Embed Size (px)
Citation preview

Critical review
Page 1 of 6
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Dennis B, Gunter O. Surgical procedures in the intensive care unit: a critical review. OA Critical Care 2013 May 01;1(1):6.
Surgical procedures in the intensive care unit: a critical review
BM Dennis*, OL Gunter
AbstractIntroductionIncreasingly, surgical procedures are performed at bedside in the inten-sive care unit (ICU). Cost savings and gaining timely access to the oper-ating room (OR) have helped to spur this trend towards more ICU-based procedures. Patient physiology and the patient transport concerns have made performing bedside proce-dures a more attractive option than the OR in certain settings. DiscussionICUs have begun to adapt to accom-modate these bedside surgical proce-dures. Specialized personnel have been trained to facilitate and support procedures in some hospitals. Because the operating room remains the best location for most surgical procedures, there are only a few indi-cations to perform bedside surgical procedures. These indications include lesser procedures for which the OR costs and transport risks are not justified or emergent proce-dures in patients are too unstable for transport to the OR. The most common procedures performed in the ICU include percutaneous trache-ostomy, percutaneous endoscopic gastrostomy tube and inferior vena cava filter. Performing these proce-dures in the ICU is equally safe and more cost effective than performing them in the OR. Procedures of a more urgent nature can also be performed in the ICU and include laparotomy and damage control orthopaedics. Patient instability often dictates
the need for these procedures to be performed in the ICU.ConclusionThe operating room is no longer the only location that surgical proce-dures can be performed. The ICU is becoming a more common location where selected bedside procedures are being performed. Reasons to perform bedside procedures in the ICU rather than the operating room include cost savings, elimination of risks of transporting critically ill patients, and avoidance of OR avail-ability concerns. The operating room remains the preferred location for almost all surgical procedures, but the ICU offers an attractive alterna-tive for certain selected patients and procedures.
IntroductionBedside surgical procedures performed in the intensive care unit (ICU) have become more commonplace in recent years. Much of this is because of the acceptance by surgeons and inten-sivists that procedures once thought to be performed exclusively in the operating room (OR) may be safely and easily performed in the ICU. In many cases, it has been demon-strated that significant cost savings can be achieved by performing these procedures in the ICU without sacri-ficing patient safety1–5. Additionally, difficulties gaining timely access to the OR, either because of patient instability or OR availability, have made bedside procedures an attrac-tive alternative that often allows for more efficient care4,6. Most impor-tantly, there are inherent risks to transport critically ill patients and some studies have demonstrated that serious adverse events, including death, can occur in up to 30%–45% of intra-hospital transports involving
critically ill patients7–9. These risks can be mitigated by performing select procedures at bedside in the ICU.DiscussionThe authors have referenced some of their own studies in this review. These referenced studies have been conducted in accordance with the Declaration of Helsinki (1964) and the protocols of these studies have been approved by the relevant ethics committees related to the institution in which they were performed. All human subjects, in these referenced studies, gave informed consent to participate in these studies.ICU as an ORCare in the ICU mirrors that in the OR for a number of reasons. The monitoring and equipment capabili-ties in the ICU are nearly identical to the OR. Ventilators in most ICUs have mechanical ventilation capa-bilities beyond standard OR ventila-tors. While inhaled anaesthetics are not readily available, intravenous sedatives are routinely used and are easily accessible. Additionally, ICU personnel are analogous to OR staff. Critical care nurses, respiratory ther-apists and patient care assistants replace circulating nurses, anaesthe-tists and OR attendants. The scrub nurse, however, is a position without a natural counterpart in the ICU. Many hospitals have developed systems that bring the OR to the ICU. This typically involves an OR staff, which brings the necessary equipment and supplies from the OR to the ICU. This can be an arduous and difficult task, especially in time-sensitive situa-tions or at inconvenient times, such as nights or weekends. At our institu-tion, we employ the use of specialised procedure support nurses (PSNs) in our trauma and surgical ICUs10. These nurses are specially trained to set up
* Corresponding authorEmail: [email protected] Division of Trauma and Surgical Critical Care, Vanderbilt University Medical Centre, Nashville, TN, USA
Optim
izin
g P
atient
Care

Critical review
Page 2 of 6
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Dennis B, Gunter O. Surgical procedures in the intensive care unit: a critical review. OA Critical Care 2013 May 01;1(1):6.
and perform essential roles during the various bedside procedures.
We have come to view the PSN role as the lynchpin of bedside surgical procedures. The PSNs are involved in many aspects of the periproce-dural care of the patient. The PSN can confirm that appropriate informed consent has been obtained by the physicians and lead the pre-surgical timeout. Similar to an OR scrub nurse, the PSN ensures that all the
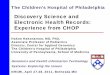
appropriate instruments are avail-able and sterilised, and they play integral roles during the various procedures. For example, during bedside percutaneous tracheostomy, our PSN is expected to manage the endotracheal tube during the proce-dure (Figure 1). We have intentionally limited the number of PSNs to mini-mise the variability and maximise the safety of the procedures. Their small number and consistent presence for
procedures mean they have extensive experience in the narrow spectrum of procedures performed at bedside in our hospital. In this regard, they are invaluable in setting up and executing bedside procedures in an efficient and consistent manner, especially important in emergent, time-sensi-tive situations. Furthermore, this experience translates into being a de facto bedside procedure expert, who plays an important role in teaching the techniques of bedside surgery to many residents and fellows.
It is important to note that there are certain limitations to procedures that can be performed in the ICU, and some procedures clearly belong to the OR. Contraindications to bedside surgery include risk of major bleeding, insertion of prosthetics and long, complex procedures. As a general rule, bedside procedures should be reserved for two situations as follows: lesser procedures for which transport to OR is not justified, because of difficulties of transport, OR expense or OR availability and lifesaving, emergency procedures for patients too unstable for transport11. Low complexity procedures that are ideal for the ICU setting, include placement of percutaneous trache-ostomy, percutaneous endoscopic gastrostomy (PEG) and inferior vena cava filters (IVCFs). More emergent procedures, such as exploratory laparotomy and damage control orthopaedics are also possible at the bedside. The aim of this critical review was to discuss surgical proce-dures in the ICU.
Percutaneous tracheostomyTracheostomy is the gold standard for patients requiring long-term mechan-ical ventilation or upper airway obstruction. The percutaneous dila-tional techniques first described by Ciaglia and the subsequent modifica-tion (Figure 2) employing the Ciaglia Blue Rhino® kit (Cook Medical’s Critical Care division, Bloomington, IN) have made the percutaneous technique arguably the procedure
Figure 1: Surgical critical care team starting bedside percutaneous tracheos-tomy. Procedure support nurse is pictured in middle at the head of bed in order to manage endotracheal tube.

Critical review
Page 3 of 6
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Dennis B, Gunter O. Surgical procedures in the intensive care unit: a critical review. OA Critical Care 2013 May 01;1(1):6.
of choice for tracheostomy place-ment12,13. Bedside percutaneous tracheostomy (Figure 3) has been shown repeatedly to be a safe alter-
native to open surgical tracheos-tomy in the OR2,5,10. Meta-analysis by Higgins showed percutaneous trache-ostomy to have lower wound infec-
tion rates, less scarring and shorter case lengths when compared to open tracheostomy5. Bedside percutaneous tracheostomy has been shown to be substantially more cost-effective than open tracheostomy performed in the OR. Studies have shown savings between $1100 and $3400 per proce-dure1,14,15. The Johns Hopkins Percuta-neous Tracheostomy Program Group showed that a hospital-subsidised multidisciplinary team performing bedside percutaneous tracheosto-mies can decrease complications and length of stay in ICU resulting in a net increase in hospital revenue4,6. The safety of bedside percutaneous trache-ostomy even in high-risk groups, such as the obese, was recently demon-strated in two large retrospective studies. Complication rates in high-risk patients in these studies were 1.0% and 1.7%, respectively10,16.
Percutaneous endoscopic gastrostomySince its first description, PEG is a procedure, which was an obvious choice to be performed outside the OR17. The combined endoscopic and percutaneous techniques have low risk and are relatively easy to perform at the bedside (Figure 4). Even in the initial cases, Ponsky and colleagues used only local and topical analgesia18. Other techniques and devices exist for percutaneous feeding access, but the PEG remains the gold standard. Indications for PEG are related to the requirement for long-term feeding access and include severe neurological injuries, prolonged mechanical ventilation, inability to swallow (e.g., head and neck cancer, trauma, etc.), high risk of aspiration, severe facial trauma and severe malnutrition in debilitated or demented patients19. Although few, but some potential contraindications to PEG are haemodynamic insta-bility, recent oesophageal or gastric surgery, coagulopathy, inability to oppose the gastric wall to anterior abdominal wall, inability to pass a flexible endoscope and gastric outlet obstruction. Relative contraindica-
Figure 2: Dilation of tracheotomy using Ciaglia Blue Rhino® during bedside percutaneous tracheostomy.
Figure 3: Standard equipment set up for bedside modified percutaneous tracheostomy using Ciaglia Blue Rhino® kit.

Critical review
Page 4 of 6
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Dennis B, Gunter O. Surgical procedures in the intensive care unit: a critical review. OA Critical Care 2013 May 01;1(1):6.
tions include gastric varices, diffuse gastric cancer and limited remaining life expectancy19. Bankhead and colleagues compared gastrostomy
techniques and concluded that PEG was the preferred technique over laparoscopic or open gastrostomies. Procedure duration of PEG was
shorter, tube feedings were able to be started sooner and complications were fewer in the PEG group20. More recently, a meta-analysis performed by Gomes found that patients with PEGs had lower rates of subsequent intervention failure (e.g., clogged tube, interruption of feedings, etc.) compared to patients with nasogas-tric tubes with no difference in other complications including mortality21.
Inferior vena cava fi lterCritically ill patients are inherently at high risk of deep venous thrombosis (DVT), by virtue of exhibiting charac-teristics of Virchow’s triad, including venous stasis, hypercoagulability and endothelial damage. Frequent, diag-noses or injuries preclude certain patients from receiving appropriate pharmacologic DVT prophylaxis or treatment. To prevent venous throm-boembolism (VTE) in this high-risk group, IVCFs are a reasonable option. Initially, these procedures were exclusively performed in the OR. With modernisation of filter design and delivery systems, the IVCF proce-dure evolved into a percutaneous technique that could be performed in angiography suites. Since that time, it has migrated into the ICU as well. The key to the IVCF procedure is to ensure deployment of the filter in the proper infra-renal location of the vena cava. This is made possible by image-guided placement in the form of ultrasonography (transabdominal or intravascular) or C-arm fluoroscopy with iodinated contrast or carbon-dioxide, either of which can be performed at bedside3,22–24. Complica-tion rates are exceedingly low in IVCF and are comparable to those proce-dures performed in the OR and angi-ography suites23,24. Cost savings by performing the IVCF procedure in the ICU are tremendous. Multiple studies have demonstrated significant cost savings by placing IVCF in the ICU rather than in angiography suites or the OR3,23. Nunn and colleagues reported that annual savings for IVCF placed at bedside compared to angi-
Figure 4: Bedside percutaneous endoscopic gastrostomy tube placement.
Figure 5: Bedside laparotomy with abdominal washout. Procedure support nurse (right) acts as scrub nurse. Critical care nurse (left) administers sedation and monitors vital signs.

Critical review
Page 5 of 6
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Dennis B, Gunter O. Surgical procedures in the intensive care unit: a critical review. OA Critical Care 2013 May 01;1(1):6.
ography suite and OR were nearly $69,800 and $118,300, respec-tively3. Neither of these cost analyses accounts for the hidden costs of the time and personnel, required to transport critically ill patients, nor do they include the costs of the poten-tial risks incurred in transport of this high-risk population.
LaparotomyBedside laparotomy can be neces-sary in cases of abdominal compart-ment syndrome, severe abdominal trauma and specific emergency general surgical conditions. Abdom-inal compartment syndrome is often the result of aggressive fluid resuscitation after trauma or sepsis. The resultant bowel and intersti-tial oedema may lead to pulmonary compromise, diminished venous return and decreased cardiac output. The result is severe hypoventila-tion and combined cardiogenic and hypovolemic shocks. The profound haemodynamic and respiratory insta-bility that can develop secondary to abdominal compartment syndrome
obviates safe transport of the patients to the OR and necessitates immediate surgical intervention in the form of decompressive laparotomy.
Damage control operations with temporary abdominal closure have been well established in patients with severe torso injuries in the setting of the so-called lethal triad of hypo-tension, acidosis and coagulopathy. The initial operation is performed in the OR and is primarily focused on controlling haemorrhage and gaining source control of sepsis. A temporary abdominal closure system is typi-cally applied, and the patient may be transferred to the ICU for ongoing resuscitation and stabilisation25. The decision regarding when and where to re-operate is dependent on factors, such as operative complexity and patient physiology. Simple procedures, such as removal of intra-abdominal packing and fascial closure may be performed at the bedside in the ICU (Figure 5), particularly for patients with significant respiratory compro-mise requiring high levels of ventilator
support. More complex procedures, such as restoration of bowel conti-nuity may also be performed in the ICU provided the appropriate equip-ment is available (Figure 6), and can be considered on a case-by-case basis. Care must be exercised to maintain patient safety principles as would be expected in the OR setting.
While there are many diagnoses that may benefit from bedside lapa-rotomy, there are few, if any, defi-nite indications. Diaz reported the use of a protocol for bedside lapa-rotomy. As defined by the protocol, the four primary clinical indications for bedside laparotomy in patients felt to be unsuitable for transport to the OR were as follows: abdom-inal compartment syndrome, acute haemodynamic instability caused by intra-abdominal haemorrhage, washout or closure of a previous open abdomen and intra-abdominal sepsis26. Damage control laparoto-mies had previously been shown to carry higher rates of complications than the more traditional explora-tory laparotomy, particularly intra-abdominal abscess and fistula27. However, after employing the bedside laparotomy protocol, Diaz demon-strated intra-abdominal abscess and fistula rates that were equivalent to studies involving damage control laparotomies performed in the OR26. Additionally, as with the previ-ously discussed procedures, signifi-cant cost savings can be realised by avoiding transport to the OR with bedside laparotomy being shown to save as much as $5300 per case27.
Damage control orthopaedic proceduresJust as the bedside laparotomy is a damage control procedure for general surgeons, orthopaedic surgeons are occasionally required to perform operative procedures at bedside. While there are sparse reports in the published literature of bedside ortho-paedic procedures, they are frequently practiced at our institution in select circumstances. Indications for bedside
Figure 6: Instruments used at our institution for beside laparotomy, including removal of packing and fascial closure. Additional instruments may be required for more complex procedures, such as bowel anastomoses or ostomy creation.

Critical review
Page 6 of 6
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Dennis B, Gunter O. Surgical procedures in the intensive care unit: a critical review. OA Critical Care 2013 May 01;1(1):6.
orthopaedic procedures reflect those for bedside laparotomy with one addi-tional indication. Reasons for bedside orthopaedic procedures include the following: compartment syndrome, haemorrhage control, debridement and irrigation of wounds and tempo-rary fracture stabilisation in patients too unstable for transport to the OR. Ebraheim et al. recently reported the first series of bedside fasciotomies for compartment syndrome. Their study investigated 34 patients, who were treated with fasciotomies at the bedside using sedation and local anaesthetic. The authors observed an infection rate of 9%, similar to the published rates for fasciotomies performed in the OR and no deep infections, osteomyelitis, amputa-tions or death were observed28. Haemorrhage control of an open or badly mangled extremity in unstable patients, with multiple injuries, is sometimes necessary, particularly in patients with moderate-to-severe traumatic brain injuries. Fluid and blood product resuscitation may at times be insufficient to keep up with the ongoing losses from a severely injured extremity. In these rare instances, bedside exploration and washout are required to prevent secondary brain injury from hypo-tension due to haemorrhagic shock. Traditional orthopaedic surgical prin-ciples would hold that formal irriga-tion and debridement should occur within six to eight hours. For patients with extended periods of instability preventing safe transport to the OR, irrigation and debridement can be performed at the bedside with rela-tive ease.
Fracture stabilisation may be also performed at the bedside in a closed technique or with skeletal traction pins. However, stabilisation with external fixation is possible in the ICU as well, and our own orthopaedic colleagues will employ this in select cases. As with previous indications, these patients usually have multiple injuries and require significant critical care supportive measures. A typical scenario would include a patient, with
multiple long bone fractures that are believed to contribute to a continued systemic inflammatory response.
ConclusionIt is important to remember that OR is still the preferred venue to perform the vast majority of surgical proce-dures. However, the OR is no longer the only location, in which operative procedures can be safely and effec-tively performed. Because of either necessity or convenience, the ICU has become an accessory theatre, in which surgical procedures are now routinely performed. In fact, there are some advantages to perform procedures in the ICU. Eliminating risks associated with transporting critically ill patients, avoiding OR availability issues and cost savings, are all advantages to perform select procedures in the ICU. Properly training the ICU personnel, including a specially trained PSN or mobile OR personnel, is essential for the safety and success of the ICU procedures. Additionally, appropriate patient and procedure selection for the ICU setting are paramount to minimise the risk of adverse outcomes.
Abbreviations listDVT, deep venous thrombosis; ICU, intensive care unit; IVCF, inferior vena cava filter; OR, operating room; PSN, procedure support nurse.
References 1. Van Natta TL, Morris JA Jr, Eddy VA, Nunn CR, Rutherford EJ, Neuzil D, et al. Elective bedside surgery in critically injured patients is safe and cost-effective. Ann Surg. 1998 May;227(5):618–24. 2. Freeman BD, Isabella K, Cobb JP, Boyle WA 3rd, Schmieg RE Jr, Kolleff MH, et al. A prospective, randomized study comparing percutaneous with surgical tracheostomy in critically ill patients. Crit Care Med. 2001 May;29(5):926–30. 3. Nunn CR, Neuzil D, Naslund T, Bass JG, Jenkins JM, Pierce R, et al. Cost-effective method for bedside insertion of vena caval filters in trauma patients. J Trauma. 1997 Nov;43(5):752–8. 4. Mirski MA, Pandian V, Bhatti N, Haut E, Feller-Kopman D, Morad A, et al. Safety,
efficiency, and cost-effectiveness of a multidisciplinary percutaneous trache-ostomy program. Crit Care Med. 2012 Jun;40(6):1827–34. 5. Higgins KM, Punthakee X. Meta-anal-ysis comparison of open versus percuta-neous tracheostomy. Laryngoscope. 2007 Mar;117(3):447–54. 6. Pandian V, Miller CR, Mirski MA, Schiavi AJ, Morad AH, Vaswani RS, et al. Multidisciplinary team approach in the management of tracheostomy patients. Otolaryngol Head Neck Surg. 2012 Oct;147(4):684–91. 7. Beckmann U, Gillies DM, Berenholtz SM, Wu AW, Pronovost P. Incidents relating to the intra-hospital transfer of critically ill patients. An analysis of the reports submitted to the Australian Incident Monitoring Study in Intensive Care. Inten-sive Care Med. 2004 Aug;30(8):1579–85. 8. Winter MW. Intrahospital transfer of critically ill patients; a prospective audit within Flinders Medical Centre. Anaesth Intensive Care. 2010 May;38(3):545–9. 9. Parmentier-Decrucq E, Poissy J, Favory R, Nseir S, Onimus T, Guerry MJ, et al. Adverse events during intrahospital transport of critically ill patients: inci-dence and risk factors. Ann Intensive Care. 2013 Apr;3(1):10. 10. Dennis BM, Eckert MJ, Gunter OL, Morris JA Jr, May AK. Safety of bedside percutaneous tracheostomy in the critically ill: evaluation of more than 3,000 procedures. J Am Coll Surg. 2013 Apr;216(4):858–65. 11. Mayberry JC. Bedside open abdominal surgery. Utility and wound management. Crit Care Clin. 2000 Jan;16(1):151–72. 12. Ciaglia P, Firsching R, Syniec C. Elective percutaneous dilatational tracheostomy. A new simple bedside procedure; prelim-inary report. Chest. 1985 Jun;87(6):715–9. 13. Byhahn C, Wilke HJ, Halbig S, Lischke V, Westphal K. Percutaneous tracheos-tomy: ciaglia blue rhino versus the basic ciaglia technique of percutaneous dila-tional tracheostomy. Anesth Analg. 2000 Oct;91(4):882–6. 14. Cobean R, Beals M, Moss C, Breden-berg CE. Percutaneous dilatational trache-ostomy. A safe, cost-effective bedside procedure. Arch Surg. 1996 Mar;131(3):265–71. 15. Barba CA, Angood PB, Kauder DR, Latenser B, Martin K, McGonigal MD, et al. Bronchoscopic guidance makes percuta-neous tracheostomy a safe, cost-effective,

Critical review
Page 7 of 6
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Dennis B, Gunter O. Surgical procedures in the intensive care unit: a critical review. OA Critical Care 2013 May 01;1(1):6.
and easy-to-teach procedure. Surgery. 1995 Nov;118(5):879–83. 16. Kornblith LZ, Burlew CC, Moore EE, Haenel JB, Kashuk JL, Biffl WL, et al. One thousand bedside percutaneous trache-ostomies in the surgical intensive care unit: time to change the gold standard. J Am Coll Surg. 2011 Feb;212(2):163–70. 17. Gauderer MW, Ponsky JL, Izant R Jr. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg. 1980 Dec;15(6):872–5. 18. Ponsky JL, Gauderer MW. Percu-taneous endoscopic gastrostomy: a nonoperative technique for feeding gastrostomy. Gastrointest Endosc. 1981 Feb;27(1):9–11. 19. Sabiston DC, Townsend CM. Sabiston textbook of surgery: the biological basis of modern surgical practice. Philadelphia, PA: Elsevier Saunders; 2012. 20. Bankhead RR, Fisher CA, Rolan-delli RH. Gastrostomy tube placement
outcomes: comparison of surgical, endo-scopic, and laparoscopic methods. Nutr Clin Pract. 2005 Dec;20(6):607–12. 21. Gomes CA Jr, Lustosa SA, Matos D, Andriolo RB, Waisberg DR, Waisberg J. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst Rev. 2012 Mar;3:CD008096. 22. Rosenthal D, Wellons ED, Lai KM, Bikk A, Henderson VJ. Retrievable inferior vena cava filters: initial clinical results. Ann Vasc Surg. 2006 Jan;20(1):157–65. 23. Paton BL, Jacobs DG, Heniford BT, Kercher KW, Zerey M, Sing RF. Nine-year experience with insertion of vena cava filters in the intensive care unit. Am J Surg. 2006 Dec;192(6):795–800. 24. Sing RF, Jacobs DG, Heniford BT. Bedside insertion of inferior vena cava filters in the intensive care unit. J Am Coll Surg. 2001 May;192(5):570–5.
25. Barker DE, Kaufman HJ, Smith LA, Ciraulo DL, Richart CL, Burns RP. Vacuum pack technique of temporary abdominal closure: a 7-year experi-ence with 112 patients. J Trauma. 2000 Feb;48(2):201–6. 26. Diaz JJ Jr, Mejia V, Subhawong AP, Subhawong T, Miller RS, O’Neill PJ, et al. Protocol for bedside laparotomy in trauma and emergency general surgery: a low return to the operating room. Am Surg. 2005 Nov;71(11):986–91. 27. Diaz JJ Jr, Mauer A, May AK, Miller R, Guy JS, Morris JA Jr. Bedside laparotomy for trauma: are there risks? Surg Infect (Larchmt). 2004 Spring;5(1):15–20. 28. Ebraheim NA, Abdelgawad AA, Ebra-heim MA, Alla SR. Bedside fasciotomy under local anesthesia for acute compart-ment syndrome: a feasible and reliable procedure in selected cases. J Orthop Traumatol. 2012 Sep;13(3):153–7.