Embed Size (px)
Citation preview
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 1/56
Surgical Problems in Children
BY Ragheb Assaf ,MD

8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 2/56
ProblemsGASTROINTESTINAL- Pyloric stenosis- Malrotation
- Midgut volvulus- Duodenal atresia- Meconium ileus- Intussusception
- Meckel¶s diverticulum- appendicitis- Hirschsprung¶s disease
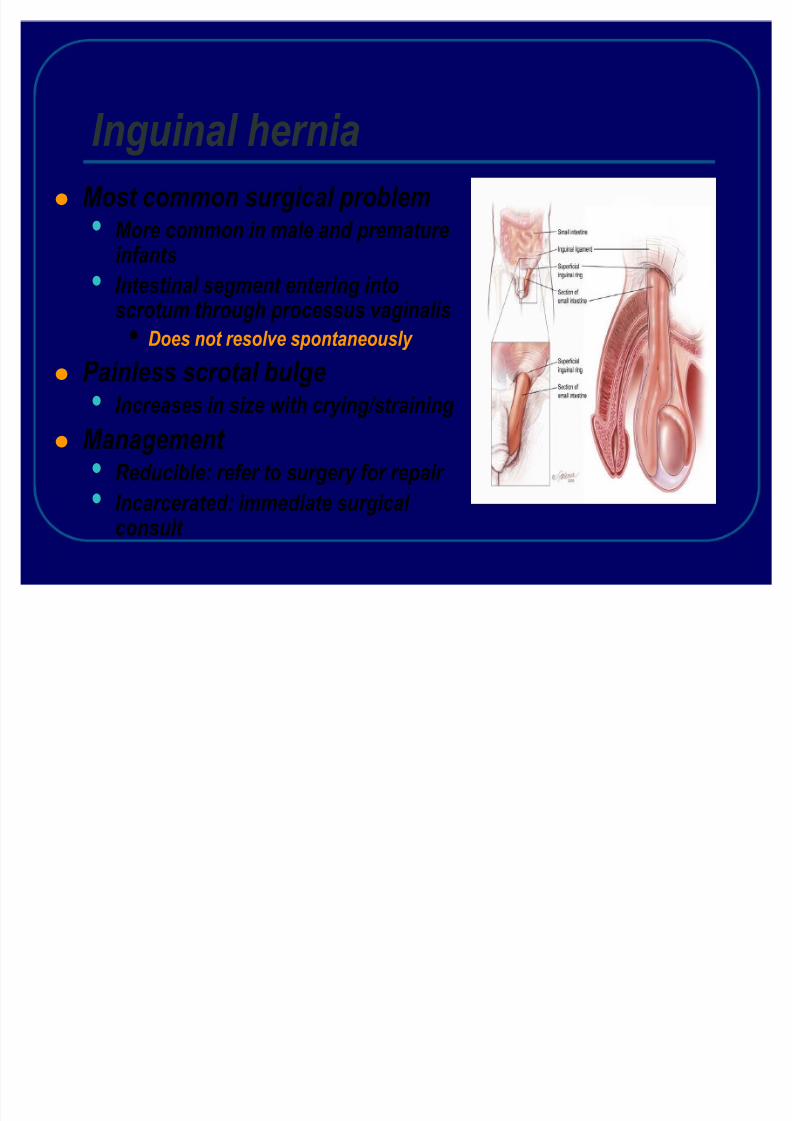
GENITOURINARY ± Inguinal hernia
± Umbilical hernia- Hypospadias- Phimosis/paraphimosis- Cryptorchidism- Hydrocele- Testicular torsion
OBJECTIVES
-Recognize-Diagnose-C onsult surgery

8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 3/56
Pyloric stenosisHypertrophy of the gastric outlet
1:150 males, 1:750 females2-12 weeks of age
Repetitive vomitingProjectileNon-bilious
DehydrationHypochloremic alkalosis
ExamVisible peristaltic wavePalpable ³olive´ to right of umbilicus
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 4/56
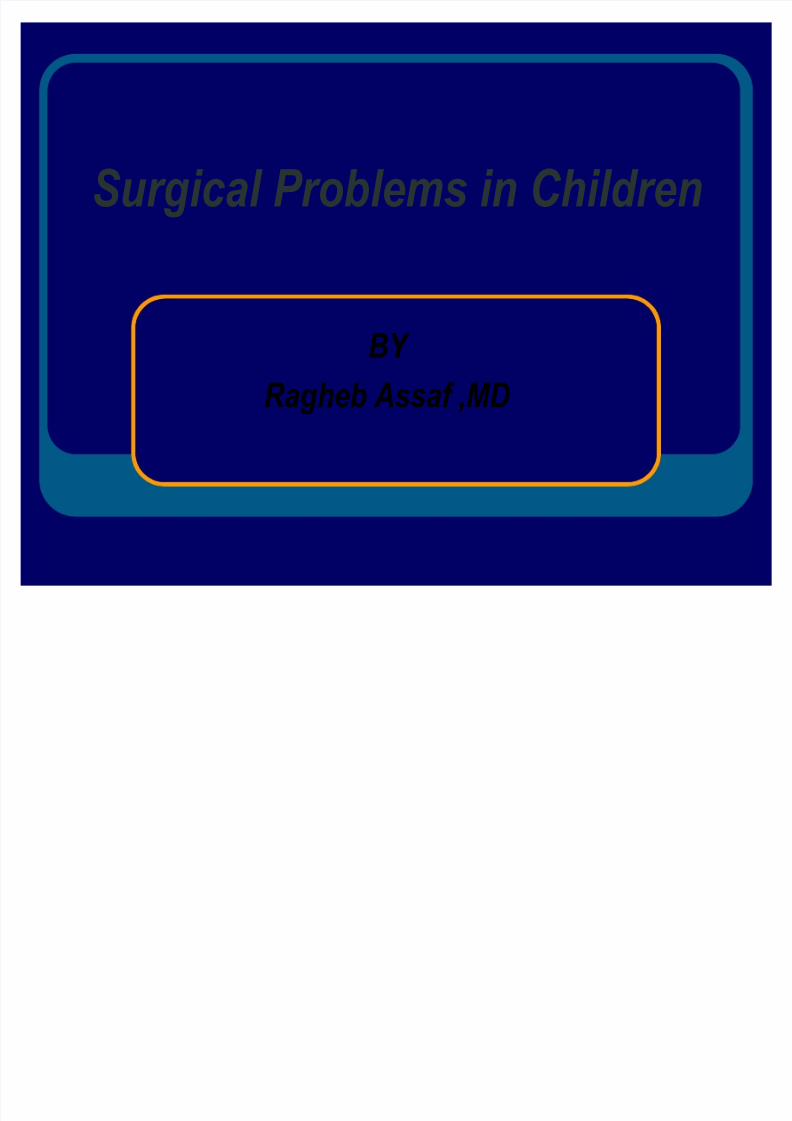
Pyloric stenosis: DiagnosisUG I
Delayedpassage of barium throughthickened pyloricchannel
U ltrasound
Thickened,elongatedpyloricchannel
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 5/56
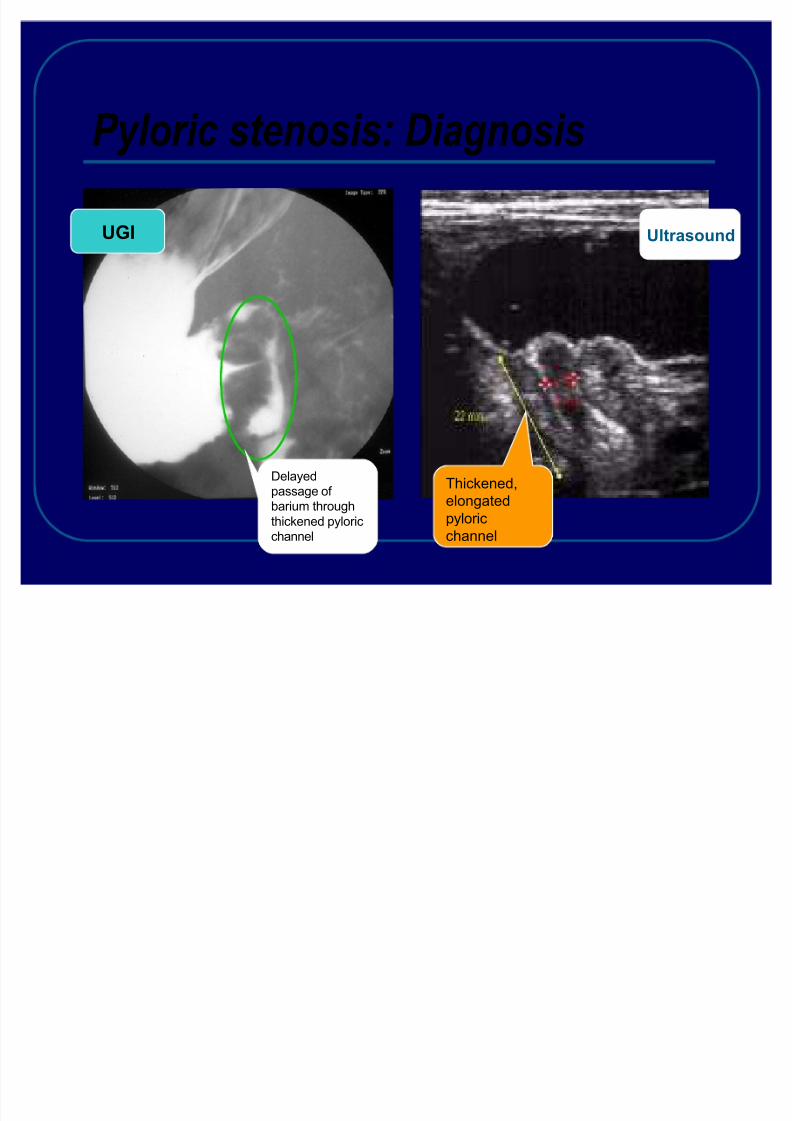
Pyloric stenosis :treatment
Hypertrophy of pylorus
E ndoscopic balloon dilation
S urgical tx = pyloromyotomy

8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 6/56
Surgical treatment
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 7/56
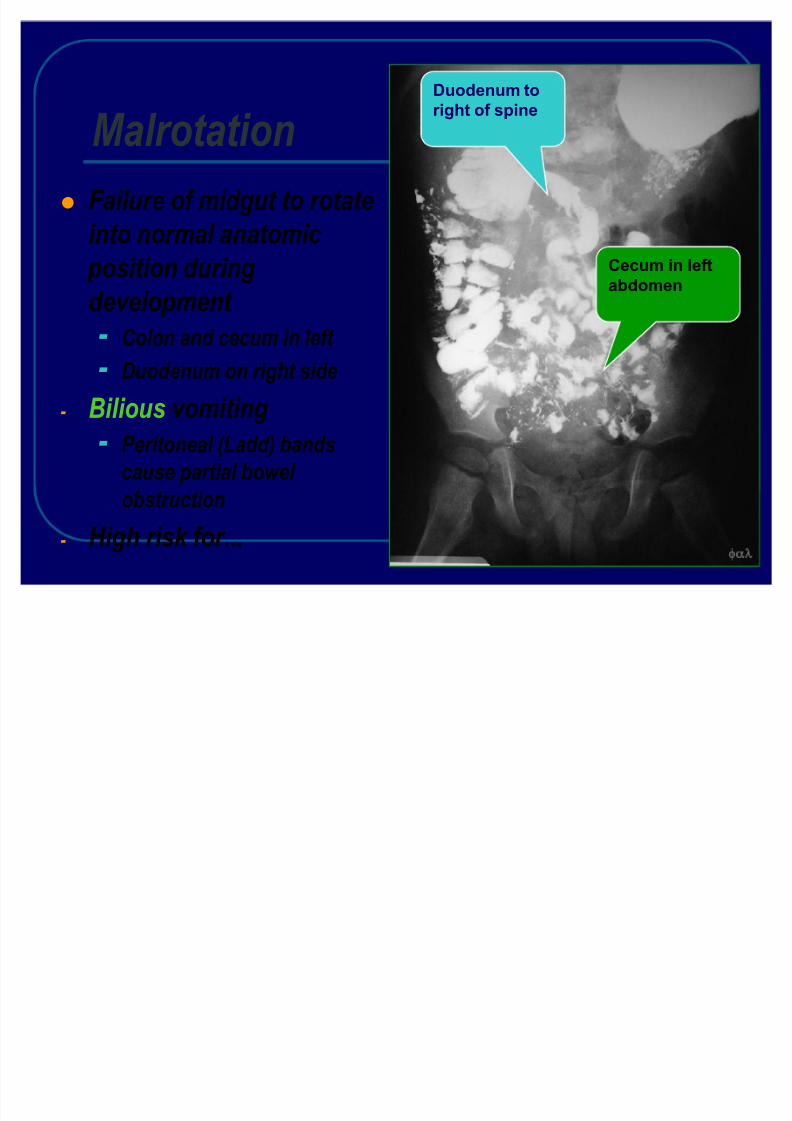
MalrotationFailure of midgut to rotateinto normal anatomic
position duringdevelopment - Colon and cecum in left - Duodenum on right side
- Bilious vomiting- Peritoneal (Ladd) bandscause partial bowel obstruction
- High risk for...
Duodenum toright of spine
C ecum in leftabdomen
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 8/56
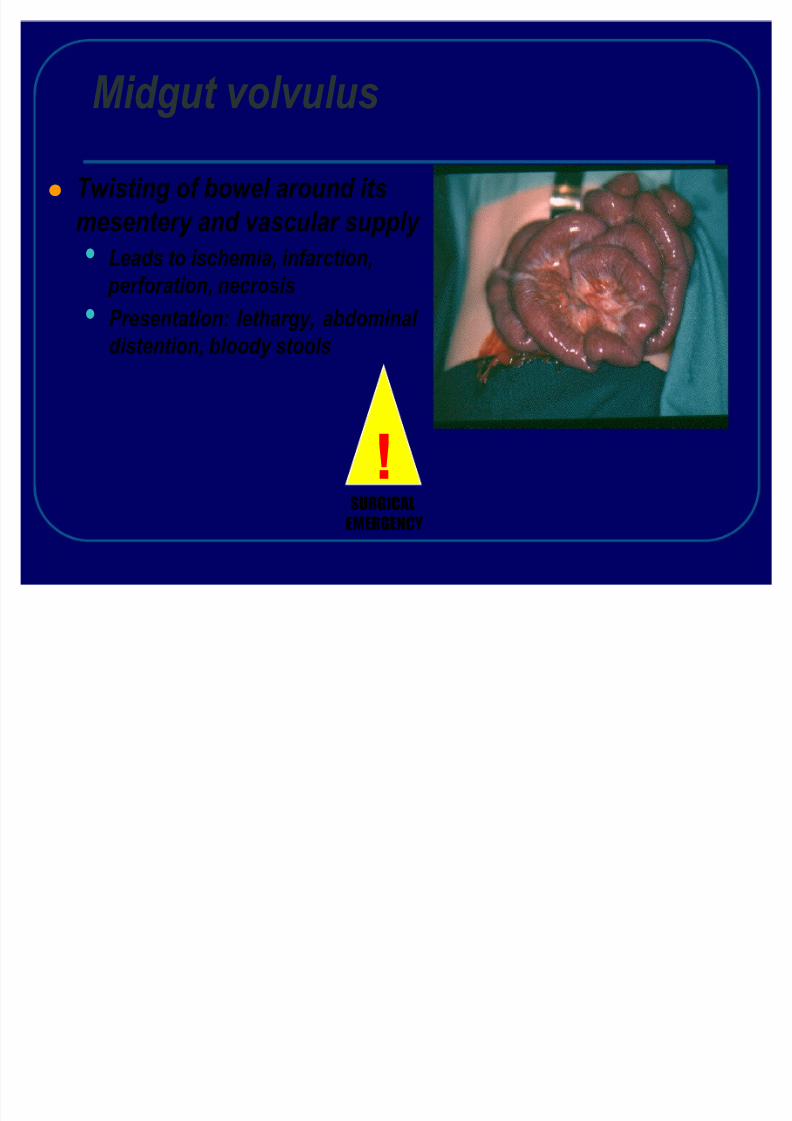
Midgut volvulus
Twisting of bowel around itsmesentery and vascular supply
Leads to ischemia, infarction, perforation, necrosisPresentation: lethargy, abdominal distention, bloody stools
!SURGICAL
EMERGENCY
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 9/56
MALROTATION
M ust consider in every infantwith bilious emesis
30% present within first week of life50% within first monthM idgut volvulus with necrosisdisastrous
C an lead to SBS, death
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 10/56
C LINI C AL P RE S ENTATION of
MALROTATION
Sudden onset of bilious emesis in 95 %
A bdominal distention common
Blood stool +
Bloody vomitus or diarrhea in 30%
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 11/56
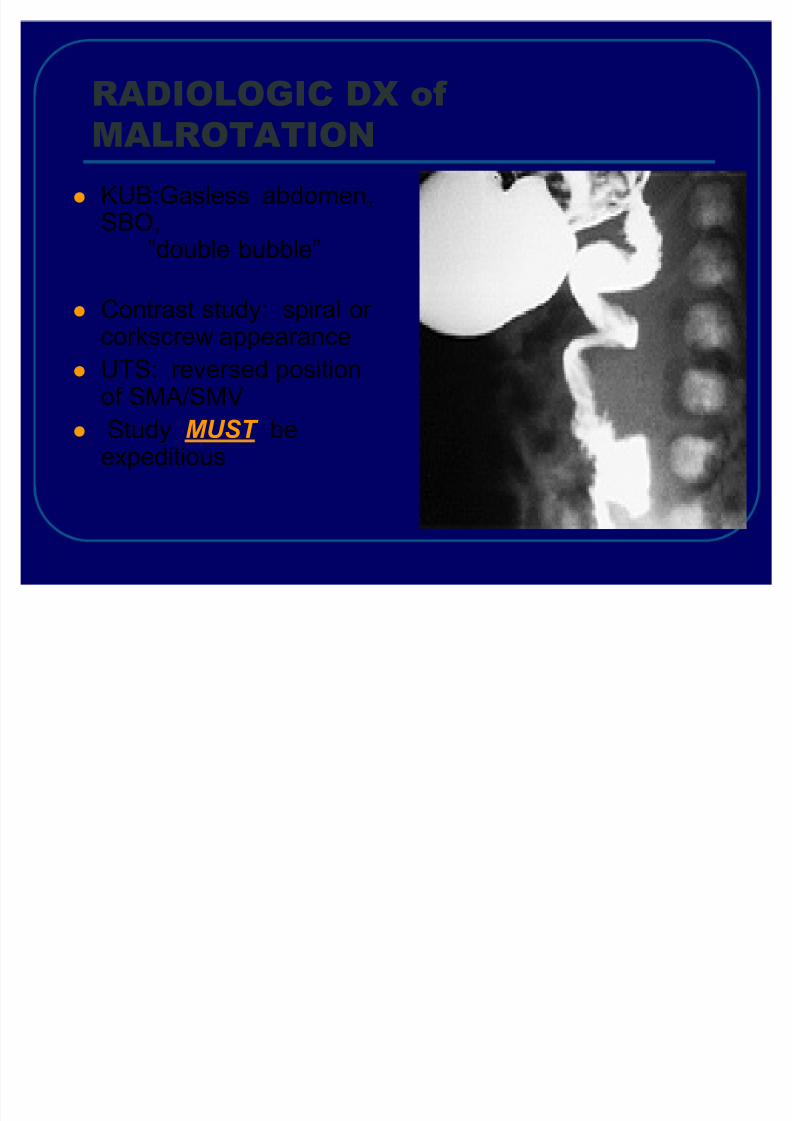
RADIOLOGI C DX of
MALROTATIONKU B:Gasless abdomen,SBO,
³double bubble´
C ontrast study: spiral or corkscrew appearanceU TS: reversed positionof S MA/ S MV
Study MUST beexpeditious

8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 12/56
P REO P ERATIVE P RE P ARATION:
MALROTATIONW
ITH VOLVULU
SL abs / unnecessaryM ortality remains as high
as 28 %P reoperative preparation?? N O N E !!
... GO TO OR« . QUICK LY
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 13/56
O P ERATIVE C ORRE C TION of
MALROTATION
L add procedure
P osition of corrected malrotationSmall bowel descends on RightL arge bowel on L eft A ppendix potentially in L U Q p Removed
Role of second look operation

8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 14/56
Duodenal atresiaObliteration of lumen
Failure to recanalize
Neonatal bilious vomiting Associations
Prematurity Congenital heart defects
Trisomy 21C omplete
small bowelobstruction
Doubl ebubbl e sign
!SURGICAL
EMERGENCY
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 15/56
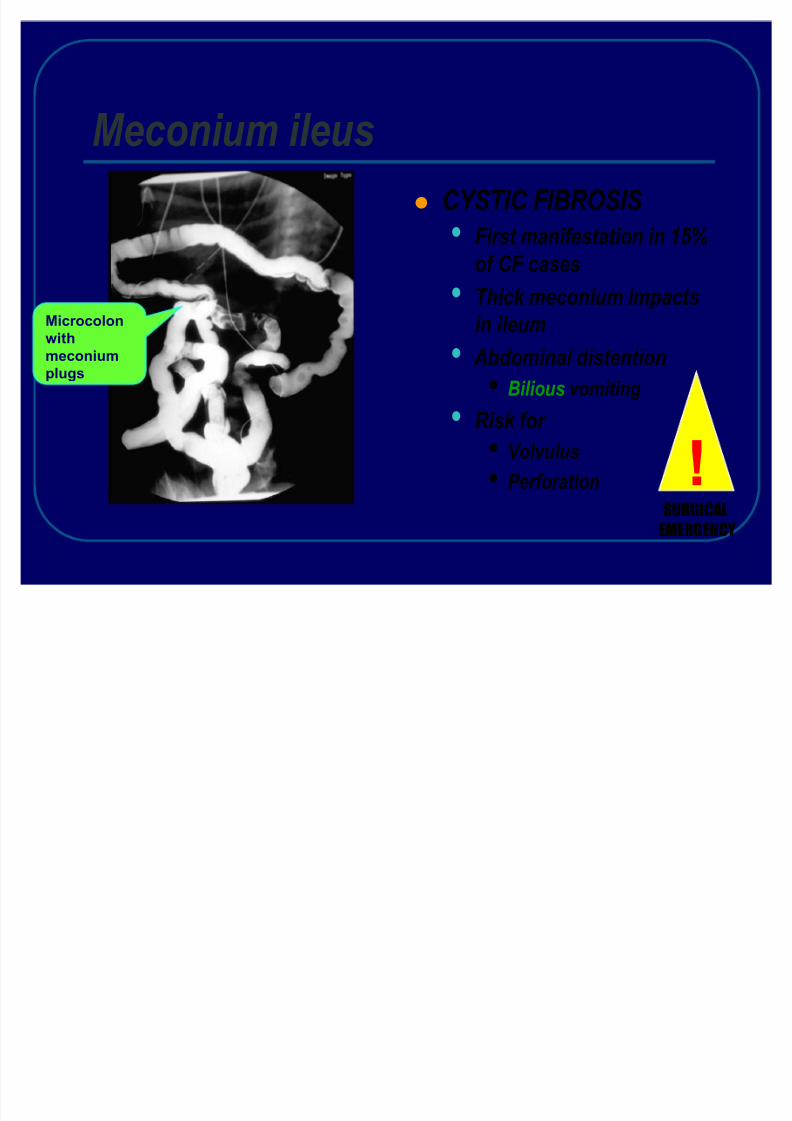
Meconium ileusCYSTIC FIBROSIS
First manifestation in 15%of CF casesThick meconium impactsin ileum Abdominal distention
Bilious vomiting
Risk for VolvulusPerforation
M icrocolonwithmeconiumplugs
!SURGICAL
EMERGENCY
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 16/56
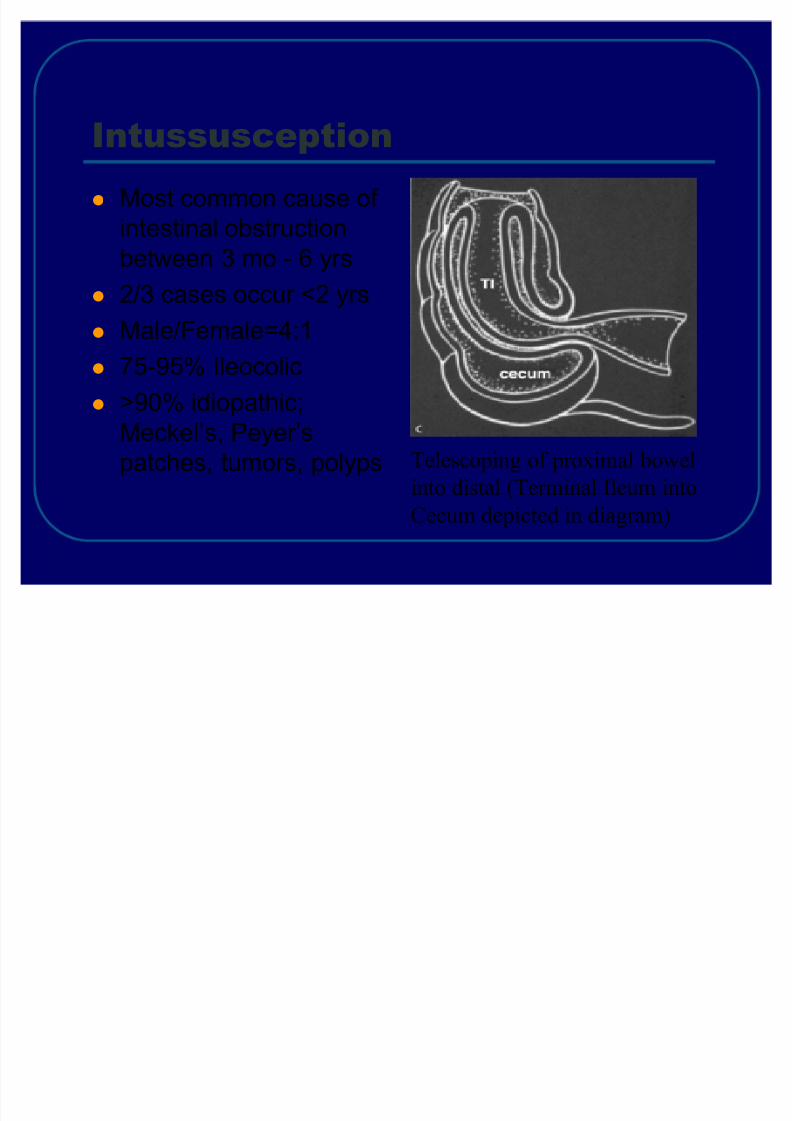
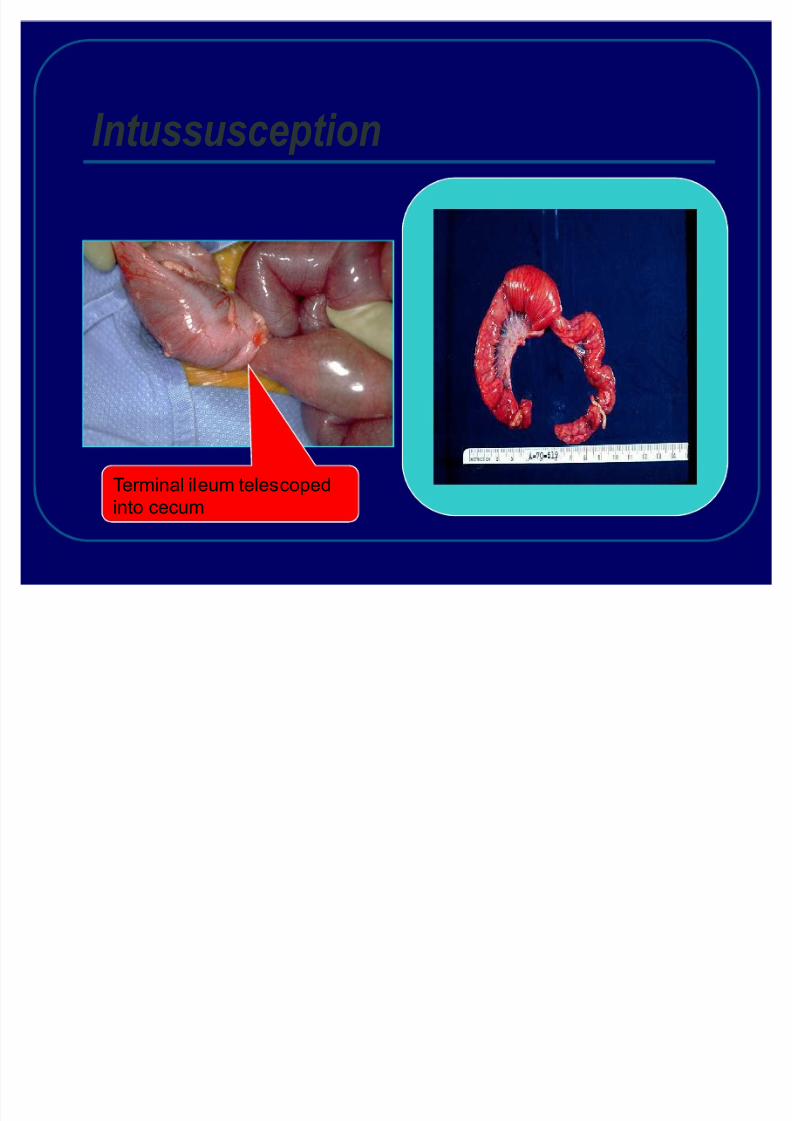
I ntussusceptionM ost common cause of intestinal obstructionbetween 3 mo - 6 yrs2 /3 cases occur <2 yrsM ale /F emale=4:175-95 % Ileocolic>9 0% idiopathic;M eckel¶s, P eyer¶spatches, tumors, polyps Telescoping of proximal bowel
into distal (Terminal Ileum intoCecum depicted in diagram)
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 17/56
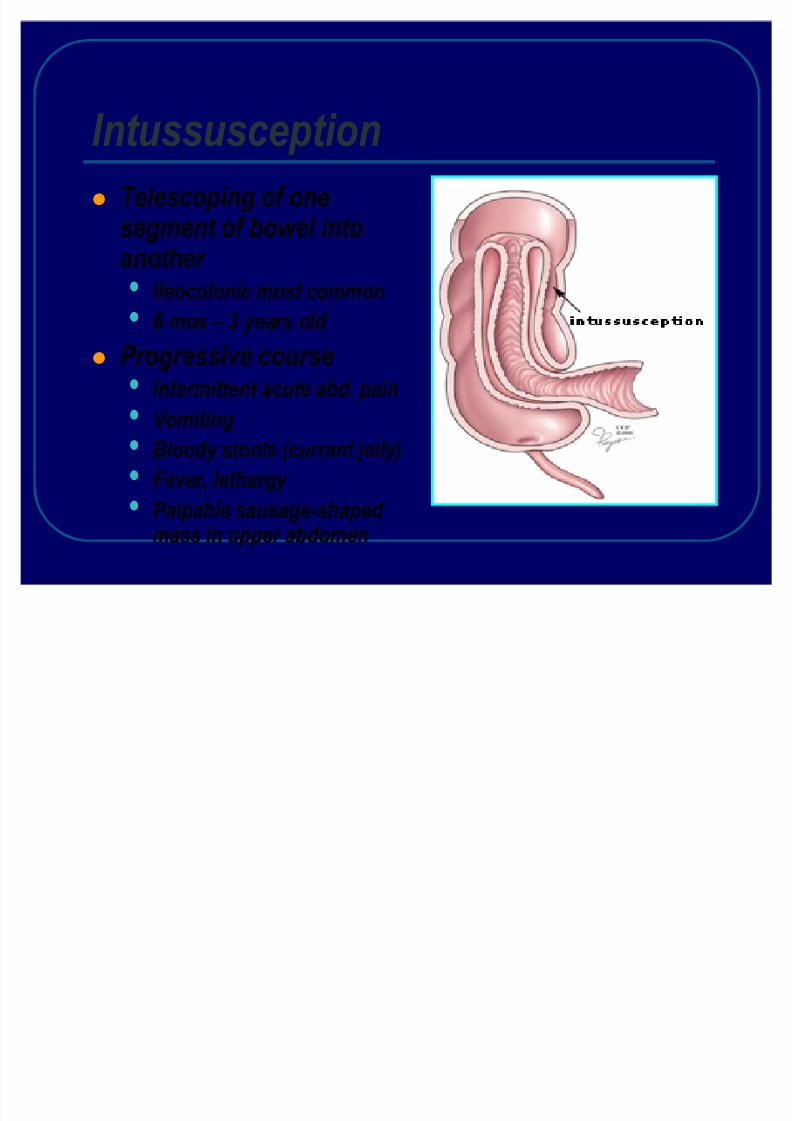
IntussusceptionTelescoping of onesegment of bowel intoanother
Ileocolonic most common6 mos ± 3 years old
Progressive courseIntermittent acute abd. pain
VomitingBloody stools (currant jelly)Fever, lethargy Palpable sausage-shaped mass in upper abdomen
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 18/56
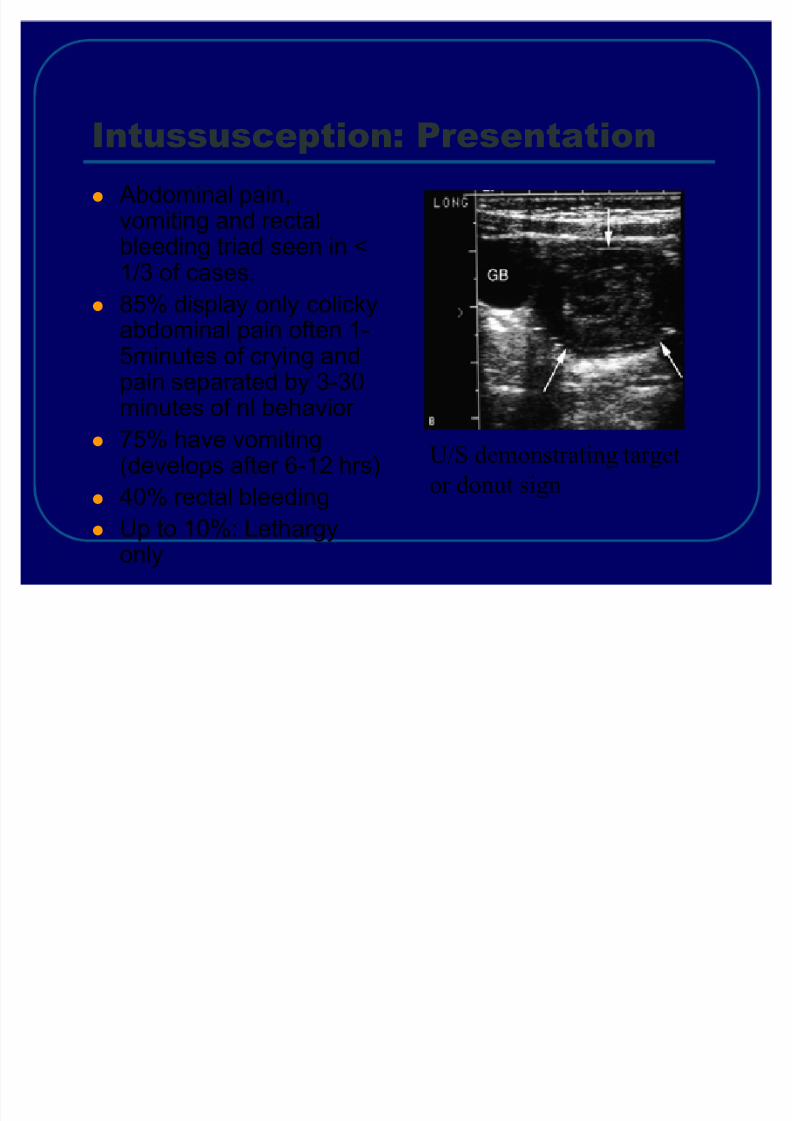
I ntussusception : PresentationA bdominal pain,vomiting and rectalbleeding triad seen in <
1 /3 of cases .85 % display only colickyabdominal pain often 1-5minutes of crying andpain separated by 3 -30
minutes of nl behavior 75 % have vomiting(develops after 6-12 hrs)40% rectal bleedingU p to 1 0% : L ethargyonly
U/S demonstrating targetor donut sign
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 19/56
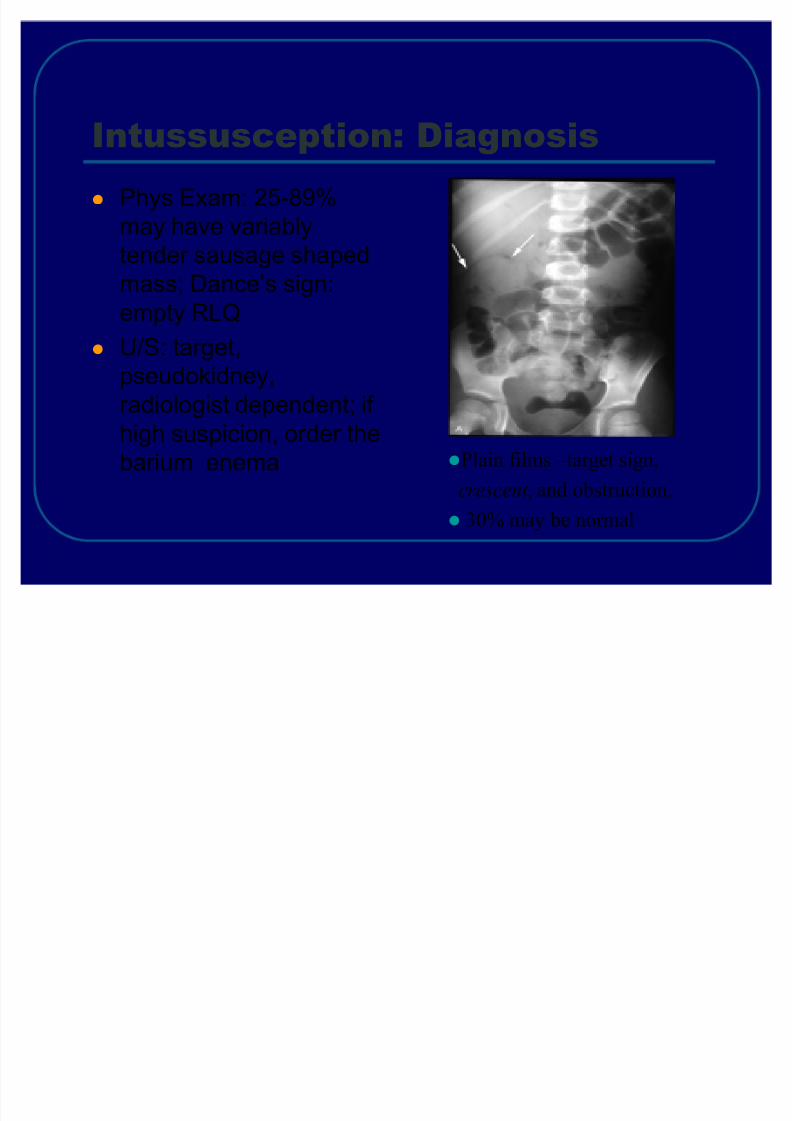
I ntussusception : D iagnosisP hys Exam: 25-89 % may have variablytender sausage shapedmass; Dance¶s sign:empty R L QU /S: target,pseudokidney,
radiologist dependent; if high suspicion, order thebarium enema P lain films ±target sign,
crescent , and obstruction,30% may be normal
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 20/56
I ntussusception : M anagementEnema: diagnostic & therapeutic, ³coiledspring´
Surgery must be consulted prior to study.
Barium vs . A ir- 80% correction if within first 12-24 hrs .
A ir Enema- safer if perforation
5-10%
recurrence rate in first 24-48h after barium enema reductionIf free air on films or signs of peritonitis, do notadminister barium, prepare child for surgery
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 21/56
Intussusception Management
Ultrasound : Hydrostatic pressure reduces theintussusception
Surgeon must be involved directly If enema reduction failsSmall bowel intussusceptions requiresurgical reduction
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 22/56
Intussusception
Terminal ileum telescopedinto cecum
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 23/56
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 24/56
A ppendicitis80 ,000 cases in children /year /in U S A
Rare in children < 2years20 -4 0% misdiagnosed on initial exam50 -7 0% perforation rate in pre-schoolM ortality Rates of 5 % in perforated vs0 .1% in non-perforated appendicitis
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 25/56
A ppendicitis
P athophysiology: obstruction of appendix by fecalith or lymphoidtissue causes congestion,
distention, ischemia, infection &perforation .
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 26/56
H istoryM igration of pain from initial periumbilicalto R L Q was 64 % sensitive and 82 %
specificA norexia is the most common of associated symptoms
V omiting is more variable, occuring inabout ½ of patients
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 27/56
Physical Ex amF indings depend on duration of illnessprior to exam .
Early on patients may not have localizedtendernessWith progression there is tenderness to
deep palpation over M cBurney¶s point

8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 28/56
Physical Ex amM cBurney¶s P oint: just below the middleof a line connecting the umbilicus and
the A S ISRovsing¶s: pain in R L Q with palpation toLL Q
Rectal exam: pain can be mostpronounced if the patient has pelvicappendix
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 29/56
Physical Ex amF ever: another late finding .
A t the onset of pain fever is usually notfound . Temperatures > 3 9 C are uncommon infirst 24 h, but not uncommon after
rupture
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 30/56
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 31/56
D iagnosisImaging studies: include X-rays, U S, C TXrays of abd are abnormal in 24-95 %
A bnormal findings include: fecalith,appendiceal gas, localized paralyticileus, blurred right psoas, and free air
A bdominal xrays have limited use b /c thefindings are seen in multiple other processes
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 32/56
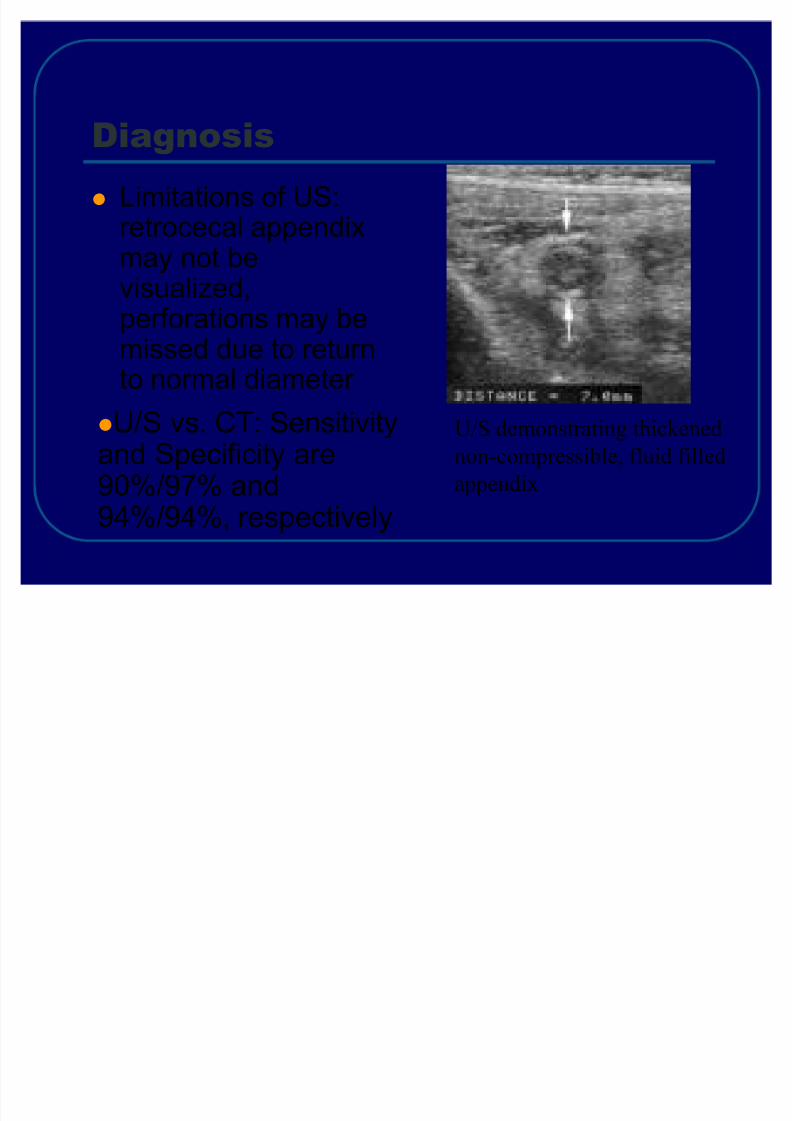
D iagnosisL imitations of U S:retrocecal appendixmay not bevisualized,perforations may bemissed due to returnto normal diameter
U/S demonstrating thickenednon-compressible, fluid filledappendix
U /S vs . C T: Sensitivityand Specificity are90%/ 97 % and94 %/ 94 % , respectively
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 33/56
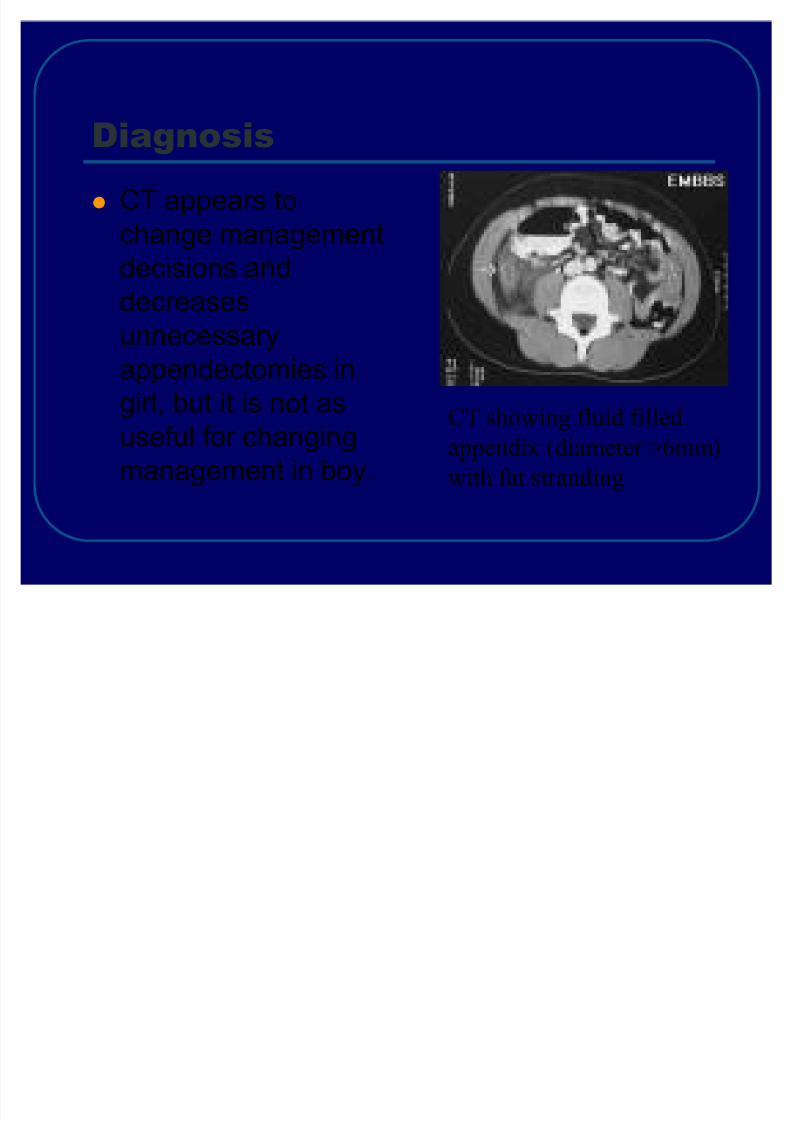
D iagnosisC T appears tochange management
decisions anddecreasesunnecessaryappendectomies ingirl, but it is not asuseful for changingmanagement in boy .
CT showing fluid filledappendix (diameter >6mm)with fat stranding
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 34/56
T reatmentA ppendectomy is the standard of careP atients should be N P O, given IVF , andpreoperative antibioticsA ntibiotics are most effective when givenpreoperatively and they decrease post-
op infections and abscess formation
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 35/56
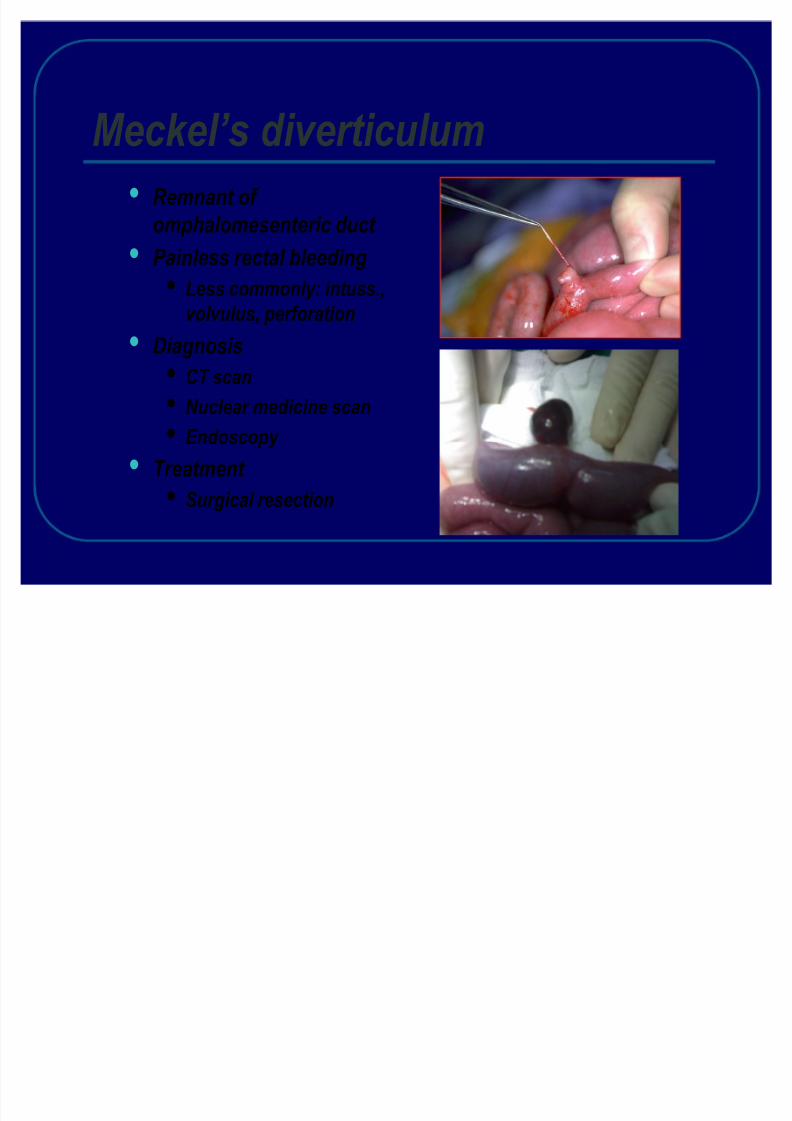
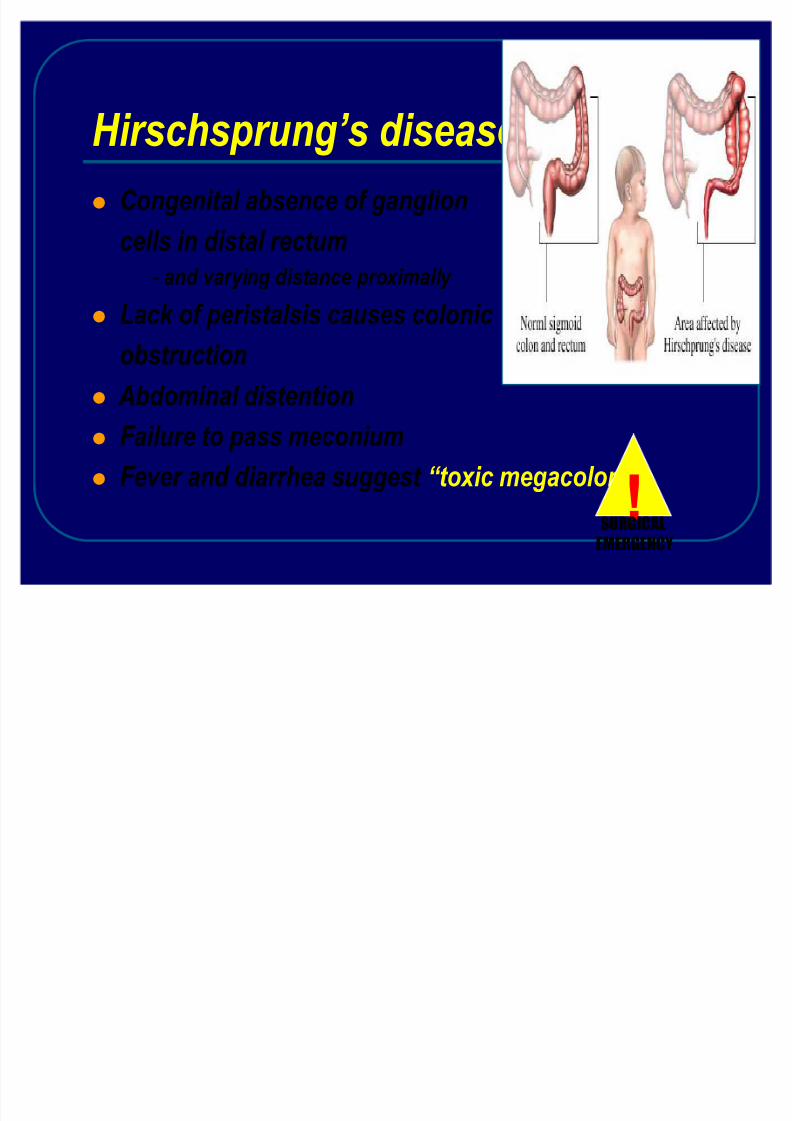
Hirschsprung¶s diseaseCongenital absence of ganglioncells in distal rectum
- and varying distance proximally Lack of peristalsis causes colonic obstruction Abdominal distentionFailure to pass meconiumFever and diarrhea suggest ³toxic megacolon´ !
SURGICALEMERGENCY
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 36/56
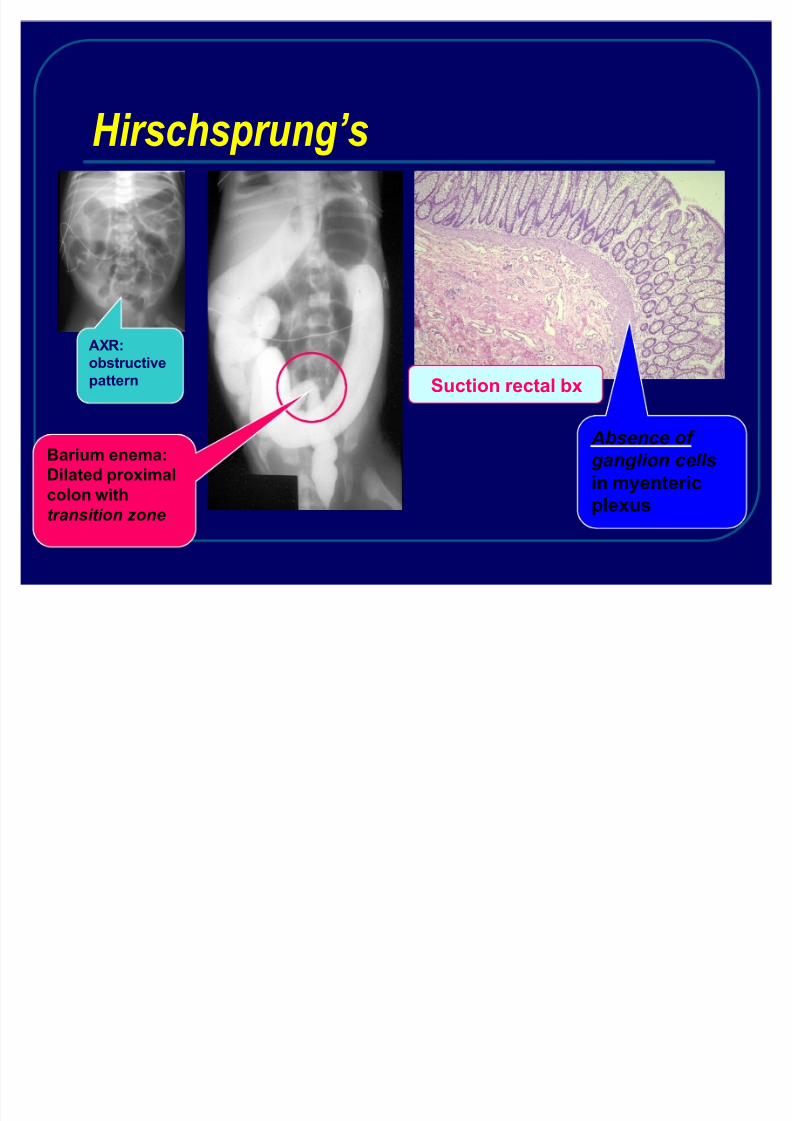
Hirschsprung¶s
AX R:obstructivepattern
B arium enema:Dilated proximalcolon witht ransi t i o n z o ne
S uction rectal bx
A b sence of g an gl i o n ce ll sin myentericplexus
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 37/56
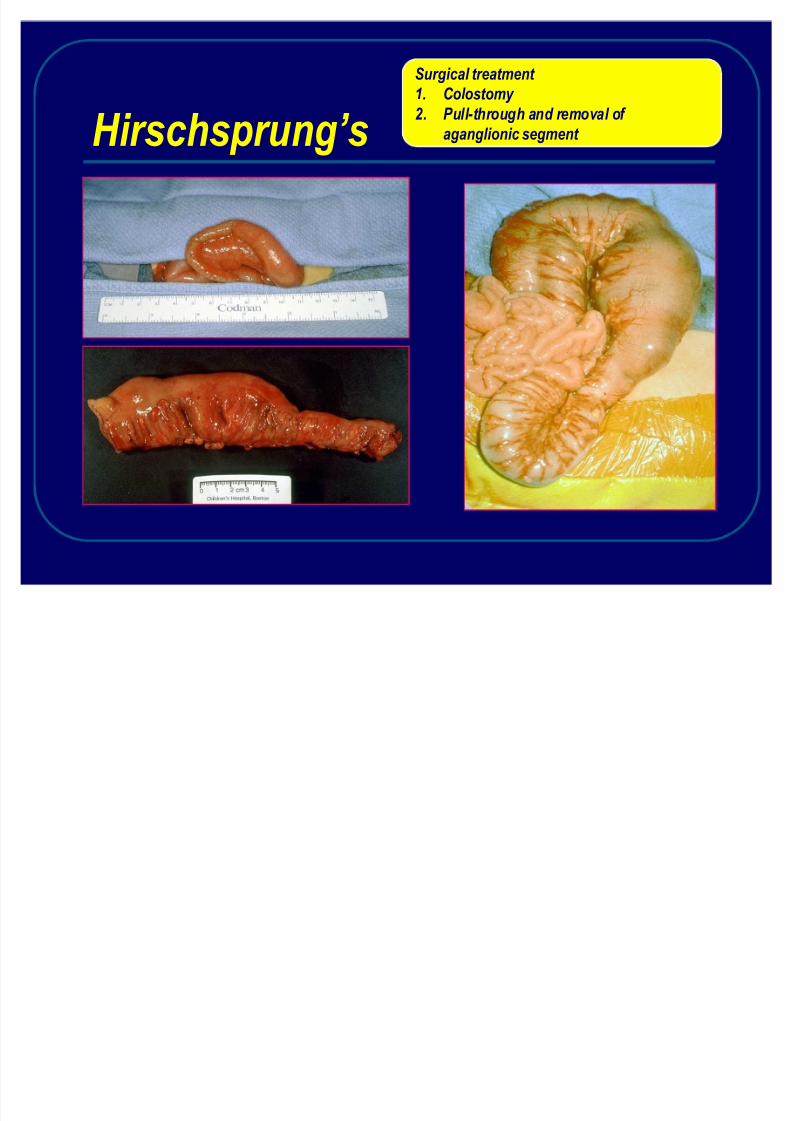
Hirschsprung¶s
Surgical treatment 1. Colostomy 2. Pull-through and removal of
aganglionic segment

8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 38/56
T ransanal pull-through
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 39/56
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 40/56
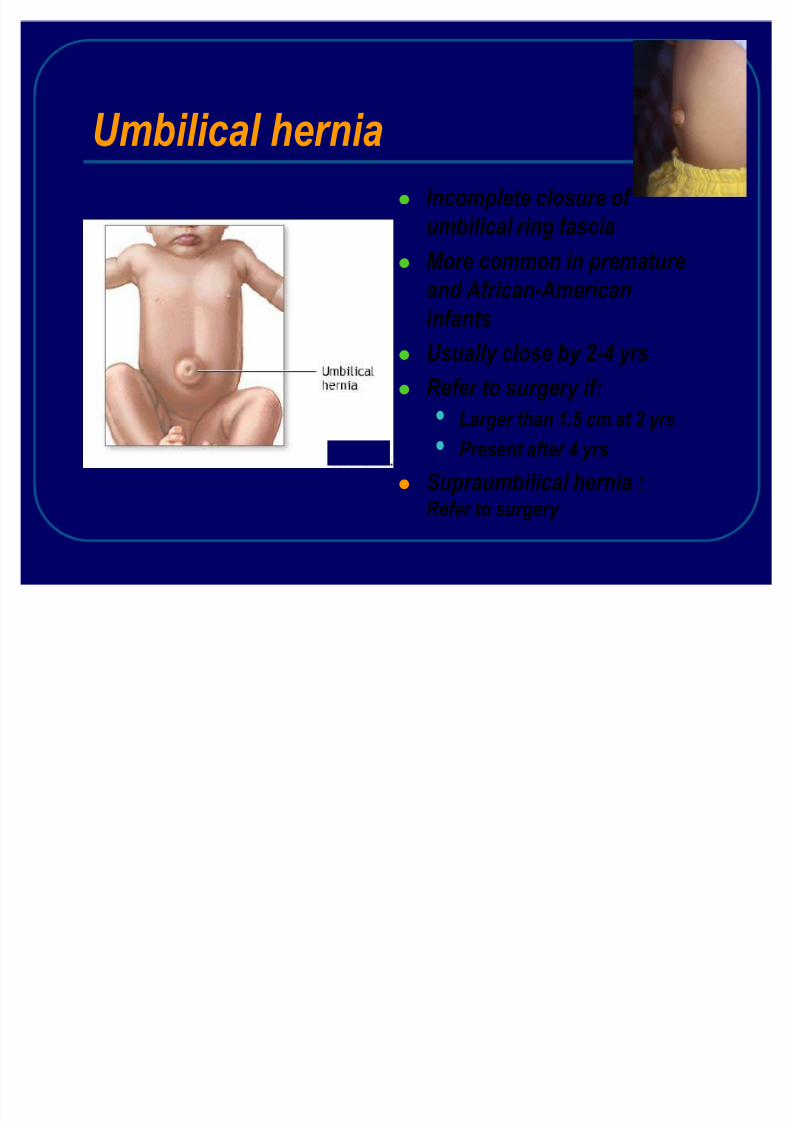
Umbilical herniaIncomplete closure of umbilical ring fasciaMore common in prematureand African-AmericaninfantsUsually close by 2-4 yrsRefer to surgery if:
Larger than 1.5 cm at 2 yrsPresent after 4 yrs
Supraumbilical hernia :Refer to surgery
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 41/56
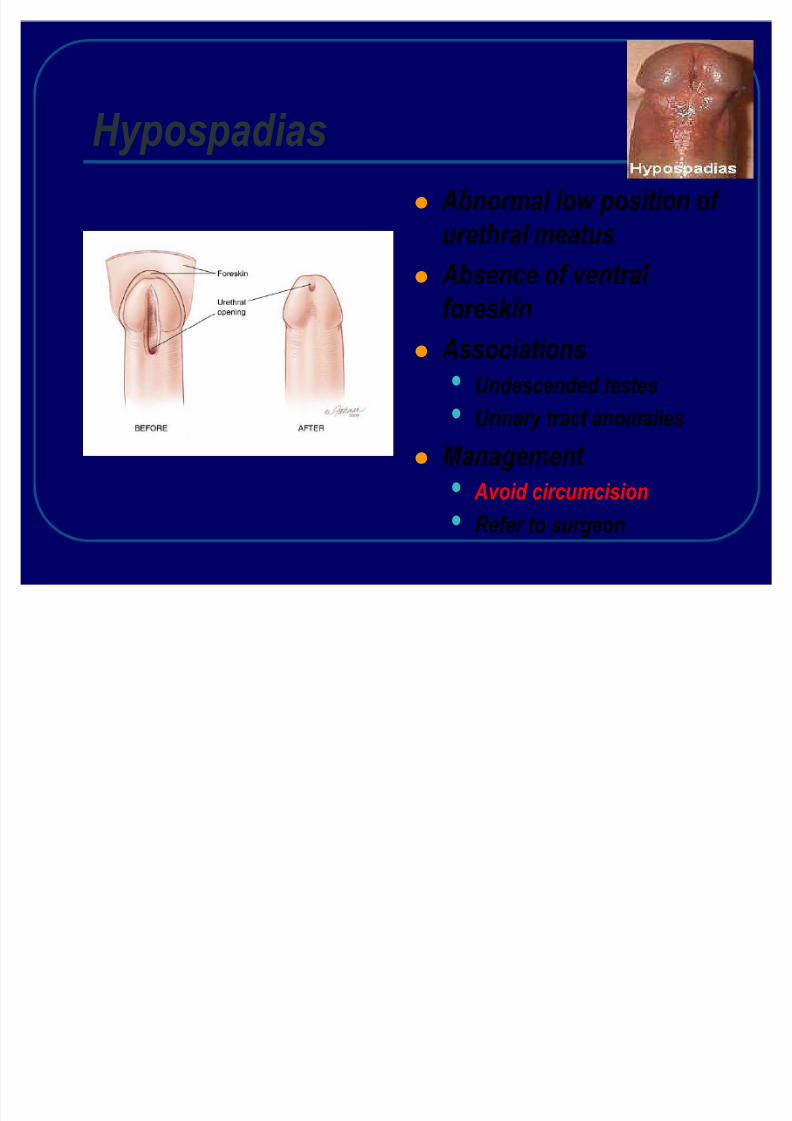
Hypospadias Abnormal low position of urethral meatus
Absence of ventral foreskin Associations
Undescended testes
Urinary tract anomaliesManagement
Avoid circumcisionRefer to surgeon
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 42/56
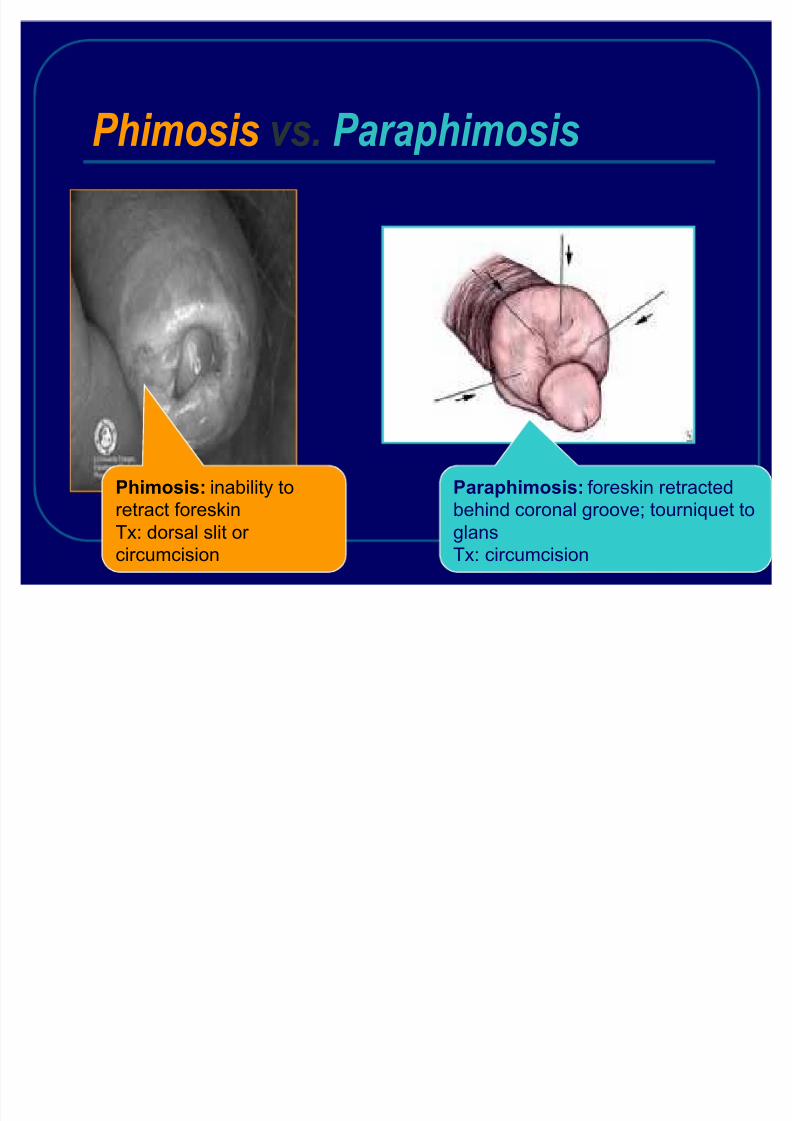
Phimosis vs. Paraphimosis
P himosis: inability toretract foreskinTx: dorsal slit or
circumcision
P araphimosis: foreskin retractedbehind coronal groove; tourniquet toglans
Tx: circumcision
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 43/56
Scrotal swellingPAINLESS
Hydrocele
VaricoceleSpermatoceleInguinal hernia
PAINFULTesticular torsion
EpididymitisOrchitisIncarcerated hernia
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 44/56
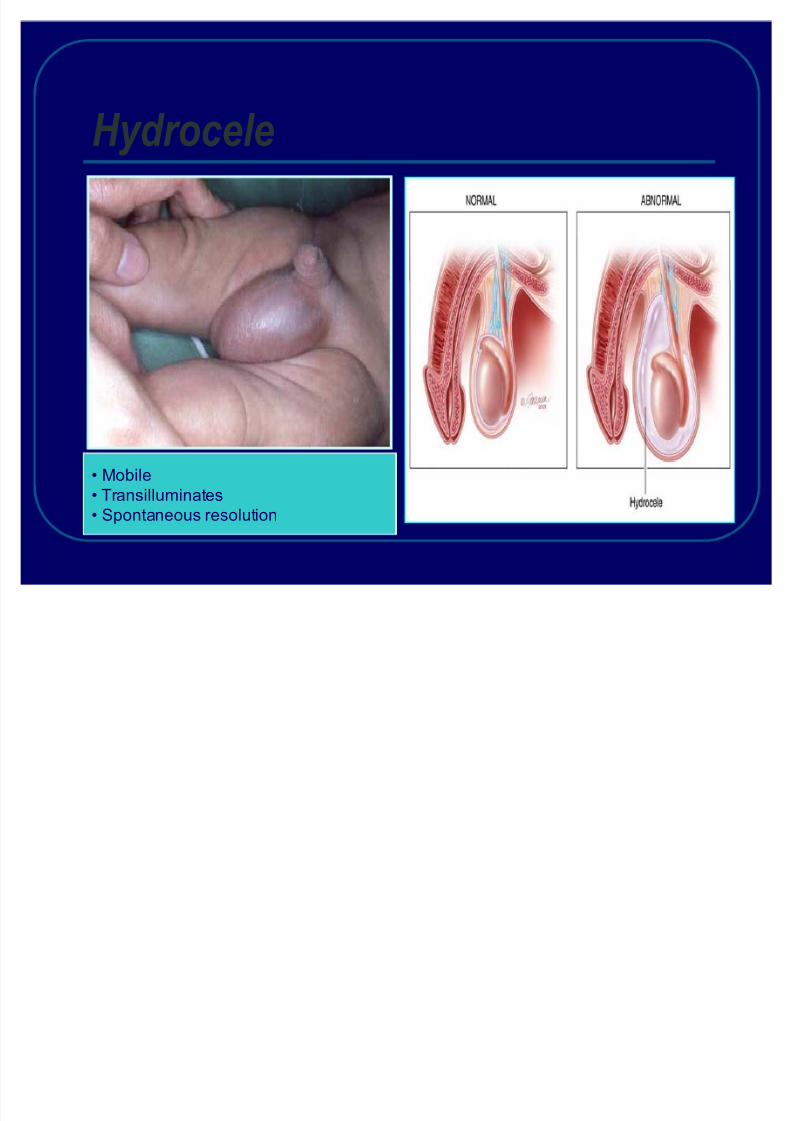
Hydrocele
M obileTransilluminatesSpontaneous resolution
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 45/56
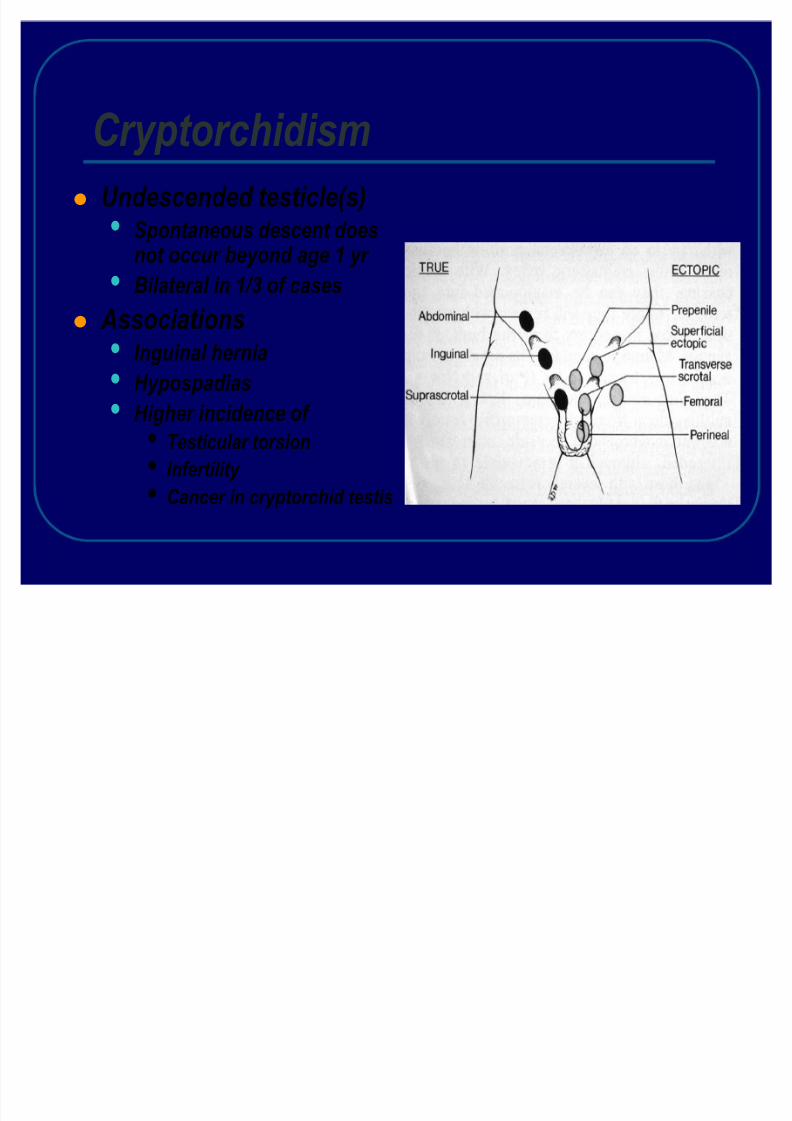
CryptorchidismUndescended testicle(s)
Spontaneous descent doesnot occur beyond age 1 yr
Bilateral in 1/3 of cases Associations
Inguinal herniaHypospadias
Higher incidence of Testicular torsionInfertility Cancer in cryptorchid testis
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 46/56
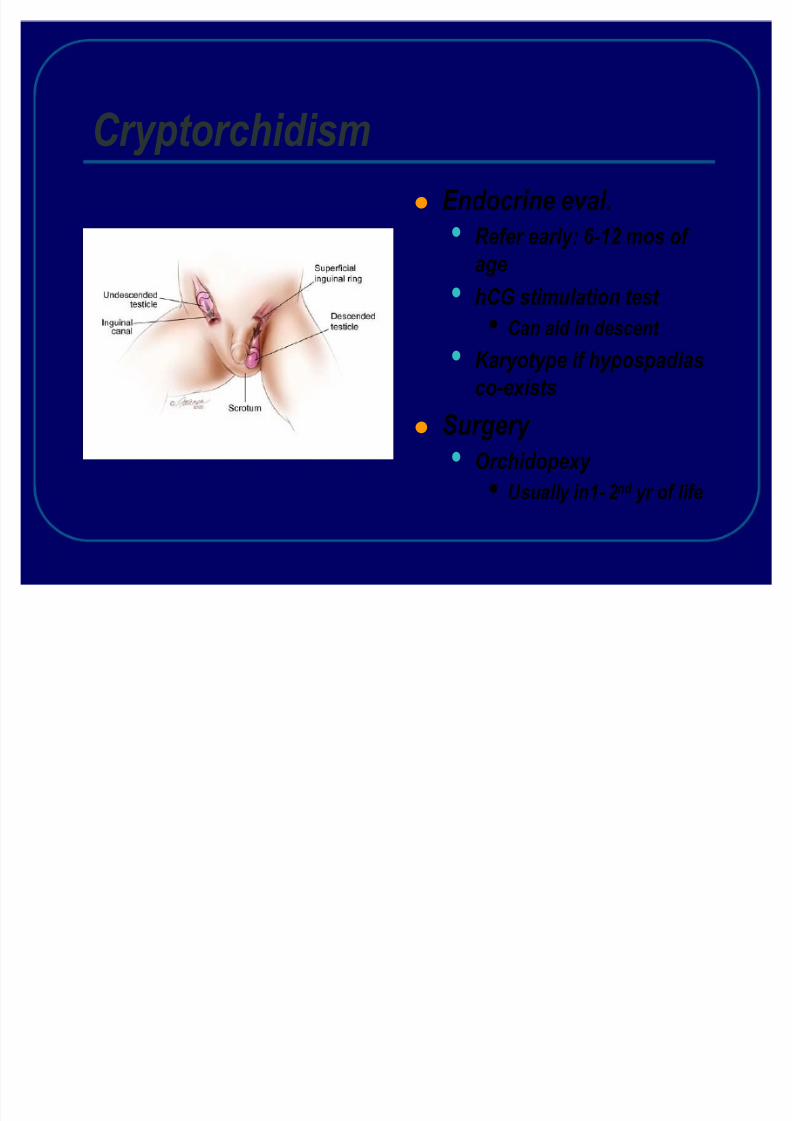
CryptorchidismEndocrine eval.
Refer early: 6-12 mos of agehCG stimulation test
Can aid in descent
Karyotype if hypospadiasco-exists
Surgery Orchidopexy
Usually in1- 2 nd yr of life
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 47/56
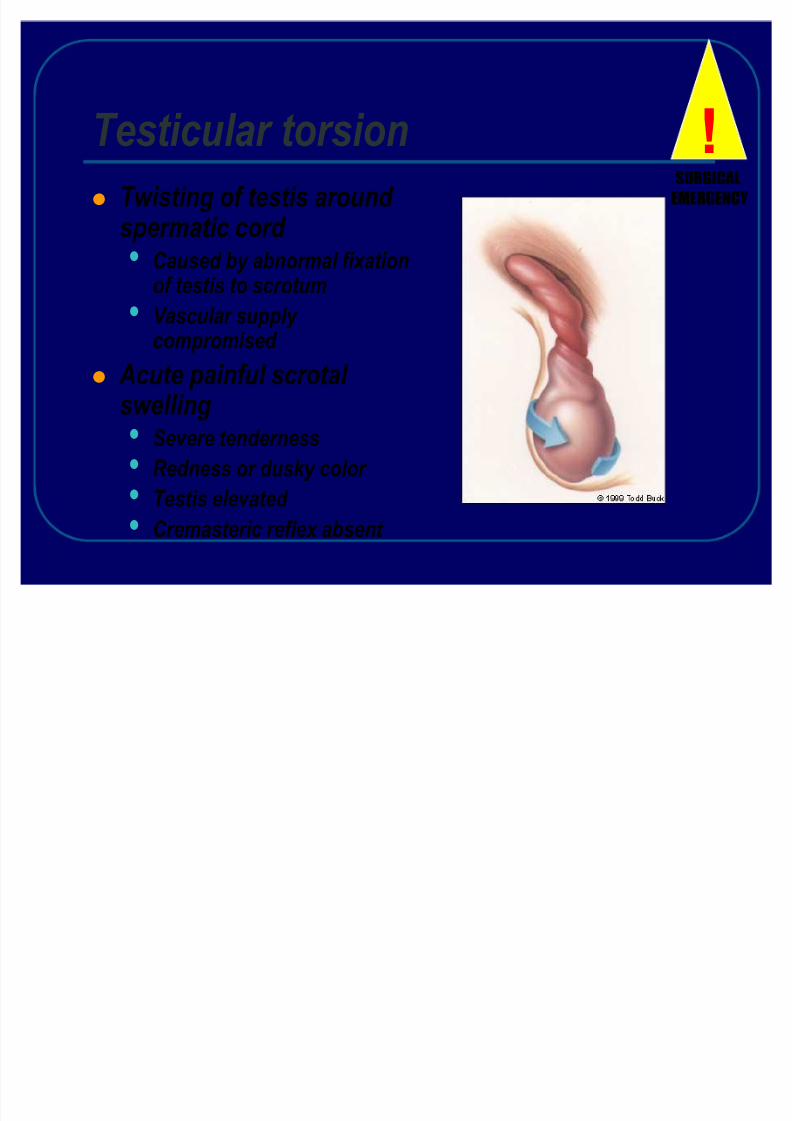
Testicular torsionTwisting of testis around spermatic cord
Caused by abnormal fixationof testis to scrotumVascular supply compromised
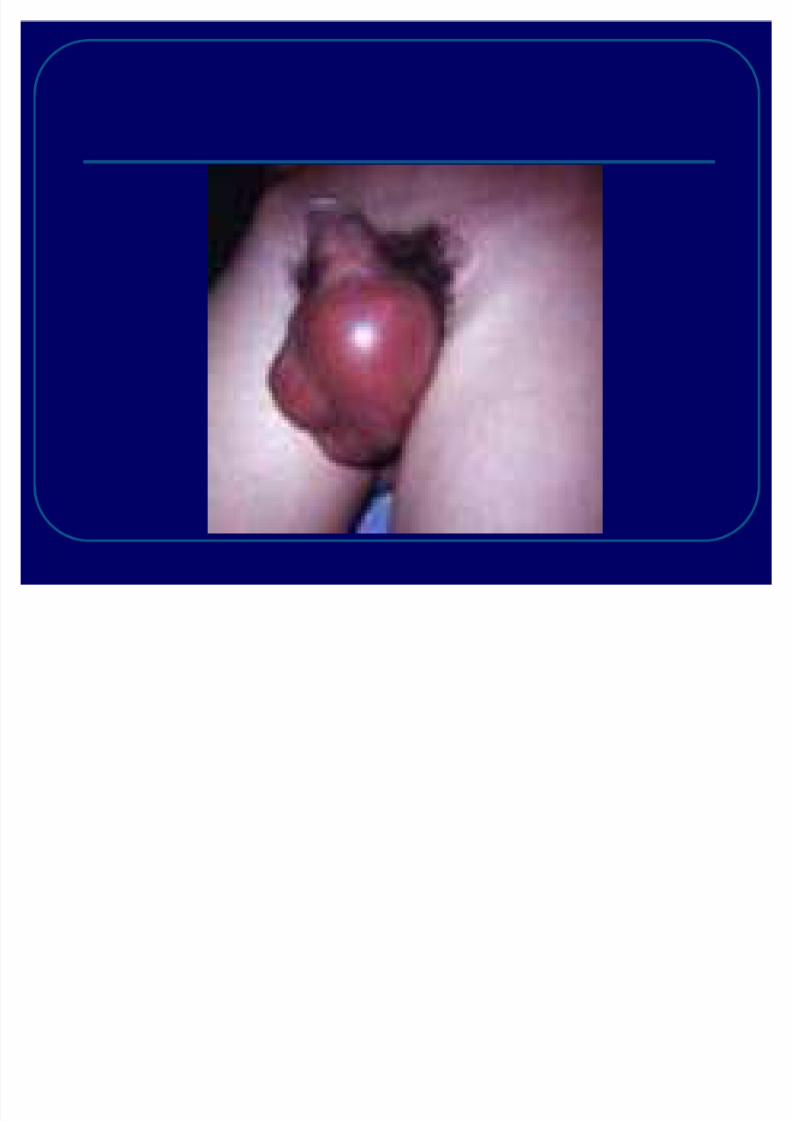
Acute painful scrotal swelling
Severe tendernessRedness or dusky color Testis elevated Cremasteric reflex absent
!SURGICALEMERGENCY
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 48/56
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 49/56
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 50/56
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 51/56
management
In the patient with acute surgical scrotalpain ,immediate surgical consultation is
essential .
Surgical exploration , detorsion and
fixation .
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 52/56
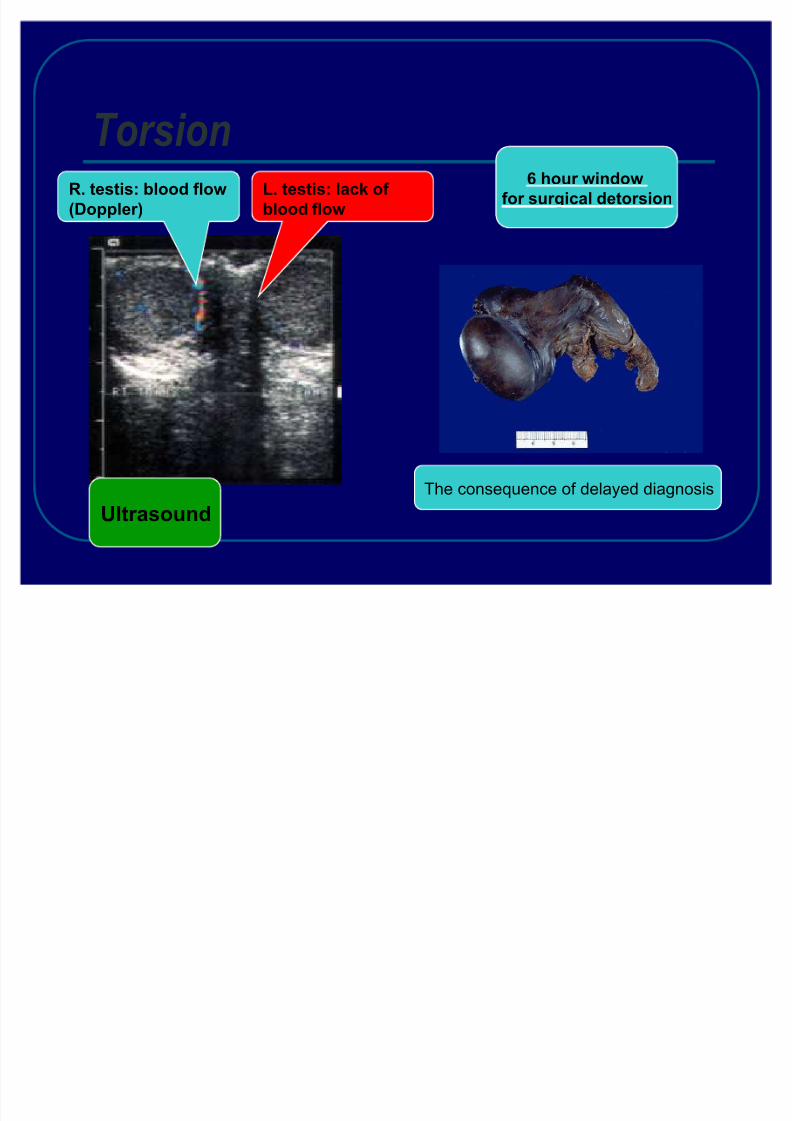
O utcome
Ischemic testicular damage related tothe number of turns of the spermatic
cord and the duration of torsion .A ll cases with a torsion > 3 60* and > 24h
duration will have testicular loss or severe
atrophy if the testis left in situ .
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 53/56
What to do?A lways undress the childfor examDon¶t forget
Intussusception inlethargic childrenU tilize imaging liberallywhen child looks sickand know your
radiologist¶s expertise
A ny type of blood instool may be due toIntussusception (not only
currant jelly)V omiting in infantsshould not be takenseriouslyBe conservative with
children w/
unclear dxBe sure that the parent(s) understand return precautions . If
they do not, then observe child
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 54/56
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 55/56
Q uestions or C omments
8/8/2019 Surgical Problems in Children
http://slidepdf.com/reader/full/surgical-problems-in-children 56/56
























![Gastrointestinal Surgical Disorder in Children [Autosaved]](https://img.pdfslide.net/doc/110x75/5695d0161a28ab9b0290e6b2/gastrointestinal-surgical-disorder-in-children-autosaved.jpg)