monte F McDermot MW,Al-Mefty O,eds. AL-Meftys, Meningiomas. Sec-ond edition. pheladelphia, thieme; 13, pp107-118, 2010.
8-Greenberg MS. Tumour, In: Greenberg M.S.: Handbook of neurosurgery. 7th ed., New York : Thieme; vol 1, 21, pp 613-620, 2010.
9-Krisht AF. Clinoidal meningiomas. In: DeMonte F, McDermot MW, Al-Mefty O, eds. AL-Mefty, sMeningiomas. Second edition pheladelphia, thieme; (24), pp. 228-237, 2010.
10-Mariniello G, deDivitiis O, Seneca V, Maiuri F. Classical pterional compared to the extended skull base approach for the removal of clinoidal meningiomas. Journal of Clinical Neuroscience; 19 : 1646–1650, 2012.
11-Morokoff AP, Zaubermanj, Black PM: Surgery for convexity meningiomas.
Neurosurgery 63 (3) : 427 - 433, discussion; 433-434, 2008.
12-Pamir MN, Belirgen M, Ozduman K, KiliT and Ozek M. Anterior clinoidal meningiomas: analysis of 43 consecutive surgically treated cases. Acta Neurochir (Wien); 150 (7) : 625 - 635, discussion 635-636, 2008.
13- Pirotte B and Brotchi J. Lateral and Middle Sphenoid Wing Meningiomas. In: Sekhar LN. Fessler RG, eds. Atlas of Neurosurgical Techniques: Brain. New York, NY: Thieme; (39), pp 623-632, 2006.
14-Rhoton AL. The sellarregion. Neurosurgery; 51 [Suppl 1] : 335–374, 2002.
15-Rockhill J, Mrugala M and Chamberlain M.: Intracranial meningiomas: an overview of diagnosis and treatment. Neurosurg Focus; 23(4): 1-7, 2007.
16-Roser F. Sphenoid Wing Meningiomas. In: Ramina R, Aguiar PH, Tatagiba M, eds Samii’s Essentials in Neuro-surgery. Verlag Berlin Heidelberg, springer; (11): 99-108, 2008.
17-Russell SM, Benjamin V. Medial sphenoid ridge meningiomas: classification, microsurgical anatomy, operative nuances, and long-term surgical outcome in 35 consecutive patients. Neuro-surgery; 62 (3, supp 1) : 38-50, discussion 50, 2008.
- 14 -