Embed Size (px)
Citation preview
8/10/2017
1
Surgical Reconstruction: Integrating Patient Preferences
Marta J. Van Beek, MD, MPHChief of Staff | University of Iowa
C William Hanke Professor of Dermatology Surgery
No relationships with industry
No financial conflicts
Patient Preferences• Why do they matter?
– Patient perspective differs from yours• Physical features that bother them• What they can tolerate pre and post surgery
– Patient satisfaction quality measure / payment
– Compliance• Wound Care• Outcome
8/10/2017
2
Topics for Today
• What we know – Pre / Intra / Post surgery
• Simplifying complicated repairs– Decreasing time and effort for patients
• Simplifying wound care– Giving patients skin in the game for their surgical outcome
What Do We Know?• Patients like:
– To eat before and after surgery– To have distractions such as music, friends & family– To be called after their surgery for a “check in”– Fewer visits—same day surgery / evaluation
• Patients don’t like:– Pain– 2 staged procedures
• Hafiji J, et al. Patient satisfaction with post‐operative telephone calls after Mohs micrographic surgery: a New Zealand and U.K. experience. Br J Dermatol. 2012 Sep;167(3)• Locke MC, et al. Assessing the Correlation Between Patient Anxiety and Satisfaction for Mohs Surgery. J Drugs Dermatol. 2015 Sep 1;14(9):1070‐2.• Fernandez, et al. Do surgeons understand what their patients want? A comparison of patients' expectations and surgeons' perceptions of these expectations as a basis for effective
communication. J of Am Col Surg. September 2011 Vol 213(3), supp s122
Same Day Surgical EvaluationsRetrospective Review of: 233 patients: • Different‐day eval patients • Same‐day eval patients
No significant difference in:• Rate of any surgical complications (p=0.84)• Delay of surgery (p=0.29)• Number of patients requiring an anxiolytic prior to
surgery (p=0.14)
• Ferguson, et al. Comparison of Same‐Day Pre‐operative Evaluation to Different‐Day Pre‐operative Evaluation for Mohs Micrographic Surgery: Outcomes & Complication Rates. ACMS 2014
8/10/2017
3
Pain with Anesthesia
• 30 gauge needle
• Buffered with bicarb
• Room temperature
• Subdermal injection—into fat
• Slow infiltration
• One needle piercing
Strazar AR et al. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013 Sep;132(3):675‐84
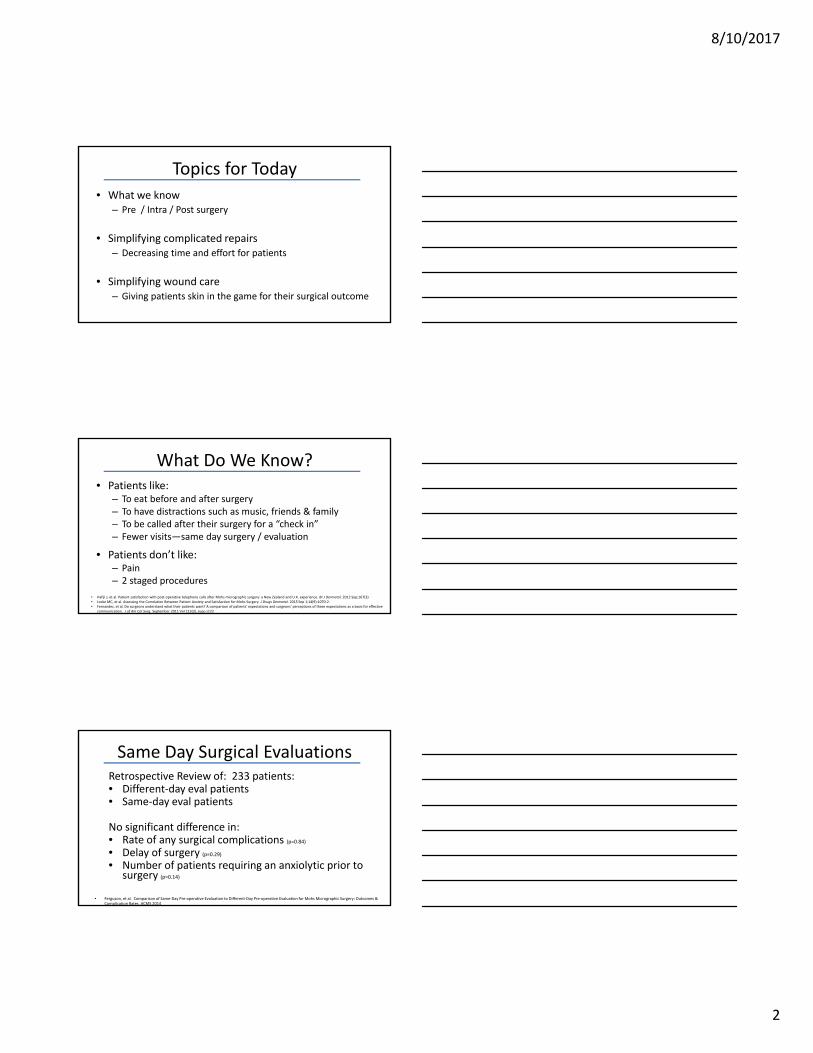
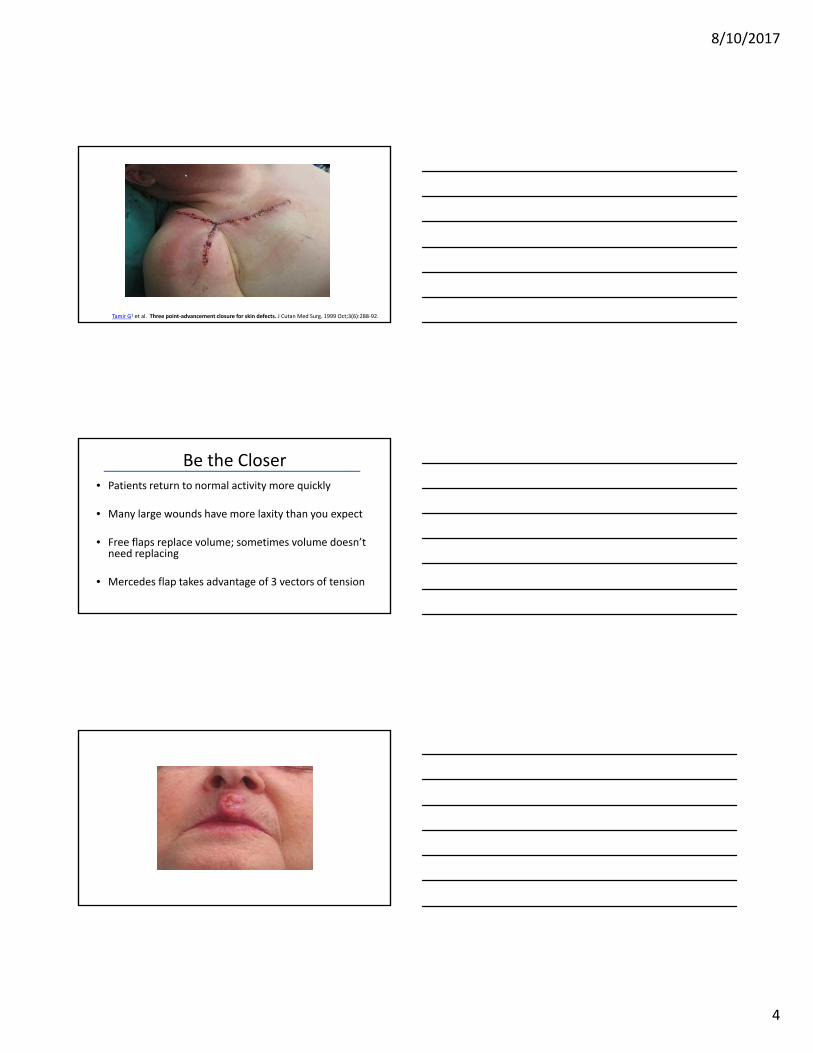
54 y.o. male with DFSP, ortho repair: plan for wound vac and free flap
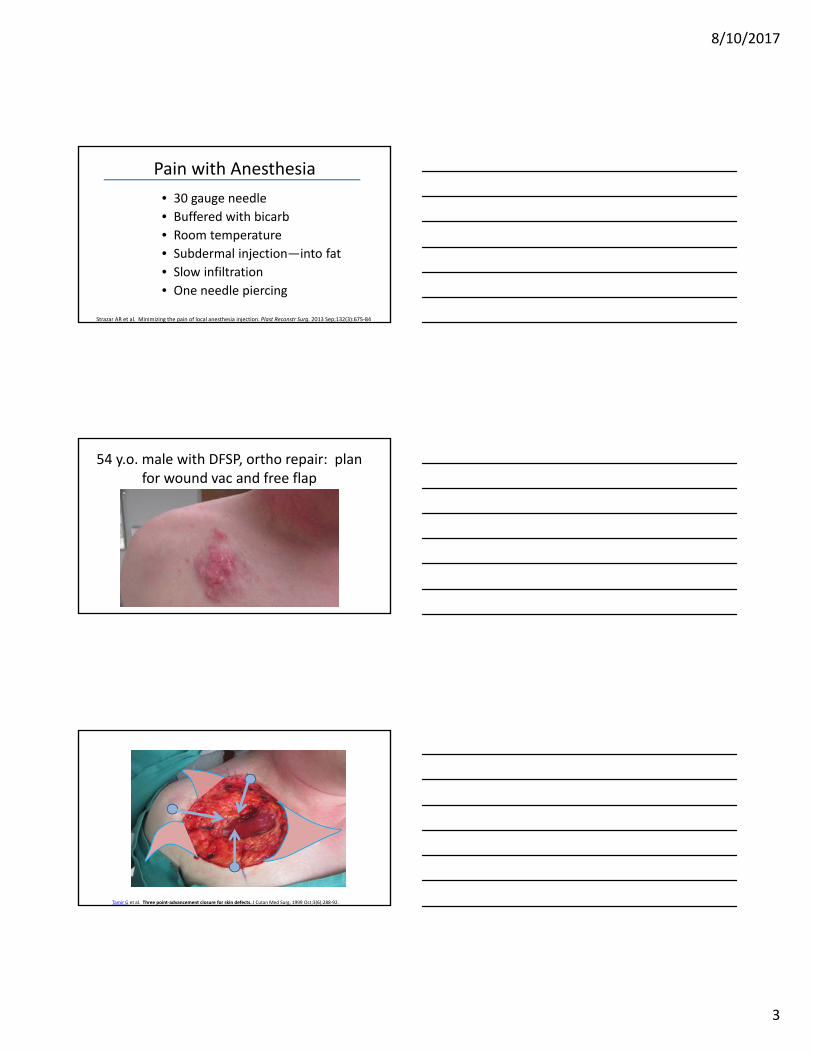
Tamir G et al. Three point‐advancement closure for skin defects. J Cutan Med Surg. 1999 Oct;3(6):288‐92.
8/10/2017
4
Tamir G1 et al. Three point‐advancement closure for skin defects. J Cutan Med Surg. 1999 Oct;3(6):288‐92.
Be the Closer• Patients return to normal activity more quickly
• Many large wounds have more laxity than you expect
• Free flaps replace volume; sometimes volume doesn’t need replacing
• Mercedes flap takes advantage of 3 vectors of tension
8/10/2017
5
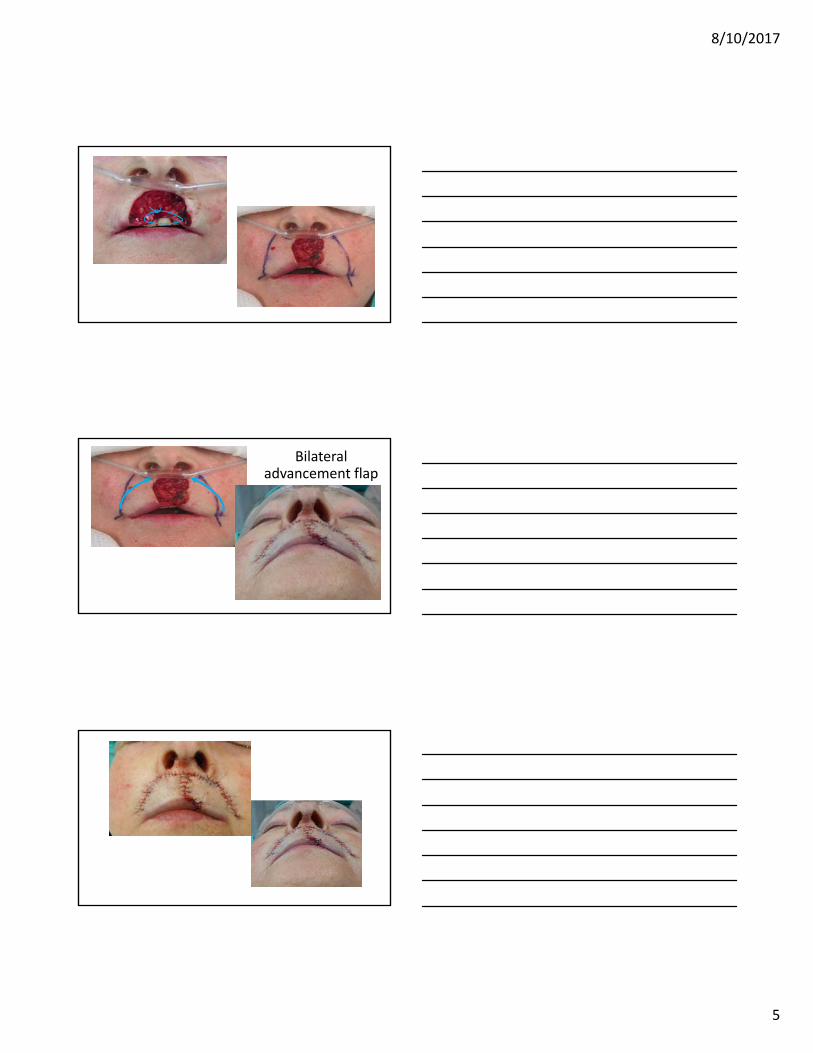
Bilateral advancement flap
8/10/2017
6
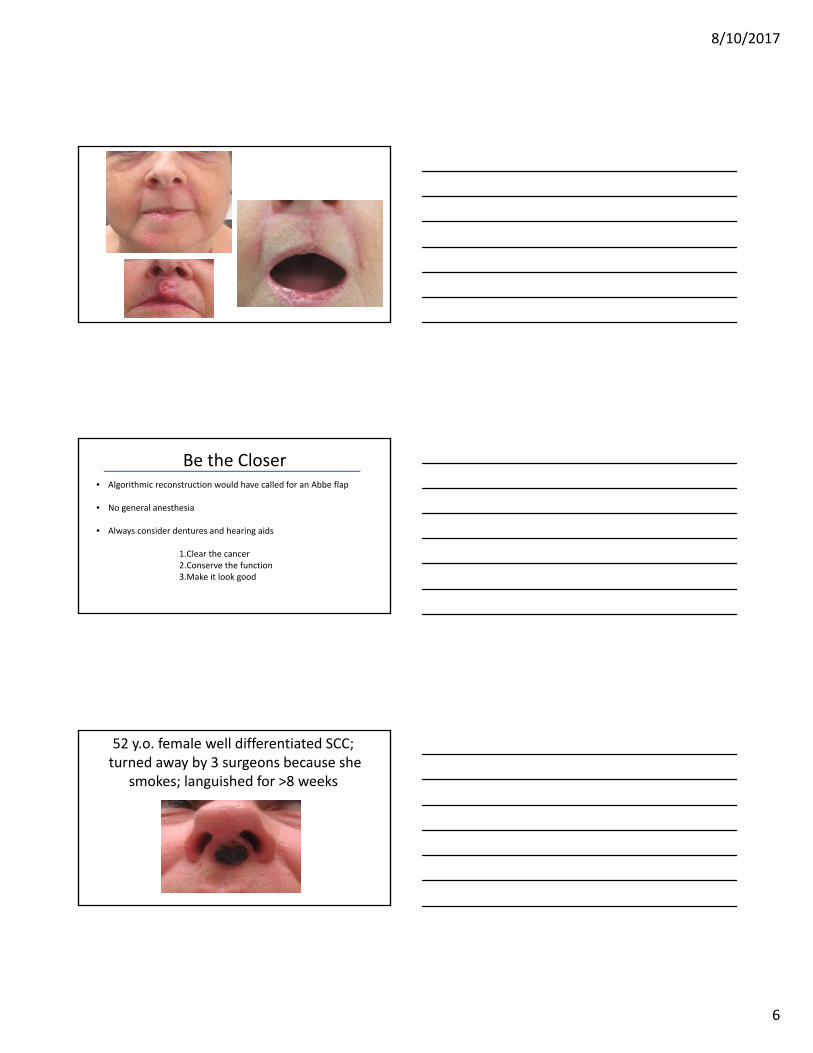
Be the Closer• Algorithmic reconstruction would have called for an Abbe flap
• No general anesthesia
• Always consider dentures and hearing aids
1.Clear the cancer2.Conserve the function3.Make it look good
52 y.o. female well differentiated SCC;turned away by 3 surgeons because she
smokes; languished for >8 weeks
8/10/2017
7
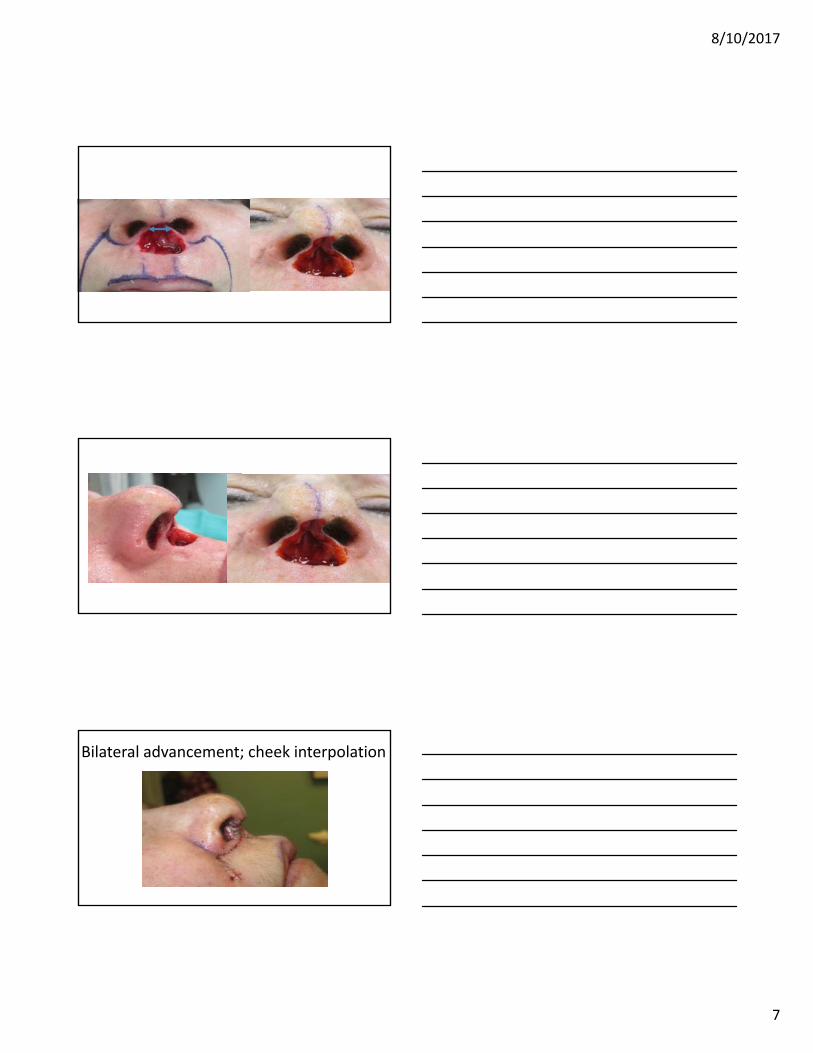
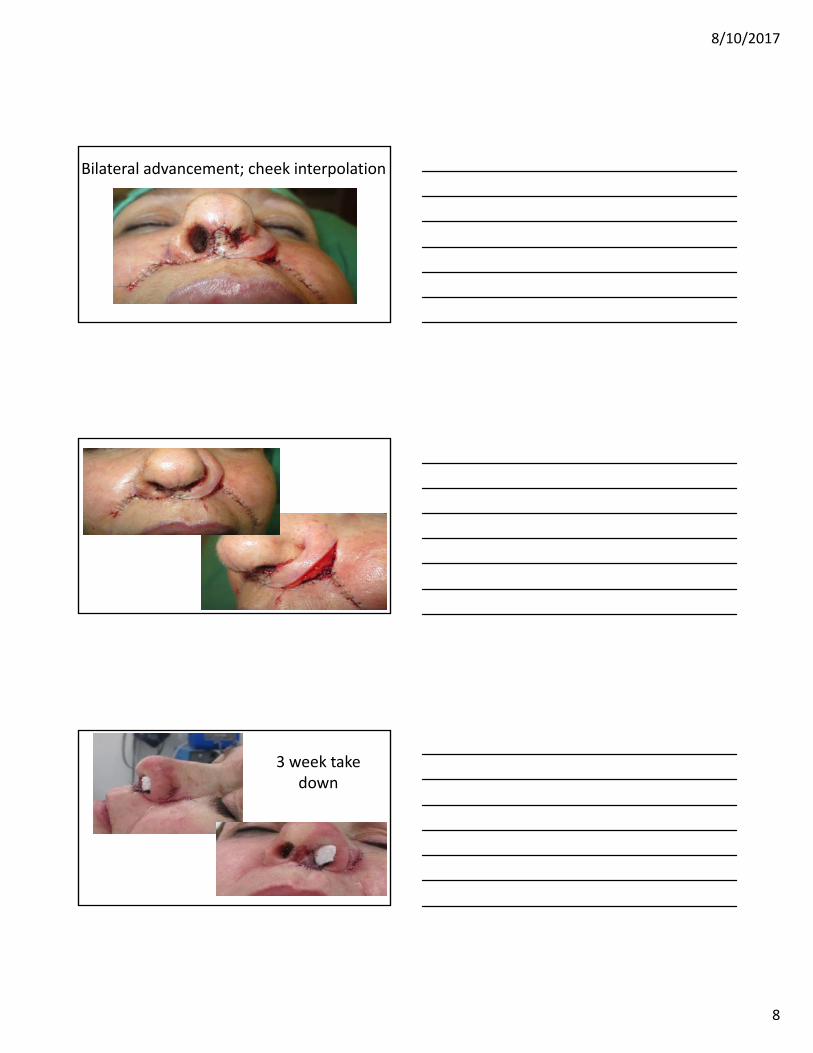
Bilateral advancement; cheek interpolation
8/10/2017
8
Bilateral advancement; cheek interpolation
3 week take down
8/10/2017
9
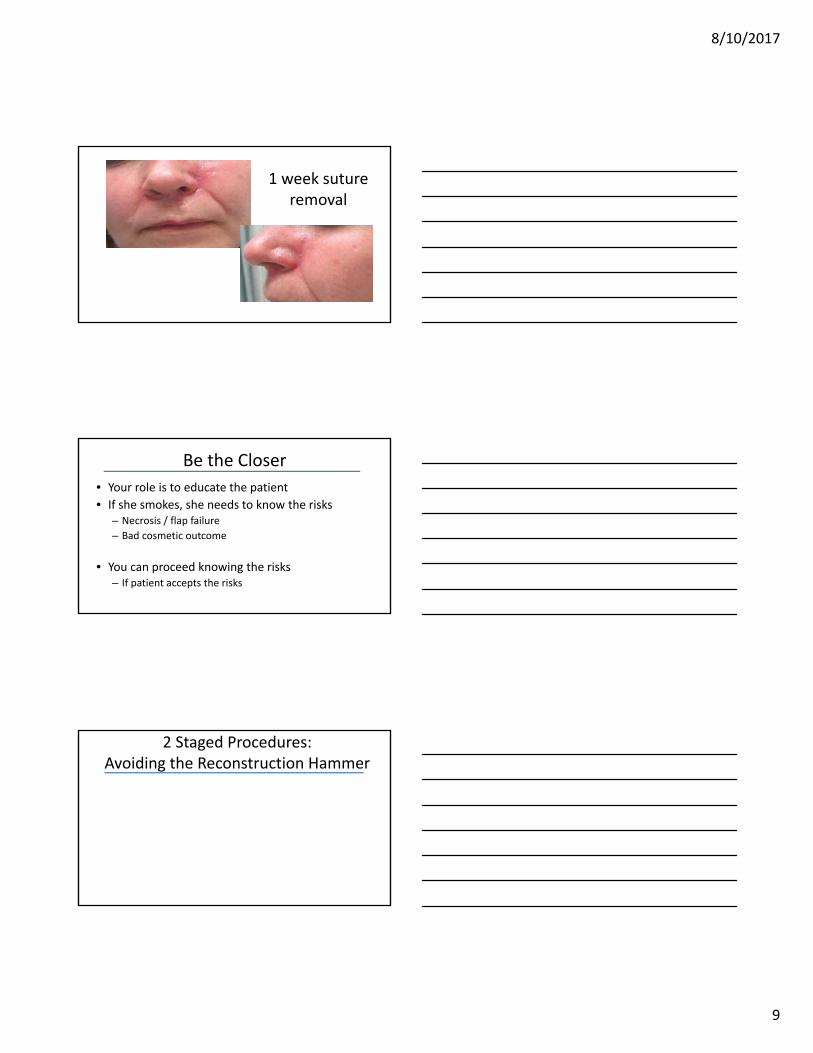
1 week suture removal
Be the Closer
• Your role is to educate the patient
• If she smokes, she needs to know the risks– Necrosis / flap failure
– Bad cosmetic outcome
• You can proceed knowing the risks– If patient accepts the risks
2 Staged Procedures: Avoiding the Reconstruction Hammer
8/10/2017
10
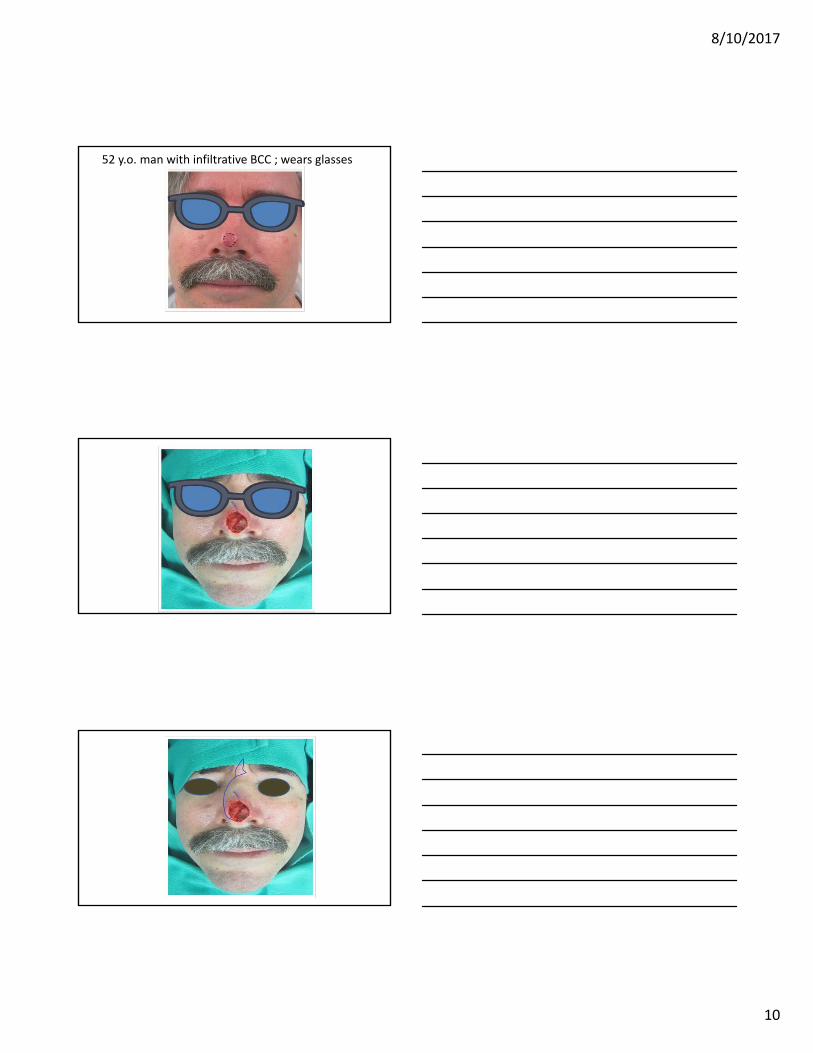
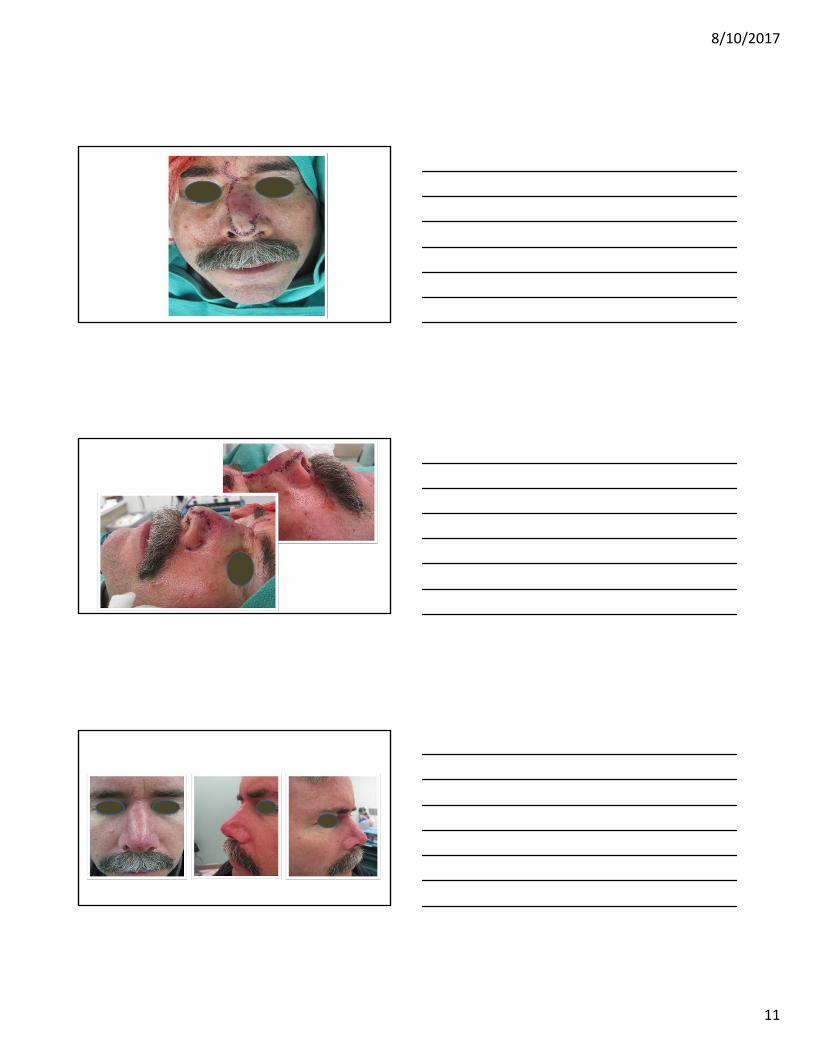
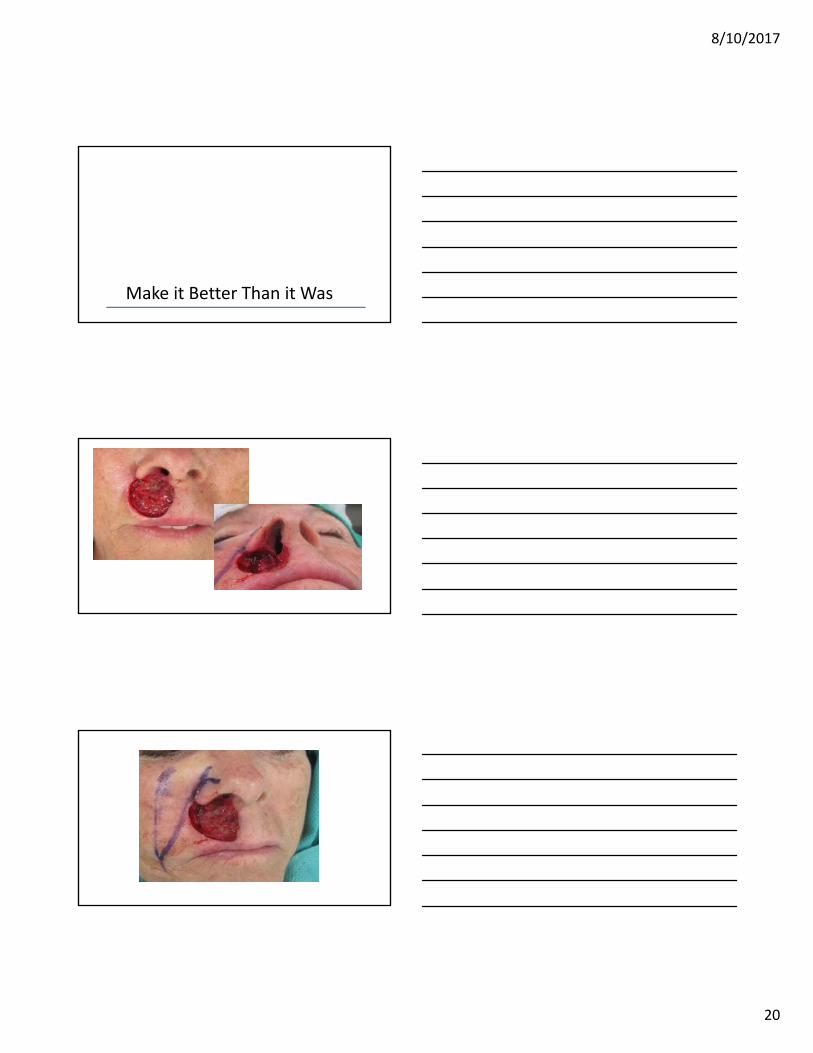
52 y.o. man with infiltrative BCC ; wears glasses
8/10/2017
11
8/10/2017
12
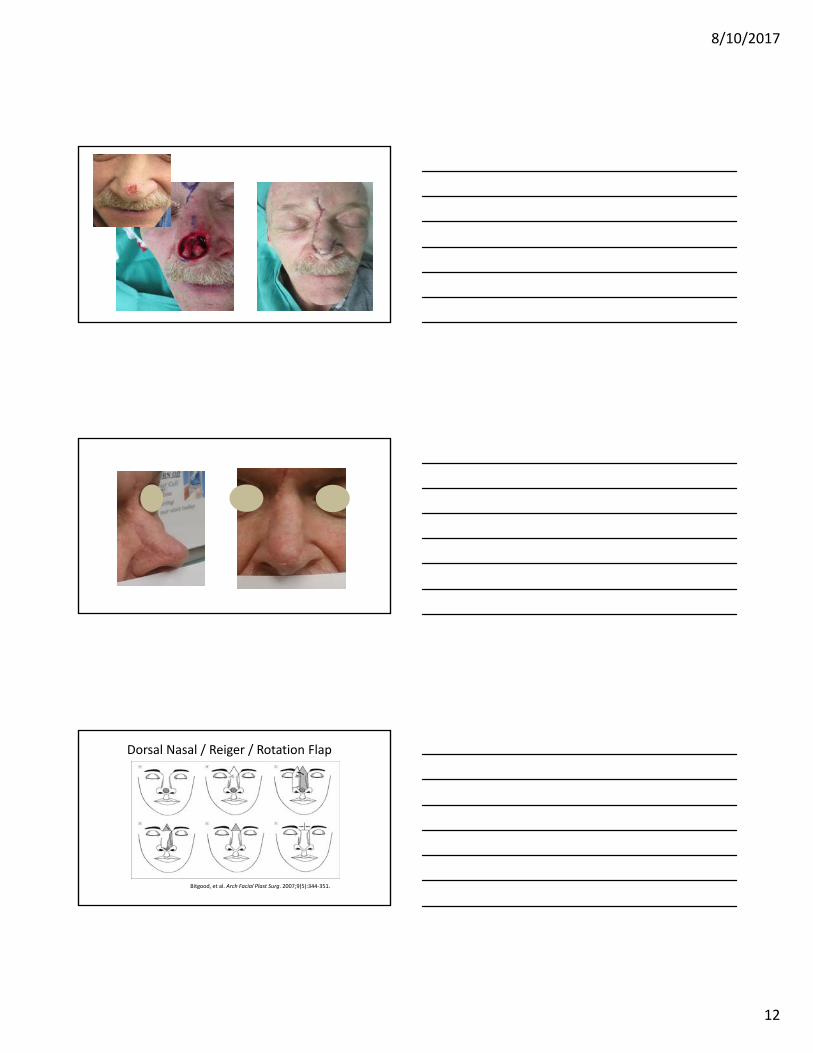
Dorsal Nasal / Reiger / Rotation Flap
Bitgood, et al. Arch Facial Plast Surg. 2007;9(5):344‐351.
8/10/2017
13
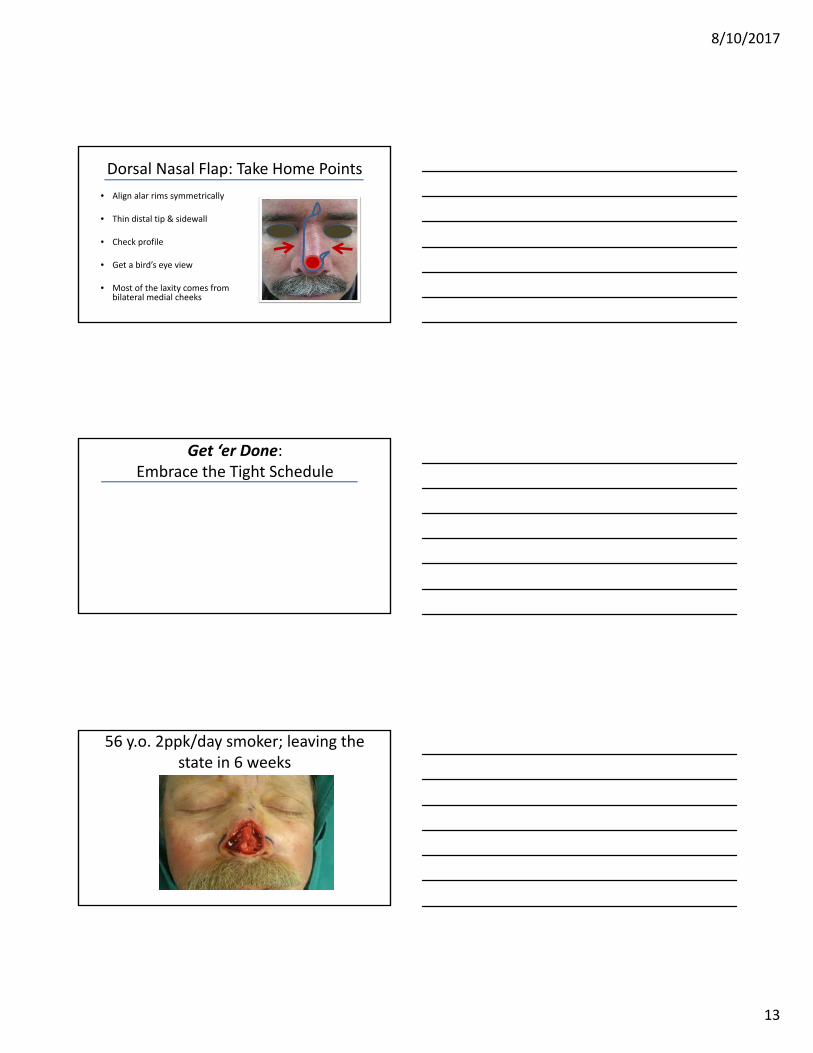
Dorsal Nasal Flap: Take Home Points
• Align alar rims symmetrically
• Thin distal tip & sidewall
• Check profile
• Get a bird’s eye view
• Most of the laxity comes from bilateral medial cheeks
Get ‘er Done: Embrace the Tight Schedule
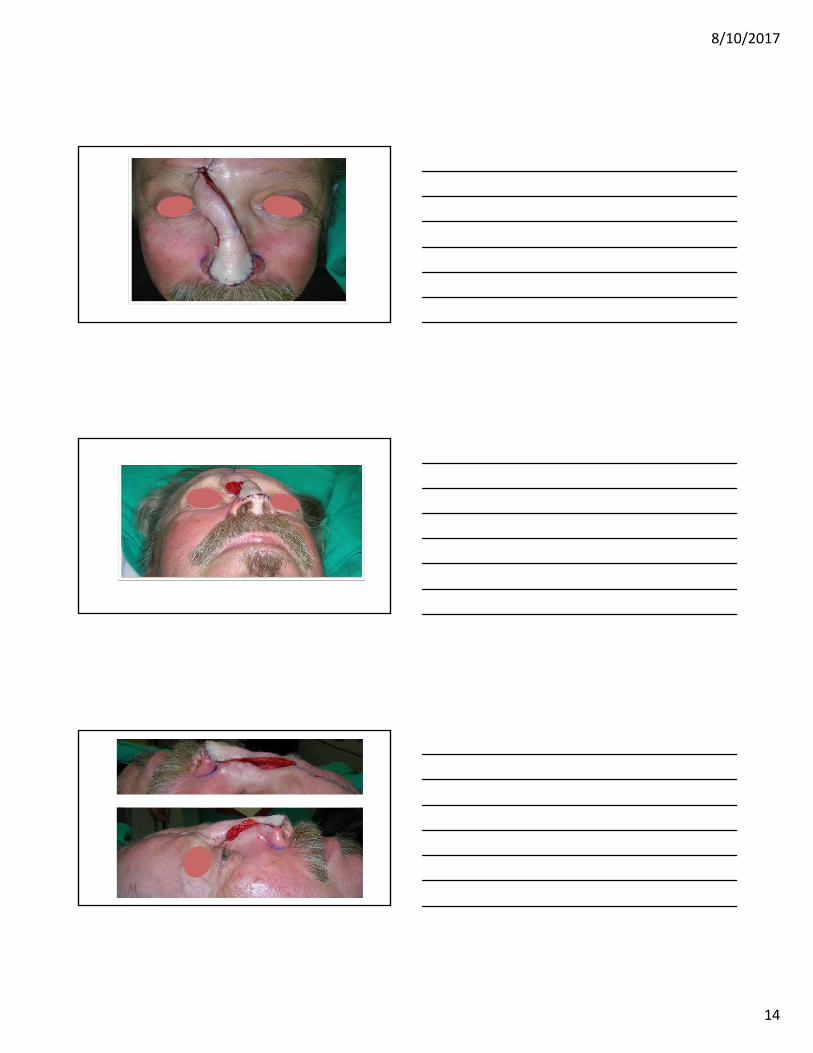
56 y.o. 2ppk/day smoker; leaving the state in 6 weeks
8/10/2017
14
c
8/10/2017
15
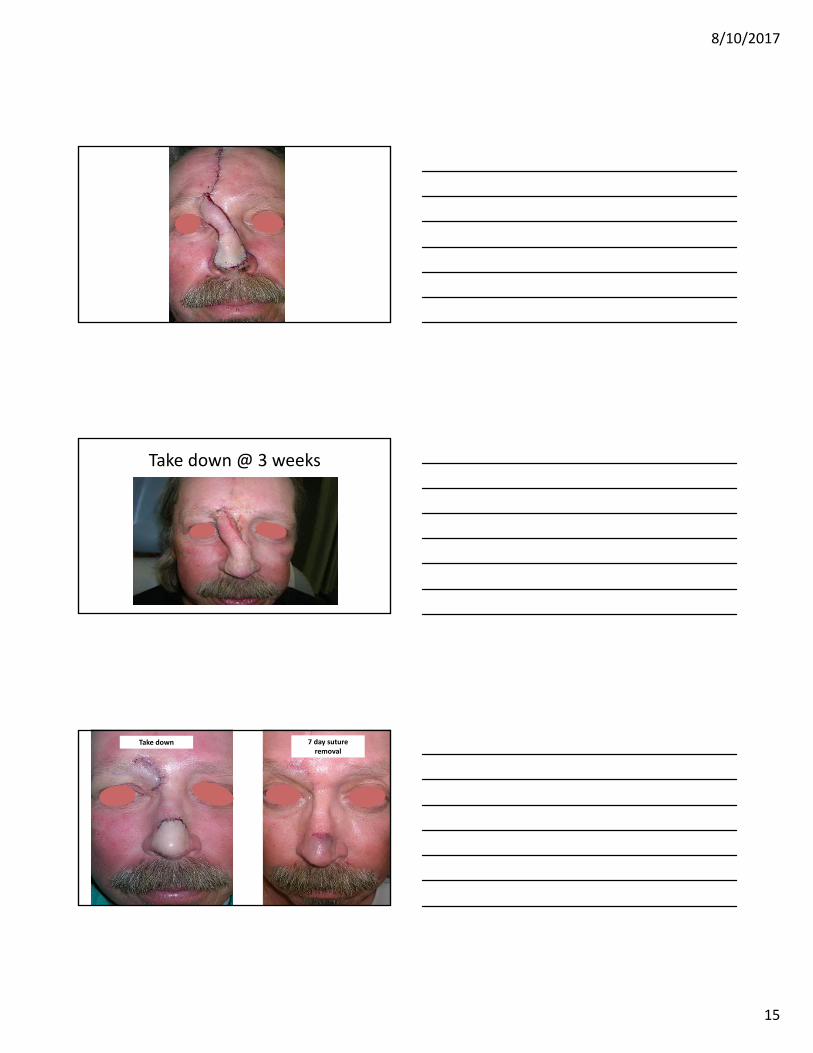
Take down @ 3 weeks
Take down 7 day suture removal
8/10/2017
16
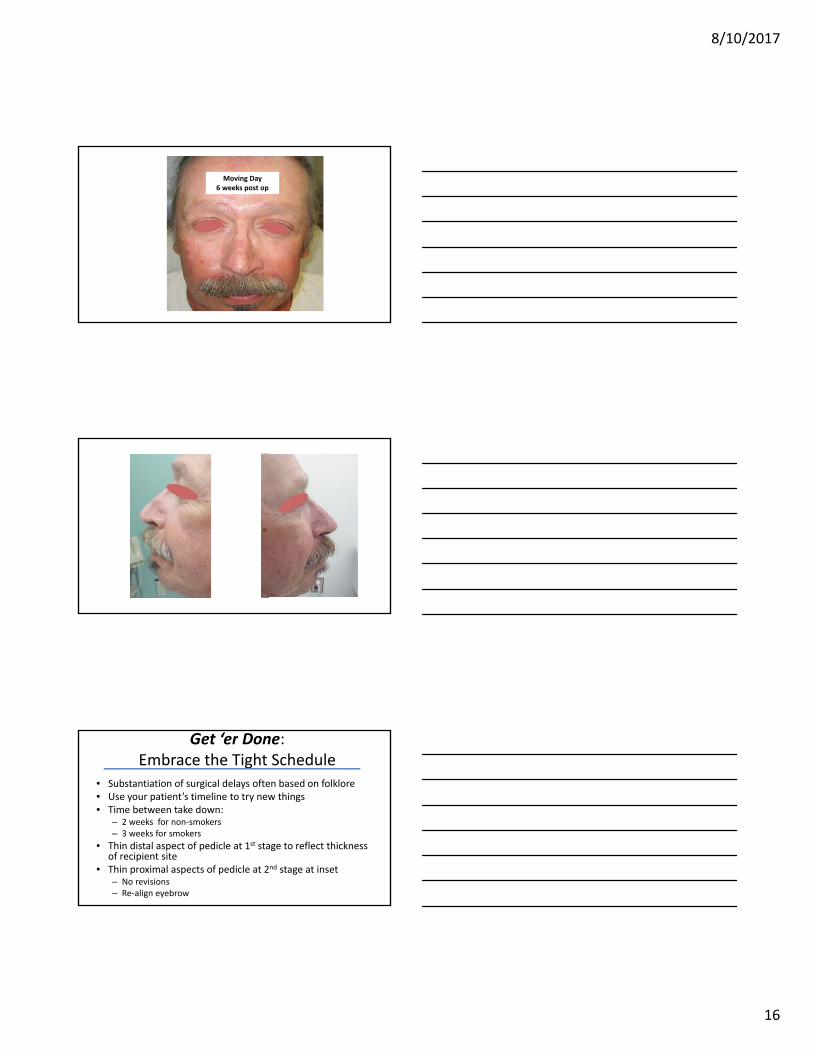
Moving Day6 weeks post op
Get ‘er Done: Embrace the Tight Schedule
• Substantiation of surgical delays often based on folklore• Use your patient’s timeline to try new things• Time between take down:
– 2 weeks for non‐smokers – 3 weeks for smokers
• Thin distal aspect of pedicle at 1st stage to reflect thickness of recipient site
• Thin proximal aspects of pedicle at 2nd stage at inset– No revisions– Re‐align eyebrow
8/10/2017
17
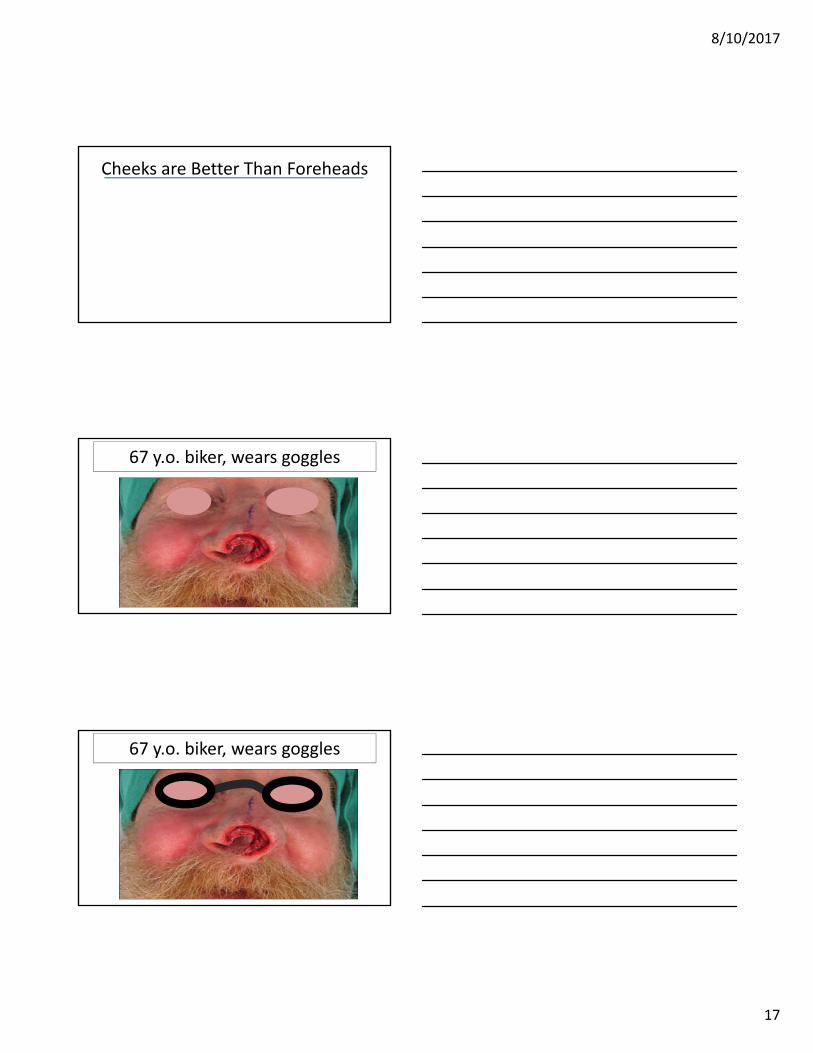
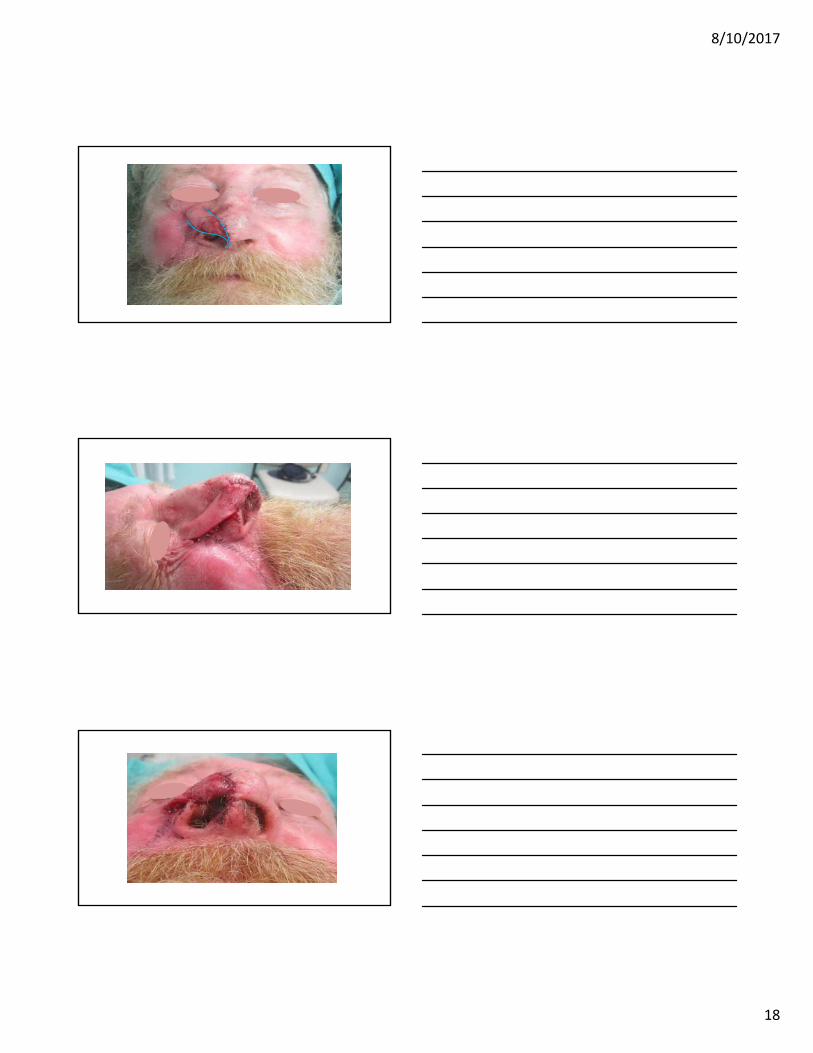
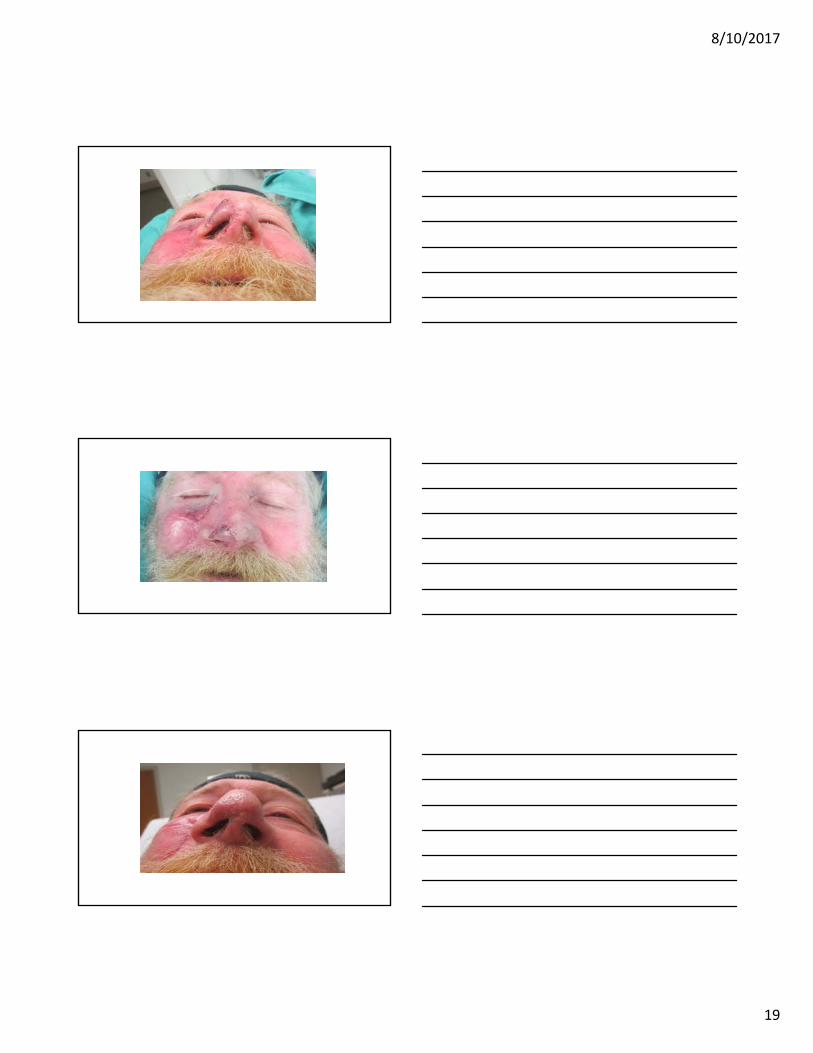
Cheeks are Better Than Foreheads
67 y.o. biker, wears goggles
67 y.o. biker, wears goggles
8/10/2017
18
8/10/2017
19
8/10/2017
20
Make it Better Than it Was
8/10/2017
21
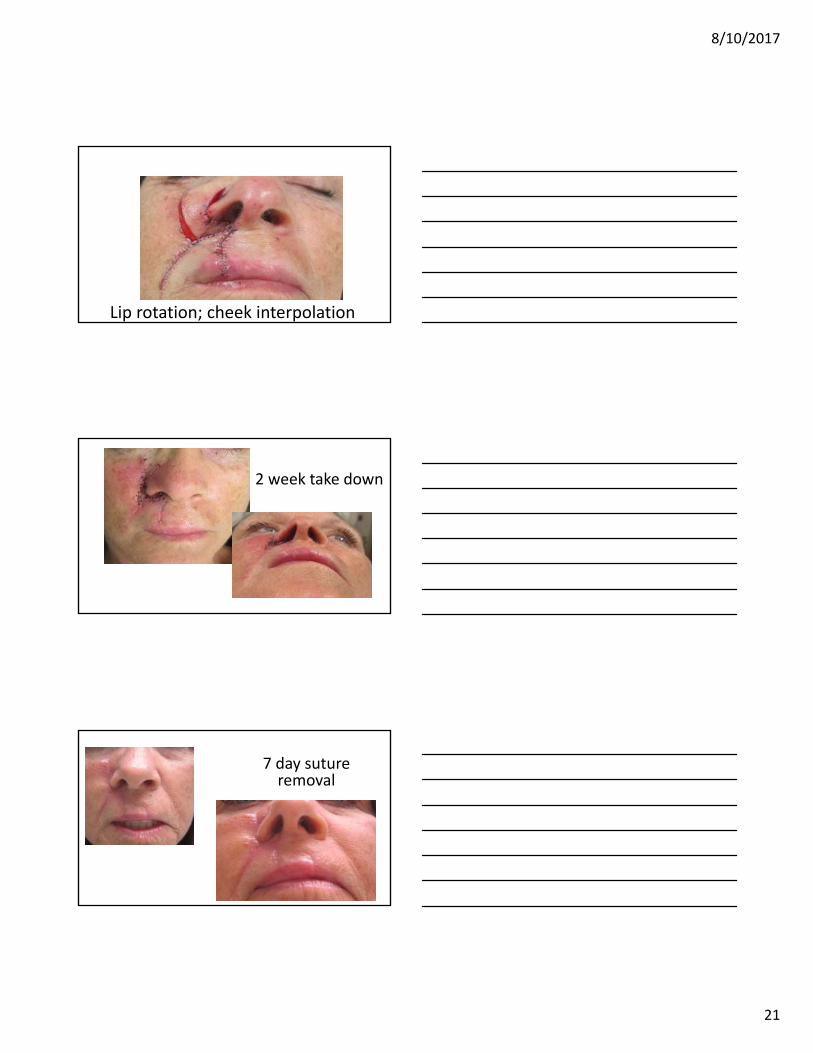
Lip rotation; cheek interpolation
2 week take down
7 day suture removal
8/10/2017
22
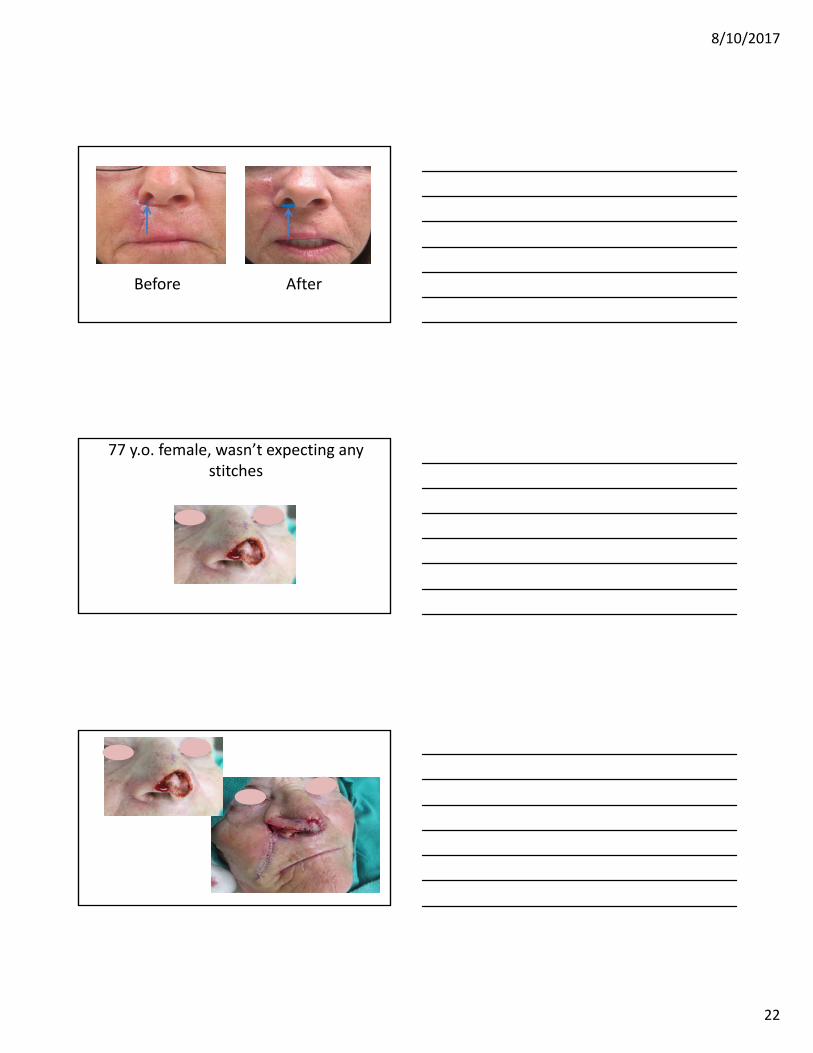
AfterBefore
77 y.o. female, wasn’t expecting any stitches
8/10/2017
23
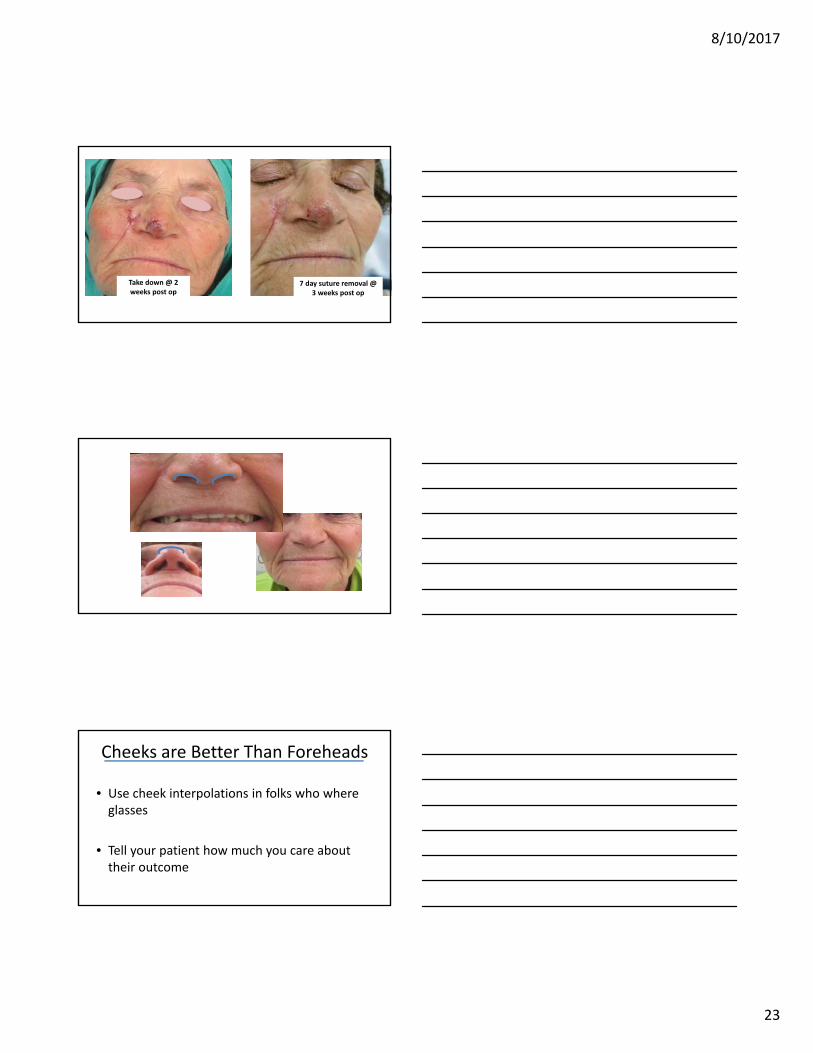
7 day suture removal @ 3 weeks post op
Take down @ 2 weeks post op
Cheeks are Better Than Foreheads
• Use cheek interpolations in folks who where glasses
• Tell your patient how much you care about their outcome
8/10/2017
24
What kind of bandage?
What kind of bandage?• No evidence to suggest that covering surgical wounds healing by primary intention
– reduces the risk of SSI
• No evidence that any particular wound dressing is more effective in:– reducing the rates of SSI– improving scarring– pain control– patient acceptability – ease of dressing removal
• Most trials in this review were small and of poor quality.
• Based on the current evidence, decisions on wound dressing should be based on dressing costs and the symptom management
Dumville JC, et al. Dressings for the prevention of surgical site infection. Cochrane Database Syst Rev. 2011 Jul 6;(7)
When to remove the bandage?• 3 trials identified for inclusion‐‐all at high risk of bias • Participants were randomized to:
– early dressing removal (removal within 48 hrs after surgery) (n = 140)
– delayed dressing removal (continued dressing of the wound beyond 48 hours) (n = 140)
• No statistically significant differences between groups in:– superficial surgical site infection within 30 days – superficial wound dehiscence within 30 days – serious adverse events within 30 days
Toon CD, et al. Early versus delayed dressing removal after primary closure of clean and clean‐contaminated surgical wounds. Cochrane Database Syst Rev. 2013 Sep 5;9
8/10/2017
25
Dayton P1, Feilmeier M, Sedberry S. Does postoperative showering or bathing of a surgical site increase the incidence of infection? A systematic review of the literature. J Foot Ankle Surg. 2013 Sep‐Oct;52(5):612‐4. doi:
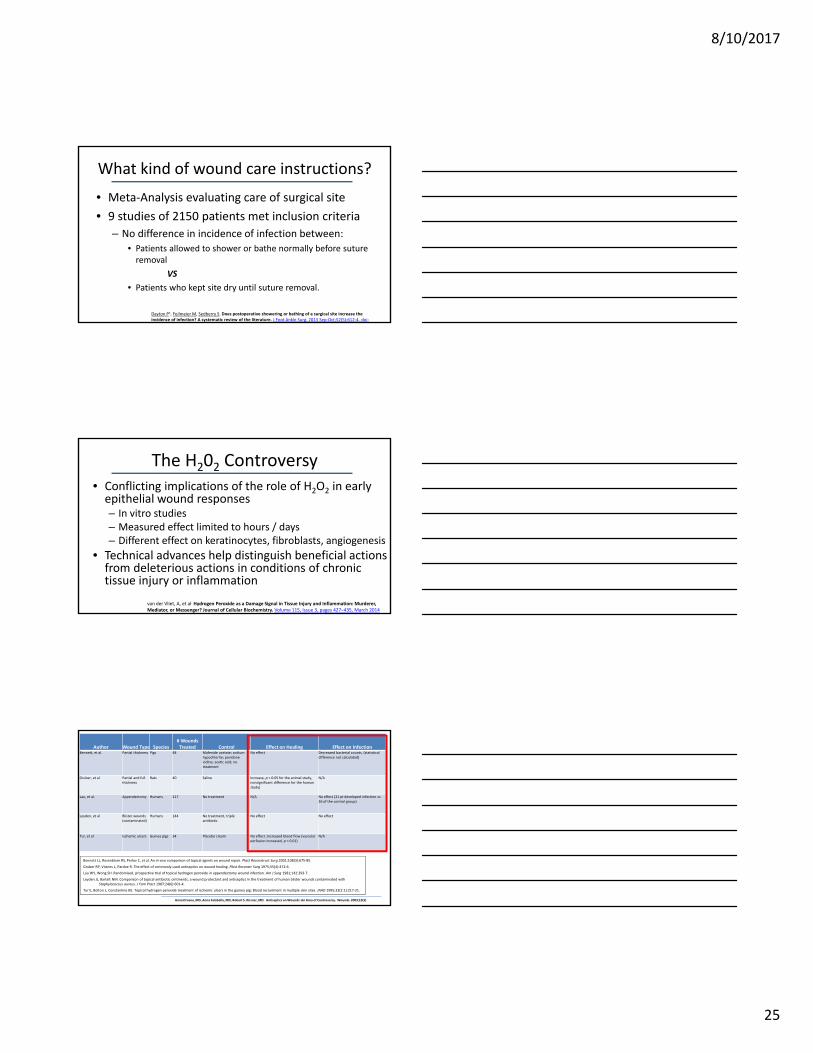
What kind of wound care instructions?
• Meta‐Analysis evaluating care of surgical site
• 9 studies of 2150 patients met inclusion criteria
– No difference in incidence of infection between:
• Patients allowed to shower or bathe normally before suture removal
VS
• Patients who kept site dry until suture removal.
The H202 Controversy• Conflicting implications of the role of H2O2 in early epithelial wound responses– In vitro studies– Measured effect limited to hours / days– Different effect on keratinocytes, fibroblasts, angiogenesis
• Technical advances help distinguish beneficial actions from deleterious actions in conditions of chronic tissue injury or inflammation
van der Vliet, A, et al. Hydrogen Peroxide as a Damage Signal in Tissue Injury and Inflammation: Murderer, Mediator, or Messenger? Journal of Cellular Biochemistry. Volume 115, Issue 3, pages 427–435, March 2014
Author Wound Type Species# Wounds Treated Control Effect on Healing Effect on Infection
Bennett, et al. Partial thickness Pigs 48 Mafenide acetate; sodium hypochlorite; povidone iodine; acetic acid; no treatment
No effect Decreased bacterial counts, (statistical difference not calculated)
Gruber, et al Partial and full thickness
Rats 40 Saline Increase, p < 0.05 for the animal study, nonsignificant difference for the human study)
N/A
Lau, et al. Appendectomy Humans 217 No treatment N/A No effect (21 pt developed infection vs. 26 of the control group)
Leyden, et al Blister wounds (contaminated)
Humans 144 No treatment, triple antibiotic
No effect No effect
Tur, et al Ischemic ulcers Guinea pigs 34 Placebo cream No effect ;increased blood flow (vascular perfusion increased, p < 0.01)
N/A
Bennett LL, Rosenblum RS, Perlov C, et al. An in vivo comparison of topical agents on wound repair. Plast Reconstruct Surg 2001;108(3):675‐85.
Gruber RP, Vistnes L, Pardoe R. The effect of commonly used antiseptics on wound healing. Plast Reconstr Surg 1975;55(4):472‐6.
Lau WY, Wong SH. Randomised, prospective trial of topical hydrogen peroxide in appendectomy wound infection. Am J Surg 1981;142:393‐7.
Leyden JJ, Bartelt NM. Comparison of topical antibiotic ointments, a wound protectant and antiseptics in the treatment of human blister wounds contaminated with Staphylococcus aureus. J Fam Pract 1987;24(6):601‐4.
Tur E, Bolton L, Constantine BE. Topical hydrogen peroxide treatment of ischemic ulcers in the guinea pig: Blood recruitment in multiple skin sites. JAAD 1995;33(2:1):217‐21.
Anna Drosou, MD, Anna Falabella, MD, Robert S. Kirsner, MD. Antiseptics on Wounds: An Area of Controversy. Wounds. 2003;15(5)
8/10/2017
26
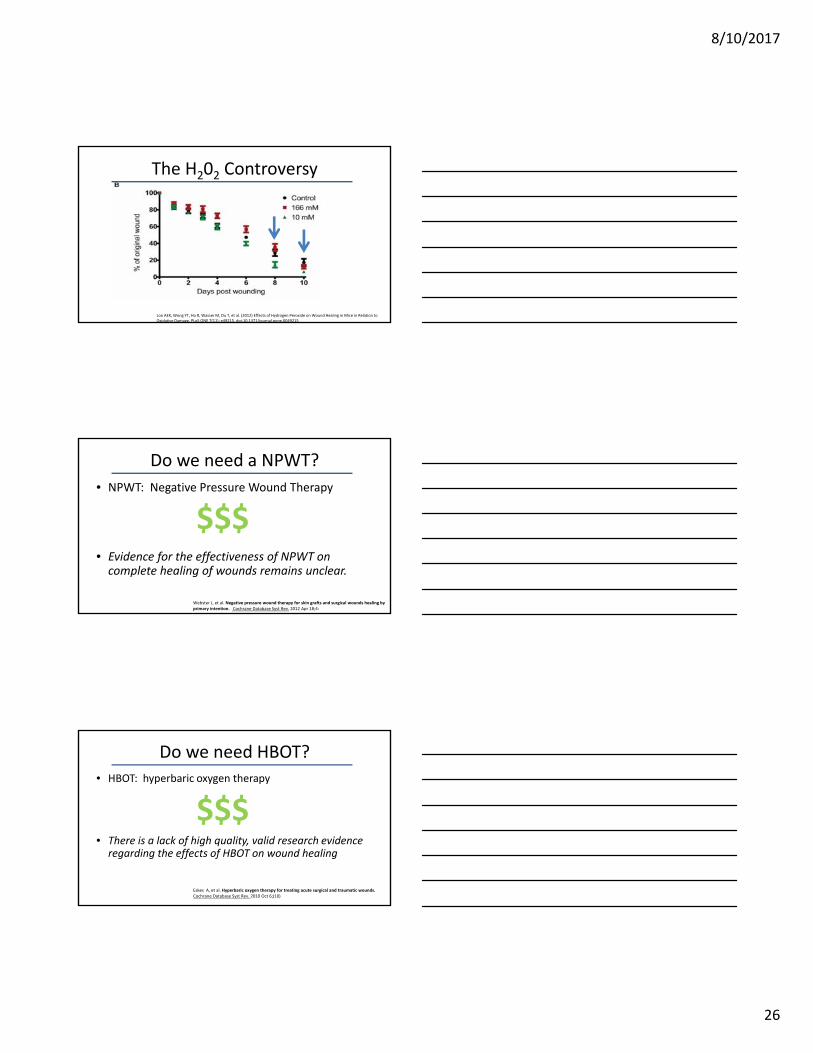
Loo AEK, Wong YT, Ho R, Wasser M, Du T, et al. (2012) Effects of Hydrogen Peroxide on Wound Healing in Mice in Relation to Oxidative Damage. PLoS ONE 7(11): e49215. doi:10.1371/journal.pone.0049215
The H202 Controversy
Do we need a NPWT?
• NPWT: Negative Pressure Wound Therapy
• Evidence for the effectiveness of NPWT on complete healing of wounds remains unclear.
Webster J, et al. Negative pressure wound therapy for skin grafts and surgical wounds healing by primary intention. Cochrane Database Syst Rev. 2012 Apr 18;4:
$$$
Do we need HBOT?
• HBOT: hyperbaric oxygen therapy
• There is a lack of high quality, valid research evidence regarding the effects of HBOT on wound healing
Eskes A, et al. Hyperbaric oxygen therapy for treating acute surgical and traumatic wounds. Cochrane Database Syst Rev. 2010 Oct 6;(10)
$$$
8/10/2017
27
Do we need a skin substitute?• Human derived / animal derived / etc
• No clinical efficacy data from RCTs are available for the large majority of the skin substitute products identified in this report
$$$
Skin Substitutes. ECRI. AHRQ Contract Number: HHSA 290‐2007‐10063. http://www.ahrq.gov/research/findings/ta/skinsubs/HCPR0610_skinsubst‐final.pdf
Contract Number: HHSA 290‐2007‐10063
Skin Substitutes: Path for Approval
• PMA: Premarket approval by FDA is the required process of scientific review to ensure the safety and effectiveness of Class III devices
• A 510(k) is a premarketing submission made to FDA to demonstrate that the device to be marketed is as safe and effective, that is, substantially equivalent, to a legally marketed device that is not subject to PMA.
• AHRQ contracted review of published studies on skin substitutes
• Overall, publications heavily biased,‐‐considered low quality or “insufficient” by reviewers– No studies reported blinding of the person assessing wound healing – All the studies in the evidence base reported “some” benefit of skin
substitutes over the control treatments at 8‐16 weeks• nonadherent dressing• saline‐moistened gauze
• Data on wound recurrence limited and varied widelySkin Substitutes. ECRI. AHRQ Contract Number: HHSA 290‐2007‐10063.
http://www.ahrq.gov/research/findings/ta/skinsubs/HCPR0610_skinsubst‐final.pdfContract Number: HHSA 290‐2007‐10063
Skin Substitutes
8/10/2017
28
• Only generally healthy patients were enrolled • Studies excluded patients with:
– infected wounds– medications that could impede wound healing– significant medical conditions– peripheral vascular disease– nutritional compromise– uncontrolled diabetes
• Paucity of studies comparing skin substitute products (2)
Skin Substitutes. ECRI. AHRQ Contract Number: HHSA 290‐2007‐10063. http://www.ahrq.gov/research/findings/ta/skinsubs/HCPR0610_skinsubst‐final.pdf
Contract Number: HHSA 290‐2007‐10063
Skin Substitutes
Do we need a fancy scar cream?
• Or a bandage with silicone sheeting?
• No available unbiased published material*
*The entire internet; accessed August 2017
$
Irrefutable Evidence• Moist or occlusive dressings • Keeping it clean (nothing fancy)• Basic surgical suture techniques• The smaller the better BUT large scale inflammation
obscures scarring• Host factors are imperative
– Smoking– Coagulation– Immunity
8/10/2017
29
All a Matter of Opinion
• Antiseptics
• Types of sutures
• Type of stitch
• Bandages
• Patient activity (within reason)
Post Surgical Wound Care Recommendations
• Less is More
• Listen to your MA’s/ Nurses / Surg techs
• Put the onus on the patient for the surgical outcome
QUESTIONS?Marta J. Van Beek, MD, MPH