Embed Size (px)
Citation preview

Great Title for the Slide
SUSTAINABILITY OF OFF-PATENT DRUG POLICIES IN THE QUEST FOR VALUE
Diana BRIXNER, PhD, RPh, Professor & Executive Director, Department of Pharmacotherapy, University of Utah, Salt Lake City, UT, USA;
Nikolaos MANIADAKIS, MSc, PhD, Professor, Department of Health Services Organization and Management, National School of Public Health, Athens, Greece;
Jie SHEN, PhD, Head of Market Access, Abbott, Basel, Switzerland;
Zoltán KALÓ, MD, MSc, PhD, Associate Professor, ELTE University;CEO, Syreon Research Institute, Budapest, Hungary
Workshop 30:
Great Title for the SlideIssue Panel Agenda
• Is Health Technology Assessment Obsolete once a Drug goes Off-Patent?– Cost becomes main driver
• There are Value Issues (cost vs. outcome) – Drug shortages
– Generic manufacturing quality
– Bioequivalence
– Variance in clinical outcomes
– Adherence
• Should evidence based decision making persist in the off-patent space?
6. Nov. 2013 16th European ISPOR Congress, Dublin 2

Great Title for the SlideFaculty
Introduction of Faculty, Agenda D. Brixner
Value considerations for off-patent products D. Brixner
International policies applied in the off-patent arena in context to the concept of health care efficiency
N. Maniadakis
Value versus lowest price Z. Kaló
Perspective on value creation in the off-patent drug industry J. Shen
Discussion D. Brixner
6. Nov. 2013 16th European ISPOR Congress, Dublin 3
Great Title for the SlideAgenda
• Introduction of Faculty, Agenda D. Brixner
• Value considerations for off-patent products D. Brixner
• International policies applied in the off-patent arena in context to the concept of health care efficiency N. Maniadakis
• The impact of generics policy on health care at the example of Hungary Z. Kaló
• Perspective on value creation in the off-patent drug industry J. Shen
• Discussion D. Brixner
6. Nov. 2013 16th European ISPOR Congress, Dublin 4
Diana Brixner, PhD, RPhProfessor and Chair, Department of Pharmacotherapy
Executive Director Outcomes Research CenterCollege of Pharmacy
Director of OutcomesPersonalized Health Care Program. University of Utah
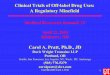
Great Title for the SlideShould value-based decisions be made for all products?
» Including all off‐patent products, it can be assumed, that over 80% of patients are treated with off‐patent drugs (Originators, Branded Generics, INN Generics)
» After patent loss, decisions are increasingly based on price
Unbranded Generics
Branded Generics
Off‐patent originators
On‐patent
Total Prescriptions
Off‐Patent Drugs
Value‐Based Decisions
Price‐Based Decisions
INN = International Non‐proprietary Name
6. Nov. 2013 16th European ISPOR Congress, Dublin 5
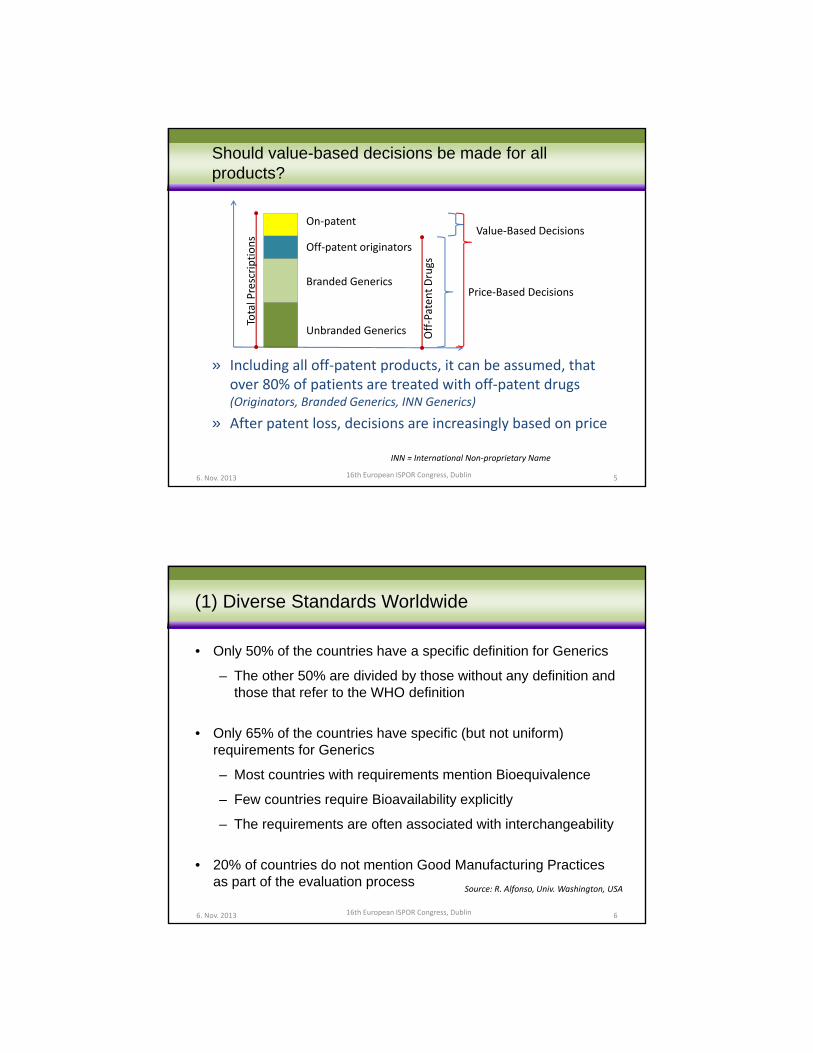
Great Title for the Slide(1) Diverse Standards Worldwide
• Only 50% of the countries have a specific definition for Generics
– The other 50% are divided by those without any definition and those that refer to the WHO definition
• Only 65% of the countries have specific (but not uniform) requirements for Generics
– Most countries with requirements mention Bioequivalence
– Few countries require Bioavailability explicitly
– The requirements are often associated with interchangeability
• 20% of countries do not mention Good Manufacturing Practices as part of the evaluation process
Source: R. Alfonso, Univ. Washington, USA
6. Nov. 2013 16th European ISPOR Congress, Dublin 6

Great Title for the Slide(2) A Systematic Review
6. Nov. 2013 16th European ISPOR Congress, Dublin
Imke Schall, Bakk, Diana Brixner, RPh, PhD
Kim Saverno, PhD, RPh, Martina Mitrovic, Mag., Agnes Luzak, MPH, Holger Gothe, MD, Uwe Siebert, MD, MPH, MSc, ScD 1,
Institute of Public Health, Medical Decision Making and Health Technology Assessment; Department of Public Health and Health Technology Assessment,
UMIT – Univ. Health Sciences, Medical Informatics and Technology, Eduard Wallnoefer Center I, A‐6060 Hall i.T., Austria
The Impact of Generic Substitution on Health Outcomes and Costs
7
Poster PHP 28
Great Title for the SlideResults
• 40 studies across 10 therapeutic areas. – 13 of the studies with narrow therapeutic index drugs (NTI)
– 121 outcome comparisons were included in the review.
• 66% of the outcome comparisons reported similar clinical outcomes for generic and original brand drugs
• 64% suggested that brand products had lower costs compared to generic substitution.
• Thus the first hypothesis of similar clinical outcomes was largely supported, however the second hypothesis that generic drugs save money was largely rejected.
6. Nov. 2013 16th European ISPOR Congress, Dublin 8

Great Title for the Slide
• Switching among generics, and or brands, repeatedly leads to increase bleeding events in Afib patients
• In epilepsy such switching between generics lead to increased health care costs due to more hospitalizations
• Increased generic market share is correlated with an increase in side effects
• 42% of nurses surveyed reported an increase for in-patient dispensing mistakes due to generic substitution
• For bisphosphonates increased generic availability is correlated to a decrease in adherence
• Increase generic use causes patient confusion and is linked to cecreased willingness and ability to take medicines as described.
Examples of Key Outcomes
6. Nov. 2013 16th European ISPOR Congress, Dublin 9
Great Title for the Slide
1. S. R Ghate, J. E. Biskupiak, X. e, M. Hagan, W. J. Kwong, E. S. Fox, D. I. Brixner. 2011. “Hemorrhagic and Thrombotic Events Associated with Generic Substitution of Warfarin in Patients with Atrial Fibrillation: A Retrospective Analysis.” Annals of Pharmacotherapy 45 (June 10): 701–712.
2. MS Duh, F Andermann, PE Paradis, J Weiner, R Manjunath, PY Crémieux. 2007. “The Economic Consequences of Generic Substitution for Antiepileptic Drugs in a Public Payer Setting: The Case of Lamotrigine.” Disease Management 10 (4): 216–25.
3. MS Duh, KE Cahill, PE Paradis, PY Cremieux, PE Greenberg. 2009. “The EconomicImplications of Generic Substitution of Antiepileptic Drugs: a Review of Recent Evidence.” Expert Opinion on Pharmacotherapy 10 (14) (October): 2317–2328.
4. Hellström, Jörgen, and Niklas Rudholm. 2009. “Uncertainty in the Generic Versus Brand Name Prescription Decision.” Empirical Economics 38 (3) (March 6): 503–521
5. H Håkonsen, H Skjønhaug Hopen, L Abelsen, B Ek, and EL Toverud. 2010. “GenericSubstitution: a Potential Risk Factor for Medication Errors in Hospitals.” Advances in Therapy27 (2) (February): 118–126.
6. Ström, O, and E Landfeldt. 2011. “The Association Between Automatic Generic Substitution and Treatment Persistence with Oral Bisphosphonates.” Osteoporosis International
7. Håkonsen, Helle, and Else-Lydia Toverud. 2012. “A Review of Patient Perspectives on Generics Substitution: What Are the Challenges for Optimal Drug Use.” Generics andBiosimilars Initiative Journal 1 (1) (February 15): 28–32. doi:10.5639/gabij.2012.0101.008.
References
6. Nov. 2013 16th European ISPOR Congress, Dublin 10

Great Title for the SlideConclusions• The economic savings of generic drug substitution may
be overstated.
• Evidence shows that the anticipated savings may not be realized in real world settings
• Due to the heterogeneity of the results further research is needed.
• Based on these results Health Technology Assessment of generic substitution is warranted and should be considered when making broad-based policy decisions
6. Nov. 2013 16th European ISPOR Congress, Dublin 11
Great Title for the Slide(3) Drug shortages. It is about patients getting their therapy.
16th European ISPOR Congress, Dublin6. Nov. 2013 12

Great Title for the Slide(3) The majority of drug shortages are driven by cost containment measures
Lack of profitability 37%
(Parallel) Export 20%
Restrictive reference pricing 17%
Tender side effect 17%
Dependency from 1 or few manufacturers 17%
Manufacturer capacity problem 15%
Upfront payments / delayed payments 15%
Regulatory insufficiencies 15%
Increasing demand 12%
Production / Quality Issue () 12%
Political / economic issues 12%
Cheapest product substitution policy 10%
Distribution inefficiencies 10%
World‐wide supply chain issues 10%
Lack/Reduction of local manufacturing 7%
Procurement inefficiencies 5%
Lack of API 2%
Corruption 0%
(N = 41)
Holtorf, et al. 2012. ViH 15 (7)
6. Nov. 2013 16th European ISPOR Congress, Dublin 13
Great Title for the Slide(3) Pricing regulations and drug shortages
• “A more comprehensive approach to drug shortages, including better incentives for manufacturers, is necessary to prevent drug shortages in the USA”.(Woodcock and Wosinska 2013)
• “More value based approaches to purchasing as an alternative to exclusively price driven mechanisms”(E R Fox and Tyler 2013)
• [Same observations] supported by an economic analysis of the causes for drug shortages.(Haninger, Jessup, and Koehler 2011)
6. Nov. 2013 16th European ISPOR Congress, Dublin 14

Great Title for the Slide
16th European ISPOR Congress, Dublin
banana: Same generic name – but not always the same experience ...
Source: AP Holtorf, Sao Paolo, Brazil, 2013
6. Nov. 2013 15
Great Title for the SlideDifferent Perspectives on Off-Patent Drugs
6. Nov. 2013 16th European ISPOR Congress, Dublin
Patients
Regulators
The payer
The industry• Generic• Brands
Providers
Off‐Patent Drug
Policies
16

Great Title for the SlideAgenda
• Introduction of Faculty, Agenda D. Brixner
• Value considerations for off-patent products D. Brixner
• Health care efficiency and regulation policies N. Maniadakis
6. Nov. 2013 16th European ISPOR Congress, Dublin 17
Prof. Nikolaos Maniadakis BSc, MSc, PhD, FESC
Associate Dean and Department Director
Health Services Organisation & Management
National School of Public Health
Greece
Great Title for the SlideAnalysis of pharmaceutical policies, regulation and efficiency
• Pricing of on/off patent and generic products
• Indirect price and expenditure controls
• Breadth, scope and depth of cover
• Pharmacy dispensing policies
• Pharmaceutical demand and prescription control
• To map and describe pharmaceutical systems and main policies
• To classify pharmaceutical policies based on regulation
• To cluster systems based on pharmaceutical policies
• To analyse patterns and pharmaceutical policy trends
• To investigate any relation between policies & efficiency
POLICY DOMAINS AIMS OF RESEARCH
6. Nov. 2013 16th European ISPOR Congress, Dublin 18
Posters: PHP199 & PHP201; Pres.: PR2Maniadakis et al. 16th Europ. ISPOR Congr, Dublin 2013

Great Title for the SlideCountries reviewed (sample: 5,6 billion population, 73.7 trillion $ GDP, 809 Billion $ drug expenditure)
Europe Americas Middle East &
Africa
Asia & Pacific
Austria Malta Argentina UAE Australia
Belgium Netherlands Brazil Saudi Arabia Bangladesh
Bulgaria Poland Chile Iran China
Cyprus Portugal Colombia Egypt India
Czech Republic Romania Mexico Ethiopia Indonesia
Denmark Slovakia Venezuela Nigeria Iran
Estonia Slovenia Canada South Africa Japan
Finland Spain USA New Zealand
France Sweden Pakistan
Germany Unit. Kingdom Philippines
Greece Norway South Korea
Hungary Russia Thailand
Ireland Switzerland Vietnam
Italy Turkey
Latvia Ukraine
Lithuania Luxembourg
19
Posters: PHP199 & PHP201; Pres.: PR2Maniadakis et al. 16th Europ. ISPOR Congr, Dublin 2013
6. Nov. 2013
Great Title for the SlidePrevailing pricing policies worldwide
6. Nov. 2013 16th European ISPOR Congress, Dublin 20
Pricing on‐patent
pharmaceuticals
Pricing off‐patent
pharmaceuticals
Pricing generics
pharmaceuticals
Free pricing and little controls Free pricing and little controls Free pricing and little controls
Internal reference pricing Internal reference pricing Internal reference pricing
External reference pricing External reference pricing External reference pricing
State controls wo negotiation State controls wo negotiation State controls wo negotiation
Cost plus pricing Cost plus pricing Cost plus pricing
Price setting through tenders Price setting through tenders Price setting through tenders
Value based pricing (w/wo HTA) Cost plus pricing State decisions w/o
negotiation
Direct negotiations (w/wo HTA) Dynamic pricing Dynamic pricing
Conditional pricing Price reduction at patent
expiration
Price reduction at patent
expiration
Posters: PHP199 & PHP201; Pres.: PR2Maniadakis et al. 16th Europ. ISPOR Congr, Dublin 2013

Great Title for the SlidePharmaceutical policies and regulation: pharmaceutical dispensing
16th European ISPOR Congress, Dublin
Polices based on literature review and expert assessment
6. Nov. 2013 21
1.01.5
3.0 3.0
4.04.5
5.0 5.0
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Mean
LCI
UCI
Median
22
% o
f GD
P S
pend
on
all
drug
s
Degree of regulation (off-patent drug pricing)
Total pharma expenditure as % GDP and off‐patent regulation
Public pharma expenditure as % GDP and off‐patent regulation
% o
f GD
P p
ublic
S
pend
on
drug
s
6. Nov. 2013 16th European ISPOR Congress, Dublin

perc
enta
ge o
f GD
P
Spe
nd o
n dr
ugs
Degree of regulation (dispensing)
23
Total pharma expenditure as % GDP and dispensing regulation
perc
enta
ge o
f GD
P
Spe
nd o
n dr
ugs
Public pharma expenditure as % GDP and dispensing regulation
Degree of regulation (dispensing)
perc
enta
ge o
f GD
P
Spe
nd o
n dr
ugs
Degree of regulation (off-patent drug pricing)
Total pharma expenditure as % GDP and off‐patent regulation
Per
cent
age
of g
ener
ic p
enet
ratio
n
Degree of regulation (generic drug pricing)
6. Nov. 2013 16th European ISPOR Congress, Dublin 24
Generic % volume and regulation of generic prices
Generic % volume and regulation of dispensing
Degree of regulation (dispensing)

Degree of demand control regulation
6. Nov. 2013 16th European ISPOR Congress, Dublin 25
Total pharma expenditure as % GDP and demand control policies
Pub
lic d
rug
Spe
nd
(% o
f G
DP
)
Public pharma expenditure as % GDP and demand control policies
Tota
l dru
g S
pend
(%
of
GD
P)
Gx Vol % and demand control policies
% G
x of
tota
l ph
arm
a vo
lum
e
Degree of demand control regulation
26
Degree of overall regulation
6. Nov. 2013 16th European ISPOR Congress, Dublin
Public pharma expenditure as % GDP and overall regulation
Pub
lic d
rug
Spe
nd
(% o
f G
DP
)
Tota
l dru
g S
pend
(%
of
GD
P)
Total pharma expenditure as % GDP and overall regulation
Gx Vol % and overall regulation
% G
x of
tot
al
phar
ma
volu
me

Degree of health efficiency
6. Nov. 2013 16th European ISPOR Congress, Dublin 27
% G
x of
tota
l ph
arm
a vo
lum
e
Gx Vol % and healthcare efficiency scores
Degree of health efficiency D
egre
e of
ove
rall
regu
latio
n
Overall degree of regulation and healthcare efficiency scores
Great Title for the SlideConclusions
• There are many different policies applied to regulate the domains ofpharmaceutical markets
• Different policies are characterised by different degrees of regulationand countries use mixtures
• A common assumption is that more regulation leads to lower drugexpenditure and greater efficiency
• Early evidence suggests that heavily regulated policies do notnecessarily lead to efficiency gains, but instead often they may haveopposite effects
• Demand control may the most efficient measure to increase genericuse and to decrease expenditure
• By contrast, our findings do not support the use of pricing as aneffective means to control expenditure
6. Nov. 2013 16th European ISPOR Congress, Dublin 28

Great Title for the SlideAgenda
• Introduction of Faculty, Agenda D. Brixner
• Value considerations for off-patent products D. Brixner
• International policies applied in the off-patent arena in context to the concept of health care efficiency N. Maniadakis
• Value versus lowest price Z. Kaló
• Perspective on value creation in the off-patent drug industry J. Shen
• Discussion D. Brixner
6. Nov. 2013 16th European ISPOR Congress, Dublin 29
Jie Shen, M.B.AHead of Market Access
Abbott Established Pharmaceuticals Division
Great Title for the SlideConsider 4 Domain, Multiple Criteria in Pricing, Reimbursement, Tender Policies of Off-Patent Medicines
Domain: Health Care System
• Sustainability (Does the Policy account for majority patients are treated by Gx?)
• Efficiency (Does the policy increase/ decrease overall health care system efficiency?)
Domain: Outcome
• Clinical Outcomes (variability in clinical outcomes)
• Patient Adherence
• Economic Outcomes (total treatment costs)
Domain: Products
• Bio‐equivalence
• Indications
• Formulations
• Excipients & Process technology
Domain: Manufacturer
• GMP (No/ WHO‐certified/ EMA‐certified)
• Supply reliability
• Value‐Added Partnership

Great Title for the SlideProof of bio-equivalence
6. Nov. 2013 16th European ISPOR Congress, Dublin
• FDA: consider a product as “bioequivalent” if the 90% CI of the relative mean Cmax, AUC of the test (generic formulation) to reference (innovator brand formulation) within 80.00% to 125.00% in the fasting state
• EMA:
– 2000: consider a product “bioequivalent” if the 90% CI of the ratios for AUC and Cmaxbetween the two preparations lie in the range 80.00 – 125.00%
– 2010: highlight the need for a more restrictive acceptance interval 90.00 –111.00% for NTI drugs
– 2013: in the process of developing product-specific guidance on the demonstration of bioequivalence, aiming at a transparent, predictable and scientifically robust framework in the interests of all stakeholders (1st set guidance at CHMP, Oct, 2013)
Figure 1: Bioequivalence and Non-bioequivalence (modified from FDA, 2007)
• 2 products considered bio-equivalence may still have individual variations
• 2 Gx which are bio-equivalent to the reference product are not necessarily bio-equivalent to each other
31
Great Title for the SlideExample: Dissolution Curve of Hydrochlorothiazide (China)
Three batches of originators Three batches of domestic generics32

Great Title for the SlideDifferences in Excipients and Process Technology
6. Nov. 2013 16th European ISPOR Congress, Dublin
• Excipients may differ, such as salts, esters, ethers, isomers, mixtures of isomers, complexes or derivatives1
– Some inactive ingredients (e.g. lactose, gluten, color) may cause allergic reaction
• Different production process – Coating of a tablet 2
– Physicochemical and clinical stability3
• Different ingredients and manufacturing process may influence product shelf-life4
Reference: 1. EMA & CPMP2010; 2. Borgherini 2003; 3. Genazzani & Pattarino 2008; 4. Ngo & Barnes 2010
33
Great Title for the SlideEffect on Patient Adherence
6. Nov. 2013 16th European ISPOR Congress, Dublin
• Patient adherence is a key driver in managing health outcome and costs
• INN prescribing and Gx substitution may cause insecurity and confusion (changing product shape, size, color, taste, application)
– 1/3 patients among 20 studies report negative experiences (poor adherence, medication errors) under generic switching1
• When used interchangeably, adverse outcomes have been reported
– Poor treatment effects or adverse events as a consequence of substitution2
– In multiple therapies, e.g. antiepileptic drugs3, atrial fibrillation (warfarin)4, depression5, musculoskeletal disorders (alendronate)6; antihypertensives7; calcineurin inhibitors8, levothyroxine9, asthma10
• Decreasing persistence when HCPs and patients are not given the option to chose the most appropriate therapy
Reference: 1. Håkonsen & Toverud 2011; 2. Margolese 2010; 3. Bautisa 2011; Gagne 2010; 4. Ghate 2011; 5. Erikson 2011; 6. Grima 2010; 7. Håkonson 2009; 8. Bartucci 1999; 9. Copeland 1995; 10. Kalo 2012
34

Great Title for the SlideDrug quality management is a comprehensive process across the product life cycle
6. Nov. 2013 16th European ISPOR Congress, Dublin 35
Stage Key Steps
Development
Quality originated in the design
Management of development data
Risk-benefit control
Production
Continuous GMP compliance
Management of abnormal deviation
Management of change control
Recertification and prevention
Distribution
Management of materials tracking
Recall of defective products
Management of product returns
UtilizationAdverse reactions monitoring
Advertising and packaging
Source: RDPAC analysis of key aspects affecting drug quality
Great Title for the SlideExample: Tender listing considers 4-level of GMP standard (Vietnam)
WHO GMP certified
Gen
eric
EU‐GMP certified
Originator Products with a
compound patent issued by one of the following patent offices:
•Austria
•Australia
•Brazil
•Canada
•China
•EU
•Spain
•Finland
•Israel
•Japan
•Korea
•Russia
•Sweden
•US
•Germany
•United Kingdom
Products manufactured at site inspected as per
•EU GMP
•ICH GMP
•Japan GMP
•US‐CGMP
•PIC/S GMP
•Canada GMP
•TGA‐GMP
Other products
36

Great Title for the SlideSupply reliability
6. Nov. 2013 16th European ISPOR Congress, Dublin
• Increasing drug shortages across the globe
• Increased from 34 events in 2000 to 128 events in 2011 alone in the US and Europe 1
• Leading causes (in Europe) are lack of profitability, parallel export, restrictive reference pricing, tender, dependancy on a single or few manufaturers, manufacturer capacity issues
• To ensure patient access to their drugs and delivery to the public system, consider supply reliability as a criteria in public and private sector procurement decisions, e.g.
• Proven and well-established supply chain and distribution systems
• Consistent production processes and supply / demand adaptability
Reference: 1. Holtorf et al 2012, ViH
37
Great Title for the SlideValue-Added PartnershipExample. Disease Outcome Solution
6. Nov. 2013 16th European ISPOR Congress, Dublin
• «save drug costs» or «save healthcare expenditure»?
• «buying drugs» or «buying health outcomes»?
•Risk stratification enabling targeting of high risk/cost patients or geographies
• Behavioral change programs(Cardiovascular disease, diabetes)
•Diagnostic aids to ensure that the right patient gets the right therapy(Pancreatic Exocrine Insufficiency)
•Patient‐focused medication monitoring & management enabling efficient use of budget (Myocardial Infarction)
38

Great Title for the Slide
• Public-private-partnerships between government, non-government and industry stakeholders can jointly help build-up local healthcare infrastructure to improve access to medicine for the population.
• In India, a 2005 partnership by India Space Research Organization (ISRO), Apollo Telemedicine Networking Foundation (ATNF), Development of Humane Action (local NGO) and Philips developed DISHA (Distance Healthcare Advancement) to provide healthcare to low-income rural population where Philips provides a customized tele-clinical van with diagnostic equipment and medical staff; ISRO provides free satellite connectivity; ATNF provides the health services and the NGO provides the linkages to cover 500,000 population.
• In China, a 2006 pilot disease management program with Shanghai CDC and Pfizer to manage hypertension and CV risk factors through community health centers for 1,400 hypertension patients through training disease mgt specialists to educate clinicians, patients, and monitor progress. This project achieved successful results and in 2008 expanded to all Shanghai 49 community health centers of over 13,000 hypertension patients.
• In Vietnam, a 2011 partnership between Vietnam National Institute of Nutrition, Bach Mai Hospital, Hanoi Medical University, Boston University’s Global Health Collaborative and Abbott saw a comprehensive, coordinated approach to strengthen clinical nutrition within hospitals in Vietnam by targeting three critical needs: conducting staff training and integrating clinical nutrition into inpatient hospital care; expanding clinical nutrition education; and conducting and sharing research results on clinical nutrition best practices.
Value-added PartnershipExamples: Public-Private-Partnership
6. Nov. 2013 16th European ISPOR Congress, Dublin 39
Great Title for the Slide
• Off-patent medicines are used for majority of patients. Health Policy on off-patent medicines and their manufacturers are important for the public health system
• Generic medicinal products are not identical. They differ in terms of bio-availability, excipients and process technology
• Policies which mandate INN prescription, Gx substitution may diminish patient adherence, persistence and treatment outcomes, and may not save costs as expected
• Pricing, Reimbursement & tender Policies which target low(est) drug acquisition price may not be the optimum choice for the Health Care System
• Quality, reliable and consistent manufacturing and delivery are critical to ensure patient access, public system supply and effectiveness & safety in health care provision
• Multiple criteria and systematic value-based policy making can introduce right incentives, engage multiple stakeholders including industry to build a more resilient and sustainable health care system
Conclusions
6. Nov. 2013 16th European ISPOR Congress, Dublin 40

Great Title for the SlideAgenda
• Introduction of Faculty, Agenda D. Brixner
• Value considerations for off-patent products D. Brixner
• International policies applied in the off-patent arena in context to the concept of health care efficiency N. Maniadakis
• Value versus lowest price Z. Kaló
• Perspective on value creation in the off-patent drug industry J. Shen
• Discussion D. Brixner
6. Nov. 2013 16th European ISPOR Congress, Dublin 41
Great Title for the SlideAre there Value Issues (cost vs. outcome) with Off-patent Products and what to do against them ?
• Variance in clinical outcomes
• Adherence
• Drug shortages
• Tender ‘side effects’
• GMP certification
• Capacity
• Quality
• Bioequivalence
Product related
Manufac‐turerrelated
Outcomes related
Market related
6. Nov. 2013 16th European ISPOR Congress, Dublin 42

Great Title for the SlideIs Technology Assessment Obsolete once a Drug goes Off-Patent?
Price drivenEvidence driven
6. Nov. 2013 16th European ISPOR Congress, Dublin 43
Great Title for the SlideIf Value Based Decision, which criteria should be considered?
Supply reliability
Total therapy costs
Local investment
Local productionLocal
employment
Environmental responsibility
Bio‐equivalence
Quality control / Assurance
Real life Patient adherence
Real life Patient persistence
Pharmaco‐vigilance
Continuous drug adaptation to
needs
6. Nov. 2013 16th European ISPOR Congress, Dublin 44

Great Title for the SlideIs there a value in freedom of choice?
6. Nov. 2013 16th European ISPOR Congress, Dublin 45
?Sometimes
• Strict regulations withsome exceptions (NTI, anti‐psychotics)
Yes, but ...
• Core regulations (Quality)
• Most appropriate therapy for each patient (EBM)
• Priv. Funding of ‘extras’
Yes
• Market regulates demand• Therapy based on patient and physician peferences (Patient centered)
No
• Strict regulation and equal access for everybody
• Incentives and penalties
• Cost‐containment
EBM = Evidence Based MedicineNTI = Narrow therapeutic window drugs
And if so, where is the right balance between regulation and freedom of choice?
Great Title for the SlideWhat is the Right Level of Regulation to maximize Efficiency?
6. Nov. 2013 16th European ISPOR Congress, Dublin 46
Policy Level High freedom Highly regulated
Licensing No Gx approval needed Full data submission
Pricing Free pricingState decision; regular
price cut
ReimbursedEverything, everybody, 100% covered
Reference products only; co‐pay
Listing No formal process Essential drug list only
PrescribingDoctor decides with patient
INN
Buying Free negotiationBlinded Tender for lowest
price / pack
Substi‐tution None Mandated

Great Title for the SlideThank you
6. Nov. 2013 16th European ISPOR Congress, Dublin 47
Value
Increase Sustainability of Gx Polcies
Evidence based off-patent policies
If you would like to join the network and receive more information, please leave your card or E‐Mail Address or send a mail to us:value@health‐os.com