Embed Size (px)
Citation preview
Swallowing rehabilitation in Head and Neck cancer
Marika Muttilainen, SLP
Tampere University Hospital
ELS Workshop Helsinki 10.6.2019
The importance of swallowing
● Dysphagia is strongly associated with psychological distress, poorer quality of life, social isolation, and is a top priority concern for HNC survivors●Dysphagia can lead to malnutrition, dehydration and pulmonary issues
Wilson et al., 2011, Rhoten et al., 2018
11.6.2019
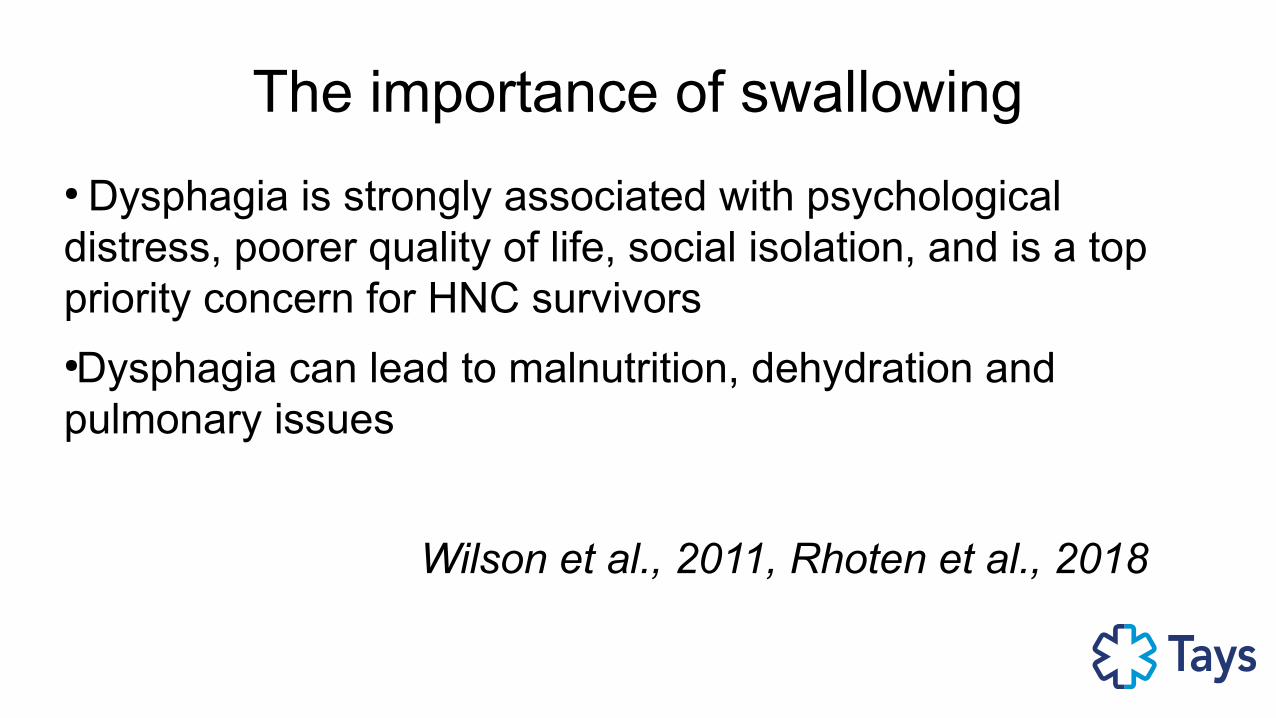
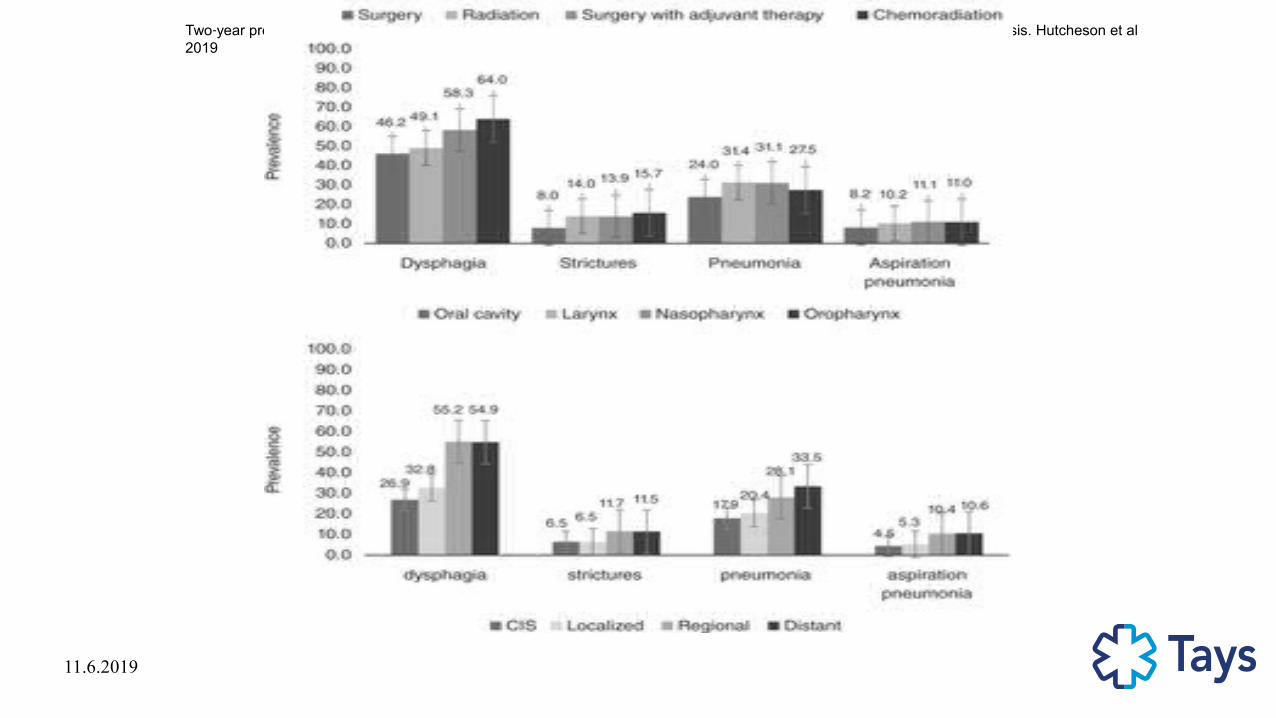
Two year prevalence of dysphagia and related outcomes in head and neck cancer survivors: An updated SEER Medicare analysis. Hutcheson et al ‐ ‐2019
11.6.2019
Two year prevalence of dysphagia and related outcomes in head and neck cancer survivors: An updated SEER Medicare analysis. Hutcheson et al ‐ ‐2019
Guidelines for swallowing rehabilitation●SLPs are core members of MDT
●Head and neck cancer (HNC) guidelines recommend regular multidisciplinary team (MDT) monitoring and early intervention to optimize dysphagia outcomes.
●The pathway provided patients with access to regular supportive care and provided staff opportunities to provide early and ongoing dysphagia monitoring and management.
● However, implementing and sustaining a HNC pathway is complex, requiring significant staff resources, financial investment, and perseverance.
Messing et al., 2018
Guidelines for swallowing rehabilitation in H&N Cancer
”Guidelines that clearly delineate standard of care dysphagia treatment are lacking and services provided to Head and Neck Cancer (HNC) patients
are not always consistent.”
Lawson et al 2017
Guidelines for swallowing rehabilitation in H&N Cancer
● Speech and swallow rehabilitation in head and neck cancer: United Kingdom National Multidisciplinary Guidelines
Clarke et al., 2016
● Framework for Speech-Language Pathology Services in Patients with Oral Cavity and Oropharyngeal Cancers.
Arrese & Hutcheson, 2018.
Dysphagia evaluation
● Patient reported outcome
SSQ, MDADI, EORT QLQ-C30+H&N35, EAT-10
● Objective measures
VFS, FEES, PAS, 100ml water swallowing test, maximal jaw opening
● Feeding status
FOIS, PSS-HN
Arrese et al., 2019
Dysphagia treatment●Rehabilitation
●Compensatory techniques
●Food texture modification
●Alternative feeding devices
●Swallowing-respiratory system training
Dysphagia treatment
Rehabilitation:
“Rehabilitative exercises are those meant to change and improve the swallowing physiology in force, speed or timing, with the goal being to produce a long-term effect /…/
Rehabilitative exercises also involve retraining the neuromuscular systems to bring about neuroplasticity, since pushing any muscular system in an intense and persistent way will bring about changes in neural innervationand patterns of movement. ”
Langmore & Pisegna 2015
Dysphagia treatment
●Rehabilitation:
Swallowing, challenging the system
Swallowing manouvers
Non-swallowing task
- lingual strength
- Shakers exercise
Dysphagia treatment
Compensatory techniques:
●Liquid washes
●Swallowing manouvers
● Chin tuck, head tilt
Dysphagia treatment
Food texture modification:
● Choosing foods that are easy to swallow
● Adding sauce, oil etc to foods
● Modified food consistencies, soft or pureed foods
● Thickening liquids

Dysphagia treatment
Alternative feeding devices:
● Glossectomy spoon
+
● Intraoral prosthetics

Dysphagia treatment
Swallowing-respiratory system training:
● Swallow- breathing cordination
● Expiratory muscle training (EMST)
Head and Neck cancer survivorshipThere are 3 phases of survivorship:
Acute survivorship starts at diagnosis and goes through to the end of initial treatment. Cancer treatment is the focus.
●Extended survivorship starts at the end of initial treatment and goes through the months after. The effects of cancer and treatment are the focus.
●Permanent survivorship is when years have passed since cancer treatment ended. There is less of a chance that the cancer may come back. Long-term effects of cancer and treatment are the focus.
●American Society of Clinical Oncology, 2019
Acute phase
Cancer treatment is the focus.
The goal for SLP: to keep the patient eating.
After surgery returning to oral diet
Eating/swallowing through (chemo)radiation
Proactive or reactive excesizes
Acute phase
After surgery returning to oral diet
Hiararchy:
-saliva management
- introducing oral feeding (safety)
- increase volume-increase complexcicity
Early training can lead to better swallowing function in tongue cancer.
Hsiang et al., 2019
Proactive swallowing excercises●Excercises are introduced before swallowing detoriation, usually first weeks in C/RT
●Goal to minimize disuse of muscles and to help maintain oral nutrition during treatment●Evidence supporting prophylactic swallow exercises for patients with head and neck cancer (HNC) has not been universally demonstrated
Proactive swallowing excercises●lingual strengthening,
● Masako maneuver,
●effortful or supraglottic swallow,
●Mendelson maneuver
● Shaker exercise.
●A TheraBite® Jaw Motion Rehabilitation System™ (www.atosmedical.com) is dispensed and instruction provided when a patient is identified as having reduced incisal opening as measured by the TheraBite® measuring device to be less than 40 mm.
●Expiratory muscle strength training (EMST) devices are utilized as part of the treatment program to improve airway clearance and airway protection in patients who are at risk for penetration and aspiration .
●Patients were encouraged to complete their prescribed exercises twice daily, 6 days a week
John Hopkins Medical Cente Greater Baltimore, Messing et al 2019
Proactive swallowing excercises
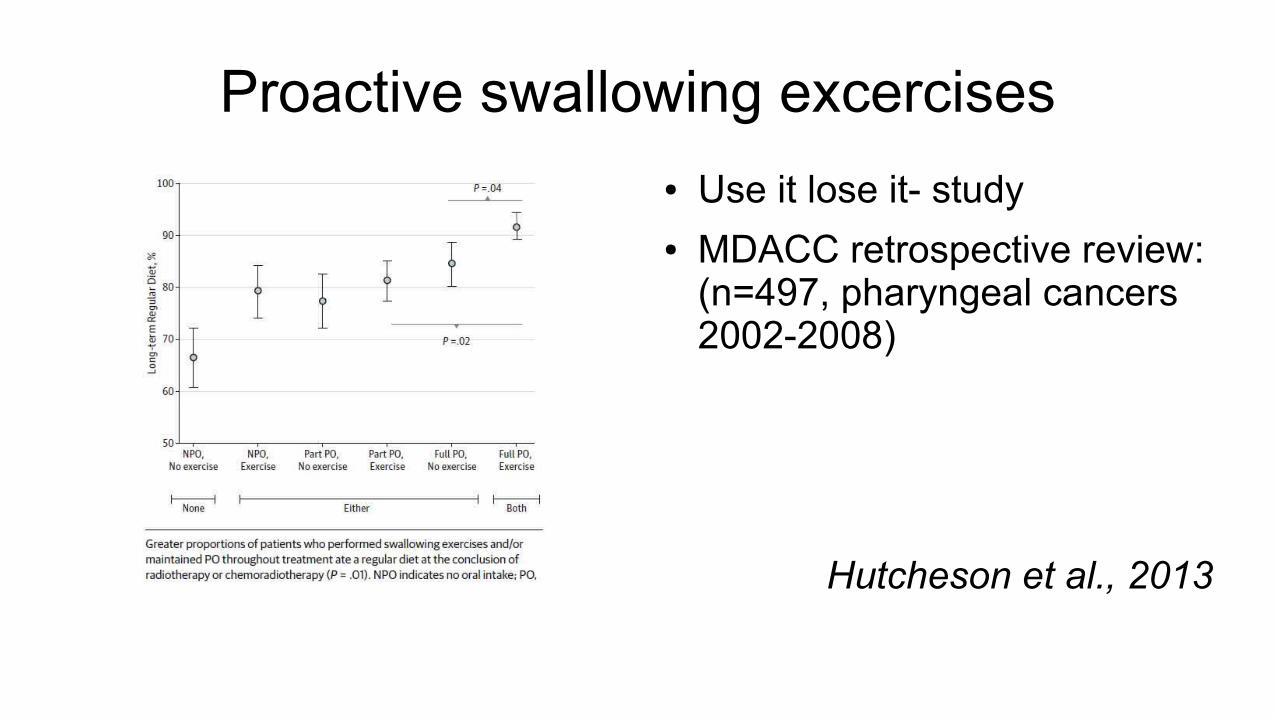
● Use it lose it- study ● MDACC retrospective review:
(n=497, pharyngeal cancers 2002-2008)
Hutcheson et al., 2013
Proactive swallowing excercises
●Mendelsohn
●Jaw/FOM stretch
●Supraglottic
●Masako
●Effortful
3 sets, 10 reps
Eat All Through (EAT) RT
● EAT diet staircase (food
hierarchy)
● Mealtime routine
M.D.Anderson Cancer Center, Texas, Hutcheson 2019
Proactive excercises● Ongoing research:
● Swallowing therapy and progressive resistance training in head and neck cancer patients undergoing radiotherapy treatment: randomized control trial protocol and preliminary data. Hajdu et al.2017
● https://clinicaltrials.gov/ct2/show/results/NCT03455608?view=results
Subacute phase
The effects of cancer and treatment are the focus.
The goal for SLP: evaluate the swallowing and rehabilitate when needed
Intensive rehabilitation
Returning to as normal as possible oral diet
Minimizing aspiration
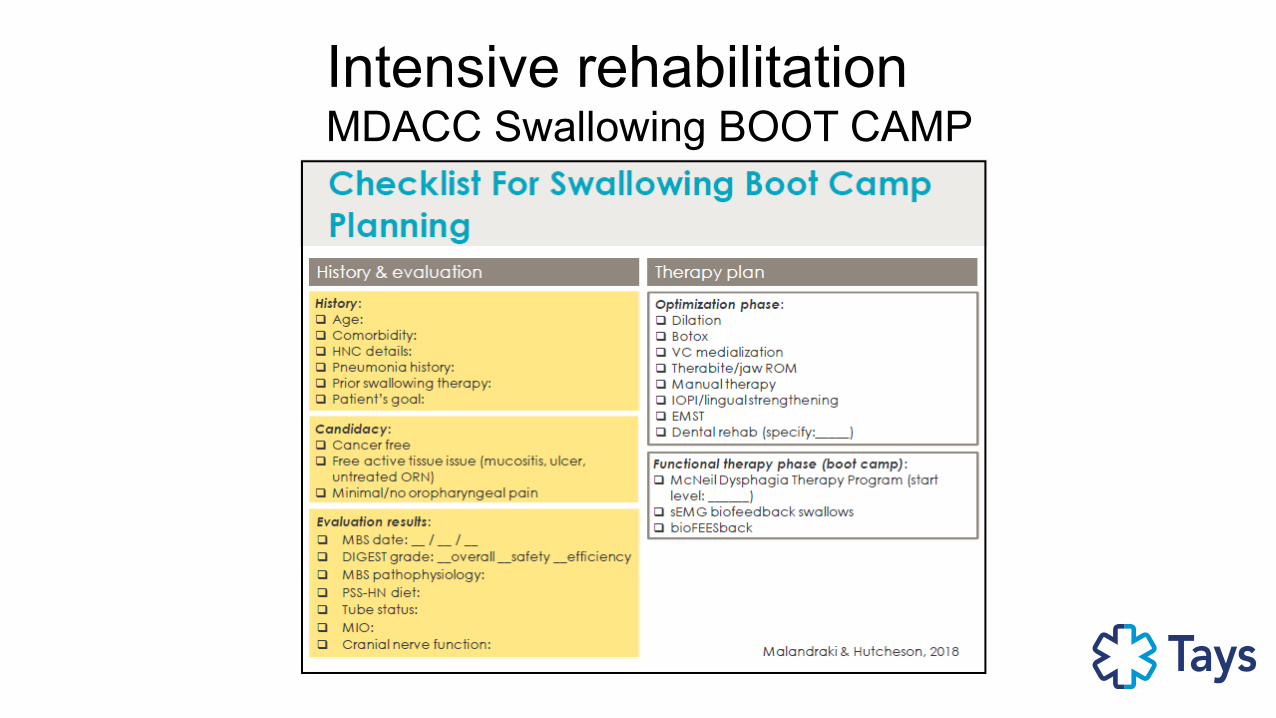
Intensive rehabilitationMDACC Swallowing BOOT CAMP
Progressive resistive functional exercise program:
sEMG Biofeedback “device-driven”
or
MDTP
“bolus- driven”
• Home carry-over
(min 6-8 wks)
• “Mass practice”– Intensive, daily– QD or BID– 2-3 weeks• FUNCTIONAL task= swallowing• Intensifies over time = progressive,Resistive swallowing (exercise)paradigm
Intensive rehabilitationMDACC Swallowing BOOT CAMP
Late phase
Long-term effects of cancer and treatment are the focus.
The goal for SLP: help the patient to adjust to ”new normal”, evaluate when needed.
The swallowing is not likely to get better.
Few patients experience lower cranial neuropathy (median latency 8 years)
Aspiration prevention
Late dysphagia rehabilitation
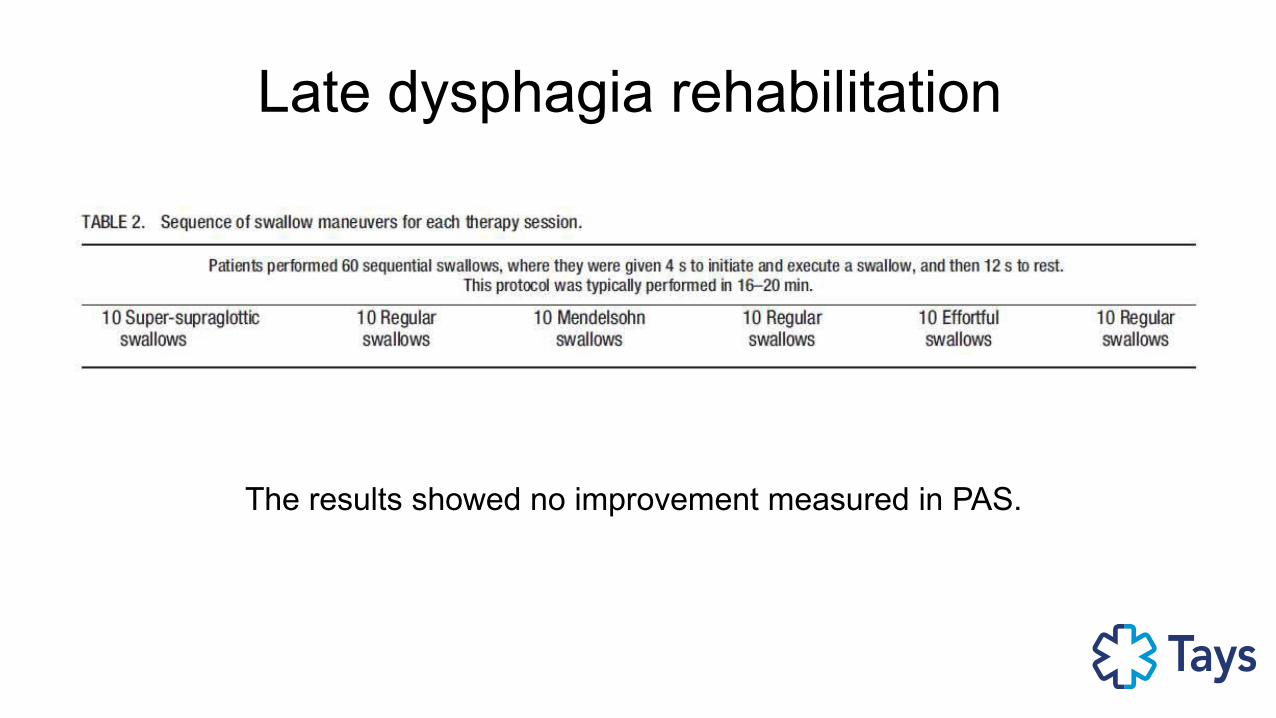
Late dysphagia rehabilitation
The results showed no improvement measured in PAS.
Late dysphagia rehabilitation
Beginning a swallowing therapy program within 1 year of completion of radiotherapy demonstrates more consistent improvement in QOL and diet performance compared to later periods
Van Daele et al., 2019
11.6.2019
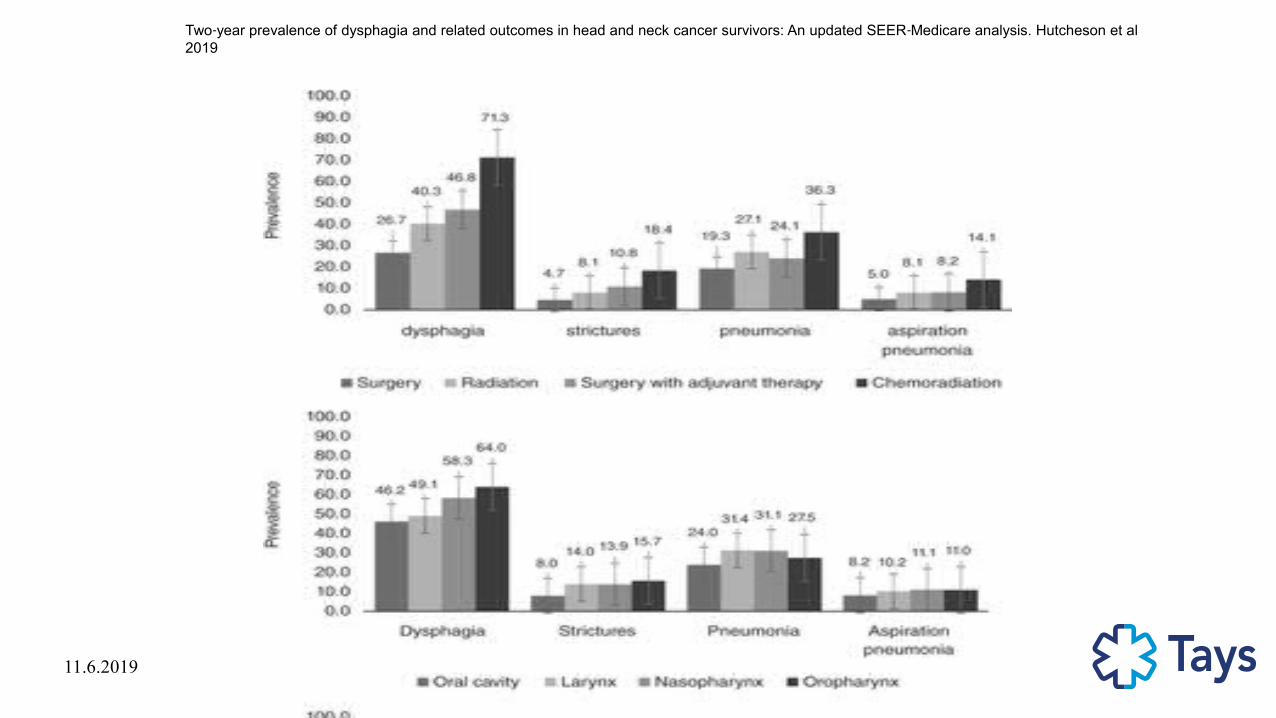
Two year prevalence of dysphagia and related outcomes in head and neck cancer survivors: An updated SEER Medicare analysis. Hutcheson et al ‐ ‐2019
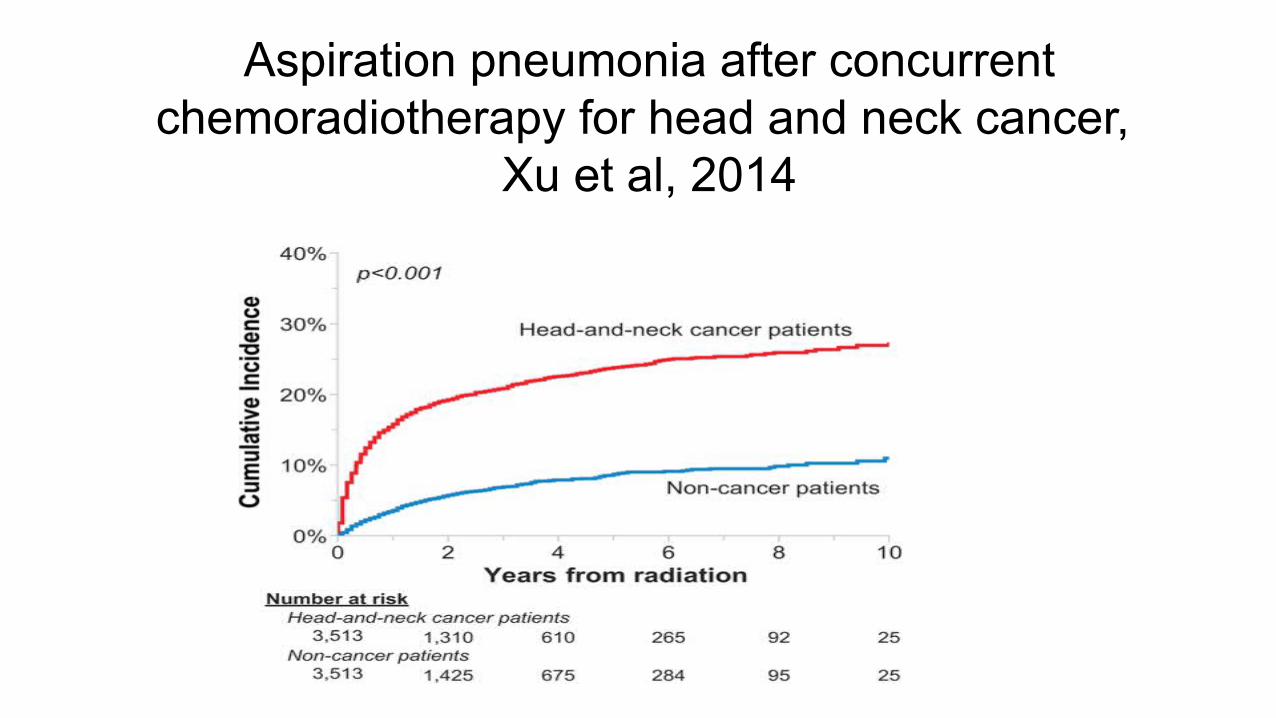
Aspiration pneumonia after concurrent chemoradiotherapy for head and neck cancer,
Xu et al, 2014
Prevention of aspiration pneumonia
Swallow breathing cordination
Expiratory muscle training (EMST)
Oral hygiene
Swallow breathing cordination
HNC patients were trained to initiate swallows during the midexpiratory phase of quiet breathing and continue to expire after swallowing, by using visual biofeedback.
Improvements in 3 MBSImP component scores: laryngeal vestibular closure , tongue base retraction , and pharyngeal residue.
Significant improvements were also seen in PAS scores (P<.0001).
Martin-Harris et al., 2015
EMST / other resipiratory training
●Expiratory muscle strength training (Sapienza)
●Expiratory Muscle Strength Training can increase swallowing safety in HNC patients.
Hutcheson et al., 2018

Oral hygiene
A meta-analysis could only be done on 4 trials; analysis showed a significant risk reduction in pneumonia through oral care interventions
Kaneoka et al., 2017
Novel ideas
●
● Efficacy of a novel swallowing exercise program for chronic dysphagia in long term head ‐and neck cancer survivors.
Kraaijenga et al, 2017

Thank you!
References
Aggarwal, P., Zaveri, J. S., Goepfert, R. P., Shi, Q., Du, X. L., Swartz, M., . . . Hutcheson, K. A. (2018). Symptom burden associated with late lower cranial neuropathy in long-term oropharyngeal cancer SurvivorsSymptom burden associated with late lower cranial neuropathy in long-term oropharyngeal cancer SurvivorsSymptom burden associated with late lower
cranial neuropathy in long-term oropharyngeal cancer survivors. JAMA Otolaryngology–Head & Neck Surgery, 144(11), 1066-1076. doi:10.1001/jamaoto.2018.1791
Arrese, L. C., Schieve, H. J., Graham, J. M., Stephens, J. A., Carrau, R. L., & Plowman, E. K. (2019). Relationship between oral intake, patient perceived swallowing impairment, and objective videofluoroscopic measures of swallowing in patients with head and neck cancer. Head & Neck, 41(4), 1016-1023. doi:10.1002/hed.25542
Clarke, P., Radford, K., Coffey, M., & Stewart, M. (2016). Speech and swallow rehabilitation in head and neck cancer: United kingdom national multidisciplinary guidelines. The Journal of Laryngology & Otology, 130(S2), S180. doi:10.1017/S0022215116000608
Hsiang, C., Chen, A. W., Chen, C., & Chen, M. (2019). Early postoperative oral exercise improves swallowing function among patients with oral cavity cancer: A randomized controlled trial. Ear, Nose & Throat Journal, , 0145561319839822. doi:10.1177/0145561319839822
Hutcheson, K. A., Barrow, M. P., Plowman, E. K., Lai, S. Y., Fuller, C. D., Barringer, D. A., . . . Lewin, J. S. (2018). Expiratory muscle strength training for radiation-associated aspiration after head and neck cancer: A case series. The Laryngoscope, 128(5), 1044-1051. doi:10.1002/lary.26845
Hutcheson, K. A., Nurgalieva, Z., Zhao, H., Gunn, G. B., Giordano, S. H., Bhayani, M. K., . . . Lewis, C. M. (2019). Two-year prevalence of dysphagia and related outcomes in head and neck cancer survivors: An updated SEER-medicare analysis. Head & Neck, 41(2), 479-487. doi:10.1002/hed.25412
Kaneoka, A., Pisegna, J., Miloro, Lo, Saito, H., Riquelme, L., . . . Langmore, S. (2015). Prevention of healthcare-associated pneumonia with oral care in individuals without mechanical ventilation: A systematic review and meta-analysis of randomized controlled trials doi:10.1017/ice.2015.77
Kraaijenga, S. A. C., Molen, L. v. d., Stuiver, M. M., Takes, R. P., Al-Mamgani, A., Brekel, Michiel W. M. van den, & Hilgers, F. J. M. (2017). Efficacy of a novel swallowing exercise program for chronic dysphagia in long-term head and neck cancer survivors. Head & Neck, 39(10), 1943-1961. doi:10.1002/hed.24710
Langmore, S., Pisegna, J., Krisciunas, G., Meyer, T., & Pauloski, B. (2016). A closer look at residue in the post-radiated HNC population
Lawson, N., Krisciunas, G. P., Langmore, S. E., Castellano, K., Sokoloff, W., & Hayatbakhsh, R. (2017). Comparing dysphagia therapy in head and neck cancer patients in australia with international healthcare systems.International Journal of Speech-Language Pathology, 19(2), 128-138. doi:10.3109/17549507.2016.1159334
Malandraki, G., & Hutcheson, K.,A. (2018). Intensive therapies for dysphagia: Implementation of the intensive dysphagia rehabilitation and the MD anderson swallowing boot camp approachesdoi:10.1044/persp3.SIG13.133
Martin-Harris, B., McFarland, D., Hill, E. G., Strange, C. B., Focht, K. L., Wan, Z., . . . McGrattan, K. (2015). Respiratory-swallow training in patients with head and neck cancer doi://doi-org.libproxy.tuni.fi/10.1016/j.apmr.2014.11.022
Messing, B. P., Ward, E. C., Lazarus, C., Ryniak, K., Kim, M., Silinonte, J., . . . Lee, G. (2019). Establishing a multidisciplinary head and neck clinical pathway: An implementation evaluation and audit of dysphagia-related services and outcomes. Dysphagia, 34(1), 89-104. doi:10.1007/s00455-018-9917-4
Pisegna, J., & Langmore, S. (2015). Efficacy of exercises to rehabilitate dysphagia: A critique of the literaturedoi:10.3109/17549507.2015.1024171