Embed Size (px)
Citation preview

1
Surgical Meeting
Cardiorespiratory focus
Carlos F. Agudelo
VFU – Brno
Cardiac arrhythmias
Carlos F. Agudelo
VFU – Brno
The arrhythmia
Importance
-Decrease in cardiac output: hypotension a decreased tissue and coronary perfusion
-Sign of extra-cardiac disease (trauma, inflammation, cancer)
-Sudden death
The arrhythmia
- Signalement
-Breed:
WHWT, Springer Spaniel, Boxer, Doberman, etc.
-Colour
- History
Exercise intolerance
Dyspnoea
Palpitations
Fanting episodes
Long term cardiac disease (drugs)
Trauma
Inflammation
Cancer (therapy)
- Clinical
Hypotension
Pale MM
Irregular heart beats
Pulse deficit
Sudden death
The arrhythmia
Ventricular arrhythmia
-Cardiomyopathy
-Myocarditis / endocarditis
-Myocardial hypoxia
-Congenital heart disease
-Digitalis intoxication
-Electrolytic abnormalities
-Hypothermia
-Systemic disease
Supraventricular arrhythmia
-Enlargement of the atria
-Myocarditis / endocarditis
-Ongoing heart disease
-Ischemic foci in the atria
-Drugs (digitalis, anesthetics)
-Abnormal AV pathways
-Systemic disease
The arrhythmia
Diagnosis
ECG Holter–event recorders
2
The arrhythmia
Diagnosis
Atropine SC, IM, IV: 0.02–0.04 mg/kg
The arrhythmia
Classification according to…
1-Rhythm
2-Origin and transmission
3-Time interval
4-Frequency
5-Aetiology
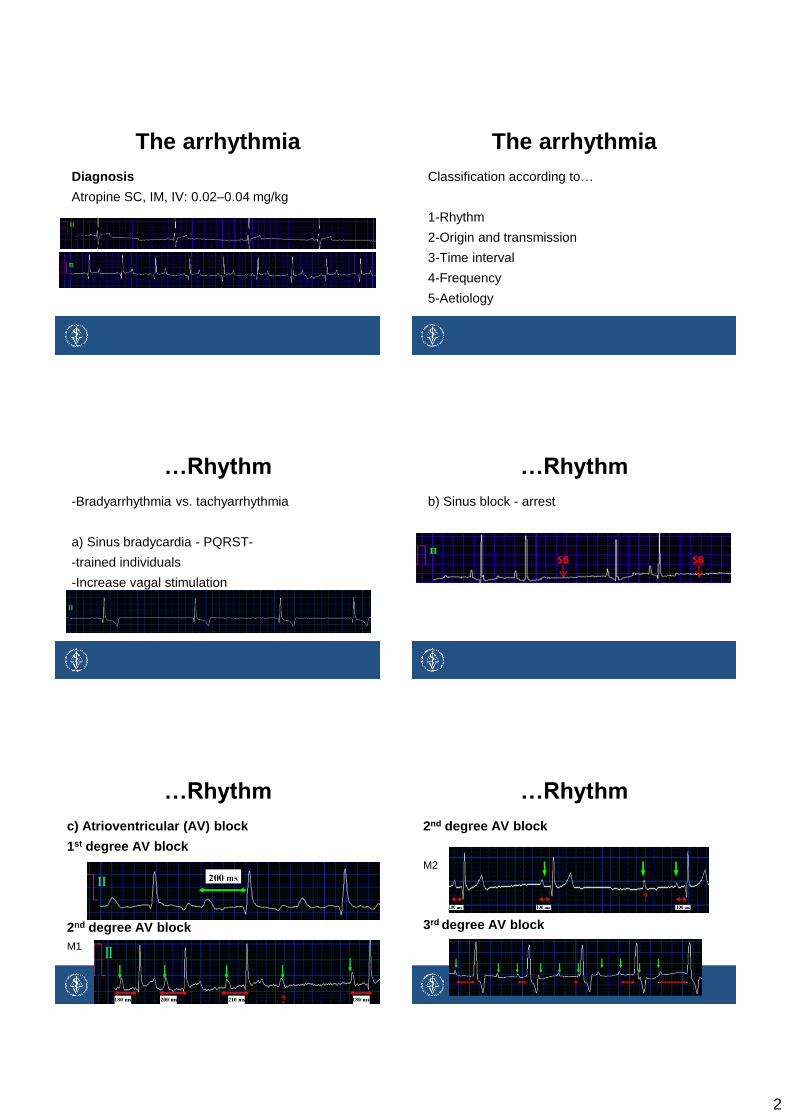
…Rhythm
-Bradyarrhythmia vs. tachyarrhythmia
a) Sinus bradycardia - PQRST-
-trained individuals
-Increase vagal stimulation
…Rhythm
b) Sinus block - arrest
…Rhythm
c) Atrioventricular (AV) block
1st degree AV block
2nd degree AV block
M1
…Rhythm
2nd degree AV block
M2
3rd degree AV block

3
…Rhythm
Tachycardia
a) Sinus tachycardia
…Rhythm
b) Atrial tachycardia
c) Ventricular tachycardia
…Origin and transmission
a) Supraventricular
Atrial premature complexes
Atrial fibrillation
…Origin and transmission
b) Nodal – junctional – escape complexes
Nodal complex
Nodal rytmus
…Origin and transmission
c) Ventricular Ventricular tachycardia Slow vent. tachycardia (accelerated idioventricular rhythm) Idioventricular rhythm
…Time interval…
-Premature
-Escape (after pauses)
4
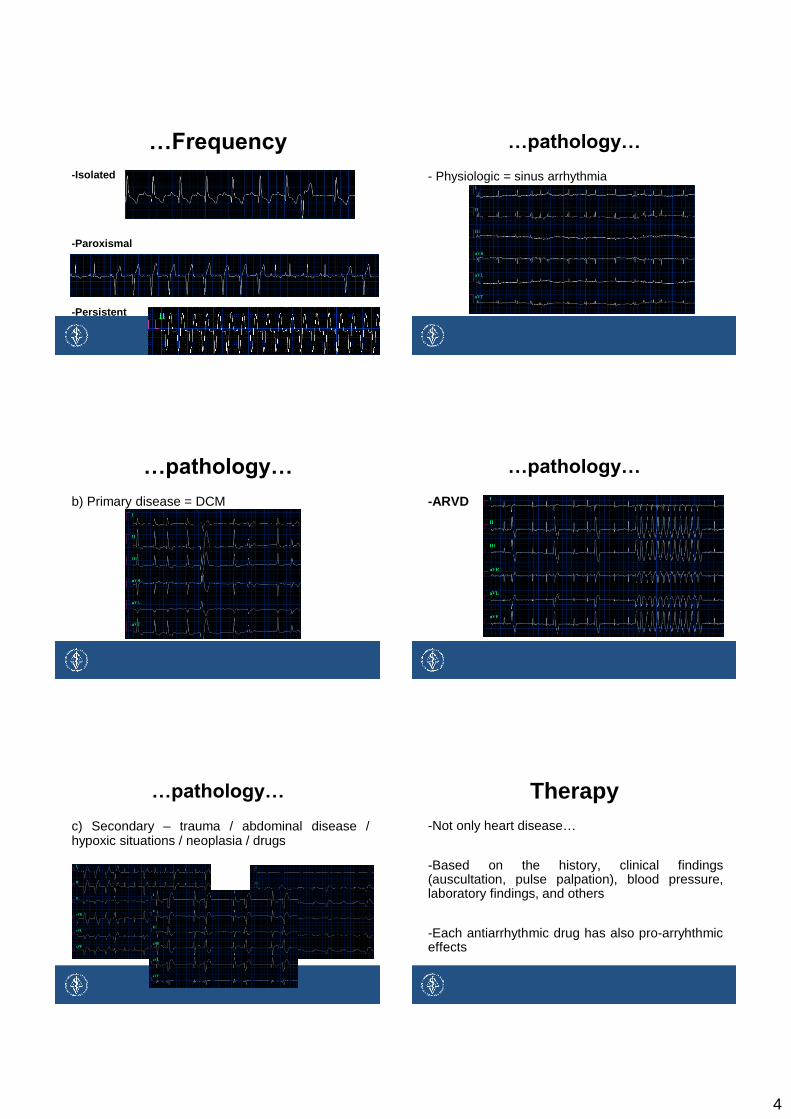
…Frequency
-Isolated
-Paroxismal
-Persistent
…pathology…
- Physiologic = sinus arrhythmia
…pathology…
b) Primary disease = DCM
…pathology…
-ARVD
…pathology…
c) Secondary – trauma / abdominal disease / hypoxic situations / neoplasia / drugs
Therapy
-Not only heart disease…
-Based on the history, clinical findings (auscultation, pulse palpation), blood pressure, laboratory findings, and others
-Each antiarrhythmic drug has also pro-arryhthmic effects
5
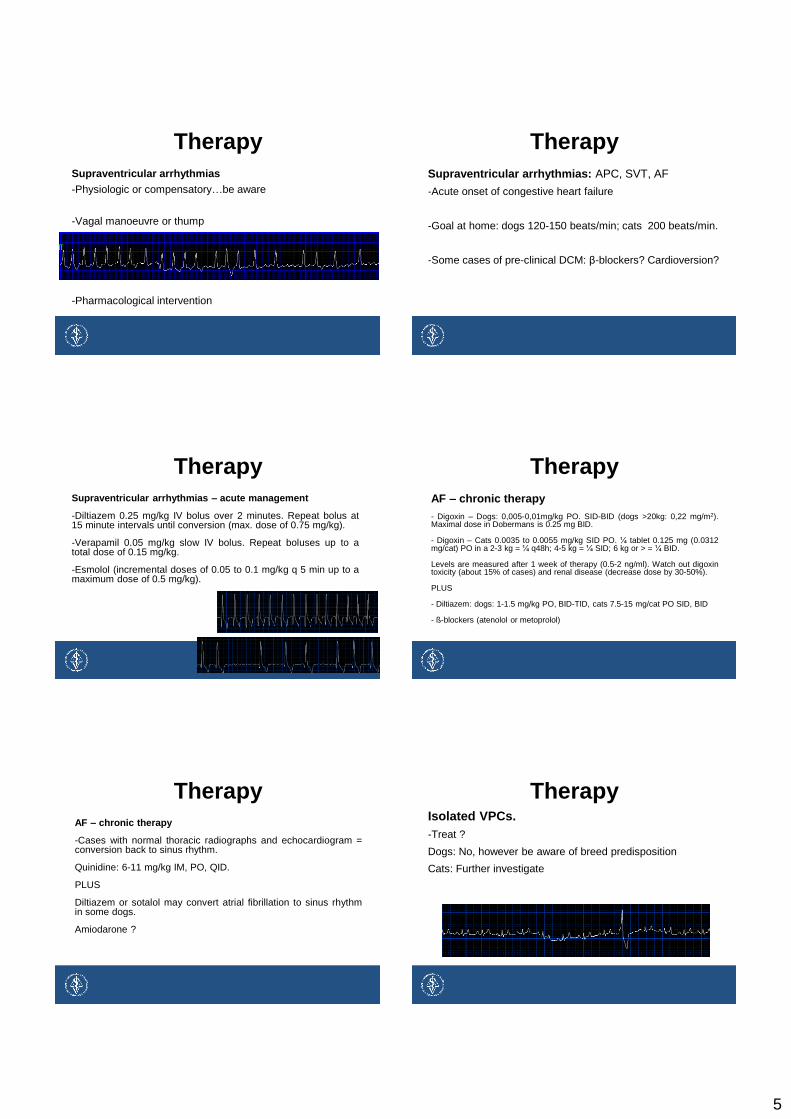
Therapy
Supraventricular arrhythmias
-Physiologic or compensatory…be aware
-Vagal manoeuvre or thump
-Pharmacological intervention
Therapy
Supraventricular arrhythmias: APC, SVT, AF
-Acute onset of congestive heart failure
-Goal at home: dogs 120-150 beats/min; cats 200 beats/min.
-Some cases of pre-clinical DCM: β-blockers? Cardioversion?
Therapy
Supraventricular arrhythmias – acute management
-Diltiazem 0.25 mg/kg IV bolus over 2 minutes. Repeat bolus at 15 minute intervals until conversion (max. dose of 0.75 mg/kg).
-Verapamil 0.05 mg/kg slow IV bolus. Repeat boluses up to a total dose of 0.15 mg/kg.
-Esmolol (incremental doses of 0.05 to 0.1 mg/kg q 5 min up to a maximum dose of 0.5 mg/kg).
Therapy
AF – chronic therapy
- Digoxin – Dogs: 0,005-0,01mg/kg PO. SID-BID (dogs >20kg: 0,22 mg/m2). Maximal dose in Dobermans is 0.25 mg BID.
- Digoxin – Cats 0.0035 to 0.0055 mg/kg SID PO. ¼ tablet 0.125 mg (0.0312 mg/cat) PO in a 2-3 kg = ¼ q48h; 4-5 kg = ¼ SID; 6 kg or > = ¼ BID.
Levels are measured after 1 week of therapy (0.5-2 ng/ml). Watch out digoxin toxicity (about 15% of cases) and renal disease (decrease dose by 30-50%).
PLUS
- Diltiazem: dogs: 1-1.5 mg/kg PO, BID-TID, cats 7.5-15 mg/cat PO SID, BID
- ß-blockers (atenolol or metoprolol)
Therapy
AF – chronic therapy
-Cases with normal thoracic radiographs and echocardiogram = conversion back to sinus rhythm.
Quinidine: 6-11 mg/kg IM, PO, QID.
PLUS
Diltiazem or sotalol may convert atrial fibrillation to sinus rhythm in some dogs.
Amiodarone ?
Therapy Isolated VPCs.
-Treat ?
Dogs: No, however be aware of breed predisposition
Cats: Further investigate

6
Therapy
Ventricular trigeminy – duplets and triplets.
Treat ? +/-
Yes: clinical signs or recent or known cardiac disease (predisposition)
No: without findings and normal heart frequency. Further investigation
Therapy
Monomorphic slow ventricular tachycardia (<180 beats/min) – ventricular bigeminity.
Treat ?
Yes: digoxin, clinical signs or recent or known cardiac disease (predisposition)
Therapy
Polymorphic ventricular tachycardia.
Treat ?
Yes
-Several locations. Be aware of worsening at any moment
Therapy
Ventricular tachycardia (heart frequence higher than 200 beats/min)
Yes
-Risk for sudden death
Therapy
Persistent ventricular tachycardia
Yes
-General myocardial dysfunction
-Sudden death
-Secondary pathology
Therapy
Ventricular tachycardia
-Lidocain: bolus 2,2 mg/kg slow IV. Max. 4 applications (total 8,8 mg/kg). Continue CRI (40-75[100] μg/kg/min)
-If ineffective = combination of different antiarrhythmic drugs

7
Therapy
Ventricular tachycardia
If ineffective…
β-blockers
Esmolol: Bolus 50-100 μg/kg IV up to 500 μg/kg. Continue CRI 50-200 μg/kg/min (Tilley et al 2010).
Amiodarone: Bolus 3-5 mg/kg IV. Continue CRI 20-150 μg/kg/min (Ware et al 2011).
Therapy
*Ventricular tachycardia – chronic oral therapy
Metoprolol: 0,2-0,5 mg/kg BID
Amiodarone: 8 to 15 mg/kg BID for 7 days, then 5 to 10 mg/kg BID
Sotalol: 1-3,5 mg/kg PO, BID.
Atenolol: 0.75-1.5 mg/kg BID alone or in combination with mexiletinem (5-8 mg/kg BID-TID).
Therapy
Ventricular Fibrillation
-Immediate electrical defibrillation
-Drug therapy alone (virtually ineffective)
*Intravenous amiodarone (3-5 mg/kg) and magnesium (0.15-0.3 mEq/kg)
*Low doses of epinephrine
Therapy
Bradyarrhyhtmia.
Low probability of pacemaker implantation…
-sinus bradycardia,
-sinus arrest or block
-1st degree and some cases of 2nd AV blocks
Therapy
Bradyarrhyhtmia.
High probability of pacemaker implantation…
-Advanced 2nd AV block
-3rd AV block
-Sick sinus syndrome
Therapy
Bradyarrhyhtmia
-Negative = (no reaction) = pacemaker implantation
-Positive or limited pacemaker implantation
-primary problem
Salbutamol: 0,05 mg/kg PO, BID
Aminophillyn: 5-10 mg/kg PO, TID-QID (extended release)

8
Questions?