Embed Size (px)
DESCRIPTION
Surgery
Citation preview

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 1/45
SURGICAL FACTS FOR THE EXAM(Derived mostly from past exam questions)
How do you examine a path pot?
• What is the organ?
•
Where is the pathological process?• What is the pathological process?
o Use pathology terms & definitions
o Mechanisms – cellular, tissue, organ or systemic
• Aetiologic clues
• Sequelae & complications
• Misc processes! related and incidental
• Differential diagnoses
How do you describe a lump?
1. Size
• ! size! more likely it is to be malignant
• Multiple bony lumps is suggestive of multiple hereditary exostosis & ollier’s disease
2. Site
• Describe precisely in exact anatomical terms, measuring distances from bony points
• Closer to joint (ie metaphysis)! more likely to be a tumour (benign or malignant)
3. Shape
• Remember it is 3-Dimensional
4. Surface
• May be smooth or irregular, or a mixture of surfaces
5. Margin/edges
• Well defined margin! likely to be benign
• Irregular margin! likely to be malignant tumour, fracture callus or inflammatory new bone
6. Tenderness
• Suggestive of active inflammation, recent callus, rapidly growing sarcoma or tumourimpinging on surrounding structures
7. Composition
7a. Consistency
• Stony hard : not indentable
• Rubbery : hard to firm, but slightly squashable
• Spongy : soft & very squashable
• Soft : squashable & no resilienc

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 2/45
7b. Fluctuation (fluid-filled)
• Can only be elicited by feeling at least two other areas of the lump whilst pressing on a third – if 2 areas on opposite aspects of the lump bulge when a 3
rd area is pressed in, the lump
fluctuates & contains fluid
7c. Fluid thrill
• Detected by tapping one side of the lump & feeling the transmitted vibration when it reaches
the other side
• Place patient’s/assistant’s hand on lump midway between your percussing & palpating hands
7d. Transillumination (fluid-filled)
• Light will pass easily thru clear fluid (water, serum, lymph, plasma), but not thru solid tissuesor opaque fluids (eg blood)
• Place small torch behind lump in dark room & shine towards tour eye. If it glows red it
transilluminates.
7e. Resonance
• Solid & fluid-filled lumps are dull to percussion
• Gas-filled lumps are resonant
7f. Pulsatility
• Pulsation can be caused by the lump itself (true expansile pulsation, eg aneurysm or vascular
tumour) or by transmitted to lump from elsewhere
• Place a finger of each hand on opposite sides of the lump :
o Fingers being pushed apart! true expansile pulsation
o Fingers being pushed in same direction (upwards)! transmitted pulsation
•
Listen for bruits – vascular lumps may have a systolic bruit• Check neurovasculature of limb distal to the lump
8. Reducibility
• Compress lump to see if reducible, a feature of herniae
• If patient coughs, the lump may return &/or expand (cough impulse)
7. Mobility/fixation of lump & its tissue layer
• Skin! lump moves when skin moves (eg sebaceous cyst, epidermoid cyst or papilloma)
• Subcutaneous tissue! skin can be moved over the lump (eg neurofibroma, lipoma)
• Muscle/tendon ! contraction of muscle limits the lump’s mobility (eg tumour, haematoma)
•
Nerve! pressing on the lump may elicit pins and needles in nerve distribution; Lump cannot be moved in the longitudinal axis but it can be moved in the transverse axis
• Bone! lump is immobile, tethered (eg callus, subperiosteal haematoma, 20 ossification
centre, tumour)
10. Overlying skin
• Signs of inflammation : redness (rubor), heat (callor), swelling (tumor), tenderness (dolor)

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 3/45
• Colour & texture, eg smooth & shiny
11. Regional lymph nodes
• Check regional LNs & other major LN groups (cervical, axillary & groin)
12. Other
• Muscle wasting
• Joint movements (eg " ROM due to mass)
• Gait (? Limp)
• General physical examination : cachexia, SOB/cough/haemoptysis etc
ORTHOPAEDIC SURGERY
How do you report fractures to an orthopaedic registrar?
1.
Name & details of patient & technique (types of views performed & position)2. Anatomical site : which side, which bone, where it is (proximal #, mid-shaft or distal #)
3. Open or closed (gas in soft tissue may indicate open # or infection)4. Appearance of fracture line
a) Transverse/oblique/spiral/comminuted/greenstick b) Complete or incomplete
5.
Degree of displacement or angulation of the distal segment
o Undisplaced = fragments in " anatomical position, reduction not required
o Displacement is due to traumatic force, gravity &/or muscle pulla) Displacement/apposition :What % of bone ends remain in contact (eg
undisplaced, $ a diameter displaced, completely displaced) & in what direction
(eg dorsal vs volar, valgus vs varus) b) Angulation/tilt : By drawing a line along both major fragments & measuring the
angle of intersection (anterior or posterior, medial or lateral)
c) Rotation : About longitudinal axis, distal fragment cf proximal fragmentd) Length of bone : distraction (! length) or overlap/impaction (" length)
6. Involvement of articulationsa) Does # line involve a joint or the epiphysis ?
b) In kids, involvement of epiphyseal plate (Salter-Harris classification)7. Bone texture : Does the bone look normal or is there evidence that it is a pathological # ?
8. Soft tissue : calcification, gas, FBs, etc9. Neurovasculature – presence of pulses; motor & sensory function; compartment syndrome
How do you examine a fractured limb?
• Always compare w/ normal side
• Closed vs open # : look for skin openings (need invasive therapy urgently)
• Assess distal neurovascular function o Circulatory function : capillary refill, peripheral pulses, skin colour (if blood flow
is compromised, get urgent orthopaedic consult)

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 4/45
o Neurology : test motor & sensory function of major peripheral nerves
• Local inspection : swelling, lump, shape, normal anatomy
• Test anatomical structures for tenderness, crepitation, deformity
• Active & passive & stress testing of bone/s & ligaments! ROM, continuity, pain,crepitation, stability & motion abnormalities (if –ve X-ray)
•
Examine joints above & below (eg # involvement, synovial swelling, fat pad)• Consider child abuse in infants with #’s
What are the complications of fractures?
Immediate (hrs) Early (hrs-wks) Late (months-yrs)
Local - Haemorrhage
- Damage to arteries/nerves
- Damage to surrounding
structures/viscera (eg spine)
- Infection (Clostridia)
- Compartment syndrome*
- Implant failure
- Fracture blisters
- Deformity – malunion or
non-union; growth probs
- 20 OA; joint stiffness
- Avascular necrosis*
- Osteomyelitis
- RSD (Sudeck’s atrophy)
- Myositis ossificans
- Tendon/muscle damage
- Ischaemic contracture
Systemic - Hypovolaemic shock - Fat embolism (< 48h)
- DVT/PE
- Septicaemia, pneumonia
- ARDS
- DIC
- Crush syndrome! ARF
Describe compartment syndrome, its clinical features & management
• Soft tissue swelling (oedema) & bleeding into tight osteofascial compartment ! ! compartment pressure (non-expansile)! impaired venous drainage (if pressure > 40mmHg)! ultimately, occlusion of arterial input! ischaemic necrosis of contained muscles & nerves
(within 12hrs)! later muscle fibrosis
•
Major causes : # of forearm, elbow or upper tibia; vascular compromise, reperfusion injury,compressive dressings, any MSK injury
o Most commonly involves anterior compartment of calf following closed tibial #
• Complcn :! fibrotic contractions of muscle (eg Volkmann’s ischaemic contracture offorearm flexors); nerve damage; myoglobinuria
• Early S&S – diagnosis is made almost solely on the clinical findingso Swollen & tense limb – palpation of firm, tender compartmentso Unrelenting pain out of proportion to the injury which is not relieved by opiates
o Passive hyperextension of toes or fingers will !! pain in calf or forearm
o Loss of sharp sensation
• 6 P’s : pain, pallor, pulselessness, perishing cold, paraesthesia, paralysis
•
Ix : measure intracompartmental pressure (" urgent Tx if > 40mmHg) – normal is 0-10mmHg
• Mx if > 30mmHg : elevate & ice limb; hyperbaric therapy! some advocate fasciotomy !
• Mx if > 40mmHg : decompression of skin & fascial compartments (open fasciotomy) within
4hrs ! wound left open until swelling has subsided
o Monitor UO for signs of myoglobinuria & ARF

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 5/45
Describe the parts of a normal bone
• Diaphysis : shaft or long, main portion
• Epiphysis : Extremity or end of bone
• Metaphysis : Region where diaphysis joins epiphysis – in growing bone includes theepiphyseal plate or physis (hyaline cartilage)
• Articular cartilage : Thin layer of hyaline cartilage covering epiphysis where bone formsarticulation with another bone
• Medullary (marrow) cavity : Central part – houses bone marrow & trabeculae
• Periosteum : External covering of bone (except articular surface)o Outer fibrous layer – dense fibrous CT (with BV’s, lymph V’s, nerves)
o
Inner osteogenic layer – mesenchymal osteoprogenitor cells (can becomeosteoblasts or osteoclasts)! bone growth in diameter, repair
• Endosteum : Internal covering – CT monolayer of osteoprogenitor cells
Describe the 2 types of bone growth
Intramembranous ossification (ALK p131)
• Occurs within a membrane (eg flat bones of skull, mandible) w/o a cartilage intermediate1. Mesenchymal cell aggregate (TGF-%, FGF etc)! osteoprogenitor cells! osteoblasts
2. Bone deposition (osteoblasts) & remodelling (osteoclasts) forms trabecular bone3. ! bone formation on outer & inner surfaces forms cortical plates of bone
4.
Residual mesenchymal tissue becomes haemopoeitic bone marrow (medulla)
Endochondral ossification (ALK p 133-134)
• Occurs in most bones, eg long bones
1. Hyaline cartilage model from mesenchymal tissue
2. Outer layer of mesenchymal cells, chondroblasts & osteoprogenitor cells form perichondrium 3. BVs enter diaphysis, with chondrocyte proliferation (! length/width) & osteoblasts beginning
osteoid formation ! primary ossification centre 4. Continued osteoid formation & remodelling forms central network of trabecular bone
5. After birth, BV’s invade the epiphysis & bring osteoprogenitor cells, which convert thecartilage model into trabecular bone, forming the secondary ossification centre
6.
Remaining hyaline cartilage forms epiphyseal plate in the metaphysis & articular cartilage 7. Epiphyseal plate allows for growth of bone in length! Growth of cartilage on epiphyseal
side of epiphyseal plate & its subsequent replacement with bone on the diaphyseal side
8. Puberty! !! hormones# !! bone growth > cartilage proliferation # epiphyseal platenarrows & disappears! epiphyseal line
• Bone can grow in diameter/width throughout life by appositional growth : As bone is beinglaid down from the periosteum by osteoblasts, osteoclasts remove bone matrix on the inner
(endosteal) surface# Enlarges marrow cavity while retaining cortical thickness

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 6/45
What are the layers of the epiphyseal plate? (ALK p139/135)
• Involves growth of cartilage on the epiphyseal side of the epiphyseal plate and its subsequentreplacement with bone on the diaphyseal side
1. Zone of resting cartilage ( reserve zone) – hyaline cartilage, w/ continuous cell division2. Zone of proliferation (epiphyseal side of plate) – active proliferation (hyperplasia) of
chondrocytes which !! the length of the bone3. Epiphyseal growth plate (hyaline cartilage)
4. Zone of hypertrophy (diaphyseal side of plate) – Chondrocytes enlarge (hypertrophy) –salter-harris fractures affect this part
5.
Zone of calcifying cartilage : calcification of the matrix (via alkaline phosphatase !
calcium salts), which eventually cuts off nutrient supply & prevents waste removal
6. Zone of cartilage cell death ( vascular invasion ) – Imprisoned chondrocytes die (lack of blood supply). BV’s invade this zone.
7. Zone of ossification & bone reabsorption – Osteoblasts invade (via BV’s) & lay downosteoid on the calcified cartilaginous matrix. Deposited bone is remodelled by osteoclasts as
it gets incorporated into the diaphysis.
• NB Cell stays at same point in bone & goes thru the various stages# zone migrates, not the
cells ! forcing plates away from each other# ! length
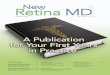
Describe Salter-Harris fractures using a diagram
• Epiphyseal plate (physis) injuries – usually affects the zone of hypertrophy (diaphyseal sideof growth plate)
• Most commonly occur in children aged 10-15 years
• Make up & 1/3
rd of all skeletal injuries in children
• Can cause severe deformity in later life if a bony bridge forms across the # site & prevents
growth on one side of the bone.
• Type I : # line extends thru the epiphyseal line (horizontal shearing force) - not visible on x-ray
• Type II : Separation of epiphysis w/ triangular fragment of metaphyseal shaft attached to it(lateral displacement force) – most common type !!
•
Type III : Vertical # thru epiphysis extending into epiphyseal plate• Type IV : # line passes thru both epiphysis, physis & metaphysis – may cause growth arrest
& joint deformities.
• Type V : Compression of epiphyseal plate. Commonly assoc/ w/ growth arrest.

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 7/45
See radiology recall p638
SALTR
Separated (type I)
Above (type II)Lower (type III)
Through (type IV)Ruined (type V)
What are the orthopaedic emergencies?
• Open fracture/dislocation (OT within 6hrs)
• Vascular injuries
• Compartment syndrome
• Neural compromise, esp. spinal injury
•
Acute septic arthritis or osteomyelitis• Exsanguinating pelvic #
• Hip dislocation
What are the indications for open reduction of fractures?
• N - Non-union, failure of closed reduction or unstable fractures prone to redisplacement afterreduction
• O - O pen # (needs ex fix)
• C – Compromise of neurovasculature; Compartment syndrome; Co-morbidities, eg elderly, paraplegia
•
A – Articular surface malalignment (intra-articular #, requires anatomic reduction)• S – Salter-Harris III or IV
• T – Trauma patient’s – earlier mobilisation & " risk of ARDS
• Pathological #’s
Principles of fracture management
1. Reduction of the fracture – open or closed2. Immobilisation of # fragments – relieve pain & prevent mal-union

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 8/45
3. Rehabilitation of the soft tissues & joints (early mobilisation)
What is external fixation? Why is it used? What are the complications?
• A scaffold or gantry attached to threaded pins set in the bone fragments (eg ring fixator)
•
Reasons for using external fixation – see NO CAST aboveo Open fractureso Fractures with skin loss or infection
o Able to easily adjust position of fragments
o Non-union or malunion
• Complications
o Non-union (if hold fracture fragments too tight)
o Pin-track infection
o Neurovascular damageo Refracture when Ex Fix is removed
What is a Colles #? What are the complications? Why use external fixation?
Colle’s fracture
• FOOSH in older women
• Fracture of distal radius, with dorsal angulation & displacement of distal fragment, often w/associated # of ulnar styloid
•
‘Dinner fork’ deformity : dorsal angulation & displacement, radial deviation, supination & proximal impaction
• Mx controversial : if displaced, reduce & apply cast from elbow to MCPJs (with wrist inflexion & ulnar deviation); Cast worn for 4 weeks, check at 1 week
Complications• Median N damage/compression – runs right across site of Colles’ fracture
• Rupture of EPL tendon – EPL runs across # site on dorsum of wrist
• Sudeck’s atrophy (reflex sympathetic dystrophy, RSD) – disturbance of sensory & autonomic
innervation of bone/BVs – hand becomes stiff, blotchy & cold)
• Malunion – fracture is unstable & bone is crushed – may require operative intervention
External fixation
• Primary external fixation (possible including percutaneous pin fixation) should be considered
for intra-articular, displaced fractures
How do you manage open fractures?1. An open fracture is suspected if there is : wound at # site, ooze from puncture wound (leaking
haematoma) or protruding bone fragments
2. Emergency management & assessmenta. ABCs
b. Assess entire limb, esp neurovasculaturec. Assess wound : state of skin around wound, does wound communicate with # ?

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 9/45
d. Assume contaminated – remove gross debris, clean wound w/ sterile saline,
chlorhexidine & cetrimide; cover wound w/ sterile dressinge. Reduce # & place in backslab, keep NBM
3. Give antibacterial prophylaxis – antibiotics (IV fluclox + benzylpen +/- gent/Flagyl) &Tetanus toxoid/Ig
4.
OT within 6hrs for debridement – extend wound, thoroughly irrigate, remove dead tissue, pack wound & leave open for DPC in 3-5 days
5. OT to treat the fracture – Grade III requires Ex Fix
What is neurapraxia?
• Neurapraxia** = minimal nerve damage (localised demyelination or compression) – axonsintact, but conduction ceases transiently
o Spontaneous recovery in days or weeks
• Axonotmesis (axonal separation) = severe axon damage by compression or traction
o Distal portions degenerate, but investing sheath remains intact # usually getdelayed recovery (1-2mm/day)
•
Neurotmesis = complete severance of a peripheral nerveo Spontaneous recovery does not occur! needs surgical repair
o Assoc/ w/ degeneration of the nerve fibre distal to the point of severance
Clinical features
• Symptoms : numbness, sensory alterations (eg paraesthesia), weakness
• Inspection : skin smooth & shiny; muscle wasting
• Palpation : " power, " sensation, Tinel’s sign
• Tinel sign : A sensation of tingling felt at the lesion site or more distally along the course of anerve when the latter is percussed; indicates a partial lesion or early regeneration in the nerve
What nerve would you use for a graft? Why?• Open injuries – explore at primary operation – if cleanly divided repair immediately,
otherwise leave alone & re-explore at 2-3 weeks
• Closed injuries – usually nerve sheath is intact, so repair will occur – if healing does not
occur, a nerve graft (eg Sural nerve) can be used, followed by splintage
• Only thin nerves are useful, as thick nerves undergo central necrosis after grafting
What are the signs of facial nerve palsy? How do you tell if it is UMN or LMN?
Relevant anatomy
• The facial nerve provides motor function to the muscles of facial expression, as well as taste
via the chorda tympani• Motor course –lateral surface of pons! thru internal acoustic canals! internal auditory
meatus! exits skull at stylomastoid foramen! thru parotid gland ! splits into its 5
branches
• The UMN from the motor homunculus innervates the facial nerve nucleus in the brainstem
• Facial nucleus receives crossed & uncrossed fibres by way of the corticobulbar tract

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 10/45
• The UMN from the right innervates the whole right nucleus as well as the forehead area of
the left nucleus. Conversely, the left UMN innervates the whole left nucleus and the foreheadarea of the right nucleus.
• # Facial muscles below the forehead receive contralateral cortical innervation, while those
muscles of the forehead receive bilateral innervation (NB Skin of forehead via CNV 1)
Facial nerve lesion
• # A LMN lesion of the facial nerve will cause ipsilateral complete paralysis of that side ofthe face including the forehead
o May be pontine, posterior fossa, petrous temporal bone, #, viral infectiono If before chorda tympani branches off, will also have taste loss
• An UMN lesion will cause contralateral paralysis of the facial muscles below the level ofthe forehead, with the frontalis & orbicularis oris spared (bilateral cortical innervation)
Examination of CNVII
• Facial asymmetry – During conversation may see unilateral drooping of corner of mouth,
smoothing of wrinkled forehead (may be symmetrical if bilateral)• Look up & wrinkle forehead ! look for loss of wrinkling (frontalis – LMN lesion) & feel
muscle strength by pushing down against corrugation either side
• Shut eyes tightly – compare how deeply the eyelashes are buried on the 2 sides & then try toforce open each eye (if LMN palsy, will get upward mov’t of eyeball & incomplete closure ofeyelid on ipsilateral side)
• Grin & compare nasolabial grooves (smooth on the weak side)
• Taste on anterior 2/3 of tongue – distinct substances placed separately each side
Causes of facial weakness
• Pons : MS, vascular lesions,
•
Cerebellopontine angle : acoustic neuroma, meningioma, basal meningitis• Petrous temporal bone : Bell’s palsy (idiopathic inflammation of CNVII within petrous
temporal bone – LMN palsy, usually temp), middle ear infection, trauma, HZV, tumours
o Chorda tympani joins facial N here
• Within the face : parotid gland tumours, mumps, sarcoidosis
• Other (often bilateral) causes : GBS, MND, myasthenia gravis, myotonic dystrophy
Ulnar nerve palsy: what are the causes & clinical features?
Causes
• Ulnar nerve entrapment at cubital tunnel : mechanical trauma (eg overhead throwing
athletes), osteophytes, loose bodies, synovitis, thickened fascia• Elbow fracture
Anatomy
• Medial side of arm (medial to brachial A) ! superficial course thru ulnar groove (cubitaltunnel) next to medial epicondyle of the ulna (vulnerable to injury = funny bone)! medial to
ulna in forearm

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 11/45
• Motor : FCU & medial $ FDP & the intrinsic muscles of the hand (interossei, lumbricals 3
& 4, adductor pollicis, hypothenar)! fine motor control of the hand
• Myotome : Finger abduction; Fromet’s sign (paper b/w thumb & II finger)
• Sensory : Skin of medial 1/3 of hand, little finger (V) & medial $ of ring (IV) finger (palmar& dorsal surface)
Clinical features
• Impaired adduction & abduction (interosseus 1-4)
• Flexion of wrist moves radially (by FCR)
• Hypothenar muscle wasting
• Ulnar claw hand when attempt to straighten fingers
o Hyperextension of MCPJ 4&5 (lumbricals gone)
o Unable to flex 4th and 5th fingers at DIPJ’s, PIPJ’s bent
o Abducted thumb (adductor pollicis)
CNXI (accessory nerve) injury: what are the causes & clinical features?
• The spinal branch of CNXI provides motor innervation to the SCM & trapezius muscles
(cranial branch assists in swallowing)
• Test by getting patient to shrug the shoulders & turn head against resistance
o NB R sternocleidomastoid turn head to L# inability to rotate head to contralateral side of lesion, but lack of trapezoidal shrug on ipsilateral side
o Look for a torticollis – overactivity of SCM – head appears turned to one side
Causes of palsy
• Trauma to neck or base of skull
•
Poliomyelitis• Syringomyelia
• Tumours near jugular foramen
What are the causes of LBP? List > 6 pathological conditions
Classification of LBP
• LBP can be classified into mechanical, non-mechanical & non-spinal back pain by history &examination
• In > 90% of patients, no precise anatomical cause of LBP is found, although " 70% are presumed to be caused by intervertebral dysfunction. < 10% have structural lesions.

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 12/45
Pathological causes of LBP**
Vascular Aortic aneurysmAcute aortic dissection
Infective Osteomyelitis
DiscitisTB
Inflammatory Ankylosing spondylitis
Rheumatology disorders
Neoplastic Primary tumours (rare)Metastases – breast, prostate, bronchus
Degenerative/MSK Spondylogenic (simple mechanical) – vertebral dysfunction (IV discs &/or facet joints)
Spondylosis
Prolapsed IV disc
OsteoarthritisSpondylolisthesis
Sacro-iliac dysfunction
Idiopathic Paget’s disease
Scheuermann’s disease
Congenital KyphoscoliosisSpina bifidaSpondylolisthesis
Traumatic Vertebral fracturesLigamentous injury
Muscle tears
Endocrine/metabolic Cushing’s syndromeOsteoporosisOsteomalacia
Psychogenic Depression
Psychosomatic backache
Visceral GIT – penetrating peptic ulcer, Ca rectumPancreatic CaBiliary disorders
Renal disorders – Ca, renal calculus, inflammatory diseaseOBGYN – uterine tumours, PID, endometriosis
List > 8 red flag signs for LBP indicating radiologic investigation

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 13/45
• Age : < 20 or > 50
• Significant trauma
• Hx of malignancy, corticosteroid use, diabetes, drug or alcohol abuse, or HIV
• Constitutional symptoms: malaise, febrile, weight loss
• Pain worse at night; constant pain not relieved when supine
•
Widespread neurological signs or symptoms • No improvement > 1 month
• Bowel/bladder dysfunction &/or perianal anaesthesia (cauda equina syndrome)
• Deformity
• ! ESR
List > 5 conditions in which bone scan investigation of LBP would help
• Metastases or primary malignancy – 90% positive
• Infections
• Fractures
•
Osteomalacia/osteodystrophy
• Spondyloarthropathies (ankylosing spondylitis, psoriasis, IBD, reactive arthritis) – SI joints
positive
• Hyperparathyroidism – 50% positive
• Paget’s disease
" Plain x-rays are only 70% sensitive & give the diagnosis only 33% of the time.
Scoliosis
What is scoliosis?
•
Abnormal lateral curvature &/or twisting of the spine – seen from behind & accentuated by bending forwards
What are the causes & classification of scoliosis?
• Postural (non-structural) scoliosis – compensatory to some condition outside the skin, egshort leg, pelvic tilt or prolapsed IV disc
o Disappears on sitting
• Structural scoliosis – caused by bony abnormality or vertebral rotation – secondary curves
nearly always develop to counterbalance the primary deformityo Deformity is fixed & does not disappear with changes in posture
o
Major types1. Adolescent idiopathic scoliosis** - usually thoracic curve convex to the right
– presents before puberty & progresses until skeletal growth ceases2. Infantile (congenital) scoliosis – may regress3. Neuromuscular scoliosis, eg polio, cerebral palsy
4. Osteopathic scoliosis – due to congenital vertebral abnormalities
What are the clinical signs?

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 14/45

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 15/45
What are the causes of a painful hip?
Causes of painful hip Hip diagnostic calendar
Referred pain
• Discogenic disease
Joint disorders
• Infection
• Perthes’ disease
•
Slipped epiphysis• RA
• OA
• Osteonecrosis Periarticular disorders
• Hernia
• Tendinitis
• Bursitis
0 (birth)
0-55-10
10-20Adults
CDH/DDH
InfectionsPerthes’ disease or TS
SUFEOA
Avascular necrosisRAProlapsed disc
Trendelenburg test
What is the Trendelenburg test? What indicates a positive Trendelenburg sign?• Patient asked to stand, unassisted, on each leg in turn – lift other leg by bending knee (not
hip)
• Normally the weight-bearing hip is held stable by the abductors & the pelvis rises on the
unsupported side (negative Trendelenburg test)
• If the hip is unstable, or very painful, the pelvis drops on the unsupported side ( positive
Trendelenberg sign)
What may cause a positive Trendelenburg sign? Give ! 4 causes
1. Dislocation or subluxation of hip (eg CDH)
2. Weakness of the ABductors : gluteus medius & minimus via superior gluteal N
3.
Shortening of the femoral neck4. Any painful disorder of the hip (causes gluteal inhibition)
What is Perthes disease? What are the classic radiologic findings?
• Idiopathic avascular necrosis of the femoral head – precipitating factor is probably a jointeffusion following trauma or non-specific synovitis.
• Causes hip or knee pain, limp & " ROM in 3-8 year olds (' > ()

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 16/45
• DDx = transient synovitis (irritable hip)
Radiological signs (Dandy p316; Dixon p180) – Frogleg view
1. Initially normal (cold on bone scan) – bone necrosis
2. ! density of epiphysis & widening of the joint space – revascularisation & repair
3.
Fragmentation of the epiphysis (collapse & remodelling)4. Epiphysis flattened & enlarged (coxa plana & coxa magna)
Management
• Containment of femoral head within acetabulum (# more likely to retain normal shape) byabduction & internal rotation using ‘broomstick’ plaster or a removable splint
• Alternative is osteotomy (late Dx)
What is SUFE? What are the classic radiologic findings?
•
Slipped upper/capital femoral epiphysis caused by fracture thru the physis – related tohormonal imbalances
• Occurs during pubertal growth spurt; esp in fat '’s
• Causes pain in hip or knee &/or limp – O/E leg is shortened & externally rotated; " ROM inabduction & internal rotation
Radiologic findings (Dixon p173)
1. Epiphysis for head of femur is displaced posteriorly &/or medially2. Widening of the physis3. Trethowan’s sign - line drawn along superior surface of neck remains superior to head instead
of passing thru it
Management
• Mild displacement – fix epiphysis with 2 threaded pins
• Severe displacement - 2 threaded pins, followed by compensatory osteotomy
CDH
•
Recurrent subluxation or dislocation of the hip secondary to acetabular dysplasia, abnormalligamentous laxity or both
• More common in (’s (oestrogen ! laxity); L hip > R hip; related to breech delivery or FHx
List ! 4 clinical features suggesting CDH
Routine post-natal exam
• Ortolani’s test – baby’s thighs are held b/w thumb & forefingers w/ hips flexed to 900 – hip is
slowly abducted – if a hip is dislocated, as full abduction is approached femoral head will be
felt slipping into acetabulum +/- an audible ‘click’
• Bartlow’s test – fix pelvis b/w symphysis & sacrum – then attempt to dislocate the hip bygentle backward pressure during abduction & adduction
(Remember Ortolani’s is outwards, Bartlows is backwards)

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 17/45
Late features
• Asymmetrical skin creases (unilateral DDH)
•
" hip abduction (tested at 900
hip flexion)
• Leg is shortened & rotated externally
•
Trendelenburg test is positive• Gait – dip on affected side, or waddling gait if bilateral
What investigations are necessary? What are the radiographic signs?
• Ultrasound – essential for all babies with Ortolani click, family Hx or predisposing factoro Decisions on treatment based on U/S findings
• X -ray: AP pelvis may be helpful after 6 months (Dandy 340), Putti’s triad1. Acetabular dysplasia : shallow acetabular socket & ! acetabular angle
2. Small upper femoral epiphysis
3.
Delayed ossification of femoral head4. Superolateral displacement of femoral head – loss of Shenton’s line, movement lateral
to Perkin’s line (lateral margin of acetabulum) & movement superior to Hilgenreiner’s
line (tri-radiate cartilage of acetabulum)
What is the initial management (after USS)?
• At birth : Nurse baby in double nappies or abduction pillow for 1st 6 weeks
• 6 weeks : re-examine – if hips stable, observation only for 6 months. Babies with persistent
instability need formal abduction splinting until radiological confirmation of acetabulardevelopment (usually 3-6 months).
o Splintage : Ensure the hips are reduced first (confirm by U/S). Apply splintage to
hold hips at 1000
flexion & somewhat abducted. Infants will require a Von Rosen’ssplint , Pavlik harness or Cambridge splint .
• 6 months – 6 years : gradual closed reduction (over 3 weeks by traction) followed by plasterspica (hips flexed, abducted & internally rotated) for 6 weeks
• > 6 years : Operative reduction +/- osteotomy
What are the risks of management?
• Avascular necrosis of femoral head
• Incomplete healing may predispose the child to secondary OA in later life.
• Splinting without first ensuring that the hip is satisfactorily reduced – poor position.
• Unnecessary treatment – most dislocatable hips self-stabilise within a few days of birth.
What is acetabular dysplasia?
• Consists ofo
! acetabular angle (steeply sloping roof), &
o Shallow acetabular fossa
• Predisposes to spontaneous dislocation or subluxation

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 18/45
How can acetabular dysplasia be reversed?
• Abduction splinting in neonates, as per DDH
• In older children, surgery may be necessary: an osteotomy of the femur to restore jointalignment, or osteotomy of the pelvis to restore correct acetabulum shape.
What are the pathological causes of limp in a child?
• Vascular (ischaemia) – Perthes’ disease
• Infection – septic arthritis, osteomyelitis
• Inflammation – transient synovitis, juvenile RA
• Neoplastic – tumour, leukaemia
• Congenital/developmental – CDH/DDH, SUFE
• Trauma – SUFE, fracture
• Neuromuscular – cerebral palsy
Acute Subacute Chronic
FractureTransient synovitis
Septic arthritisOsteomyelitis
Juvenile RATumour/leukaemia
Acute on chronic SUFE
Cerebral palsyCDH/DDH
Perthes’ diseaseChronic SUFE
Hip timeline
0 (birth) CDH
0-5 Infections
5-10 Perthes’ disease; Transient synovitis
10-20 SUFE
Adults OA, RA, avascular necrosis
Elbow dislocation
What neurovascular structures are in danger?
• 90% are posterior dislocations
• Median nerve injury – test by touching thumb to 5th
finger
• Ulnar nerve injury – test by spreading fingers apart
• Radial nerve injury – extend thumb, fingers & wrist
• Brachial artery injury – palpate brachial artery at elbow & palpate ulnar & radial arteries
– compare to other side
How do you manage a dislocated elbow?
1. Analgesia2. Check neurovasculature
3. Obtain x-ray promptly to exclude fracture-dislocation4. Reduce dislocation ASAP under regional (eg Bier’s block) or general anaesthesia
a. Apply traction to forearm, with countertraction applied to distal aspect of humerus –also correct any medio-lateral displacement with counterforce simultaneously

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 19/45
b. Gently flex the elbow to accomplish the reduction – often hear/feel clunk
5. Reassess neurovascular function & flex/extend elbow to check reduction6. Apply posterior splint with elbow at 90
0 flexion
7. Obtain post-reduction x-rays
What is a Dupuytren’s contracture? What are the causes?
• Contracture of the palmar fascia which can involve the skin! flexion deformity
• May only affect 1 finger (usually the little finger) or entire hand (Dandy p367)
• Often symmetrical, commoner in ', may run in families
Causes
• Idiopathic
• Familial
•
Liver disease• Alcoholism
• Diabetes
• Epilepsy
Management
• Slight deformities are best left untreated
• Surgical correction involves excising the contracted tissue
• Severe, uncorrectable deformity may require amputation of the affected digit
GASTROINTESTINAL SURGERY
Colorectal neoplasia
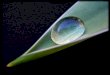
Identify the lesion on the above pictures?
• Left : pedunculated polyp

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 20/45
• Right : sessile polyp
What types of polyps are there (ie classify large bowel polyps)?
Shape (Robbins p827)
•
Sessile – small, flat projection into lumen (more likely to be villous architecture)• Pedunculated – contains a stalk (more likely to be tubular architecture)
Aetiology
• Neoplastic (adenomatous polyp) – result of epithelial proliferative dysplasia –adenocarcinoma generally arises from adenomas
o > 100 are present in FAP (familial adenomatous polyposis – defect in APC gene) &
Gardner’s syndrome
• Hyperplastic polyp : composed of well formed, mature glands & scant lamina propria – resultfrom delayed shedding of surface epithelial cells – usually found in distal colon
o Histology – hyperplastic crypts have a serrated or saw-tooth outline
•
Inflammatory polyps : found in IBD (Crohn’s &/or ulcerative colitis)• Hamartomatous polyps : normal tissue in abnormal configuration – sporadic & usually found
in kids – also seen in Peutz-Jegher’s syndrome
Adenomatous polyps
• Tubular adenoma : tubular glands; smooth surface; usually pedunculated ; most commontype
• Villous adenoma : villous frondlike projections (look like broccoli heads); usually sessile;
greatest risk of malignancy (villous = villain)
• Tubulovillous adenoma : mixture
Risk of malignancy (ie. progression to adenocarcinoma)• Polyp size : adenomas > 2cm have 50% risk of carcinoma
• Architectural type : villous 40%, tubulovillous 20%, tubular 5%
• Severity of epithelial dysplasia
What are the risk factors for CRC?
•
! age (incidence raises sharply after 50yrs)
• Family Hx (20% occur in setting of FHx, esp. if 1st degree relative < 50yrs at Dx)
• Presence of FAP, HNPCC or adenomatous polyps
• Low dietary fibre intake
• Excess intake of dietary fat, refined carbohydrates & red meat
•
Ulcerative colitis (long-standing)
• Physical inactivity & obesity
• Alcohol & tobacco
• Irradiation
What is the adenoma-carcinoma sequence? What is the evidence to support it?

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 21/45
• Most colorectal carcinomas arise from, or within, pre-existing benign adenomas – a process
that evolves over 5-15 years
• Ca develops from progressive accumulation of multiple genetic mutations – there is progressive increases in size, level of dysplasia & invasive potential
• Normal colonic epithelium! Hyperproliferative epithelium! Early adenoma! Late
adenoma! Carcinoma • Most sporadic cancers develop via the chromosomal instability pathway (A), due to
inactivation of tumour suppressor genes (eg APC, p53, LOH) & activation of oncogenes (eg
K-ras)
• All HNPCC & some sporadic cancers follow the microsatellite instability pathway (B), beginning with APC mutation, then defect/s in DNA mismatch repair genes, hMLH1 or
hMSH2
Evidence for the adenoma-carcinoma progression = HI TEC
• H istology : adenomas commonly harbour carcinoma
•
I ntervention : screening programmes for adenomas " incidence of CRC
• T opology : colorectal distributions are similar to that of adenomas
• E pidemiology : populations with high prevalence of adenomas also have high risk of CRC
• C hronology : peak incidence of adenomas antedates peak incidence of CRC
Genetic factors
• 20% of colorectal Ca occurs in setting of a FHx; 5% due to HNPCC; <1% FAP
• FAP patients exhibit a somatic mutation in the tumour-suppressor APC gene – mutations inthis gene also occur in sporadic cancers
• Hereditary mutations in DNA mismatch repair genes occur in hereditary non-polyposis
colorectal cancer (HNPCC), aka Lynch’s syndrome – sporadic cancers can exhibit the samedefect
o Autosomal dominant mutation in hMLH1 or hMSH2
o Diagnosis requires > 3 relatives with CRC spanning 2 generations
o 80% lifetime risk of colorectal Ca – also ! risk of gynaecological tumours
o Requires 2nd
yearly colonoscopy from 25 yrs & gynaecological screening
What treatment is used for CRC?

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 22/45
• Aim is to excise the cancer with an adequate margin of surrounding tissue (usually 2cm, somesay 5cm but ? effect on survival) & lymphovascular clearance
o A large segment of colon (up to 15cm) is usually resected because of the extent of
lymphovascular clearance
•
Usually results in an anastomosis via staples or sutures• Procedure may be open or laparoscopic
• Surgical resection : attempts to remove area of bowel containing tumour complete with its
lymphatic drainage (pericolic LNs) – as lymphatic drainage follows arterial supply, the axialartery is ligated at its origin, creating an ischaemic segment of bowel for excision
• Chemotherapy – 5-Fluorouracil + levamisole (or folinic acid) is usedo To ! survival in Stage C cancerso In advanced disease as palliation (! survival 6 months)
• Radiotherapy – may be used pre- or post-op for T3-T4 rectal cancers to " local recurrence
• Metastases may be treated by resection, embolisation, chemotherapy &/or XRT
o Liver mets can be resected with a 1-2cm margin + adjuvant chemoRx
•
FOLLOW-UP is essential to detect recurrence (most occur in 1st 3 years) – colonoscopy &CEA (at 1 year, then every 3-5 years)
What is the treatment for a Ca at the hepatic flexure?
• Right hemicolectomy (Clunie p184)
o Laparotomy or laparoscopic approach
o Excision of caecum, ascending colon & part of transverse colon & overlyingomentum
o Division of ileocolic, R colic & R branch of middle colic vessels (SMA)
o Anastomosis of ileum to transverse colon
IBD: CD vs UC
What are the features of UC vs CD on contrast examinations?
Crohn’s disease Ulcerative colitis
- SBS/SBE :# oedema & separation of bowel loops;
$ skip lesions;% string sign (terminal ileal stricture);
& deep rose-thorn ulcers; ' cobblestone appearance;
( fistulas
- Ba Enema : patchy involvement of colon. Rectum
may or may not be involved
- AXR : thumb-printing (mucosal oedema); dilatation
- SBS/SBE : normal (or backwash ileitis)
- Ba Enema : rectum always involved
Acute : granular colonic margin w/ thumbprinting
Subacute : pseudopolyposis & superficial ulcerations
Chronic : pipe-stem colon – smooth, narrowed &
shortened colon with lack of haustrations
Eisenberg p149, Dixon p115
What are the perianal features of CD?
• Present in & 50% of CD patients
• Perianal skin tags
• Fissures

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 23/45
• Perianal sepsis
• Anorectal strictures
Compare UC vs CD
Micro pathology
Depth of inflammation Mucosal (submucosal rarely) Transmural (full thickness)
Wall thickening Not seen (minimal fibrosis) Common (“lead pipe”), often fibrosis
Crypt abscesses Common Common
Pseudopolyps Marked Not uncommon in colonic CD
Granulomas (noncaseating) Not seen Granulomas common (> 50%)
Ulcers / fissures Superficial (no fissures) Deep, linear! fissures
Lymphoid reaction Mild Marked
Ulcerative Colitis Crohn’s Disease
Macro pathologyBowel region Colon only Mouth! Anus
Rectal involvement Always – involvement proximally
from rectum up
Rectum often spared (50%)
Distribution of lesions Continuous Skip lesions / cobblestone
Mucosal appearance Friable, purulent, diffusely
involved; may be atrophy
Patchy ulceration, fissured &
cobblestoned
Associated ileal disease Only in ‘backwash ileitis’ 50% have combined ileal and colonic
involvement
Creeping mesenteric fat Not seen Common
Serosa Normal Granular, fibrous or ‘flared’
Clinical features
Symptomatology Diarrhoea w/ blood & mucus;
Cramping abdo discomfort;
urgency/tenesmus
Diarrhoea (watery or bloody); Abdo
pain (obstructions)
Abdominal O/E Tenderness over colon or NAD Tenderness; RIF mass;
Perianal abscess/fistulas Rare (< 25%) Yes (75%)
Fat/vitamin malabsorption No Yes (ileal disease) – wt loss
Response to surgery Good (colectomy = cure) Poor-fair (recurrence !)
Complications
Intestinal obstruction Late / rare Common
Intestinal fistulas Not seen Common, 80%

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 24/45
Bowel obstruction
What are the causes of SBO & LBO?
SBO (remember HANS had an SBO) LBO
• Hernia
• Adhesions***
• Neoplasia
• Stricture
• Intussusception
• Volvulus, gallstone, bezoar, CF, abscess
• Neoplasia
• Diverticular disease
• Volvulus
• In lumen : faeces, FB, bezoar, barium
• In wall : stricture, Hirschsprung’s
• Outside wall : tumour, hernia, adhesions
What are the S&S?
Symptoms1. Colicky abdominal pain
2. Vomiting (provides relief) – early in high SBO, late or absent in LBO3. Abdominal distension – epigastric or hypogastric in SBO, generalised in LBO
4. Absolute constipation – failure to pass flatus (obstipation) & faeces – occurs early withLBO, late in SBO
Signs
• Look for cause – scars, hernias, abdominal mass etc
• Inspection – abdominal distension, visible peristalsis
•
Palpation – tenderness
• Percussion – hyper-resonant
• Auscultation – bowel sounds louder, more frequent & high pitched (‘tinkling’)
• PR exam – faeces, blood or mucus
What investigations should be performed? What are the radiological features?
Intestinal perforation Occasionally Rare
Intestinal haemorrhage Common Rare
Toxic megacolon Occurs rarely Very rare
Colorectal carcinoma 10% (dysplasia common) Rare
Extraintestinal manifestations
Sclerosing pericholangitis Common Rare
Uveitis or arthritis Common CommonPyoderma gangrenosum Rare Not seen

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 25/45
• Supine & erect AXR, erect CXR
• FBC, U&Es
• SBS or abdominal CT to determine level & extent of obstruction
Radiologic signs of obstruction
•
Supine : gas-distended loops of bowel – level of obstruction determined by number of loops& amount of plicae (jejunum has multiple plicae, ileum has minimal)
o Bowel distal to obstruction will be devoid of gas (the ‘cut-off’)
o String of beads sign – as bowel progressively fills with fluid, get " gas – some gasremains trapped b/w adjacent plicae forming small beads of gas in a line
• Erect : air-fluid levels
• Volvulus: huge, distended gas-filled loop of sigmoid/caecum with a long-fluid level on erectfilm. Sigmoid volvulus presents ‘bent inner tube sign’ . Caecal distension > 10cm suggestsimminent perforation.
SBO vs LBO on plain radiographs*** Small bowel obstruction Large bowel obstruction
Luminal folds Plicae circulares extend across width of
lumen (step-ladder appearance)
Haustra (plicae semicirculares) extend only
partway across the lumen
Position Central Peripheral
Fluid levels Short (3-5cm), but more numerous Long fluid levels, but less numerous
Colonic/rectal gas Absence of colonic gas Absence of rectal gas
Other String of beads sign (fluid-filling) May be huge distended loops
What is the management of SBO?
• Conservative – ‘Drip & suck’ used if incomplete/uncomplicated obstruction or paralytic ileus
– monitor closely, operate if persists• Surgical – if complete/complicated – LOA or herniorrhaphy
Haemorrhagic loop of bowel caused by adhesions SBO
• Adhesion! internal herniation of bowel contents! bowel obstruction & " venous drainage
! engorgement & haemorrhage! " arterial inflow! infarction
Stomas
What is a stoma ?
•
Ostomy : operation that connects the GI tract to the abdominal wall skin, or the lumen ofanother hollow organ (man-made fistula)
• Stoma : the opening of the ostomy
• Epithelialisation (mucosa to skin) prevents closure
What is the difference b/w a temporary & a permanent stoma ?
• Temporary stomas are usually loop ileostomy/colostomy & can be removed at a later date bya minor operation +/- anastomosis

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 26/45
• Permanent stomas are usually end ileostomy/colostomy & are more difficult to reverse
When is a stoma indicated ?
• Temporary
o To protect a distal anastomosis & allow healing, eg ileal pouch-anal anastomosis, low
colorectal anastomosiso To divert stool from the distal anorectum, eg perianal Crohn’s disease, anorectal Ca,
severe perineal sepsis, faecal incontinence
o Caecal volvulus
• Permanento Following colectomy if cannot anastomose, eg insufficient bowel remaining to
anastomose, risks of anastomosis
o Following removal of anorectum, eg APR
o Severe faecal incontinence
What is the pre- & post-op stomal care ?
• Pre-operative stoma siting, counselling & stoma eduction are important
• Viability of stoma is examined periodically in the post-op period
• Defer oral feeding until intestinal peristalsis recommences & ileostomy has passed gas &
effluent, usually 2-5 days after surgery
• Normal output ranges 500-1000mL/day – higher outputs may cause dehydration, while loweroutputs indicate obstruction
• Stomal education commences pre-op & continues post-op using stomal therapist o
! psychological adjustment
o
Fitting & changing of applianceo Warning signs to look for, eg infection, ischaemia
• Stoma is remeasured for new appliances at 4 weeks (after oedema resolves) – proper fitting
essential to avoid leakage & skin excoriation
• Dietician advice
o Initially low-residue diet
o After 3 weeks introduce food, but must avoid foods that affect the stoma, eg nuts, popcorn, corn, string vegetables, fruit peels
• Option for stomal irrigation, whereby patient can irrigate & empty the stoma every few days.This removes the need to wear a bag appliance, and a cap over the stoma can be worn instead.
What are potential complications of a stoma ?
• High output causing dehydration
• Ischaemia – may require urgent laparotomy & refashioning of the stoma
• Stricture – due to ischaemia, parastomal sepsis, recurrent CD, etc
• Bleeding
• Fistula
• Parastomal abscess

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 27/45
• Parastomal ulcer
• Parastomal hernia
• Ileostomy retraction – may require surgical revision
• Small bowel obstruction – due to adhesions, volvulus or internal herniation
• Skin irritation
Meckel’s diverticulum
What is a Meckel’s diverticulum & what is its embryological origin ?
• Solitary true diverticulum on the anti-mesenteric side of the terminal ileum, within 2 feet ofthe ileocaecal valve
• Caused by failure of of involution of vitelline duct (connects lumen of primitive midgut gut
to yolk sac)
What are its complications & resultant symptoms ?
• Ulceration (ectopic gastric mucosa)! bleeding (red blood PR) or perforation
• Meckel’s diverticulitis – resembles appendicitis
• Obstruction – as volvulus or intussusception
Meckel’s “rule of 2’s” ) Found in 2% of population
) 2% are symptomatic) Found & 2 feet from the ileocaecal valve
)
Most are 2 inches long) Most symptoms occur < 2 years
) One in 2 will have ectopic tissue
Haemorrhoids (Browse p430)
What is the cause of haemorrhoids ?
• Haemorrhoids are submucosal vascular ‘cushions’ within the anal canal that represent dilated submucosal veins of the internal haemorrhoidal plexus
• Occur 20 to persistently ! venous pressure within haemorrhoidal plexus* constipation;
pregnancy (venous stasis); collaterals in portal HT• Classically they are situated at 3, 7 & 11 o’clock when the surgeon is looking at the patient in
the lithotomy position = left lateral, right anterior & right posterior positions
What are the clinical features ?
• Intermittent, bright red bleeding after defaecation – on toilet paper or dripping into bowl
• Palpable lump after defaecation

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 28/45
• Perianal discomfort & pruritus
• PR mucus discharge
• " Uncomplicated piles do not cause pain – but thrombosis/strangulation cause severe pain
How are haemorrhoids described & graded ?
Location
• External haemorrhoids : develop in inferior haemorrhoidal plexus # located below anorectal
(dentate) line (skin tags)
• Internal haemorrhoids : dilation of superior haemorrhoidal plexus
Degree of internal haemorrhoids
• 1
0 haemorrhoids : small haemorrhoids that bleed, but remain in the rectum
• 20 haemorrhoids : prolapse on defaecation (or Valsalva) & retract spontaneously
• 30 haemorrhoids : prolapse on defaecation (or Valsalva), but require manual replacement
• 40 haemorrhoids : prolapse from anus & despite attempts to replace them fall out again
In a 55 yo patient with PR bleeding & obvious haemorrhoids, what else must be excluded ?
• Haemorrhoids & CRC may co-exist in the same patient
• Any doubt, especially in pt’s > 50, altered bowel habit or sigmoidoscopic appearances of
altered blood present! colonoscopy is essential
• Haemorrhoids usually don’t cause anaemia – look for CRC !!
What does haemorrhoid banding do ?
• Used to treat 20 & 3
0 internal haemorrhoids
• Performed thru a lubricated proctoscope
•
Haemorrhoidal tissues are drawn by a pair of forceps into the barrel of a special band ligator –upon release of the trigger, the elastic band is released to encompass the haemorrhoidal tissue
at the level of the anorectal ring
• This draws the prolapsing haemorrhoid back up into the anal canal & may lead to itsdestruction (via necrosis)
• Complc’n : haemorrhage, sepsis, pain (due to thrombosis)
Common sites :3, 7 & 11 O’clock

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 29/45
What are the other treatment options for haemorrhoids ?
Conservative
• Dietary fibre, eg psyllium
• Local hydrocortisone & analgesia – topical or suppositories
• If symptoms persist for 4-6 weeks, surgery is recommended
Surgical
• Injection sclerotherapy (eg 5% phenol in almond or arachis oil) by proctoscopy
•
Infrared photocoagulation • Haemorrhoidectomy – suture apex of haemorrhoid & excise – complications incl
haemorrhage, infection, anal stenosis & faecal incontinence
Incisional hernia
Identify from this picture (Browse p338). What is an incisional hernia ?
• A protrusion of the peritoneum (the sac) & abdominal contents into the subcutaneous plane
thru a defect at the site of a scar following an abdominal operation
• Patients present with an obvious bulge & often c/o nagging discomfort
•
Signs – reducible lump with an expansile cough impulse underneath an old scar – tend to beaccentuated by tensing the recti
What are the risk factors & predisposing factors ?
• Occurs in fibrous scars that become weakened
• Surgical technique & post-op care : factors incl

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 30/45
o Incision – angulated incisions, incision parallel to previous incisions, T- & V-shaped
incisions, location (midline wound > paramedian wound; upper > lower wound)o Ragged or devitalised tissue left in wounds (predisposes to infection)
o Strength & type of suture material – sutures should be non-absorbable or should last9-12 months until healing process is complete
o
Wound infection – most common cause• Patient characteristics
o ! age
o Obesity – causes ! intra-abdominal pressure & " muscle toneo General factors – corticosteroids, DM, malnutrition
o Local factors – foreign body, haematoma, movement
How do you treat an incisional hernia ?
• All incisional hernias should be surgically repaired – they ! in size over time & ! risk ofcomplications (irreducibility, obstruction & strangulation)
• Pre-operative weight reduction, physiotherapy & smoking cessation is recommended
• Repair technique 1. Define the sac & neck – if hernia is irreducible, open sac & mobilise contents by
dissection. Omentum within the sac should be excised.2. If edges of defect can be apposed it can be closed directly with strong non-absorbablesutures.
3. If edges of defect cannot be brought together, the defect is covered by placing a prosthetic mesh either beneath the muscle layer in the extraperitoneal plane or on top
of the muscle layer in the subcutaneous plane.4. Prophylactic AB’s are used & wound is drained with suction drain for short time.
HEPATOBILIARY & PANCREATIC SURGERY
List > 3 differentials for circular lesions in the liver at USS
• Metastases
• HCC (multi-focal)
• Nodular regenerative hyperplasia
• Lymphoma
• Sarcoidosis
• Hydatid cysts
• Multiple abscesses

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 31/45
• Fatty infiltration
• Cirrhotic (regenerating nodules)
CBD obstruction
Describe the anatomic & metabolic pathways by which bilirubin is conveyed from its site ofproduction until its excretion from the body ?
• RBC degradation occurs in reticuloendothelial cells (macrophages) in the spleen (also liver& bone marrow)! old or defective RBCs removed from circulation
• The globin portion is degraded to $$’s which are recycled
• Haem ring (" 250mg/day) is opened via haem oxygenase into linear biliverdin (green)
o By products : carbon monoxide & Fe3+
• Biliverdin converted to bilirubin (yellow) by biliverdin reductase
o Lipophilic# bound to albumin in plasma (unconjugated – cannot enter urine)
o Excess unconjugated bilirubin pools in sclera, fat & skin
• Unconjugated bilirubin taken up by hepatocytes from plasma (" 40% refluxes back into
blood) [NB “free” bilirubin w/o albumin is neurotoxic]
• Bilirubin binds to glutathione S-transferase & Z-protein
• Conjugated with glucuronide twice in ER, via bilirubin UDP-glucuronyl transferase to
bilirubin diglucuronide (conjugated bilirubin)! water soluble
• Conjugated bilirubin excreted into biliary canaliculi & flows with bile into duodenum &colon (some bile reabsorbed in terminal ileum)
• Bacterial action in colon deconjugates & modifies bile! colourless urobilinogen &
stercobilinogen, then yellow urobilin & dark red-brown stercobilin (gives stool its colour)
& excreted in faeces • Some urobilinogen (water soluble) reabsorbed from intestine into portal blood
o Taken up by liver & re-excreted, or
o Excreted by kidneys into urine (small amt)! slowly becomes urobilin on exposureto air
What imaging investigation would you use to confirm extrahepatic biliary obstruction ?
What are the advantages of this ?
• Ultrasound is the modality of choice – can easily diagnose acute cholecystitis, gallstones &other causes of RUQ pain unrelated to the GB
•
US can demonstrate :o Dilated extrahepatic & intrahepatic bile ducts suggestive of obstruction
o Gallbladder stones
o CBD stones (33% of time – often obscured by duodenal gas)
o Exclude cholangitis & cholecystitis (wall thickening > 3mm)
• Advantages
o Non-invasive & relatively painless
o Quick & cheap

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 32/45
o No ionising radiation
• ERCP or PTC can be used to assess degree of dilatation & site of stone/s & may also allowstone removal
• Other Ix : FBC, E/LFTs, blood cultures
List ! 3 important causes of extrahepatic biliary obstruction.
• Choledocholithiasis
• Tumour : pancreatic head, ampulla, bile duct (cholangioCa) or duodenum
• Strictures : post-surgical, post-inflammatory
• Pancreatitis or pancreatic pseudocyst
• Lymphadenopathy
• Ampulla of Vater dysfunction
• Parasites
Identify the picture – what is it & where is it inserted ?
• T-tube – inserted into CBD following choledochotomy – T part in CBD, long part goes outthru the skin

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 33/45
Give 3 reasons for placing a T-tube in the CBD ?
• To avoid leakage from choledochotomy
• To enable later (7-10 day) T-tube cholangiogram to ensure no residual stones in CBD orhepatic radicles
• Post-CBD trauma to prevent bile leakage
When would you remove T-tube ? What precautions would you take before removing it ?
• Usually removed after 7-10 days post-op
• Patient must be in a satisfactory state (eg not toxic, not too unwell)
•
Bile drainage must be clear & non-infected• Perform T-tube cholangiogram prior to removing to ensure no residual stones
Cholangitis
What is Charcot’s triad ? What is Reynold’s pentad ?
• Charcot’s triad indicates cholangitis
o RUQ pain (& tenderness to palpation)
o
Jaundiceo Fever/rigors – usually intermittent & occurring every few days with exacerbation
of pain & jaundice (ball-valve mechanism)
• Reynold’s pentad : severe cholangitis may cause septicaemia resulting in
o Altered mental status
o Hypotension/shock (due to vomiting & dehydration)
What is the diagnosis ? What may be the underlying cause ?

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 34/45
• Cholangitis
Causes of cholangitis
• Choledocholithiasis – most common cause
•
Stricture• Extrinsic compression – tumours, pancreatic pseudocyst, pancreatitis
• Instrumentation of bile ducts, eg PTC, ERCP
• Biliary stent
What is the pathophysiology of this sign ?
• Blockage of CBD! build-up of pressure within the biliary tree (RUQ pain) & obstructive
jaundice! overgrowth of gut flora (retrograde via sphincter of Oddi) ! may lead tosepticaemia and septic shock! fever, tachycardia, hypotension
Laparoscopic cholecystectomy
What do you tell the patient pre-op about the risks ?
• “Key hole” surgery – involves & 4 small incisions 0.5-2.5cm long made in the abdomen used
to insert the laparoscope & other devices via ports
• Benefits – in most cases will relieve pain & prevent complications of gallstones
• Risks of not having surgery – symptoms continue, potential for complications & sequelae
• May need to convert to open cholecystectomy if not possible to do lap approach (5-10%conversion rate)
• May need to insert T-tube or wound drain
General risks/complications
• Reaction to anaesthetic &/or contrast
• Wound haematoma
• Infection
• Atelectasis +/- pneumonia
• Incisional hernia
• DVT/PE
Specific risks/complications
•
Mortality < 1 in 1000• Gas embolus – heart, lungs or brain
• Collection – bile (biloma), blood or pus
• Bile leaks – caused by injury to CBD, R hepatic duct or cystic duct – causes external biliary
fistula
• Bile duct stricture
• Damage to vasculature (eg R hepatic artery) causing haemorrhage
• Damage to nearby structures – liver, colon, porta hepatis, diaphragm

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 35/45
• Adhesions
• Potential for missed stones – may need ERCP or further operation
• ‘Post-cholecystectomy syndrome’
What length of hospital stay is necessary ? How long till feeling better ?
• Pain, nausea & vomiting may occur
• May need T-tube in-situ
• Usually ambulatory within 24 hrs
• May need narcotics in first 24 hrs, then oral analgesics (panadeine) for ~ 4-5 days
• NBM initially (& IV fluids), then sips of water (~ 24 hours, due to ileus), then normal diet
• Usually discharged after 1-2 days (compared with 5 days for an open procedure) – avoidstrenuous exercise & heavy lifting for > 2 weeks
• Recovery time frameso Drive after & 7 days
o Return to normal activity after ~ 2 weeks (c/w 4 weeks for open procedure)
Acute pancreatitis
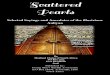
What are the above sign’s called ?
Left = Cullen’s sign ; Right = Grey-Turner’s sign
What is the underlying pathogenesis & cause ?
• Haemorrhagic acute pancreatitis – bleeding into parenchyma & retroperitoneal structures with
extensive pancreatic necrosis – indicates severe pancreatitis has been present for several days
• Cullen’s sign : bluish discolouration of the periumbilical area – caused by retroperitoneal
haemorrhage tracking around to the anterior abdominal wall thru fascial planes (think –cUllen’s sign = Umbilicus)

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 36/45
• Grey-Turners sign : ecchymosis or discolouration of the flank – caused by retroperitoneal
haemorrhage (think – Grey-Turner = turn on side to see it)
• Fox’s sign : ecchymosis of the inguinal ligament
List ! 6 causes of pancreatitis
GET SMASHED :
• Gallstones**
• Ethanol**
• Trauma
• Steroids
• Mumps, Mycoplasma
• Autoimmune : PAN, SLE
• Scorpion stings
• Hyperlipidemia/ Hypercalcemia
• ERCP
•
Drugs, eg azathioprine
What are the other causes of this sign ?
• Other causes of retroperitoneal bleeding may produce these signs – ruptured AAA,malignancy, coagulopathy
What are the other clinical features of acute pancreatitis ?
Symptoms
• Severe constant epigastric pain that often radiates to the back
o
Acute onset – builds up over 15-60 min
• Nausea & vomiting
Signs
• Sepsis : tachycardia, hypotension, pyrexia, jaundice
• Epigastric tenderness (or diffuse abdominal tenderness)
• " bowel sounds due to paralytic ileus
• Large pseudocyst ! constant abdo pain, palpable abdo mass
• Severe ! hypoxaemia, hypovolaemic shock
What is the biochemical investigation of choice ?
• Serum amylase > 1000U/L (also do serum lipase FBC, E/LFTs, glucose, calcium, ABGs,USS, plain CXR & AXR)
• Damage to pancreas! release of amylase into bloodstream! rapid rise in serum level (it isalso rapidly cleared within 24hrs)
What criteria are used to assess the severity of pancreatitis ?

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 37/45
• Ranson’s criteria (2 or more signs assoc/ w/ ! incidence of haemorrhagic pancreatitis &death)
• Imrie (Glasgow) scores
• APACHE II
•
The more criteria present, the more severe the illness
List ! 2 criteria which indicate a worser prognosis.
• On admission : GA LAW
o Glucose > 10 mmol/l
o Age > 55 yrso LDH > 600 U/L
o AST >120 U/L
o WCC > 16,000
• Within 48 hours : Calvin & HOBBS
o
Calcium < 2 mmolo Haematocrit fall >10%
o Oxygen - pO2 < 60 mmHgo Base deficit > 4
o BUN rise >0.9 mmol/L
o Sequestration of fluid > 6L
•
! number of positive criteria! ! mortality (7-8 criteria = 100% mortality)
• In addition, serial assessment of CRP is a useful indicator of progress & severity
What is the management of pancreatitis ?
Medical management• Supportive therapy & intensive monitoring (T/P/R, BP, O2 sats, urine output) : often in ICU
• Regular assessment of U&Es, Ca2+
, blood sugar & LFTs – correct abnormalities
• NBM
• IV fluid resuscitation with both colloid & crystalloid
• Correct hypoxia! O2 &/or ETT
• Opioid analgesia (meperidine, not morphine)
• Nutrition – pancreatitis is hypercatabolic – often require NG tube &/or TPN
• Antibiotic prophylaxis (eg imipenem, cefuroxime)
• H2-blocker
Surgical management
• Complications such as pseudocyst necessitate surgical management
• Drainage essential for pseudocyst – may be percutaneous, endoscopic or surgical (drainageinto stomach/duodenum – cystgastrostomy)
• ERCP – performed to clear CBD of gallstones if this is the cause
• Laproscopic cholecystectomy – if caused by gallstones to prevent recurrence

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 38/45
VASCULAR SURGERY
Peripheral vascular disease
What are the major RF’s for atherosclerosis ?
• Non-modifiable RF’s
o ! age & sex (' & postmenopausal ()
o FHx/geneticso PHx IHD/CVA
• Modifiable RF’s :
o Hypercholesterolaemia & hyperlipidaemia
o Smoking
o Hypertension
o Diabetes mellitus
o Obesity, physical inactivity & poor diet
o
Hyperhomocysteinaemia, excess alcohol, stress/personality, haemostatic factors
In what ways can lower limb occlusive disease present ?
• Asymptomatic
• Intermittent claudication
• Rest pain (critical limb ischaemia)
• Acute occlusion
What are the common sites of involvement ?
•
Superficial femoral artery (SFA) – most common site of arterial occlusion is in the adductor(Hunter’s) canal, 15cm below the inguinal ligament
o Calf pain
• Aorto-iliac region
o * Buttock &/or thigh &/or calf pain
• Popliteal artery
Describe differences b/w intermittent claudication & rest pain ? How do you assess it ?
Intermittent claudication
• Ischaemic pain of the leg that is precipitated by ambulation & relieved by rest
o
Typically a cramp-like pain & varies from an ache to acute severe paino Cyclical pattern of exacerbation & resolution due to progression of disease &
subsequent dev’t of collaterals
• Location of pain depends on arteries affected
o SFA (most common) = calf pain
o Iliac A = calf, thigh &/or buttock pain
• Other useful information

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 39/45
o Claudication distance – distance travelled before pain occurs – usually reasonably
constant, but will be reduced when walking uphillo Relief – pain will be relieved by rest, often after a reasonably constant time-period
o Duration of symptoms
o Severity of symptoms – does the claudication force patient to stop walking ?
•
5% limb loss at 5 years• DDx : neurogenic claudication, sciatica, OA
Rest pain (critical limb ischaemia)
• Pain in the foot or toes that arises at rest
• Classically occurs at night – will wake from sleep & requires opiate analgesia to enable sleep
• Resolved by hanging the foot over the side of bed or standing/walking – gravity affords some
extra flow to the ischaemic areas
• Ulceration & gangrene may be present
• " Indicates threatened loss of limb (critical limb ischaemia) – more than 50% of patients willhave amputation of the limb at some point
What are the signs of lower limb ischaemia (see Browse p170 – describe the features seen in
this foot ? what is the underlying pathology ?)
Inspection
• Thin, shiny, atrophic & pale skin
• Loss of hair
• Muscle atrophy
• Dry, thin & brittle nails
• Ulceration (usually on toes/feet), infection &/or gangrene
•
Venous ‘guttering’ – veins empty due to inadequate circulation
Palpation
• " skin temperature
• Capillary return (> 3 seconds is abnormal)
• " or absent peripheral pulses – femoral, popliteal, dorsalis pedis & posterior tibial pulses
• Occasionally can detect palpable collateral vessels (eg medial side of knee joint)
• Buerger’s sign – elevation of leg causes pallor – on dependency affected limb will regain itscolour more slowly than the healthy limb, followed by a rubor due to reactive hyperaemia
Auscultation
•
Auscultate the main vessels – systolic bruit indicates stenosis at that level or higher up
Gangrene (Browse p171)
• Gangrene : necrosis due to obstruction, loss, or diminution of blood supply
• Dry gangrene : dry necrosis of tissue without signs of infection (‘mummified tissue’)
• Wet gangrene : moist necrotic tissue with signs of infection
• May be a clear demarcation b/w dead & living tissue

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 40/45
• Dead tissue is brown or black & gradually contracts into a crinkled, withered, hard mass –
infection causes the dead tissue to become soft & boggy, with pus at line of demarcation
• Extent of necrosis varies from a black patch to extensive gangrene of the foot – it startsdistally on the toes & extends proximally
• Dead part is senseless & not painful
Ulceration
• Ischaemic ulceration usually begins in a pressure area, usually on the foot
• Dead tissue is usually present & granulation tissue is absent
What are suitable investigations ?
Assess extent of PVD
• ABI – ratio of systolic BP at ankle to systolic BP at arm : Normal ) 1, claudication " 0.6-0.9,rest pain 0.3-0.6
• Duplex USS with colour Doppler – non-invasive
•
DSA – gold standard but invasive
Look for a cause
• FBC, U&E, lipids, glucose, syphilis serology
What would you warn a patient about to undergo DSA about to obtain consent ?
Pre-procedure preparation
• Ask about allergies (esp iodine) & previous exposures to x-ray contrast
• Determine medications & past history
• Check & document pulses prior to puncture
•
Laboratory studies : PT, APTT, U&Es, FBC• Withhold aspirin, warfarin & metformin prior to procedure
• Correct coagulopathies using FFP
Required preparation
• Shave & prep groin
• Clear liquids & 8 hours prior to procedure
• IV fluids to maintain hydration
Procedure
•
Arterial access via the Seldinger technique (Radiology recall p209), commonly via thecommon femoral artery (below inguinal ligament) or brachial artery
• Guidewire is advanced into vessel under II guidance – catheter is then passed over wire into
vessel lumen, and guidewire is then removed
• Catheter is then manipulated to desired location & contrast injected
Post-procedure care

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 41/45
• Apply firm manual compression for > 15 minutes
• Patient must lie flat with limb straight for 6-8 hours
• Evaluate distal pulses & regular observations (cardio, neuro, puncture site)
Complications
•
Mortality < 0.05%• Contrast
o Anaphylactoid reactiono Nephrotoxicity
• Vascular access
o Haemorrhage or haematoma (5%)
o Pseudoaneurysm
o AV fistulao Infection
o Nerve damage
• Distal vasculature
o
Thrombosiso Embolism
o Dissection
o Perforation
• Potential interventions
o Surgical
o Worst case scenario is amputation
What are the management options ?
Conservative
•
P entoxifylline (" blood viscosity) • Aspirin or ticlodipine
• C essation of smoking & treat other RF’s
• E xercise
Surgical
• Ischaemic rest pain necessitates urgent surgical intervention
• Angioplasty : radiologically-guided balloon angioplasty +/- stent placement is effective in patients who have a short segment of stenosis (usually < 3cm) – most patients have long ormultiple segments of SFA disease
• Endarterectomy : diseased intima & media are ‘cored out’
•
Bypass graft : a graft is made to bypass the diseased segments of artery & improve distalflow, provided there is minimal arterial disease in the distal vessels – graft can be a synthetic
PTFE tube graft, dacron graft or a vein graft (veins have a longer patency rate)o Fem-pop bypass : bypass SFA occlusion with graft from femoral artery to popliteal
artery above the knee
o Fem-distal bypass : bypass from femoral artery to a distal artery (peroneal artery,
anterior tibial artery or posterior tibial artery)

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 42/45
Acute limb ischaemia
List ! 5 causes of acute limb ischaemia
•
Embolisationo Cardiac – mural thrombi (AF, MI), vegetations (endocarditis)o Aneurysms (aorta, femoral or popliteal)
o Atheroemboli
• Acute thrombosis of an atheromatous lesion
• Vascular trauma – arterial transection, AV fistula, intimal dissection
What are the clinical features
Sudden onset of :
• Pain
•
Pallor – fixed mottling heralds the onset of gangrene• Pulselessness
• Perishing cold (others say poikilothermia or polar)
• Paraesthesia & sensory disturbances – impending irreversible ischaemia
• Paralysis – muscle rigidity implies that the damage is irreversible
List the immediate emergency measures for the treatment of a patient with acute limb
ischaemia. List the initial baseline investigation that you would undertake.
• Anticoagulate with IV heparin – bolus followed by constant infusion – prevents furtherthrombosis
•
Angiogram• Also do ECG & echo looking for embolic source
" Unless blood flow is restored within 4-6 hours, irreversible tissue damage will occur, leading
to possible amputation.
Definitive management
• Surgical embolectomy or thrombectomy via arterial cutdown & Fogarty balloon catheter
• Thrombolysis (streptokinase, urokinase, t-PA) may be infused locally to lyse a thrombus

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 43/45
Leg ulcers
Describe the ulcer seen in the photo
Probably a venous ulcer
• Edge is sloping & made of new epithelium
• Base is clean & pink
• Surrounding tissue looks healthy
" Remember SEBS – site/size/shape/severity, edge, base, surrounding tissue/LNs
Site/position & its anatomic relations
Venous – medial side of lower leg Arterial – pressure areas of dorsum of feet,lateral side of lower leg & tips of toes
Neuropathic – weight-bearing areas Neoplastic – sun-exposed areas

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 44/45
Size, shape, colour & tenderness
# Edge
“Sloping” edges indicates healing (# not arterial or neuropathic)
$
Base/floor• Usually consists of slough or granulation tissue
• Contents of floor
o Ischaemic : dry or extended base or necrotic eschar
o Venous : superficial with fibrinous exudate & ooze
• Colour :
o Black = necrosis
o Yellow = slough
o Red = granulationo Pink = epithelium
% Depth • Record in millimetres & anatomically (described structures penetrated)
& Discharge
• Quantity & type of discharge – serous, sanguinous or purulent
' Surrounding skin/tissue
• Colour – local blood supply, inflammation
• Sensitivity
• Pulses
• Look for evidence of previous ulcers
( Regional lymph nodes
• May be enlarged &/or tender due to secondary infection or neoplasia
Indicates rapid death & minimal healing
Rapid growth of tissue at edge of ulcer = carcinoma
Slow growth of tissue at edge of ulcer (rodent ulcer)

7/17/2019 Surgical Pearls
http://slidepdf.com/reader/full/surgical-pearls 45/45
What are the causes of leg ulcers ?
Venous ulcers (75%)•
Varicose veins• Post-thrombophlebitis
Arterial ulcers • Ischaemic – diabetes, artherosclerosis, embolism
• Vasculitic – Buerger’s disease, SLE, RA, scleroderma
Neuropathic ulcers • Neuropathic (trophic) – diabetes, alcoholism, syphilis
• Spinal cord lesion – spina bifida, tabes dorsalis,
syringomyelia
Traumatic • Pressure sores (decubitus)
• Ill-fitting footwear
• Traumatic lesions
• Self-inflicted
Neoplastic •
SCC
•
BCC
• Malignant melanoma
• Kaposi’s sarcoma
Haematological • Spherocytosis
• Sickle cell anaemia
Infective • Tropical ulcer
• Mycobacteria
• Post-cellulitis
• Chronic infected sinus
Miscellaneous •
Pyoderma gangrenosum• Spider/insect bites
What questions would you ask the patient to determine a cause ?
• Onset & duration of ulcer
• Has ulcer changed since it first appeared ?
• What do they think caused the ulcer ? – may note precipitating injury
• Pain – ischaemic ulcers are painful, venous ulcers have minimal pain, neuropathic ulcers painless
• Bleeding/discharge
•
PHx :
o Venous – DVT or PE, varicose veins, previous surgery on leg
o Arterial – intermittent claudication & rest pain; cardiovascular diseaseo Other – diabetes, RA, vasculitis, IBD, chronic skin ulcers
• Medications : %-blockers, ergotamine, corticosteroids, NSAIDs, nifedipine
i l b