Embed Size (px)
Citation preview
Sustaining Integration: It’s about more than money
Sustaining Integrated Practice
Getting Paid
Always improvingMovers & Shakers
Leadership Support
LeadershipSupport

Who are we and where are we from?
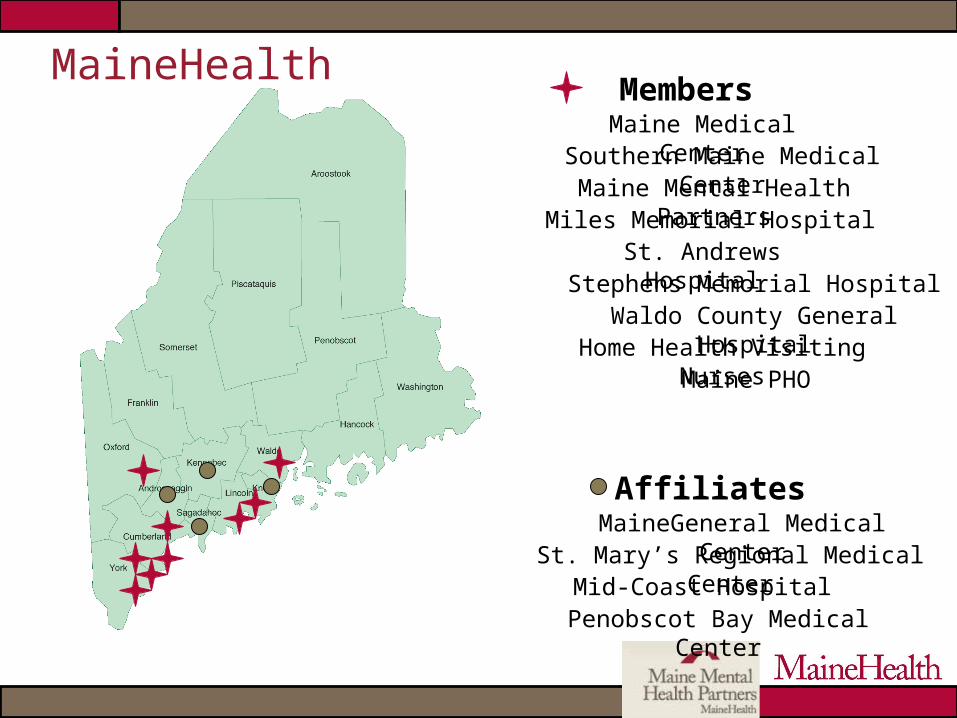
Members
Affiliates
Maine Mental Health PartnersMiles Memorial HospitalSt. Andrews Hospital
Home Health Visiting NursesMaine PHO
Mid-Coast Hospital
MaineGeneral Medical Center
Maine Medical Center
Penobscot Bay Medical Center
Stephens Memorial Hospital
St. Mary’s Regional Medical Center
Waldo County General Hospital
Southern Maine Medical Center
MaineHealth
Objectives:
Participants will be able to: Describe factors that affect the present system of
billing & reimbursement in an integrated setting Identify reimbursement & programmatic elements
that contribute to sustainable integrated programs
Identify strategies to support sustainability of integrated practice
What are you hoping to get out of this session?
Getting started: more than plunking a clinician in the practice and
expecting it to work

Where to start?
“Who was first?”
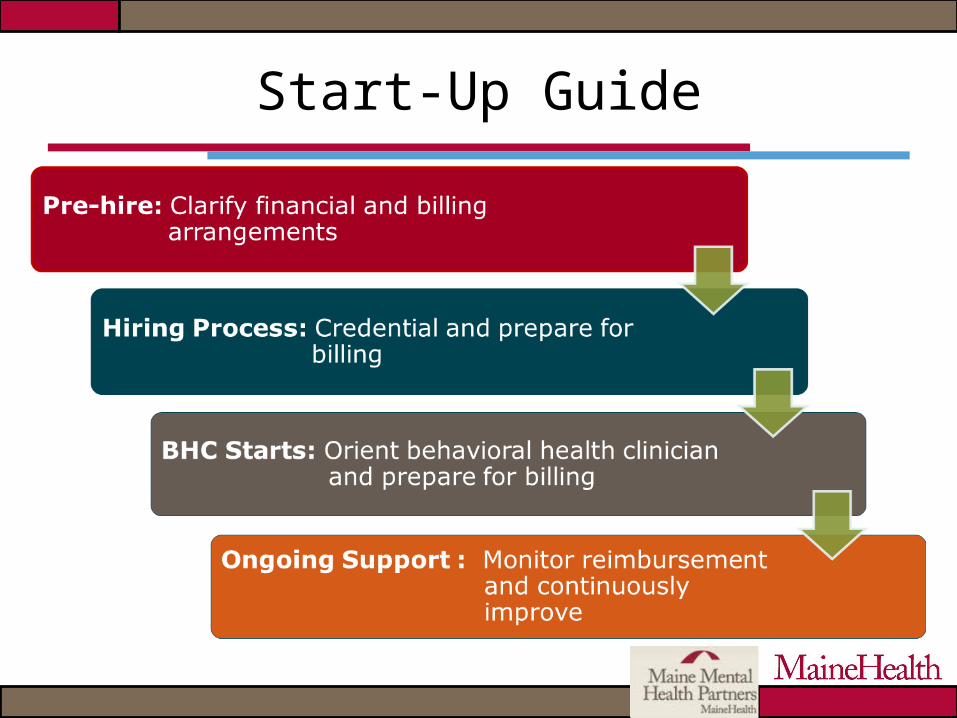
Start-Up Guide
Where are you in the process?

I. Pre-Hire – clarify financial and billing arrangements
Overview of MHI Clarify facility rules Understand services being delivered
including potential new billing practices Discuss service with commercial insurers Develop contracts Train staff on behavioral health billing Identify resource needs and ongoing
review process
II. Hiring process - Credential and prepare for billing
Credentialing – Behavioral vs. Medical? Help BHC understand link between service
and billing codes Clarify supervision requirements Fill out credentialing paperwork
III. Orient Behavioral Health Clinician (BHC) and prepare for billing
Identify staff needed for behavioral health billing
Connect billers/coders with BHC
Track charges, denials Clarify expectations
Medical vs. behavioral Documentation Prior authorization

IV. Ongoing support - Monitor reimbursement and continuously improve
Review practice level data: Services delivered Charges billed Payments received Charges denied and reasons Other problems
Regular meetings – between BHC and billers to problem solve
Track bills to ensure proper coding, documentation and reimbursement
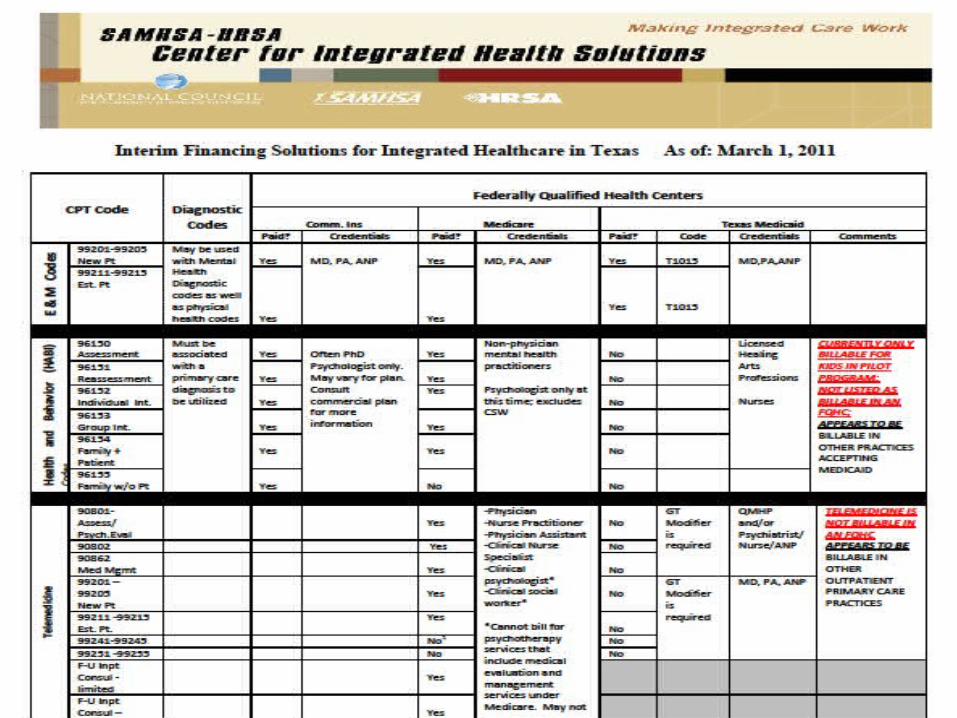
Getting Paid
Questions to ask:
Licenses? Setting (who is billing, where are pts
registered?) Payers and credentialing
Commercial Medicare Medicaid
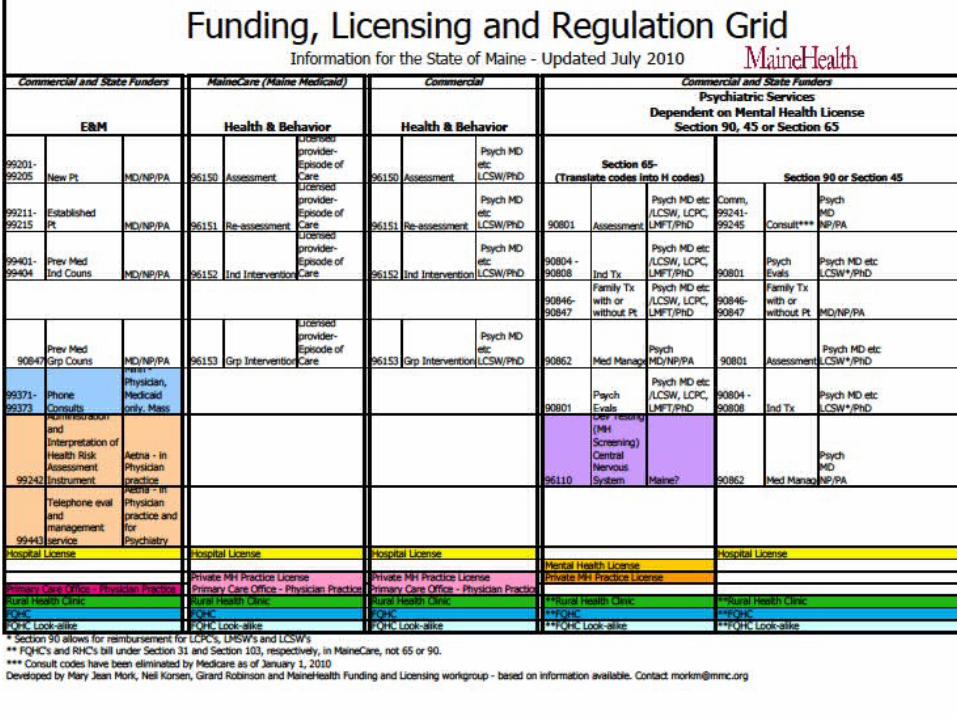
Types of Practice arrangements
Mental Health Agency and Individual Behavioral Health Clinician
Independent (Medical) Practice i.e., “Doctors’ Office”
Provider Based - Hospital Owned Practice Federally Qualified Health Center (FQHC) Rural Health Clinic (RHC)
What is your setting and practice type?
Mental Health Agency Bills
Pros No additional:
credentialing behavioral health
contracting Affordable Allows independent
practitioners to be co-located
May link to community mental health
Cons Intended for persons with
severe/persistent mental illness
Intended for longer term treatment
Limited H&B code billing Extensive paperwork May require that practice
get licensed Separate registration
process Separate record Less reimbursement?

Mental Health Agency challenges – continued
Any time you introduce “separate” functions, you are getting away from integrated and coordinated treatment, or at least making it more difficult.
Any time you require a comprehensive treatment plan, you are getting away from brief focused treatment, the treatment of choice in a primary care setting.
Provider Based or Independent Practice Bills
Pros Intended for patients in
medical settings Same medical record Supports link between
medical and mental health Higher reimbursement? Cost of BHC covered by
medical provider Able to bill H&B codes Medical practice
“ownership” for integrated practice
Cons Requires medical practices to:
Credential Contract Bill commercial insurance
Cost is generally with medical provider
May restrict to LCSW’s or psychologists due to Medicare rules
Requires “order” from provider; documentation of ongoing involvement in treatment
FQHC or RHC Bills
Pros Encounter billing for all
services Cost generally covered by
RHC/FQHC Intended for patients in
medical settings Shared record Link between medical and
mental health Able to bill H&B codes Medical practice “ownership”
for integrated practice Reduced documentation
Cons Must be designated
RHC/FQHC Previously some confusion
around coding Requires medical practices to
take on behavioral health billing Credentialing Contracting Commercial insurer
confusion Cost is generally with medical
provider
Conclusion:
Medical practices should do the billing No need for patients to “register” in a new
organization Allowance for additional revenue through
Health & Behavior codes – only allowed in medical billing
Reduced and more reasonable documentation requirements; better matches practice needs
Both parties need to share investment in the successful outcome

Various payers and various rules
Medicare Medicaid Commercial
Insurers Mental Health vs.
Medical codes Licensing rules
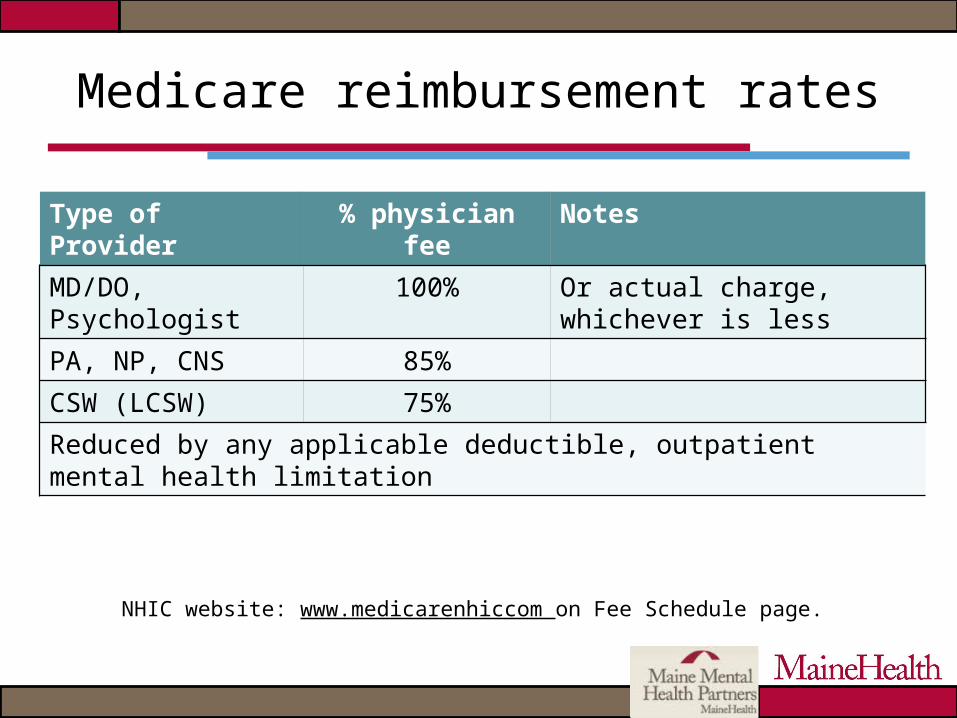
Medicare reimbursement rates
NHIC website: www.medicarenhiccom on Fee Schedule page.
Type of Provider
% physician fee
Notes
MD/DO, Psychologist
100% Or actual charge, whichever is less
PA, NP, CNS 85%
CSW (LCSW) 75%
Reduced by any applicable deductible, outpatient mental health limitation
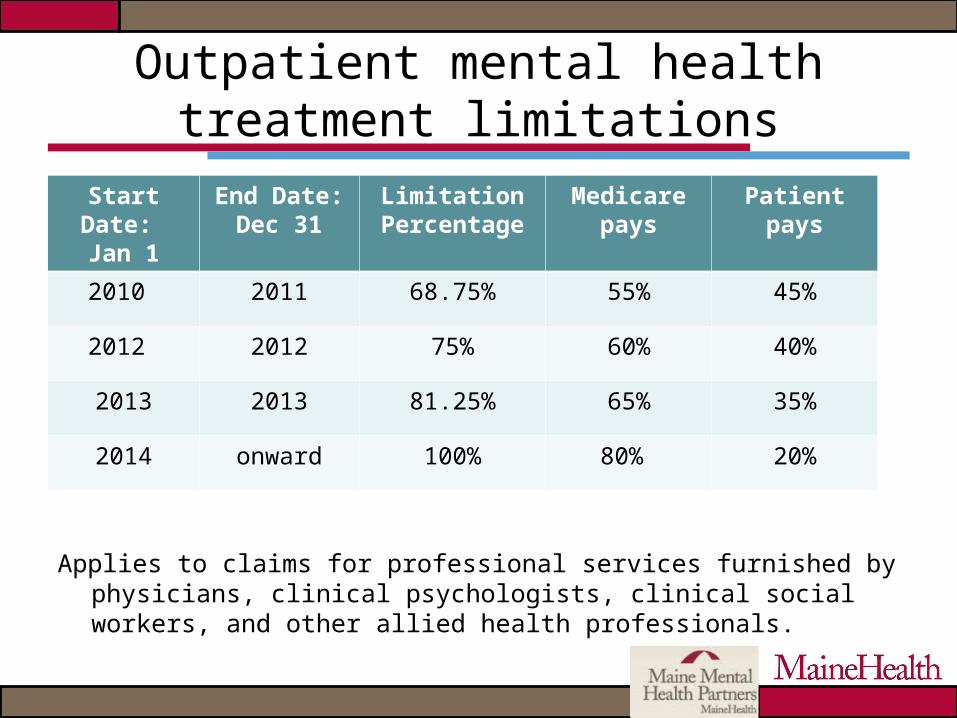
Outpatient mental health treatment limitations
Applies to claims for professional services furnished by physicians, clinical psychologists, clinical social workers, and other allied health professionals.
Start Date: Jan 1
End Date:Dec 31
Limitation Percentage
Medicare pays
Patient pays
2010 2011 68.75% 55% 45%
2012 2012 75% 60% 40%
2013 2013 81.25% 65% 35%
2014 onward 100% 80% 20%
Medicare mental health limitation exceptions
Diagnostic Services – Limitation does not apply to diagnostic tests
and evaluations Include psychiatric or psychological tests and
interpretations, diagnostic consultations, and initial evaluations (90801)
Diagnosis of Alzheimer’s Disease or Related Disorder
Brief Office Visits for Monitoring or Changing Drug Prescriptions

New Mental Health Code Changes for 2013
The old and the very new
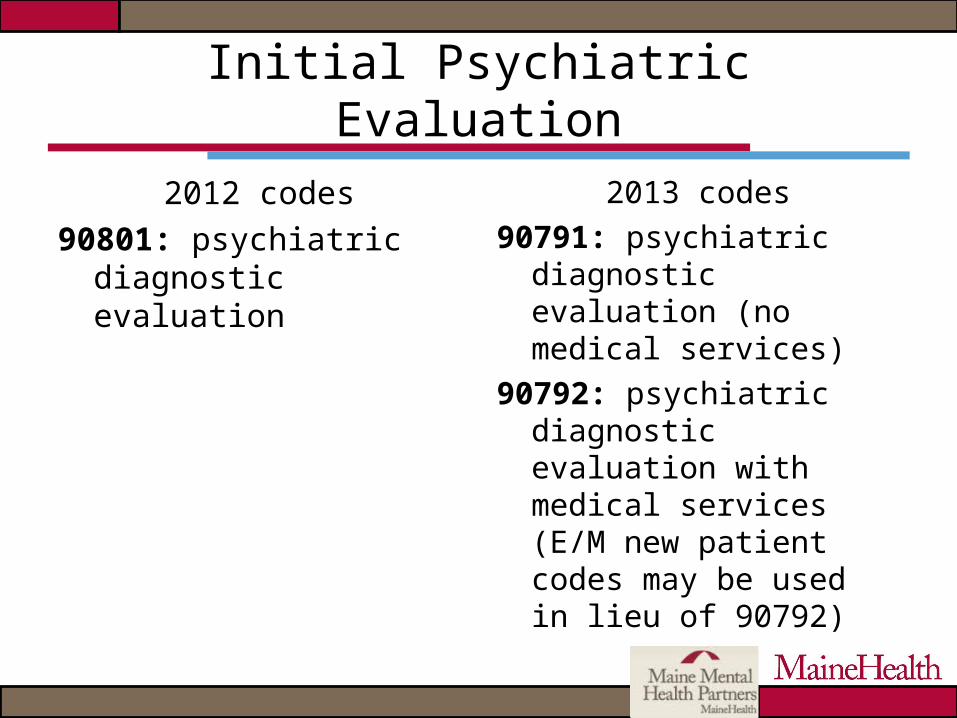
Initial Psychiatric Evaluation
2012 codes90801: psychiatric
diagnostic evaluation
2013 codes90791: psychiatric
diagnostic evaluation (no medical services)
90792: psychiatric diagnostic evaluation with medical services (E/M new patient codes may be used in lieu of 90792)
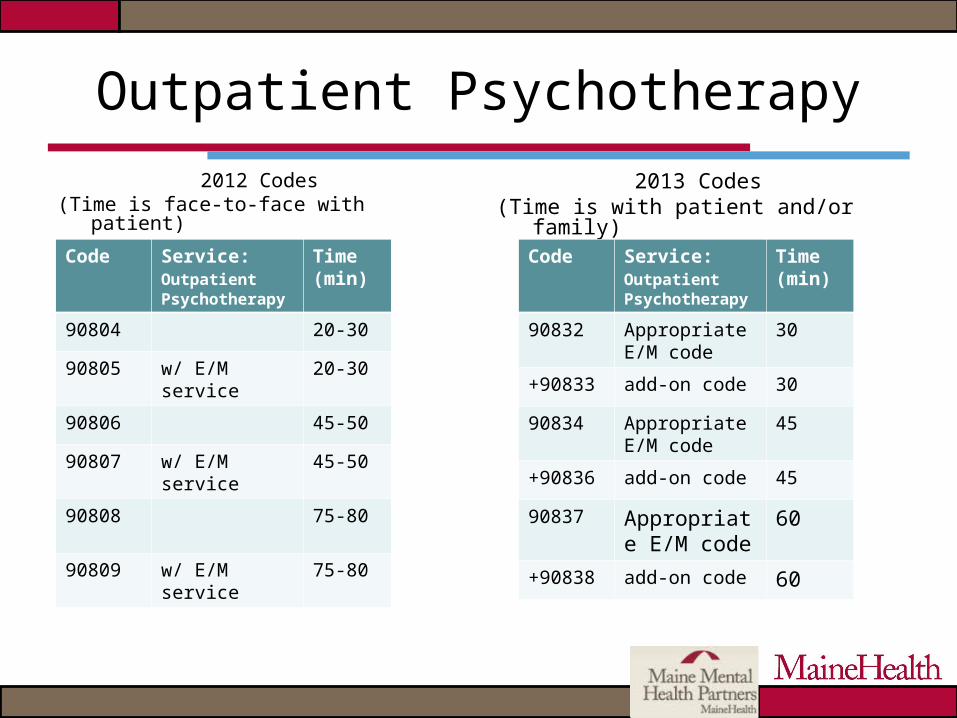
Outpatient Psychotherapy
2012 Codes(Time is face-to-face with patient)
2013 Codes(Time is with patient and/or family)
Code Service: Outpatient Psychotherapy
Time (min)
90804 20-30
90805 w/ E/M service
20-30
90806 45-50
90807 w/ E/M service
45-50
90808 75-80
90809 w/ E/M service
75-80
Code Service: Outpatient Psychotherapy
Time (min)
90832 Appropriate E/M code
30
+90833 add-on code 30
90834 Appropriate E/M code
45
+90836 add-on code 45
90837 Appropriate E/M code
60
+90838 add-on code 60
What do they mean for integrated practice?
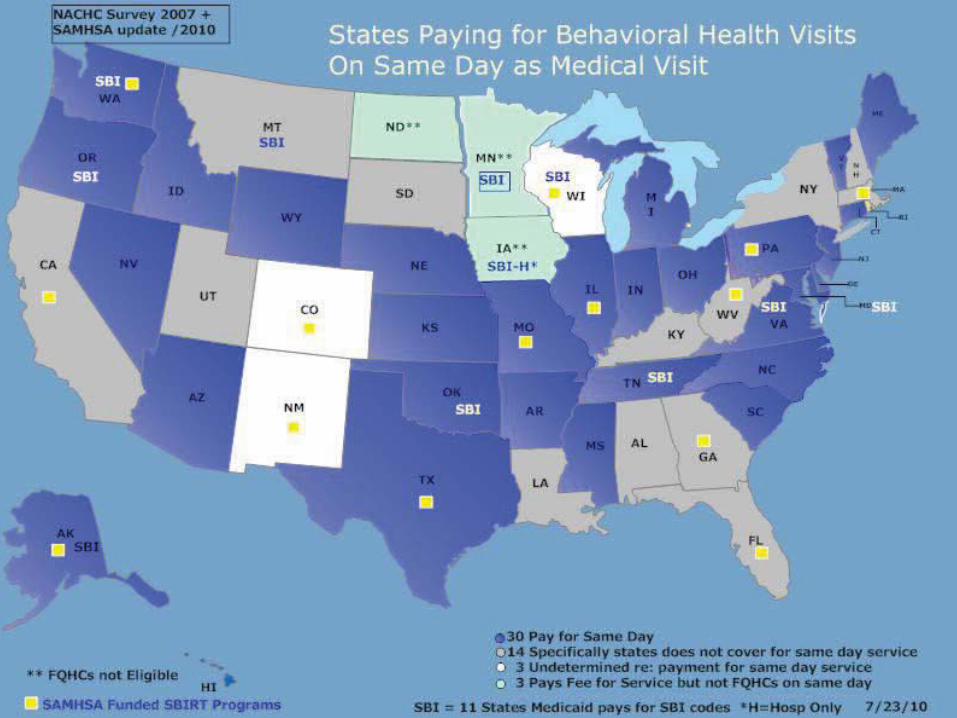
Medicaid
States have flexibility: Covered mental health services Two services (mental health and medical) on
same day Contract with managed care
Billing: Requires diagnosis and procedure code Some states limit procedures, providers and/or
practices that can use these codes
Commercial Insurance
Inconsistencies among various insurers Lack of clarity around covered services Difficulty finding “experts” to answer
specific questions about reimbursement Carve outs
Different systems Different reimbursement streams
Other problems?
Tips: Commercial Insurances
Know expectations of payers Clarify whether in-network medical and/or
behavioral health Reimburse for Health & Behavior codes? Confusion about medical vs. behavioral health
service Be clear at point of service Have documentation support service
Recommendation to bill for service, if service was appropriately delivered, to establish “need” for reimbursement
Some key questions
Payment for 2 encounters in the same day?
Reimbursement for Health & Behavior codes?
Pre-authorization required for mental health visits?
Full assessment required before treatment can begin?
Some additional considerations
“Take this and make it much more difficult than it needs to be.”
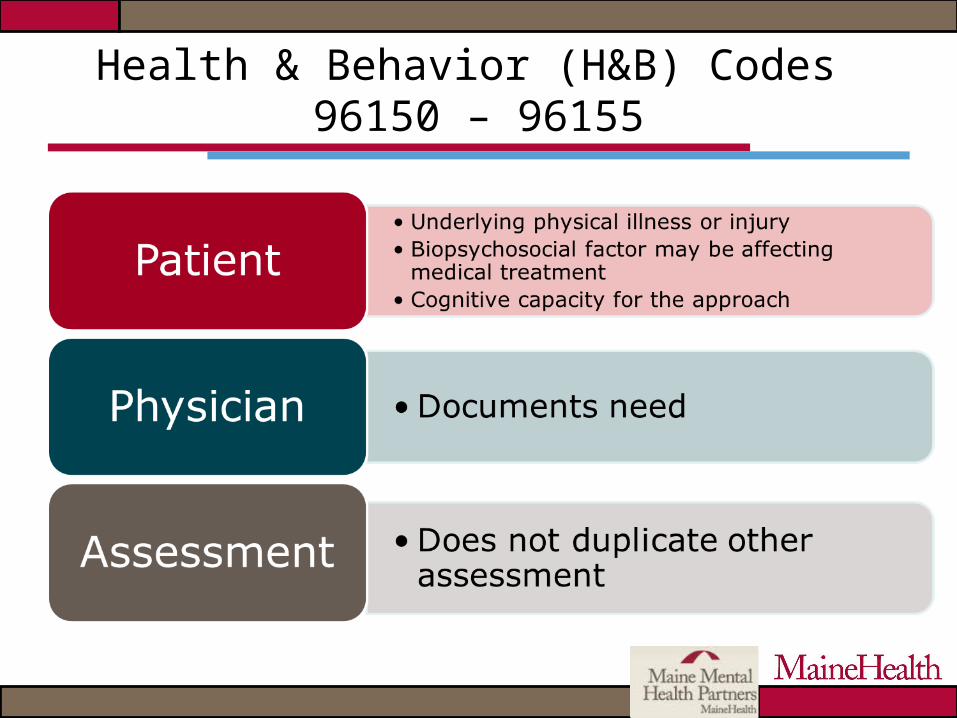
Health & Behavior (H&B) Codes 96150 – 96155
Billing for H&B
Medical diagnosis Medical bill – not mental health Billed by practice with BHC:
Hospital license Primary care office Rural Health Clinic Federally Qualified Health Center

Examples
Adult H&B examples
55 year-old: Hx of AMI, HTN, cholesterol, family history of CVD. High risk - cardiac complications.
35 year-old: diagnosis chronic asthma, HTN, panic attacks. Seen for assessment and follow-up. Original assessment - emotional, social and medical history, including ability to manage problems r/t chronic asthma, hospitalizations & treatments.
Pediatric H&B examples
10 yr-old: Dx - sickle cell anemia. Focus of assessment – biopsychosocial factors r/t pain management and sickle cell disease.
8 yr-old: juvenile rheumatoid arthritis (JRA) for reassessment & treatment. Original referral for nausea, vomiting, panic reactions prior to weekly injections of methotrexate. Assessment: Child - history of JRA, when methotrexate was started, who gives medication, reactions, management of past responses, anxiety & depression questionnaires; Mother - problem-solving skills.
Adolescent H&B examples
16-year-old: fibromyalgia, hx numerous pain episodes, poor school attendance, isolation from peers. Prior to disease: school attendance normal, difficulties with peers not reported. Previous attempts by rheumatology service & pain team: manage pain and facilitate positive school adjustment not successful.
15-year-old: acute lymphoblastic leukemia recently began maintenance phase of treatment. Monthly blood cell counts suggest chemotherapy was not being taken, physician spent considerable time with patient discussing potential consequences. Referral for suspected non-adherence.

Meet Denise

Denise
Experiencing great deal of anxiety after separating from husband and starting new job
Has asthma, not managing it well 2 children at home, now a single parent,
no time for herself
Options
Referral: improve asthma management
Health and Behavior Assessment
Medical referral and diagnosis
Brief, focused assessment and intervention
Referral: reduce anxiety
Mental Health Assessment Medical referral
needed? Mental Health diagnosis “Comprehensive”
assessment and treatment

The Codes
H&B codes 96150: Assessment 96151: Reassessment 96152:
Individual intervention 96153:
Group intervention 96154:
Family intervention
Mental Health Codes 90801:
Initial Assessment 90804, 90806, 90808:
Individual Therapy 90807, 90809:
Ind. Therapy + E/M 90846, 90847:
Family Therapy 90853:
Group Therapy 90862:
Med Management

Insurance Ramifications
H&B codes: Covered by some
insurers, not all Discipline reimbursable
for some, not all Medical benefit: No pre-
auth, no carve-out, no different co-pay
Medical practice bills
Mental Health codes: Covered by most
insurers Generally reimbursable Contract & credentialing
with behavioral health carve-out needed
May eventually need pre-auth
May require larger co-pay
Back to Denise – What do you do?
Depends on: Needs Diagnosis Service delivered
Reimbursement will depend on insurance and discipline of clinician
Can go from H&B to mental health, but not both together
It’s easy to get overwhelmed!
There’s Hope
Many of us: Are successfully working with
integrated practices. Have overcome the challenges of the
complicated system. Have strong support for this work.
We can talk with each other and share what we know.

Measuring Quality
Quality Measures
Quality Measures - Clinician
Building relationships/trust = increased referrals
Training/Measuring core competencies Patient outcomes:
Are patients getting better Are patients engaged in treatment
Quality Measures - Practice
Patient show rate Billing/productivity Access - 3rd next available appt Level of integration– Site Self Assessment
(SSA) www.mehaf.org Screening – yes/no Patient satisfaction
Quality Measures -Program
FTE and type of BHC Process Improvement Provider/staff satisfaction Financial/reimbursement trends/patterns Improved access to community resources

Ongoing Support
Administrative Team Meeting:
the “friendly forum”
Clinicians, provider rep, billers/coders, practice managers, leadership
Data - show rates, referrals, volume: What’s working, not working? Targets?
Payment information: Codes reimbursed/ denied
Communication issues/improvement suggestions: R/t patients, providers, practice
Clinical practice issues: E.g. length of sessions, frequency/duration of treatment
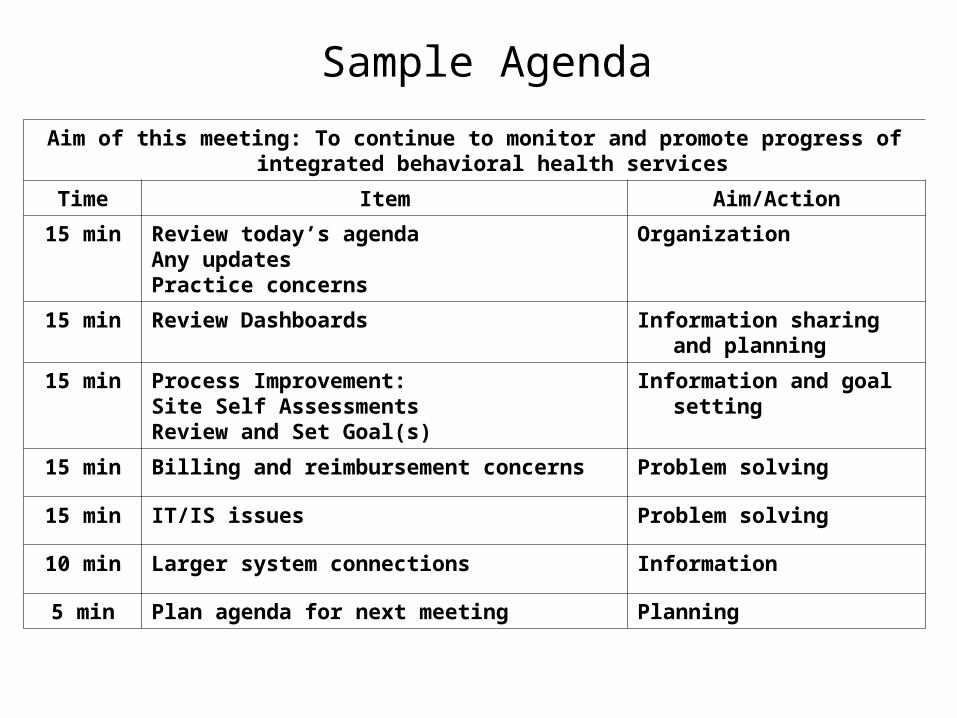
Aim of this meeting: To continue to monitor and promote progress of integrated behavioral health services
Time Item Aim/Action
15 min Review today’s agendaAny updatesPractice concerns
Organization
15 min Review Dashboards Information sharing and planning
15 min Process Improvement:Site Self AssessmentsReview and Set Goal(s)
Information and goal setting
15 min Billing and reimbursement concerns Problem solving
15 min IT/IS issues Problem solving
10 min Larger system connections Information
5 min Plan agenda for next meeting Planning
Sample Agenda
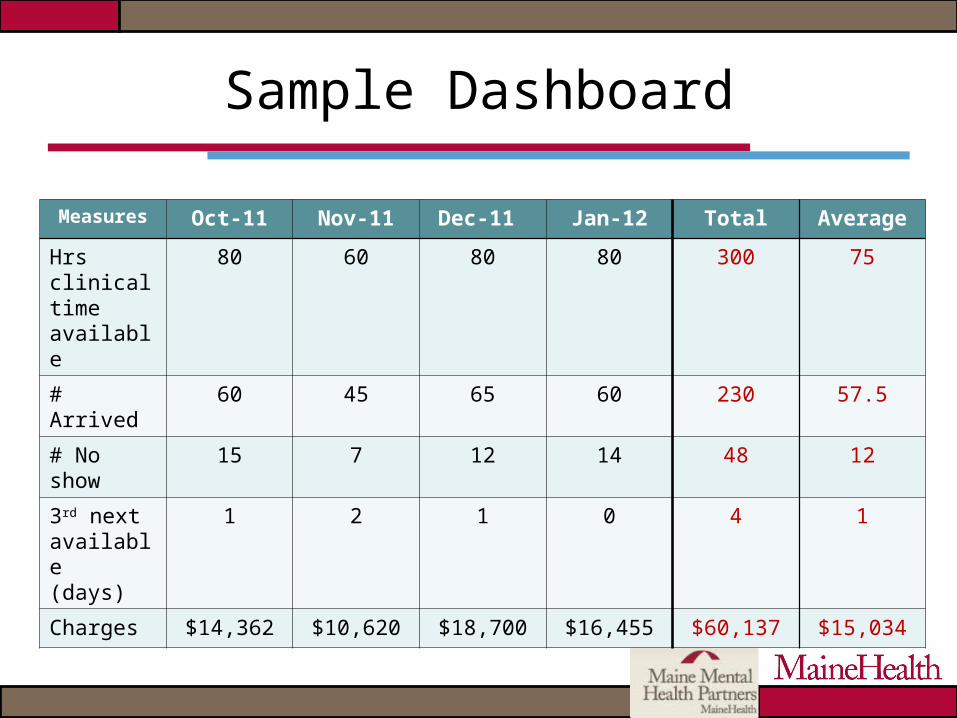
Sample Dashboard
Measures Oct-11 Nov-11 Dec-11 Jan-12 Total Average
Hrs clinical time available
80 60 80 80 300 75
# Arrived 60 45 65 60 230 57.5
# No show
15 7 12 14 48 12
3rd next available(days)
1 2 1 0 4 1
Charges $14,362 $10,620 $18,700 $16,455 $60,137 $15,034
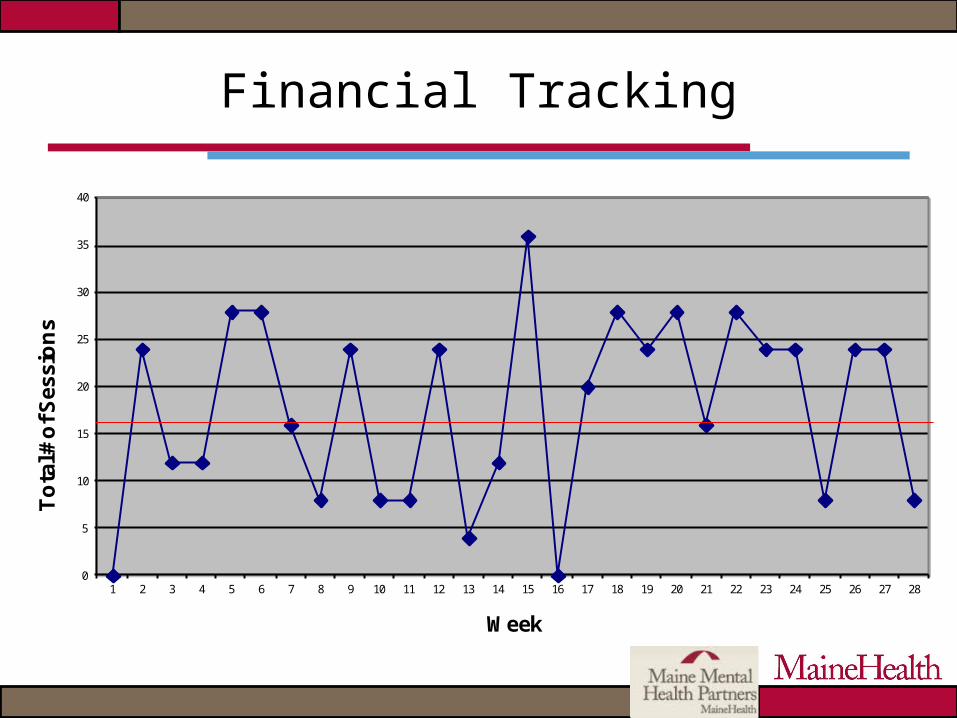
Financial Tracking
0
5
10
15
20
25
30
35
40
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
To
tal #
of S
essi
on
s
Week
Movers and Shakers(what really makes it sustainable)
Willingness to learn new things
Ability to tolerate bumps and address problems
Capacity of team to work together to move this forward
Leadership
Willing to take risk, create vision, support process improvement, and believe in the purpose of the integrated service

We’re optimistic about the future of integrated behavioral health and
primary care
Resources
www.mehaf.org – Maine Health Access Foundation www.thenationalcouncil.org – the National Council for Community
Behavioral Healthcare www.ibhp.org – Integrated Behavioral Health Project www.mainehealth.org/mentalhealthintegration
Medicare Links http://www.cms.gov/Manuals/IOM/list.asp http://www.cms.gov/Transmittals/01_overview.asp Medicare Documentation Guidelines for Evaluation and Managements
Services 95 & 97 http://www.cms.gov/MLNEdWebGuide/25_EMDOC.asp NHIC http://www.medicarenhic.com/
Contacts
Mary Jean Mork, LCSW, [email protected], 207-662-2490Cynthia Cartwright, MT RN MSEd,
[email protected], 207-662-3529Melissa (Missy) Cormier, LCSW
[email protected], 207-661-7128Neil Korsen, MD MS, [email protected]





























