Embed Size (px)
Citation preview


Survey ofPhilippine DevelopmentResearch III

Survey of
Philippine, DevelopmentResearch IIi
P/S PHILIPPINE INSTITUTEFOR DEVELOPMENT STUDIES

Board of Trustees
ChairmanHon. Solita Coll_s-Monsod
MembersDr. Gelia T. CastilloDr. Edita A. Tan
Dr. Filologo Pante, Jr.
All Rights Reserved byTHE PHILIPPINE INSTITUTE FOR
DEVELOPMENT STUDIES, 1989
The Philippine Institute for Development Studies isa nonstock, nonprofit, government research institutionengaged in long-term, policy-oriented research. It wasestablished on September 26, 1977 by virtue OfPresi-dential Decree No. 1201.Throughthe Institute'sactivi-ties, it is hoped thatpolicy-oriented research on Philip-pine social andeconomicdevelopmentcanbe expandedin such a manner as to more directly and systematicallyassist the government in planning andpolicymaking.
PIDS publishes the outputof its researchprogram aspart of its efforts topromote the use ofreseamh findingsand recommendations. The views expressed in thisbook, however, do not necessarily reflect those of theInstitute.
Printed in the Philippinesby Kolortech, Co.
RP-2-89-500ISBN 971-128-015-9

Foreword
This third volume of the Survey of Philippine Development, Research
compiles the papers presented during the seminar-workshop on "A Pro-gram of Research on Health and Development" held on December 17-18,.
1986, sponsored by the Philippine institute for Development Studies
(PIDS) and the University of the Philippines' School of Economics
(UPSE).
These state-of-the-art review papers on health were put together to
identify research gaps and issues on health policies to assist PIDS in
formulating a research agenda on health.
It is therefore hoped that these .papers will contribute to the efforts of
identifying future directions for health policies in the country.
_JR.
PreS'kal_nntPhilippineInsatute for D_tvetIopment Studies
Febmary1989

Contents
Foreword vTables and Figures xii
HEALTHAND DEVELOPMENT: A REVIEWOF THE DETERMINANTS AND CONSEQUENCESOF HEALTH IMPROVEMENTS IN THEPHILIPPINES by AlejandroN. Herrinand MaricarGinsonBaustista
I. Introduction 1
II. Health Problems:An Overview 2
SourcesandAdequacyof Data 2Mortality 3Morbidity 6
Nutrition 6 •Summary 11
III. DeterminantsandConsequencesof HealthImprovements:ConceptualFramework 11
Determinants 11
AlternativePerspectives 11ConceptualFramework 12Hypotheses:ProximateDeterminants 15Hypotheses:SocioeconomicDeterminants 17
Consequences 18

viii Contents
IV, DeterminantsandConsequencesof HealthImprovements:Evidence .19
ProximateDeterminants 19SocioeconomicDeterminants 27
SocioeconomicDeterminantsof ProximateVariables 28SocioeconomicDeterminantsof HealthOutcomes 31
Consequences 36
V. Summaryof Findingsand ResearchDirections 38
Bibliography 41
STRUCTURES AND INTERVENTIONS IN THEPHILIPPINE HEALTH SERVICE DELIVERY SYSTEM:STATE OF THE ART by VictoriaA. Bautista
I. Introduction 45
I1. ConceptuaIBackground 46
A. OrganizationalStructure 46PublicVersusPrivate 46CentralizedVersusDecentralized 47
SectoralVersusIntegrated 47B. Strategies 48
II1. Trendsand Patterns 49
A. PluralisticVersusUnitaryStructure 50GovernmentalNetwork 50PrivateNetwork 51Assessment 51
B. Decentralizationto Recentralization 52BroadPolitical-AdministrativeFramework 52MOH Effortsto Decentralization 53
C. PrimaryHealthCare 54Background 54Streamliningof MOH Structureto AccommodatePHC 56EmpiricalStudiesonPHC Experiences:Publicand Private 56
D. CurativeVersusPreventiveand OtherAspectsof Health 60CurativeandPreventiveComponents 60Other Componentsof Health 62
E. RelianceonWHC, TWC and PHC 64

Contents ix
F. FocusonSelected Sectors 65Women andChildren 65
TargettingCouples 69Work Force 71
IV. PolicyProblems/Issues 73
A. Froma Pluralisticto a UnifiedHealthProgram 73B. PHC as a Strategy 74
PHC orCommunity-Based? 74Community-OrientedorCommunity-ManagedPHC? 75BarangayHealthWorkers 76Westernizedto PHC Resources/Technology 78Centralizationto Decentralization 78
C. Curativeto Promotive/Preventive/RehabilitativeMedicine 79D. FocusonOtherSectors 80
E. An InterdisciplinaryModelto Assessthe Effectivenessof Structuresand Interventions 80
F. Participatoryand IntegratedApproachesatAll Levels 81
Bibliography 82
DEMAND FOR HEALTH CARE: A REVIEW by Panfila Ching
I. Introduction:Need, DemandAndThe PurposeOf DemandAnalysis 89
I1. A SelectiveReviewof ForeignLiteratureOn Health Care 92
A. Simple UtilityMaximizingModels 92B. Utility-MaximizingModelwithTime Cost 92C, HouseholdProductionModel 93
D. HumanCapitalModel 93E. HumanCapitalModel withCoinsurance 94F. The InducementHypothesis 95G. Demand inLow-IncomeCountries 95
II1. StudiesOn The PhilippineHealthCare 96
IV. FactorsAffectingDemand For HealthCare 97
A. Income 97B. Price 99
MoneyPrice 100

x Contents
Time Price 101C. Health Insurance 102D. DemographicFactors 103
AgeComposition 103Sex Composition 104Family Size 104
E. Knowledgeand Information 104Education 104
Health,KnowledgeandBeliefs 105F. Health Need 105
G. Availabilityof HealthService 105H. Time andAllocationof Mother 106i. Locationand Residence:Urbanor Rural 106J. Distanceof HealthService 106
V. ResearchGaps And PolicyImplications 107
A. Do DoctorsGenerate TheirOwn Demand? 107
B. Specificationof the DependentVariable 108C. Specificationof the Health StatusVariable 109D. ShouldDemandAnalysisIncludePeople
Who are Notin Need? 109E. Price, Non-Usersand Data Problems 110
Bibliography 112
HEALTH FINANCING IN THE PHILIPPINES: A REVIEW OF THELITERATURE by Ma. Concepcion P. Affiler
I. Introduction 117
I1. Objectives 118
III. Health Financing:Conceptualand MethodologicalIssues 119
Defining/Delimitingthe HealthSector 120FinancingSources 121AssessingHealthCare FinancingSchemes 124MethodologicalIssues 125
IV. Health Financinginthe Philippines 126
Sector-WideStudies 127

Contents xi
Public/PrivateResources 128NationalHealth Insurance 129Community/PrimaryHealthCare Financing 132USAID PrimaryHealthCare FinancingProject 132
V. Researchand PolicyImplications 135
Bibliography 137

xii Contents
Tables and Figures
Herdn and Bautista Paper
1 Selected Estimates of Mortality, Philippines, 1948-1980 ..................... 42 Death Rates By Leading Causes, Philippines, Selected Years ........... 53 Ten Leading Causes of Mortality Rate By Age Group, 1983 ............... 74 Infant Mortality: Ten Leading Causes, Rate (Per 1,000 Live Births),
Philippines, 1980 - 1984 and Five-Year Average 1975-1979 .............. 85 Ten Leading Causes of Morbidity, Philippines, 1978 - 1984 ................ 96 Ten Leading Causes of Morbidity by Region, 1983 ............................. 107 Percentage Distribution of RespondentsConsulting Health
Workers for Ante-Natal Care By First Reference, 1978 ....................... 238 Distribution of Attendance at Birth By Categoryof Attendant,
1978 -1981 ........................................................................................... 239 Trends in BreasffeedingPrevalence and Duration, Philippines,
1973 - 1983 .......................................................................................... 2410 Trends in BreasffeedingPrevalence and Duration By Selected
Characteristics, Philippines, 1978 and 1983 ........................................ 2611 Percentage Distributionof HouseholdsBy Distance in
Kilometers to Various Health Facilities Nearest tothe Household, 1978 and 1981............................................................ 27
Fig. 1 Conceptual Framework for Analyzing the Determinants ofHealth Outcomes ................................................................................. 13
Bautista Paper
Fig. 1 Assessingthe EffectivenessofStructures�InterventionsforHealth ...................................................... 81

Survey ofPhilippine DevelopmentResearch III

Health and Development:A Review of the DeterminantsAnd Consequences of HealthImprovements in the Philippines
Alejandro N. Herrin and Maricar Ginson Bautista*
I. INTRODUCTION
In the broadest sense, health is defined as a state of completephysical,mental and socialwell-being(WHO, 1978)oPeopleplace greatvalueonhealth andgovernmentsrecognizehealthas a basichumanright.The PhilippineDevelopmentPlan1987-1992 notedthat "Theyearsfollow-ing 1975 witnesseda s!ackeninginthe advancetowardsimprovedhealthandnutritionalstatusandattainingsmall-sizedfamilies."Howdoesone tryto acceleratesuchanadvanceinthe faceofsevereresourceconstraintsatbothnationaland householdlevels?To properlyanswersucha question,one must have a clear understandingof whatdeterminesvarious healthoutcomesasbasisformakingchoicesregardingthemostappropriateformsofpublicinterventionsgivenscarceresources,andregardingwhichhealth-promotingactivitiescan bestbe leftto individualsand households.Implicitinthe abovequestionis a commonunderstandingof theconsequencesofchanges in health status. How much do we know about such conse-quences?Are theyseriousenoughto justifythe reallocationof thealready
* Professor and Chairman, Department of Economics, University of the Philippines, ..Schoolof Economics and Assistant Professor, Department of Economics, Ateneo deManila University, respectively.

2 AlejandroIV.Herrin& MaricarGinsonBautista
limitedresourcestowardhealth-promotingactivities,at theexpenseofotheractivities?
Thispaperattemptsto reviewavailableinformationthataddressestheabovequestions.It is hopedthatthisreviewwillhelpclarifywhatwe knowandilluminateareas aboutwhichwe wouldliketo knowmore.Thispaperisorganizedas follows:SectionII providesa quick overviewof the healthsituationin the Philippines.Section III presentsa simple frameworkforanalyzingthedeterminantsandconsequencesofhealthstatuschangeanddescribesvarioushypothesesregardinghealthanddevelopmentinterac-tions.SectionIV reviewstheempiricalevidenceforthe Philippines.Thefinalsectionsummarizesthe findingsand suggestsresearchdirections.
II. HEALTH PROBLEMS: AN OVERVIEW
Althoughseveralindicatorshavebeen usedorproposedto measurethe various dimensionsof health_P_aqueo1976;Andrews 1981; Sintoneni981), it is still common to describe the health status of the population interms of traditional indicatorssuchas mortalityand morbidity rates. Intermsof mortality, the life expectancy at birth and infant and child mortality ratesare the commonly used measures. Morbidity rates by leading cause ofillness have also been utilized to provide a rough indication of changinghealth situation.
Sources and Adequacy of Data
Getting an accurate description of the health status of the populationis hampered by inadequate and often defective information on even suchtraditional measures as mortality and morbidity rates. Common sources ofdata such as the vital registration systems for deaths, and the death anddisease reporting system of the then Ministry of Health invariably producedata that tend to beunderestimatesof the true mortalityand morbidity rates.Moreover, becauseof differential coveragesof reporting of specificcausesof deaths or of illnesses, the data also tend to present a distorted pattern ofthe relative importance of various diseases and causes of death.
As an alternative, direct mortality and morbidity information can beobtained from surveys. But suchinformation are too expensive to get (e.g.the sample sizes required to obtain stable estimatesare quite large), andmay alsobedefective (i.e.understated becauseoffailure to reportall deathsin thecase of mortality, andrecallproblemsand inaccurate reportsof causesof illnesses in the case of morbidity).
Indirect estimates of mortality rates from census and vital registrationdata provide another source of information of the health status of thepopulation. In the Philippines, these estimates are available only at few

HealthImprovements:DeterminantsandConsequences 3
discretetime periodsandare oftennotcurrentenoughtobe readilyusefulto detectmore recentchangesandtrends.
Inspiteof suchdata shortcomingshowever,itis stillpossibleto get abroad descriptionOf the more salient health problemsfrom availablemortalityandmorbidityinformation.
Mortality
LEVELS, TRENDS AND DIFFERENTIALS. Table 1 presentsselectedestimatesof the crudedeath rate, life expectancyat birth, infantmortalityprobability,andthe life tablechildsurvivalratestogetherwiththeir respec-tiveaverageannuallinearchangesoverselectedperiods.Asthedatashow,the progresstowardsmortalityreductioninthe Philippineshavebeenquiteuneven.Mortalitydeclinewas very rapidduringthe 1950s, sloweddownconsiderablyin the 1960s, but picked up again in the 1970s. Progresstowardsraisinglifeexpectancyat birth,however,appearsto havesloweddowninthe secondhalfof the 1970scomparedto the firsthalf, as are thechildsurvivalrates.The downwardtrendininfantmortalityrate in the firsthalfof the 1970s appearsto be sustainedinthe secondhalf. By 1980, thelifeexpectancyatbirth reached62 years,theinfantmortalityratedeclinedto58 per 1000births,andthechildsurvivalratefrombirthto age5 yearsroseto 907 per 1000 births. Data for the 1980s, however,are hard to obtain.There is speculationthat progresstowardsmortality reductionwouldbeslowerinthe 1980scomparedtothe 1970sbecauseoffactorsrelatedtothedeclineineconomicI:>erformancein 1980s (Herrin and Paqueo 1985).
If mortalitydata at the national level are hard to obtain,data onmortalitydifferentialsare evenharderto get.The very littledata available,however,doshowlargemortalitydifferentialsbyregion(Flieger,eta/. 1981).In 1970,whilethenationalaveragelifeexpectancywas56 years,thisvariedfroma highof60 yearsinSouthernLuzon(includingMetroManila)to a lowof 48years in Westem Mindanao.This differenceof 12 years is morethanthedifferenceinthenationallifeexpectancyobservedbetween1948-50and1960, the periodwiththemostrapidmortalitydeclineinthepostwarperiod.Theinfantmortalityrate(qo)alsovariedfrom75inSouthemLuzon(includingMetroManila)to 135 inNorthernMindanao;thedifferenceis comparabletothe declineinthe nationalrate fromthe eady 1950sto 1975.
Indirectestimatesof infantmortalityratesfrom the 1978 Republicofthe PhilippinesFertilitySurvey (RPFS) alsoshowlargevariationbysocialgroupsdefinedbythecharacteristicsofthe mother(Esc/amad, de Guzmanand Engracia 1984).Theinfantmortalityrate (q_ per 1000birthsvariedfrom52 among mother,s_withcollegeeducationto 118 amongmotherswithnograde completed;from 69 among motherswho can read to 130 amongmotherswhocannotread;froma rangeof48to 72amongChristianmothers

Table 1- SELECTED ESTIMATES OF MORTALITY, PHILIPPINES, 1948-1980
Child Survival Rates at
Exact Ages
Life Expectancyat Infant Mortality (-J'-)ls (11__o) _.Year Crude Death Rate Birth (eo°) Probability (xqo) Age 5 _o Age 10 "o
Average Average Average Average Average __Annuat Annual Annuat Annual AnnuaI
Level Change Level Change Level Change Level Change Level Change '_
(x1000) (x1000) (Years) (Year) (x1000) (x1000) (x1000) (x1000) (x 1000) (x1000)
1948-50 21.6 - 42.5 - 166.5 - 751 - 700 -1960 12.8 0.80 52.8 0.93 113.3 •4.8 834 7.5 821 11.0 =1970 10.8 0.20 55.8 0.30 93.2 2.0 866 3.2 853 3.2 _'1975 8.7 0.42 59.4 0.72 76.6 3.3 888 4.4 877 4.81980 8.8 0.02 61.8 0.48 58.3 3.7 907 3.8 898 4.2 _"
o
SOURCES:'•For .1948-50, estimates of crude death [ate and fife expectancy at birth are taken from Mac_gan (1965), while estimates of infantmortatity probabitity andchifd survival rates are obtained by interpolation from Model Life Table, West, Levels 9and 1I. For 1960, 1970and 1975, mor_ estimates are from Rieger, et al. (1981). For 1980, mortality estimates are from Concepcion and Cobigon (1984). "_

-t_lealthImprovements:DeterminantsandConsequences 5
tO 174 amongMuslim-and from 46 amongblue collarworking-rnothersto 74 amongfarm-relatedworkingmothers.Such social groupdifferences,except for the last category,are muchwider than the entiredifferenceinthe nationalinfantmortalityratefrom 1960 to 1980.
CAUSE OF DEATH. Table 2 showsthe major causes of death. Theseincluderespiratorydiseases,gastro-infestinaldiseases,cardiovascularandneoplasms,andvariousdiseasesrelatedto infancy and early childhood,includingnutritionaldeficiency.In 1980, the ten leadingcausesof deathconstitutedroughly42 percentof all deaths,Moreover,of the ten leadingcauses of death in 1980, close to half (49 percent) was attributedtorespiratoryandgastro-intestinaldiseases.
Table 2: DEATH RATES BY LEADING CAUSES,PHILIPPINES, SELECTED YEARS
Death Rate Per 100,000 Population
Causes 1950 1960 1970 1980 1984
Pneumonia 136.7 100.4 118.2 93.6 89.3Influenza 26.1 ....Bronchitis 100.6 57.2 27.9 - -Respiratorytuberculosis 135.5 92.1 77.0 59.6 52.9Gastro-enteritis 57.7 60.5 35.0 - -Dysentery 7.0 ....Diarrhea - - - 27.9 27.8Heart disease 18.7 27.6 34.0 60.8 61.0Diseaseof vascularsystem - 20.6 35.8 43.8 39.6Malignantneoplasm 8.6 18.2 25.6 33.2 30.2Ill-defineddiseaseof
early infancy - 32.5 19.1 - -Nutritionaldeficiency 113.6 54.4 25.5 15.3 13.4Measles 38.3 - - 10.7 9.8Nephritis,neophrotic
syndrome,nephrosis - - - 9.3 8.5Accidents - 14.6 24.8 18.7 16,8
SOURCE.°,:PhilippineHealthS_tics series1926-1972(Manila:DiseaseIntelligenceCenter,DepartmentofHealth):PhilippineVitelStatisticsRepot1series1972-1977(Manila:N_EDA); PhilippineHealthStatistics1981.1984(HeallhIntelligenceService,IV_nislryofHealth)asreportedinZablan(1986).

6 AlejandroN.Herrin&Ma/fcarGin$onBautista
The age patternof mortalityin 1983 fromthe ten leadingcausesisshowninTable 3. Pneumonia,diarrhea,measlesand nutritionaldeficien-ciesareseentobethemajorcausesofdeathofinfantsandyoungchildren.(See alsoTable 4 forthetenleadingcausesof infantdeaths.)Tuberculosisprogressivelygainsinimportanceasa majorcauseof deathfromage 15tolateradulthood.Incontrast,cardiovascularand neoplasms arethe majorcausesof deathof adultstowardsthe endof theireconomicallyproductivelife.
Morbidity
Table5 showstheten leadingcausesofmorbidityfrom1978 to 1984.In1984,respiratorydiseasesaccountedfor61percentofallmorbiditycasesamongthe ten leading causes,whilediarrhea accountedfor another24percent.Ofgreatinterestistheincreaseinmorbidityratessince1980. Couldthis be related to the increasingeconomicstress associatedwith thedecliningperformanceof the economywhicheventuallyculminatedintheeconomiccrisisof 1983 and1984?
RegionalmorbidityratesbyleadingcausesshowninTable 6 revealwidevariations.Region12 (CentralMindanao)exhibitsthehighestmorbid-ityrateswhiletheNationalCapitalRegion(MetroManila)exhibitsthelowestrates.Otherdiseasesarearea-specific.TheincidenceofmalariaishighestinCagayanValleyand WesternMindanao,whileschistosomiasisisoneofthe ten leadingcausesin EasternVisayas.
Nutrition
The majordiseases(respiratory,gastro-intestinalandotherinfectiousdiseases(i.e. measles)whichaffect infantsandchildrenare often associ-ated with malnutrition.Malnutritionin itseffis also shownas one of theleadingcausesof death.Thus, inadditionto mortalityand morbidityrates,itwouldbeusefulto examineavailabledataon the nutritionalstatusofthepopulation.
The nutritionalstatusofthepopulationisgenerallydescribedintermsof (a) energyandproteininsufficiency;(b)growthfailure,especiallyamongpre-schoolchildren;and(c)micronutrientdeficiencies.Surveysconductedby the Food and NutritionResearchInstitute(FNRI) reveal the followinglevelsof adequacy:for energy,88.6 and 89.0 percentin 1978 and 1982,respectively;whilefor protein,93.2 and 99.6 percentin 1978 and 1982,respectively(FNRI, 1981; 1984). Behindthese nationalaggregatesarevariationsby region, rural and urban location,householdincome, andoccupationofhouseholdheads.Inadequaciesinmicronutrientintakeshavealso been revealed in the FNRI data. For example, in 1982 the percent

Table 3: TEN LEADING CAUSES OF MORTALITY RATE BY AGE GROUP, 1983 =,
Avitamino- __Diseases Tuber- Diseases ses and Nephritis,
Age Group Pneumo- of the cufosis, of the MaJignant Other Nutri- Acci- Nephroticnias Heart All Vascular Neoplasms Diarrheas Measles tionaf De- dents Syndrome and ._.
Forms Systems ficiencies Nephrosis
Under1 yr. 950.3 24.9 3.1 7.7 10.7 373.2 137.1 1572. 10.0 5.11 - 4 yrs. 279.3 6.7 2.8 2.2 4.5 83.4 96.3 34.2 8.1 4.0 _'5 - 9 yrs. 38.5 4.1 1.1 1.9 3.2 16.4 12.0 4.2 6.8 1.8 _"
10 - 14 yrs. 13.2 6.8 0.8 2.8 4.7 5.5 1.8 1.3 6.3 i.515 - 19- yrs. 8.7 10.9 17.9 4.1 4.0 2.4 0.3 0.7 8.1 2.0 ="20 - 24 yrs. 9.9 16.5 17.8 8.4 6.3 2.7 0.2 0.9 11.5 3.025 - 29 yrs. 11.7 21.6 28.6 11.4 9.6 2.3 0.09 1.1 12.1 4.130 - 34 yrs. 13.1 28.9 40.8 18.5 17.0 2.8 0.1 1.5 12.8 4.5 "_35 - 39 yrs. 14.3 38.3 59.2 28.7 29.0 3.3 0.04 1.8 12.6 6.7 R40 - 44 yrs. 20.7 60.0 90.2 46.9 50.7 4.0 0.2 2.6 14.4 8.8 p_45 - 49 yrs. 26.6 82.0 123.2 73.1 75.3 7.3 - 3,2 14,6 12.650 - 54 yrs. 38.2 120.2 174.2 122,5 114.6 10.7 - 4.6 17.0 17.655 -59 yrs. 57.9 169.6_ 219.2 174.4 148.7 13.7 - 8.7 15.8 27.060 - 64 yrs. 102.9 292.9 330.9 280.1 198.6 22.7 0.3 13.9 20.6 40.265 - 70 yrs. 132.2 427.7 394.9 423.5 245.8 28.0 0.4 21.6 23.4 64.370 yrs.and
above 530.1 1279.9 272.8 1097.3 354.2 73.6 3.1 108.2 42.7 150.4
SOURCE:PhilippineHealthStatistics,1983,HealthIntaffigenceService,Ministryof Health,as reportedby Cari_o(1986). ,,,4

8 Alejandro N. Herrin & Maricar Ginson Bautista
Table 4: INFANT MORTALITY: TEN LEADINGCAUSES, RATE (PER 1,000 LIVE BIRTHS)PHILIPPINES, 1980-1984 ANDFIVE-YEAR AVERAGE, 1975-1979
1975-1979
Causes Average 1980 1981 1982 1983 1984
Pneumonia 13.4 11.4 10.5 10.2 10.2 11.5
Respiratory Conditionsof Foetus and Newborn 2.6 5.5 5.3 6.1 6.2 5.3
Diarrhea 4.9 4.0 4.7 3.4 4.0 3.4
Congenital Anomalies 1.8 2.4 2.0 2.1 1.9 1.7
Avitaminoses & OtherNutritional Deficiencies 5.1 2.1 2.0 1.4 1.7 0.9
Birth Injury and DifficultLabor 0.9 1.5 1,5 1.1 1.5 0.4
Acute Bronchitis andBronchiolitis 1.5 1.0 1.0 0.7 1.1 -
Measles 1.0 1.0 1.3 1.2 0.7 1.5
Meningitis 0.7 0.6 0.5 0.5 - -
Dysentery, all forms 0.2 0.3 - - 0.6 0.04
Septicemia - 0.5 0.4 - -
Tetanus ..... 0.9
SOURCES:PhilippineHealthStatistics,Health IntelligenceService,Ministryof Health,1980-1984asreportedbyZablan(1986),andNEDA(1985).

Table 5: TEN LEADING CAUSES OF MORBIDITY, PHILIPPINES, 1978-1984 _:(Rate Per 100,000 Population) °
YEARCauses =
1978 1979 1980 1981 1982 1983 1984 ""
Bronchitis 455.6 471.3 427.3 507.1 552.2 577.8 1039.5 _Intluenza 488.7 406.0 419.9 445.5 445.5 447.9 783.3
Diarrheas 462.6 466.2 413.0 482.7 435.6 443.6 962.6
Pneumonias 248.8 272.2 242.7 248.6 108.3 237.5 337.6 _.
All Forms 260.5 233.6 232.4 235.8 206.2 179.2 268.0 _Tuberculosis,
Malaria 77.7 68.2 82.1 89.1 68.9 88.0 207.4 ._
Malignant Neoplasms 43.6 43.4 59.8 50.0 - 49.7 50.6Dysentery, All Forms 60.7 60.7 56.7 54.4 66.7 - - ==Measles 61.2 62.8 55.4 54.6 67.3 71.7 126.5
Whooping Cough 33.5 - 41.1 38.7 31.3 27.4 -
Infectious Hepatilis - 19,0 - - 16,5 17.6 28.3Accidents ....... 156.8
SOURCE: PhilippineHealthSta#stics,I978-t984.HealthIntelligenceService,Minisfryof Healthas reportedby Zabfan(1986)

Table 6: TEN LEADING CAUSES OF MORBIDITY BY REGION, 1983 o(Rate Per 100,000 Population)
RegionCauses
t ff ftf IV V Vf VII Vffi IX X Xf Xff NCR
Bronchitis 675.3 957.3 914.3 345.5 294.7 765.8 586.0 437.1 752.0 815.0 708.5 1344.6 693.9Diarrhea 531.6 867.0 804.4 305.6 296.3 489.4 445,6 537.4 923.9 575.1 370.8 1125.4 309.5Influenza 418.5 834.0 883.4 247.2 132.2 330,4 213.2 334,8 1167.6 422.2 528.3 1735.7 200.9Pneumonia 236.7 158.1 327.7 123.4 170.7 204.1 180.0 331,6 283.0 401.8 193.6 698.2 127.'ITuberculosis :_
AllForms 187.8 148.0 201.2 132.3 309.3 245.0 150.7 328.5 244.2 168.5 164.9 323.9 177.5 _"Measles 88.3 65.0 96.1 56.4 63.3 56.5 63.0 106.9 108.0 128.4 99.0 116.0 91.5 _"Dysentery, ._
AllForms 70.2 64.3 30.5 11.8 27.1 84.4 145.2 9.5.4 207.5 200.8 173.2 332.2 -Malignant
Neoplasms 43,4 27.9 49.7 42.2 26.0 54.2 57.6 28.5 34.2 82.4 45.2 40.5 • 81.4 _"Malaria 30.6 681.8 19,1 117.9 8.9 - - - 510.0 198.7 165.2 73.5 -WhoopingCough 29.7 28.9 21.2 25.5 25.7 27.6 10.3 95.8 73.1 45.2 36,3 78.4 -Infectious _"
Hepatitis ..... 20.7 9.7 - - - - - 23.4 "
Schistosomiasis ....... 42.1 ..... _.Diptheria ............ 17.1
H-Fever ............ 11.6
SOURCE: Ph#ippineHealthStatistics,HealthIntelligenceService,IL_'nisttyof Health, _

HealthImprovements:DeterminantsandConsequences 11
adequacyofintakesofiron,calcium,thiamine,riboflavin,niacinandascor-bic acidwere 91.5, 80.4, 71.8, 56.3, 119.7 and91.1, respectively.
A salientfeatureofthe nutritionproblemisthe nutritionalstatusof pre-schoolers.Surveydata from FNRI revealthatundemutdtion(lessthan 85percent of standardweight-for-height)among pre-schoolerswas 13.8percentin 1978 and9.5 percentin1982. Data fromthe PhilippineNutritionSurveillanceSystem (PNSS) cited by Florentino (1986) revealed thatundernutrition,similarlymeasured,was 13.3 percent in 1984 and 14.3percentin 1985. If the data are indeed comparablewiththe FNRI data, itappearsthattherehasbeenan increas_inundernutdtionratesamongpre-schoolersafter 1982, a findingthat is not inConsistentwith decliningincomes,increasingunderemploymentand risingpricesofbasiccommodi-ties,especiallyfood, duringthe period.
Summary
Philippine health problems have much In common with the healthproblems in the developing world. Respiratory,gastro-intestinaland otherinfectious diseases together with nutritional deficiency constitute majorcausesof death and of morbidity. Cardio-vascular and neoplasms, how-ever, are alsoimportantcausesof death and are expectedto become evenmore so. Facedwith tnesedisease patterns, the country isnow challengedto cope with highly differentiated majorcategodes of diseases in terms ofetiology and methods of control, and, will have to do this with severeresourceconstraints.
Policychoices can be facilitated by informationregarding economic,social, biological and environmental determinants of various health out-comes that can serveas basisfor assessingalternative health - promotingstrategies.On the other hand, there isalso a needfor empirical informationon the economicand socialimpacts of mortality and health improvementsto serve as basis for strengthening commitment to the allocation of re-sources toward health promotion and disease control.. The subsequentsectionsof this paper reviewthe state of knowledgeon both determinantsand consequences of health statuschange.
III. DETERMINANTS AND CONSEQUENCES OF HEALTHIMPROVEMENTS: CONCEPTUAL FRAMEWORK
Determinants
ALTERNATIVE PERSPECTIVES. In reviewinghealth-relatedfieldstudiesindevelopingcountdes,Mosley(1984) notesthatthese "arecardedout byeitherbiomedicalorsocialscientists,eachapproachingtheproblemsfrom

12 AlejandroN.Herrin& MaricarGinsonBautista
theirown disciplinaryperspectivewithvery littlerecognitionaccordedtobiosocialinterrelationships"(p.4). Biomedicalfieldstudiestypicallyattemptto identifycriticalriskfactorsassociatedwithspecificdiseasesthatmightbemodifiedby specificinterventionprograms.Thesestudies,however,havelittleto say aboutthe role of socioeconomicdeterminants.Socialsciencestudies,on the otherhand,typicallyattemptto relatehealthoutcomeswithvarioussocioeconomicprocesses.However,these studiesoften producevarious health outcomeslargely unspecifiedor untested because themechanismsthroughwhichtheseprocessesoperateareexaminedontheirown.Whileeachapproachmaycontributetoilluminatingspecificaspectsofthe determinationof healthoutcomes,a broaderperspectiveis neededtoanalyze biosocialinteractionsas a basisfor informingpublicpolicy.In anattemptto providesucha broaderperspective,Mosleyand Chen(1984)proposedan analyticalframeworkfor analyzingthe determinantsol childsurvivalthatincorporatesboththesocialandmedicalscienceperspectives.Thekeytotheiranalyticalframeworkistheidentificationofa setofproximatedeterminants,or intermediatevariables,that directlyinfluencethe riskofmorbidityand mortality.Social and economicdeterminantsare seen toaffecthealthoutcomesthroughtheirimpactontheseintermediatevariables.Schultz( 1984) adoptsa similarconceptualframework,andexplicitlycon-siderstheeconometricspecificationsneededtoobtainvalidstatisticaltestsof the interactionsbetweensocioeconomicdeterminants,proximatevari-ables andhealth outcomes.A simplifiedbutcomprehensiveframeworkisdescribedbelow.Thistakes accountof the above analyticalcontributions,andatthesame timehighlightstwootheraspects,namely:the dynamicsofindividual/householddecision making, and the impact of exogenouschanges,principallythoseresultingfrompublicpolicies/programsincludinghealth-promotingand disease controlpolicies/programs,on health out-comes.
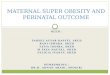
CONCEPTUAL FRAMEWORK. A simple framework for analyzing thedeterminantsof health outcomesand for organizingthe review of theliteraturecan bedescribedwiththe aidof Figure1. The basiccomponentsofthisframeworkarethe healthOutcomes,theproximatedeterminants,thesocioeconomicdeterminants,andthe exogenousshocks.Underlyingthisframeworkis a modelof individual/householddecisionmaking.
As mentionedearlier, health is a multi-dimensionalconcept.Whileattemptshavebeen madeto measurevariousaspectsof physical,mentaland socialwell-being,most of the researchso far undertakenuse thetraditionalindicatorsof healthoutcomes,i.e. mortality,morbidityandnutri-tional status.Attentionwill be focusedon the determinantsof mortality,morbidity,andnutritionalstatus,specificallyon infantsandyoungchildren.
AsconvenientlydescribedbyMosleyandChen(1984 ),baseduponacarefulreviewof biomedicalliterature,the proximatedeterminantscan be

PublicPoliciesandPrograms t !andOtherExogenousChanges
.............. -,_- ........... ._
Individual/Household Co unity I
i endowments environment 1
I li°-'l I i _Maternal Environmental Nulrierd Injury
factors contamination intake
,[ i i Il "L.......... ] i 1
Healthy Mal- Morlality
1_ nourished
Preventiveand Lcurativehealthcare r"
/
FIGURE1: CONCEPTUALFRAMEWORKFORANALYZINGTHEDETERMINANTSOF HEALTHOUTCOMES

14 AlejandroN.Herrin& Ma#carGinsonBautista
grouped into five major categories:(a) reproductivefactors: parity,birthinterval;(b) environmentalriskfactors:air, food/water/fingers,skin/soil/inanimateobjects,vectors;(c) nutrientintake:calories,protein,micronutrkents; (d) injury: a_idental, intentional;and (e) health care: preventivemeasures,medicaltreatment.The firstfourcategoriesofproximatedeter-minantsinfluencethe =rateofshiftofhealthyindividualstowardssickness,"i.e. morbidityrates,whilethe lastcategory influencesbothmorbidityrate(throughprevention)and the rate of recovery (throughtreatment). Ulti-mately, sicknesseither leads to complete recovery(healthystate) or togrowthfalteringorotherdisabilityamongsurvivors,and/or death.
Socioeconomicdeterminantscan beclassifiedintothree majorcate-godes: (a) individualendowments:unobservedbiologicalendowments,age, education,preference,beliefs,attitudes;(b) householdendowments:income/wealth,age-sex compositionand human capital of householdmembers;and (c) communityenvironment.The communityenvironmentincludesa varietyoffactors.Theseare(a) theecologicalsettingandnaturalresource endowments:climateand soil; (b) the structureof marketsandpricesforproductsandfactorsof production,includinglabor;(c) thesizeandstructureofthepopulation;(d)socialstructureandorganization;(e)physicalinfrastructures,andeconomicand socialservicesotherthanhealth;and(f)healthinfrastructureandservices.
Exogenouschanges includechanges arisingfrom externalshocksand from public policies and programs.Changes arising from externalshocksincludechangesinthepricesofexportandimportcommoditiesthataffect the livelihoodofa largeproportionof the population,thedevelopmentof new health technology,and, additionalhealthresourcesfrom interna-tionalorganizations.A majorsourceof shocks,however,isthe setofpublicpoliciesand programs,notableamongwhich are economicpoliciesandprogramsaffectingpricesof productsand factorsof production,the provi-sionof agriculturalandindustrialsupportservices,and publicexpenditureon physical infrastructuresuch as roads, irrigation,flood control,andelectrificationas wellas socialinfrastructuresand servicesinthe fieldofeducation,health,nutrition,environmentalsanitationand familyplanning.
Inthisframework,the individual/household,in anattemptto improveitswelfare, is assumedto make variouskindsof decisionssubjectto a setofopportunitiesandconstraintsdefinedby itsindividual/householdendow-mentsand by the communityenvironment.Exogenousshocksaffect thestructureof opportunitiesand constraintsfacing individual/householdseitherdirectlyby increasingindividual/householdendowments,orindirectlythrough the community,either by increasingcommunityresources andServicesavailableto individuals/householdsorby modifyingthe structureof economicincentives,i.e. pricesandwage rates.The individuals/house-holdsarethenexpectedtorespondtothesechangesina mannerperceivedtoimprove,orat leastpreventa deteriorationof, theirpresenteconomicand

HealthImprovements:DeterminantsandConsequences 15
socialwelfare includingtheir healthstatus.Dependinguponthe natureofemerging structureof opportunitiesand constraints,a "muitiphasicre-sponse"isexpectedfromtheseindividuals/householdsintermsofdecisionsregardingsavings/consumption,investmentinphysicalandhumancapital,time allocationand labor force participation,fertility,migration,diseaseavoidance and medical treatment. These decisions in turn affect theproximatedeterminantsand ultimatelythe health outcomestogetherwithothersocioeconomicoutcomes,e.g. incomes,employment,educationofchildren,etc.
HYPOTHESES: PROXIMATE DETERMINANTS. In developingcountrieswhereinfantand childmortalityare stillhigh,itisinterestingtosee themajorproximatedeterminantsof sucha situation.The reviewof the proximatedeterminantsof child survivalundertakenby Chen (1933) and selectedstudiesfoundin MosleyandChen ( 1984b ) are particularlyuseful.
Childsurvivaluptoage 5 isgenerallyinfluencedbythefive proximatedeterminantsshownin Figure 1. When viewed from the stand-pointofmothersandchildrenandviewedinteractively,thefive proximatedetermi-nants can be reclassifiedin terms of the followingfactors, The first ismaternal factors,includingage, parity,the intervalbetween births, andmaternal nutritionalstatus. These factors affect the mother's biologicalresourcesforprovidingadequatenutdtiontothefetusduringpregnancyandto the infantduringbreastfeeding.The second is nutritionalfactorswhichincludedietandfeedingvariables.The mother'sdietduringpregnancyandlactationinfluencesthe nutritionof the fetusand the child, respectively.Since breastmilk alone cannot provide complete nutritionbeyond 4-6months,continuationof breast-feedingand the timeliness,adequacy,andpattern of supplementationbecome importantuntilthe child is able toconsumea regulardiet. The thirdfactor is infectionswhichmay affect thechildbothduringpregnancyandearlychildhood.Maternalinfectionduringpregnancyis believedto contributeto low-birthweightand highneonatalmortality risk. During the first five years of life, the child inevitablywillexperience many infections,mainly respiratoryand gastrointestinalinnature, resultingfromexposureto varyingdegrees of environmentalcon-tamination. These infectionsare the major causes of infant and childmortality,andhavebeenknownto interactwithmalnutrition.Thelastfactorischildcare,whichincludestheavailabilityofchildhealthservicesandchildcare behaviorin responseto illness.
In reviewingthe evidence regardingthe role of these proximatedeterminants,the followingrelationshipsappearto be importantand rea-sonablygeneralizable(Chen 1983 ).
(1) Maternal factors: Childbearingat very young(under 17) andvery old(over35) agesenhancesmortalityrisks.Parityaffectschildhoodmortality:theriskassociatedwifhthefirstbirthis high,

16 AlejandroN. Herrin& MaricarGinsonBautista
decliningduringthesecondandthirdbirths,andusuallymono-tonicallyrisingthereafter.Highparityimpliesmorebirthsatolderagesandatcloserbirthintervals,the lamercan adverselyaffectthe indexchildbyprematurelyinterruptingbreastfeeding,reduc-ing food supplementationand compromisingchild care time.Closebirthintervalscouldalsocompromisematernalnutritionalstatusduringpregnancy,
(2) Nutritional factors: Maternal dietandnutritionalstatusduringpregnancyaffect fetal growthand birth weight;maternalfoodsupplementationduringpregnancyreducetheproportionof low:birth-weightinfantsandneo-natalmortality.Breastfeedingistheoptimal form of infant feeding:duringthe first 4-6 months itprovidesthe followinguniqueadvantages:nutrientadequacy,sterility,immunizationagainstinfections,antiallergenicproper-ties,psychologicalbonding,andlowcost.Fullybreastfedinfantstendto havelowermortalityratesthanbottle.fedinfants.Partofthisrelationshipisduetotheinteractionbetweenartificialfeedingand either environmentalcontamination or nutritionalintake:artificialformulaeare often mixedwith contaminatedwater incontaminatedbottles,introducingorallytransmittedinfections;moreoverthe formulae may be dilutedbecauseof prohibitivecost, thereby reducingthe childs'net nutrientintake.
(3) Infection and environmental contamination: Maternalinfec-tion (e.g. mycoplasmainfectionsof the genital=urinarytractamongpregnantwomen) is one cause of lowbirthweight andhighinfantmortality.Afterbirth,a childcannotavoidinfections,the most significantof which involvethe gastrointestinalandrespiratorytracts.The infectionrate anditsseverityculminatingin death is influencedbyexposureto communicablepathogen,the susceptibilityof the host(partly determinedby nutritionalstatus),and healthbehaviorin responseto illness.
(4) Child care factors: Manydeathsdue toinfectiousdiseasesandmalnutritionmaybeeitherprevented(e.g.immunization,sanita-tion, adequate feeding) or treated successfullywith curativeservices (e.g. oral rehydrationtherapy,anti-bioticsand nutri,tional rehabilitation).Childcare practicesthus assumeimpor-tanceindeterminingmortalityriskeitherin influencingexposuretoinfectionsandmalnutritionorininfluencingutilizationofhealthcare services.
(5) Injury: This includesbirth injury, physicalinjury,burns andpoisoning.Birth injuriescan be preventedby correctdeliveryproceduresandadequatehandlingof complicatedcases. Acci-dental injuriesare influencedby environmenta!risks, theseevents,however,aredifficultto determine.

HealthImprovements:DeterminantsandConsequences 17
(6) Interaction betweenproximatedeterminants: Theinteractionbetweenthe proximatedeterminantsisextremelycomplex,andas Chen (1983) observes:"is still inadequatelydocumented,poorlyunderstood,and probablyvariablecross-culturally"(p.176).
HYPOTHESES: SOCIOECONOMIC DETERMINANTS. The relationshipsbetweensocioeconomicfactorsand healthoutcomescan be examinedintermsofthe former'sinfluenceontheproximatedeterminantsorintermsofthe former'snet effecton healthoutcomes.
The major factorsoften hypothesizedto influenceboth proximatedeterminantsand health outcomesare (a) individual/householdendow-ments(wagerates,education,householdwealth/assetsorincome)and(b)communityenvironment(measuresof healthinfrastructuresand services,pricesofbasiccommoditiesincludinghealthservices,and indicatorsofthephysical environment).The specific hypotheses linkingsocioeconomicfactorsand proximatedeterminantsmay be describedas follows:
(1) Wage rate of household head and household wealth/assets- an increase in wage rate and householdnon-laborincomeincreasesthe demandfor children,for nutritiousfood,sanitaryfacilities(water, toilets,housing),and preventiveand curativehealthservices.
(2) Wage rate of the wife - an increaseinwage rate reducesthedemandforchildrenandthetimeallocatedtochildcareandothertime-intensivehealth-relatedhomeactivities.
(3) Mother's education - highereducationincreasesproductivityorefficiencyin the productionof health inputs,i.e. nutritiousfood,childcare, use of healthcare services,and is relatedto prefer-encesfor smallfamilysize.
(4) Prices of health services - highermonetaryandtimecostsofhealthcare servicesreducedemandfor suchservices.
(5) Prices of other commoditlea - higher prices of food andsanitationfacilitiesreducedemand for suchgoods.
(6) Environment - adversephysicalcharacteristicsincreasesex-posureto the riskofinfectionandinfestation,andaffecttimecostof healthcare services.
The hypothesisconoemingthenet effectof socioeconomicfactorsonhealthoutcomesmaybe describedas follows:
(1) Wage rateof household head and household wealth/assets- an increase in wage rate and non-laborincome increasesinfant/childsurvivalrates.
(2) Wage rate of wife - the effectof an increasein wage rateon

18 AlejandroIV.Herrin& Mar_carGinsonBautista
infant/childsurvivalrateis ambiguous.Itcouldincreasesurvivalratethroughitseffecton income,oritcould reducesurvivalratethroughitseffecton childcare. Takingintoaccountintrahouse-holdsubstitution,the net effectwouldtend to be positive.
(3) Mother's education -thehighertheeducationofthemother,thehigherthe survivalrateof children.
(4) Prices of commodities Including health services -the higherprices,the lowerthe survivalrateof infant/children,
(5) Environment - adverse environmentalconditions increasesinfant/childmortality.
The abovehypothesesapplyaswellto morbidityratesandnutritionalstatusof children.
Consequences
Shownin FigureI as brokenlines,healthoutcomesaffectindividual,householdandcommunitywelfare.Butwhatare themechanismsinvolvedbywhichdifferenthealthoutcomesaffectwelfare?AndreanoandHelminiak(1986) recentlysuggesteda typologyof disease impacts. Althoughthestudyfocusedontropicaldiseases,the typologyis readilygeneralizableforotherdiseasesandotherhealthoutcomes.Thesocialandeconomicimpactofdiseaseandotherhealthoutcomesmaybecategorizedasfollows:
HEALTH CONSUMPTION EFFECTS - the mostapparentef-fects of diseaseare thosethat diminishthe enjoyment(or consump-tion)of goodhealth amongaffected persons.This categoryincludesthe direct pain and sufferingassociatedwithdisease/infection,theshortenedenjoymentof life resultingfrom prematuremortality,thegriefof personsaffectedbyeitherphysicalincapacityor the stigmaofdisease,griefrelatedtoimpendingearlymortality,andgriefofrelativesand friendsof thoseaffectedby a disease.
SOCIAL INTERACTION AND LEISURE EFFECTS - includesstressesand constraintsimposedon interactionsbetweeninfectedpersonsand other membersof their householdsand communities;leisuretime and recreationmay alsobe reduced.
SHORT-TERM PRODUCTION EFFECTS - these includebothmarket and non-marketimpacts.Amongthe formerare effects onlaboras a factorof productionwhichincludeanyof the following:(a)the temporary loss of labor days due to inabilityto work; (b) thepermanentlossof laborsupplydaysdueto mortality;and (c) reduc-tionsin the efficiencyof labordayssupplieddue to debility.On theotherhand,non-marketproductioneffectsarethoseaffectingproduc-tion of commoditiesfor homeconsumptionand householdservicessuchas childcare, productionof nutritiousmeals,etc.

HealthImprovements:DeterminantsandConsequences 19
•LONG -TERM PRODUCTION/CONSUMPTION EFFECTS °theseinclude(a)demographiceffects(reducedmortalityandpopula-tiongrowth)on consumption,laborsupplyandcapitalformation;(b)effectson landand laborsupply,for example,diseaseswhichhaveespeciallyhigh transmissionpotential in certain land areas mayreducethe supplyof productiveland, because the settlementandemploymentoflandisdiscouraged;and (c)effectsofbetterhealthandnutritionon intellectualdevelopment,motivation,better academicperformance,innovativebehaviorand altitudetowardsrisk.
IV. DETERMINANTS AND CONSEQUENCESOF HEALTH IMPROVEMENTS: EVIDENCE
Proximate Determinants
Studieson the role of proximatedeterminantson specifichealthoutcomesbased on nationalor large samplesare hard to come by. Theavailablestudiesincludemultivariateanalysisof the determinantsof childmortality(Martin etaL 1983), morbidityamonghouseholdmembers(Layo1977), and nutritionalstatusof pre-schoolers(Battad 1978,Popkin 1980),andbivariateanalysisoftherelationshipbetweenbreastfeedingandmater-nal and child health care factors,and child survival(Zablan 1986 ). Inadditionto theabovestudies,we examineddatafromthe Ministryof Health,National Health Surveys of 1978 and 1981 as well as data from othersourcesconcerningsuchfactorsas maternal healthcare, breastfeeding,health services availability,and environmentalcontaminationvariables(Herrin 1985).
MULTIVARIATE ANALYSIS. Usingdata from the 1978 Republicof thePhilippinesSurvey(RPFS), Martin,el al.(1983) assessedthe socio-eco-nomicandproximateco-variatesof childmortality.Theproximatedetermi:nantsofinterestarethemother'sageatbirthoftheChild,thebirthorder,andtwo environmentalcontaminationvariables.The results revealthat childmortalityrisk(conditionalprobabilityof dyingat a givenage,giventhatonehassurvivedtothatage) is significantlyhigheramongchildrenborn amongmothersage lessthan20 yearsthanamongmothersage 20-34 or 35 andover.Betweenbirths among mothersintheages20-34 yearsand 35 yearsandover,however,themortalityriskisonlyslightlyhigherin.thelatterthanin the former althougha much higher mortality risk is expected amongchildrenbornofoldermothers.The resultsalsoshowthatchildmortalityriskis lowerwith the firstbirth, higherwith the second and third births, andhighestwiththefourthand higherorderbirths,althougha muchhigherchildmortalityriskis expectedwiththefirstbirth thanwiththe secondandthird

20 AlejandroN, Herrin& MancarGinspnBautista
births.Thusthe findingsof Martin,et al.( 1983) partiallysupportthe com-monly expectedrelationshipsbetweenchild mortalityand age and birthorder,respectively.
Martin,et al. (1983)also foundthat the qualityof sanitaryfacilities(toilet,facilityinsidethe housevs.outsidethe houseor none)is negativelyrelatedto childmortalityrisk.The type of watersupply(pipe/artesianwell/other), however, is not significantlyrelatedto child mortalitydsk. Theseresults for environmentalcontaminationvariables must be interpretedcarefully,however,asthe authorscaution.Bothvariablesare measuredatthe time of the surveyandnotat the time thebirthsoccurred.
Layo(1977) usinghouseholdsurveydata from a randomlyselectednational sample of 3,000 householdscollected under the Population,Resources,EnvironmentandthePhilippineFuture(PREPF)project,exam-ined the relationshipsbetween the number of reported illness in thehouseholdduring the 30 claysprior to interviewdate to a numberofsocioeconomicandproximatevariables.Theproximatevariablesofinterestarethe qualityof drainage,ventilationandwater supply.The resultsshowthat qualityof waterandqualityof ventilationare importantfactorsintotalillness.These factors,togetherwithqualityofdrainageare alsofoundto besignificantfactorsinchronicillnesses.The resultsaregenerallyconsistentwith expectations.
Inexaminingthedeterminantsof childnutritionalstatusmeasuredbythe child'spercentageof standardweightina Lagunasampleof 578 pre-schoolers,Battad(1978) testedtheeffectofproximatedeterminantsalongwith severalsocio-economicfactors.The proximatedeterminantsare thenutritionalstatusof the mother(mother'spercentageof weightforheight),andthe numberof childrenage 0-6 years.The resultsof the multivariateanalysisshowthatmothers'nutritionalstatushada positiveeffecton childnutritionalstatusamongchildrenaged6-23 months,butnosignificanteffectamongolderchildren.Moreoverthe numberof childrenage 0-6 yearshada strongnegativeeffect amongchildrenaged 24 monthsandover, butthestrongesteffectwas among childrenage 24-47 months.The effect onchildrenlessthan 2 yearsof age was not significant.
In interpretingthe results,Battadnotesthat the significanteffectofmothers'nutritionalstatuson the nutritionalstatusof youngerchildrenbutnotonolderchildrenreflectsthe effectof mothers'nutritionalstatusonthefetusandthe children'sbirthweight,as wellas subsequentbreastteedingeffects.Ontheother,thestrongernegativeeffectofthenumberofpreschoolchildrenon the nutritionalstatusof children2-4 yearsoldas againstthe4-6 yearsoldmeansthatthe lattergroup"are betterable to copewithshiftsintheirmother'sattention."Moreover,theinsignificanteffectofchildrenage0-6 yearsonthe nutritionalstatusof children6-23 monthsis interpretedtomean that "Lagunamothersconcentratemore attentionon the youngerpreschoolersthanolderones."

HealthImprovements:DeterminantsandConsequences 21
Inanotherstudy,Popkin(1980)examinedtheproximatedeterminantsof the nutritionalstatus (weight-for-ageand height-for-agemeasures)ofpreschoolchildreninLaguna.Nutritionalstatusismodelledto bea functionof childcare time, dietaryintake,mother'snutritionalstatusandqualilyofwater supply.A problemwith the study is the limited sample (n = 68)availableforanalysisaftertakingintoaocountthevariousdatarequirementsto estimatethemodel.The resultsshowthatvery fewofthecoefficientsarestatisticallysignificantand theamountof variationexplainedbytheregres-sionislow. inspiteofthis,itis interestingto notethat amongthe significantcoefficients,therelationshipsseemtobean increaseinpercapitachildcaretime mothers with increases in the child's nutritionalstatus, whereasincreasesinper capitachild caretime of oldersiblingsreducesthe child'snutritionalstatus. This suggeststhat a substitutionof "higher quality"mother'schildcare timefor =lowerquality"oldersibling'schildcould haveunfavorableeffectson child'snutritionalstatus.
BIVARIATEANALYSIS.Anotherproximatefactorthat affectschild healthand survivaliswhetheror notthe childisbreastfedduringinfancy.Recentwork relatingbreastfeedingand infantsurvivalhas been done by Zablan( 1985,as reported in Zablan 1986). Basedondata fromthe 1983 NationalDemographicSurvey (NDS)), Zablan found that the proportionof infantswhosurvivedupto the firstyear was higheramongbreastfedthan amongnon-breastfedinfants: 0.864 vs. 0.583. For all childrenborn betweenJanuary 1978 andthe 1983 NDS, higherinfantandchildsurvivalratesarealso foundamong breastfedthan non*breasffedchildrenafter controllingseparately for source of water supply and presence of sanitary toiletfacilities.Forthe lastchildbom betweenJanuary1978 and the 1983 NDS,higherchildsurvivalratesare foundamong breasffedthan non-breastfedchildrenafter controllingfor prenatalcare, place of deliveryand deliveryattendant.Several importantinteractionscan alsobe notedfromthedata.Theseare: (a) highestchildsurvivalrate isfoundamong breastfedchildrenand wherewater supplysourceis pipedwater,whilelowestsurvivalrate isfound among non-breasffedchildrenand where water supplysource issurfacewater:0.960vs.0.793; (b)highestchildsurvivalrateisfoundamongbreastfedchildrenandwherehouseholdhassanitarytoiletthanamongnon-breastfedchildrenand where householdhas no sanitarytoilet:0.961 vs.0.783; (c) for the last child, highestchild survivalrate is found amongbreastfedchildrenwho were immunizedthan childrenwho were neitherbreastfednorimmunized:0.985 vs.0.843; and(d)forthe lastchild,highestsurvival rate is observedamongbreastfedchildrenandwherethe motherhadprenatalcare and lowestwhen neitherwas the case:0.978 vs.0.873.
TakingadvantageofZablan'sbasictabulations,onecanexaminethebivariaterelationshipsbetween child survivalof the last childbornduring1978-1983 and several maternaland child health practices. Analysis

22 AlejandroN.Herrin& MancarGinson8autista
suggeststhat childsurvivalratestendto be higheramongchildrenwhosemothershad some prenatalcare, who were deliveredin hospital/clinic,whose birthwas attendedby a doctoror trainedmidwife,and who hadreceivedimmunizationwithinthe first6 monthsof life,thanamongchildrenwho had neitherof thesecharacteristics.
The above resultstogetherwiththoseon breastfeedingprovidethemostrecent nationalevidenceon the roleof proximatedeterminantsandtheir interactionin affectingchild survival. The bivadate nature of theanalysis,however,precludeassessmentofthe partialeffect of a particularproximatedeterminanton childsurvivalholdingother variablesconstant.Furtheranalysisof the data usingmultivariatetechniquesisclearlycalledfor.
INFERENCES FROM BASICINFORMATION.Howmuchprogresscanbeachieved in improvingchild health and survival may be inferred fromavailablenationalinformationonspecificproximatedeterminants.Someoftheseinformationis examinedhere (Herrin 1985).
Prenatalcare is associatedwith higherchildsurvival ratesas wasnotedearlier.Thisrelationshipisexpectedtooperatethroughproperadvice
• on maternal nutrientsupplementationand dietduringpregnancy,timely-medicalinterventionfor possiblematernalinfection,andproperadviceonchildfeeding, all of which couldaffect birth-weightsand child nutritionalstatus.Thusonefactorthatcouldsignificantlyaffectchildhealthandsurvivalin the Philippinesmay be the qualityandtimelinessof prenatalcare thatpregnantwomen obtain.Data from the MOH, NationalHealth Survey in1978 shownin Table 7 revealthat 65 percentof pregnantwomen obtainprenatalcareoradvicefromnon-professionalhealthpractitioners,i.e.hilots,herbolariosand others.The qualityof prenatalcare obtainedfromthesepractitionersmaybeexpectedtobe lowerthanthatwhichcouldbeobtainedfrom professionals.Regardingthe timelinessof prenatalcare, the samedatashowthat39 percentofwomenwentforprenatalcare/adviceduringthefirstorsecondtrimester,while61 percentsoughtorobtainedprenatalcare/adviceonlyduringthe thirdtrimester,andof the latter,85 percentsoughtnon-professionalhealthpractitioners.
In 1980, 3.3 percentof totatreportedinfantdeathswere due to birthinjuriesanddifficultlabor.A largepartof thesedeathscouldprobablyhavebeenavoidedbyproperdeliveryproceduresandadequateemergencycare.DatashownfromMOH inTable8 revealthathalf(53 percent)oftotalbirthsforthe period1979-1981weredeliveredby non-professionalhealthatten-dants,i.e. hilots,herbolarios,relativesandothers.The popularityof hilotswasattributedbyrespondentsmainlyintermsofthe former'saccessibility.Fiftypercentof respondentsmentioned=nearestthe house"as the mainreasonfor seekinghilots,whileanother11 percentmentioned"trustandconfidence."Thusitappearsthatthe popularityof hilotsis partlyduetothe

Health Improvements: Determinants and Consequences 23
Table 7: PERCENTAGE DISTRIBUTION OFRESPONDENTS CONSULTING HEALTH WORKERSFOR ANTE-NATAL CARE BYFIRST REFERENCE, 1978°
Trimester of Pregnancy
Health Worker Percent First Second Third
Physician 14.7 42.9 26.9 3.0
Nurse 1.6 2.9 3.3 0.6
Midwife 18.8 30.0 43.7 6.2
Hilot 11.9 20.1 24.1 5.1
Herbolario, Mother/Mother-in-law, etc. 53.0 4.0 2.0 85.1
Total Percent 100.0 100.0 100.0 100.0
Total Respondents 6,924,497 1,043,733 1,657,365 4,223,399
* Datareferto lastpregnancy.SOURCE: Ministryof Health,NationalHealthSurvey,1978.(Table20).
Table 8: DISTRIBUTION OF ATTENDANCE AT BIRTHBY CATEGORY OF ATTENDANT, 1978 AND 1981
Birth Attendant 1978a 1981b
Physician 9.0 17.6
Nurse 0.8 2.2
Midwife 11_9 27.0
Hilot 26.3 45.5
Relative and Others 52.0 7.7
Total Number of Births 6,924,492 3,860.638
° Datareferto birthof lastchild.Datareferto birthduringpast threeyears 1979-1981.
SOURCE: Ministryof Health,NationalHealthSurvey,1978andNationalHealthSurvey,1981.

24 Alejandro N. Herrin & Maricar Ginson Bautista
difficult access of a large number of pregnant women to professionaldelivery attendants.
Another proximate factor that affects infant/child health and survival iswhether or not the child was breastfed during infancy. Table 9 presentssurvey data on breastfeeding prevalence and duration in the Philippinesbased on national demographic surveys. The data reveal that 85 percent ofchildren born three years prior to the 1978 RPFS were breastfed. Compa-rable data for Thailand, Republic of Korea, and Indonesia show thatbreastfeeding prevalence rates inthese countries is 90 percent or above. Of10 countries where comparable data were available at around 1978, the
Table 9: TRENDS IN BREASTFEEDING PREVALENCEAND DURATION, PHILIPPINES, 1973-1983
Source and Nature Percent DurationYear of Data Breasffed Mean Trimean n
(mos.) c (mos.) d
1973 N DS (last child)a 86.8 - 12.3 7,190
1978 RPFS (All children bornthree years beforesurvey date, 1978b 84.6 12.6 11.4 7,780
(9,531)e
1983 NDS (All children bornbetween 01/78 and
12/82 83.1 10.4 9.6 11,846(9,531)"
NDS (All children bornbetween 01/78 and
07/83 83.2 11.2 9,6 12,865(10,677) •
• Na_onalDemographicSurvey.
bRepublicof thePhilippinesFertilitySurvey.
Adthmeticmeanbasedonreporteddura_bn.
" Locationalaveragecomputedas: Tdmean= (T,_+ZT, + T_)4• Samplesizesfor dataonduration.
SOURCE:Zablan(1985),TablesI and2.

HealthImprovements:DeterminantsandConsequences 25
Philippinesranked second lowest in both breastfeedingpractice andbreastfeedingduration(Zab/an, 1985).
The data in Table 10 also suggestthat in 1978 and 1983, higherbreastfeedingprevalenceratestendtobeassociatedwithyoungermothers,rural residenceand lower mother's education.Longerdurationis alsoassociatedwith ruralresidenceand lowereducationalstatusof mothers.However,youngermotherstendtobreastledtheirinfantsatshorterdurationthan older women. Comparingthe data between 1978 and 1983, thereappearsto be a slightdeclineinoverallbreastfeedingpracticeand inthemeandurationofbreast/eeding.Theoveralldeclineinbreasffeedingpreva-lenceratesisreflectedindeclinesinallage categories,among ruralwomen,among other areas outsideMetro Manila, and amongwomen of lowereducationalstatus.Breastfeedingprevalencerates, however,appear toincrease among urban women, especiallyin Metro Manila and amongwomenwithhighschoolor highereducation.Withrespectto duration,thisappears to decline acrossvarious categoriesof women except amongwomen in urbanareas, in MetroManila, and'with highereducation(highschoolormore). Insum,thereappearstobea decliningtrend inbreastfeed-ingpracticeanddurationof breastfeedingamongsub-groupsof the popu-lationwhere breasffeedingis most likelyto have an importanteffectoninfant/childsurvival.Moreover,effortstoencouragebreastfeedingappearsto be more effectiveamongurbanand highlyeducatedwomen.
Childhealthandsurvivalare alsoassociatedwiththe availabilityanduse of healthservices.Dataon these (measuredin termsof distancetonearesthealthfacilities)fromtheMOH,NationalHealthSurveyfor1978and1981 donotinspiremuchconfidenceas totheirreliability.The 1981 surveydata for example,showlarge proportionsof householdsunderthe catego-ries"unaware/notconcerned"or"notstated",foreachtypeof healthfacility,whichare not reflectedin the 1978 survey.The data, shownin Table 11however,suggestthat a large proportionof householdsdo nothave easyphysicalaccess to specific health facilities. This can easily act as aconstraintto theuse of suchfacilities.
Finally,childhealthand survivalare associatedwithenvironmentalcontaminationvariables.Datafromthecensusrevealthat76 percentoftotalhouseholdsin1980haveaccessto safewatersupply,an improvementfrom61 percentin 1970 and 49 percentin 1960. However,only 49 percentofhouseholdshavesanitarytoiletsin 1980. Nonetheless,this is an improve-mentfrom 23 percentin 1970 and 8 percentin 1960.
Whileitiseasytosaythatfurtherprogresscanbeachievedinreducinginfant/childmortalityand morbidityby improvingthe levelsof the variousproximatedeterminants,itisnotclearwhichof thesefactorsshouldbegivenprioritygivenscarceresources.Policychoicesneedto beguided,ontheonehand, byknowledgeregardingthe relativeeffectof eachof these variableson overall healthand mortality,and on the otherhand, bythe knowledge

26 Alejandro IV. Herrin & Maricar Ginson Bautista
Table 10: TRENDS IN BREASTFEEDING PREVALENCEAND DURATION BY SELECTED CHARACTERISTICS,PHILIPPINES, 1978 AND 1983(FOR CHILDREN BORN 2 YEARS BEFORETHE 1978 RPFS, AND FOR CHILDREN BORNBETWEEN JANUARY '78 AND DECEMBER '82REPORTED IN THE 1983 NDS)
% Ever-Breasffed" Mean Duration (mos.)"Characteristics
1978 1983 197,P 1983"
ALL BIRTHS 84.6 83.1 12.6 11,3
1, Current Age of Mother
15-24 87.8 85.3 11.4 10.425-34 85.4 83.3 12.6 10.935:49 80.1 81.3 13.5 12.7
2. Residence
Urban 72.2 73.8 9.0 9.7Rural 89.1 87.8 14.4 12.0
3. Region
Metro Manila 65.0 67.9 6.6 7.8Other Luzon 85.4 84.1 13.3 11.4Visayas 89.1 87.9 15.0 12.9Mindanao 86.6 83,9 12.2 10.8
4. Mother's Education
No Schooling 93.3 90.8 17.0 12.5Primary 92.3 89.4 15,9 12.4Intermediate 87.4 87,7 13.6 12.0
High School 64.2 67,5 10.0 10.6College 1+ 64.2 67.5 7.3 7,9
• Excludes cases with no information on breastfeeding practice, on the selectedcharacteristics or on both.
b Prevalence/incidencemean based onproportions still breastfeeding.
Arithmetic mean based on reported duration of breasffeeding for children who wereweaned, had died. and those still breastfeeding dudng the 1983 NOS.
SOURCE: Zablan (1985, Tables4 and5).

HealthImprovements:DeterminantsandConsequences 27
Table 11: PERCENTAGEDISTRIBUTION OF HOUSEHOLDSBY DISTANCE IN KILOMETERS TO VARIOUSHEALTH FACILITIES NEAREST TO THEHOUSEHOLD, 1978 AND 1981
Distance
Type of Health Not Aware/Facility 10kms. Not Concerned
< 3 kms. 3-9 kms, and over Not Stated
1978
Govemmenthospital 25.1 27.2 47.7 -
Privatehospital/clinic 41.2 29.7 29.0 -
RHU/PC 46.5 34.3 16.7 2.5
BarangayHealthStation 67.2 27.6 5.2 -
1981
Governmenthospital 21.3 18.6 28.6 31.5
Privatehospital/clinic 32.8 18.1 14.6 34.5
RHU/PC 40.4 24.7 8.2 26.7
BarangayHealth Station 42.3 14.3 1.8 41.6
SOURCE: MOH, National Health Survey. 1978 and 1981.
regardingthe behavioraldeterminantsofthese proximatevariables.Infor-mationregardingthe first, is yet to be firmedup by more carefulstudiesbasedon reasonablygeneralizablestudypopulations.Informationregard-ingthe secondisthe subjectof the nextsub-section.
Socioeconomic Determinants
The relationshipsbetween socioeconomicfactors and health out-comes can be empiricallyexamined using two possible approaches,namely,(a)singleequationmethodswherebymeasuresof healthoutcomesand measures of proximatedeterminantsare jointly determined by acommonsetof exogenoussocioeconomicfactors;and(b)structuralequa-

28 AlejandroN.Herrin& MaricarGinsonBautista
tionmethodswhereby socioeconomicfactorsnotsystematicallycorrelatedwith biological endowments or preferences influences proximate determi-nants, while health outcomes are influenced by endogenously determinedproximate determinants (Schultz 1984 ). Much of the literature on thesocioeconomic determinants of health outcomes adopt neither of theseapproaches. Instead,the common approaches employed are (a) to directlyreÁat'ehealth outcomes with socioeconomic determinants or (b) to relatehealth outcomes with both socioeconomic and non-endogenously deter-mined proximate variables. The latterapproach is considered methodologi-cally incorrect (Schultz 1984).
SOCIOECONOMIC DETERMINANTS OF PROXIMATE VARIABLES.Several multivariate analysisof the determinants of dietary/nutrient intake,breastfeeding andchild care have been undertaken using survey data fromLaguna collected in 1974through 1977 (see Evenson 1978for descriptionof survey). These studies include those of Gonzalo and Evenson (1978),Valenzuela ( 1978), Popkin ( 1978; 1980), and King and Evenson ( 1980).Studies on the demand for health care and health service utilization is thesubject of a separate review by Ching (1986), and hence will not be dealtwith in this paper; so also with studies on fertility since these have beenreviewed elsewhere (Herrin 1980).
Gonzalo and Evenson (1978), in a studyof 573 Laguna households,found that the per capital householddietary intake of calories, protein andVitamin A, respectively, aswell as per capital householdfood expendituresvaried positively with per capita household income (exclusive of wife'scontribution) and household wealth, and negatively with household size.These results are as expected. The effects of mother's education andworkstatus, however, differed by income level. At high levels of income, themother's laborforce participationincreases per capita intake of calories butreduces the per capita intake of Vitamin A. At low levels of income, themother's laborforce participation reduces the household's per capita intakeof calories. On the other hand, at high levels of income, an increase inmother's schooling reduces the household's per capita intakeof calories. Atlow levels of income, however, an increase in mother's schoolingtends toincrease per capita intake of the various nutrients but each relationship isinsignificant. It is difficult to interpret these results unambiguously. Themother's laborforce participation ( the mother'swage rate might have beenthe proper variable to use) may be capturing both the income effect andsubstitution effects at high levels of income, and the substitution effect (i.e.market work takes mother'stime away from home production) mainly at lowlevels of income. Mother's schooling at high levels of income may berepresenting less tasteor preference for home production.
Valenzuela ( 1978 ) usinga sampleof 543household members repre-senting 97 households in the Laguna case study, related individual dietary

HealthImprovements:DeterminantsandConsequences 29
intakemeasuredas a percentageof recommendeddailyallowance(RDA)of calories,protein, VitaminA and VitaminC, respectively,as well as anoveralldiet rating,witha set of socioeconomicdeterminants.Inadditiontoage and sex, these'determinantsincludefamilysize, mother'seducation,timespentinfoodpreparation,percapitafoodexpenditure,percentmone-tary incomecontributionof householdmember,and employmentstatusofthe mother.The resultsfor eachnutrientindicatethatincreasedfamilysizereducesnutrientintakeadequacy,particularlysignificantfor caloriesandVitaminA. An increasein mother'schooling(reflectingskills)significantlyincreasesnutrientintakeadequacyof caloriesbut has nosignificanteffecton others nutrients.The time spent in food preparationsignificantlyin-creases nutrientintakeadequacyof calories, proteinand Vitamin A butdecreasesintakeadequacyof VitaminC. Thisresultis difficultto interpret.Moretimeinfoodpreparationmaymeangreaterproductionofnutrients.Onthe other hand,morenutritiousmeals maytake moretime to prepare.Anincreaseinfooclexpenditures(reflectingincome)increasesnutrientintakeadequacyofbothcaloriesandproteinbuthasnosignificanteffectonVitaminA andVitaminC.The laborforceparticipationofthemother(partlyreflectingincome) increases nutrient intake adequacyof calories and vitaminA.Finally,the income contributionof the householdmember is generallypositivelyrelatedto nutrientintakeadequacy,althoughitis significantonlyforVitaminA. Vale_n_zuelaconsideredthisresultasproviding=supportforthehypothesis-thatfamilies do take earning opportunitiesinto account indistril_Jtingfoodamongmembers"(p. 175).
Withrespectto anoveralldiet rating(meannutrientintakeexpressedasapercentageofRDAdividedbythenumberofnutrientsx 100),theresultsindicatethat an increase in diet rating is positivelyrelatedto mother'seducation,mother'slaborforceparticipation,per capitafoodexpendituresandfoodpreparationtime,andnegativelyrelatedtofamilysize.Thevariableindicatingthe income contributionof the member,while positive,is notsignificant.
Popkin(1980), usingdatafromthe Lagunasurveyon 99 householdswhichyieldeda totalof 70 preschoolers,examinedthe socioeconomicanddemographicdeterminantsoftheiraveragedailycalorieandproteinintake.The independentvariablesincludethe mother'sage, education,and laborforceparticipation,percapitaincomeofotherhouseholdmembers,electric-ityinthe home,numberof childrenindifferentage and sexcategories,andnumberof otherpersonslivinginthe household.The resultsindicatethatmother'sage, education,andlaborforceparticipationwhichmaybe takento represent experience, skill and additionalincome, respectively,arepositivelyrelatedto the preschooler'saverage calorie intake, but onlymother'sage is positivelyrelatedto the preschooler'saverage proteinintake.The presenceof infantsinthe householdreducesthepreschooler'saverageintakeofcaloriesandprotein,respectively,perhapsindicatingthat

30 AlejandroN.Herrin& MaricarGinsonBautista
mother'sattentiontendsto beconcentratedon theinfantattheexpense ofother preschoolers.The numberof boys aged 7-15 years increasesthepreschoolerscalorieand proteinintake,respectively,whilethe numberofgirlsaged 7-12 years hasa positiveeffectonlyon averageproteinintake.Theseolderchildrenare expectedto supplementmother'stimeinthe careand feeding of preschoolers.The numberof other personslivingin thehouseholdhasa negativeeffectonboththecalorieintakeandpmt_inintakeof preschoolers.Givenhouseholdincome,it appearsthat the presenceofotherpersonstendsto reducefoodavailableto preschoolers.
In the same study, Popkinexaminedthe determinantsof childcaretime (hoursper week)andotheractivities,basedon a total sampleof 571mothers.Amongthe significantresultsarethefollowing.Mother'schildcaretime increaseswiththe presenceof infantsinthe homeat the expenseofleisure and market production.The presenceof other preschoolersin-creasesbothchildcare timeandhomeproductiontime andreducesleisuretime. The presenceof otherpersonsinthe householdincreasesmother'schildcare time but reduces her.homeproductiontime. Apparentlyothermemberssubstitutefor mother'shomeproductiontime thus allowingthemothertodevotemoretimetochildcare.Theothervariablesincludedintheanalysis,i.e. education,mother'sworkparticipation,per capitaincome ofhouseholdmembersotherthanthemother,andtheelectricityvariable,werenot significant. ......
Popkinalsoexaminestheeffect of mother'slabor-f0rceparticipationonintrahouseholdtimeallocation.Theresultsshowthatmother'slaboi;forceparticipationdoes not significantlyaffect childcare time but significantlyreducesher own leisuretime. Mother'slaborforceparticipation,however,increaseschildcare time of oldersiblings.
In anotherstudyusingthe Laguna surveydata on 99 householdswhichyielded314 infants,Popkin(1978)examinedthe socioeconomicanddemographicdeterminantsof breastteeding.The resultsof regressionanalysisfor the total sampleindicatethe following:Higherbreastteedingparticipationis positivelyrelatedto mother'sbeliefthat breastmilkis best,the numberof siblingsage 1-6 years,andto some extent,the numberofotherpersonsinthehousehold.Increasesinthe predictedwage rateofthemotherin rich householdsreducebreastfeedingparticipation,but is notsignificantin poorhouseholds.The numberof girlsaged 13-15 years isnegativelyrelatedto breastfeedingparticipationamongwomen in poorhouseholds,but is not significantinrichhouseholds.
Withrespecttothedurationofbreastfeedingthebeliefthatbreastmilkis best and the presenceof preschoolerchildrenincreasesduration.Anincreaseinthe numberofgirlsaged13-15 yearswhocansubstituteforchildcare reducesdurationof breastfeedingin poor households,but is not asignificantfactor inrichhouseholds.
Othervariableshypothesizedto influencebreastfeedingparticipation

HealthImprovements:Detormin_tsandConsequences 31
and duration such as income (father's wage rate and income of otherhousehold members)andthe nutritionalstatusofthe motherwerefoundtobe insignificant.
A moregeneral studyof the determinantsof time allocationamongLaguna householdswas undertakenby King and Evenson(1980). Timeallocation(obtainedbydirectobservationin97 households)of thewifeandhusbandwas distinguishedbetweenmarkettime, leisuretime and homeproductiontime,the latterincludeschildcare time (feedingand caringforchildren),foodpreparationtimeandotherhomeactivities.The resultswithrespectto mother'stime revealthefollowing.Anincreaseinwife'swageratedoes not significantlyreduceher hometime but an increasein husband'smarketwage does. Homecapital increaseshome time. The presenceof
young childrenage 0-6 years, butespeciallyinfants,increaseshometimeof the mother. The numberof older children in the household has nosignificanteffect on hometime.An increasein wife'seducation however,reducesherhometimein favorof markettime.Controllingforherwagerate,educationrepresentswife'spreferencesformarketworkoverhome produc-tion.
Summingup,theabovestudiesindicatethatthe proximatevariables(dietaryintake,childcare andbreastfeeding)are significantlyinfluencedbysocioeconomicanddemographicfactors.Amongthe mereimportantdeter-minantsare incomeand mother'seducationfor dietaryintake and demo-graphicvariableson childcare and breastfeeding.
SOCIOECONOMIC DETERMINANTS OF HEALTH OUTCOMES. Avail-able studiesrelatingsocioeconomicfactors directly to health outcomesused several approaches.These includethe use of simplecorrelationsbetween regional life expectancy or infant mortality rate and selectedregionalsocioeconomicindicators(Hertin 1981;Flieger, et al. 1981; West1981),multivariateanalysisofprovincialinfantmortalityrates.(West 1981),multiyariateanalysisof infant mortalityrate based on constructedtimeseriesdata (Herrin and Paqueo 1985), and rnultivariateanalysis,basedonhouseholdsurveydata ofchildmortally (Martin, etal. 1983;Herrin 1984),morbidity(Layo 1977 ), and nutritionalstatus of preschoolers (Battad1978:Paqueo 1977,and Popkin 1980). An examinationoftheseisinorder.
TakingadvantageoftheregionalhealthindicatorscompiledbyZablan(1977) for 1970 orthereabouts,Herdn(1981) computedzero ordercorre-lationcoefficients(r)betweeneachoftheseindicatorsandthe 1970regionalmale lifeexpectancyof birthestimatedbyFlieger,et al. (1981).The resultsrevealstrongercorrelationbetween regionalmale life expectancyat birthwithpercentliterateofpopulationage 6yearsandover(r=0.72)andpercentof malesinfarmingoccupations(r = 0.71), thanwithindicesof sanitation(r= 0.43)or withthepercentageoffamilieswithannualincomesbelow P5000(r = 0.28). Moderate correlations(r between 0.50 and 0.61) were found

32 AlejandroN. Herrin& MaricarGinsonBautista
betweenmale life expectancyandindicesof healthfacilities,healthman-power,infrastructures(percentof existingroads made of concrete),andurbanization,respectively.These correlationssuggestthat both basicdevelopmentfactors(literacy,economicstructureandinfrastructures)andhealthserviceandrelatedfactors(sanitationandhealthfacilitiesandhealthmanpower)andimportantin explainingregionalmortalitydifferentials.
Anotherstudyof areal differentialsof mortalityis that conductedbyFlieger,et al. (1981), where provinciallife expectancieswere foundto becloselycorrelatedwithseveralsocioeconomicindicators.These indicatorsinclude(a) percentof populationurban(r = 0.51); (b)percentof townswithelectricity(r =0.73); (c) percentof population25 years and over with noschooling(r= -0.64):(d)percentofpopulation25yearsandoverwithcollegeeducation(r = 0.54); and (e) manufacturingestablishmentsper 10,000population(r = 0.47).
A studybyWest (1981)examinedcorrelatesof infantmortalityattheregionaland provinciallevels.Usingdata on infantmortalityderivedfromFlieger, et al. (1981) estimatesand variousindicatorsfrom the NationalHealthSurvey andthe Area FertilitySurvey,the studyfoundthe followingbivadaterelationships:higherregionalinfantmortalityisassociatedwithlowleveloffemale education,lowsocioeconomicstatusindex,highproportionofthepopulationwithpoorgarbagedisposalpractices,lowproportionof thepopulationhavingaccessto safewater supply,highproportionof womenusingtraditionalhealthattendants,andgreaterproportionofthe populationlivinga great(morethan5 kilometers)distancefroma hospital.Onthe otherhand,usingdatafromthecensusandFlieger,et al. (1981)provincialinfantmortalityestimates,and applyingregressiontechniques,the studyfoundthatprovincialinfantmortalitywasnegativelyassociatedwiththeproportionof rural females with elementaryeducation, proportionof householdsowninga radio,andproportionofhouseholdswithpumpedwatersupply;butpositivelyrelatedwith the proportionof males who are farmers, and theproportionof womenwho marriedearly.
Recently,ithas beenpossibleto examinemore rigorouslythe macrodeterminantsof mortalityusingtime seriesdata on infantmortalitymeas-ured as the lifetable infantmortalityprobability,qo(Herrin and Paqueo1985). The time series data on infant mortalityprobabilities(qo) wereconstructedbytakingthe infantmortalityrate(IMR) estimatesderivedfromvitalregistrationandcensusdata as reportedbythe DiseaseIntelligenceCenterofthe MinistryofHealth,andcorrectingthese for underenumerationand definitionaldifference(IMR vs. qo)usingFlieger's,et al. (1981) esti-matesof qofor 1960, 1970 and1975.Thecorrectionfactorfor1950 wassetat slightlyabovethatfor 1960, sincetherewas nocomparableestimateofqofor 1950. Correctionfactorsfor each year in the intervals 1950-1960,1960-1970 and 1970-1975 were derived by linear interpolationbetweenbenchmarkyears.The rawdataas wellas theresultingestimatesof infant

HealthImprovements:DeterminantsandConsequences 33
mortalityprobabilitiesare discussedin Herdn and Paqueo (1985). Theresultingestimatesof infantmortalityprobabilitiesfor theperiod1957-1977werethenrelatedtothe followingmacrovariables:employmentrate infull-time equivalents,reel priceof food, realper capitapersonalconsumptionexpenditures,and real cumulated per capita health expenditures.Theresultsrevealedthat infantmortalityratesare positivelyrelatedto the realfoodpriceandnegativelyrelatedto alltheothervariables.Theauthorsthenconjecturedthat in view of the unfavorabletrends in all these macrovariablesinthe 1980s,thetrendinthefirsthaftofthe 1980sislikelyto showa slowingdownof infantmortalitydeclines.
We now turn to household-levelstudiesof child mortality,generalmorbidity,and nutritionalstatus.
The studyby Martin,et al. ( 1983) describedeadier with respecttoproximatedeterminantsalsoexaminedthe socioeconomicdeterminantsofchildmortality.The socioeconomicdeterminantsincludemother'seduca-tion,father'seducation,regionof birth,urban/ruralresidence,and electric-ity.The resultsshowthatthe parent'slevelofeducation,specificallythatofthe motheris negativelyrelatedtochildmortality.Thepresenceofelectricityin the householdwhich the authorsconsidered a reflectionof higherhouseholdincomeand communitydevelopmentis also associatedwithlower mortality. In terms of regionof birth, child mortalityis highest inMindanaoandlowestinMetroManila,reflectingdifferentialsocioeconomicdevelopmentandaccessto healthfacilities.The effect of urbanresidenceis interesting.Inthe univariatemodel,urbanresidenceis associatedwithlowerchildmortality.However,whenothervariablesare introducedinthemultivariatemodel,theeffectof urbanresidenceispositive.These results,accordingto theauthors,suggestthatfactorsassociatedwithlowermortal-ity are overrepresentedin urban areas. When the effectsof these otherfactorsaretakenintoaccount,theapparentadvantageof urbanresidenceare significantlyreduced, and in fact reversed. Note, however,that theregionof birth,electricityandurban/ruralresidenceare allmeasuredattimeof survey,while child mortalityrefers to past events. Hence, the usualcautionin attributingcausalityfromthe observed relationshipsis inorder.
Ina studyin MisamisOrientalprovince,Herrin( 1984) examinesthesocioeconomiccorrelatesof childsurvival,definedastheproportionsurviv-ingofchildreneverborntowomenage35 yearsorless.The resultsindicatethat mother's education,rural residence (residence in coastal or inlandbarangaysvs.residenceinmunicipalpeblacions),and thenumberofyearsthe community have had electricservice from the rural electrificationprogramare allpositivelyrelatedto childsurvivalrate. Lowersurvivalrate,however, is associatedwith greater distance of the householdto themunicipalpoblacion.The resultsrelated to mother'seducationis as ex-pocted.Moreover,likeMartin,etal.(1983) findings, childsurvivalis higherin rural than in urban settings after controlling for other factors. The

34 AlejandroN.Herrin& MaricarGinsonBautista
electrificationvariablepartiallyrepresentsthe Supplyof health service.Earlierexploratorystudiesinthe provincesuggestthatruralelectdficaUonis associatedwith the establishmentof small emergencyhospitals,withincreasedefficiencyin the provisionof health servicesin the ruralhealthunits,andwiththeincreasedaccesstosafewatersupply(Herrin,1979 ).Theeffectof distanceto poblacion,which representsaccessto health careservices,isas expected.Householdincomeorwealthvariablesproxiedbyhousingconstructionindexandownershipof house,houselotand agricul-tural land,respectively,as wellas the predictedwage of the husbandandthewife, respectively,werefoundto be not significant.
With respectto morbidity,the studyby Layo(1977 ) relatedacute,chronicortotalillnessinthe household(numberof reportedillnessduringpast30 dayspriorto interviewdate)to a numberofdemographic,economic,andsocialvariables;more specifically:numberof householdmembersinspecificage groups,educationof mother,per capitahouseholdincome,locationof residence(ruralvs. urban),andhealthand nutritionbeliefsand_nowledge,inadditionto threeproximatevariablesdescribedearlier.Layofoundthe followingrelationships:First,age is the mostsignificantpositivefactorof morbidity.Fortotalandacute illness,the mostsignificantpositivefactorwasthe numberof childrenage 0-5 years.Forchronicillnesses,themostsignificantfactorwasthenumberof householdmembersage 65 yearsand over. These resultsare consistentwith the common age patternofmortalityandmorbidity.Secondly,traditionalhealthbeliefshavea positiverelationshipwith chronicillness.Thirdly, educationof mothers beyondelementaryschoolinghas a negativeeffectontotaland chronicillnesses.Fourthly,per capitaincomedid not havea significanteffecton any of themorbiditymeasures.Finally,highermorbidityratefortotalor acuteillnessesis foundin urban as opposedto ruralareas, a findingconsistentwiththefindingsof Martin,et al. ( 1983) and Herrin( 1984) forchildmortality.
Finally,withrespectto thesocioeconomicdeterminantsof nutritionalstatusof preschoolers,Battad( 1978 )in a Laguna case studydescribedearlierfoundthatthe per capita householdincomeexclusiveof mother'scontributionispositivelyrelatedtonutritionalstatus,and itseffectincreasesfromtheyoungest(lessthantwoyears)totheoldestage group(4-6years).However,the effect of incomeis small.Evenfor the 4-6 years age groupwheretheeffectofincomeisgreatest,theestimatedincomeelasticityisonly0.02, meaningthata doublingofincomeisassociatedwithonlya 2.0 percentrise in nutritionalstatus (percentageof standardweight by age usingHarvardstandardat50th percentile).Battedspeculatesthatthelowincomeelasticitymaybedueto the factthat "increasesin incomeare notdirectedto preschoolchildnutritionalstatus"(p. 163). She notesthat ina studyofLaguna households,a doublingof incomewas associatedwith a fourpercentriseinhouseholdpercapitaintakeofcaloriesandproteins(twicetheeffect of income on an individualchild's nutritionalstatus). She thus

HealthImprovements:DeterminantsandConsequences 35
concludesthat "unlessincreasesin incomeare directed to preschoolersthroughspecificeducationornutrition,theincomeeffectmaybe largelylost"(p. 163).
Battadalsofoundthat mother'seducationwhichrepresentsmother'sproductivityinchildcare,hasa positiveeffectonnutntionalstatus;theeffectis largestamongchildrenlessthantwo years.
Paqueo(1977), alsoin a Lagunacase study,estimateda nutritionalstatusequationwhereintheproportionofthirdandseconddegreeprotein-caloriemalnutrition(basedonweightforagemeasure)amongpreschoolersisa quadraticfunctionofpercapitahouseholdincomeexclusiveofthewife'scontributionandtheeducationofmother,respectively.The resultssuggest•thattheremaybe somethresholdincomebelowwhichthenutritionalstatusof preschoolersmay tend to deteriorateas their parentsacquire moreincome. Beyondthe threshold,increases in income reduce preschoolchildren'smalnutritionrates but at a diminishingrate. The same type •ofrelationshipwas observedwith respect to the educationof the mother.Paqueo,however,was unableto providean explanationfor the observedempiricalrelationshipsand urged further examinationof the underlyingcausal mechanisms.
Using data from the Laguna survey, Popkin(1980) estimated areduced-formnutritionalstatusequationfroma sampleof269 households.Nutritionalstatuswas measuredalternativelyas (a) averagechildweightaspercentageof normalweight for age; and (b) average child height aspercentageof normalheightforage.Mother'seducationwasfoundto havea significantpositiveeffecton bothnutritionalstatusmeasures.The pres-ence of infantshasa positiveeffectbut the numberof otherpreschoolershave a negativeeffect on nutritionalstatus (weightfor age). Because ofPopldn'sinterestinexaminingtheroleofmother'smarketworkonchildcare,he includedmother'slabor tome participationin the equation,the resultindicates that mother's labor force participation negatively affectspreschooler'snutritionalstatus(weightforage). However,Popkinnotesthatthe effectappearsto be quitelargeand out of line relativeto what can beinterredfromthe resultsofa morecompleteanalysiswhichheundertookinthesamestudy(theresultsofwhichwerediscussedearlierunderproximatedeterminants).Moreover,the resultsregardingmother'slaborforcepartici-pationcannotbe takenas conclusive,becauseittoo is a decisionvariablethat shouldhave been endogenouslydeterminedinthe model.
In sum,thesestudiesindicatethe mostconsistenthouseholdsocio-economicfactor stronglyinfluencing increasedchild survivalis mother'seducation.Controllingforsocioeconomicfactors,the urbanenvironmentisrelatedwithincreasedchildmortalityriskormorbidityrates.Thismaybe dueto greater crowding and pollution in urban areas than in rural areas.Nutritionalstatusisclearlyinfluencedbymother'seducationandhouseholdincome.Several macro-policyvariablesare alsoseer_to significantlyintlu-

36 AlejandroIV.Herrin& MaricarGinsonBautista
enceinfantmortalitytrends,particularlyfoodprice,publichealthexpendi-tures, employmentandpersonalconsumptionexpenditures.
Consequences
Inreviewingempiricalresearchontropicaldiseaseimpacts,Andreanoand Helminiak(1986) notedthat researchconductedthusfar has beenmainlyrestrictedtoshort-termmarketproductioneffects,and littleattention,if any, has been givento examininghealthconsumptioneffects, socialinteractionand leisureeffects, short-termnon-marketproductioneffects,and many of the hypothesizedcomponentsof long-termproduction/con-sumptioneffects,
After reviewingthe evidenceconcerningthe effect of health andnutritionon output,Gwatkin(1983) concludedthat the resultsof macro-economicresearchlinkinghealthand/ornutritionalstatusontheonehand,andeconomicgrowthontheotherhavebeeninconclusive.Interestingly,hefindsthat'.., theminorityofstudiesshowingnorelationshipbetweenhealth/nutritionstatusandeconomicoutputappearsingeneralto bemethodologi-callysuperiortothe majoritywhichsuggeststheexistenceof suchrelation-ships"(p. ii).Moreover,Gwatkinfoundthatfieldresearchhas been largelyrestrictedtoschistosomiasis,energyintakeandirondeficiency,andthatthisresearch,withtheexceptionofirondeficiency,hasthusfarfailedtoestablishany consistentrelationshipbetweenimprovedhealth or nutritionand in-creasedoutput.
In another reviewof the health and developmentliterature,Barlow(1979)remarks that the empiricalstudieson the whole are neitherveryconvincingnor easilygeneralizablebecauseamongothers,eitherthesestudiesarecharacterizedmorebyanecdotalevidencethanbyquantitativeanalysis,orthe numberof sampledobservationsis oftenvery inadequate,or when correlationsbetween two variablesare reported,the directionofcausationis\notcarefullyanalyzed.
In the Philippines,population-basedstudieson the economicandsocialconsequencesof healthoutcomesare hard to come by. The fewrecent studiesincludethoseof Popkinand Lira (1977) on the effectofnutritionalstatuson learning,Paqueo(1985) on the effect of illnessonchild'seducationalattainment,andHen-in(1986) on perceptionsregardingdiseaseimpacts.
In a studyof 240 urbanandruralchildrenfromManilaand Bulacan,PopkinandLira (1977 ) examinedthe effectof nutritionalstatusofchildrenage 10-14yearson learningwhichtakesplaceduringtheirformalschoolingyears.Data on the learningprocesswere collectedthroughachievementtestsandothersurveyinstrumentsdevelopedbythe Surveyof Outcomesof Elementary Education(SOUTELE) researchgroup. Data on nutritionwereobtainedfromanthropometricandbiochemicalmeasurementsonthe

HealthImprovements:DeterminantsandConsequences 37
sample children.The findingsshow that measures of nutritionalstatussignificantlyaffect measures of'the learning process after taking intoaccountsocioeconomicandbackgroundfactorsin a multivariateanalysis.These findings are interpretedto mean that a well-nourishedchild, asopposedtoonewhoisnot,isbetterabletoutilizetheopportunitiesavailablefor learning(i.e.familybackground,schoolquality,andcertaincharacteris-ticsofthepupilandhisclosestfriends).Theauthorssummarizetheirspecificfindingsas follows:
Children with an average income and other backgroundfactors and low-nutritional status have a composite learningindex which is 45% below that of high nutritional status childrenwith the same background (school, peer, SES). Similarly, theamount of learning increase associated with backgroundchanges is shown to be somewhat dependent on the nutritionalstatus of the child. Theseresults are quite consistent for each ofthe SOUTELEachievement tests. Wealso found thatnutritionalstatus is positively associated with the concentrationof studentsand their participation level in extra-curricular activities andinversely related to their absenteeism level.
The authors,however,pointto a numberof reservationsconcerningthe interpretationof results.Themostimportantonesconcernthe natureofthe samplepopulationandthe lackof an initialabilityvariable.The sampleincludesonlychildrenwhodoattendschool.These are mostlikelyto have,onthe average,highernutritionalstatusthanthosenotenrolled.Moreover,because the point of referenceis the leamingprocessduringthe Child'sformalschoolingyears,there isa needto controlforthe initialabilityofthechildpriorto schooling.Data limitationprecludesatisfactoryinclusionoftheinitialabilityvariablein=the analysis.
In a recent studyusing nationalsurveydata (1982 HouseholdandSchoolMatchingSurvey), Paqueo (1985) noted that due to problemsofrepetitionanddroppingout,theproportionof 16-yearoldchildrenwhohavenot completedgradesixisstillsubstantialat35 percentin 1982;amongthe14-yearolds,thepercentageis48. Inorderto understandthisphenomenon,Paqueoundertooka multivariateanalysisofthedeterminantsofeducationalattainmentamongelementary schoolage childrencontrollingfor variouschildcharacteristics,socioeconomicanddemographicfactors,andcommu-nitycharacteristicsaffectingschoolingaccess and job opportunities.Theresultsrevealthatamongchildren7-12 or7-13 yearsold(thesamplesizesbeing3,414 and3,907, respectively),thepoorhealthstatusofthechild(childhas a chronicor persistentdisease)significantlyreducedhis/hereduca-tionalattainment(i.e.highestlevelofschoofingcompleted).The resultsalsoindicate that child'seducationalattainmentis positivelyrelated with the"modemity"ofmother'sviewsaboutillnessand healthcare."Theseresults",

38 AlejandroN. Herrin&MaricarGinsonBautista
accordingto Paqueo, =probablyreflect the effects of illnessand lack ofproperhealthcareon absences,droppingoutandfailureto meetacademicrequirements"(p. 377 ).
Basedonanongoingstudyof thesocialandeconomicconsequencesof schistosomiasis,Herrin (1986) recentlyreportedon data concerningindividualperceptionsof diseaseimpacts.Thedata suggeststhatindividu-als,whethercurrentlyinfectedor not,are generallyaware of the potentialadverseconsequencesofschistosomiasisonvariousaspectsof individualandhouseholdwelfare,includingthoseaspectsinwhichlittleisknown,i.e.healthconsumptionand socialinteractioneffectsandnon-marketproduc-tion effects.Amongthe dimensionsof short-termhealthconsumptionandsocialinteractioneffectsthatare revealedto be importantare pain,stigma,and socialinteraction. Inthe long-run,infectionis perceivedto seriouslyaffect marriageprospects,socialmobilitythroughmarriage,andlongevity.Moreover,infection is perceivedto hampereconomicmobilityand affectlabor supply.With respectto non-marketproductioneffects, infectionisperceivedto adverselyaffect homeproductionactivitiesof mothersandschoolperformanceofchildren.One mayalsoviewschoolperformanceintermsof humancapitalformationwhichhaslong-termimplicationsfor laborsupplyandeconomicmobility.
In the literature,the moststudiedeffectsare the short-termmarketproductioneffects.The data on perceptionsreveala very highagreement(70 percentor more) amongrespondentsthat schistosomiasisadverselyaffects productivityin termsof levelof effort, speed,and numberof claysworked.Moreover,infectionof thehouseholdheadisperceivedto seriouslyaffecthouseholdincomeandmaterialwelfare.
Herdndiscussescertainpointsregardingtheinterpretationofthedatafromthe standpointof understandingand predictingbehaviorrelatedtodiseaseavoidanceanddemandfortreatment.Forthis review,sufficeit tosaythatthemoredifficulttomeasureorevaluatediseaseimpacts,i.e. healthconsumptioneffects,etc.and,therefore,lessstudiedimpacts,arenonethe-lesssalienttothosewhoare affected.Innovativeresearchesare therefore,neededto addresssomeof these measurementissues.
V. SUMMARY OF FINDINGS ANDRESEARCH DIRECTIONS
The researchproducedthusfar basedon nationalpopulationdata,multivariateanalysis or innovativeapproaches has clarified a certainnumberof relationshipsandsuggestednew areasand methodsforfurtherexpandingour knowledgebase concerningthe determinantsand conse-quencesof varioushealthoutcomes.

HealthImprovements:DeterminantsandConsequences 39
PROXIMATEDETERMINANTSANDHEALTHOUTCOMES. Currentinfor-mationonlevels,trendsanddifferentialsonproximatedeterminantsarestillveryuneven.Thereare interestingtrendsanddifferentialsinbreasffeedingandnutritionalstatus,basedondatafromdemographicsurveysandnutritionsurveys,and on environmentalsanitationvadablesfrom the censuses.However,there is very littleconsistentinformationregardingtrendswithrespectto maternalandchildhealthcare, especiallywithrespectto infant/child immunization,access to various health care services,and actualhealthcare utilization.
Atthehouseholdlevel,suchproximatedeterminantsasmother'sage,birthorder,birthintervals,breastfeeding,maternalnutritionalstatus,sani-tation, and child care has been shownto be related to specifichealthoutcomesinthehypothesizeddirection.However,analysiscanbe improvedbytestinga morecompletestructuralmodel.The failureof past.analysestoundertakesuchtestsispartlydueto the lackofdetaileddataneededforthistask. Past effortsto collectsuch data, however,have been parUculadyimaginativeandnoteworthy,e.g.theLagunastudybyateamof economists,nutriUonistsandotherhealth specialists,and theyprovidea strongfounda-tionfor furtherwork.
SOCIOECONOMIC DETERMINANTS OF PROXIMATE VARIABLES.Majorinformationregardingtheserelationshipscomesfroma setofcarefuleconometricanalysesof the Lagunasurveysconductedin 1974 to obtaingeneralsocioeconomicdata andbetween1974 and1977to obtaindetailedinformationon nutrition,child care, breastleedingand time allocation.Among the more clear cut and readily interpretableresults from thesestudiesarethepositiveeffectsof incomeorwealthandmother'seducation,andthe negativeeffect of householdsize onvariousdietaryintakemeas-ures.Alsointerestingisthe findingthatthe presenceof infantsreducestheaverage dietary intake of preschoolers,perhaps because the mother'sattentiontends tobeconcentratedoninfants,and thatthepresenceofolderchildrenage 7-12 years Increasesaveragedietary intakeof preschoolersperhaps becausethesechildrensupplementchildcare time ofthe mother.With respect to breastleeding,beliefthat breastmilkis best significantlyincreasesbreastfeedingparticipation.Of interestis that this belief is notcorrelatedwitheducation,implyingthatmuchcanbe gainedbyinformationcampaignsto encouragebreastfeedingespeciallyamong less educated,and usuallyhighfertility,woman.Whilethese findings are revealing,theyreferonlyto ruralLagunahouseholds.Arethese findingsgeneralizabletothe restof the population?It mightbe usefulto replicatethese studiesinother Philippinesettings at the same time improveupon some of theapproachesto modelingbehavioradopted by these studies.Moreover,thesestudieshavenotaddressedotherproximatedeterminants,especiallythose related to environmentalcontamination,i.e. sanitary toilets, safe

40 AlejandroIV.Hen'in&MaricarGinsonBautista
watersupply,personalhygiene,etc.*The objectiveof suchstudieswillbeto learntheconstraintswhichindividualsandhouseholdsface, andsubse-quentbehaviormodification.
SOCIOECONOMIC DETERMINANTS OF HEALTH OUTCOMES. At thehouseholdlevel, mother's educationcomesup as the mostconsistentfactorrelated to improved child survival rates, reducedmorbidity ratesand highernutritionalstatusof preschoolers. Incomeorwealth variableswhen they areincluded in the analysis do not appear to be significant except with respectto thenutritionalstatusof preschoolers. Exogenouscommunity level factorswhich proxy for health serviceavailability appearimportant determinants ofchild mortality. Of great interest is a consistent finding in three separatestudies,two on mortality andone on morbidity, that an urban setting, whenother socioeconomic factors are controlled for, tend to have an adverseeffect on health.The urban setting mayrepresentcertain health hazards, i.e.overcrowding,pollution, etc.that haveyet to be explicitlyincorporated in theanalysis. Finally,health beliefs, independent of mother's education, appearto be a significant factor in increasing morbidity rates. This suggests thatinformation campaignsto modify health-related beliefs and practices couldwell be an important component of any health-promoting strategy.
Atthe national level, the resultsof the only study usingtime seriesdataidentify the macroeconomic context inwhich further infant mortality declinecan beexpected. The macrovariables,i.e. real food price, employment rate,per capita consumption expenditures and real per capita health expendi-turesare highly sensitive to variouseconomic policies and public expendi-ture priorities.
Analysis of the socioeconomic determinants of health outcomes,specifically mortality, are often difficult to undertake not so much becauseof methodological problemsbut more so because of data problems. Deathsare rare events and data collection can easily become an expensiveundertaking. For the other health outcomes, regular national demographicand nutritional surveys could be designed to allow collection of moresocioeconomic data, while regular household surveyson employment andincomes could be designed to allow collection of health-related data.Analysis of these richer data sets could help increase current limitedinformation for policy guidance.
CONSEQUENCES OF HEALTH OUTCOMES. Of all health and relation-ships, empirical evidence on the social and economic consequences ofvarious health outcomes is the most limited. Yet this isprobably one areawhere strong evidence isneeded inorder to justify the demand for a greatershare of the currently available scarce resources for health-promotingactivities.The few studies reviewed in this paper suggest that suchconse-quences are not trivial. Exceptfor the study of perceptions, the remaining

Health Improvements: Determinants and Consequences 41
studies cover only health impacts on learning and educational achievement.There is practically no reliable quantitative information regarding impact onthe other dimensions of welfare to guide policy decisions. At the level of thehousehold, the perception data reveal that disease is perceived to havepotentially adverse consequences on several dimensions of social andeconomic welfare. Yet not much is known on how people actually perceiveand give importance to each of these specific dimensions to affect theirdecisions regarding health-promoting or disease-avoidance activities, andtherefore, regarding their allocation of household resources for health.
As a final note, itcan be asked: isit possible to know everything wantedand needed? In a rather pessimistic tone, Barlow (1979), after reviewing theliterature, concludes: "The relationships between health and economicdevelopment are so complex that the definitive study in this area will neverbe made" (p. 47). From a purely scientific standpoint, this view is probablycorrect. But from the standpoint of policy guidance, what is only needed,recognizing that information is costly, is to generate enough relevantinformation to help policy makers improve their decision-making processessuch that the probabilityof making correct decisions is higher than the usual50 percent easily obtainable from a pure guess. How much higher than 50percent depends upon the importance of the policy decision to be made andthe cost of information.
BIBLIOGRAPHY
Andreano, R. and T. Helminiak. "Economics,Health and Tropical Disease: AReview." Paper prepared for the Meeting on the Economicsof TropicalDiseases,Manila,September2-5, 1986.
Andrews,F.M.. "SocialIndicatorsandHealth-For-All,"Social Science and Medicine(1981), 15C: 219-223.
Barlow R. "Health and EconomicDevelopment: A Theoretical and EmpiricalReview,"Research inHuman CapitalandDevelopment, Vol.1,JAIPress,Inc,1979.
Battad,J.R. "Determinantsof NutritionalStatusof Preschoolers,"The PhilippineEconomic Journal, 17(1-2) (1978): 154-167.
Chen,L.C. "ChildSurvival:Levels,Trendsand Determinants,"in R.A.BulataoandR.D. Lee, eds., Determinants of Fertility inDeveloping Countries, Washing-ton, D.C.: NationalAcademyPress,1983.
Concepcion,M.B.andJ.V.Cabigon."LevelsandTrendsof Mortality,Philippines:AnAssessment in 1980," Universityof the PhilippinesPopulation Institute(mimeo), 1984,

42 Alejandro N. Herrin & Maricar Ginson Bautista
Esclamad, K•, E.A. de Guzman and L.T. Engracia."Infant and Child Mortality in thePhilippines: Levels, Trends and Differentials," in L.T, Engracia, C.M.Raymundo and J.B, Casterline, eds•, Fertility in the Philippines: FurtherAnalysis of the Republic of the Philippines Fertility Survey 1978, Voorburg,Netherlands: International Statistical Institute, 1984.
Evenson, R.E. "Philippine Household Economics: An Introduction to the Sympo-sium Papers," The Philippine Economic Journal, 17(1-2): (1978) 1-31.
Flieger, W., M.K•Abenoja and A•C. Lira. On the Road to Longevity: 1970Nationaland Provincial Mortality Estimates for the Philippines, Cebu City: San CarlosPublications, 1981•
Fiorentino, R, "Nutrition•"Paper prepared for UNICEF, 1986.
Food and Nutrition Research Institute (FNRI). First National Nutrition Survey,Philippines, 1978,Manila: National Science Development Board, 1981.
• Second Nationwide Nutrition Survey, Philippines, 1982, Manila:National Science and Technology Authority, 1984.
Gonzalo, S.Y. and R.E. Evenson, "Production and Consumption of Nutrients inLaguna," The Philippine Economic Journal, 17 (1-2) (1978): 136-153,
Gwatkin, D.R• 'Does Better Health Produce Greater Wealth? A Review of theEvidence Concerning Health, Nutrition, and Output," (unpublished manu-script),1983.
Herrin,A.N. "Rural ElectrificationandFertilityDeclineinthe SouthernPhilippines,"Population and Development Review, 5 (1979):61-86.
•Population and Development Research in the Philippines:A Survey•NationalEconomicandDevelopmentAuthority,1980.
• "Populationand Developmentinthe Philippines:A Status Report,"ASEAN/AustraliaPopulation Project: Population-DevelopmentDynamicsandthe Man/ResourceBalance,1981.
._Socio-economic-DemographicImpact:TheCase ofRuralElectrifica-tion."Perspectives for Population and Development Planning, Manila:Com-missionon Populationand NationalEconomicand DevelopmentAuthority,1984.
• "Give the Childa Chance:ChildSurvival,healthand the PhilippineFuture." Paper preparedfor the Seminaron EconomicDevelopmentin thePhilippines:Analysisand Perspectives,(December5-6, 1985).
• "Perceptionsof Disease Impacts:What Can They Tell Us," Paper

Health Improvements: Determinants and Consequences 43
preparedfor the Meetingon the Economicsof TropicalDiseases, Manila(September2-5, 1986).
and V.B. Paqueo. "DemographicTrends, PopulationPolicyandtheEconomic Crisis,"Transactions of the Nmional Academy of Science andTechnology, Republic of the Phil4opines,7:1985, 335-357.
King, E. and R.E. Evenson,"Time Allocationand Home Productionin PhilippineRuralHouseholds,"inM.Buvinic,etal., eds., Womenand Poverly in the ThirdWorld,Baltimoreand London:The JohnsHopkinsUniversityPress,1980.
Layo, L. "Morbidityand the PhilippineWelfare inthe Year 2000," Paper No. '13,Population,Resources, Environmentand the PhilippineFuture: A FinalReport,Vol. IV-1.A, 1977.
Madigan,F.C. "Some RecentVitalRatesandTrendsinthe Philippines:Estimatesand Evaluation,"Demography, 2:(1965), 309-316.
Martin, L., et al. "Co-Variatesof ChildMortalityinthe Philippines,IndonesiaandPakistan:AnAnalysisBasedonHazard Models,"Population Studies, 37(3):(1983), 417-432.
Mosley,W.H. "ChildSurvival:ResearchandPolicy,"Population and DevelopmentReview, Supplementto Vol. 10: (1984), 3-23.
and L.C. Chen. "An Analytical Frameworkfor the Study of ChildSurvival in DevelopingCountries,"Population and Development Review,Supplementto Vol. 10: (1984), 25-45.
, eds."ChildSurvival:StrategiesForResearch,"Population andDevel-opment Review, Supplementto Vol. 10, 1984.
Ministryof Health.Philippine Health Statistics, variousyears.
NationalEconomicandDevelopmentAuthority(NEDA). Philippine Statistical Year-book, 1985.
Paqueo, V.B. "Social Indicatorsfor Health and Nutrition,"in M. Mangahas, ed.,Measuring Philippine Development, DevelopmentAcademy of the Philip-pines,1976.
•"PREPFHealthandNutritionScenariosforthe Year2000,"Paper1.1,
Population,Resources, Environmentand the PhilippineFuture: A FinalReport,Vol. IV-l, 1977.
_m" "AnEconometricAnalysisofEducationalAttainmentAmongElemen-tary SchoolAgeChildren:PreliminaryAnalysis,"Transactions of the NationalAcademy of Science and Technology, Republic of the Philippines, 7: 1985,359-380.

44 Alejandro N. Herrin & Maricar Ginson Bautista
Popkin,BM. "EconomicDeterminantsof Breast-FeedingBehavior:The Case ofRuralHouseholdsinLaguna,Philippines,"inW.H. Mosley,ed., Nutrition andHuman Reproduction, New YorkandLondon:PlenumPress, 1978.
• "RuralWomen, Work, and Child Welfare inthe Philippines,"in M.Buvinic,et al., eds., Women and Poverty in the Third World, BaltimoreandLondon:The JohnsHopkinsUniversityPress, 1980.
Schultz, T.P. "Studyingthe Impact of Household Economicand CommunityVariablesonChildMortality."Populationand Development Reviews, Supple-mentto vol. 10: 1984, 215-236.
Valenzuela,R.E. "A Studyon NutrientDistributionWithinthe Familyand FactorsAffectingNutrientIntake," The Philippine Economic Journal, 17 (1-2), 1978.168-184.
West,S. "InfantMortalityinthe Philippines:CausesandCorrelates,"(unpublishedmanuscript)1981.
WorldHealthOrganization(WHO), PrimaryHealth Care: Reportof the InternationalConference on PrimaryHealth Care,Alma-Ata,USSR, 6-12September1978,Geneva: WorldHealthOrganization,1978.
Zablan,Z.C. "TheProspectsofMortalityintheYear2000,"TechnicalReportNo.2.1Population,Resources, Environmentand the PhilippineFuture: A FinalReport, Vol. 111-2,1977.
• "PhilippineTrends in BreastfeedingPractice,"Universityof thePhilippinesPopulationInstitute(mimeo),1985.
•"DemographicandHealthperspectivesof the Statusof Women andChildreninthe Philippines,"ReportpreparedforUNICEF, 1986.

Structures and Interventions in thePhilippine Health Service DeliverySystem: State of the Art
Victoria A. Bautista*
I. INTRODUCTION
This paper discusses the state of the art of the structuresandinterventionsinthe Philippinehealthservicedeliverysystem.Thefollowingtopicswilladdressthispurpose:(1)the conceptualframeworkwhichwillbethe basisfor describingthe structuresand interventionsfor healthservicein the Philippinecontext; (2) a descriptionof the trends and patterns instructuresand interventionsas componentsof the health servicesystemanda discussionoftheinsightsgainedregardingeachpatternbasedonthereview of literature;(3) an analysisof the gaps in the knowledgeandthepolicyproblemsindicatedor impliedin thesematerialsthat mayconstitutea researchprogramin healthpolicy.
Existingbibliographiesonhealthhadbeenreviewedinthepreparationof thisstudy,notablythosebythe PhilippineCouncilfor Health Researchand Development(PCHRD) particularly:the Inventory of Completed Re-searches 1980-84,Inventory of OngoingResearches 1984anda computerprint-outof current researches furnishedby the same office and thebibliographypreparedby LedivinaV. Carittowiththe assistanceof RosaCordero,bothof the U.P. Collegeof PublicAdministration.
* Associate Professor, College of Public Administration, University of the Philippines. Theauthor wishes to acknowledge the assistance of Rosa Cordero in gathering some of thematerials in the preparation of this paper. She also wishes to express gratitude to Dr.Ledivina V.Cari_o and Prof Ma. ConcepcionP. Affilerfor enabling her touse some of theilmaterials.

46 VictoriaA. Bautista
Some publicationsof key academic and research•institutionscon-cemedwithhealthresearchanddevelopment,composedof bothempiricalstudiesandreflectiveessays,hadbeen reviewedto determinethe currenttrendsandpatterns.Theseinstitutionsinclude:the De la Salle University,PopulationCenterFoundation,UNICEF (UnitedNationsChildren'sFund),U.P. Instituteof PublicHealth, U.P. InstituteofSocialWorkandCommunityDevelopment, U.P. College of Public Administrationand WHO (WorldHealth Organization).Documentspreparedby serviceinstitutionsespe-ciallythosereleasedbythe MinistryofHealthandtheTask ForcePeople'sHealth,a voluntaryorganizationwere alsostudied.
Consideringthevoluminousmaterialswrittenonthe subjectmatter,aconsciouseffortwas requiredto retrievethosethat reviewpastresearcheson a given area and to highlightthe findingsand conclusionsof thesematerials.
II. CONCEPTUAL BACKGROUND
The national health system can be defined as the _coherentwholeofinterrelatedcomponentparts ... whichproducea combinedeffect on thehealthof the population"(Kleczkowski et al. 1984a:5). The majorcompo-nents of a health system include:the health resources,the organizedarrangementof resources,the deliveryof healthcare, economicsupport
• andmanagement(Kleczkowskietal. 1984b:13).Thispaperfocusesmainlyontwoofthesecomponents,namely:theorganizationalstructureforhealthservicesandthedeliveryof healthcare (ortheactualstrategiesadoptedforthe extensionof healthservices).
A. Organizational Structure
The firstcomponent,organizationalstructure,refersto the arrange-ment of resourcesthat are =necessaryto bring health resourcesintoeffectiverelationshipswitheachother,andalsoto bringindividualpatientsor communitygroupsinto contactwiththe resourcesthroughhealthcaredeliverymechanisms"( 1984b:19). Thestructuremaybeclassifiedaccord-ingto degrees of formalityor levelof institutionalizationoftheorganization.In otherwords,is the structureduly recognizedwithina legalframework?Some structuresmaybe constitutedformally,and someinformally.
PUBLIC VS. PRIVATE. The concernfor health may be spearheadedby"actionsofgovernment"andbythose"outsideofgovernment"(Kleczkowskiet al. 1984b: 19). Actionsof governmentrelatedto health includethoseundertakenbynationalhealthauthoritiesandothergovernmentalagencies.The nationalhealth authorityis often the principalgovernmentagency

Health_prviceDeliverySystem 47
taskedwith healthactivities.Othergovernmentagencies inturn, may beconcernedwith parts of the health system whether independentlyor incollaborationwiththe nationalhealth authority.
Outside of government, some organizationalarrangements con-cemed with health servicesmay be undertakenby privatehospitalsandclinics.Othernon-governmentalorganizations(NGOs) maybetaskedwithextendingvoluntaryhealth servicesfor the publiclike those initiated byfoundations,religiousinstitutions,civic clubsand internationalorganiza-tions.Some institutionsor groupsmay alsoforge healthactivitiesfor theirrespectiveconstituencies,suchas industrialfirms.or laborunions,whichmay protect the health and safetyor their membersfrom diseases andhazardsrelated to the work environment.Further,someindividualsmayindependently extend health care services exemplifiedby the effortsofprivatemedicalpractitioners,para-professionals(e.g., rnidwives), and tra-ditionalhealers (e.g., hilots, herbolarios).
CENTRALIZED VS. DECENTRALIZED. Within the structureof govern-ment, two broad classificationsare needed in order to understand theorganizationof resourcesfor health.
One has to do with the locus of decision-making in fulfillingtheactivitiesof planning,implementationand monitoring/evaluationof healthactivities.Two optionsare available:centralization or decentralization(See Bautista 1984a:1).Centralizationis a stateor conditionin a govern-mentsystemwherethereisconcentrationof powersand responsibilitiesatthecenter. Decentralization,intum,entailsdispersalofpowersand author-ity to the differentlevelsbeyondthe topmostleadershipin the hierarchy.Decentralizationmay be achievedthrough(1) devolution- bytransferringpowers and functionsof a higher level to those in the pedphenj or (2)deconcentration- by delegatingauthorityfrom central headquartersof aministryto subordinateunitsto enablethemto decidecasesand problemsarisingwithintheirfunctionalresponsibilities.Unlikedevolution,deconcen-trationdoesnotentaildelegationof substantiveresponsibilitiesto thefieldofficesbutonlysomeminorresponsibilities,whichare oftenadministrativein nature (Bautista 1984a:1).
SECTORAL VS. INTEGRATED. A second structuralarrangementwithingovernment has to do with the number of functions pursuedby thenational health ministry.This arrangement may either be sectoral orIntegrated. A sectoralstructu_is one which "purportsto cover 'withinhealth' functions,i.e. any asl:)C_ctof preventive,promotive,curative orrehabilitativemedicineor any combinationof these" (Caritlo 1982:7).Ontheotherhand,an integratedstructureundertakes"programs,involvednotonlyin allorcertainaspectsof healthcare, but also inotherservicessuchas othersocial(education,welfare),economic(infrastructureconstruction,

48 VictoriaA. Bautista
income-generatingprojects),political(organizationor electoralactivities,political re-education),and cultural (those relative to religion) (CarifJo1982:7).These activitiesaltogether,are seento improvetheoverallhealthstatusandwell-beingof the population.
B. Strategies
The secondcomponentof the healthsystemconsideredhere, is theinterventionsor strategiesapplied in the deliveryof health care. Morespecifically,thiscomponentrespondsto the issueof theactualprocessesappliedinthedeliveryof healthcare, There arevariouswaysbywhichthistopicmay be tackledbutforthe purposeof thispaper,the followingwillbeconsidered:
[] The levelof citizen-participationinthe differentprocessessuchas planning,implementationand monitoring/evaluationof healthandhealth-relatedactivitiesor anycombinationof theseactivities.
[] Health care delivery accordingto the objective delivered -whether promotional, preventive, curative, rehabilitative and/orsociomedical(see Kleczkowskt et al. 1984b:23).Kleczkowskiet al.,definethese activitiesas follows:
... thepromotion of health extendfarbeyond thetraditionalfunctions of health care institutions and aim at creating en-vironmental conditions and human behavior that can con-t#bute positively to health. Preventive activities are di-rected not only against communicable diseases, but alsoagainst many otherpreventable conditions such as rickets,endemicgoiter, anddental ca#es. Theyinclude in additionto immunizations, such interventions as vitamin supple-mentation, iodination of salt, flouridation of water, and theprovision of guards on the machinery to prevent industrialinjuries. Curative activities consist in the use of drugs,surgery, or other procedures to interrupt a pathologicalprocess or to reduce harmful consequences of a disease.... Rehabilitation ... aims at the restoration of physical,mental, and social functions through relevant medica/pro-cedures: this is often done with social services (e.g.,sheltered work, reorganization). Soclomecllcal card ap-plies particularly to irreversit_rofound disability or pro-gressiveillness inwhich neithertreatment norrehabilitationcan bring improvement (1984b:23).
[] The levelofcomplexityorsequentialorderinwhichhealthneedsof the populationare servedwhetherprimary;secondaryor tertiary

'HealthServiceDeliverySystem 49
(Kleczkowski et al., 1984b:23). Thesestrategiesof healthcare hadbeen distinguishedby Affiler ( 1984:5-6 ) in the followingmanner.Pnmarycare is a health service which requiresminimummedicalfacilityandequipment.Thisisoftenextendedonan"out-patientbasis."Secondarycare is deliveredby a medicalpractitionerand requiresbasichospitalfacilitiesand multidisciplinarysupportof otherdoctorsand services.Tertiarycare isrenderedbya specialistfor complicatedcasesneedingspecializeddiagnosticand treatmentfacilitiesand mul-tidisciplinarysupportservices,This is usually performedon an 9n-patient"basis.
I--I Extentofrelianceon scientificmethodsandstrategiesinadmini-stedng health services.Three approacheshad been describedbyCarillo ( 1986:15.16) namely,Traditional,Westernizedand PrimaryHealth Care. Traditional Health Care (THC) is charactedzed,byrelianceon indigenoushealers(e.g.,herbolados, hilots )whoseskillshad been derivedpdmadlyfrom nativetalentor fromacquisitionofskillsbasedonculturalpracticesorsomesupematuralbeliefs.West-emized HealthCare(WHC) emphasizesthecentralityofhospitalsandmedicalprofessionalsinthe administrationof healthwhosestrategiesand approacheshad been derivedfrom scientifictraining. Further-more,W.I-I_;considershealthastheabsenceofillnessand regardsthepassive role of the communityin respondingto health problems.PrimaryHealthCare (PHC), thethirdapproach,considersthe impor-tant role of file paramedics,indigenoushealth workers,as well asprofessionalswhoseskillsand technologyare basedbothonscienceandindigenousaspectsofhealthcare.Thecommunityisviewedasanactive participantin the maintenanceof "well-being"ratherthan ofhealthproblemsonly.
[] Deliveryof healthservicesaccordingtocertaingroupsorsectorsin the populationlike those targettingthe young, the mothers,thecouples,thedisabled,theoccupationalgroups,the aged, and thelike.
III. TRENDS AND PATrERNS
The Vends and patterns in the Philippinehealth system may besummarized into the followingpoints: (1) the existence of a pluralisticapproach in dealing with structuresof health service delivery; (2) thecompetingtendenciestowardsdecentralizationandcentralizationforplan-ningand implementingdevelopmentprogramsof govemmentwhichlimitthe effortsfor health and otherrelatedactiviaas; (3) the impetusgiventoparticipatory strategies in health propelledby the launchingof PdmaryHealthCarebythegovemmontandtheprivatesector;(4)thepradominance

50 VictoriaA. Bautista
of curativeexpendituresover promotiveand preventivehealthcare activi-ties;(5) the existenceof Westemized,TraditionalandPrimaryHealth Careapproachesand the variable factorsinfluencingreliance;(6) the growingconcerntowardsselectedgroupsinthepopulationlikewomen,childrenandcouplesto the neglectof othersectorslikelaborandthe disabled.
Eachof thesepatternswillbediscussedinthefollowingsectionsandtheinsightsgainedfromthe reviewof literature.
A. Pluralistic versus Unitary Structure
TherearevarioushealthdeliverysystemsinthePhilippinesotherthanthoseprovidedbythe government.Pursuedindependently,these varioushealthprogramsforthepublic,signifythepluralisticstrategyofgovernmentindealingwiththese structures.Thus far, there is no unifiedstructureofpublichealthservicefor the citizenry.
GOVERNMENTAL NETWORK. Inthe government,the primeagencyre-sponsiblefor implementingthe publichealth programis the MinistryofHealth(MOH). Othergovernmentagenciesprovidesupportorcooperateinthe implementationof the healthprogramsuchastheMinistryof Education,Culture and Sports (MECS) for health education;Ministryof Labor andEmployment(MOLE) for the maintenanceof health of theworkforce andenforcementof safetystandardsinthework environment;and, the Philip-pineCouncilforHealth ResearchandDevelopment(PCHRD)asthe agencyin chargeof coordinatingresearchanddevelopmenteffortsin the healthsector.TheMOH alsocooperateswithotherinstitutionsas itpromotestheirrespectiveorganizationalobjectivesand commitments.For example,thefamilyplanningand nutritionconcernsof the Commissionon Population(POPCOM) and NationalNutritionCouncil (NNC), respectively,are bothintegratedintothe healthdevelopmentprogramimplementedbythe MOH.
Withinthegovernmentalstructure,healthserviceinthe ruralpopulacehas improved substantiallysinCe the RestructuredRural Health CareDeliverySystem (RRHCDS)was institutedin 1975. This moveexpandedruralhealth servicewiththe creationof barangayhealthstations(BHSs) asthesatellitestationsundera ruralhealthunit(RHU) locatedinthe centerofa municipality.The BHS is manned by a midwife, while the RHU iscomposedof the rural health physician,rural sanitaryinspectorand ruralhealth midwife.Both unitsperform primary care activities.These unitscomplementthe hospitalnetworkwhichresponds to primary, secondaryandtertiarycases.
As of 1984,there are 367 publichospitals,1991 RHUsserving1,700municipalitiesand 7,991 BHSs to a total of 43,000 barangays (NCSO
' 1985:276). Thus, each BHS covers3,000 to 5,000 people,althoughtheidealratiois1 to2,750 (WorldBank 1984:48).The problemisthattheRHUs

HealthServiceDeliverySystem 51
andBHSshavealsoacquiredsomenotorietyfortheir lackof facilitiesandstaffers(M. Tan 1986:7)whichaffecttheireffectivedeliveryof services.
Other relatedservicesare renderedthroughspecializedclinicslikechest clinics,skin clinics,family planningclinics,socialhygieneclinics,mentalhygieneclinics,dentalclinics,malariaunits,schistosomiasisunits,filariasiscontralunitsandnutriwardunits.
Thehospitalnetworkis alsostratifiedaccordingto thecare itrenders,whetherprimary,secondaryortertiary. In 1981, 14.3 percentof the publichospitalsextendprimarycare;28.2 percent,secondary;and, 57.5 percent,tertiary.
PRIVATE NETWORK. The healthservicesrenderedby the privatesectorisdonethrougha networkof privatehospitals,privatephysicians,traditionalhealers and voluntarynon-governmentalorganizations.There are morehospitalsmannedbythe privatesectorthanthe publicsector.Of the totalnumberof 1,594 hospitalsin1984 (Pujalte 1986:26),1,227or70.7 percentbelongto theprivatesector.About72 percentof physiciansand50 percentof allcategoriesof formallytrainedhealthmanpower(doctors,nursesandmidwives)are alsoemployedby thissector (World Bank 1984:50).Tradi-tionalhealerslikehi/ots numberabout 39,556, 37.7 percentof whomhadbeentrainedasof 1985 byMOH as resourcebase for primaryhealthcare(Carido 1986:20). About331 non-governmentorganizationsalso inde-pendentlyundertakehealth programs(Reodica, 1983). (For a detaileddescriptionof these organizations'programs,see Angara 1978; Cadl_o1980;and Reodica 1983).
ASSESSMENT. It may be worthyto note, though,that these availableresourcesfromthe publicandprivatesectorsareinequitablydistributedinthe country,withthe urbanand accessibleplaceslargelybenefitingfromthese resources(World Bank 1984:50).Thisis becausewhilegovernmenthospitalsare welldistributedon a regionalbasis,onlyabout54.4 percentofhospitalbedsare locatedinthe ruralareas. Furthermore,pdvatehospitalsare confinedto largerurbanareas and two thirdsof privatephysiciansareconcentratedin three urbanizedand richer regions.Also, while primaryhealthcare can easilybe extendedby93 percentof the RHUs and BHSswhichare outsideManila, the ruralclinicsareoftenlocatedintownswhichare inaccessibleto peopleresidingin mountainousand remoteplaces.
A promisingdevelopmentisthe increasingthrustof NGOs to embarkon a community-basedapproachwhichessentiallysharesthe same fea-turesasthe primaryhealthcare (PHC) approach.Theseeffortscanbe fullymaximized, accordingto Reodica (1983:49), by institutinga system ofinformationexchangeand disseminationamong theNGOs,thegovernmentandthe communityto benefitfromthe experiencesineachother'sefforts.Reodicaalsosuggestedthe importanceof a jointor coordinatedevaluation

52 VictoriaA. Bautista
of programsand projects.implementedby bothsectorsto pointout whataspectsintheirrespectiveprogramsneedmodification,aswellastoprovidehealthplannerssupportivedata for further planning.
Cariho(1981:205) hasfor a longtime nowcalledfora needto realizethe mandatethatdeliveryof healthcare isa jointresponsibilityofthe publicand the privatesectors.She saidthat itis urgentfora countrywithmeaslyresourcesto embark on a concerted effort to avoid redundanceandduplication.Shesuggestedthat"governmentshouldtaketheprivatesectordeploymentof healthresourcesintoaccountwhenplanningitsown:wherea privatepractitioner/clinic/hospitalexists,governmentshouldnotduplicatecostlyresourcesby locatingthere also"(Cari_o 1981:205). Theseprivatehealth network could thenbe made a partof the referral system.
B. Decentralization to Recentralization
BROAD POLITICAL-ADMINISTRATIVE FRAMEWORK. The contextualframework in which the national health ministn]operates could affect healthplanning and implementation to be more responsive to the needs of thegrassroots. The extent to which the people themselves can get involved inthe decision-makingprocess dependsuponthegeneral characteristicof thestructure - whether it is centralized or decentralized.
The experience of the Philippines with martial rule under deposedPresident Marcos showed contradictory tendencies for centralization anddecentralization in the planning and administrative framework ofgovernment (Bautista 1984a).After martial law was declared in 1972, theIntegratedReorganization Plan (IRP)was passed and this ushered a majorrevamp in the structure of government. The plan aimed to decentraliz_powersandresponsibilitiesto field unitsandhopedto make thegovernmentcloser to the people. A key innovation in the planning structure is thedecentralizationof the planning effort through the formulation of Region_Development Councils (RDCs) in all the regional centers.The councilsareto be composed of representativesof government agencies implementingsectoral programs. Electiveofficialsare also a partof thesecourcils inorderto ventilate the needs and demands of their respective local areas. Inpractice, however, national officers pursuing sectoral programs primarilydetermine th priorities of their respective field offices and the developmentplan is formulated within the guidelines prepared by the national offices.Development councils have only operated as "talking fora" rather than asbodies that formulate substantiveprograms in response to local demands.Central control has been enhancedfurther by.thepresidential appointmentof the RDCChairman in the region. Hence, the line of control comes directlyfrom the Officeof the President rather than from the planning ministry.
In the administrative machinery, the IRP has mandated the need tolocate,field offices of national ministries implementing nationwide develop-

HealthServiceDeliverySystem 53
mentprogramsin uniformregionalcenters. This movewasenvisionedtofacilitatecooperationandinteractionamongthedifferentfieldoffices.Therewereattemptstodecentralizeresponsibilitiesto thelocalofficesof nationallineministries,butthesewerepredominantlyadministrativeinnature(e.g.,appointmentofpersonnel,promotion,approvingleavesofabsence) ratherthan substantive(Bautista 1984a). Hence, decentralizationwas under-taken mainlythroughdeconcentrationratherthandevolution.
Withregardto national-localgovernmentrelationships,thereare alsocompetingtendenciestowards centralizationand decentralization.The1973 Constitutionexpressed concern for the state to "guaranteeandpromote autonomy"to local governmentunits "to ensure their fullestdevelopmentas self-reliantcommunities".Yet, contradictorypoliciesandpracticeshaveworkedagainstthefullrealizationof localautonomy.Accord-ingto localgovernmentexpertslikeOcarnpoand Panganiban(1984a:4),=localgovernmentswere progressivelystrippedof importantfunctionsandpowersduringthe lastdecade.*
The attemptto recentralizelocalgovernmentpowersoccurredwhenthetraditionalfunctionsof administeringpoliceservices,localfinanceandlocalutilitieshadbeenreferredbacktothe nationalgovernment.Whiletheyassumelocaltaxingpowers,therevenuesfromthisactivityare for the mostpart transferredtothenationalcoffers.Inspiteofthehugeearningsof somelocalunits,they have had to depend on the allotmentsand aid fromthenationalgovernment.Then,asmentionedearlier,localgovernmentslargelydependon nationalagenciesto implementmajordevelopmentprogramsintheir respective areas. Substantiveplanningand implementationhingeprimarilyon nationalgovernmenteffortsthusunderminingautonomyandlocalinitiative.
MOH EFFORTS TO DECENTRALIZATION.On the whole,the MOH hadattempted to be responsivetowards decentralizingpowers and responsibili-ties to local field offices. In response to the call of the IRP to bring thegovernment closer to thepeople, structural innovations inthe administrativeframework had been undertaken through the introduction of the RRHCDSin 1975.Thiswas a big leapin its effortssince1953,when public health careand medical serviceswere delivered mainly through hospitals and clinics,mostly located in urban areas. Then in 1954,city health offices in populatedareas and rural health units in townswere established. However, as noted
* Asabackgrounder,localgavernmentsare"poli'&_alandodministrativesul0divisionsofthenation*stateandarelegallythecorporateentitieswiththepowerstoelecttheirgoverningbodies,imposetaxes,provideservices,andperformothergov_nmentalfunctionswithintheirgeographicjurisdictions"(OcampoandPanganiban1984b:1).Asof1982,thereare73provinces,60charteredcitiesand1,507munidpalitiesaltogetheremployingnearly145,000electiveandappointiveofficials.Atthelowestlevelofthehierarchyare45,000barangays.

54 VictoriaA. Bautista
earlier,despiteeffortstodeliverservicesatthe lowestlevelofthebarangaythroughRRHCDS, the BHSsare stilllocatedin moredevelopedareas.
The secondmajoreffortto streamlinetheMOH bureaucraticmachin-eryoccurredwhenExecutiveOrderNo.851wasput intoeffectonDecember2, 1982.Thisdirectivehas ledtothe integrationof healthandmedicalunitsat thefieldoperationslevel,earliercardedoutindependentlyby the RHUsandDistrictHospitalsat themunicipallevel.TheRHUswereconcernedwithpromotive,preventiveandprimarycare activities.The DistrictHospitalandotherrelatedunitswereconcernedwithcurativefunctions.Byvirtueof E.O.851, the DistrictHospitalbecamethe integratingunit for bothhealthandmedicalservices.At the provinciallevel, integrationwaseffecte_betweenthe ProvincialHospitalandthe ProvincialHealthOfficeunderthedirectionof the IntegratedProvincialHealth Office(IPHO). This mergeralsomeantthe consolidationof the budgetforthe twostructureswhichwere formerlymanaged by the Regional Health Office, thus transferring the routinefinancialandadministrativefunctionsoftheRegionalOfficeto the IPHO. Anadditionalfeatureofthisdirectiveisthe needtoprovidefora monitoringandevaluationsystemtodeterminethe performance-ofMOHprograms.Onthewhole,however,theMOH machineryisstillquitecentralizedinitseffortsasthe fieldpeople have limitedflexibilityto adaptcertain proceduresto localsituations(Demographicand ResearchFoundation,19:119). Substantiveresponsibilitiesarestillcentrally-directed.Onlytheadministrativeresponsi-bilitiesare delegatedto the fieldunits.
A thirdlandmarkintheeffortstodecentralizationistheimplementationofprimaryhealthcare(PHC), particularlyin ruralareas.Whilethe twoearlierinnovationsare remarkable efforts towards streamlininga "top down"deliverysystem,the institutionof PHChasjuxtaposedgrassrootsparticipa-tionwiththeformerstrategy.Furthermore,PHC entailssubstantivepartici-pationamongthecommunityresidentsindefininghealthandhealth-relatedactivitiesfor their area. Thus, PHC will be separatelydiscussedin thefollowingaction.
C. Primary Health Care (PHC)
BACKGROUND. PrimaryHealth Care, as a strategyfor healthcare, hasbeengiven a lotof attentionandsupportbyboththe publicandthe privatesectors.Itwas formallylaunchedas a nationwidestrategybythe MOH onSeptember 11, 1981. Then, itwas held that the healthservicesextendedthroughPHC can supplementthe publichealth care services that MOHimplementsthroughitsprimary,secondaryandtertiaryhealth care outlets.
The experienceof the privatesector,however,antedatesthe MOHeffort.InJaimeGalvez-Tan'saccount(1986:3),PHChasbeenimplementedbyindependentpractitionersaffiliatedwithhospitalsandclinicsevenbeforethe WHO AlmaAtadeclarationforthe universalapplicationof PHC, Since

HealthServiceDeliverySystem 55
the late 60s, thesedoctorswere: De La Paz withthe KatiwalaPrograminDavao City,Viterboof Roxas City,Macagba of La Union, Flavierof thePhilippineRural ReconstructionMovement,Camposof the Universityofthe PhilippinesComprehensiveCommunityHealth Program, Solon ofPaknaanCebuInstituteof MedicineProjectandWaleofSillimanUniversity.Tan pointedoutthough,that theseeffortswere quitelimitedandwere notfelt nationwideuntil1975. When the Rural Missionariesof the Philippineslaunchedtheirpilotcommunity-basedhealthprograms(CBHPs)indifferentparts ofthe country,the approachwas givenprominentattention.Thereaf-ter, their experienceswere adoptedby the NationalCouncilof Churches(Protestantgroup) in 1977 and by AKAP (seculargroup) in 1978, bothspearheadingnationwideactivities.J. Tan (1986:3) pointsout that theseCBHPs havetheirnationalandregionalcoordinatingbodies.
The chief characteristicof PHC is peopleparticipationin planning,implementingandevaluatinghealthcare activitieswhichare at the sametime integratedintothesocio-economicdevelopmentof the localcommu-nity. Hence, PHC necessarilymerges both participatoryand integrativestrategies.Furthermore,to effectivelyrespondto the needsof the commu-nity,intersectoralcollaborationisemployedto harnesstheavailabletalentsof thegovernment,theNGOs andthecommunity.Sinceitemphasizestheimportanceof engaginginhealthactivitiesat a "cost" thatis "affordable"tothe community,relianceonindigenousresourceslikeherbalmedicinesareencouraged.
PHC hasoftenbeenlikenedtothegovernment'scommunitydevelop-ment(CD)'approachwhichbeganinthe 1950's.Okamura(1986a)and DiazandNierras(1986),however,cautionthattheCD approachmainlyinvolvesthe deploymentofmulti-purposeworkerswhoweregiventhe responsibilityfor organizingthe communityand for makingmembersidentifyfelt needsthatare largelycentrally-directed.PHC,on theotherhand,expectspeopletoidentifytheirownneedsanddemandsindependentof theexpressionsofnationalhealthauthorities.Peopleshouldactuallyget involvedindifferentphases of planning,implementationand evaluation.Okamura says thatparticipationshouldveer towardsthe "attainmentof power in terms ofeconomicand politicalactionand accessto resources.Sucha change inpower relations..,isa necessaryconditionforthestructuralchangesandtheredistributionof resources,wealthandprivilegesthatisimpliedinthe notionof development"(Okamura 1986a:14).
The levelsof participationmentionedby Okamura (1986a:14) andHollnsteiner(1976:11-18),roughlycoincidewiththe threetypologiesof PHCformulated by J. Tan (1986) and Cariho (1986). These are: "community-oriented," "community-based"and "communitymanaged" PHC. Thesetypologiesmaybe usefulinassessingthelevelof PHC implementationbycertainentities."Community-orientedPHC considerscommunityresidentsas beneficiariesof health programs.While voluntaryhealthworkersare

56 VictoriaA. Bautista
tapped from among the members, community organizingis a means tochangepeople'sattitudesenablingthemto cooperatewholeheartedlywithhealthauthorities.A "community-based"PHC,ontheotherhand,considers
community residents as partners in health care and other communityprograms.Voluntaryworkersare tappedas volunteersfor healthservicesand as communityorganizers.Communityorganizingthen becomesanopportunityfor peopleto developleadershipand management.The thirdcategory,a =community-managed"PHC,ischaracterizedbythe activeroleoftheresidentsas managersoftheirowncommunity.Voluntaryworkersareonlytapped as partof the managementteam. Communityorganizingisconsidered the main tool for empowermentand a lastingsafeguard toprotectthe community'sinterests.
STREAMLINING OF MOH STRUCTURETO ACCOMMODATE PHC. Thestructure of the government machinery, has been streamlined to makeparticipatory involvement more effective. Primary Health Care Committees(PHCCs) have been constituted in the different levels of the hierarchybeginning with the lowest political subdivision of the barangay, to themunicipality, the province, the region and then, the national level. TheBarangay Primary Health Care Committee (BPHCC) is envisiQned toidentifyhealth needs, mobilize local resources,manage and monitor healthand health-related action programs of the community. The higher levelcommittees are to oversee, monitor and provide policy framework for PHCplanning and implementation. These are committees for collaborative.efforts since they are composed of representatives from government and
theprivatesector. Incidentally,the PHCcommitteesare atthe same timethe inutrition committees. Regular participation among the different committeemembers is a nagging problem which may stunt the effective implementa*tion of PHC activities (Tortes 1985:156).
The programs are to be implemented by the volunteer workers calledthe Barangay Health Workers (BHWs) who are the indigenous manpowerto be trained in managing community-based health and related projects.These may include management of the Botika sa Barangay, propagationand utilization of herbal medicines, income-generating activities and othercommunity projects, like drainage construction.
EMPIRICAL STUDIES ON PHC EXPERIENCES:PUBLIC AND PRIVATE.Considering the innumerable materials on PHC, the review on its statusshall be made around the following topics: (1) the role of PHC in effectiveservice delivery; (2) a comparison of the performance of government andprivate-sponsored PHC; and (3) the factors affecting the effective implem-e_!ation of PHC andother issues or dilemmassurrounding PHC implemen-tation.

HealthServiceDeliverySystem 57
1. PHC Effectiveness
The studyof Carihoand Associates( 1982)focusedon the interrela-tionshipbetweenparticipationand integratedapproachesas factorsthatcouldaffect the effective delivery of health and health-related services.Program effectiveness was measured in terms of MOH health indicators,people's awareness of the program, clientele coverage and people's levelof satisfaction. Focusingon four development programs (e.g., Makapawa,Sudtonggan Human Development Project, Comprehensive CommunityHealth Program and ProjectCompassion)which altogether combine thesetwin approaches vis-a-vis the sectoral strategy of the RHU, affirms thehypothesisfortwo PHCstrategies.Lesseffectivenessonthepartof the twoother PHC strategies cannot be attributed to the failure of PHC itself since"citizen participation" has not fully materialized and the administrativecomponent for PHC (e.g., personnel) has notbeen sufficient to respond tothe multiple responsibilitiesof an integrated strategy. The study ends witha comment that: "the most successfulare the programs which are based inthe community, touching on the holistic needs of the human person andchallenging the people themselvesto take responsibility for their own stateof health" (Carifio and Associates 1982:224). A sad note to this finding,though, is that these community-based activities have not filtered down tothe more depressed sectorsof the population. The moreaffluent were theones who derived more benefitsfrom these efforts.This argument is furtherconfirmed by Castillo's review and evaluation of participatory approachesimplemented by various development programs. Her interim verdict was:=benefitsfrom participatorydevelopment haveyet to substantially accrue tothe rural population'"(1983:581).
2. Comparing Public and Private-Sponsored PHC
A comparisonof =success"stories in the private and public sectorsimplementing PHC undertaken by Cariho and Carada ( 1986 ) shows themore "impressive" performance of PHC managed by an NGO. The casescompared were the Community GovernmentCollaborationfor the Improve-ment and Maintenance of Health (CGCIMH) administered by Region VIII-MOH and the Makapawa,managedby the RomanCatholic Church inLeyte.
The two institutions emphasized disease prevention as an importantaspect of its health activities. Both also consideredthe citizen's involvementin performing community activities. However, Makapawa is more effectivein itsthrust sincecitizenparticipationis consideredboth asa meansand animportant result.CGCIMH, on the other hand, considers participation as asignificant means to achieve results. The results that are particularlymonitored are those concerninghealth. Thus, Makapawa puts a lot of efforton the process of self-evaluationto enablethe BHWs and the community to

58 VictoriaA. Bautista
reflect on how to effectively implementparticipatorystrategy.Another distinction is the way health is viewed. Makapawa considers
health as an entry point rather than the main problem, unlike CGCIMH'semphasisonhealth. InMakapawa, problemidentification ismore holisticorcomprehensive inscope. The exercise is even infused with =classanalysis"and because of this, Makapawa was held suspect by the past regime forbeing left-leaning.
A comparison of the BHWsefforts shows that in Makapawa, commu*nity organizing is given more attention than by their counterparts inCGCIMH. The BHWs of CGCIMH devoted time on administrative require-ments rather than on community organizing.Consequently,Makapawa hasmore lasting effects on its constituency than CGCIMH. Based on Carir_o's(1986) typology of the different levels of PHC, CGIMH still remains to be"communityoodented"asthetasksor activitiesare largely centrally-directed.BHWs form part of the MOH network and complements the health servicedelivery. Makapawa is nearly "community-managed" since the communitymembers ratherthan BHWstakean active role inprovidingleadershipto thedifferent activities of the community which are beyond health.
3. Factors Affecting Effective Implementationof the PHC Strategy
The factors that are influential indeterminingthe effectiveness of PHCmaybe grouped into the following broad categories: those that concern thecommunity,the BHWs;the development agencyimplementing PHCand thesociety at large. Other issues will also be raised as each broad factor isanalyzed. The factors or issues peculiar to the MOH-PHC and the PHCinitiated by NGOs, will be discussed subsequently.
A major concern in promoting participation among the communityresidents is the adequacy of their social preparation to engage andmanage communityactivities through self_reliance. (Alfiler 1982a, 1982b;Castillo 1983; Diaz and Nierras 1986; Okamura 1986b; Torres 1985;Valenzuela,n.d.).A major stumblingblock to participation in "social prepa-ration" activities may be the economic difficulties among the constituency.
People become moreconcernedwith problemsof self-sufficiency. AsCastillohasonce lamented,"the poordo nothave assetsand yetthe burdenof development is entrusted to them" ( 1983:581).Okamura respondsto thisdilemma by suggesting the need to improve the people's socio-economicstatusbefore expecting their full mobilization for collective action (Okamura1986b:223). Thus, he says, it is not unusual that economic activities takeprecedence over matters related to health in PHC.
On the part of the Barangay Health Workers, it has been a commonconcern to make them attuned to the process of "community organizing"(Alfiler 1982a:89; Cari_o 1986:73; Okamura 1986b:226) rather than of

HealthServiceDeliverySystem 59
deliveringresultsfor healthonly.Thebarangay healthworkers(BHWs)arenot simply health delivery persons, but are also facilitators enabling thecommunities to identify in a concerted manner, their needsand demandsand to workon waysto respondto these demands.The problem is thatsomeprojects implementing the PHC strategy fail to extend to the BHWsenoughflexibility to modify their approaches (Guerrero and Jurado 1983:171 ).They are notadequatelypreparedor encouragedto adopta =self-correcting"process (Alfiler 1982a:85)thus enabling themto modify approachesthatdonot work out well. Other overriding issues raised in different papers(Alfiler 1982a; Cari_o 1986;Okamura 1986b;J. Tan 1986) are: howtheBHW's efforts and commitment may be sustained; what incentives can beprovided to prevent them from dropping out; and should BHWs be paid atall? If PHC encouragesthat health bewoven intothe socio-economic devel-opment of thecommunity, should a voluntary worker be better oft as a multi-purpose worker rather than as a healthworker?
On the part of the implementing agency,there has been an overridingclamor for leaders to be oriented towards makingpeople actively involvedin thedifferent levels suchas planning, implementation andevaluation. Theleaders' commitments could affect the overall thrust of PHC or the mannerinwhich PHCpolicieswill be implemented.In addition,intersectoralcollabo-ration among the different sectorsshould be fully encouraged. This meansshiftingorientation from a "top-down"to a =bottom'sup"processindecision-makingand is realizedby linkingupwith existingorganizations,and, with thecommunity. There is also the persistent problemof development agencieshighly oriented towards Westernized technology instead of exploring andmaximizingindigenous resources.DiazandNierras(1986:140.142 )seetheneed for gathering relevant ethnographic information regarding social,economicand culturalbiasesexistingwithinand betweendifferentcommu-nitiesto comprehendlocalpotentials.
As far as PHC and societyare concerned,the criticalfactor is thepoliticalwillandresolvetoenforcetheprogram.Often,PHCimplementationhas been marredby suspicionsof what it can offer. It has often beenassociatedwith"subversive"work.Thecountry'spoliticaleconomywhichisimpingeduponby Western developedtechnologies,researchesand effi-cientmarketingoutletswhichswamplocaleffortsinhealthtechnology(bothmodernandindigenous)isclearlya problemtoo.To date,drugmanufactureis carriedout by the privatefirms whichimport all basic drugs and rawmaterialsata costof P600millionandprocessthemintodosageform(WorldBank 1984:53). World Bank( 1984:53) furtherreportsthat of the 15,000brandnamesof drugson the marketvery few havetherapeuticeffectsforcommunicablediseases. Publicfactorieshaveinsufficientproductionandtheir manufactureis limitedto experimentalbatchesbecause of qualityproblems.WorldBankalsoreportsthatthe programto promoteindigenousherbaldrugshas notprogressedpast the experimentalstate.

60 VictoriaA. Bautista
The Torres study (1985), contains the most recent comprehensivestudyof the performance of the MOH-PHC, delineated additional problemspeculiar to the government's implementation of the program. Most of theproblems citedhere,centerson MOHbeing largely "community-oriented" inits emphasis rather than being truly resolved in having PHC as "communitymanaged." Hence, the problems detailed in the Torres study concerns theactual processes by which PHC has been implemented. These are:
a. Lack of orientation of Barangay Health Midwives on communityorganization since health service delivery is given primaryemphasis.
b. Lack of involvement of the community in selecting memberswhich will constitute the Primary Health Care Committees(PHCC), The PHCC members are mostly recruited by localofficials.
c. Lack of involvement of the community members in planning andimplementing PHC activities and least of all, in evaluation.
d. Independent planning for the barangays by sectoral agenciesrather than through concerted efforts.
e. Primary attention to health activities inspite of prevalent eco-nomic problems,
f. Less emphasis for non-health activities as suggested by theconduct of monitoring for health activities only.
On the part of the PHCs inspired by NGOs, the salient questions/problems raised are (Alfiler 1982b:20; Cari_o 1986:67-68):
a. What are the measures to be adopted to enable the PHCcommunities to veer towards self-management? What are theindicators that may be adopted to determine if communitiesalready have the capability to engage in planning, implementa-tion and evaluation of its activities?
b. Structures for PHC that give priority alone to process may findless time in setting targets or planning its activities so thatassessment of accomplishments is difficult to ascerlain.
c. Medical practitioners may not be prepared to take a backseatbecausethe problems that areinitially confronted are non-healthin nature.
d. The tendency to viewthe community organizers as patroness ofresourcesmay unknowingly, impinge on the process of inspiringthe emergence of local leadership, thus hampering the road to"community management."
D. Curative versus Preventive and Other Aspects of Health
CURATIVE AND PREVENTIVE COMPONENTS. The emphasis on thecurative component of health isevident in the updatedMOH planfor theyear

HealthServiceOefiverySystem 61
1986 (See Demographic Research and Development Foundation1985:37). The plan has identifiedfive major programs (otherwiseknown asthe Five Impact Programs) such as: Comprehensive Maternal and ChildHealth Program, Tuberculosis Control Program, Control of Diarrheal Dis-eases, Malaria Control Program and Schistosomiasis Control Program.This focus maybe attributed to thefact thatcertain diseases havepersistedover time in spite of efforts to prevent andcontrol them. Based on the MOHdata for the year 1979-1983 (see M. Tan 1986:3-6 ), communicablediseases remained to be the leading causes of morbidity, mortality and -infant mortality. Morbidity patterns have changed minimally in the lastdecadewith the topten changing only in their ranks. The top ten as of 1979-1983 (from highest to lowest) in incidence are: chronic obstructive pulmo-nary diseases, diarrheas, influenza, pneumonia, tuberculosis, malaria,dysentery, measles, cancers and whooping cough, There had been adecreasein the incidenceof influenza, tuberculosis andwhoopingcough buthad alarming increases for chronic obstructive pulmonary diseases, ma-laria, dysenteries and cancers.
Mortality for 1979-1983 is also caused by communicable diseases forthe mostpart, although this cause has declined to a third of total deaths vis-a-vis 40 percent in the late 70s. The top ten causes of death are pneumo-nias, diseases of the heart, tuberculosis, diseases of the vascular system,cancers, diarrheas, accidents, avitaminosis and nutritional deficiencies,measles andchronic obstructive pulmonarydiseases. Thesewere also thetop ten factors in the last decade but only changed in ranks.
Ascertaining infant mortality rate (IMR) is more difficult, says M_Tan(1986:6), Variable figures had been released by the Health IntelligenceService (HIS) and the Planning Division, both of MOH. HIScited an IMR of42 per 1,000 live births for 1983while Planning Division gave 58 for 1985.The top 10causesof IMR citedfor 1979-1983are: pneumonias, respiratoryconditions of the newborn and fetus, diarrheas, congenital anomalies,avitaminosis and other nutritional diseases, birth injury and difficult labor,measles, chronic obstructive pulmonary diseases, acute respiratory infec-tions and meningitis.
The prevalence of communicable diseases despite the fact that sixdiseases are immunizable (like tuberculosis, diptheria, poliomyelitis,
• measles, tetanus neonatorum andwhooping cough), has several implica-tions. One of them is clearly the need to further increase the immunizationcoverage and to improve the support structures for the promotion ol healthand the prevention of diseases (e.g., environmental sanitation, nutrition,child care practices and maternal education) (Cari4o 1986:37-39 ).
An assessment of the budgetary allocation by type of health careshows an increase in emphasis for curative activities in the past twentyyears, based on the data prepared by the Financial Management Services,Budget Division of MOH (1986). In 1966,it only got 31 percent of the total

62 VictoriaA, Bautista
MOH current operating expenditures. By 1976, this increased to 51.6percent; and at present, it is up to 61.2 percent. The remaining amount isdivided among preventive care, research and support services.
However, relying on expenditure patterns alone, may not reveal thetotal efforts extended to the preventive component of health care. SincePHCwas institutedin 1981,the preventivecomponent of health is supposedto be served nationwide through the network of BHWs. While PHC hingeson the mobilization of these voluntary workers to support primary care(which combines both preventive and simple curative responsibilities), thesavings that this effort has brought about should also be considered inanalyzing expenditure patterns. How much would the effortsof a BHW costif MOH relied on their services as a regular employee of the organization?Furthermore, there maybeother resources (materialandhuman) thatcouldbe tapped and can contribute to the overall effort towards the prevention ofdiseases. Thus, relying on MOH expenditure patterns alone may not signifythe mode of financing for PHC activities and may underrate the total thrustfor preventive activities vis-a-vis the curative.
In addition one also has to contend with the other roles of the BHWwhich may have nothing to do with health but may be a precondition forattaining a healthy status. These activities need to be monitored in order tounderstand how they contribute to the well-being of the community. Theirimpact on health may not be felt during the initialstages of PHC implemen-tation since the process of organizing Jsa critical factor in planning commu-nity activities. Thus, it is important to ascertain the level of implementationof PHC in a community to determine if it is already appropriate to evaluateprogram results. If it is only in the early process of being mobilized, it maynot be reasonable to measure the effect on well-being.
OTHER COMPONENTS OF HEALTH. The rehabilitative component ofhealth care is not reflected in the expenditure patterns of the MOH. This isbecause rehabilitation is integrated into the objectives of general healthservicesor otherservice institutions.For example, the 1982National HealthPlan of MOH (1982: 15)for Mental Health considersas oneof its objectivesthe training of physicians, psychologists and social workers in order toprovide a responsive service for early case finding, treatment, as well asrehabilitation of mental patients. These health workers may also refermental patients to proper agencies who can better respond to their needs.
The appeal towards enhancing rehabilitative medicine has beenbrought to public attention when the first National Conference on theRehabilitationof the Disabledwascalled by a privatefoundation in 1974.Onthis occassion, former Secretary of Health Clemente Gatchalian, tried tocorrect the impressionthat rehabilitation isonly fororthopediccases andthementally retarded. He saidthat rehabilitationdoes not only include the deafand theblind andthose withmental defects, it also includes those with heart

HealthServiceDefiverySystem 63
diseases,thediabetics,theconsumptives,thechronicallyillchildrenand theadults past employment stage (1974: 23). He has recognized that thegovernment has not done enough for this sector. The burden had beenshouldered by civic agencies for the most part.
In the same conference, five medical professionals and concernedindividuals spoke about problems and policy issues on rehabilitation(Anselmo 1974;Arzaga 1974; Esguerra 1974;Pangalangan 1974; Reyes1974).The recurrent appeal made by these speakers was for government
to set up a coordinatingbodyorstructure thatwill unity theapproach towardsrehabilitation. This body is to respond to medical, social, educational,psychological and vocational rehabilitation. The ultimate objective is toimprove thequality of lifeof the disabledand to enable them to become self-reliant and productive citizens (Reyes 1974: 104).This could be achievedthroughintersectoralcollaborationof the government,theprivatesectorandthe affected community. It was further stressedthat these efforts should bedirected to benefit the "lowest economicstrata" in thedifferent regionsof thecountry (Reyes 1974: 103).
In 1974,disability ratio was reported to be 1 to every 10citizens of thecountry or a total of 4 million Filipinos (Reyes 1974: 99). O! this total, only3 percent received rehabilitation and the rest did not. The magnitude ofdisability has not changed until 1982 (Periquet 1982:37). In 1982,Periquet(1982:44 ) claimed that the basic problem of disabled persons is theabsence of rehabilitativecenters in rural areas. Hence, the disabled personin a barrio or town hasto goto a city in hisprovinceoranother provincewherethere is a rehabilitative center.
A significant effortof the government to respondto rehabilitationneedwas thecreation of the NationalCommission ConcerningDisabled Personson June 11, 1978. This Commission was mandated to formulate the FirstNational Rehabilitation Plan,to conduct a national disability survey and aninventory of researchdata andstatisticson disability, and to set up a referralsystemto recommenddisabledpersonsto rehabilitationagencies, employ-mentand other pertinentinstitutions.The Commissionserves as a coordi-nating authority for all disability related services and programs.
As a resultofthis directive,a FiveYear DevelopmentPlanon DisabilityPrevention and Rehabilitation was formulated for the year 1983-1987(Benedicto 1985:5).One importantfeature of the plan is the ideaof buildinga community-basedrehabilitationserviceforthedeliveryofprimarypreven-tion and rehabilitationservices. A pilot project was started in Bacolod(Periquet 1982), and subsequently,five more areas in the country(Benedicto 1985:6 ).
In 1984,the NationalDisabilitySurveywascompletedalthoughit hadbeen saddledbya numberof methodologicalproblemswhichhampersonefrom obtainingan accurate pictureof disability(Rodriguez 1984:37 ).Hence,moreup-to-dateinformationonthenatureandproblemsofdisability

64 VictoriaA. Bautista
is necessary in orderto rationallyplanthe activities,services and institutionsthat may be set up by government.
Furthermore, there seems to be a need to establish and implement astructure of a referral system to enable the disabled persons reach out theappropriate agencies.
E. Refiance on WHC, TWC and PHC
Cari_o (1986) reviewed six empirical researches (Carit_oand Associ-ates 1982;Jimenez et al. 1986; Lariosa 1982; MOH 1981; Bicol Study ofMOH in World Bank 1984;Osteria and Siason 1985; Torres 1985),on theutilization of a particular type of health service delivery network for health-related problems. Her conclusion is: "home care particularly by the mothermay be the first resort for most ailments" (Carino 1986:17). Thereafter,traditional, Westernized (or allopathic) or primary health care approach orany combination of these are relied upon. The dependence on a particularhealth network outside the home may be attributed to a number of factorssuch as the social classorigin of the user; rural,urban or regional residence;the perceived severity of illness; the availability and accessibility of thehealth services; and, the cost and acceptability of the treatment and theservice provider (Cari_o 1986:21-23).
A middle or upper classclient is more likelyto approach a professionalservice-provider rather than an indigenous healer_ Indigenous serviceproviders (e.g., faith healers) may only be called upon in case of severeillness. The opposite pattern is noted among the lower classes. Severity ofillness may mobilize the poor to seek out a private physician in the end aftera traditional healer has failed.
A client who resides in an urban area turns to a private clinic, a(government orpuericulture) health center, a government hospital, a privatehospital and a barangay health station, in that order, after home remedieshave been tried out.The rural folk, on the other hand, relyon the BHS first,then the health center, the private clinic and the government/private hospi-tal, in that order of preference.
Another determinant of preference for a type of service is the acces-sibility of the health network. This means that a potential user depends ona service which is nearby or can be reached by transportation. Anotherimportant factor is the quality or characteristics of the providers such asbeing service-orientedor trustworthy.There isalso the economic factor, i.e.,the service is Inexpensive so it is preferred. Thus, no dominant pattern canbe ascertained based on these studies, accordingto Cari_o (1986).No onetype of health care is relied upon. Several factors may influence thepreference of the user for a type of health care.
A distinct preference for Westernized care will be noted when thematerial and human resourcesdevoted to it is examined. A scrutiny of the

HealthServiceDefiverySystem 65
gross value added in medicine arid health in national accounts by Cari5o( 1986:20-21 ) shows that this has generally increased from 1971 to 1985.These accounts include the cost of health and medical care in privatehospitals and clinics, as well as the production of drugs, medical apparatusand other technology, and the construction of health facilities.
However, there is need for caution in making conclusions about theextent of relianceof the community on PHCover WHCor THC. WhileCariho(1986) suggests that the best indicator so far is the attendance by a BHWor the BHS of a given client, there could be reservations about this. First ofall, the nature of health provided through PHC is often promotive and theapplication of cures is for simplecases only. More complicated cases needto be referred to secondary or tertiary outlets. Thus far, the outlets that canrespond to more complicated cases which are attuned to the community-based approach havenot yet been identified. These network may form partof a referral system whose perspectives could be aligned with the goals ofthe PHC strategy, such as for example, recognizingthe utilityof indigenousresources like herbal medicines.At present, it is assumed that complicatedcases are referred by the MOH-BHW to the appropriate tier of the hospitalreferral system, which is largely Westernized or allopathic in approach (M.Tan 1986:11 ).Therefore, it is necessaryto train the other tiers of the referralsystemto the philosophyof PHC so that its approaches could synchronizewith those Ofthe BHW. The networkthat will be trained should be distin-guished from the WHCandTHC providers to make an effective assessmentof how the PHC network has affected the status of the population.
Also, in monitoring reliance on a giventype of service provider, it maybe necessary to sort out the type of ailments or complaints referred to theserviceprovider. For example, primary care cases may rely on a traditionalhealth care approach. Preferences may differ when one goes to a higherlevel of ailment.
The indicator for PHC's effectiveness is qualitatively different fromTHC andWHC approaches. This is because, PHCintegrates orweaves thehealth activities into the relevant socio-economic plans of the community.Hence, indicators for improvement in status can not only rely on the healthcomponent. It should be based on the well-being of the entire community.
F. Focus on Selected Sectors
There are some selected sectors of the population which haveparticularly been focused on in the health program of the government: thewomen and children and the couples about to be married or married.However, there are others which have not been given as much attention,such as those of the work force and the disabled. The latter have beendiscussed in connection with rehabilitation.

66 VictoriaA. Bautista
WOMEN AND CHILDREN. In the Situation Analysis for Women andChildrenin thePhilippines,Cariho (1986),pointsout thatconcern forwomenand children has had a long history. Even during the American period,.thematernal and child health (MCH) program was already in the developmentplan. Cariho laments that in spite of continuing efforts for MCH in post-warPhilippines, "such concern has not been translated into direct benefits tothese important groups" (Cadr]o 1986:32).
To date, the concern for women andchildren constitutes a significantaspect in the MOH Component Plansfor 1988-1992 (MOH:n.d.). Of the fivemajor impact programs to be implemented in the context of PHC, the onesthat have a direct bearing to women and children are two out of five, suchas comprehensive maternal and child health (which includes MCH, familyplanning, nutrition and dental health) and control of diarrheal diseases. Theother three impact programs are malaria control, T.B. control and schis-tosomiasis control.
1. Comprehensive MCH Program
The comprehensive MCH program has been instituted in view of thefact that mothers and children constitute about 62 percent of the 1985populationof 54,378,000. Ironically,their health conditionstill remains to bea problem ("Five Impact Programs"MOH 1986). Infant mortality rate is 58per 1,000 live births in 1985 while maternal mortality rate is 0.81 per 1,000live births. These deaths had been largely attributed to nutritional deficien-cies of mothers and children, low percentage of completed dosage ofimmunization of children and prevalence of communicable diseases. Thespecific strategies to address these problems include: maternal care,breastfeeding, establishment of under-six clinic, expanded program onimmunization and nutrition program. Family planning program is alsoanother strategy but will be considered in a separate section as this is aprincipal program that targets couples as well. Another program is hilottraining, which is a support strategy in order to improve the provision ofmaternaland child care.
a. Maternal Care
Maternal care entails the prenataland postnatal supervision of moth-ers. Prenatal service includes the identification of "high risk cases" forappropriate r_ferral and obtaining vital care such as monitoring bloodpressure and weight, examination�palpation of the abdomen and determi-nation of hemoglobin. Other services include giving advices on the impor-tance of regular check-ups, nutrition and family planning. These servicesmay be extended by health professionals or by trained hilots. Postnatalservices entail blood pressure check-up, physical examination, referral for

HealthServiceDeliverySystem 67
internalexamination,advicesondiet,breastcare,infantcare,immunizationandfamilyplanning.
BasedontheMOH NationalHealthSurvey(NHS)in198I,theprenatalservicesoftenrenderedtoatleast82 percentofthemothersarebloodpressuretaking,physical/abdominalexaminationandweighttaking.Hemo-globindeterminationisratedtheleastbecauseoflackoffacilitiesandtrainedpersonneltodo it.Thisreport,suggeststheextensionofsuchservicesasfamilyplanning;preparationfordeliveryand lactation;and,servicestoimprovenutritionalstatusandmentalhealth.Thesearesuggestedbecauseofproblemsofbirthspacing,breastfeedingpracticesandlackofpreparationfordelivery.Moreskillsarealsoconsiderednecessarytocleterminehighriskfactorsinpregnancyandlabor(MOH 1981:49-51).
Postnatalservicesincludebloodpressuremonitoringand infantfeeding.The lowestpercentageforservicereceivedisforinternalexamina-tion.Thissuggeststheneedformorehealthe_Jucationofthemothersontheimportanceofthisservice(MOH 1981:52).Itwas suggestedintheNHSthatthenurseormidwifebe allowedtoperformthisfunction.
b. Breastfeeding
The promotionof breastfeeding is now being encouragedas partof thecomprehensive MCHprogram.This includes among others,the provisionofrooming-in of newborns after delivery. Breastfeeding is considered to beeconomical and also protects the children against diarrhea and otherdis_eases.Cariho's (1986) situation analysis of rooming-in indicates thatmuch has yet to be done in terms of changing attitudes and institutionalpractices. It appears that hospitals are averse to the idea of rooming-inbecause of: (1) the unfounded belief that the infant will be exposed toinfections that may be transferred by the mother and (2) the higher cost ofmaintaining personnel (Carii_o 1986:28-29 ). Then, of course, there is theproblem of contending with huge multinational corporations which engagein all sorts of gimmickryto increasethe patronageof manufactured infantformula(M. Tan 1986: 12). A billonbreastfeedingstillawaitspassagelongafterit had been submittedfor legislationin October1984,
c. Under-Six Clinic
The Under-Six Clinic is a special type of clinic geared towardsprovidingpreventive,promotionaland curativeservicesto preschoolers.The specialfeatureofthisserviceisthe involvementof mothersinmonitor-ingthegrowthandnutritionofthe0-6 yearsoldthroughtheuseofthegrowthchart and homebased record,The initialimpactof thisstrategymay begleanedfrom the fact that 73 percentof the motherswho deliveredtheirchildrenin under-sixclinicsbreastfedtheirchildren(Carif_o 1986:39 ).A

68 VictoriaA. Bautista
problem that has been identified with the implementation of Under-SixClinics is that mothers still perceive that it is the health workers' task tomonitor the children's growth rather than assuming this responsibility asMOH has stipulated.
d. Immunization
The prevalence of preventable and curable diseases as causes ofmorbidity, mortalityand infant mortalityseems to indicatethat immunizationstill has to be effective!y waged to bring about significant results. While anExpanded Program of Immunization has been launched since mid-1976,three (tuberculosis, measles and whooping cough) of the immunizablediseases are still in thetopten leadingcauses of morbidity;two (tuberculosisand measles) are among ten leading causes of mortality; and, one(measles), among the top tenleading causes of infant mortality, in spite ofthe gains in the coverage of immunization, high incidence of deaths haveincreaseddue to inadequate provision of support activities such as environ-mental sanitation, nutrition, child care practices and maternal education(Cari_o 1986:39 ).
e. Nutrition
The nutrition program is concerned with the improvement of .thenutritionalstatusof "vulnerablegroups" likethe infants, pre-school children,pregnant and lactating mothers. This is to be undertaken through suchactivities as food assistance and through the referrals of malnourished pre-schoolers to nutrewards or feeding centers.
In a situation analysis of the nutritional statusof mothers and childrenin the Philippines by Florentino et al. (1986), it was noted that malnutritionstill plagues infants and young children below four years 01dand thenfollowed by older pre-schoolers, school children, pregnant and nursingwomen in that order. Sincethe 1950sno significant change hastaken placeinterms ofthe nature of nutritionalproblemsthatafflict these differentgroupsas a whole. These problems that have recurred over time are: protein-energy malnutrition (PEM), iron-deficiency anemia, as well as deficienciesin Vitamin A and iodine. While Florentino et aL, note that improvementshavebeen made from 1978to 1982in the diets of the children,these are stillway below the acceptable standard. Avitaminosis and other nutritional de-ficiencies had been observed to be included in one of the top ten leadingcauses of child mortality which may also have caused infectious diseases.
Florentino et aL claim that the critical factor that affects malnutrition isnot the inadequacyof supply for food but the "low effective demand for food"among those with poor economic resources. Hecalls to attention the plight

HealthServiceDefiverySystem 69
of "nutritionally high-risk groups"which mustbe givenpriority like:deep ruralbarangays, slash-and-burn farmers, small/hired fishermen, the unem-ployed/underemployed, and those with large families and lowly educatedmothers (Florentino et al. 1986:3).
A measure directed at the marco level is to alleviate the critical foodsupply and demand. At the micro level, Florentino et al., suggest conver-gence of services upon highly focused and mutually agreed upon targets(Florentino et al. 1986:3).
2. Control of Diarrheal Disease
Another impact programthat directlyaffects the young is the control ofdiarrheal disease. The rationale for prioritizing this program is becausediarrheal disease has consistently been one of the leading causes ofmorbidity and mortality for the last twenty years (MOH 1986). It is thesecond leading cause of death in the 0-4 years age group. In 1984, themortality rate for this agegroupwas 1.33 per 1,000population (MOH 1966).It was further reported by MOH that 7 out of 10 deaths resulted for thisparticular age group due to diarrhea.
The chief strategy adopted to control diarrhea is the introduction ofOral RehydrationTherapy (ORT). MOH, however, reports that this indige-nous technology has not been widely accepted by some communities, aswell as by some doctors themselves. There is still a strong preference forWesternizedtechnology likeanti-diarrheals andantibiotics for the treatmentof diarrheal diseases. Another factor is the limited access of physicians tothe ORT supply of MOH.
TARGETTING COUPLES. Family planning is a particular program thattargets the pre-marriage groups and married couples of reproductive age.While the Commission on Population (POPCOM) claims that it targets thepre-schoolers, youth, program influentials and program professionals, thecouples are thedirect recipientsot the benefitsthataccruefromthis program(Jamias 1985:100 ).
Through the Outreach Project, the population program has deployedabout 3,000 personnel and 50,000 barangay service point officers (BSPO)(Jamias 1985:11 ). This project is a collaborative effort of both POPCOMand the local government. The project has a community-based and clinic-based service delivery system because it has tapped the services of bothvoluntary workers such as the BSPOs and the regular workers paid by thegovernment.
A state of the art review had been made on the performance of thefertility program by Perez and Cabildon (1985). In their paper, results of 8surveys had been analyzed to cull general patterns and trends concerningthe fertility program. These surveys were: the National Demographic Sur-

70 VictoriaA. Bautista
veys (NDS) conductedin 1968,1973 and1983; Republicof thePhilippinesFertility Survey (RPFS) in 1978; the National Acceptors Survey (NAS) in1976; the 1972 Survey of the then Bureau of Census (now the NationalCensusandStatistics) and the Community Outreach Survey (COS) in 1978and 1980.
Perez andCabildonconcludethat while therehas been a decline in theusageof contraceptive methods by the target groups (the married couplesof reproductive ageor married women of reproductive age), an increasingrelianceon moreeffectivemethodshad been observed.
Factorsassociated with contraceptive usage include those related tothe socio-economiccharacteristicsof the user,the levelof urbanizationandextent of modernization of the user's community, and the appropriateknowledge and favorable attitude towards family planning. These variableswere positively related with contraceptive use.
Some programvariables which positivelyaffected the effectivenessofthe programwere the accessibilityofthe family planningclinicsandeffectiveperformance of the outreach workers and the BSPOs.
The non-outreachprojectinputswhichsubstantially influencedcontra-ceptive usage was accessibility of medical facilities and barangay healthstations.
Non-correlatesof program effectiveness were the mass media, thefield workers of participating agenciesand IEC materials.
A significantfinding is that the community-basedworkers and privatedoctors who directly communicate with the couples generate better resultsthan those who depended on IEC inputs. Further, between the non.volunteer and the volunteer workers, the latter were more effective inservicingthe clients.
On the whole, the paper pointsout the need to:1. increase the overall contraceptiveprevalence.2. restructure the systemof delivering information materials, par-
ticularly the IEC strategiesimplemented by the service deliveryworkers.
A more recent study had been undertaken by Varela(1986)todetermine the roleof religiousbeliefs and fertility control policies of govern-menton thefamily planningbehaviorof samplemarriedwomen of reproduc-tive age. They weredrawn from three religiousgroups: Catholics, Iglesia niCristo (INC)and Muslims. Varela'sstudy showsthat fertility control policiesof government contradictwith the religiousdoctrines of the Catholic and theMuslim groups. Both favor family planning using natural means only. Themore liberal group is the INC whichdoes notsee any doctrinal impedimentin the practice of family planningstrategiesrecommendedby government.On the whole, these three different sectors believe that their religiousdoctrines influence their family planning behavior. That is, the Muslimsdonotpracticefamily planningasmuchas the INCsdo.The Catholic group also

HealthServiceDeliverySystem 71
sharesthesentimentoftheMuslimsbutarenotas"hard-core"(Varela 1985:276 ) becausetheCatholic'sresponseis affectedbysuchfactorsas placeof residence,age andincome.More specifically,the urban,the averagedage, and highincomeCatholictendsto be a contraceptiveuserthan therural,young,and old,and lowincomecounterpart.On the basis of thesefindings,the policyagendaraisedbyVarela were:
1. the need to involvethe religiousgroupsin formulatingfertilitycontrolpolices;
2. the importanceoffittingIEC strategiesto the religiousbeliefsofthe differentsectors.
3. the need to launcha massivecampaignregardingfertilitypoli-cies to enhancefamilyplanningbehavior.
An evaluationofthe PremarriageCounsellingProgram(PMCP) whichtargetscouplesabouttobe marriedrevealsthecontributionofthe programin improvingknowledge,attitudeand potentialpracticeof familyplanning(KAP) (Bautista 1984b). Three factors stand out in terms of positivelyaffectingKAP. These are: the clients'socio-demographiccharactedstics(beingeducatedand female) andthe counsellor'seffectiveperformance(e.g., being betterprepared,disseminatedIEC and reliedon visualaidsduringthe counselling).The beneficiarieswithhigheducationalattainment,thoseexposedtobetterpreparedcounsellors,thosewhoreadIECmaterialsandthosewhowereexposed to morevisualaidsin PMCP hadhigherKAPscores.
Somekeypolicyagendaconcerns:(1)thepossibilityof exemptingtheeducatedgroupfromPMCorsegregatingthemduringPMCsessionssothattheywillnotget bored,(2) theneedto stepupcampaigntowardsthe maleswhodid notperformas wellas thefemales,and (3) the needto make IECmaterialsmore relevant.
To summarize,the general patternfor performingbetter after the•exposuretothefamilyplanningprogramisbeingeconomicallyandculturallymoreadvanced.Then, there is alsothe administrativecomponentswhichhaveto bemonitoredas theysubstantiallyinfluencethe gainsthat maybeachievedina program.
WORK FORCE. The sectorthat has not been given muchattentionandsupportinourdevelopmentalprogramisthe laborforce.Inspiteof thefactthat thissectoris vital in the productionprocess,governmentinstitutionshavenotgivenadequatebudgetarysupportandsufficientandwell-trainedmanpower to implementa programto upgrade this sector'shealth andsafety. Hence, participantsfrom governmentand private sectorsin theSeminar-WorkshoponOccupationalHealthandSafety(OHS)sponsoredbythe U.P. Instituteof PublicHealthand the Federal Republicof Germanyissueda statementof concernin 1983 regarding"OccupationalHealthandSafety in the Philippines".The manifestodeoriedthe problems in the

72 VictoriaA. Bautista
implementation of OHS programs and standards such as: lack of logisticsupport; lack of coordination and support among government and privateagencies; lack of adequate information/education and training on OHSamong health workers, employers, top decision-makers and the generalpublic; inadequate research activities on OHS; low priority given to OHS insmall to medium-scaleindustries andamong agricultural workers; and, lackof a continuing and systematiceducation and training on OHSwith empha-sis on small and medium-scaleindustries (UP-IPH and Federal Republic ofGermany 1983:34 ).
The current support systems in OHS are government agencies likeMOH, Ministry of Labor and Employment, Bureau of Mines and Geo-Sciences and Fertilizer and Pesticides Authority. They work closely withnon-governmentalorganizations like SafetyOrganizationof the Philippines,Federationof Farmer'sAssociationand PhilippineOccupational and Indus-trial Medical Associations (Parrado 1983:69).
Some academic institutions cooperate by conducting research andtraining in OHS. These major institutions are UP-IPH, and the toxicologysection of the Department of Pharmacology of the University of the Philip-pines - College of Medicine. It was pointedout by Reverente,Jr. (1985: 28)that the areas for field research in OHS is very wide. These include theidentification of "man-made"hazards peculiar to certainwork-related activi-ties. Reverente, Jr. (1985: 28) stresses the need to find and adopt tresholdlimitvalues (TLVs)which is locally applicablefor some chemicals emitted inthe production process. These can be the basis for formulating controlmeasures to safeguard the health of the labor sector.
An important development (Reverente Jr., 1985:27) that may help inforging concerns forOHS is thecreation of the NationalTripartite Council forthe Improvement of Working Conditions which initiates, coordinates andimplements projects involving OHS. The Council has established thePhilippine Foundationfor Occupational Health and Safety.
In 1984, a National Tripartite Conference on Improving WorkingConditions and Environmentwas held.The participantsof this Conference,composed of workers, employers and government officials discussed themajor problems regarding OHS in the Philippines. This is the non-compli-anceof employers regarding healthand safetystandards (MOLE: 1984:39-40). The firms had been able to get away with these violations because ofthe suspension of routine monitoring. This conference also reiterated theproblem of lack of sufficient information and statistics on diseases. Thegroup recommended the courses of action adopted by the 1983 seminarworkshop on OHS sponsored by UP-IPH and the Federal Republic ofGermany. These were:
1. creation/designation of a national coordinating center for re-search and training;
2. conducting a sustained, coordinated and effective information

Hea/thServiceDeliverySystem 73
and educationalprogram on occupationalhealth and safetythroughoutthecountry;
3. linkingup and coordinatingOHS activitiesand servicesof allsectoralorganizations,entities,and individualsconcerned;
4. creatinggreaterawarenessof OHS standards,rulesand regu-lationsandpertinentlegislationsor decrees inthis respect;
5. urging the integrationof OHS in the school jcurricula fromelementaryto the collegelevel;
6. seekingstdcterenforcementof sanctions,existingandprospec-tive, to discourageviolationsof OHS standards;and,
7. callingupontopdecisionand policymakersto promulgateclear-cut, consistentpolicieson OHS foreasiercompliancebythoseaffected,especiallyamongsmalland mediumscale industries.
Reverente,Jr.(1985:29-30) claimsthatOHS ispresentlyinthe =take-offstage"inthe Philippinesbut '1hereisa needto bringoccupationalhealthto a levelof sophisticationequalto if notbetter thanthatfoundin industri-alizedcountries."
IV. POLICY PROBLEMS/ISSUES
Based on the previousdiscussions,this sectionwill highlightsomebroadpolicyproblemsorissueswhichmayconstitutetheagendaforpolicyresearch in the area of structures and interventionsfor health servicedelivery.
A. From a Pluralistic to a Unified Health Program
The experienceof the Philippineswith regard to structuresandapproachesin healthservicedeliveryshowsthe dominantpolicyof plural-ism.There is no unitarystructureresponsiblefor extendingpublichealthservices.Indeed,thisapproachiscommendablebecauseitenablesvariousentitiesto respondto healthproblemswhichgovernmentmay not be ableto copewith.The existenceofvariousserviceoutletscanalsobe helpfulintermsof keepinghospitaladministratorsontheirtoesinmaintaininginstitu-tionalstandardslessthey be swampedbybetterinstitutions.
However,itseemsimperativethatthe nationalhealthministryformu-late a unifiedor comprehensiveprogram for health which takes intoconsiderationtheavailableresourcesbothfromthepublicandprivatehealthdeliverysystems.This,therefore,impliesthe needforintersectoralcollabo_rationin orderto rationallyplanthe distributionof resources- manpower,technologyand health facilities.Intersectoralcollaborationmayfacilitateinteractionandexchangeof information.Governmentcan, thus,plan outwhereto locateitsresourcesandnotonlyduplicatetheinputsof theprivatesector.

74 " VictoriaA. Bautista
While the IRP has mandatedthat the structurefor developmentalplanningof nationalprogramsconsiderintersectoralcollaborationin thedevelopmentcouncils,these bodieshave notfullytappedthe participationof the privatesector.The PHCapproachmayhavestronglyemphasizedtheimportanceofpublic-privatesectorcollaboration,yet,thecompositionofthedifferent PHC committeesis the same as the nutritioncommitteesof thedevelopmentcouncils.The nutritioncommitteesare made up mostlyofmembers from the differentsectoralagencieswho give more priorityinimplementingtheir respectiveprogramconcerns.
Accurateand up-to-datestatisticsis needed on public-privatesectordistributionof resourcesandhowtheseresourcesmatch the needs ofthepopulation.It is remarkablethat some NGOs have already taken theinitiativetolocatetheirservicesinthedepressedareaswhichhavenotbeenadequatelyservedbygovernment.Thiswasa steptakenbyMakapawa,forexample.
Respondingto the plightofthe ruralandpoorFilipinosremainsto bea naggingproblem.Howto addresstheirneedsisstillanopenissue.Healthresources (manpower and facilities) are still predominantlylocated inbarangaysnearthe bigtownand cities.Accordingto Cari5o (1986:74):
What is needed is some focused targetting. This meansmaking differentiations among areas according to certain socio-economic andgeographic conditions,popu/ation size, avai/abi/-ity and competence of service providers, communityprepared-ness and disease patterns and draw targets according/y.
The recenteffortofthecurrentgovernmenttoinvolvetheprivatesectorin itsplanningexerciseisan importantachievement.Similareffortsmay beencouragedandmustbedocumentedtodeterminethe gainsthathavebeenmade inthecollaborativeeffort.
B. PHC as a Strategy
Primary Health Care (PHC) is an effectiveapproach to generatingmorelastingand commendableachievementsinthe healthand well-beingof thosewho are involvedinit.PHC meritscontinuingconcernand interestonthe partofthegovernment,theprivatesectorandthe community.SomepolicyissuesthatconcernsPHC includethe following:
PHC OR COMMUNITY BASED? It has been a generalobservationthatPHC as a strategy has not only encouragedthe formulationof healthactivities.In fact, in some areas, non-healthactivitieshave taken prece-dence over the health needs of the populace, In particular,copingwithproblemsof economicself-sufficiencyis prevalentand has become the

Hea#hServiceDeliverySystem 75
primordialconcernof the community.In fact, some incomegeneratingactivitieshavestartedfirstevenbeforerespondingtotheproblemsofhealth.
One criticalissuethatcan be raisedis, howadequatelyhasthe BHWrespondedto thenon-healthneedsof the population?Howeffectiveis theBHW in addressingnon-healthproblems?Does the trainingof the BHWprovideappropriateskillsto reactto non-healthproblems?IstheBHW abletotapothermanpowerresourcesintheneighborhoodwhichformpartofthereferralsystem,whetherformallyorinformally?Ifthereisanexistingreferralsystemfor health, coulda similarone also be structuredfor non-healthactivities?
Since non*healthconcerns (particularlyeconomic) are often thepriorityproblemsof the community,does it meritimplementinginsteadacornmunlty-basedstrategywherehealthisnottheonlypriorityservicethatisplannedtobedelivered.Rather,thetypesofactivitiesto be implementedwillbebasedontheactualproblems,needsanddemandsarticulatedbythepopulace?
Thisthrustmeansa majorrestructuringofthe entirebureaucracybutifthiswillmakethe bureaucracymoreresponsive,thenitmaybeworththeexercise. Developmentalplanningshould hinge on the expressionsofpopularwillandthiswillentailmakinga decisionintermsof activitiesthatanswerthe people'splightwhichare notonlyin health.
COMMUNITY-ORIENTED OR COMMUNITY-MANAGED PHC? It seemsthat the MOH-PHC strategyhas not substantiallydeparted from the CDapproachwhichhadbeen launchedinthepast.This is because,the MOH-PHC hasremainedto be "community-oriented"ratherthanbeing"commu-nity-managed."Activitiesare largelycentrally-plannedand directed andleavevery littleroomforthe BHWto be innovative.Infact, healthactivitiesaretheonesmonitoredbyMOH andthisfocusgivestheBHWsmorereasontoemphasizehealthratherthanotheractivities.ThedifferencebetweentheBHWandtheBarangayDevelopmentWorkerundertheCD approachisthatthe latter is a regular employeeof the national ministry.However, theservicesrendered by both are determinedby their respectivenationaloffices.In fact,thevery rationaleforthe institutionof PHC alreadysuggeststhatthe PHC networkis moreofan adjuncttothe nationalhealthministry'sdelivery system. PHC is emphasizedto augmentcommunity'smeagerresourcesfor health insteadof 1ulfillingthe objectiveof =empoweringthecommunity"to enable them to managetheir own affairs and therefore,becometrulyself*reliant.
The questionis, howwillingare the membersof the bureaucracyindelegatingsubstantiveresponsibilitiesatthe local level?Howpreparedarethe differentcommunitiesfor self-management?What are the necessarycomponentsfor self-management?Assumingthatthe communityhas thecapabilityfor self-management,when willthe developmentagency know

76 VictoriaA. Bautista
how to exit?
BARANGAY HEALTH WORKERS. The BHWs are the critical frontliners inthe health service delivery system. They are not only expected to respondto the health needs of the populace but also of the other needs of thecommunity. They are also entrusted with community organizing in order toconsolidate the residents' efforts towards planning and if possible, imple-menting and evaluating the performance of certain activities that they haveidentified. Hence, the BHW is expected to be versatile in responding to themultiple needs ofthe population.Some recurrent issues loom, resulting fromthe BHW's experience with what they can do as against what they shoulddo.
1. BHW and Barangay Development Worker (BDW)
What seems to be a critical responsibility of the BHW is communityorganizing if PHC is for "community management" rather than merely"community oriented." From this effort will flow the opportunity for inspiringcommunity members to define what activities need to be pursued andwhocan implement these activities. If the objective is to make the community"manage" their own affairs, the voluntary worker should not "direct" theneeds of the peoplefor health needs only. The BHW is only a facilitator. Butthe Torres (1985: 145)studyshows that BHWs were trained extensively forthe delivery of health services rather than organizing.
Hence, thequestion that maybe raised is: Dowe only need a BHW ora Barangay DevelopmentWorker (BDW)? If the BHW can notably respondto the multiple needs of the population, should the BHW's training beredirected to one that prepares him/her as a multi-purpose worker? Orbetter still, should a Barangay Development Worker be tapped to comple-ment the BHW's responsibilities regarding health care? The BDW willperform a separate function of community organizing while the othersectoral voluntary workers (e.g., the BHW of MOH, the Barangay NutritionScholar of the NNC and the Barangay Supply Point Officers of POPCOMform part of the referral system of the BDW. The referral system mayconstitute both the public and the private sector network and can beconsulted for sectorally-linkedproblems. Then, the othervoluntary workerscan devote full time attention to their roles for which they are adequatelytrained than assuming multiple responsibilities.
Re-directing the responsibilities of the BHWs towards multiple rolesmay not entail broad restructuring of the bureaucratic machinery. This isbecause the national health ministry can still perform the function ofcoordinating and providing support structures to enhance the capabilities ofthe BHW in community organization and trouble-shooting for sectorally-linked problems. On the other hand,assigning a BDW who will perform thesole function.ef¢Qmmu_tyorganization entails a biggerstructural modifica-

HealthServiceDeliverySystem 77
tion.This maymean,assigning to anotherministry(e.g., the Ministryof LocalGovernment) the responsibilityof coordinating, supervising, and providingsupport structures for volunteer community organizers. The issue is: Howwilling is the top leadership to encourage participatory strategies in thedifferent sectors of the bureaucracy? This is because the aftermath of theefforts of the BDW is expectedly in the direction of greater communityawareness andgreater community expressionof a need for managing theirown affairs. The effort of a BDW may bring to a wider scale the notion ofparticipatory management and may require more intense collaborationamong the various agencies of government with particular sectoral con-cerns. Second, collaboration is also necessary between government, theprivate sector and the community.
2. Incentives for BHWs
Another recurrent issue that has been raised concerns how thevoluntary workers' efforts can be sustained. In the past PHC efforts, aprevalent problem was the fast turnover of BHWs. Hence, it is important toask what incentives can be offeredto maintain the enthusiasm and the com-mitment of the BHWs so that the efforts poured intotraining them will not bewasted. What are the implications of giving remunerations to BHWs?
3. Concern for Process and Results
It seems that pastefforts of governmenthad givenprimary attention tothe effects or results ratherthan of the process involved in implementing thePHC strategy. The common indicators pertainto the attainmentof a healthystatus e.g., morbidity, mortality, availability of potable water, etc. Very littleattention is given to the dynamics by which the participatory strategy hadbeen implemented suchas: what activities hadbeen inspired by the BHWsto encourage citizen involvement in planning, implementation and evalu-ation of health and health related activities. What is the quality of citizenparticipation - its scope, duration and intensity.'?What factors influence thequality of citizen participation?
Also, as the implementationof the participatory strategy is evaluated,it can also be askedif the participants engage in circumspection to be ableto "correct" or make improvements in the process.To what extent have thecommunity members been involved in self-analysis is another significantmatter.
4. Participatory Evaluation
Of the three activities - planning, implementation and evaluation -participatory evaluation is the leastconsidered of all. The activity that hasbeen most participatory is implementation, then followed by the planningprocess. Some questions that may be raised are: what are the methodsapplied to effect participatory evaluation? What is the comparative experi-

78 VictoriaA. Bautista
enceof thepublicandtheprivatesectorsinparticipatoryevaluation?Whatlessonscanbe learnedfromtheeffortsofNGOs inparticipatoryevaluation?Is the result of participatoryevaluation effectively utilized for a "self-correcting"processin PHC? What are the requirementsof part!cipatoryevaluation?
WESTERNIZED TO PHC RESOURCES/TECHNOLOGY. In spiteof thefactthattheMOH-PHCstrategyhasemphasizedtheneedto adoptorutilizeindigenousresourcesfor health,there hasbeena resistanceonthe partofsomemedicalprofessionalsto applyindigenousstrategies.For example,the applicationof ORT for diarrhealdiseaseshas been difficultbecausedoctorsstillprefer manufacturedmedications.Even citizensthemselvesseemto preferpackagedmedicationsthanherbalmedicines(Tortes 1985:150).
Training at all levels seem to be necessary to correct attitudesregarding the value of indigenous resources. Medical professionals whosetraining have been largely influenced by a Western curriculum put a lot ofemphasis on science-based technology. As J. Tan claims (1986: 11-12):"The medical, dental, nursing and midwifery curricula are still Westernoriented and primary health care, preventive and promotive health are justgiven lip service by our health education institutions." To be able to fullyeffect PHC, medical professionals should be re-trained to appreciate andrecognize local resources which may have a scientific basis (e.g., herbalmedicines).
The community should also learn from an information campaignregarding the value of indigenous resources for health care. This is ofcourse,difficultto wage becausethe socio-economicsettingwhich givespremiumto importedand Western-developedtechnologyneeds to bereeducatedto appreciatethe value of what is locallyavailable, it may besupportiveto PHCtechnologyif controlmeasuresare legislatedconcerningdrug companies that rely heavilyon imported materials.
Furthermore,the indigenous workers should be retrained so that theirservices can be tapped and attuned to modes that are scientifically accept-able.The task of the development agencythat givespremiumto PHC ratherthan to a Westernized mode of health care is, therefore, onerous. Givingpremium to PHC requires:
1. Assessing the local indigenous resources and determiningwhether they are scientifically acceptable;
2. Disseminating andcampaigning for the utilization of "validated'indigenous resourceswhich may be less expensive and moreabundant than manufactured/processedresources.
CENTRALIZATIONTO DECENTRALIZATION.The political-administrativeframework within which PHC operates has to be contended with as the

Hea/thServiceDefiverySystem 79
frameworkcoulddeterminehowPHCobjectivescouldbefullyrealized.It isapparentthatPHC asa strategycanonlyfulfillitsthrustundera decentral-ized structure.This is because PHC hingeson the participationof thecommunitytowardsdevelopmentalplanning,implementationand evalu-ation,Acentralizedstructuremaynotenablelocaldecisionstobe achievedbecause substantiveresponsibilitiesare lodged in the central body orauthority.Thus, the matterof grantingcommunityresidentsfullopportuni-tiesfor participationdependsuponwhetheror notdecentralizationwillbeputto effectinthe governmentalmachinery.Thenofcourse,care shouldbemadeindistinguishinga policystatementfromhowitisimplemented.Inthepast regime,decentralizationhadbeenan overridingtheme inthe politicaladministrativemachinery,butcentralistpracticeshad been manifestedbythe nationalauthorities,
Some policyquestionsthey may be asked are: What decentralizedformsorstructuresaremostfacilitativeofa PHCstrategy?Howwillingisthepoliticalleadershipto shiftto these forms?What is the experienceof theautonomousregions(IXandXII)in realizingthe PHCstrategyas againsttherestof the regions?
C. Curative to Promotive/Preventive/Rehabi/itativeMedicine
The recurrenceof certaincommunicablediseasesin spiteofthe factthat theseare bothcurableand preventableseemsto pointtothe need formore substantialattentionto promotiveand preventivehealthcare. Itmaybeaskedtowhatextentgainshadbeenmadetopromotehealthandpreventdiseases.Someinitialstudieshadbeenundertakento assessthe impactofimmunizationas a strategyto preventdiseases.Inspiteofincreasesinthecoverage of those immunized,a lot has yet to be done to wage thiscampaign,What supportstructuresare necessaryto maximizethe effortsfor universalimmunization?What improvementshad been made intermsof fullillingthe promotiveand preventivecomponentsof healthcare? Towhat extent has PHC as a strategycontributedto the promotionandpreventionof diseases?
The rehabilitativecomponentalso needsstrengtheningas an aspectof healthcare. Muchhas yet to be done in termsof rationallyplanningforrehabilitation,No up-to-datestatisticsisavailableregardingthe magnitudeof disability- physical,mental,socialand psychological- whichwillbe thebasesfor formulatinga comprehensivedevelopmentpolicyfor rehabilita-tion.Also,thedisabledgroupmustbewillingto participateinthissurveysothat theirneeds andproblemsmay be identified.Some initialefforts hadbeeninitiatedforparticipatoryrehabilitationtocomplementthe rehabilitationnetworkof the government.An assessmentof the achievementsof theseeffortsmustbeunderstoodanddisseminatedsothatothersmaylearnfromthese experiments.

80 VictoriaA. Bautista
D. Focus on Other Sectors
Women, children and couples constitute the sectors that had beengiven prominence in the past development plans. With regard to women, ithasbeen noted that they perform a critical role in terms of making decisionson the health practices in the family. Women have also been tapped asBHWs. It has been askedwhether children(Torres, 1985) and the youth canalso be involved in these activities? What are the potentials of children andthe youth as voluntary workers? Do children and the youth get involved inparticipatory decisionmaking in PHC?
In targettingcouples as a sectorto realizethefamily planningprogram,women are the ones usually askedaboutthe family planning practices to beadopted or currently adopted in their respective homes. Is this becausewomen arethe onesoften directly involved inthe practiceof family planning?What is the role of the male in family planning? In a study assessing theknowledge, attitude andpotential practice of family planning after exposureto premarriage counselling, males did not perform as well as the females(Bautista 1984b).Is this because malesdo nothave an equal responsibilityin family planning and therefore, not as keen to respond to governmentprograms?
There are other sectors that had notbeen given as much attention likethe labor group (and the disabled sectors which were discussed underrehabilitation).The labor sectoris the onedirectly involved in the productionprocess and whose health and safety must be safeguarded. Some gaps inthe knowledge concerning this group are: the causes of diseases andillnesses peculiar to aworking environment; theways/strategies in respond-ing to these ailments; the mechanics of promoting, preventing and curing"man-made" ailments; the effectiveness of the existing structures in coordi-natingand regulatingefforts foroccupational health andsatety; and, the roleof the employers in safeguarding the health and safety of the laborers.
ASthese different sectors are studies, it may beworth asking: Hasthepoor and underprivileged segment been able to obtain an equal sharein thebenefits from thedifferentprograms formulated?lf"health for all" isthe mottothat guides authorities, health should not only be the prerogative of the rich,urban and educated Filipinos. It should tilter to the rest of the populace,particularly the marginalized Filipinos.
E. An Interdisciplinary Model to Assess the Effectiveness of Structuresand Interventions
In analyzing the factors that affect the performance of the differentstructures and strategiesfor health, the lessonthat may be learnedfrom thereadingsis that these factors are multiple andcomplex. Thus, it is necessaryto be guided by a model or perspective that considers various factors such

HealthServiceDefiverySystem 81
as: those pertainingto the community,other characteristics pertainingto thedevelopment agency, those pertaining to the actual mechanics of imple-mentingthe structuresand strategies,the existenceof related agenciesthatfulfill the same objectives as the development agency, and the ecologicalcontext (e.g., its political economy) in which structures/strategies areembedded. This model is presented in Figure 1. Since the components ofeach factors are varied multiple, an interdisciplinary approach could behelpful in comprehending the subject matter.
FIGURE 1. ASSESSING THE EFFECTIVENESS OF STRUCTURES/INTERVENTIONS FOR HEALTH
Characteristics ofthe Community
Other Characteristics __
of the DevelopmentAgency
Structures/ I_, Interventions --_ Effectiveness
i (Ideal vs. Actual)Related Agencies
Ecological Variables
F. Participatory and Integrated Approaches at All Levels
The considerablegains obtainedin the adoptionof the participatoryand integratedapproachesinthe areaof healthcanserveas a challenge!0thedifferentsectorsofgovernmentandthecommunity.Whataboutembrac-ing these strategies in the deliveryof services at all levels? These ap-proachesgenerate self-relianceinthecommunity,are lessburdensometogovernmentand bringmore lastingresults.

82 VictoriaA. _utista
BIBLIOGRAPHY
Alfiler, Ma. Concepcion."PrimaryHealth Care and Related Approaches:A Reviewof PhilippineResearchesand Experiences."Paper prepared for the U.P.Management EducationCouncil'sSeminarWorkshopon AdministrationofHealth Services:Focus"on Primary Health Care, held at Asian InstituteofTourism,March5 & 6, 1982.
. "ComparativeCase Studiesof CommunityBasedProjectsinHealthand FamilyPlanning:An IntegratingReport."U.P. Collegeof PublicAdmini-stration.Preparedfor the PopulationCenter Foundation(1982).
."FactorsthatPromoteorDeterPopularParticipationinDevelopment:ThePhilippineExperience."PhilippineJouma/ofPub/icAdministration XXVII,No. 1, 1983.
•"PrimaryHealthCare inthe Philippines:A CloserLookata Policyanda Program."Paper prepared for the Commissionon Audit'sPolicy AuditSeminar,State Auditing=ndAccountingCenter,QuezonCity,September3-14, 1984(mimeographed).
Amor,BonifacioL (ed.). TheDisabledin Nation Building.Reportofthe FirstNationalConferenceon the Rehabilitationof the Disabled.Quezon City: PhilippineFoundationfor the Rehabilitationof Disabled,Inc, 1974.
Angara,Andres."ObservationsonRural HealthCare DeliverySystemsinthe Phil-ippines, 1978." World Health Organization Regional Office for WesternPacific,December1978.
Anselmo, Romualdo. "PsychiatricRehabilitation." Proceedings of the NationalConference on the Rehabilitation of the Disabled. Quezon City: PhilippineFoundationfor the Rehabilitationof the Disabled,1974.
and Wilfredo B. Carada. "ParticipatoryDecentralizationand PrimaryHealth Care: A Comparisonof Governmentaland Non-GovernmentalAp-proaches."Preparedfor the FirstProjectReviewMeetingonDecentralizationfor RuralDevelopment,21-26 April,Chiengmai,Thailand,1986.
Castillo,Celia. How Participatory is Participatory Development: A Review of thePhilippine Experience. Manila:Philippineinstitutefor DevelopmentStudies,1983.
Colmenares, Pinky,."The AccessibilityLaw Would Make it Possiblefor DisabledPeopleto Mov"eAround."Concernfor the Disabled Filipino.(October-Decem-ber 1984)5:4.
De Guzman, RaulP. "Towardsa More EffectiveCoordinationof Planningand Ira-plementationof DevelopmentPrograms/Projects:The IntegratedAreaDay,"

Health Service Delivery System 83
opment (lAD) Approach," Paper prepared for the National Conference of LocalGovernment Executives, 31 January-5 February, Philippine Plaza and 24th
World Congress of Local Authorities (IULA), Philippine International Conven-tion Center, Manila, Philippines, 1979.
De Jesus, Jose P. and Carmencita T. Abella. "The Primary Health Care Strategy:Reorienting the Bureaucracy for Partnership: A Case Study on InstitutionalInnovations in the Health Sector." Prepared for the Asian and Pacific Devel-opment Centre,
Demographic Research and Development Foundation, "An Assessment of thePopulation Health and Nutrition Programs, 1978-1985," Manila: DRDF, 1985.
Diaz, Manuel P. and Rose Marie Nierras. "Popular Participation in Primary HealthCare: Directions for the Social Scientist" Participatory Approaches to Devel-
opment: Experiences in the PhJTippines.(eds.) Trinidad Osteria and JonathanRokamura. Manila: De La Salle University Research Center, 1986.
Arzaga, Maria Paz B. "Vocational Rehabilitation," Proceedings of the NationalConference on the Rehabilitation of the Disabled. Quezon City: Philippine
, Foundation for the Rehabilitation of the Disabled, 1974.
Bautista, Victoria, "Structure of the Philippine Administrative System." Manila: U,P.College of Public Administration. (mimeographed). 1984.
, "An Evaluation of the Premarriage Counselling Program." Manila: U.P.
College of Public Administration. (For the Population Center Foundation),1984,.
. "Structures for Health Service Delivery in the Philippines: The Case o!
the Primary Health Care Approach." Paper presented in a Workshop Confer-ence on "Delivery of Public Services in National Development: Problems, Al-ternative Solutions and Structural Adjustments," Asia Hotel, Pattaya, Thai-
land, july 1-5, 1985.
Benedicto, Julita. "A Special Report on the 1984 NCCDP Accomplishments."Concern for the Disabled Filipino, (January-March 1985). 4:1.
CariSo, Ledivina. "Policy Directions for Health inthe 80s." Philippine Journal of PublicAdministration, (April 1981) 25:2.
and Associates. Integration, Participation and Effectiveness: An Analy-sis of the Operations and Effects of Five RuralHealth Delivery Mechanisms.Manila: Philippine Institute for Development Studies, 1982.
."Situation Analysis for Women and Children in the Philippines: TheHealth Policy and Management Sector." Manila: U.P. College of PublicAdministration, 1986.

84 Victoria A. Bautista
Jimenez, Pilar, et al. Health and Nutritional Problems and the Utilization of Health
Services. Vol. I (The Situation Among Pre-schools in Depressed Metro ManilaCommunities). Manila: De La Salle University Research Center, 1986.
Kleczkowski, Bogdan M. et al, System Support for Primary Health Care. Geneva:World Health Organization, 1984.
/
• National Health Systems and Their Fteorientation Towards Health forAll: Guidance for Policy Making, England: World Health Organization, 1984.
Lariosa, Teresita Ramirez. "Household Seeking Behavior and Expenditure Patternsfor Primary Health Care in Cabagan, Isabela." Manila, 1984,
Ministry of Health• National Health Survey 1981, Manila: MOH, 1981
• "National Health Plan for 1982." Manila: MOH, 1982_
"'Five Impact Programs." Manila: MOH. (mimeographed 1986.
. "Utilization of Rural Health Services: Republic of the Philippines•"Document for the Regional Seminar on the Use of Rural Health Services,Manila, January 20-26, 1986.
. "Status of PHC Implementation." (mimeographed).1986.
• "Ministry of Health Budget, 1946-1986." Prepared by Financial Man-agement Service Budget Division. 1986.
, "Component Plans, 1988-1992." Manila: MOH. (mimeographed).
Ministry of Labor and Employment. Humanizing Work: Proceedings of the NationalTripartite Conference on the Improvement of Working Conditions and Environ-ment. Manila: Ministry of Labor and Employment and International LaborOrganization, 1984,
National Census and Statistics Office, Philippine Yearbook• Manila: NCSO, 1985.
National Economic and Development Authority and United Nations Children's Fund."Mid-Term Review: Second Country Program for Filipino Children." Organizedby NEDA in cooperation with UNICEF, Quezon City, July 24-25, 1985.
Ocampo, Romeo and Elena Panganiban. "Local Autonomy and Centralism in thePhilippines." Paper presented at the International Studies Association Con-vention, Atlanta, Georgia, March 27-31, 1984.
, "Local Government and Community Development in the Philippines:Participation and Performance in the Local Political System, Revised Proposalfor Comparative Research." Presented at the Comparative Research Project

Health Service Delivery System 85
Meeting held at Seoul, Korea October 23-25, 1984, at Seoul National Univer-
sity, 1984.
Okamura, Jonathan. "Popular Participation in Development in the Philippines." Par-ticipatory Approaches to Development: Experiences in the Philippines (eds.)Trinidad Osteria and Jonathan Okamura. Manila: De La Salle UniversityResearch Centre, 1986.
• "Towards a Strategy for Popular Participation in Development." Par-ticipatory Approaches to Development Experiences in the Philippines (eds.)Trinidad S. Osteria and Jonathan Y. Okamura. Manila: De La Salle UniversityResearch Centre, 1986.
Osteria, Trinidad S. and Ida M. Siason. Alternative Strategies for Financing PrimaryHealth Care: Lessons from Six Case Studies. Manila: United States Agencyfor International Development, 1985.
and Jonathan Okamura (eds.). Participatory Approaches to Develop-ment: Experiences in the Philippines. Manila: De La Salle University, 1986.
Pangalangan, Evelina. "Social Rehabilitation." Proceedings of the National Confer-ence on the Rehabilitation of the Disabled. Quezon City: Philippine Founda-tion for the Rehabilitation of the Disabled, 1974.
Parrado, Nelsie. Occupational Health and Safety in the Philippines: Analysis andRecommendations. Proceedings of a multi-sectoral seminar-workshop onOccupational Health and Safety in the Philippines, sponsored jointly by theU.P. Institute of Public Health and the German Agency for Technical Coopera-
tion, Baguio City, November 28-December 3, 1983.
Perez, Aurora E. and Josefina V, CabJgon. "Contraceptive Practice in the Philip-pines: A Synthesis," Philippine Population Journal (March 1985). 1:1.
Periquet, Antonio O. The Rehab Column. Quezon City: National Commission
Concerning Disabled Persons, 1982.
Pilar, Nestor, et al. "Social Development Policies and Programs in the Philippines:Focus on the Delivery of Health Services. "PhilippineJoumalofPublicAdminkstration, Philippine Journal of Public Administration (July-October 1978). 22:3&4.
Population Center Foundation. "A Progress Report of the Implementation of thePrimary Health Care Approach in the Philippines." Prepared for the Ministry ofHealth, Manila: PCF. 1983.
Presto, MarJs, "Lecture Series # 6: Ensuring Filipino Workers' Health and Safety."Health Policy Development Consultation Series. Quezon City: Health ActionInformation Network. 1986,

86 Victoria A. Bautista
Pujalte, Jose. "Our Poorly Distributed Physician Population." Utilization of RuralHealth Services: Republic of of the Philippines, Document for the RegionalS_minar on the Use of Rural Health Services, Manila, Jan. 20-26, 1986.
Reodica, Carmencita. "Survey of Non-Governmental Organizations in PHC." Ma-nila: Ministry of Health, 1983.
Reverente, B.R, "Current Situation on Occupational Health in the Philippines,"OccupationalHealth in Developing Countries inAsia, ed. W.O. Phoon & C. N.
Ong. Tokyo, Japan: Southeast Asian Medical Information Center (SEAMIC).1983.
Reyes, Tyrone. "Medical Rehabilitation." Proceedings of the National Conference onthe Rehabilitation of the Disabled, Quezon City: Philippine Foundation for theRehabilitation of the Disabled. 1974,
Rodriguez, Thannie. "Commitment is the Key to Success of B.P. 344." Concern forthe Disabled Filipino. (October-December 1984), 5:4.
Sanchez, Augusto, et al. Work Accidents 1983. Manila: Bureau of Labor andStandards, Ministry of Labor and Employment. 1985.
Tan, Jaime Galvez. "Primary Health Care: Health in the Hands of the People." HealthPolicy Development Consultation Series. Quezon City: Health Action Informa-tion Network, 1986.
Tan, Michael L. "State of the Nation's Health." Health and Policy Development Con-sultation Series. Quezon City: Health Action Information Network, Task ForcePeople's Health. 1986.
Tortes, Amaryllis. "Documentation of Specific Area Experiences in Primary HealthCare: Phase I1." Manila: Population Center Foundation, For the Ministry ofHealth. 1985.
United Nations Children's Fund/World Health Organization (UNICEFNVHO).
"lnterregional Consultation on Primary Health Care in Urban Areas." Manila,Philippines. 7-11 July, 1986.
University of the Philippines = Institute of Public Health and German Agency forTechnical Cooperation Occupational Health and Safety in the Philippines:Analysis and Recommendation: Proceedings of a Multi-sectoral SeminarWorkshop on Occupational Health and Safety in the Philippines. Sponsoredjointly by the U.P. Institute of Public Health and German Agency for TechnicalCooperation, Baguio City, November 28-December 3, 1983.
Valenzuela, Amanda B, et aL "Activities of Midwives in Primary Health Care andStatus PHC Implementation According to Midwives." Manila: UP-IPH.(mimeographed).

Hea/th Service Delivery System 87
Varela, Amelia P. and Associates."ReligiousBeliefs and FertilityControlPoliciesandFamilyPlanningBehavior."Manila:U.P,CollegeofPublicAdministration.(mimeographed).1985.
WorldBank, "Population,HealthandNutrition:A SectorReview,"ReportNo.4650-PH, TwoVolumes (January13, 1984), WorldBank. 1984.

Demand for Health Care
Panfila Ching *
I. INTRODUCTION: NEED, DEMAND ANDTHE PURPOSE OF DEMAND ANALYSIS
Distinguishingdemandfromneed isa matterof great importanceforpolicymaking.Shouldsociety'sresourcesbe allocatedaccordingto thehealthneedsof itsmembersor accordingto theirdemand?To answerthisquestion,the conceptsofneed anddemandmustbe clear.
Is need greater or lesserthan demand? Either case could be thesituationina country.Inthesame manner,a particularhealthservicecouldhavethe same situation.The pointis thatthe levelsof needsanddemandmay notbe equal.Certain needsare never translatedintodemand whilecertaindemandsareactuallynot needed.
Matthew( 1971) clearlydistinguishedneedfromdemand:
The 'need' for medical care must be distinguished from the 'de-mand' forcareand fromthe useof servicesor 'utilization'.A needfor medical care exists when an individual has an illness ordisability forwhich there is an effectiveand acceptable treatmentor cure. It can be defined either in terms of the type of illness ordisability causing the need or of the treatment or facilities fortreatment required to meet it. A demand for care exists when an
* Assistant Professor, School of Economics. University of the Philippines.

90 Panfila Ching
individual considers that he has a need and wishes to receivecare. Utilization occurs when an individual actually receivescare. Need is not necessarily expressed as demand, and de-mand is not necessarily followed by utilization, while, on the otherhand, there can be demand and utilization without real underly-ing need for the particular service used.
The relationship between demand and need has been presented byCooper ( 1974 ) in the following diagram:
WANT DEMAND NEED
A slateofhealthAnindividual's Thoseofhiswants assessedas inownasessment thattheindividual needof treatmentofhishealth convertsinto bya medicalslate-- his demandbyseeking practitioner.wantforbetter _ theassistanceofa -.-e Notalldemandshealth, medicalpractitioner, willbecomeneeds
andnotallneeds"feltneeds" "expressedwants" willfindexpres-
sionasdemands.
Mooney((1986) has come upwith a more detailed layout of Cooper'sdiagram based on the argument that the source of all demand is want,although not allwants are expressed as demand. Some wants and demandsare judged as needs, but not all needs are contained in demands or wants.Medical practitioners may define a particular need which is neitherwant nordemand. Mooney thus views want, demand and need as follows:
WANTS DEMANDS NEEDS
._ Demandedwants _ Demandedandwanted
needs
Undemandedwanted
S needsUndemandedwants Undemandedunwantedneeds
All these arguments however pointto the need for an efficient resourceallocation. Policymakers are interested to know how competing claims onhealth care ought to be met. Two approaches to these problems have beensuggested. One is to leave the market alone, that is, let health care be
distributed among competing claims by the willingness and ability to pay amarket cleadng price. The other is to entrust to the state the responsibilityfor ensuringthat sufficientresnurces were made available to meet society'sneeds as assessed by medical practitioners.
j,

Demand for Health Care 91
The secondapproach is prevalent in developed countries wheremedical care has been considered a "right". Developing countries, on theother hand, do not even have the luxuryof guaranteeing their populationsthe right not to starve (Ricardo-Campbell 1982 ).
The second approach was based on a misconception of the nature ofthe need for health care. The concept of sickness as an absolute andunambiguous state led to the false hope that unmet needs could beeliminated. In practice, need proved to be a relative concept capable ofalmost infinite interpretationby bothpotential patients and medical practitio-ners. There is nofinite allocation of resources that could meet allhealth care
needs. According to Cooper ( 1974 ):
Need seemingly tends to grow in line with provision, as doctorsreact to any expansion in supply by realigning their conception ofneed further along the possible continuum.., like an iceberg, themore resources devoted to melting it, the more need seems tofloat to the surface.
If need is likelyto result inmisallocation of resources, what then shouldthe state do if it does not wish to adopt the first option, that is, leave themarket alone? The answer is government planning according to demand.
This is not to say that need should be neglected. Need is actuallyincluded in planning according to demand. Need is generated by theincidence of illness, while demand is generated by the incidence of illness(need) and other factors (such as income and price). So, need is only onefactor affecting demand for health care. To plan for future utilization ofservices, demand rather than need must be projected (Sorkin 1975; P.Feldstein 1979 ).
To integrate the discussions so far, it would be helpful to keep in mindthe figure of Lee ( 1983 ):
NEEDS of thecommunity$
FELTNEEDS i.e., thatpercentageof the
totalneedsofthecommunity
whichareperceivedbyitsmembers
DEMAND i.e.,thatpercentageofthefeltneedsofthecommunitywhichareexpressedbyindividualstothehealthsen/ices
UTILIZATION the interactionofdemandandsupplyfactorsto determinethequantityandqualityofcaregiven

92 PanfilaChing
One purposeof studying demand is to enable planners to bring abouta change in utilization if they sodesire. This could be done by analyzing thefactors behind demand and their extent. Moreover, with separate studiesmadeon these factars, future utilization may be projectedmore accurately,for various population groups and among areas.Another important reasonfor demand analysis is the removal of impediments to access to services.Forthis interest, patient demand must be identified and explained.
Forclarity inthe discussion, Fuchs' (1972) definition of health servicesis being adopted. He defines health services thus:
1. Labor personnel engaged in medicaloccupations such as doc-tors, dentists, nursesandother personnelworking directly undertheir supervision such as practical nurses, receptionists andorderlies.
2. Physicalcapital:the plantand equipmentused by these person-nel, for example, hospitals and x-ray machines.
3. Intermediate goodsandservices:for example, drugs, bandagesand purchased laundry services.
I1. A SELECTIVE REVIEW OF FOREIGN LITERATUREON HEALTH CARE
A selective review of studies made on countriesother than thePhilippinesis herebypresented.The focusis ontheconceptualmodelsondemandanalysis.
A. Simple Utility-Maximizing Mode/
Earlierresearchesonhealthservicewerebasedonthisconventionalmicroeconomicmodel.Themodelviewsthe consumeras makinga rationalchoiceundera budgetconstraint,thatis,medicalcare isa product- butnotparticularlyunique- availableto the utility-maximizingconsumer.
Althoughmany studiesdid not mentionthis model,they did use itspredictions.While manyof these studiesstartfromthe specificationof ademandequation,suchan equationis actuallyderivedfromthe firstorderconditionswhichcharacterizetheutility-maximizingframework.The modelpredictsa negativeown-priceeffect and a positiveimpactof incomeonmedicalconsumption,The work of Andersenand Benham( 1970) repre-sentsone of the earliestresearchesemployingthe traditionalmicroecon-omic model.
B. Utility-Maximizing Mode/with Time Cost
Usingthe precedingutility-maximizingstructure,Acton( 1975, 1976)

DemandforHealthCare 93
incorporatedtime costsintothebudgetconstraint.To consumegoodsandservices,notonly moneypricesbutalsothe amountof time are involved.]]me is valuedat the wage rate.
Of interestto Actonwas the impactof time as insuranceor welfareprogramsdrivethe money priceof medicalcare to zero. He predictedthatdemand becomesrelativelymore sensitiveto time as money price falls.Throughthisprediction,he suggestedthat comparedto userswho payformedicalcare, usersof free medicalserviceswillbe more sensitiveto timecosts.
Anotherpredictionisontheunlikelyinfluenceof wageandnon-wageincomeon demand.Grantingthat medicalservicesare normalgoods,anincrease in non-wage income will lead to an unambiguousincrease indemand.Therationaleisthatpeoplewithhigherabilitiestopaywillbuymoreof all normal goods. However, an increase in wage incomecannot bedetermineda priori. Anincreaseinwageincomeraisesnotonlyincomebutalsothevalue oftime.The riseinincomewillmeanincreaseddemand,butthe riseinthevalueoftimewillmeandecreaseddemandfortime-intensiveactivities.Thedominantoffsettingforcesamongthesehowever,cannotbeascertained.
C. Household Production Model
In thismodel,the consumeris assumedto maximizeutilityovertwocommoditiesproducedinthe homeusingas inputsmarketgoodsand theconsumer'stime. The innovatorsof the model are Holtmannand Olsen( 1976 ) basedon earlierworkson Holtmann(1972 ) and Becker( 1965 ).
Holtmann and Olsen applied the model to the demand for dentalservices.The modersdistinctivefeature is its replacementof the simplenotionthat consumersderiveutilitydirectlyfromthe consumptionof dentalserviceswiththe moreplausibleassumptionthatthe sourceof utilityisthecharacteristicproducedbythese services,dental hygiene.Peopledo notbuygoodsandservicesforthepleasuretheygive. Instead,peopleare altermorefundamentalobjectsofchoice,objectswhichare producedbygoodsand services,objectscalledcommodities,objectssuchas dentalhygiene.
HoltmannandOlsengavepredictionssimilartotheprecedingmodels.For example, money price and time are also negativelyrelated to thedemandfordentalvisits.
D. Human Capital Model
Takingnoteofthe Mushkin(1962) expositioncomparinghealthandeducation,1Grossman( 1972a, 1972b) extendedthehouseholdproduction
(1)Healthprogramsincreasethenumbersintheworkingforceaswellasthequality

94 PanfilaChing
theoryto developa modeltreatingthedemandformedicalservicesas bothan investmentand a consumptionactivity.
Grossmanstartedwiththeassumptionthatthecommodityconsumerswishtopurchaseisgoodhealth,andnotmedicalservices.Medicalservicesaredemandedonlybecausetheyareinputstotheproductionofgoodhealth.It is clear therefore that the demandfor medicalcare is derivedfromthemorebasicdemandfor health.
Consumersinthe Grossmanmodelhavea demandfor healthfor tworeasons.First,healthis a consumptioncommodity;it makesthe individualfeel better. Second, it is an investmentcommodity;a state of health willdeterminethe amountof time availableto a person.Consumersdemandgood healthbecausea decreaseinthe numberof sickdayswilldeterminetheamountof timeforleisureandwork.Thereturntoan investmentinhealthis the monetaryvalue of thedecreasein sickdays.
The modelhasthe followingpredictionswithrespectto wage,educa-tionandage.The higherthewage rate,thegreaterthedemandformedicalcare.Thispredictionfollowsfromthefactthatthehighertheperson'swagerate,thegreaterthemonetaryvalueofan increaseinhealthydays.'A-I-so,thepersonwhoispaida highwageratewouldratherbuymoremedicalservicesthanincreasethetimehedevotesto preventivemeasureswhen producingthe commodityhealth.Thus,demandfor healthcare servicesis hypothe-sizedto be positivelyrelatedto wage rate.
Educationishypothesizedtohavea negativeeffectonthedemandformedicalcare2. More highlyeducated people are expectedto be moreefficientinproducinghealth,thuspurchasingfewer services.
Age and demandfor medicalservicesare predictedto be positivelyrelated.Asa personages,the rateatwhichhisstockof healthdepreciatesincreases.Overthe lifecycle,peoplewilltry to offsetthe increasedrateofdepreciationby increasingtheiruseof medicalcare.
E. Human Capita/Mode/with Coinsurance
Newhouseand Phelps( 1974, 1976) expandsthe precedinginvest-mentmodelofGrossmanbyincorporatingPhelps'(1973) theoryofdemandfor insurance.
Assertingthatthe theoreticallycorrectmoneypriceof health service
oflabor'sproduct.Educationchieflyaffectsthequalityoftheworkers.(2)Unitsofqualitychangethroughhumancapitalformationbyhealthprogramscannotbedefinedastidilyasunitsofeducationembodiedinthelaborforce.(3)Wehavenoindexesofdifferencesinearningsreflectinggradationsinhealth,(4)Educationinvestmentisadevelopmentalprocesswhichferretsoutandencouragesnativetalent.Heall_programsseektopreventa hostileenvironmentfromkilling,
Thissituationholdsifthedemandforhealthinvestments(orthemarginalefficiencyofcapitalschedule)isinelasticwithrespecttothepriceofhealthinvestments.

DemandforHealthCare 95
is thecoinsurancerate timesgrossprice,PhelpsandNewhousehavethefollowingresults.Oneis, if thecoinsurancerateis lowandthe time priceishigh, as in free publicclinics,the time priceelasticityis relauvely high.Anotheris,itthecoinsurancerateishighandthe timepriceislow,asinhomevisits,the money-priceelasticityis relativelyhigh.
PhelpsandNewhousehavecarefullybuilta realisticmodel.However,the model is relevant for developed countriesbut not for low-incomecountrieswhere only a small percentageof the populationis covered byinsuranceandwherepatientcost shadngis notas widespread.
F. The Inducement Hypothesis
Traditionaleconomictheory assumesthat pdce and outputmay beexplainedbytheinteractionof Independentsupplyanddemand.Therehasbeena challengetothisassumptioninthe marketformedicalservices.Thealternative demand-shiftor inducementhypothesisstates that medicalpractitionershavetheabilitytogeneratedemandfortheirservices;orstatingitdifferently,they havetheabilitytoshiftthepositionofthepatients'demandcurve.
Empiricalstudiesaboundwiththis supplier- induced-- also calledprovider- determined-- utilization(Monsrna 1970; Evans 1974; Fuchs1978; Kohn and White 1976).To make the empiricalworksconvincing,anumberof studiesevenattemptedto formulatea microeconomictheoryofconsumerand producerbehaviorcompatiblewiththe hypothesis(Green1978; Richardson 1981).
Literatureon the inducementhypothesisindicatesthat doctorsdorespond to incentivesinherentindifferentpayment systemsanddo influ-ence demand. This behavioris shownto be true whether doctors areconcernedwithincomemaximization(Monsma1970), orwithsocialstand-ingandthe esteemwithwhichpatientsregardthem (Richardson 1981).
The reasonfor so muchdiscussiononthe influenceof providersonconsumersisthepolicyimplicationofthephenomenon.The introductionofinsurance,whichactsto reducethecostofhealthcaretothepatient,willleadto increasedutilizationandthus,pressureonscarcehealthresources.Theappropriatepolicythen is to launch strategiesto affect the behaviorofproviders,insteadof consumers.
Just how, important is the inducement hypothesis?Newhouse(1981) cited evidencewhich showsit is not that important;Fuchs andNewhouse( 1978)pointedoutthedifficultyofshowingthatitexists,letaloneestablishingitsmagnitude.Butthe debatecontinues.
G. Demand in Low.Income Countries
Unlikedevelopedcountries,householdsinlow-incomecountrieshave

96 PanfilaChing
certain characteristicswhichcall the specialattentionof researchers. Forexample, the system of sewerage, the cleanliness of drinking water, thestateof health knowledgeandbeliefs are quite different here.These specialconditions are accoqnted by Heller ( 1976), whose model is considered acomplicated version of Acton's.
Hellerdefineshealth needasan inversefunction of healthstatuswhichin turn is determined by economic as well as environmental factors. Aconsumer maximizes utility over the consumption of three kinds of goods:preventive health services, discretionary medical care (care beyond theminimum necessary level), and all other goods.
An innovation of Heller is the definitionof necessary anddiscretionarycare as two different goods. In so doing, he did not have to resort to aninvestment model just to incorporate need.
He predicts that demand for preventive services would fall if theirmoney or time price rises,andsimilarly for discretionaryservices. However,demand for necessary care may not fall with pdce increases.Consumptionof other goods would be sacrificed in order to be able to purchase thenecessarymedical services.
Iii. STUDIES ON PHILIPPINE HEALTH CARE
Demand analyses on Philippinehealth care have been based onpdmary date gathered by multidisciplinaryhouseholdsurveys. Rimando(1976) utilizeda multipurpose surveyconductedintheprovinceof Laguna
in 1975. Paqueo (1977) employedthe GINA survey -- a 1975 nationalsocioeconomicsurveyofPREPF (Population,Resources,Environmentandthe PhilippineFuture).Akin,GuilkeyandPopkin(1981) usedthe1978 BMS(BicolMultipurposeSurvey),conductedinBicol,oneofthe poorestregionsof the Philippines.Subsequently,the same Bicoldata wasutilizedbyAkineta/. ( 1985 ) andChing( 1985, 1986).
The five works mentioneddo not have the same unit of analysis.Rimando ( 1976 ) and Paqueo ( 1977 ) worked on the household.Akin,Guilkeyand Popkin( 1981) andAkinand hiscolleagues(1985 ) preferredto studyindividuals,inparticular,childrenandadults.Althoughsheusedthesame Bicoldata, Ching( 1985, 1986) investigatedthe family3 instead.4
These five studiesinvestigatedthe use of varioustypes of healthservices and determinedthe factors associatedwith use. Their modelsfollowa general demand systemwhereinthe choiceor use of a service
= Familyisdifferent fromhousehold.A householdiscomposedof themembersof thefamily,and also residentdomesticservantsand otherpersonswho may be livingwith thefamily.
' Samplesize of Rimandois 570; Paqueoused 2902 households;Akin, GuilkeyandPopkinhad411 childreninneed;Akinandcolleagueshad401 adultsand566 children;Ching,379 families.

DemandforHealthCare 97
dependsonthe relativemoneyandtimecostsassociatedwiththe service,theconsumer'sincome,anda setofcontrolvariables(social,demographicand biological).
The resultsof Rimandosuggestthat incomelevel, insurancecover-age, educationandbeliefsof mothers,as well as demographic(age) andphysiological(felt needs)characteristicsof householdsdo havesignificantimpactson theirdemandfor typesof health services.Onthe otherhand,Paqueofounda bigeffect of residenceon demandwith ruralhouseholdsbeingat a disadvantage.The sickchildrenstudiedbyAkin, GuilkeyandPopkinwere influencedbydistance,incomelevel,mother'seducationandtime costs.
Akinet aL (1985) arrivedat an interestingresult.Economicvariableshadso littleexplanatorypowerinanyofthe models.Income, cashand timecosts were not important predictorsof choice of health service. Theimplicationthe authorssuggestisthatpovertyandcostshadvery littletodowithfailureto use existingservices.Other factorssuchas educationandperceivedseriousnessof illnessplayedstrongerrolesin determiningusepatterns.
Ching(1985) alsofoundsimilarnon-significanceofeconomicfactors.Afterdealingwithmulticollinearityand othereconometricproblems,Ching( 1986) obtaineda numberof significanteconomicfactors,mostlyprices.This indicatestheinterdependenceof healthfacilities,whichare organizedintoa referralsystembutwhichatthe sametime is a competitivenetwork.Nevertheless,theresultsdo notinvalidatethefindingsof Akinet aL (1975)thatpovertyandcostshadvery littletodowithfailuretouseexistingfacilitiesandservices.
IV. FACTORS AFFECTING DEMAND FOR HEALTH CARE
A. Income
Higherincomefamiliestend to availmoreof healthservicesbecausethey are ableto affordthe cost. However,sincethese familiesare usuallyableto affordpreventivecare andcouldthusbehealthier,theycan therebyreducethe use of health services.This is the so-calleddouble effectofincome.
While the effectof changesinincomeonthe demandfor a particularhealthservicecannotbe accuratelypredictedinadvance,thereis nodoubtthat expenditure(quantitytimes price) for health services, as a whole,increaseswithincome.Whatis lessclear iswhetherthe demandfor healthservices is elasticor inelastic,i.e., whetherthe percentageincrease inexpendituresis more, or less, than the percentage increasein income.Researchers suggestthat the elasticity is below unity (Andersen andBenham 1970: Paqueo 1977; Rosette and Huang 1973; Feldstein andSeverson 1964).

98 PanfilaChing
One should distinguishbetween wage and non-wage income.Grossman'sinvestmentmodel( 1972a, 1972b)generatedthestrongpredic-tion that non-wage income shouldhave no effect on demand. It alsodeterminedan unambiguouspositiverelationshipbetweenwage rate anddemand for healthcare.s The study of Newhouse and Phelps (1974,1976 ) empiricallysupportsthe investmentmodel. It needspointingout,however,that althoughthe signsoftheirelasticitiesareconsistentwiththeinvestmentmodel,theabsolutevaluesofthe elasticitiesare lessthanunity.
Under the consumptionmodel,6 there is a positive relationshipbe-tween non-wageincomeand demandfor healthservices.7 However,theeffectsof a changeinthewage ratecannotbedeterminedapriori becauseof offsettingforces.An increaseinwage rate producesan income effect,whichactsto increasedemand. Italsoproducesa priceeffect-- by raisingthe opportunitycost of time -- which reducesdemandfor time-intensiveactivities.Acton( 1975, 1976) found thatthepriceeffectof a wagechangedominatesinthe demandfor publiccare andtheincomeeffectdominates
Under the investment model, the commodity "good health"can beproducedby goodsandservicesproducedinthe marketaswellas bythe timedevotedto preventivemeasures.In this framework,the demand for health care is derivedfrom themore basicdemand forhealth.
Consumersdemand"goodhealth"becausea decrease in the numberof sickdayswillincreasethe timeavailableforworkand leisure;the retumsto an investmentinhealth is themonetaryvalueof thedecreasein sickdays. Therefore,thehigherthe wage, the greater themonetaryvalue ofan increasein healthydays, therebyintensifyingthedesireof consumersto investin health.
When producingthecommodity"goodhealth,"a consumerwhoispaida highwage ratewillsubstitutepurchasesofhealthcareservicesforhisowntime, i.e.hewouldratherbuymorehealth services (such as consultinga doctor for multi-vitamins)than increase the time hedevotesto preventivemeasures(suchas preparingnutritiousmeals morefrequently).
= The formalconsumptionmodelisdevelopedintermsof atwo_]oodutilityfunction.Thetwo goods that enter the individual'sutilityfunctionare: health services,h, and a compositegood,X. Peoplepay inbothmoneyandtimeforeach good. Iftheproportionof moneyand thetime price per unit of the good remelnsfixed and the full wealth assumptionis used, theobjectiveis to maximizeU = U (h, X) subjectto
(p + wt) h + (q +ws) X_Y = y +wTwhere
U = utilityp = out-of-pocketmoney pdce per unitof healthservicest = own-timeinputper unitof healthservices consumedq = money priceper unitof Xs = own-time inputper unit of Xw = eamingsper hourY = total (full)incomeY = non-wageincomeT = totalamountoftimeavailableformarketandownproductionofgoodsandservices,' The assumptfonsthataresufficienttomake moneyfunctionasa price indetermining
demandforhealth servicesare alsosufficientto meanthatan increaseinnon-wageincome,willleadtoan increaseinthedemand forhealthservices.Thesufficientassumptionsare thatthe firstdedvativesof the utilityfunctionwithrespect to a good are positive,that thesecondderivativesare negative, and that the cress-partialderivativesare positive.

DemandforHealthCare 99
inthedemandforprivatecare.He alsofounda positiverelationshipbetweennon-wageincomeandthe demandforhealthservices,thussupportingtheconsumptionmodel.However,althoughthe signsofActon'selasticitiesareconsistentwiththeconsumptionmodel,the absolutevaluesof the elastici-tiesare lessthanunity.
Heller(1976) foundthatforWestMalaysia,incomeisnota statisticallysignificantdeterminantof the totaldemandfor healthservices.Neverthe-less,incomestronglyincreasesdemand for privatemoderncare relativetopublicfacilities. In the case of sick Filipinochildren,Akin, Guilkey,andPopKin(1981) foundthat income does not significantlydeterminethe,Choiceof healthfacility.
Suchinsignificantfindingswithrespecttoincomearecluetothedoubleeffectof incomeon healthcare, In low-incomecountries,it is the doubleeffectofpovertythatapplies,itdirectlyaffectsaccessibilitytohealthserviceandindirectly,itaffectsthediseasepatternofa familyora community.Low-incomepeople tendto have a loweruse of healthservicebecausetheycannot affordthecost.However,sincethesefamiliesare usuallyunabletoaffordpreventivecare andwouldthusbe unhealthier,they are morelikelyto increasetheiruse of healthservices.
Instead of current income, permanent income is said to be thetheoreticallyappropriatevariable. Such a course, however, presents nu-merous difficultiesOf measurement.Assetsare normallyan alternative.Assetsaccumulatedovertimeyielda highlevelofwealth.Assets,heldintheformof land,bankdepositsoranimals,enhancethe capacityto use healthservicessincetheycaneasilybeencashedformedicalneeds.Ontheotherhand,assetsalsosuggesta healthierhouseholdand a lowerlevelofmedicalneed. One can immediatelysee a doubleeffectof assetssimilarto thatofincome.Itis notsurprisingtoseehard-to-interpretresultswithrespecttotheassetvariable.
B. Price
A firmlyestablishedconclusionaboutthedemandfor healthservicesisthat the quantitydemandedis not very responsiveto pricechanges. Ingeneral,price elasticitieshave been negativebut vary widely. The priceelasticityfor patient daysrangesfrom-0.20 to -0.70; for physicianofficevisitsthe variationin price elasticityis from -0.05 to -0.20; for hospitaladmissionsthe priceelastidtyis between-0.30 to -0.50 (Rosenthal 1970;Martin Feldstein 1971;Newhouse and Phelps 1976; Coffey 1983 )._
, NotethatDavisandRussell(1972)estimatedpriceelasticitiesgreaterthanone./_cordingtoNewhouse,PhelpsandMarquis(1980),theDavis-Russellresultissuspectbecausethe insurancevariableis rnisspedfied.Thelargeelasticitiesarelikelyanartifactcausedbymisspedfication.Thepresentstudydiscussesthespecificationofinsurermeasitisrelatedtothepricevariable,inthetextandinIoo_ote11.

100 Panfila Ching
The Heller study of West Malaysian health services also found thattotal demand for modern medical care was insensitive to price. Neverthe-less, the decision of whether or notto use public facilitieswas responsive tothe price of private care; similarly, the decision of whether or not to usetraditional practitioners was sensitive to the price of modern care.
Prices may yield confusing results due to cultural factors. In somecultures, health facilitiesthat do notcharge a price are perceived to have lowquality services. In Zaire (Lashman 1975),for example, mission churchesand mobile health teams found that villagers were unreceptive to serviceswhich did not cost money. However, after fees were imposed for services,demand increased.
A widely recognized aspect of the price of health care is that it has twocomponents. One is the nominal or money price. The other is time price.
1. Money Price
For the nominal component, the relevant and appropriate price is netof insurance benefits 9 and subsidies (P. Feldstein 1979; Newhouse andPhelps 1976; Newhouse, Phelps and Marquis 1980 ).1oThe gross price orcharges stated by a health care provider are often not what is paid by thepatient. Part or all of the gross price is paid by a third party or by thegovernment on the patient's behalf. Any estimate of price elasticity ofdemand should be based upon the net orthe out-of-pocket price paid by thepatient: physician and hospital charges, fee for treatment and drugs, travelcost, and all other out-of-poCket expenses incurred during a visit, lessamount paid by third-party payor (insurance benefits) and by the govern-ment (subsidized health care).
In the literature, the most common specification of the money price isgross price and a dummy variable that takes the value one if the consumer
has any insurance. Such a specification is shown to cause inconsistency inthe estimated coefficient of the gross price variable." Whether the inconsis-tency is toward or away from zero cannot be established a prion.
, Butincludespremiumcosts.'= Newhouse,PhelpsandMarquis(1980)believe,thoughthatthetheoreticallyappro-
priatespecification,(giventhatindividualswithdeductiblesareexcludedfromthesample),isthemarginalprice,whichisdefinedas thecoinsuranceratetimesthegrosspdce.
Deductiblesare fixedamountsperyearwhichmustbe spentbeforethe insurancecoverageaffectsthepriceof healthcare.Coinsurancereferstofractionalpaymentsforcarebyconsumers.
Newhouseandcolleaguessuggestexcludingindividualswithdeductiblesbecausethetheoreticallycorrectpricecannotbeobservedinthepresenceofdeductibles.Toincludetheseindividualswouldproduceinconsistentcoefficientestimateswherethe directionof theinconsistencycannotbesignedaprior/.Ontheotherhand,excludingtheseindividualswouldgenerateunknowneffects.(in the dateusedby the authors,the sampleselectionhavenegligibleeffects.)
" Thespecificationassumesthatallthosecoveredbyinsurancehavethesamekindof

Demand for Health Care 101
Non-monetary factors, such as time pdce, are expected to assume anincreasingly important role ininfluencing the demand for health care as theout-of-pocket price falls. As net or out-of-pocket price falls, either becauseof increasing insurance coverage or the availability of subsidized care,demand becomes relatively more sensitive to changes in time price.Moreover, demand for free health services is expected to be more respon-
•sive to changes in time prices than demand for non-free sources, since timeis a greater proportion of total price at free than at non-free facilities (Acton19;'8).
2. Time Price
Time has an opportunity cost and should be viewed as one of theresource constraints facing the consumer. The time price of a health serviceis the value of time multiplied by the natural units of time, (e.g., minutes) toobtain care. Time to obtain care refersto travel, waiting and treatment time.
The value of time as an activity is the opportunity cost of time inalternative activities. The value of market time, (i.e., wage rate) is typicallyused as the opportunity cost although theoretically, this may be incorrect(Coffey 1983 ).1_
An alternative is to measure time price in natural units only. Acton(1976), in a study emphasizing the role of time, found that the bias resultingfrom the error in measuring the opportunity cost of time is greater than thebias caused by omitting it from the specification. Moreover, if time price ismeasured as wage rate times time, the resulting time price variable will be
insurance.Sinceindividualshavedifferentkindsofinsurance,thisspecificationinvolvesanerrorthathasanegativecevadancewiththetrueco-insurancerate:forinsuredpersons,theerroris 1-cwhorec is the coinsurancerate. (For uninsuredpeoplethereis no error.)Newhouse,PhelpsandMarquis(1980)haveshowntttatthisnegativecovanancebetweentheinsurancedummyandthemeasurementerrorwill,ingeneral,causetheestimatedcoefficientofthegrosspricevariable,whichisusedtoestimatethepriceelasticity,tobe inconsistent.
,2 Thehome-productionmodelimpliesthatthevalueof timeequalsthewage.rateunderfourassumptions:Theindividual(1)worksinthelabormarket,(2)isfreetochoosethenumberofhourstosupply,(3)hasnopecuniaryutilityordisutilityformarketworkand(4)facesnofixedcostsof holdinga job.
Individualswhoarenotemployedpresentempiricalproblemssinceobservationsontheirwagerates=remissing.Researchersdevisedvarioustechniquesofestimatingthemissingobservations.Forexample,NewhouseandPhelps(1976)usedthe instrumentalvariableapproachwherebytheyestimatedawageequationIorthoseinthe laborforceandusedtheresultingequationto estimatevaluesoftimeforthosenotinthelaborforcebyset_ngweeksworkedequalto zero.
Acton(1976)arguedthatsincetheopportunitycostoftimehadtobe imputedtonon*workingpersonsandis notentirelypreciseevenforworkingpersons,the wagerateismeasuredwitherror.Thiserrorwillbiasthe¢oeflidentson..the timevariablestowardzero_
Conceptually,thevalueof timeforapemonnotinthelaborforceisthehypotheticalwagethatwouldatlracthimtoworkandis knownintheliteratureas the reservationwage.Coffey(1983)measuredthereselvatienwagedirectlybysunleyquestionnaire.Thosenotintheworkforcewereaskedtostatethe lowestwageperhouritwouldtakeforthemtoacceptajob.

102 PanfilaChing
highlycorrelatedwithwageincome.Inclusionot bothvariableswillresultinmultiCollinearity.Thus, the alternativespecificationwhere time priceis innaturalunits is favored by an increasingnumberof researchers(Heller1976;Acton 1976).
Acton(1976) foundtravel-timepriceelasticitiesrangingfrom-0.25 to-0.34 for privatecareandfrom-0.60 to-1.00 forpubliccare. Asexpected,demandforpubliccare is moreresponsiveto changesintravel-timepricesthan demandfor privatecare.
The effectof waitingtime issimilarto traveltime as a determinantofdemand. However,demandfor health servicesare predictedto be moreresponsiveto changesintraveltimethanto changesinwaitingtimesincetravel requiresa monetaryexpensethat varieswithdistanceortime, whilewaitingtimedoesnotinvolvethisadditionalmonetarycharge.Actonfoundthatthewaiting-timepriceelasticityis-0.05 forprivatecareandis-0.12 forpubliccare. As predicted,the elasticitieswithrespectto waitingtime aresmallerin absolutevalue thanthe elasticitieswithrespectto travel time.However,justas inthe case caseof traveltime, demandfor publiccare ismoreresponsivetochangesinwaitingtimethanisdemandforprivatecare.
Heller (1976) foundthat it is the relativetravel time rather than therelativetime requirementsfortreatmentandwaitingthat provesimportantinthe choiceof a publicratherthanprivateclinic.
Indevelopingcountrieswheresomepeoplecanspendhours,ifnotanentireday,doingnon-productiveactivities,thesemarginalmagnitudesmaynotbe relevant.Therefore,to viewtimeas havinganopportunitycost maynot be meaningfulin suchcases. In addition,there can be factors whichamelioratethetimelostfromotheractivities.Forexample,inWestMalaysia,waitingtimedidnotimpedeuseofgovernmentand privateclinicsbecausepatientsmay haveviewedwaitingtime as a chance to socialize (,Heller1976). Moreover,patientsmayperceivea positiverelationshipbetweenthequalityofcare receivedandthetimespentintreatment(andhence,thetimespent waiting for one's turn). The actual effect of waiting time is thuscomplicated.
Demandanalysisof anyonetypeof healthserviceshouldincludethepricesof itssubstitutesandcomplements.Certaintypesof servicescansubstituteforothersinthetreatmentofan illness.An analysisofdemandforanyonetype isincompleteif itomitsthe substitutabilityorcomplementarityof othertypes. Hence, in anydemandequation,one expectsto see own-money,cross-money,own-timeandcross-timeprices.
C. Health Insurance
Asidefrom reducingthe net priceof healthcare, insurancemay beviewedas a methodof financingthe demandfor health care. It not onlyreducesthecost ofcare butalsoincreasestheabilityof thefamilyto secure

DemandforHealthCare 103
healthservices.Healthinsuranceisthusexpectedto raisetheutilizationandexpendituresfor healthcare.
Eveniftheonlyavailablemeasureof insurancecoverageis a dummy(yes/no)variable,thisvariableshouldbe includedin the modelbecauseinsuranceisdesignedto reducerisk,i.e., increasethe stabilityofthe.healthservicesconsumptionstreambyreducingtheamountof moneythat mustbe set asidefor emergencies.An incomeeffectis thusfelt bypeoplewithhealthinsurance.Ifa shiftvariableis notincludedtocapturethiseffect,thecoefficienton incomewillbebiased(Grossman 1970;Akin et al. 1985 ).
A naggingproblemaccompanyinghealthinsuranceis costinflation.By loweringthecostof care to patientat the pointof delivery,insuranceislikelyto increaseutilizationandexpendituresforhealth care andthus,putpressureon scarce resourcestherebyleading,on the aggregate,to anappreciabledseincosts.Suchis theAmericanexperience.To combatcostinflation,suchitemsas deductiblesand cotnsurance,whereinthe patientsharespartof the expenditures,were introduced.These schemes,whichworkon the consumer,wouldleadto reducedutilizationinthe absenceofpractitionerinfluence.The presenceof doctor-induceddemandandutiliza-tionwouldmake thesemeasuresweak.
Mountingcriticismsontheineffectivenessofdeductiblesandcoinsur-ance incostcontainmentledto theprepaymentsystem,wheretheinsuringagencyandprovidingagencyare thesameinstitution.The consumerpaysan annualsubscriptionand in returnis offeredcomprehensivecare. Theprovidingagencyhasa financialincentiveto limitunnecessarycare. Sincesuchsystemsrequireconsiderablecapital investmentand a largecatch-meritpopulation,an alternativeknown as a healthmaintenanceorganiza-
, tionhasbeendeveloped. A primarycaredoctorprovides, purchasesand,supervisesall primarycare andin retumreceivesa capitationpaymentforeachconsumer(insteadof eachservice,as inthe fee-for-serviceschemecommonlypracticedingeneralhealthinsurancesystems).Theincentiveforcost containmentin health maintenanceorganizationscomes from twosources:the amalgamationof the insurerand provider functions,andcompetitionforsubscriberswithconventionalinsuranceagenciesandotherhealth maintenanceorganizations.One potential problemthough,whencapitationpaymentis practicedis when the numberof people registeredtendto be maximizedand the servicesgiventendto be minimized.That iswhysomeorganizationsgive saladesinstead;but a danger hereis thatofminimizingactivities(Mills, 1983). The best systemhasyetto be carefullystudiedInthe lightofproviderinfluenceandfactorsaffectingtheirbehavior.
D. Demographic Factors
1. Age Composition

104 PanfilaChing
The incidenceof illnessvarieswithage, and thereby,the need forhealthcare. Thepresenceof childrenandelderlypersonsinthe familywillraisethefrequencyof illnessresultingin an increasein the use of healthservices.Paqueo(1977) foundthepredictionto betrueofchildren0-5 yearsold. WirickandBarlow(1964)andSilver (1972) foundthat age ispositivelycorrelatedwithhealthexpenditures.
2. Sex Composition
Inorderto isolatethe effectof sexondemand,age,health statusandall otherfactors shouldbe consideredin a modelspecification.However,attemptstodosoyieldsweakresultsandmarginaldifferencesinusagewerediscovered.Sex is foundinsignificantinexplaininghealthcare demandofFilipinochildren(Akin, Guilkey and Popkin 1981).
Sexdiscriminationis actuallythe majorunderlyingreasonfor expect-ing differencesin health service usage by men and women. In manysocieties,a lowperceptionoftheeconomicvalueofwomentothehouseholdleadsto lowhealthserviceusageby females.
3. Family Size
Familysize affectsuse of health servicesinan unpredictableway.Alargerfamilywillhavea higherfrequencyof illnesssinceithasmorepotentialpatients.However,a largerfamilyhas lessincomeper capitathan thatof
•a smallfamilywiththesame income,anda lowerpercapitaincomereducesthe family'sabilityto purchasehealth services. In addition,a largerfamilymayhaveenoughpeopleat hometocare foran individual,thussubstitutingfor additionaldaysof hospitalcare.
E. Knowledge and Information
1. Education
A higherlevelof educationmayenablea familyto recognizethe earlysymptomsof illness,resultingina greaterwillingness•to seek early treat-ment.Such a familyis likelytospendmoreforpreventiveservicesandlessforcurativeservices.Grossman(1972b) suggeststhateducationincreasesefficiencyinproducinghealth,suchthatbettereducatedpeopleare likelytoproducehealth withfewer health care services;consequently,educationwouldhavea negativeeffectondemand.FeldsteinandSeverson( 1964)foundthatmedicalcare expendituresare negativelycorrelatedwitheduca-•tion.Silver(1972) foundthateducationisnegativelycorrelatedwithhospitalexpenses but positivelycorrelatedwith medicineand doctor expenses.Acton (1976) had similarresults- educationhas a negativeeffect on

DemandforHealthCare 105
hospitaloutpatient department visits and clinic services while it has apositive effect on private physician visits. These results tend to confirm thehypothesis that better-educated persons spend more for preventive care,resulting in low hospital expenditures but high physician and medicineexpenses.
Itis the mother's education,in particular,which is crucial because sheusually supervises the household. Inthe Philippines,for example, mother'seducationwas foundimportant indeterminingwhether or nota sickchild wastaken for treatment. The most educated mothers used private modempractitioners in over 50 percent of the cases while the least educatedmotherschose the same typeonly 25 percentot the time (Akin, GuilkeyandPopkin 1981).
2. Health, Knowledge and Beliefs
The family's stateof health knowledge andbeliefs affects its efficiencyin the production of health through dietary, hygienic and preventive meas-ures. It also affects the choiceof a health facility-- traditionalversusmodern.
F. Health Need
Demandfor healthcareis baseduponfelt needs; if noneedsare felt,there will be no demand. Doctorsassesswhether felt needs are actualneeds;someturnouttobeso,whileothersdonot.Theimportantpointisthatself-perceivedneed will determinewhether or not an individualis in themarketfor healthcare. Itistheimmediatecauseof thedecisiontoseekcare.In demandanalysis,everyoneinthe samplebydefinitionbelieveshimselftobe ill,orinneed.Hence,it makesmoresenseto measurehealthneedbyitems such as type of illnessor its perceived seriousness. Akin et al.(1985) foundperceivedseriousnessof illnessanoverwhelminglyimportantexplanatoryvariablewhich cut acrossall socioeconomiclinesand forcedboth poor and richalike to act inthe same manner, that is, seek privatemoderncare.
G. Availability of Health Service
Inpractice,demandcannotbemeasureddirectlyandisobservedfromdata thatmeasureratesofutilizationresultingfromthe interplayof demandandsupply.Asa result,demandanalysistakesintoaccountbothsupplyanddemandfactors. It is idealthen, to controlthe supplyfactorin demandbysucha measureasthedoctor-to-populationratioor hilot-to-populationratio.This isintuitivelysaicltobeessentialbecauseto someextentinthe medicalfield, supplycreates itsowndemand.

106 PanfilaChing
Availabilitymeansmorethanthe merepresenceof a healthservice.It referstothe capacityto meetthe demand.Thus,the numberof servicesper capitaratherthanjust the numberol servicesis the usualindicatorofavailability.
H. Time Allocation of Mothe[
Motherswho stayat hometo care for childrenor are able to engageininformalmarketworkathomeareexpectedto havefewertimeconstraintsthan motherswho musttravelto, and putin hoursat, a formaljob.Hence,motherswho are constrainedbyformalworkwouldnaturallybe driventoprivatefacilitiesdespitethe influenceof price, incomeor any of the otherfactors.
Rimando (1976) found lower utilizationof health services amongworkingruralFilipinowomen.PopkinandSolon(1976) hadsimilarresults.
I. Location of Residence: Urban or Rural
While there is greateravailabilityof healthservicesinurbanthan inruralareas,therealsotendsto benegativehealtheffectsof urbanlifesuchascrowding,pollution,exposureto accidents,a highleveloftensionandthelike.Itseemsthaturbanresidenceisa proxyforanassortmentof variables.
Ina well-specifiedmodelthatincludesexplanatoryvariablessuchasdistance,availabilityof services,education,healthknowledgeandbeliefs,and employment,theurbanvariablemaybea measureoftheefficiencywithwhich householdconsumptionand productionare undertaken.In urbanareas,timerequiredtopedormhouseholdchoresmaybe lowerandchoiceswider than in rural areas because of greaterspecializationand broadermarkets. Inaddition,urbanmaybea proxyforthepersonalitytraitsof urbanmigrants.Urban migrantsare self-selectedindividualswhotendto be thehealthiestamongruralfolksandareadaptableto modernmedicalconcepts(Akin et aL1985 ).
J. Distance of Health Service
Distance of health services from the family residence measuresaccessibility. Distancehas beenthe moststudied hindranceto healthfacilityuse. The moredistanta facility is from potentialusers,the less likely aretheyto visit it: Akin, Guilkey and Popkin (1981) found this to be true of childoutpatient visits in the Philippines.
Akin etaL (1985), however,argues that thepreoccupationof plannerswith distanceto health facilities may indicate attention to an inappropriateproxy for true items of interest -- travel cost and travel time:

DemandforHealthCare 107
Thereis a one-to-one relationship among these variablesonly ifeveryoneuses exactly thesame mode of transportation,such aswalking at exactly the same speed. Reducing the distance triptime and transportation costs.., the economic "distance" tofacilities can be reduced by improving roads or providing newforms of transportation.
V. RESEARCHGAPS AND POLICY IMPLICATIONS
A. Do Doctors Generate Their Own Demand?
A majorapplicationof demand analysisin the healthindustryis topredicthowutilizationandcostwill changeif determinantsof demandorsupplychange.LiteratureonthePhilippinesassumesthatinsurancehasanuncomplicatedeffecton utilizationand cost,thatis,insurancesimplyshiftsthe demand curve in some fashion (Rimando 1976; Akin 1985; Ching1985 ). Similarly,providerinfluenceis viewedas a plain demand shifter(Rimando 1976; Ching 1985, 1986).
With respectto insurance,sucha viewis plausiblesince insurancecoversonlya minorportionofthemarket.Withrespecttoproviderinfluence,however,future researchstillhas to prove its existenceand establishitsmagnitude-- a task considereddifficult even for developed-countriesresearch.
Thecommonprocedureinthe literaturestudiedinvolves,first,speci-fying a demand equation from a traditionalmicroeconomicmodel of asovereignconsumer,then,estimatingtheequationwithsomemeasuresofvolumeof utilizedservicesas the dependent variables. In other words,demand cannot be measured directly but is observed from data thatmeasureratesofuse resultingfromtheinterplayofdemandandsupply.Asa result,demand analysis'takes into accountboth supplyand demandfactorsSupplyfactorsin demandfunctionare taken into accountbysuchmeasuresas physician-to-populationratio(Ching 1985, 1986)oravailabil-ity/non-availabilityof service(Rimando 1976).The rationalefor this isthatdoctorsgeneratedemandfor theirservices.
Thetestof inducementboilsdowntothe examinationof howquantityorpdceofmedicalservicesvarieswiththeabundanceof services.However,findinga positivecorrelationbetween resourcesand eitherutilizationorpricedoesnot necessarilyshowinducement(Fuchs and Newhouse 1978;Newhouse 1981).Under the no-inducementhypothesis,mo_eprovidersinan area tend to lowerwaitingtime whichwill raise demand. Moreover,simultaneitybetween supply and demand prevents the acceptance ofinducementhypothesisjustfrom the positiveassociationbetween supplyand utilization.One shouldascertainwhetheran area has a highersupplybecause it has a high demand or vice-versa.This has provedto be a

108 PanfilaChing '
herculeantask.One could sense an apprehension in accepting the inducement
hypothesisbecause it truly poses a seriouschallenge to the estimateddemandfunctionsreviewedin this paper.Nevertheless,somedescriptivestudiesindicatethat doctorsdo influencedemand(Monsma 1970; Evans1974; Fuchs 1978 ).The existenceof inducementcallsfor a more realisticmodelof demandwheretheconsumerdecideswhetheror nor to enter thehealthsystem,andthe doctordeterminesthe treatment.
The reasonfor so muchdiscussionon the influenceof providersonconsumersisthe policyimplicationof thephenomenon.The introductionofinsurance,whichactsto reducethe costof healthtothe patientat thepointof delivery,will leadto increasedutilizationandthus, pressureon scarcehealthresources.The appropriatepolicythenisto applystrategiesto affectthe behaviorof providers,not consumers.For example, a prepaymentsystemthatgivesfixedsalariesto providers,wouldbe morecost-effectivethan deductible/coinsurancethat workson the consumerside,when pro-vider influenceis strong.
As for research implication:if doctors do respond to incentivesinherentin differentpaymentsystemsanddo influencedemand,then oneshouldall the more studythe factorsof providerbehaviorin the face ofinsurance.Examplesof suchfactors are work hoursof the doctor, hisincome,hispatient'sincome,grossfee andinsurancerebate,assumingthathisutilityisa functionofsocialstatus,leisureandesteemwithwhichpatientsregardhim. Researcherscouldtry andtest, as a firststepinthe Philippinesetting,theoreticalmodelsalreadydeveloped(Richardson 1981 )..
B. Specification of the Dependent Variab/e
A perenniallycontroversialissueconcernsthe selectionof an appro-priatedependentvariable.Twomeasures,medicalexpendituresandquan-titiesof medicalserviceshavebeencommonlyused.Bothhavedisadvan-tages._
Expendituresare inaccurateindicatorswhen pricediscriminationispracticedbysomedoctorsor whenthere arevariationsinthe qualityoftheproductitself.Medicalexpendituresmaybiasthe effectsoffactorsbelievedto influencedemand(priceandincome),ifunadjustedforpricechangesandqualityvariations.
The majorweaknessof usingquantitiesof presumablycomparableservicesistheabsenceof a commondenominator.Quantitiesof heteroge-neousservicesare difficultto combineandcompare.Nevertheless,quan-titiesallowmoreaccuratecomparisonsof the amountofuse of a particularservice.
It isevidentthatexpenditures_a___ndquantitiesare indicatorso! use,notdemand.A moreappropriatedemandmeasureis the numberof episodes

Demandfor HealthCare 109
of medicalservicewhichisdefinedasthe numberof requestsfortreatment(Stoddart 1981).
C. Specification of the Health Status Variable
Healthstatusrepresentshealthneedandthusinfluencesdemandforhealthservices.Healt_ statusmeasuredby illnessexperience(as recalledbythe respondent)maynotfullyrepresentthe realhealthneedof a person.Yet, thereis nooverallhealthindexto measurean individual'shealthstate.Effortsshouldbe directedto increasethe comprehensivenesswithwhichhealthis measured;physical,social,mentalandphysiologicaldimensionscan be included.For example, Manning, Newhouseand Ware (1982)supplementedself-assessedgeneral health perceptionwithmeasuresoflimitationof function,psychologicalstateand socialactivity.
it isworth noting,however,that indemand analysis,everyoneinthesamplebydefinitionbelieveshimselfto be in need. Hence, it makesmoresenseto measurehealthneedby itemssuchastypeof illnessorperceivedsedousness.
D. Should Demand Analysis Include People Who are Not in Need?
One shortcomingof somestudiesis the failureto descdbewhethertheirsampleinregressionanalysisincludesonlysickpeopleor healthyonesas well.What is the appropriatesampleto study?
Atthispoint,itishelpfulto recallthe processesbywhichan individual'sdemand for healthcare are met inthe healthyindustry(Lee 1983 ):_
NEEDS
LFELT NEEDS
LDEMAND
1UTILIZATION
Demandfor health care is based uponhealth needs;if no needsarefelt, therewillbe nodemand.Doctorsassesswhetherfeltneeds areactualneeds;some turnoutto be so, other do not. The important point is self-perceived(orfelt) needwilldeterminewhetheror notan individualisinthemarketforhealthcare. ideally,demandanalysisshouldbe concernedwitha sampleof peoplewhofeel they are inneed and do expressthisneed by

110 PanfilaChing
requestingfor treatment. This reasoningis the argumentof Akin et al.( 1985) for wantingto studysickpeopleonlyhence:
In examining the use of medical services, the point of interest isnot what the whole population does, but what sick people do.Hospitals, clinics, and medical schools are not constructed tocare for the healthy. Questions of policy, which revolve aroundcosts of welfareprograms and why people use specific types ofservices, are questions of demand that cannot be answered byreferring to health capital formation. People who do not considerthemselves sickgenerally haveno demand formedical services;they are therefore irrelevant to the problem, ff thought about inthis manner, the issue of demand for medical services appearsto be much simpler than any of the analysts have assumed.
Perhaps,whatworriessome analystsisthe healthywho do demandcare,inparticular,preventivecare.Theappropriatesampleherewouldstillbepeoplewhofeel andexpressneed(thoughtheyarenotsick). Needcouldactuallyembodycurativeandpreventiveconcepts.Need hasbeendefined(Culyer 1978) to existwhen(1) thepotentialforavoidance of reductionsinhealth statusexists(preventionand somecare); and (b) the potentialforImprovements in healthstatusabovethelevelitwouldotherwisebeexists(cure andsomecare). If theappropriatesamplein demandforpreventivecare are the peoplewho perceivethey are in need, but not sick, then ademandanalysison preventivecare, separatefromcurativecare iscalledfor.Nevertheless,the pointthatthe appropriatesampleis peoplewhofeelin needand do expressit, remains.
Theprecedingstatementmaynotsoundmoraltosomeplannerswhothinkpersonsactuallyinneed,butdonotexpressit(andmayor maynotfeelinneed),shouldreceivecare.Themarketstructurefor healthsimplycannotaccommodatesuch peoplebecausethe structureonly allowsfor peoplewho felt and expressedtheirneeds. •
Thepurposeofthissectionisto encouragefutureresearchto domoreadequatedescriptionsof theirempiricalwork, and not to worry about aseeminglylimitedsample13-- peoplewho report themselvesas sick mwhen studyingdemandformedicalservices.However,ifoneisstudyingtheproductionof health,anentirelydifferentproblemis athandwhichrequiresa sampleof both sickand healthypeople.
E. Price, Non-Users and Data Problems
Estimationof healthcare priceleaves muchto be desired.Nowhere
'= Usuallydue to data limitationsarisingfromthe surveyquestionnaireitself.

DemandforHearthCare 111
canonefindobservationsonpricethewayeconomistsdefineit,whichisona per-unitbasisandisexogenoustothehousehold.TheusualpraclJceistoapproximatepriceswith expenditures.A problemoccursfor non-users:thereisno correspondingprice(expenditure)observationforthem.Awidelyusedprocedureisto imputeexpendituresfor non-usersonthe basisof theaverageexpendituresofusers,Suchprocedurecastsdoubtonthe interpre-tationof thepricecoefficient.
The pricespecificationclosestto the correctonewouldbe a facility-reportedcost or usualfee paid for a visit.One has to undertake hisownsurveyforthis,however,ifnotcontainedinmultipurposesurveys.Data fromsocialexperiments(suchas the HealthInsuranceStudyof Rand Corpora-tion)havebeenquitehelpfulinstudyinginsuranceanddemandforservicesin developedcountries,itwouldbe a welcomemoveto undertakesimilarexperimentsinthe Philippinesfor thepurposeofenhancingitshealthdatabase.
Anotherproblemdirectlydependentuponthesampleof observationsis multicollineadty.14Takeforexamplehygienicsewerageand healthstatus,whichareoften seenasdeterminantsof demandinlow-incomecountries.These factorsare oftencorrelated.The existenceof a hygienicseweragesystemaffectstheconditionof sicknessor healthwhichinturndeterminesdemand.However,ifthesampleof observationsinvolvessickpeopleonly,thenonecandrophygienicseweragebecausethere isnoa priorireason toexpectthat sewerageaffectsthechoiceof practitioner'sornumberofvisitsmade once the individualgets sick. Consequently,a hygienic seweragevariable is not appropriatein a system of demand equationwhich areestimatedusing a sample of sick people. Health status, which may bemeasuredbytype orfrequencyof illnessremains.
" The easiest way to det_ multio_Hineadtyis _oexamine the standarderrorsof thecoefficients, if several coefficientshave highstandard ermm and droppingone or morevariablesfrom theequationlowersthestandardenorsofremainingvariables,multicoilineadtyis mostlikelypresent.
One's judgmentshouldbe usedwhen__,'Je__.'dmgwhether or nottodrop an explanatow,variablebecause the gainin the reductioninstandarderrorofremainingvariables,when thevariable is dropped,mustbe tradedoffagainst the possibleintmduc_n of biasdue to mis-specificationof the equation.

112 Panfila Ching
BIBLIOGRAPHY
Acton, J.P. "Non-monetaryFactorsin the Demand for MedicalServices:SomeEmpiricalEvidence."Journal of Political Economy. (1975) 83 (3) :595-614.
. "DemandforHealthCareamongthe UrbanPoor,withSpecialEmpha-sis on the Role of Time." In Rosett,Richard N. (ed.), The Role of HealthInsurance in the Health Services Sector. New York: National Bureau ofEconomicResearch. 1976.
Akin,J.S., Guilkey,D.K.and Popkin,B.M. "The Demandfor ChildHealthServicesinthe Philippines."Social Science and Medicine. (1981) 15C:249-257.
Akin,J.S., Griffin,C.C., Guilkey,D.K. and Popkin,B.M. The Demand for PrimaryHealth Services in the Third World. Totowa, New Jersey: Rowman & AI-lanheld.1985.
Andersen,R. and Benham,L. "FactorsAffectingthe RelationshipBetweenFamilyIncomeand MedicalCare Consumption."In Klarman,H.E. (ed.), EmpiricalStudies in Health Economics. Baltimore:TheJohns HopkinsPress.1970.
Becker,G.S. "A Theoryofthe Allocationof Time." Economic Journal75 1965:493-517.
Ching,P. "Measuringthe Incidenceof HealthExpendituresI1:Use of PublicHealthFacilitiesin Bicol."PhilippineInstituteforDevelopmentStudies,1985.
. "PublicProvisionand DemandforHealthServices:A Case StudyofBicol."Ph.D. Dissertation,Schoolof Economics,Universityofthe Philippines.1986.
Coffey,R. "The EffectofTimePriceonthe DemandforMedical-CareServices."TheJournal of Human Resources. 18 (3) 1983:407-424.
Cooper,M. "Economicsof Need:The Experienceof the BritishHealthService." InPerlman, M. (ed.) The Economics of Health and Medical Care. Proceedingsof a Conferenceheldby the InternationalEconomicAssociation,April1973,Tokyo.London:Macmillan,1974.
Culyer, A.J. "Need, Values and Health Status." In Culyer, A.J. and Wright,K.G.(eds.). EconomicAspects of HealthServices.London:MartinRobertson&Co.Ltd, 1978.
Davis,K.andRussell,L.B."TheSubstitutionofHospitalOutpatientCare for InpatientCare." The Review of Economics and Statistics. 54 (2) 1972: 109-120.
Evans, R.G. "Supplier-lnducadDemand:Some EmpiricalEvidenceand Implica-tions."In Perlman, M. (ed.), The Economics of Health and Medical Care.

Demand for Health Care 113
Proceedingsof aConferenceheldbythe InternationalEconomicAssociation,April1973, Tokyo.London:Macmillan,1974.
Feldstein,M.S,"HospitaJCost Inflation:A Studyof Non-ProfitPrice Dynamics."American Economic Review.61 (5) 1971: 853-872,
Feldstein,P.J. Health Care Economics. New York:JohnWiley & Sons,inc, 1979.
andSeverson,R•M. "TheDemandforMedicalCare,"inReportoftheCommissiononthe Costof MedicalCare. Vol. 1, Chicago,AmericanMedicalAssociation:pp.57-76. CitedinKlarman,H•E. TheEconomics of Health. NewYork: ColumbiaUniversityPress, 1965•
Fuchs,V.R. (ed.) Essays in the Economics of Health and Medical Care.New York:ColumbiaUniversityPress,1972.
. "TheSupplyofSurgeonsandthe DemandforOperations."JoumalofHuman Resources13, Supplement•1978.
Fuchs, V.R. and Newhouse, J.P. "The Conferenceand UnresolvedProblems."Journal of Human Resources 13, Supplement.1978•
Green, J. "Physician-inducedDemandfor Medical_are." Journal of Human Re-sources 13,(1978) Supplement.
Grossman, M. "Commenton "FactorsAffectingthe RelationshipBetweenFamilyincomeand MedicalCare Consumption,"In Klarman,H.E. (ed.), EmpiricalStudies in Health Economics. Baltimore:The JohnsHopkinsPress, 1970.
The Demand for Health: A Theoretical;and Empirical Investigation.New York:NationalBureauof EconomicResearch,1972.
• "On the Concept of Health Capital and the Demand for Health."Journal of Political Economy.80 (2) 1972:233-255.
Heller, P.S. "A Model of the Demand for Medicaland Health Services in WestMalaysia." DiscussionPaper No. 62, Center for Research on EconomicDevelopment•AnnArbor:Universityof Michigan,1976.
Holtmann, A.G. "Price,Time, and Technologyinthe Medical Market•"Journal ofHuman Resources. 7 1972:179-90.
Holtmann, A.G. and Olsen, E.O. Jr. "The Demandfor Dental Care: A StudyofConsumptionandHouseholdProduction."Journal of Human Resources. 111976:546-60.
Kohn,R. andWhite,K.L, (eds.) Health Care: An International Study. Reportof theWorldHealthOrganization/InternationalCollaborativeStudyof Medical Care

114 Panfila Ching
Utilization.London:OxfordUniversityPress,1976.
Lashman,K. Syncrisis: TheDynamics of Health. An Analytic Series on the Interac-tions of Health and Socioeconomic Development. Vol. 14, Zaire. DHEWPublicationNo.*(OS) 74-50, 019. Washington,D.C.: Office of InternationalHealth, Divisionof Planningand Evaluation,U.S. Department of Health,EducationandWelfare, 1975.
Lee, K. "ResourcesandCostsinPrimaryHealthCare."InLee,K.andMills,A. (eds.)TheEconomics of Health in Developing Countries.Oxford:OxfordUniversityPress, 1983.
Manning,W.G., Newhouse,J.P. andWare,J.E.,Jr. '_rheStatusofHealthinDemandEstimation;orBeyondExcellent,Good,Fair,and Poor."InFuchs,V.R. (ed.),Economic Aspects of Health. NationalBureauofEconomicResearchConfer-ence Report.Chicago:The Universityof ChicagoPress,1982.
Matthew,G.K. "MeasuringNeed andEvaluatingServices."in McLachlan,G. (ed.)Portfolio for Health. London:Oxford UniversityPress, 1971.
Mills,A•"EconomicAspectsofHealth insurance•"InLee,K.andMills,A. (eds.), TheEconomics of Health in DevelopingCountries.OxfordUniversityPress.1983.
Monsma,G.N.,Jr. "MarginalRevenueandtheDemandforPhysician'sServices•"InKlarman,H.E. (ed.), Empi_cal Studies in Health Economics. Baltimore:TheJohnsHopkinsPress, 197.0•
Mooney,C.H. Economics, Medicine and Health Care.Sussex:WheatsheafBooksLtd., 1986.
Mushkin,S.J. "Healthasan Investment."JournalofPoliticalEconorny. 70, 1962(5,pt. 2, supp.):129-57.
Newhouse, J.P• "The Demand for Medical Care Services: A Retrospect andprospect."InGaag,J. vanderandPerlman,M. (eds.)Health, Economics andHealth Economics. Proceedingsofthe WorldCongresson HealthEconom-ics, Leiden,The Netherlands,September1980• Amsterdam:North-HollandPublishingCompany,1981.
and Phelps,C.E. "Price and IncomeElasticitiesfor MedicalCareServices."In Perlman,M. (ed.), TheEconomics of Health and Medical Care.Proceedingsof aConferenceheldbythe InternationalEconomicAssociation,April1973, Tokyo.London:Macmillan,1974.
• "New Estimatesof Price and Income Elasticitiesof MedicalCareServices." In Rosett,R. (ed.), The Role of Health Insurance in the HealthServices Sector. New York:NationalBureauof EconomicResearch,1976.

Demand for Health Care 115
Newhouse,J.P., Phelps,C.E. andMarquis,M.S. "OnHavingYourCake andEatingIttoo:EconometricProblemsinEstimatingthe DemandforHealthServices."Journal of Econometrics 13, 1980:365-390.
Paqueo,V. "HouseholdUtilizationofHealthCareServices:AQuantitativeAnalysis."In Final Report: Population, Resources, Environment and the Phil4opineFuture.QuezonCityiSchoolofEconomice,Universityof the Philippines,1977.
Phelps,C.E. "Demandfor Health Insurance:A Theoreticaland EmpiricalInvestiga-tion."PaperNo. R-1054-OEO/NC. Santa Monica,CA: Rand Corp., 1973.
Popkin, B.M. and Solon, F.S. "Income, "lqme,the WorkingMother, and ChildNutriture."Journal of TropicalPediatrics and Environmental Child Health22,1976:156-166.
Ricardo-Campbell,R. The Economics and Politics of Health. Chapell Hill:TheUnivemltyof NorthCarolinaPress,1982.
Richardson,J. "The InducementHypothesis:That DoctorsGenerate DemandforTheir Own Services,"In Gaag, J. van der and Perlman, M. (eds.) Health,Economics and Health Economics. Proceedingsof the WorldCongressonHealthEconomics,Leiden,The Nethedands,September1980. Amsterdam:North-HollandPublishingCompany, 1981.
Rimando,R.B:"Determinantsof HealthServiceUtilizationPatterninFilipinoBarrios:Laguna Province."M.A. Thesis, Schoolof Economics, Universityof thePhilippines,1976.
RosenthaJ,G. "PriceElasticityof DemandforShort-termGeneralHospitalServices,"In Klarman, H.E. (ed.), Empirical Studies in Health Economics. Baltimore:JohnsHopkinsPress, 1976.
Rossett, R.N. and Huang, L. "TheEffectof Health Insuranceon the Demand forMedicalCare."Journal of Political'Economy. 81(2), 1973:281-305,
Silver,M. "AnEconomicAnalysisof VariationsinMedicalExpansesandWork-LossRates." In Fuchs,V. (ed.), Essays in the Economics of Health and MedicalCare.NationalBureauofEconomicResearch.New York:ColumbiaUniversityPress, 1972.
Sorkin,A.L. Health Economics. Lexington,Massachusetts:D.C. Heath and Com-pany, 1975.
Stoddart, G.L. and Barer, M.L. "Analysesof Demand and UtilizationthroughEpisodesof MedicalServices." In Gaag, J. van der and Perlman, M. (eds.),Health, Economics and Health Economics. Proceedingsof the World Con-gress on Health Economics,Leiden, The Netherlands,September 1980.Amsterdam:North-HollandPublishingCompany,1981.

116 Panfila Ching +
Wirick,G. andBarlow,R. "TheEconomicand SocialDeterminantsof the Demandfor HealthServices."In TheEconomics of Health andMedical Care.Proceed-ingsof the Conferenceonthe Economicsof Health and MedicalCare, May10-12, 1962. Ann Arbor:Universityof Michigan,1964.

Health Financing In The Philippines:A Review of The Literature
Ma. Concepcion P. Alfiler*
I, INTRODUCTION
Withthe settingof an internationalgoal of "Healthforall by the year2000", memberstatesofthe WorldHealthOrganization(WHO) committedthemselvesto the taskof makingallcitizensoftheworld,bytheturnofthecentury,attaina "levelof healththat will permitthemto leadsociallyandeconomicallyproductivelives"(Mach and AbeI-Smith 1983p. 10).
To realizethisobjective,a GlobalStrategywas mappedoutwhereinit is specifiedthat concertedefforts mustbe exerted to include,amongothers,the generationandmobilizationoffinancialandmaterialresources(Mach and Abel.Smith 1983p. 10 ).Thisprovisionprovidesthe basisforamoresystematicattemptto matchneeds,resourcesandavailablefinancesthatcansupportnationalhealthprogramsinallsectors.TheGlobalStrategyplacesthe responsibilityfor ensuringthe efficientuse of resourcesandthegenerationof additionalresources,where necessary,on the ministriesofhealthof the memberstatesof the WorldHealth Organization(WHO).
The enunciationof sound health financingpolicies to govern andguaranteetheefficientandeffectiveutilizationofscarceresourcesforhealthneeds requiresthe maintenanceof an informationsystemfor the healthsector.To meettheseinformationneeds,ministriesof healtharetaskedwitha varietyof concerns,whichmayinclude,among others:
1) Estimationof theorderof magnitudeof the totalfinancialneedsto implementthe nationalstrategyup to the year 2000;
* Associate Professor, College of Public Administration, Universityof thePhilippines.

118 Ma.ConcepcionP. A/filer
2) Procurementof additionalnational funds for the strategy ifnecessaryand ifconvincedthatexistingfundshavebeen usedwisely:
3) Considerationofalternativewaysoffinancingthehealthsystem,includingpossibleuseof socialsecurityfunds;and
4) Provisiontotheirrespectivegovernmentsofa masterplanfortheuseofallfinancialandmaterialresources,includinggovernmentdirectandindirectfinancing;socialsecurityandhealthinsuranceschemes;localcommunitysolutionsintermsof energy,labour,materialsandcash;individualpaymentsforservice;andtheuseofexternalloansandgrants(Mach andAbeI-Smith 1983,pp. 67-68).
II. OBJECTIVES
Thispaper attemptsto reviewthe literatureand informationsourcesonhealthfinancingin the Philippines.Two mainobjectivesare hopedto beachievedin doingthis:a) determinationof howmuchis knownandwrittenon the subject, andb) on thisbasis,provisionof a startingpoint for healthpolicymakersin evolvinga researchPrOgramthat willaddress the gapsindicatedbythe reviewandthe priorityneedsof healthadministratorsandplanners.
Three moresectionsfollowthisportion.SectionIII discussesconcep-tual and methodologicalissueswhich have been raised with regardtoproblemsof healthcare financingindevelopingcountries.
SectionIV focusesattentionon Philippinematerialson healthfinanc-ing and relatedtopics.Originally,the topicscoveredin this sectionwereintendedtoserveas organizingthemesforthepresentationof the materialsdoneon the Philippinesituation.Thisis onewayof checkingthe extentbywhichthethrustsof Philippinematerialsapproximatethe concernsofthoseinthe literatureingeneral.Thespottyandfragmentarycharacterof the localmaterials,however,made thistaskdifficultso that instead,localmaterialswere simplyorganizedaroundfour majorthemes: "sector-widestudies","private-publicresources","nationalhealth insurance"and "community/primaryhealthcarefinancing."
The fifth and final section assesses the state of health financingresearch in the Philippinesand shows its implicationsfor future healthresearchpriorities.
Thispaper,however,cannotlayclaimto beinganexhaustivestudyofall localmaterialson healthcare financingdespitethe deliberateeffort toensurea systematicsearchfor secondarymaterialsthroughthe use ofexistingbibliographiesand research listing,particularly the Philippine

HealthFinancing 119
Coundlfor HealthResearchandDevelopment's(PCHRD) yearlyinventoryof ongoingandcompletedresearchstudieson health services.While nodefinitetime frame was set for the selectionof the materialsreviewed,pdoritywasgiventothosepublishedorcompletedfairlyrecently,e.g.,duringthe lateseventiesand earlyeighties.
Asidefrom the U.P. Collegeof PublicAdministrationand the LocalGovernmentCenter libraries,other library units of the Universityof thePhilippines(U.P.) systemwere alsovisited.These includethe SchoolofEconomics,Instituteof PublicHealthandtheCollegeof Medicinelibredes.Outsideof the U.P. system,materialswere alsogatheredfrom the WorldHealthOrganization(WHO) and the AsianDevelopmentBank (ADB).Thesetsof Ministryof Health(MOH) andNationalEconomicand DevelopmentAuthority(NEDA) materialswhichhavebeen accumulatedby the facuflyand staff of the Collegeof PublicAdministrationin the course of theirresearchworkonhealthadministrationhavealsobeenusefulforthisreview.Special mention must likewisebe made of colleaguesand friends whograciouslyagreedto sharehealth financingmaterialsfrom theirpersonalcollections.These includeDr. LedivinaCadttoand Dr.Victoria BautistaoftheU.P. Collegeof PublicAdministration,Dr.LoretoCabanosofNEDA, Ms.BitulnGonzalesof UNICEF,Dr.DodongCapulof USAID,andDr.AlejandroHerrinof the U.P. Schoolof Economics.
Interviewswere conductedwith officialsof the Ministryof Health,NEDA, Intercare,andthe Securitiesand ExchangeCommission.
III. HEALTH FINANCING: CONCEPTUALAND METHODOLOGICAL ISSUES
The growing literature on health financing highlights a recurring andstillunresolvedissueonhow=healthservices"canbedefinedanddelimited.Researchers on the topic are confrontedwith computationaldifficultiescausedbythelackof anacceptedaccountingframeworkwhichcanfacilitatefinancialanalysisof healthrevenuesand expendituresand minimizepos-sibilitiesof doublecounting.
Raisingrevenuesis onlyonesideofthequestion,theotherbeingthespendingcomponent.Systematicdescription,analysisand assessmentoftheflowof funds/resourcesforhealthservicesnecessitatea determinationofits relationtothe mannerandbasisof allocation/utilizationofthesefundsforspecificservicesdirectedtoparticularareasorto certainsegmentsofthepopulation.Closelyrelated to this is the estimationof the underlyingunitcostsof health services rendered,whether in privateor publicsettings.Giventhefinancingsourcesandexpenditurepatterns,unitcostper serviceis a critical input in establishingthe efficiencyor effectivenessof theinstitutionsrenderinghealthservices.

120 Ma.ConcepcionP. Alfiler
Asidefromthesedefinitionalissues,theotherthemesofthe literatureinvolve:a) financingsourcesandtheir relativeadvantages/disadvantages;b) evaluativeconceptsfor assessingfinancingschemes;and3) methodo-logicaldifficultiesinherent in undertakingcost-benefitandcost effective-nessanalysisfor health expenditures.
DEFINING/DELIMITING THE HEALTH SECTOR. Financing is generallyunderstoodasthe raisingofresources/fundstosupportor payforgoodsandservices.Amongthegoodswhichan individualoragovernmentmaydecideto pay for is health services.In this sense, health care is a "commodity,comparableto othergoodsandservicesinthatindividualhouseholdsandmany publicand privateorganizationsare willingto pay for out of theirincomesandrevenues"(Zschock 1979,p.5 ).Aswithmostothereconomicgoods, the productionof health serviceshas its costs since goods andmanpowerare expendedin the provisionof these healthservices.Theseresources,goodsandmanpowercostsmustbevalued ifoneistodetermineresourcesnecessaryto financethe productionof health services.
A basicprerequisiteinthe estimationof the costsofthese servicesisthe definitionofthe natureof thegoodandtheprocessofproducingit.Theprevailingdefinitionof what constituteshealthdoes not lend to an easydecisionon howhealthservicesmaybecosted. The WorldHealthOrgani-
zation defineshealth as a "stateof completephysical,mentaland socialwell-being and not merely the absenceof diseaseor infirmity"(cited inStraetz, Lieberman, Sardell 1981,p. 4 ).The broadimplicationsof what isnecessaryto achievethisstateof well-being,givenvaryingenvironmentalconditions,areindicativeofthedifficultyofdelimitingtheparametersofwhatconstitutesthe healthsector.
In hispioneeringstudyof healthexpendituresin sixcountries,Abel-Smith (1963) delimitedthe broad spectrum of what constitutedhealthservicesbydividingit intothree principalsections:medicalcare services,publichealthservices,andresearchandteaching.Two typesof servicesfallunder medicalcare. These includethoseprovidedbyhospitalsand thosenot providedby hospitals.Publichealth services,on the other hand, iscomposedof publichealthservicesto persons,environmentalservicesandotherservices.Personalhealthcare describesthesumofmedicalcare andthe subsectionof publichealthservicesdevotedto persons.
• Medicalcare is further defined as referringto services which areprimarilyof a diagnosticor curativecharacterwhilepublichealth servicesrefertothoseof a promotionalorpreventivecharacter.Underpublichealthservices,distinctionisfurthermadebetweenservicesprovidedto individu-alswhocanbe identified(personalservices)andactivitieswhichbenefitthecommunityingeneral(environmentalservices).Thecategory=others"coverlaboratoryandstatisticalserviceswhichdo notfitintoeithercategory(Abel-Smith 1963,p. 36).

Hea#hF_andng 121
Fifteen years later, another work on the topic observed that "acompletedefinitionof the healthsectorwouldencompassall the servicesrenderedby healthpractitionersand the institutionsthroughwhichtheseservicesare administered.This includesmedicaldoctors,nurses,para-medicalpersonnel,dentists,pharmacists,preventivehealthcareworkers,administrativeandothersupportpersonneland allthegoodsandservicesthey providethroughhealthcare institutionssuchas hospitals,clinicsandpharmaciesand throughpreventivehealthcare programs"(Zschock 1979,pp. 6-7).
A WHO manualfor planninghealthfinancingindevelopingcountdesdichotomizedhealthservices-infotwo componentparts: personalhealthservicesand health relatedactivities.Personalhealth servicesare thoseaimed at improvingthe healthofidentifiablepersonswhilerelatedactivitiesare thosewhichpromotethe healthofthepopulationcollectively(Mach andAbel-Smith 1983,p. 15).
The three operationaldefinitionsoffered above suggestthat whilemostdefinitionsareusuallycompreh.ensiveinscope,settingtheboundadesof the health sector may vary dependingon what dimensionsof healthservicesmay be stressed.
Zschock contendsthat dependingon the objectiveof the financialanalysisto be made, a "narrow"or broaddefinitionof the sector may beadopted.A narrowdefinitionmaybe preferredifthe intentionisto arguetheneedformorefinancialassistancetotheprincipalhealthsectorinstitutions.Onthe otherhand,a broaderdefinition,i.e. 'onewhichwillincludea numberofhealthrelatedactivitiesinothersectors,wouldbefunctionalifthepurposeis to.increase coordinationof health care providedthroughthe pdncipalhealthsectorinstitutionswith health relatedactivitiescarded out throughotherorganizations(Zschock 1979,p. 7).
Ithasbeen noted,however,thatalthoughthedatabaseindevelopingcountriestendstobemorelimited,thedefinitionofthehealthsectoradoptedin these countries is generallybroaderpdmadlybecauseof the "greaterdeficienciesinenvironmentalhealthcare prevalentindevelopingcountdesandthe extensiveuse of traditionalcare practitionersbythepopulationforcurativecare" (Zschock 1979,p. 7).
It can thenbe inferredthat the matterof howthe healthsectorof acountrywillbedefinedforpurposesofundertakinga finandalanalysisoftherevenuesandexpendituresof sucha sectorcouldbe an arbitraryconven-tion, dependingon what is feasibleconsidedngprevailingadministrativeconditionsanddata availability.
FINANCING SOURCES. At the heartof any healthfinancingstudyis theidentificationof actualand potentia!fund sourcesto supporttheactivitiesof
the health sector.The sources of fundsdirectly determine the volumeavailable,the regularitywithwhichfundsare remitted,collectioncostsand

122 Ma.ConcepcionP.Alfiler
thestabilityandcontinuityof sourcesthroughwhichservicesare financed.Sourcesof fundsmaybecategorizedonthe basisof: a) service tee
atthetimeofuse (indirectlyfinanced)andservicesforfullpayment(directlyfinanced)(Abel-Smith 1963,pp. 18-19lAbel-Smith 1978,p. 73 );b) publicandprivatesources(Zschock 1979,pp. 19,33); andc)agencyorbodythatoriginallyprovidedthe funds(Mach and Abel-Smith 1983,pp. 18-19).
Arguingforthe valueof tracingfundsdirectlytotheirultimateoriginorsource, Abel-Smithmade a distinctionbetweenfunds made availabletohealth servicesthroughindirectpayment and funds which persons paydirectlytothe providerin returnforgoodsandservicesreceived.Underthisscheme,indirectpaymentincludes:a) generalgovernmentfunds;b) com-pulsoryinsurancefunds; c) voluntaryinsurancefunds; d) employmentinsurance:e) charitabledonations;and f) foreignaid. Directpayment,ontheotherhand,covers"paymentsbyrecipientinreturnforservicesexclud-ing insurancepaymentto compulsoryandvoluntaryinsurancefunds?'-
Zschock'scategorizationschemeputspremiumonpublicand privatesourcesof funds. General tax revenues,deficit finandng (domesticorinternationalborrowing),salestax revenues,socialinsuranceand incomefrom lotteriesand bettingfall under the first category. Private fundingsourceswouldincludedirectemployerfinancing,privatehealthinsurance,charitablecontributions,directhouseholdexpenditureandcommunalself-help (Zschock 1979,pp. 20, 27).
AthirdclassificationdepartsfromZschock'sschemeinthatasidefromprivateand publicsources,it also considersexternal cooperationas adistinct category by itself. Under this third scheme, four sources areconsideredpublic:Ministryof Health,othergovemmentdepartments, re-gionalandlocalgovernments,andcompulsoryhealthinsurance.
Privatesourcesreferto pdvatehealthinsurance,privateemployers,localdonation(cash), and privatehousehold'sdonated labour.Externalcooperationincludesofficial or non-officialassistancefrom outsidethecountry. (Mach and Abe/-Smith 1983,pp. 18-19 ).
The methodsby whichhealthservicesare financedhave importantimplicationswhichpolicymakersmusttake note of. Abel-Smithcitestworeasonsfor this:
First, it is important to examine what different groups of thepopulation are ultimately paying towards the cost of healthservices and how this compares with the value of the servicesthey receive. Second, the method of financing can itself havemajor effects on what is provided and to whomit is provided. Ofspecial importance .for the planning of health services is whoultimately controlsthe spending (thegovernment, social securityfunds, insurance companies, profit or non-profit hospitals orother bodies) and how thatcontrol is exercised.Financial incen-

HealthFinancing 123
tives can influence the orientation of the services (for examplethe orientation given to prevention as against the cure), thesetting wherecare is provided (inpatient, ambulatory or domicili-ary), the/eve/of technology used. the quality of care provided,thegeographicdistribution ofhealth resourcesand last butby nomeans least, thecostofproviding theservices (Abel-Smith 1963,p. 74).
The mannerthroughwhichfunds/resourcesare raisedisindicativeoftheextenttowhichtheyprovideregularand substantialamountsfor health.Thus,fundingcomingfromgeneraltaxrevenuesmaybeunreliablebecauseof the uncertaintybetween budgetaryfunds and actual disbursement.Allocationof these sources is also likely to be influencedby politicalprocesseswhich may conflictwith efficiencyand equity considerations(Zschock 1978,p. 21).
Deficitfinancinghastheadvantageofbeingableto expandhealthcareover a shorterperiodof time.The problemwiththiskindof sourceis thatexpandedhealthinfrastructuremadepossibleby loansmay alsoincreasethe operatingexpenditureobligationsthat mustbe financedfrom internalresources:
Generalsalestaxesmaybedifliculftoadminister,politicallyunaccept-able andeven regressive.
Fundsfrom socialinsurance,on the other hand,may reinforcethetendencyto supporthospital-based,doctor-centeredprograms that areorientedtowardscurativehealthcare.
Amongprivatesources,privatehealthinsurancewhichspreadsthefinancialriskof illnessreducestheprivatecostsof healthservicesbut maytendtobeexpensive.Charitablecontributionsmayleadtodonors'priorities,not coincidingwiththe pressinghealthneedsof the population.Besides,these donorsmay preferphysicalfacilitiesand equipmentas visibleevi-denceoftheirdonations,leavingothersourcesto provideforthe operatingbudget necessaryto fun them. Aid from foreignbilateralor multilateralorganizationsis usuallyextended intimeof naturaldisasters.A disadvan-tage ofthissourceoffinancingisthat it maycreatedependenceonforeignhealthcaretechnologyand materialswhich developingcountriesmaynotbe abletosupportontheirownonceforeignassistanceisnolongeravailable(Zschock 1979,p. 30 ).
The amount of resourcesgeneratedby direct householdexpendi-tures, whichcovers direct paymentto health professionalswho provideservices, is affected bythe premiumof insurancecoverage.Householdswithlowerincomeor thosewithoutinsurancewillspend onlyifthe need isalreadyquiteserious,Publicly-supportedhealthservicesare stillthemajormeansof making servicesavailableto thesehouseholds,
Thealmostuniversaladoptionof primaryhealthcare as anapproach

124 Ma.ConcepcionP.Alfiler
to the deliveryof healthserviceshas shiftedattentionto communitiesasanothersourceof financingfor localhealthservices.Throughcommunityself-help efforts,donationsin kind such as communitylabour and cashdonationsmay add up to a substantialamountat the aggregativelevel.Zschock,however,seescommunity-raisedresources/fundsassupplemen-taryto, ratherthan as substitutesfor, othersourceswithwhichit mustbecoordinated(Zschock 1979,pp. 32-33 ).
On the whole, the value of the sourcesof health finances may beevaluatedthroughthe useoffivecriteria,namely:1) efficiency;2) equity;3)displacementeffects;4) impacton healthcare utilization;and5) impactonhealthcare provisions(Zschock 1979,p. 42 ).
A sourceis consideredefficientifit offersa highernetyieldfor healthcare deliveryoperations,ifit is a reliableor stablesourceof financing,andif it affords managementfreedomandflexibilityinthe use of thesefunds.
Itisequitableif itallowsthesharingofrisksOfillnessacrosspopulation(verticalequity)andiftheburdenoffinancialsupportisdistributedaccordingto abilityto pay (horizontalequity).
Funding sourcesshouldalso be evaluated in terms of whether itsadoptionwill cause the displacementof more equitablesources or theutilizationof health care as well as its effects on health care provision(Zschock 1979,pp. 43-49). "
ASSESSING HEALTH CARE FINANCING SCHEMES. Shouldassess-mentof the nationalfinancing_heme beconfinedto the meritsof eachofthe individualsourcesalone?Sincetherearevaryingeffectsofthedifferentsources,the overalleffectof all financingsourcesmustbe describedandanalyzedinorder todetermine:a) the levelof healthcare supportthat maybe justified,and b) the appropriatenessof these sourcesto generate therequiredamount.
Fiveanalyticalmodelsare normallyusedto justifythe levelof healthcare supportthat mustbe attainedin a country,namely:1) internationalcomparisonsof the levelsof resourcesallocatedto health;2) cost-benefitanalysis;3) cost-effectivenessanalysis;4) consumerdemand for healthcare;and5) minimalneedfor healthservices(Zschock 1979,pp. 35-41).
In hisdiscussionof eachof theseanalyticalmodels,Zschockarguedagainstthe useof internationalcomparisonsasa wayof settingstandardsonhowmucha countrymustspendforhealth.Differencesinexchangeratelevels of monetary units in differentcountriesand in their economy'svaluationof health serviceswithintheirdomesticmarket context makesinternationalcomparisonuntenable.
The valueof benefitsthat investmentin healthserviceswillgenerateisseenasa more rationalebasisforexplaininghowa countryshouldspendonhealth.Thedifficulty,however,of translatingbenefitsderivedfromhealthintoclearmonetaryvaluesvitiateagainstusingthecost-benefitapproachas

HealthFinan_ng 125
a justificationfor moreresourcesto be pouredintohealth.Anotherapproachwhich is often offered as an alternativeto cost-
benefitanalysisiscost-effectiveness.Insteadof calculatingbenefits,effec-tivenessmay be measuredin termsof improvementin reachingspecifictargetsof the population,or in betterhealthcare deliver,. Theseimprove-mentsmay then be relatedto the costs of providingthese services.The
•problemwiththisconcept,however,isthatoneis neverableto isolatewhicheffectsmaybe attributableto healthcare servicesalone.Thus,effects of
• healthexpenditureswhichare likelyto interactwithothersocial services.maynot alsolendto direct measurement.
The conceptualstrengthsof cost-benefitand cost-effectivenessap-proachesarethereforenegatedbymethodologicaldifficultiesencounteredwhencomputationof aggregatebenefitsoreffectsareattempted.Inviewofthese limitations,Zschockproposesthe useof consumerdemandandthedeterminationof minimalneedforhealthas basesforexplaininghowmuchshouldbe allocatedforthe section(Zschock 1979,pp. 9-41).
Consumerdemandfor healthreflected in householdsand businesspreferencesare thoughtto be influencedstronglyby theproviderof healthcare or by the availabilityof insurancecoverage.Citingfragmentaryevi-dencefroma householdsurveyandanalysisof drugsales,Zschockinfersthat householdexpenditureson healthretainsome levelof autonomyandmaybe usedas a basisfordecidinghowmuchtospendonthehealthsector.
Contrastingdemandwithneedwhichmaynotbereflectedas effectivedemandif not backedup by the capacityto pay forthe services,Zschockstressedthe value of consideringthe unmetminimalhealthcare needsoflargesectorsofthe populationas a wayof justifyingthe allocationof moreresourcesfor the healthsector.A minimalneed estimatewhich includescurative and preventive services may be transformedinto a basis formobilizingresourcesin sucha way that health resourcesare reallocatedfrompersonswhoreceivemorethanwhattheyneedtothosewho havelessthanwhat they need (Zschock 1979,p. 41).
METHODOLOGICALISSUES. Healthfinancingscholarsmustcontinuallygrapplewith methodologicaldilemmasstemmingfromtwosources:a) theabsenceof a standardaccountingframeworkwhichwillprovidethemwiththe handlesthey need indealingwith healthexpensesof varioussectors;and 2) the difficultyof measuring effects and benefitsof health sectorserviceswhichcould leadto a betterestimationof the impactof resourcesallocatedto thissector.
To deal with these problems,particularlythe first, health financingplanningmanualsfor developingcountries havebeen preparedto assisthealthofficialsinthesecountriesinsetting.upa systemforthecollectionofhealthfinanceandexpendituredateovertime.One suchmanual(E.P. MachandAbeI-Smith 1983) emphasizesthreeprinciplesforresearchersworking

126 Ma.ConcepclonP. Affiler
fromexistinginformationandaccountingsystems:
a. Ensurethat all major items of finance and expendituresareincluded;
b. Use figuresforexpenditureactuallyincurredratherthanfinancebudgeted(whichmaynothavebeenallocatedor,ifallocated,notspent);
c. Avoiddoublecountingof moneytransferredfromonesourceoffinanceto anotherbeforeitisspent,whichthusappearsinmorethan oneaccount.(E,P. Mach and Abel-Smith 1983, p. 39 ).
Payingparticularattentionto the assessmentof financialviabilityofWoildBankfundedprojects,De Ferranfirecommendsthatan "affordabilityanalysis"be madefor healthprojectsto determinewhetherthosewhoareexpectedto commitresourcesto the projectare able andwillingto do so.Essentially,thismeansestimatingforthefollowingaspectsoftheinstitutionsorgroupsinvolved:
a) the coststhey wouldbear as a resultofthe projector program;b) funds (or otherrelevantresourcessuchas volunteerlaborers)
availableto them;andc) other demandson these resourcesfor other projectsor pro-
grams.
Figuresarrivedat fromthese estimationscanthen be projectedovertimeto determinewhethersufficientfundswillbe available.
If not,then the amountof the shortfallvis-a-visthe requirementandtotalresourcesmay be determined(De Ferranti 1983, p. 53).
•IV. HEALTH FINANCING IN THE PHILIPPINES
The literatureon health financinghasconsistentlystressedthe needfor a comprehensivesector-wideperspectivein evaluatingthe differentwaysof utilizingfundsto supporthealthactivities.The connotationof sucha broadviewof the sectoris aptlycapturedby a leadingproponentof theidea, to wit:
Estimatesof all sourcesproviding means forhealth activities andof total expenditures in the health sector are essential informa-tion for those responsible for a country's health policies. Only ifa country plans the whole of its health services - public andprivate - will plans have a prospect of success ... It is proposedthat health policy makers should go beyond the conventionallimits of public health and attempt to match the financing of thetotal sector with major health goals (E.P. Mach 1978,p. 7).

HealthF/nanc/ng 127
Realizingthevalueofthisholisticperspective,thisreviewwillproceedbyfocusingfirston studieswhichattemptto examinecomprehensivelythefinancingneedsof the Philippinehealthsector.Priorityisgivento thistypeof studiesas they typifythe kind of comprehensivethinkingexpected ofplannerswhomustformulaterationalehealthpolicies.Thesekindof worksare referredto as "sector-widestudies'.Fromthe data andanalysisgiveninthese studies,anattemptto highlightsomedimensionsofthe financing/expenditureprofileof the Philippinehealthsectoris made.
Other Philippinematerialscovered in this reviewshall also be dis-cussed by clusteringthem intothe followingtopics:a) public/privatere-sources;b)nationalhealthinsurance;andc)commur,ity/pdmaryhealthcarefinancingand "demandstudies'.
SECTOR-WIDE STUDIES. Asidefrom an ongoing Asian DevelopmentBank (ADB) commissionedstudyon health financingin the Philippines(whichisexpectedto becompletedbyFebruary1987), thereappearsto beno empiricalresearchwhichdwellsolelyon thefinancingof thepublicandpdvate health sectorsof the country.Instead,the reviewshowsthat thefinancing aspects may be discussed as one of the sub-topics in anevaluationof theperformanceand resourceneedsof thissector.It ismoreof the lattertypeof studiesthat are consideredash"sector-widestudies."
Underthiscategory,three documentspreparedbytwo institutions-theWorldBankandNEDA - arediscussed.Theydescribeandanalyzehowrevenuesfor healthservicesare raisedand allocatedfor certainobjectsofexpendituresover a particularperiodoftime.
The 1984 WorldBank review of the population,health and nutritionsectorshasthree chapterson expendituretrends,programfinancingandexternaland alternativefinancingforthesethreesectors(WorldBank 1984,pp. 79-85).The 1985 NEDA proposedprogramfor improvedhealth caredeliverysystem,on the otherhand, devotesa substantialportionto thesector'sfinancialneedsand offeredproposalsaimed at developing serf-relianceamongindividualsinfinancingtheirheaKhrequirements,therebyffreeing"governmentfundsfor utilizationin the needs of indigentgroups(NEDA 1985 b ).
AnotherNEDA publication(NEDA 1982a ) analyzes,among others,trendsingovernment,familyandpersonalconsumptionpatternson healthservicesfor the decade of the seventies,usingcore indicatorsto assessprogram impact,programindicatorsto determineadequacy of programcompared to ascertained needs and access indicatorsto show serviceutilizationandthe physicalorfinancialaccessibilityofthe Ministryof Health(MOH)see'vices.It isinterestingto note,though,thatthesectordefinitionofthese works differs. While the World Bank review covers the health,populationand nutrition sectors, the 1982 NEDA document discusseshealthand nutritionand the 1985 NEDA proposalis specificto the health

128 Ma.ConcepcionP. Alfiler
sectoralone.The abovedocumentsrevealthe followingabout the financingand
expenditurepatternsof the Philippinehealthsector:
1. Health expenditures,as a percentageof total nationalgovern-ment expendituresdecreasedfrom 4.9 percent in 1970 to 3.5percentin 1980 (NEDA 1982,p. 79 ).
2. The Ministryof Health, which accountsfor 70 percent of allgovernmentspendingon health,received4.2 percentofthetotalnationalgovernmentappropriationsin1985. Using1978 pdces,theappropriationforhealthservicesfrom 1978to 1984 recordedan annual averagedecreaseof 1.8 percent (NEDA 1985 b, p.49).
3. AllocationofMOH expendituresbyregionin1981 showsthatonthe basisof the ratioof regionalexpendituresto regionalpopu-lation,expenditureswere inequitablydistributedin favor of sixout of 13 regions.By nature of inputs,suppliesand materials(includingdrugs)receivedthe largestshare (40 percent),withpersonnelservicescominginasthe secondlargestcomponent(37 percent) for the same period(World Bank 1984,p. 84).
4. In terms of nature of servicesprovided,the share of curativeservices"have fluctuatedbetween51 percent to 61 percent ofcurrentoperatingexpendituresfrom1980-1986,whileexpensesfor preventiveservicesforthe same perioddecreasedfrom 48percentto 38 percent.
5. The Family Income and ExpenditureSurvey (FIES) indicatedthat 1.9 percent of totalfamilyexpenditureswere set aside formedicalcare. This figureis not significantlyhigherthanthe 1.8percentrecordedfor 1971 (NEDA 1982a).
6. Total personalconsumptionon medical care increased fromP1.47 billionin 1977 to P1.69 billionin 1980, althoughas aproportionto total expenditures, medical care expendituresremainedconstant(NEDA 1982 a, p. 80 )i
7. In 1982, about PS0millionor 3 percentof MOH appropriationswerefinancedbyforeigngrantsandloans;21percentofthiswasspenton capitalexpendituresalone.
8. Asidefromthebudget,90 percentof MOH resourcescame fromfees for hospitalservices. From 1978 to 1982, however, theproportionofcurrentMOH expendituresreceivedthroughsew-ice chargeshas fallen from 14 percent in 1978 to 8 percent in1982 (World Bank 1984,p. 90). o
PUBLIC/PRIVATERESOURCES.Itwillbenotedthatexceptforthedataonindividualand householdexpenditures,nothingsubstantialcan be said

HealthFinancing 129
abouttheperformanceorcostsofthemedicalinstitutionsoperatingforprofitwithinthe healthsector.This is becausewhilethereare organizeddata onthe publicsector, informationon the operationsand performanceof ,theprivate sector is hardly available. This is not an uncommonproblemencounteredby healthfinancingresearchersin developingcountries.
Awelcomecontributionthatlessensthe paucityofworkinthisarea isCharlesGriffinand Vicente Paqueo's 1986 paper on publicand privatemedicalresourcesandhealthexpendituresinthePhilippines.Byorganizingpubliclyavailable data on the health sector, their paper describedthecountry'smedical system, traced its historicaldevelopment,and thenanalyzed the distributionof its fadlities. After exan ning trend data ongovernmentresourcesand expenditures,they observedthat:
1. Theprivatemedicalsectorinthe Philippinesaccountsforat leasttwo-thirdsof healthfacilitiesandexpenditures.Thissectorledanenormousexpansionand diffusionof hospitalbasedresourcesfrom 1972 to 1983.
2. MOH per capitacostsinconstant1972 pricesrosefrom1=5.61in 1961 to'P7.98 in 1980.
3. Nationalexpendituresurveysindicatethat bothruralandurbanhouseholdsspentslightlylessthan2.0 percentoftheirbudgetsinmedicalservices,withtwo-thirdsofprivateexpendituresgoingto the providersandhospitals.
4. Two-thirds of medical expendituresoriginated in householdbudgets,not governmentbudgets(Griffin and Paqueo 1986,p.33).
NATIONAl HEALTH INSURANCE. Individualhealth needs may be paidforthroughdirectfee forservice,availmentofthe nationalhealthinsuranceorthroughprivatemedicalinsuranceprograms.
The PhilippineMedicalCare Commission,whichwas organizedin1969, aimsto graduallyprovidehealthneedsof the populationby makingavailabletothema comprehensivepackageof medicalservicesthroughthecoordinateduseofgovernmentand privatemedicalfacilities.Implementedintwophases,Medicare'sPhaseIwhichtookeffectin1972coversregularlyemployedsectorof the populationwho are also membersof the Govern-mentService InsuranceSystemand the SocialSecuritySystem.Phase IIwhichhasbeenpilotedinBauan,BatangasandinUnisan,Quezonstarting1985, coversthe restof the population.By1985, PhaseI has expandedto22,783 GSIS and SSS rr_mbers and their legaldependents,comprisingsome43.8 percentof thetotalpopulation.
Medicare'scompulsorycontributionsof 2.5 percent of the monthlysalary are collected throughthe SSS and the GSIS. Employersshoulder1.25 percent of the amount with the employees paying the other 1.25percent.

130 Ma.ConcepcionP.Alfiler
Since1975, contributiontoMEDICARE hasbeen increasingexceptin1984. By1984, a totaloft_410.4 millioninbenefitpaymentswas paidfromthe funds.Of thisamount, P239.4 millionwent to SSS membersand theremainingt_171.0millionto GSIS (NEDA 1985a, p. 31).
Despiteincreasesin its rnenthlycontributionwhichresultedin GSISandSSS membersdoublingtheiraveragecontributionsbetween1972 and1981, medicarecontributions'real value fell by 40 percent (World Bank1984,p. 91). In1980, a PhilippineHospitalAssociationstudydisclosedthat54 percentof totalaccommodationsinprivatehospitalsand60 percentofgovemmentpatientsare medicarebeneficiaries.The same studylikewiseshowedthat the proportionof hospitalizationcostsubsidizedbyMedicarehasgonedownto 28 percentfrom thetarget70 percentof cost whichtheprogram originallyintendedto subsidize (NEDA 1982 a, p. 86). Morerecently,a newspaperitemcitedthe MOH DeputyMinister'sannouncementof a proposedincreaseinMedicarebenefitsof between30to 40 percent.Itwasestimatedthat Medicarepaysonly25 percentof thehospitalexpensesof itsmorethan20 millionbeneficiaries(Malaya November28, 1986,p. 3),
The MedicalCare Health InsuranceFundmanagedbythe PhilippineMedicalCare Commissionreporteda cumulativecollectionof-P3.6M anda cumulativedisbursementoPP2.9 M as of 1983. Cumulativenumberofbeneficiariesservedaddedupto 11.6 M in 1983and averagepesovalueofc!aimsprocessedis estimatedatt_273.98 forthesame year (NCSO 1985,p. 298).
Griffin,Akin,et al, intheirdescriptionand analysisof the PhilippineMedical Care Plans, notedthat even if the Medicare'sreal benefitsandcontributionscontracted,theystillcomprisea SignificantcomponentofthePhilippinehealthcaresysteminabsoluteterms.UsingWorldBankfigures,they computedMedicare'sshareofthe health sector:
"The national government allocated1=2,216 M to health pro-grams in 1981, of which: P1,814 M went to MOll. Privateexpenditures in 1980on medical care were4,988 million pesos,of which approximately 55 percent (2,743.4) was spent onhospital and physician fees. In 1981, oontributions to Medicarewere 495 million pesos. Claims payments were 340 million.Medicare contribution which represent health expenditures tothose paying represented 18percent of present expenditures onhospitals and physicians in 1980 and 27 percent of the 1981MOH budget. Therefore, while the real value of Medicare valuebenefits has declined, the program's receipts still account forabout a fifth of all expenditures in hospitals and physicianservices and about 6.5 percent of all health related expendi-tures in the Philippines (Griffin, Akin, et al. 1985,p. 17).
UsingsampleclaimsforGSISandSSS, thissamestudyexaminedthe.

HealthFinancing 131
characteristicsofparticipantsinthesetwoprograms,lookingintothenatureofdiseasesforwhichmedicalservicesweresought,claimspaymentandthehospitalutilizationpatternsevident among these members. Interestingfindingsof thissurveyindicatedthat:
1) Medicarepatientsseemto stronglypreferuse ofprivatehospi-tals exceptwhen incomeor absenceof requiredfacilitiesworkagainstthispreference.
2) Medicare'sexistingfee structureis notonlyregressivebuthighlyinelasticas well. Becausethe fee structureremainsconstant,after a certain level of income, payments as a percentageofincomefall beyondthetop bracketof the contributionscale.
3) The Medicaresystemis completelyorientedtowardscurativecare andhospitalization(Griffin, Akin, eL a11985,pp. 34 & 37}.
The influenceof Medicare'scoverageon a sickperson'sdecisiononwhoamongmedicalpractitionersiscleadydiscussedinanotherstudywhichanalyzes 1983 householdand communitydata from the Bicol region.Schwartz,Akin,eL a/discoveredthatwhileelectdtication,barangayhealthaidsandbarangayhealthstationsare predictorsof the choiceof practitio-nersfor sickadults,themostimportantexplanatoryvariablesappearto bethe perceivedseriousnessof theillnessandwhetherthe personiscoveredbyMedicare.A seriously-illpersonwithMedicarecoverageis morelikelytoselecta privatemodem practitioner.(Schwartz, Akin, et. al 1985,p. 11).Beyondthisfinding,itcan beconcludedthat a decisionlikethisoccursnotsimplybecauseof Medicarecoveragebutthe factthat thispersonis likelytobe reguladyemployed,withsomeformofstableincomeandcanthereforeaffordto pay hospitalizationfees.
Outsideof Medicare'sfinancialsupportfortheirmedicalneeds,SSSand GSIS memberscan avail of sicknessand-disabilityrelatedbenefitsmeantto replacelostincomeof individualsasa resultofsickness.GSIS andSSS providethatsicknessand incomebenefitsshallnotbe lessthenP4.00andnotmorethanP20.00/day.Membersmayqualityforthesebenefitsonlyiftheirconfinementlastat least4 daysand the workershave usedup theirsickleavecredits.In1984, SSSpaida totalofP259 millionfor healthrelatedbenefits.Thisconstituted25 percentofthetotalbenefitsfortheyear (NEDA1985a, pp. 45-46).
Private insurance companies also constitute another avenue forfinancingmedicalexpensesof thepopulation.Asof the endof 1983, therewere 99 authorizedprivatecompaniesoffering healthand accidentInsur-anceinthe Philippines,82 ofwhicharedomestic,13 are foreigncompaniesand 4 are professionalreinsurers.Total claimson health and accidentinsurancefor the same period added up to P65.8 million as againstpremiumsoft=143.7 million(NEDA 1985,p. 46).

132 Ma.ConcepcionP. A/filer
COMMUNITY/PRIMARY HEALTH CARE FINANCING. The adoptionofprimaryhealthcare asthe government'smajorapproachto the deliveryofhealth servicesushered in the stress on self-relianceand concomitantvalues such as afferdability,appropriatetechnologyand mobilizationoflocalresourcesto fulfillthe community'shealthneeds. Inkeepingwiththisphilosophy,primary health care activitiesof communitiesare gauged inaccordancewiththecommunityandthe government'scapacityto sustaintheseactivities.
To ensurethat localconditionswillbeadequatelyrespondedto, localcommunitieswere given leeway to decide for themselveshow to raiseresourcesto supporttheirbasichealthneeds.Withintheconfinesof smallercommunities,the matchingof health needs and resourcesmay be lesscomplicated,thus more manageable.There is a need, however,to coordi-nate and synchronizethesecommunityeffortson a nation-widebasistoensure complementationof community,public and private financingsources.
Meanwhile,as morecase studiesdescribingvariousexperiencesoncommunityfinancingcome to light,twoobservationsseemto characterizethese experiences:
1. The "resourcegap"betweencostsof primary health care andexpendituresbeingmade for primaryhealthcare has becomeclearer,and
2. While central governmentserves as the principalsource offinancingfortheextensionof primaryhealthcare,studiesshowthat non-governmentalexpendituresfor health were sizeable.These expenditureswerealsofoundto supportprivatecurativeservicesinsteadof promotiveor preventiveservices(Russelland Reynolds, undated, p. 11).
Theseissuesrequiredthatthere shouldbe more systematicmonitor-ing and documentationof the experiencesof communitiesin mobilizingresources,whetherintheformof cashorin kind,to support,partlyorfully,basicpreventiveorcurativehealth servicesforitsmembers.
USAID PRIMARYHEALTHCARE FINANCINGPROJECT.Twoyearsafterthegovernmentformallylaunchedthe nationalprimaryhealthcareprogramin the Philippinesin 1981, USAID introducedits Primary Health CareFinancingProject.This projecttriggeredconsiderableinterestandinitiatedpioneeringstudiesincommunityandprimaryhealthcare financingin thePhilippines.
Scheduledfor implementationby July, 1983, thisproject aimed at"increasingaccess to and utilizationof sustainableprimary health careservices managed and financed by communities and the Philippinegovernment"(USAID 1983,p. 5). The projectsoughtto accomplishthese

HealthFinancing 133
goalsthroughthree sets of interrelatedactivities:(a) the pilottesting ofvariouskindsof healthfinancingschemesindifferentpartsof the countryand with diversegroupsand institutions;(b) special studiesand policyanalysison publicand privatehealth sectorfinancing,the operationofvillagedrugstores,assessmentofthebarangayhealthvolunteersprogramand the performanceof midwives;and (c) a servicedeliverycomponentwhichwiUseektostrengthenMOWsinstitutionalcapacity(USAID 1983,pp.7-19).
At least five researchreports/publicationson healthcare financingweredoneinpreparationfor,and inconnectionwith,oraspartofthisproject.
The first is a studyon the health seekingbehaviorand expenditurepatternsfor primaryhealth care in Cabagan, Isabela.A surveyof 146householdheadsinthree barangays,lookedintothe factorsthat affectedpatternsof expendituresina ruralcommunitywithreferenceto respiratoryandgastrointestinalconditionsinchildrenbelow6 yearsold,infantnutrition,matemitycare andchildimmunizationand familyplanning.
The researchrevealedthattherewasa high(81.8 percent)incidencerateofgastrointestinalandrespiratorydiseasesintheunder-sixagegroup.Todealwiththesecases,householdsinCabaganresorttoover-the-countermedicationand home remedies. Moreover, utilizationof curative careservicesindicatespreferenceforhighlyspecialized,moderncurativeserv-ices,i.e., professionalsratherthantraditionalproviders,privatemorethanpublicservicesandphysiciansratherthanlowerlevelhealthprofessionals.
Thisstudy,likewiseshowsthat"... healthseekingforcurativecare iscrisisoriented.Factorsrelatedtothepattemsofuseof healthprovidersarecompetence,accessibilityandeconomicconsideration..Themeanmonthlyexpendituresfor respiratoryandgastroentedtisconditionsinchildrenundersix years is P7.40. This is approximately2.3 percentof the householdincome.Factorsthattendto showpositivecorrelationwithcostare thetypeofhealthproviderssought,accessibilityofhealthservicesandtheperceivedseriousnessof the disease"(Lariosa 1982,pp. 136, 151).
The secondresearchreportcommissionedas partof thepreparationfortheUSAIDprimaryhealthcarefinancingprojectwasanexploratorystudyon local resourceutilizationschemesfor selectedcommunity-basedpri-maryhealthcareprojects.Itdocumentedsevencases,representingvariousformsoflocalresourcemobilizationandutilizationschemesandfocusedonthe kindsof healthservicessupported,the degreeofpeople'sparticipationintheschemes,the=hidden"costsinvolvedand the resourcescomingfromexternalresourceswhichwere used to augment locallygeneratedfunds/support(Alfiler 1982).
Thisstudyshowsthat localresourcesutilizationschemesforcommu-nity-basedprogramsinhealthtend to be one-shotin natureandconsistofirregularfund-raisingactivitiesinitiatedand implementedby communityorganizations.Resourcesmobilizedthroughtheseeffortstendto be meager

134 Ma.ConcepcionP.A/filer
and limitedmostlyto financingthe purchaseof drugs.There are existinginsuranceschemesforthosewhoareunder-orunemployedbuttheyaretoocomplicated for the communities to manage for themselves. Theseschemesalsotend to generatelimitedresourceswhichare grosslyinade-quate to covercostsof comprehensivemedicalservicesnecessaryatthecommunitylevel.This meansthatthe resourcesgeneratedwillhaveto besupplementedwithadditionalresourcesifthey mustsupportthe provisionof adequatehealthservicestOcommunity-basedprograms(A/filer 1982,p.74).
A thirdstudywhichwas cloneinconnectionwith,but not supportedsolelyby, USAID was a two year operationsresearchprojectfunded byPrimaryHealth CareOperationsResearch(PRICOR) andcarriedout insixvillagesin Iloilo(alsothe siteof anotherUSAID project,the Panay UnifiedServicesfor Health) (Osteria and Siason, undated).
This researchsoughtactive communityinvolvementin determiningthe natureof the financingschemesand howthese could be set up andmanaged.The financingschemewhichthe sixvillageseventuallychosewas the contdbutionof a flat rate on a monthlybasis and the voluntarycontributionfromproceedsof salesand farmproduceandlivestockaswellasthe donationof services.Exceptforonebarangaywhichoptedtouse itscontributionas anemergencyloanfund,allotherbarangaysdecidedtousethemoneyraisedtofinancethe operationsof a villagedrugstore.Contribu-tionscollectedfromthehouseholdsrangedfrom=P'2.50toP7.09. Aftera yearof operations,the variousvillagedrugstoresrealizedprofitsrangingfromP120.54 to1_567.02(Osteria and Siason, undated, pp. 102and 159).
Theoutcomeofthisresearchunderscorestheneedto keepstructuresforfinancialschemesinruralareassimpleenoughforparticipant-membersto understandwhatthey are payingfor,howtheywillbebenefitedandwhatcontrolmeasuresare adoptedto safeguardtheircontributions.This expe-rience also indicatesthat singlepaymentschedulesmaybe more efficientifnocollectionsystemisfirmlyestablishedtoattendto paymentspreadoveran extendedtime period(Ostetia and Siason, undated, p. 99 ).
An evaluationof the performanceof the government'sBotika SaBarangay program,the fourthstudy,representsoneof the specialstudiescompletedunderthe USAID PrimaryHealthCare FinancingProject.Thisstudywas undertakento testthe assumptionsthat the Ministryof Health'sBotika sa Barangay (Village Drugstore) programwill succeed to makeessentialdrugs accessibleand affordableto the communityonly if thisprogram operatesas a community-basedbusinessenterprise able togeneratesufficientoperatingfundsto financethe regularreplenishmentofstocks(ARC Associates 1985,p. 6 ).
The profileof a viable(ableto generate fundsforcontinuousopera-tions) and effective(can providemajorityof village residentsaccess toneededdrugsat a pricethey can afford)villagedrugstoreturnedout to be

HealthFinancing 135
onewhich: 1)hasa capitalizationof aboulP700.00: 2)generatesanannualsaleof P1,334.00;3) observesa 24 percentmark-upon itssale price;4) ispartof a general or communitystorethat operatesin the area; and 5) ismanagedbya BotikaSaBarangayaidewhoisknowledgeableindispensingmedicineandbelongsto a householdwitha relativelyhigherincomelevel.
AmajorcomponentoftheUSAIDpdman/healthcare financingprojectisthedesignandpilotingofinnovativehealthcarefinancingschemeswhichmay be replicatedif foundworkable. Deliberationson the merit of fourproposalssubmittedto the PhilippineCouncilfor Health Research andDevelopment(PCHRD) were the objectivesof a Seminar-WorkshoponHealthCare Financingsponsoredbythe USAID andthe PCHRD.
The financingschemesconsideredfor possiblefundingwere thosewhichexploredthe useof fourprospectivefinancingmodels:a) communitybased,b)government�hospitalbased,c)enterprisebased,andd)thehealthmaintenanceorganization.The publishedproceedingsof this seminar-workshoppresentthestrengthsandweaknessesof thesefourproposalsatleastintheformtheywere initiallypresentedforpossiblefunding(rPhilippineCouncil for Health Research and Development 1985,pp. 93-110 ).
Two demand studiesutilizingdata from the 1978 and 1981 Bicolmultipurposesurveystestedthe extentto whichfactorssuchas distance,income,time andcashcostsaffectthe demand forhealthcare servicesinthe BicolRegion.Usingthe 1978 surveydata,Chingdisclosedthat neitherincome nor cost deterred the poor from availing of public health careservices.However,thosewith lowerincometendto showlowerutilizationof modemprivatefacilities(Ching 1986,pp. 149-150 ).
Onthe basisof theiranalysisof the 1981 Bicolmultipurposesupple-mentalsurveydata,Akinet.al disclosedthatvisitprice,drugcosts,transportcosts,transporttimeandwaitingdidnotgreatlyaffectdemandpatternsforessentialoroptionalhealthservices(Akin 1986,p. 773). Akinlikewisenotedthat insteadof servingthe poorersectionsof the population,free govern-mentclinicsappearto serve many higherincomepatients.Moreover,hearguedthatitmaybeknowledgeandoutlookandnotpovertywhichkeepthepoor fromusingmodernhealthservice(Akin 1986,p. 774 ).
V. RESEARCH AND POLICY IMPLICATIONS
What do the findingsof allthesestudiesimplyfor researchprioritiesinhealthcare financing?
Theearliernotionthatthereishardlyanyempiricalresearchon healthcarefinancingandrelatedtopicsinthePhilippineishardlyreliable.Itisclearthat there is a small but steadilygrowinglocal literatureon the subject.Valuabledata on publichealth servicesare availablebut they need to beorganizedand analyzedto providethe answersto policyquestions.Likemostdevelopingcountries,thereisvirtuallynosystematiccollectionof data

136 Ma.ConogpcionP. Alfiler
onthe operationsandcostsolhealthservicesprovidedbytheprivatesectorinthe Philippines.
It is interestingto notethat externalfundingagencies(WorldBank,USAID, Asian DevelopmentBank) play a conspicuouslyactive role indirectingattention_ our initiatingstudieson health care financingin thePhilippines.This phenomenonmay merelysignala currentinternationalinterestin health among financial institutions.However,this may also beindicativeof the lowlevelof priodtyattachedto healthfinancingbyhealthadministratorsindevelopingcountrieslikethePhilippines.Thismayalsobelargelybecause,when confrontedwithso muchdemand for very limitedresources, health administratorswould rather use these resourcesfordeliveryof servicesratherthan for researchactivities.
Couldthestrongpresenceofinternationalinstitutionsinthisfieldalsosuggestthe relativelylimitedappreciationfor comprehensivesector-wideplanningand pdodtizationof resourcesandexpensesamonghealthadmin-istratorsindevelopingcountrieslikethePhilippines?Healthfinancingisonlyoneof thetoolsforbringingaboutthestate'spolicyonthedesiredallocationof healthresourcesand services.Yet, evenbeforethistoolcan be utilizedfor meaningfulpolicyanalysis,a reliabledata base mustsystematicallyproducethe informationwhichwillallowperiodicanalysisof expendituresandsourcesof finances inboththe pdvateand publicsectors.
Forthispurpose,thefollowingareasforpolicyresearchareforwardedassumingthat health administratorsand plannerswill now imbibe thecomprehensivesector-wideperspectivenecessaryinanysignificantanaly-sisof healthfinancingsourcesas a meansof effectinggreaterequityandefficiencyinfunding,distributionandprovisionof healthservices:
1) The development of a low cost health financinginformationsystemthat will utilizemostof the data that are producedbyexisting management informationand accounting systemsbeingobservedinpublicandprivateinstitutions.Moretime andeffortmayhaveto be devotedto the privatesectorsince itis inthisarea wheredata is most scarce.
2) If the utilizationof existinginformationsystemsfor bothpublicandprivatesectorsis notfeasible,a basicfinancialdata collec-tionsystemwhichwillmaximizeuseof data producedinprivatehospitalsandother healthinstitutionscan be devisedto allowcomparisonsacross institutionsover time. In settingup thissystem,emphasismay be givento broad ordersof magnituderatherthan preciseaccountingforeach sourceof funds.
3) Oncethisdata collectionsystemis inplace,it canbe usedas abenchmarkfor policystudieswhichcan seek to:
3.1 identifyareaswherethenature,sizeor appropriatenessoffinancespromoteor frustratehealthpolicyobjectives;

HealthF/nanc/ng 137
3.2 showwhereresourcescouldbe used moreefficiently;3•3 demonstrateanylackof equityintheuseofresourcesinthe
publicor privatesectors;3.4 drawattentionto alternativeways oftappingresources;3.5 determinethegapbetweenthefinancialresourceslikelyto
be obtainedandthe resourcesneeded to movetowardscertaingoals•(Mach and AbeI-Srnith 1983:14 ).
4) The studiesreviewedabovealreadyindicatecertaincharacter-isticsoftheexistinghealthfinancingsystems,i.e.,theregressivenature of the MEDICARE, the factors which determinethedemandfor publicandprivatehealthservicesincertainregionsof thecountry,thelevelsandsourcesoffundsraisedbycommu-nities.Policymakerscan startdeterminingwhetherthese find-ingsconstituteadequatebasisforpolicyreviewandrevision.
A finalnoteof cautionmaybe inorderforthisreview.Thedetermina-tionofthemonetaryvalueofthepublicandprivateresourcesthatgointotheproductionof health serviceswilldefinitelyhelp in the estimationof howmuchfundswillbe necessaryto providetheseservices•It ishopedhoweverthat the generationof this informationwill lead to greater equity in thedistributionof resourcesrather than intensify the current tendency tocommodityhealth servicesandthusrenderthemevenmoreinaccessibletothe greatermajorityof the Filipino.
BIBLIOGRAPHY
Abel-Smith,Brian.PayingforHealthServices:A Studyof theCostsandSourcesofFinanceinSixCountries.Geneva:WHO,PublicHealthPapersNo.17,1963.
•AnInternationalStudyofHealthExpenditures.Geneva:WHO,PublicHealthPapersNo.32, 1967.
withAlciraLeiserson.Poverty,Developmentand HearthPolicy.Ge-neva:WHO,PublicHealthPapersNo.69, 1978.
Akin,JohnS.,CharlesGriffin,et.al."TheDemandforPrimaryHealthCareServicesinthe BicolRegionof thePhilippines."_/c Development& CulturalChange(July1986),755-782.
Alfiler,Ma. ConcepcionP. "LocalResourcesUtilizationSchemesfor SelectedCommunity-Besed/PdmaryHealthCareProjectsinthePhilippines."PreparedforUSAIDunderContractNo.492-0249-C-80-1142-O0;(November5, 1982),(manuscript).

138 Ma• Concepcion P. Alfiler
• Partnershipand Responsibilityin FinancingHealth Activities:Non-Governmentand PrivateVoluntaryOrganizationsinthe Philippines.Paperpreparedforthe WorldHealthOrganizationasbackgrounddocumentfortheTechnical Discussion,Fortieth World Assembly, (September 30, 1986),(manuscript)•
ARC Associates•"StudyonBotikasa BarangayOperations•"Vol•I• PreparedfortheMinistryof Health,QuezonCity, 1985•
AsianDevelopmentBank.Useof Rural HealthServices Proceedings'ofthe RegionalSeminar on the Use of RuralHealth Services.Manila:Asian DevelopmentBankand East-West Center (January20-25, 1986).
Berman,Peter.Equity and Cost in the Organization of PrimaryHealth Care inJava,Indonesia. DepartmentofAgriculturalEconomics,CornellUniversity:CornellInternationalAgricultureEconomicsStudy.(March,1985).
Caldwelt, J.G• and Duncan, William• Illustrative Agency Monitoring System toSupport Socio-Economic Analysis of Health Systems in the Philippines•Submittedto NEDA, PhilippineInstituteforDevelopmentStudiesundercon-tract No•492-0295-02. (August30, 1981), (manuscript).
Cayapas,Eleo. "PromotingWorkersWelfare ThroughEmployeesCompensation."Philippine Labor Review. Vol. 8 No. 3, 97-116. (Jan-July1984).
Ching,Panfila.Public Provision and Demand for Health Services: A Case Study ofBicol. DoctoralDissertionsubmittedtothe U.P. Schoolof Economics.(May1986).
De Ferranti, David• Some Current Methodological Issues in Health Sector andProject Analysis. World Bank:PHN TechnicalNote5, GEN 24. (December1983).
• Paying for Health Services in Developing Countries: An Overview.World BankStaffWorkingPapersNo: 721, 1985,
DemographicResearch and Development Foundation."An Assessmentof thePopulation, Health and Nutrition Programs, 1978-1985." Manila: Demo-graphicResearchand DevelopmentFoundation,1985.
Feldstein,PaulJ. Health Care Economics.New York:JohnWiley andSons, 1979.
Griffin, Chades,John S. Akin, et. al. =Descriptionand Analysisof the PhilippineMedicalCarePlan•"Submittedto SigmaOne CorporationandUSAIDinpartialfulfillmentof Contract ORT-0082-C-003353-00. (March 20, 1985), (manu-script).
and VicenteB. Paqueo "Publicand PrivateMedicalResources andHealth Expendituresinthe Philippines."(May 26, 1986).

Health Financing 139
Grifflths,A. and Bankowski.Economics and Health Policy. Xlllth Councilfor Inter-nationalOrganizationsof MedicalSciences(CIOMS) RoundTable Confer-ence and the Sandoz Institutefor Health and Socio-EconomicStudies.Geneva. 1980.
Havighurst, Clark C. Deregulating the Health Care Industry: Planning forCompetition. New York:BallingerPublishingCompany,1982
Kintanar, Q.L. (ed.). The Pharmaceutical industry in A-SEAN Countries:ThePhil_oines. United Nations Asian and Pacific DevelopmentInstituteandNationalInstituteof ScienceandTechnology.Manila.
Maceda, Rodolfo.Method of Cost.Analysis for Phil4opineGovernment Hospitals.OccasionalBudgetPapers(3). 1978.
Mech. E.P. "TheFinancingof HealthSysteminDevelopingCountries:DiscussionPaper.Socia/Sc/ence and Medicine. Vol. 12 No. 1C/2C. 7-11.
andBrianAbel-Smith.Planning the Finances of the Health Ses¢_: AManual for Developing Countries. WHO. 1983.
Ministryof Health."NationalHealth Planfor1979." Manila:Ministryof Health.1979.
• *Ministryof Health Budget,1946-1986."Preparedby FinancialMan-agementServiceBudgetDivision. 1986.
. Utilization of Rural Health Services. Doc_Jmentpreparedforthe Re-gionalSeminaronthe Use ofRuralHealthServices.Sponsoredby theAsianDevelopmentBankand the East-WestCenter. (January20-26, 1986).
.100 Daysin San Lazaro(The Ministryof Healththe Underthe Gov-emme'ntofPresidentCorazonAquino).
NationalEconomicfor InternationalHealth.TheCooperativeLeagueof the U.S.A.,The Group Health Associationof America, Inc. Alternative Health DeliverySystems: Can TheyServe the Public interest in3rd World Settings?Washing-ton, D.C. (August1984).
Navarro, Vicente. =ThePublirJPdvateMix in the Funding and Deliveryof HealthServices:AnInternationalSurvey.AmericanJoumal of Public Health. V01.75,No. 11 pp. 1318-1320. (November1985).
NationalCensusand StatisticsOffice.PhBppino Yearbook 1985. Manila:NCSO,(August1985).
NationalEconomicand DevelopmentAuthorily.Social Devalopment: ThePhi_neApproach. (December1980).

140 Ma. Concepcion P. A/filer
• Social Development in the Phil_pines, 1970.1980, 1982.
• RegionaIDevelopment: Issues: Strategies on Health. PhilippineDe-velopmentPlanningStudiesSeriesNo. 6. 1982.
• 1982Economic and Social Indicators.NEDA StatisticalCoordinationOffice.1983
o1984 Economic and Social Indicators. 1985,
"ProposedProgramfor an ImprovedHealthCare DeliverySystem."NEDA: PolicyCoordinationStaff.(August1985),(manuscript).
Newhouse,Joseph.TheEconomicsof Medical Care:A PolicyPerspective.Addison-WesleyPublishingCo., 1978
Osteria,TrinidadS. andSiason0IdaM.Alternative Strategies for Financing PrimaryHealth Care:Lessons from Six Case Studies. U.P. inthe Visayas. 1985.
Perlas, Antonio."CommunityHealth Financing."Lecturedeliveredat the "Seminaron PreventiveMedicine," LectureSeries No. 4 (Economicsof Health Care)conductedbytheTask ForcePeople'sHealth,QuezonCity, (April16, 1986).
PhilippineCouncilfor HealthResearchandDevelopment,NSTA andUnitedStatesAgencyfor InternationalDevelopment."Proceedingsof the Seminar-Work-shoponHealthCare FinancingSchemes,"TagaytayCity(May 28-30, 1985).
Rapoport,John, RobertRobertsonand BruceStuart. Understanding Health Eco-nomics. Aspen SystemsCorporation,1982.
Ramirez-Lariosa,Theresita."HouseholdHealthSeekingBehaviorandExpenditurePatternsfor Primary Health Care in Cabegan, Isabela."Preparedfor theUnitedStatesAgencyfor InternationalDevelopmentundercontractNo, 492-0249-C-1063-00, (July1982).
Robertson,RobertL.Review of Llterature on Costsof Health Services inDevelopingCountries. PHN Technical Note 85-21. Population, Health and NutritionDepartment.World Bank(November 1982).
Russell,SharonStantonandJackReynolds.OperationsResearch Issues: Commu-nity Financing. Maryland:Primary HealthCare OperationsCenter.
Schwartz,J. Brad,John Akin, at. al. "Analysisof the Effectsof the InfrastructureDevelopmentand MedicalServiceChangesonthe Patternsof Health CareUse inthe BicolRegionof the Philippines."Submittedto SigmaOne Corpo-rationand USAID in partial fulfillmentof USAID Contract OTR-0082-C-00-3353-00 (July1985).

Health Financing 141
Stinson,Wayne. P#mary Health Care Issues: Community Financing. Washington,D,C.: AmericanPublicHealthAssociation,1982.
Startz, Ralph, MarvinLiebermanand Alice Sardelleds• Critical Issues in HealthPolicy. LexingtonBooks,1981.
Tamesis,JesusV. "UnorthodoxIdeasonHealthCare andItsFinancing."PhilippineBudget Management. Vol. 18 No. 4 pp. 12-15 (December1980).
U.S, Agency for InternationalDevelopmentOffice of Population,Health, andNutrition*Philippines:Primary Health Care Financing Project492-0371."ProjectPaper (July1983).
WorldBank.Health Issues and Policies in the Developing Countries.StaffWorkingPaper No. 412. (August1980).
• Health Sector Policy Paper. Washington,D.C.: WorldBank(Febru-an/1980).
. Population, Health and Nutrition in the Philippines:A Sector Review.ReportNo. 4650-PH. (January13, 1984)•
WHO StudyGroup.Financing of Health Services.Geneva:WorldHealthOrganiza-tion,TechnicalReport Series625. 1978.
Zschock, Dieter K. Health Care Financing in Developing Countries.Washington,D,C. AmericanPublic Health AssociationInternationalHealth Programs,MonographSeriesNo. 1. 1979.
• =HealthCare FinancinginCentralAmericaandthe AndeanRegion'.Latin American Research Review. Vol. XV No. 3 pp. 146-168. 1980.