Embed Size (px)
Citation preview

Brain and Language 74, 383–394 (2000)
doi:10.1006/brln.2000.2364, available online at http://www.idealibrary.com on
SYMPOSIUM 2: NEURAL CORRELATES OF LANGUAGERECOVERY IN APHASIA
Organized by Cynthia Thompson* and Steve Small†
*Department of Communication Sciences and Disorders, Northwestern University,Evanston, Illinois; and †Department of Neurology, University of Chicago, Chicago, Illinois
There is substantial evidence indicating that individuals with aphasia showrecovery of language function despite sustained damage to left hemispherelanguage areas (Holland, Fromm, & DeRuyter, 1996). Converging evidencefrom clinical studies of aphasic patients, neural imaging studies, and otherdata suggest that the primary candidates for recovery include homologousright hemisphere areas and/or undamaged portions of the language networkin the left hemisphere (Basso, Gardelli, Grassi, & Mariotti, 1989; Dennis &Whitaker, 1976; Demeurisse & Capon, 1987; Cappa, Perani, Grassi, et al.,1997; Heiss, Kessler, Thiel, Ghaemi, & Karbe, 1999; Knopman, Rubens,Selnes, et al., 1984; Weiller, Isensee, Rijintjes, et al., 1995; Willmes &Poeck, 1993). There are a number of factors related to recovery of func-tion, including neurophysiological, subject (e.g., site and extent of lesion),and environmental factors. The precise influence of these variables onreorganizational processes, however, is unknown. In this symposium wewill focus on the impact of environmental variables (i.e., treatment) on re-covery.
In his opening remarks, Steve Small will briefly summarize the results ofanimal studies showing, for example, that motor learning and motoricallyenriched environments, tactile stimulation, and auditory stimulation stronglyinfluence neural organization of the primary motor, somatosensory, and audi-tory cortex, respectively (Greenough, Larson, & Withers, l985; Jenkins, Mer-zenich, Ochs, Allard, & Guic-Robles, 1990; Nudo, Milliken, Jenkins, & Mer-zenich, l996; Recanzone, Schreiner, & Merzenich, l993; Van Praag,Kempermann, & Gage, l999). He also will discuss animal studies showingthat rehabilitative training after injury results in enhancement of representa-tional plasticity (e.g., Nudo et al., 1996; Xerri, Merzenich, Peterson, & Jen-kins, 1998). The upshot of the animal work is that experience directly shapesphysiological reorganization following brain damage. Thus, it is likely thattreatment provided for aphasia influences the extent and manner of reorgani-zational processes.
3830093-934X/00 $35.00
Copyright 2000 by Academic PressAll rights of reproduction in any form reserved.
384 ACADEMY OF APHASIA MEETING
The remaining speakers will present neuroimaging studies of aphasia re-covery. Cornelius Weiller will discuss his PET work examining recoverypatterns in aphasia, including that seen in Wernicke’s aphasic patients whohave received treatment for auditory comprehension deficits. Cindy Thomp-son and Dominique Cardebat will present fMRI studies showing pre- toposttreatment activation patterns in patients with Broca’s and conductionaphasia, respectively. Thompson’s agrammatic aphasic patients receivedtreatment focused on comprehension and production of sentences with syn-tactic dependencies, whereas a Cardebat’s conduction aphasic patient wastreated for word production deficits. Both studies showed differential activa-tion patterns following successful treatment. Findings from these studies,considered together with those derived from animal work, indicate that expe-rience has a major influence on physiological reorganization following braindamage.
OUTLINE OF SYMPOSIUM 2
Introduction: S. Small, University of Chicago, Chicago, Illinois (U.S.A.)Brain Imaging in Recovery from Aphasia: C. Weiller, Neurologische Uni-
versitatsklinik, Hamburg-Eppendorf (Deutschland)FMRI studies of Agrammatic Sentence Comprehension Before and After
Treatment: C. Thompson, S. Fix, D. Gitelman, T. Parrish, & M-M Mesu-lam, Northwestern University, Evanston, Illinois (U.S.A.)
A Functional MRI Study of Language Therapy in a Conduction AphasicPatient: D Cardebat, A. Leger, M. Puel, B. Aithamon, B. Touyeras, K.Boulanouar, & J.F. Demonet, INSERM U 455 and Department of Neurol-ogy, Toulouse (France)
REFERENCES
Basso, A., Gardelli, M., Grassi, M. P., & Mariotti, M. 1989. The role of the right hemispherein recovery from aphasia: Two case studies. Cortex, 25, 555–556.
Cappa, S. F., Perani, D., Grassi, F., et al. 1997. A PET follow-up study of recovery afterstroke in acute aphasics. Brain and Language, 56, 55–67.
Demeurisse, G., & Capon, A. 1987. Language recovery in aphasic stroke patients: clinical,CT and CBF studies. Aphasiology, 1, 301–315.
Dennis, M., & Whitaker, H. A. 1976. Language acquisition following hemidecortication: Lin-guistic superiority of the left over the right hemisphere. Brain and Language, 3, 404–433.
Greenough, W. T., Larson, J. R., & Withers, G. S. 1985. Effects of unilateral and bilateraltraining in a reaching task on dendritic branching of neurons in the rat motor sensoryforelimb cortex. Behavioral Neural Biology, 44, 301–314.
Heiss, W. D., Kessler, J., Thiel, A., Ghaemi, M., & Karbe, H. 1999. Differential capacity ofleft and right hemispheric areas for compensation of poststroke aphasia. Annals of Neurol-ogy, 45, 430–438.
ACADEMY OF APHASIA MEETING 385
Holland, A. L., Fromm, V., & DeRuyter, F. 1996. Treatment efficacy for aphasia. Journal ofSpeech and Hearing Research, 39, S27–S36.
Jenkins, W. M., Merzenich, M. M., Ochs, M. T., Allard, T., & Guic-Robles, E. 1990. Func-tional reorganization of primary somatosensory cortex in adult owl monkeys after behav-iorally controlled tactile stimulation. Journal of Neurophysiology, 63, 82–104.
Knopman, D. S., Rubens, A., Selnes, O. A., et al. 1984. Mechanisms of recovery from aphasia:evidence from serial xenon 133 cerebral blood flow studies. Annals of Neurology, 15,530–535.
Nudo, R. J., Milliken, G. W., Jenkins, W. M., & Merzenich, M. M. 1996. Neural substratesfor the effects of rehabilitate training on motor recovery after ischemic infarct. Science,171(5269), 1791–1794.
Recanzone, G. H., Jenkins, W. M., Hradek, G. T., & Merzenich, M. M. 1992. Progressiveimprovement in discriminative abilities in adult owl monkeys performing a tactile fre-quency discrimination task. Journal of Neurophysiology, 67, 1015–1030.
Recanzone, G. H., Schreiner, C. E., & Merzenich, M. M. 1993. Plasticity in the frequencyrepresentation of the primary auditory cortex following discrimination training in adultowl monkeys. Journal of Neuroscience, 13, 87–103.
Van Praag, H., Kempermann, G., & Gage, F. H. 1999. Running increases cell proliferationand neurogenesis in the adult mouse dentate gyrus. Nature Neuroscience, 2(3), 266–270.
Weiller, C., Isensee, C., Rijntjes, R., et al. 1995. Recovery from Wernicke’s aphasia: A posi-tron emission tomographic study. Annals of Neurology, 37, 723–732.
Willmes, K., & Poeck, K. 1993. To what extent can aphasic syndrome be localized? Brain,116, 1527–1540.
Xerri, C., Merzenich, M. M., Peterson, B. E., & Jenkins, W. 1998. Plasticity of primary so-matosensory cortex paralleling sensorimotor skill recovery from stroke in adult monkeys.Journal of Neurophysiology, 7u9, 2119–2148.
Correspondence should be addressed to C. K. Thompson, Department of CommunicationSciences and Disorders, Northwestern University, 2299 N. Campus Drive, Evanston, IL60208-3570. E-mail: [email protected].
Brain Imaging in Recovery from Aphasia
Cornelius Weiller
Neurologische Universitatsklinik, Hamburg-Eppendorf, Germany
Two aspects are of major importance for understanding the mechanismsunderlying reorganisational changes during recovery of lost function aftercentral lesions:
1. Brain functions may occasionally be localized in distinct brain regionsbut are mainly organized in extended, connected, overlapping, and highlyparallel or reciprocal processing networks, the modular parts of which maysubstitute each other.
2. Localization is not unchangeable, even the adult human brain retainsa ‘‘plastic’’ potential.

386 ACADEMY OF APHASIA MEETING
Plastic changes represent a uniform reaction pattern of the brain and occurunder very different conditions in the intact as well as the lesioned brain asa result of learning or adaptation, with or without any concomitant changein behavioral performance, with or without any obvious teleological reason.After lesions they may either be found as a compelling consequence of thestructural defect (i.e., diaschisis) or due to active intervention (e.g., rehabili-tation).
Learning represents one prominent cause for an actively produced reorga-nization. We can differentiate between learning effects resulting in changesin the anatomical somatotopy of the primary cortices and functional effectsin higher order cortices. In the motor system, interhemispheric transfer ofinformation and interhemispheric learning is accomplished via unimodal as-sociation cortices. Learning can be seen as a refinement of connection be-tween assemblies within the preexisting network. In the normal brain, asso-ciative learning is reflected in repetition suppression of activation andincreased effective connectivity as interaction between brain regions. Afterbrain lesions, changes in representation, induced by active learning or medi-ated by use, may have different electrophysiological correlates and shouldbe interpreted in the context of these models. In recent studies again of themotor system, training-induced recovery was associated with a temporaryaugmentation of excitability, followed by a gradual normalization of excit-ability over weeks and months. When seeing stroke as a disconnection syn-drome, for recovery the brain must upregulate, best focally, its excitabilityto make use of the sparse remaining connections. Once some function hasbeen regained, repetitive use and learning will increase the effective connec-tivity of this feasible pathway and as a consequence fewer neurons will beneeded for the same effect resulting in a concomitant normalization of activa-tion.
Recovery in lesioned brains can be induced in different ways. There islongstanding evidence that brain plasticity and recovery can be influencedby drugs. For example, it is known from animal experiments that serotoner-gic drugs facilitate recovery and in a recent clinical trial on 52 patients abeneficial effect of the selective 5HT reuptake inhibitor fluoxetine in theperformance of severely affected hemiplegics was shown. The underlyingeffects of the drug-induced improvement of function on the organization ofthe brain are yet to be studied and important in understanding the rehabilita-tive mechanisms. In normal subjects, a recent fMRI study showed an in-creased activity in sensorimotor cortex and supplementary motor area duringpassive movement 5 h after ingestion of fluoxetine.
Since the times of Wernicke’s there is dispute whether recovery fromaphasia is mediated by the remaining left hemisphere language-related brainareas or by ‘‘homologous’’ right hemisphere ‘‘centers,’’ a question whichis still unsolved today. The modern brain imaging studies clearly indicatedleft and right hemisphere activations during language tasks in aphasic pa-tients.
ACADEMY OF APHASIA MEETING 387
There are studies stressing the importance of the remaining left hemi-sphere zones. There seems to emerge an agreement that left hemisphere lan-guage areas represent favorite candidates for language processing also inaphasics. However, the question could be posed how much areas in the lefthemisphere activated by language tasks must remain to suffice for recovery.
There is also quite wide agreement that right hemisphere structures doplay a role in recovery from aphasia. In a recent study aiming to assess therelation between reorganization and recovery, we investigated whether anintense comprehension training induces cortical reorganization in aphasicstroke. We studied four patients with Wernicke’s aphasia and a left perisyl-vian lesion. Language comprehension, a function that is often abolished inaphasia but tends to recover quickly, was assessed by an exerpt from a shortversion of the Token Test in 12 consecutive PET scans. Between the scans,the patients underwent intense comprehension training sessions of 8 mineach. The training-induced improvement of language comprehension duringthe scanning correlated with rCBF changes in language-related areas in theright hemisphere only (middle, superior temporal gyrus and supramarginalgyrus, respectively). This study supported the notion of the role of the righthemisphere in recovery from aphasia and substantiated the evidence thatreorganization is actually beneficial.
Again the question remains what exactly and how much can the righthemisphere do and this on an individual basis? In our opinion, there is notone single crucial component of recovery. Rather, recovery of functionseems to imply the ‘‘reconnection’’ or perhaps better the recoordination ofa network of areas, each of which may be specialized in one or more aspectof the lost function but requires the coherent support from others to reacha high level of proficiency.
FMRI Studies of Agrammatic Sentence Comprehension Beforeand After Treatment
Cynthia K. Thompson,*,† Stephen C. Fix,*,‡ Darren R. Gitelman,†Todd B. Parrish,§ and M-Marsel Mesulam†
*Department of Communication Sciences and Disorders, †Department of Neurology,‡Department of Linguistics, and §Department of Radiology,
Northwestern University, Evanston, Illinois
Several neuroimaging studies of syntactic processing in normal subjectshave shown significant activation in Broca’s area (Caplan, Alpert, & Waters,1999; Stromswold, Caplan, Alpert, & Rauch, 1996).1 Research also has
1 But see Just et al. (1996) who found activation in both Broca’s and Wernicke’s areasduring complex sentence processing as well as activation in right hemisphere homologues ofthese areas.

388 ACADEMY OF APHASIA MEETING
shown that aphasic individuals with damage in and around Broca’s areaevince sentence level deficits (Schwartz, Linebarger, Saffran, & Pate, 1987;Zurif, Swinney, Prather, Solomon, & Bushell, 1993) and that patients recoversentence comprehension and production ability with treatment (Thompsonet al., 1997). However, despite a large body of work on the role of the rightand left hemispheres in recovery (Heiss, Kessler, Thiel, Ghaemi, & Karbe,1999; Weiller et al., 1995), little is known about the neural networks recruitedfor sentence processing when the primary areas that subserve this functionare damaged.
In the present study, we investigated the neural correlates of sentence com-prehension in normal subjects and in agrammatic aphasic patients whoshowed difficulty with sentence processing operations. All subjects under-went functional magnetic resonance imaging (fMRI) to examine areas ofsignificant activation under two sentence conditions and a single-word con-trol condition. We also examined the effects of treatment on neural activityby comparing pre- vs. posttreatment scans in two aphasic subjects. Threeaphasic control subjects did not receive treatment, but language tests wereadministered and repeat scans were obtained at 5-month intervals.
Method
Subjects. Eight normal and five agrammatic aphasic individuals served assubjects. All were right-handed, monolingual English speakers; had normalhearing and vision; and were well educated. The aphasic subjects all hadsuffered a single, left hemisphere stroke and were at least 1 year postonset.Language testing using the Western Aphasia Battery and other measuresshowed patterns of performance consistent with agrammatism.
FMRI Stimuli and Procedures
Twenty semantically reversible sentences were audiorecorded in subject-cleft (e.g., It was the waiter who watched the diner) and complex object-cleft form (It was the diner who the waiter watched ). For each sentencepictures were prepared, depicting the target and its semantically reversedcounterpart. Sixty-four single words (animate nouns) also were audio-recorded and corresponding pictures were prepared. Stimuli were randomlydivided into word and sentence blocks and arranged in two stimulus runswith single-word blocks interspersed between sentence blocks, for a total of16 blocks per run.
In the scanner subjects listened to sentences (or words) and viewed pic-tures. Subjects responded by button press when auditory and picture stimulimatched. Aphasic subjects practiced the task in a simulated scanner prior tofMRI scanning.
ACADEMY OF APHASIA MEETING 389
Anatomical and Functional Scans
A 1.5-T Siemens Vision scanner was used for anatomical (T1-weighted)and functional scans. A 3D FLASH sequence was used for anatomical scanswith the following parameters: TR 15 ms, TE 6 ms, flip angle 20°, FOV 220mm, matrix 256 3 256, slice thickness 1.0 mm. Functional volumes wereacquired with the following parameters: TR 4350 ms, TE 40 ms, flip angle90°, FOV 220 mm, matrix 64 3 64. Thirty-two contiguous 4-mm axial sliceswere obtained per scan relative to the AC-PC line. Images were motion cor-rected and normalized onto a common stereotactic space using SPM-96(Wellcome Department of Cognitive Neurology, London, UK).
Treatment Procedures
HR and KG received a 20-week course of linguistically based treatment(Thompson et al., 1997) focused on comprehension and production of nonca-nonical sentences, including object extracted wh-questions (e.g., Who didthe artist chase?), object-clefts (e.g., It was the thief who the artist chased ),and object relative clauses (e.g., The man saw the thief who the artistchased ). Following a baseline period during which a battery of languagetests was administered and comprehension and production of all target sen-tences were tested, one sentence type was trained at a time until acquisitionof all sentences was demonstrated on a daily probe task. Posttreatment lan-guage tests were administered and fMRI scans were performed.
Results
Normal and aphasic subjects’ pretreatment scans. For our normal sub-jects both simple and complex sentences (compared to single words) invokedactivation of Broca’s area (Brodmann’s area (BA) 44) and the supplementarymotor area (BA 6) in the left hemisphere. Wernicke’s area (BA 21 and 22)and the supramarginal (BA 40) and angular gyri (BA 39) were activated,bilaterally. Significant activation also was noted in the dorsolateral prefrontalcortex (BA 46, 9) and the intraparietal sulcus in both hemispheres.
In contrast, only two of the five aphasic subjects showed activation in theleft hemisphere under sentence compared to word processing conditions; oneshowed activation in BA 9 and the other in BA 37. Four of the subjects,however, showed activation in the right hemisphere homologue of Wer-nicke’s area (BA 21, 22), and one showed activation in the right angulargyrus (BA 39). Two patients also recruited the dorsolateral prefrontal cortexin the right hemisphere, but none showed activation in the right hemispherehomologue of Broca’s area.
When complex sentences were contrasted with simple sentences, signifi-cant activation was seen for the normal subjects only in the left hemispherein Broca’s and Wernicke’s areas. No significant activation was noted for the

390 ACADEMY OF APHASIA MEETING
FIG. 1. Pre- and posttreatment fMRI activation patterns seen in one patient with agram-matic aphasia (HR). Pretreatment scanning (left set of scans) showed significant activation inthe right hemisphere in BA 22 and BA 46. Following treatment, increased activation in theright hemisphere homologues of Wernicke’s (BA 22, 21, and 37) and Broca’s area (BA 44,45) was noted (see right set of scans). Slices are from z 5 20 (top left) to z 5 28 (bottomright).
aphasic subjects when object-cleft sentences were contrasted with subject-clefts.
Treatment Results
Both HR and GK showed improved ability to comprehend and produce allsentences entered into treatment. Posttreatment language testing also showedimprovements, particularly on sentence comprehension and production mea-sures. Posttreatment narrative samples showed increases in MLU, the propor-tion of grammatical sentences and the proportion of verbs with correct argu-ments. Language testing of our untreated aphasic subjects showed nochanges across the two test periods.
Treatment-Induced fMRI Activation
Prior to treatment, sentence compared to single-word processing revealedsmall areas of activation in the right hemisphere: BA 22 and BA 46 for HRand BA 39 for KG. Posttreatment scans showed increased activation for both

ACADEMY OF APHASIA MEETING 391
subjects in the right hemisphere homologue of Wernicke’s (BA 22, 21, and37) and Broca’s area (BA 44, 45) (see Fig. 1). KG also showed activationin Wernicke’s area in the left hemisphere. These changes were associatedwith marked improvement in scanner task performance. Untreated aphasicsubjects showed no changes in activation patterns across scans.
Conclusions
These findings show that while normal subjects engage portions of thelanguage network in both hemispheres when comprehending complex andsimple sentences, agrammatic aphasic patients use primarily right hemi-sphere brain sites. Further, normal individuals engage only left hemipheresites for processing complex sentences (both Broca’s and Wernicke’s areas);agrammatic aphasic subjects show no differential activation when processingthe two sentence types. However, when these patients acquire the ability toprocess complex sentences they recruit cortical areas including Wernicke’sarea and its right hemisphere homologue as well as the right hemispherehomologue of Broca’s area. These data provide insight into the physiologicalbases of treatment-induced recovery from aphasia.
REFERENCES
Caplan, D., Alpert, N., & Waters, G. 1999. PET studies of syntactic processing with auditorysentence presentation. NeuroImage, 9, 343–351.
Heiss, W. D., Kessler, J., Thiel, A., Ghaemi, M., & Karbe, H. 1999. Differential capacity ofleft and right hemispheric areas for compensation of poststroke aphasia. Annals of Neurol-ogy, 45, 430–438.
Just, M. A., Carpenter, P., Keller, W. F., et al. 1996. Brain activation modulated by sentencecomprehension. Science, 274, 114–116.
Schwartz, M., Linebarger, M., Saffran, E., & Pate, D. S. 1987. Syntactic transparency andsentence interpretation in aphasia. Language and Cognitive Processes, 2, 85–113.
Stromswold, K., Caplan, D., Alpert, N., & Rauch, S. 1996. Localization of syntactic compre-hension by positron emission tomography. Brain and Language, 52, 452–473.
Thompson, C. K., Shapiro, L. P., Ballard, K. J., Jacobs, B. J., Schneider, S. L., & Tait, M.E. 1997. Training and generalized production of wh- and NP-movement structures inagrammatic speakers. Journal of Speech, Language, and Hearing Research, 40, 228–244.
Weiller, C., Isensee, C., Rijntjes, R., et al. 1995. Recovery from Wernicke’s aphasia: A posi-tron emission tomographic study. Annals of Neurology, 37, 723–732.
Zurif, E., Swinney, D., Prather, P., Solomon, J., & Bushell, C. 1993. An on-line analysis ofsyntactic processing in Broca’s and Wernicke’s aphasia. Brain and Language, 45, 448–464.
Acknowledgment: The work reported here was supported by the McDonnell-Pew Founda-tion Program in Cognitive Neuroscience (C.K.T.) and by the National Institutes of HealthGrants DC01948 (C.K.T.) and NS30863 (M-M.M.).
392 ACADEMY OF APHASIA MEETING
A Functional MRI Study of Language Therapyin a Conduction Aphasic Patient
D. Cardebat, A. Leger, M. Puel, B. Aithamon, B. Touyeras,K. Boulanouar, and J.-F. Demonet
INSERM U 455 and Department of Neurology, Toulouse, France
Very few studies have combined neuroimaging and language therapy instroke patients. Three studies only, to our knowledge, have mainly focusedon this topic so far (Belin et al., 1996; Small, Flores, & Noll, 1998; Mussoet al., 1999), using very different methodology. Such a small number ofstudies devoted to the impact of language therapy on brain reorganizationis in striking contrast with the increasing amount of neuroimaging studiesof spontaneous recovery from aphasia.
However, the relationship between spontaneous or language therapy-induced recovery from aphasia and hemispheric reorganization remains anopen question with, on the one hand, arguments for a laterality shift to theundamaged hemisphere (i.e., the right hemisphere) with mirror regions as-suming the recovered language functions (Weiller et al., 1995; Musso et al.,1999) and, conversely, arguments for recovery of perilesional regions in thedamaged hemisphere (i.e., the left hemisphere) assuming thus the recoveredlanguage functions (Warburton, Price, Swinburn, & Wise, 1999; Heiss,Kessler, Thiel, Ghaemi, & Karbe, 1999; Belin et al., 1996; Small et al.,1998).
The aim of this study is to assess the hemispheric reorganization associatedwith an intensive language therapy in a conduction aphasic by contrastingtwo tasks in which the patient showed dissociated performance. FMRI acti-vation data were obtained before and after language therapy focused on thetask with poor performance at T1.
Subject
Case study. In 1998, a 42-year-old right-handed man suffered from a leftperisylvian ischemic lesion after a spontaneous dissection of the left internalcarotid. Neuropsychological assessment showed (1) a very important deficitin oral production with numerous phonemic paraphasias in spontaneousspeech and naming, repetition, and reading tasks; and (2) a severe auditoryverbal working memory deficit contrasting with preservation of rhymingabilities (whatever the modality of presentation, auditory or visual) and spar-ing of visual memory.
Language therapy lasted 6 weeks (four sessions per week) and was basedon the preserved visual memory processes. Thirty items that belonged to thefMRI protocol were used for patient training in various oral production tasks

ACADEMY OF APHASIA MEETING 393
and the patient was asked to learn the position of articulatory gestures fromdrawings displaying the articulatory tractus.
FMRI Methods
An EPI fMRI experiment was performed on an 1.5-T imager (Siemens)with 10 axial slices parallel to the bicommissural plane, z coordinate from210 to 35 mm, covering perisylvian neocortical areas. Images were acquiredbefore and after language therapy using two tasks, one tapping on the defi-cient process (overt picture naming) and the other on the preserved process(rhyming):
1. Two sets of 30 items were used in an explicit overt picture naming task(ON), only one of which was used in therapy sessions.
2. Two sets of different items (2 3 30) were used in a rhyming task im-plying covert picture naming (Rh) in which subjects had to rise fingers whena word written in the bottom part of a screen rhymed with the name of apicture depicting an object (N 5 2 3 30) shown in the top part of the screen.
Visual stimuli were delivered centrally by a microcomputer throughspecial goggles. Each run lasted 360 s with six activation sequences(6 3 30 s) alternating with six rest sequences. Data were analyzed usingSPM 99. Height threshold was set at 0.0001, and extent threshold at15 voxels.
Results
Behavioral results. T1 Confrontation Naming: 6 hits/30 for ‘‘therapy’’items, 6 hits/30 for non-‘‘therapy items’’;
T2 Confrontation Naming: 13 hits/30 for therapy items, 10 hits/30 for non-therapy items;
T1 Rhyming: 55 hits/60items; andT2 Rhyming: 57 hits/60 items.
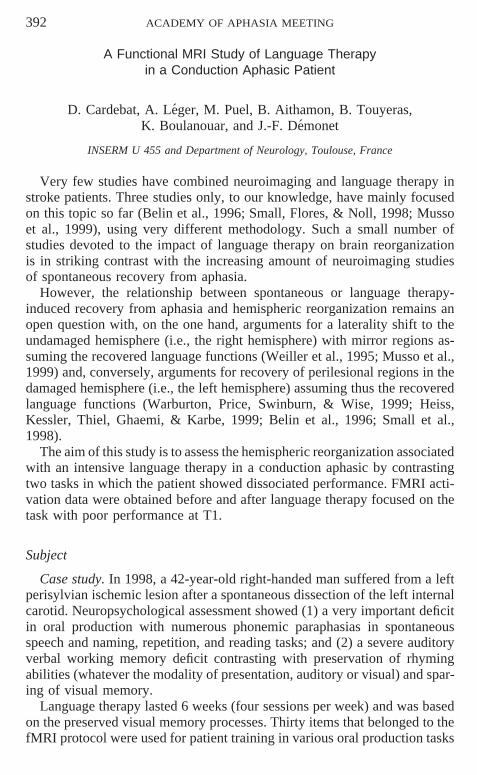
Neuroimaging results. After appropriate image processing, no specific ar-tifacts were noted in images for overt tasks (see Fig. 1). Compared to T1,significant activations for Confontation Naming in T2 were exclusively lo-calized in the left hemisphere and predominated in perilesional areas (BA 6and BA 42). For Rhyming tasks, significant activations in T2 compared withT1 were found bilaterally, involving BA 44, 45, and 46 in the left hemisphereand BA 17 and BA 44 in the right hemisphere.
Discussion
Our results indicate that a specific left perilesional activation is associatedwith therapy-induced improvement for overt confrontation naming. Theseresults are therefore in accordance with the data obtained after melody ther-apy in nonfluent aphasics by Belin et al. (1996). However, the left specificity
394 ACADEMY OF APHASIA MEETING
FIGURE 1
of the activation is not found for rhyming tasks that correspond to preservedprocesses in our patient.
In conclusion, our results highlight the interest of using a ‘‘dissociation’’paradigm (impaired vs. preserved language functions) in order to uncoverthe cerebral correlates of language recovery from aphasia.
REFERENCES
Belin, P., Van Eeckhout, P., Zilbovicius, M., Remy, P., Francois, C., Guillaume, S., Chain,F., Rancurel, G., & Samson, Y. 1996. Recovery from nonfluent aphasia after melodicintonation therapy: A PET study. Neurology, 47, 1504–11.
Heiss, W. D., Kessler, J., Thiel, A., Ghaemi, M., & Karbe, H. 1999. Differential capacity ofleft and right hemispheric areas for compensation of poststroke aphasia. Annals of Neurol-ogy, 45, 430–438.
Musso, M., Weiller, C., Kiebel, S., Muller, S. P., Bulau, P., & Rijntjes M. 1999. Training-induced brain plasticity in aphasia. Brain, 122, 1781–90.
Small, S. L., Flores, D. K., & Noll, D. C. 1998. Different neural circuits subserve readingbefore and after therapy for acquired dyslexia. Brain and Language, 62, 298–308.
Weiller, C., Isensee, C., Rijntjes, M., Huber, W., Muller, S., Bier, D., Dutschka, K., Woods,R. P., Noth, J., & Diener, H. C. 1995. Recovery from Wernicke’s aphasia: A positronemission tomographic study. Annals of Neurology, 37, 723–732
Warburton, E., Price, C. J., Swinburn, K., & Wise, R. J. S. 1999. Mechanisms of recovery fromaphasia: Evidence from positron emission tomography studies. Journal of Neurology,Neurosurgery and Psychiatry, 66, 155–161.




























![Ivy Sports Symposium #ISS2013 Twitter Recap [2 of 2]](https://img.pdfslide.net/doc/110x75/54b6675f4a795949438b46d6/ivy-sports-symposium-iss2013-twitter-recap-2-of-2.jpg)