-
8/20/2019 Swiatkowski Labor & Delivery[1]
1/59
Normal and AbnormalNormal and Abnormal
Labor and DeliveryLabor and Delivery
Valerie Swiatkowski, MDValerie Swiatkowski, MD
-
8/20/2019 Swiatkowski Labor & Delivery[1]
2/59
ObjectivesObjectives
At the end of this lecture, you will be able At the
end of this lecture, you will be able
to:to: – – Diagnose labor and define the
stagesDiagnose labor and define the stages
– – Assess a laboring patient Assess
a laboring patient – – Diagnose abnormal
labor Diagnose abnormal labor
– – Understand the cardinal movements of
labor Understand the cardinal movements of labor
– – Deliver a babyDeliver a baby
– – Understand complications of
labor Understand complications of labor
-
8/20/2019 Swiatkowski Labor & Delivery[1]
3/59
What is Labor?What is Labor?
Progressive dilation of theProgressive dilation of the
uterine cervix in associationuterine cervix in associationwith
repetitive contractionswith repetitive contractions
-
8/20/2019 Swiatkowski Labor & Delivery[1]
4/59
What is Labor like?What is Labor like?
Subjectively:Subjectively:
– – Regular contractions getting stronger,
longer,Regular contractions getting stronger, longer,closer
together closer together
– – Bloody show presentBloody show present
– – Sedation does not stop true
labor Sedation does not stop true labor
Objectively:Objectively:
– – Cervical change occursCervical change
occurs
– – Descent of the presenting partDescent of
the presenting part
-
8/20/2019 Swiatkowski Labor & Delivery[1]
5/59
What is cervical change?What is cervical change?
-
8/20/2019 Swiatkowski Labor & Delivery[1]
6/59
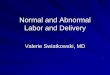
Dilation/ Effacement/StationDilation/ Effacement/Station
www.who.int/.../impac/Images_C/normal2.gif
-
8/20/2019 Swiatkowski Labor & Delivery[1]
7/59
-
8/20/2019 Swiatkowski Labor & Delivery[1]
8/59
Bishops ScoreBishops Score
0 1 2 3
Dilation (cm) 0 1-2 3-4 5+
Effacement (%) 0-30 40-50 60-70 80+
Station -3 -2 -1
Consistency firm med soft
Position post mid ant
-
8/20/2019 Swiatkowski Labor & Delivery[1]
9/59
False Labor is different!False Labor is different!
Irregular contractionsIrregular contractions
No bloody showNo bloody showNo cervical changeNo cervical
change
Head may be ballotableHead may be ballotableSedation stops false
labor Sedation stops false labor
Cervical insufficiency (incompetence):Cervical insufficiency
(incompetence):dilation without contractionsdilation without
contractions
-
8/20/2019 Swiatkowski Labor & Delivery[1]
10/59
Taking a Labor HistoryTaking a Labor History
and Physicaland PhysicalHistoryHistory ::
Know 4 factsKnow 4 facts (at least)(at
least):: – – Onset of contractions?Onset of
contractions?
– – Did the water breakDid the water break
(ROM)?(ROM)? – – Vaginal bleeding?Vaginal
bleeding?
– – Fetal movement (FM)?Fetal movement
(FM)?
PMH/ Meds?PMH/ Meds?
Last PO intake?Last PO intake?
PhysicalPhysical ::
VitalsVitalsCV/CV/Pulm/AbdPulm/Abd
FHTFHT (fetal heart tracing)(fetal heart tracing)
Tocometer Tocometer ((ctxctx tracing)tracing)
EFW byEFW by LeopoldsLeopolds
Pelvic examPelvic examFetal position andFetal position
andpresentationpresentation
-
8/20/2019 Swiatkowski Labor & Delivery[1]
11/59
Assessing labor Assessing labor
What is normal labor?What is normal labor?
-
8/20/2019 Swiatkowski Labor & Delivery[1]
12/59
Stages of Labor Stages of Labor
FirstStage:
labor onset tocomplete dilation
latent
active
SecondStage:
complete dilation todelivery of infant
ThirdStage:
delivery of infant todelivery of placenta
FourthStage: After delivery of theplacenta…
-
8/20/2019 Swiatkowski Labor & Delivery[1]
13/59
Friedman Curve 1978
-
8/20/2019 Swiatkowski Labor & Delivery[1]
14/59http://www.emedicine.com/med/TOPIC3488.HTM
-
8/20/2019 Swiatkowski Labor & Delivery[1]
15/59
-
8/20/2019 Swiatkowski Labor & Delivery[1]
16/59
Assessing labor Assessing labor
The importance of PThe importance of
P’’ssPower Power
PassagePassage
Passenger Passenger
-
8/20/2019 Swiatkowski Labor & Delivery[1]
17/59
POWER!POWER!
Measuring contractions:Measuring contractions:
Palpation: duration, frequency, intensityPalpation: duration,
frequency, intensity – – work intensivework
intensive
ExternalExternal Tocometer Tocometer : graphic
display: graphic display – – no info on strength of
contractionsno info on strength of contractions
Intrauterine pressure catheter (IUPC):Intrauterine pressure
catheter (IUPC): – – accurate feedback in
Montevideo unitsaccurate feedback in Montevideo units
-
8/20/2019 Swiatkowski Labor & Delivery[1]
18/59
IUPCIUPC
Adequate contractions are
>200 MVU in 10 minutes
http://images.google.com/imgres?imgurl=http://z.about.com/d/pregnancy/1/5/y/Z/3/internalmonitor.jpg&imgrefurl=http://pregnancy.about.com/od/laborbasics/ss/interventions_6.htm&h=248&w=400&sz=143&hl=en&start=1&um=1&tbnid=TRuIqIKd9W-zQM:&tbnh=77&tbnw=124&prev=/images%3Fq%3Dintrauterine%2Bpressure%2Bcatheter%26um%3D1%26hl%3Den
-
8/20/2019 Swiatkowski Labor & Delivery[1]
19/59
The Pelvis = PassageThe Pelvis = Passage
U to date. com
-
8/20/2019 Swiatkowski Labor & Delivery[1]
20/59
Clinical PelvimetryClinical Pelvimetry
Obstetrical conjugateObstetrical conjugate
– – anterioranterior – –
symphysissymphysis pubispubis – –
posteriorposterior – – sacral promontorysacral
promontory
– – laterallateral – –
linealinea terminalisterminalis
Diagonal conjugate (clinical)Diagonal conjugate (clinical)
– – inferior border of s.pubis to
s.promontoryinferior border of s.pubis to s.promontory
InterspinousInterspinous/ Bi/ Bi--ischialischial
diameter diameter
-
8/20/2019 Swiatkowski Labor & Delivery[1]
21/59U to date. com
-
8/20/2019 Swiatkowski Labor & Delivery[1]
22/59
Bi-ischial Diameter
-
8/20/2019 Swiatkowski Labor & Delivery[1]
23/59
Calwell-Moloy Classification
Pelvic Types
-
8/20/2019 Swiatkowski Labor & Delivery[1]
24/59
Gynecoid Pelvis
Pelvic brim is a transverse ellipse
(nearly a circle)
Most favorable for delivery
50 percent of patients
-
8/20/2019 Swiatkowski Labor & Delivery[1]
25/59
Android Pelvis
Pelvic brim is triangularConvergent Side Walls (widest
posteriorly)
Prominent ischial spinesNarrow subpubic arch
More common in white women
-
8/20/2019 Swiatkowski Labor & Delivery[1]
26/59
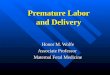
Anthropoid Pelvis
Pelvic brim is an anteroposterior elipseGynecoid pelvis turned
90 degrees
Narrow ischial spinesMuch more common in black women
-
8/20/2019 Swiatkowski Labor & Delivery[1]
27/59
Platypelloid Pelvis
Pelvic brim is transverse kidney shape
Flattened gynecoid shape
-
8/20/2019 Swiatkowski Labor & Delivery[1]
28/59
DonDon’’t forget about thet forget about
thePassenger!Passenger!
http://images.google.com/imgres?imgurl=http://www.health-in-action.org/library/pdf/Shaken%2520Baby/Images/sm%2520shake%2520baby%2520with%2520bkgd.jpg&imgrefurl=http://www.health-in-action.org/node/311&h=1200&w=1350&sz=131&hl=en&start=16&tbnid=9Z42gBPsTsefNM:&tbnh=133&tbnw=150&prev=/images%3Fq%3Dbaby%26gbv%3D2%26hl%3Den
-
8/20/2019 Swiatkowski Labor & Delivery[1]
29/59
LeopoldsLeopoldsmaneuversmaneuvers
4 maneuvers4 maneuvers
to identifyto identify
fetal landmarksfetal landmarksandand
reviewreview
fetofeto--maternalmaternal
relationshipsrelationships
-
8/20/2019 Swiatkowski Labor & Delivery[1]
30/59
DefinitionsDefinitions
PresentationPresentation -- the part that lies closestthe part
that lies closest
to the pelvic inletto the pelvic inlet
Attitude Attitude -- relationship of fetal parts
torelationship of fetal parts to
each other (flexion/extension)each other (flexion/extension)
LieLie -- relationship between long axis ofrelationship between
long axis offetus to mother fetus to mother
PositionPosition -- relationship between fetalrelationship
between fetaldenominator and the vertical (a/p) anddenominator and
the vertical (a/p) and
horizontal (r/l) planes of the birth canalhorizontal (r/l)
planes of the birth canal
SynclitismSynclitism
-
8/20/2019 Swiatkowski Labor & Delivery[1]
31/59
Williams 2001
vertex brow facesinciput
Cephalic Presentation and Attitude
-
8/20/2019 Swiatkowski Labor & Delivery[1]
32/59
Williams 2001
Breech Presentation
-
8/20/2019 Swiatkowski Labor & Delivery[1]
33/59
Williams 2001
A. Longitudinal: 99% of lie
B. Transverse: Associated with multiparity,
placentae previa, polyhydraminos, uterine
anomaly
C. Oblique: Unstable
Lie
-
8/20/2019 Swiatkowski Labor & Delivery[1]
34/59
-
8/20/2019 Swiatkowski Labor & Delivery[1]
35/59
PositionPosition
Anterior Fontanelle Posterior Fontanelle
http://www.brooksidepress.org/Products/OBGYN_101/MyDocuments4/Text/AbnormalLD/AnteriorFontanel.jpg
-
8/20/2019 Swiatkowski Labor & Delivery[1]
36/59
Determining PositionDetermining Position
OP OT
OA
http://www.brooksidepress.org/Products/OBGYN_101/MyDocuments4/Text/AbnormalLD/LOT.jpghttp://www.brooksidepress.org/Products/OBGYN_101/MyDocuments4/Text/AbnormalLD/OP.jpghttp://www.brooksidepress.org/Products/OBGYN_101/MyDocuments4/Text/AbnormalLD/LOT.jpg
-
8/20/2019 Swiatkowski Labor & Delivery[1]
37/59
Williams 2001
A. Anterior asynclitism
B. Posterior asynclitism
SynclitismSynclitism
-
8/20/2019 Swiatkowski Labor & Delivery[1]
38/59
Caput and moldingCaput and molding
www.fammed.washington.edu/.../Newbornexam.htm
http://www.fammed.washington.edu/network/sfm/NewbornExam/Newbornexam.htmhttp://www.fammed.washington.edu/network/sfm/NewbornExam/Newbornexam.htm
-
8/20/2019 Swiatkowski Labor & Delivery[1]
39/59
Abnormal Labor Abnormal Labor
Prolonged latent phaseProlonged latent phase
– – Treatment: therapeutic restTreatment:
therapeutic rest – – 85% active, 10% false
labor 85% active, 10% false labor
Protraction disorder (primary dysfunctionalProtraction disorder
(primary dysfunctional
labor)labor) – – dilation/descent occur at a
slower ratedilation/descent occur at a slower rate
Secondary arrestSecondary arrest – – cessation
of a previous normal dilation for 2cessation of a previous normal
dilation for 2
hourshours
-
8/20/2019 Swiatkowski Labor & Delivery[1]
40/59
Maximum Dilation: 10!Maximum Dilation: 10!
Finally the Second stage ofFinally the Second stage of
labor!labor!
-
8/20/2019 Swiatkowski Labor & Delivery[1]
41/59
Cardinal Movement of Labor Cardinal Movement of
Labor
EngagementEngagement
DescentDescentFlexionFlexion
Internal rotationInternal rotationExtensionExtension
External rotation (restitution)External rotation
(restitution)ExpulsionExpulsion
-
8/20/2019 Swiatkowski Labor & Delivery[1]
42/59
EngagementEngagement
descent of BPD to a level below the plane of the pelvic
inletdescent of BPD to a level below the plane of the pelvic
inletoften occurs before true labor, especially inoften occurs
before true labor, especially in nulliparousnulliparous
-
8/20/2019 Swiatkowski Labor & Delivery[1]
43/59
Flexion during descentFlexion during descent
9.5cm for9.5cm for vtxvtx / 13.5 cm for brow/ 13.5 cm for
brow
-
8/20/2019 Swiatkowski Labor & Delivery[1]
44/59
Williams 2001
-
8/20/2019 Swiatkowski Labor & Delivery[1]
45/59
Stage 2Stage 1
-
8/20/2019 Swiatkowski Labor & Delivery[1]
46/59
Our job in the delivery roomOur job in the delivery room
Control extension of the headControl extension of the head
Protect the perineumProtect the perineumCheck forCheck for
NuchalNuchal cordcord
Suction mouth and noseSuction mouth and nose Avoid
stimulation if Avoid stimulation if meconiummeconium
Catch the baby!Catch the baby!Clamp the cordClamp the cord
-
8/20/2019 Swiatkowski Labor & Delivery[1]
47/59
Delivery ComplicationsDelivery Complications
Arrest of descent Arrest of descent
NuchalNuchal cordcord
Fetal distressFetal distress
PerinealPerineal lacerationlaceration
ShoulderShoulder dystociadystocia
-
8/20/2019 Swiatkowski Labor & Delivery[1]
48/59
PerinealPerineal LacerationsLacerations
First degreeFirst degree -- may involve the vaginalmay involve
the vaginal
mucosa,mucosa, perinealperineal skinskinSecond degreeSecond
degree -- perinealperineal musclesmuscles
Third degreeThird degree -- external anal
sphincter external anal sphincter Fourth degreeFourth
degree -- anterior rectal wallanterior rectal wall
-
8/20/2019 Swiatkowski Labor & Delivery[1]
49/59
Episiotomy?Episiotomy?
Easier to repair Easier to repair
Decrease length ofDecrease length ofsecond stagesecond stage
Decreased trauma toDecreased trauma to
the perineumthe perineum
Increased blood lossIncreased blood loss
Increased traumaIncreased trauma
-
8/20/2019 Swiatkowski Labor & Delivery[1]
50/59
ShoulderShoulder DystociaDystocia
Incidence 0.2Incidence 0.2--2% of deliveries2% of deliveries
(Acker 1986)(Acker 1986)
Impingement of biImpingement of bi--acromialacromial diameter
ofdiameter ofthe fetus against the s.pubis and thethe fetus against
the s.pubis and the
s.promontorys.promontory
4040--50% occur with birth weight
-
8/20/2019 Swiatkowski Labor & Delivery[1]
51/59
ShoulderShoulder DystociaDystocia
Maternal morbidityMaternal morbidity -- postpartumpostpartum
hemorrhage, 4th degree lacerationshemorrhage, 4th degree
lacerations
Neonatal morbidityNeonatal morbidity -- asphyxia,
brachialasphyxia, brachialplexus (plexus (ErbErb palsy, 10palsy,
10--20%, 8020%, 80--90%90%
recover completely), fracture ofrecover completely), fracture
of
humerushumerus/clavicle/clavicle
-
8/20/2019 Swiatkowski Labor & Delivery[1]
52/59
ShoulderShoulder DystociaDystocia ManeuversManeuvers
Look for turtle signLook for turtle sign
Avoid excessive traction on shoulders Avoid excessive
traction on shouldersMcRobertsMcRoberts: flattens the: flattens the
lumbosacrallumbosacral curvecurve
SuprapubicSuprapubic pressurepressure
Ruben/Wood ScrewRuben/Wood Screw -- rotate shoulders to
obliquerotate shoulders to oblique
position and pushing posterior shoulder towardposition and
pushing posterior shoulder toward
fetal backfetal backDeliver posterior armDeliver posterior
arm
ZavanelliZavanelli
-
8/20/2019 Swiatkowski Labor & Delivery[1]
53/59
-
8/20/2019 Swiatkowski Labor & Delivery[1]
54/59
BabyBaby’’s out!s out!
Now What?Now What?
Stage 3: PlacentaStage 3: Placenta
-
8/20/2019 Swiatkowski Labor & Delivery[1]
55/59
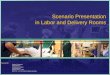
Delivery of the PlacentaDelivery of the Placenta
Signs of placenta separationSigns of placenta separation
– – rise in therise in the
fundusfundus – – firm, globular uterusfirm,
globular uterus
– – sudden gush of bloodsudden gush of
blood
– – umbilical cord lengtheningumbilical cord
lengthening
Examine the placentaExamine the placenta
Delivers within 5Delivers within 5--30 minutes30 minutes
-
8/20/2019 Swiatkowski Labor & Delivery[1]
56/59
Placenta deliveryPlacenta delivery
-
8/20/2019 Swiatkowski Labor & Delivery[1]
57/59
Care of the NeonateCare of the Neonate
Apgar Scoring System
0 1 2
AppearancePale Blue Pink
Pulse Absent 100Grimace Absent Grimace Cry
Active
Activity Limp Some tone Active
Respiration Absent Irregular Reg & Cry
-
8/20/2019 Swiatkowski Labor & Delivery[1]
58/59
ConclusionsConclusions
You will be able to:You will be able to:
– – Diagnose labor and define the
stagesDiagnose labor and define the
stages – – Assess a laboring
patient Assess a laboring patient
– – Diagnose abnormal labor Diagnose
abnormal labor
– – Understand the cardinal movements of
labor Understand the cardinal movements of labor
– – Deliver a babyDeliver a baby
– – Understand complications of
labor Understand complications of labor
-
8/20/2019 Swiatkowski Labor & Delivery[1]
59/59
Thank you!Thank you!
Any questions? Any questions?