Embed Size (px)
Citation preview

66ournalofNeurology, Neurosurgery, and Psychiatry 1993;56:626-632
Symptomatic hyponatraemia: can myelinolysis beprevented by treatment?
Cheryl P Harris, Jeannette J Townsend, J Richard Baringer
AbstractThe treatment of hyponatraemia is con-troversial because of the risk of causingcentral or extrapontine myelinolysis(EPM). Rapid correction with hypertonicsaline to a low normal sodium level hasits proponents; others feel that slow cor-rection to below normal sodium values ispreventative. Most investigators feel thatovercorrection should be avoided. It isnot known whether the magnitude ofserum sodium change is more importantthan the actual rate of correction. Wepresent three patients with hypona-traemia ranging from 103 to 105 mmoIlwho were corrected slowly with normalsaline, corrected quickly with hypertonicsaline, or rapidly overcorrected withhypertonic saline. All became comatoseand died; all had EPM with or withoutcentral pontine myelinolysis (CPM). Therate of correction, the solution used, orthe magnitude of correction did not seemto protect against demyelination. In areview of 67 reported CPM cases since1983, no patients documented as havingCPM or EPM by radiological studies ornecropsy were treated with water restric-tion only. A group of 27 hyponatraemicpatients treated only with water restric-tion and 35 with diuretic cessation alonedid not develop CPM or EPM. This maybe a reasonable approach to patientswith symptomatic hyponatraemia andnormal renal function.
(7 Neurol Neurosurg Psychiatry 1993;56:626-632)
Departments ofNeurology andPathology, UniversityofUtah MedicalCenter, Salt LakeCity, Utah, USAC P HarrisJ J TownsendJ R BaringerCorrespondence to:Cheryl P Harris, MD,Department of Pathology,University of Utah MedicalCenter, 50 North MedicalDrive, Salt Lake City,Utah, 84132, USAReceived 9 June 1992and in revised form11 August 1992Accepted 21 August 1992
Controversy continues concerning the treat-ment of patients with hyponatraemia. Someproponents argue that fast correction withhypertonic saline to below normal values isindicated,12 while others state that slow cor-
rection to below normal values will preventneurological sequelae.34 Most clinicians feelthat overcorrection should be avoided.12 Wedescribe three patients who presented withhyponatraemia. One was treated with slowcorrection, one with fast correction, and a
third was overcorrected. All developed neuro-
logical symptoms leading to coma and death.All three demonstrated neuropathologicalchanges of demyelination, either in the formof central or extrapontine myelinolysis. Wereview the various recommendations fortreating hyponatraemia and summarise vari-ous possible pathogenetic mechanisms.
Case historiesPATIENT 1A 44 year old previously healthy womandeveloped a gastrointestinal viral illness twoweeks before admission. Nausea, vomiting,and diarrhoea prompted an increase in waterintake during this period. She becamecomatose at home and was admitted to hospi-tal. On examination her temperature was38'3°C. She was described as restless butresponsive to deep pain. No focal neurologi-cal abnormalities were documented.Laboratory studies revealed a serum sodiumof 103 mmolIl, chloride of 70 mmolIl, potas-sium of 2-7 mmolIl, haematocrit of 48 and awhite blood cell count of 20 x 109/l with 85%polymorphonuclear leucocytes. A chest x raydemonstrated possible basilar infiltrates.Lumbar puncture and CT scan of the headwere normal. The patient was treated withfluid restriction and infusion of normal salineat approximately 0 37 mmol per hour. Overthe next several days her sensorium steadilyimproved and the serum sodium was 130mmol/l by the third hospital day. Two dayslater, however, she developed dysphagia,dysarthria, and a diminished state of respon-siveness. By the seventh hospital day she hadbecome increasingly apathetic and mute.Multiple cultures of urine, blood, throat, andstool were negative. A CT scan, brainstemevoked responses, and an EEG were normal.
During the next two weeks, the womanremained mute with limited spontaneousmovement of the extremities and a slightincrease in flexor tone. The pupillaryresponses were normal. Deep tendon reflexeswere hyperactive and the plantar responseswere extensor bilaterally. No source of infec-tion was located despite persistent rectal tem-peratures of 1 08°F. No seizures wereobserved. The patient died 15 days afteradmission.No infectious source was discovered at
necropsy. Incidental findings included a smalladenocarcinoma of the thyroid and a pituitaryadenoma. The brain weighed 1150 gramsand demonstrated mild cortical atrophy ofthe frontoparietal regions bilaterally. Coronalsections revealed ex-vacuo dilatation of thelateral and third ventricles. The cortical rib-bon was thinned and the sulci were slightlywidened. The basal ganglia, cerebellum, andbrainstem were normal in gross appearance.Microscopic examination of the cortexrevealed neuronal loss with astrocytosis,macrophage infiltration, and neovascularisa-tion primarily confined to the third neuronal
626 on 16 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.6.626 on 1 June 1993. Dow
nloaded from

Symptomatic hyponatraemia: can myelinolysis be prevented by treatment?
layer. The hippocampus and cerebellum hadnormal neuronal populations. Bilateral severedemyelination of the white matter tracts inthe putamen and caudate nuclei was seenwith a brisk macrophage response. The puta-men was diffusely gliotic and there was a mildloss of small neurons with a relative preserva-tion of the larger neurons. A rostral section ofthe pons did not reveal demyelination, andsections of the globus pallidus, thalamus,hypothalamus, and mamillary bodies were
normal.
PATIENT 2A 68 year old woman with a long history ofhypertension, rheumatoid arthritis, andchronic neck pain entered hospital for a cervi-cal myelogram. She had been treated withreserpine, a thiazide diuretic, and low doseprednisone for several years. Her husbandstated that an upper respiratory illness over
the previous two weeks had caused thepatient to increase her water intake.Admission laboratory studies revealed aserum sodium level of 121 mmol/l and potas-sium of 2-6 mmol/l. The cervical myelogramdemonstrated subluxation of the odontoidprocess and compromise of the anteroposte-rior diameter at C1-C2. On the day after themyelogram, the patient vomited and was
hydrated with D5 1/4 NS at 100 ml/hour.She was confused and mentally slowed, wors-
ening as the day progressed. On examination,she was disoriented to time and place but was
not dysphasic and could move all fourextremities normally. Later that day, how-ever, she became comatose with minimalresponse to painful stimulation. Pupils were
midposition but miotic, though they reacteddirectly and consensually to light.Oculocephalic manoeuvers were normal. Noposturing was noted, but bilateral Babinskisigns were present.
Because the inital lumbar puncture for themyelogram demonstrated 323 x 106/1 redblood cells, it was felt that the patient mayhave suffered a subarachnoid haemorrhage.She was treated with steroids and frusemide.Laboratory studies revealed a sodium level of104 mmol/l, potassium 2-2 mmol/l, chloride73 mmol/l, and carbon dioxide 21 mmol/l.Treatment for the hyponatraemia was begunwith 5% sodium chloride at a rate of 2 9mmol/hour with added potassium replace-ment; the steroids were continued. Withineight hours, the patient's sodium had risen to127 mmol/l, and the potassium to 3 mmol/l.Clinically, she was more alert but dysarthric,and weakness was noted in the left arm.Sodium replacement was changed to a nor-mal saline infusion, and in 24 hours theserum sodium was 130 mmol/l. By the nextmorning, however, the patient was obtundedand would not follow commands, though she
moved all four extremities spontaneously. CTscan was normal, and an EEG demonstratedbilateral synchronous periodic sharp waves.
The patient required treatment with intra-venous nitroprusside for an acute elevation ofblood pressure. Over the course of the follow-
ing week, she became comatose andremained unchanged. Serum sodium levelswere maintained between 128 and 130mmoUl. The patient died in a nursing homesix weeks later.
Necropsy revealed pneumonia and diffuseatherosclerosis. The brain weighed 1 100grams and was not oedematous. There weremild atherosclerotic changes in the circle ofWillis. Coronal sections demonstrated thin-ning of the cortex with a dark line in thelower layers at the grey-white junction, mostprominent in the frontoparietal areas. Thehippocampus was also thinned and dis-coloured. The basal ganglia, cerebellum, andbrainstem were grossly unremarkable.Microscopically, the cortex revealed neuronalloss with astrocytosis, macrophage prolifera-tion, and neovascularisation in the lower lay-ers of the cortical ribbon. The hippocampusalso contained a focal area of neuronal loss inthe pyramidal cell layer. White matter tractsin the caudate and putamen demonstratedstriking demyelination bilaterally with thepresence of macrophages. Two rostral sec-tions of the pons did not reveal any demyeli-nation, and a mild dropout of Purkinje cellswas noted in the cerebellar cortex.
PATIENT 3A 55 year old woman developed an upperrespiratory illness ten days before admission.Treatment with erythromycin did notimprove her symptoms. She developed gen-eral malaise, myalgias, nausea, and dizzinessand was admitted to hospital. She appearedpale and confused, and was unable to recallappropriate details of her medical history.Neurological examination demonstrated onlyunsteadiness of gait. While waiting for a chestx ray, the patient became unresponsive for afew seconds; a clinical suspicion of a seizurewas entertained. Laboratory examinationrevealed a serum sodium of 106 mmol/l,potassium 2-6 mmol/l, with serum osmolarity219 mOsm, and urine 330 mOsm.Haematocrit was 31-9 and the white bloodcell count was 14-3 x 109/1 with 89%neutrophils and 11% bands. Chest x raydemonstrated mild bilateral infiltrates andCT scan of the brain was normal.The patient was treated with fluid restric-
tion and phenytoin. After 12 hours, theserum sodium remained at 106 mmol/l, andshe was given 5% sodium chloride at 1-7mmol/hour, and frusemide. After nearly ninehours of this therapy, the sodium was 109mmolIl. Infusion of 5% sodium chloride wascontinued, and after an additional nine hours,her serum sodium was 150 mmol/l. Thepatient's sensorium remained clouded andthe following day she became more lethargicand tachypnoeic. Arterial blood gases demon-strated hypoxia and she was intubated andplaced on a ventilator. During this time shebecame progressively more obtunded, and bythe morning of the fourth hospital day, shewas unresponsive to verbal stimuli.Neurological examination revealed flaccidtetraparesis with minimal reaction to painful
627 on 16 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.6.626 on 1 June 1993. Dow
nloaded from

Hamis, Townsend, Baringer
stimuli. Spontaneous respirations were pre-sent. Funduscopic examination demon-strated sharp discs and no retinalhaemorrhages. Pupillary examination wasunremarkable and doll's eyes and comealreflexes were normal. No spontaneous move-ment of the extremities was seen and theplantar responses were extensor bilaterally.Serum sodium on the fourth hospital day was152 mmol/l and potassium was 3 mmolIl. Alumbar puncture revealed 456 x 106/1 redblood cells, 7 x 106/1 blood cells; protein was39 mg/dl and glucose 99 mg/dl. Cultures ofthe spinal fluid were sterile and a repeat CTscan of the brain was normal. Haematologicalstudies demonstrated persistent anaemia andthrombocytopenia. EEG showed diffuseslowing of the background with features con-sistent with a diffuse encephalopathy. Thepatient remained comatose until her death onthe thirteenth hospital day.A limited necropsy revealed bronchopneu-
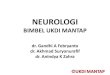
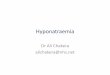
monia and acute haemorrhagic necrosis ofboth adrenal glands. Sections of the brainwere limited to the diencephalon and brain-stem. The thalamus, internal capsule, andbasal ganglia demonstrated severe acutedemyelination of the white matter tracts andpetechial haemorrhages in the thalamus andsubstantia nigra (fig 1). Microscopically,these areas showed diffuse severe myelinolysiswith neuronal cell death. The pons demon-strated numerous areas of acute demyelina-tion (fig 2).
Review of reported central andextrapontine myelinolysis casesSixty seven cases of CPM and EPM havebeen reported since 1983, when the associa-tion of myelinolysis and hyponatraemia wasfirst recognised (table 1). In 38 of these, therewas enough information to determine themanner of correction: 21 patients weretreated with hypertonic saline and 17 withisotonic saline. Fifty seven reports included
Figure 1 A coronal section through the third ventricle demonstrates acute petechialhaemorrhages with histological confirmation ofdemyelination in the thalamus andmidbrain.
Figure 2 A sectionfrom the rostral pons reveals numerouspatchy areas of demyelination centrally and laterally (luxolfast blue stain, 7).
information regarding the rate of correction:serum sodium was normalised in 26 patientswithin 24 hours, and in 31 others was cor-rected over 30 hours to five days. Of note,serum sodium in 16 of these 31 patients wasovercorrected to hypernatraemic levels.
DiscussionHISTORY AND EPIDEMIOLOGY OF CENTRAL ANDEXTRAPONTINE MYELINOLYSISCentral pontine myelinolysis (CPM) wasoriginally documented by Adams et al inpatients suffering from alcoholism or mal-nourishment.'6 Although many of the patientsreported subsequently with myelinolysis werealso alcoholics, CPM is known to occur inhyponatraemic non-alcoholic patients. Thesegroups comprise patients who have beentreated with diuretics,37Ao overhydrated post-operatively,41 become dehydrated because ofvomiting or diarrhoea,"'942 or have beencompulsive water drinkers.6 Subsequently ithas been recognised that electrolyte imbal-ances4', especially hyponatraemia,44 are com-mon antecedents of CPM. A great deal ofcontroversy in recent years has revolvedaround the underlying mechanism causingthe lesions. Most investigators feel that thecause is iatrogenic and secondary to changesin the serum sodium levels. In recentyears, the majority of patients with this syn-drome have had documented hyponatraemiaand have had their serum sodium levels
628 on 16 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.6.626 on 1 June 1993. Dow
nloaded from

Symptomatic hyponatraemia: can myelinolysis be prevented by treatment?
Table 1 Reported CPM cases since 1983
Reference PredisposingNo Age/gender condition Na-,initial Treatment Na+,after Rx Time interval Pathology55 51,f6 40,m6 48,m7 34,m8 52,f9 50,m10 46,m10 39,m3 54,f3 54,f3 60,m3 68,f3 74,f3 75,f3 77,f3 41,m
11 61,f2 59,m2 56,m2 39,m2 56,m2 53,f2 69,f2 16,m2 54,f2 49,f2 47,f2 77,f2 43,m
12 54,m13 41,m14 74,m15 54,f15 21,m15 28,f15 23,f15 23,m15 43,m15 33,m15 45,m15 18,m15 4,f15 8,f16 53,m17 20,f18 59,f19 56,f20 17,f21 28,m22 53,m23 50,f24 37,f25 58,f26 6,f27 18,f27 82,f27 52,f28 61,f29 65,m30 NA,m31 29,f32 46,m33 40,m34 55,m35 66,m35 54,m35 68,f
alcoholicH,O drinkerH,0 drinkeralcoholicoverhydrationalcoholicalcoholicalcoholicNAdiureticsdiureticsdiureticsdiureticsdiureticsalcoholicalcoholicvomitingNANANANANAdiureticsNAdiureticsdiureticsalcoholicoverhydrationoverhydrationalcoholicalcoholicbladder flushliver tKliver tKliver txliver tKliver txliver tKliver txliver tKliver txliver txliver tKalcoholicvomitingdiureticsdiureticsNAalcoholicalcoholicalcoholicalcoholicIV fluidsNAvomitingdiureticsdiureticsalcoholicalcoholicalcoholicdiarrheaalcoholicNAalcoholicDI, lymphomaalcoholicesophageal CA
94 meq/l93 mmol/l96 mmol/l111 meq/197 meq/l102 meq/l100 meq/l107 meq/l102 mmol/l109 mmol/l105 mmol/l103 mmol/115 mmol/l114 mmol/l98 mmol/l109 mmol/195 mmol/149 mmoUl129 mmol/l134 mmol/l130 mmol/l102 mmol/l100 mmol/l99 mmol/l91 mmol/l91 mmolJl96 mmol/l98 mmol/103 mmol/l104 meq/l93 mmolA116 mmol/l129 meq/l121 meq/l120 meq/l130 meq/l122 meq/l126 meq/l118 meq/l121 meq/l131 meq/l126 meq/lNA104 meq/1103 meq/l105 mmol/l113 mmol/100 meq/l126 meq/l104 meq/A108 meq/l112 meq/l110 meq/lNA126 meq/l124 meq/l99 mmol/120 mmol/l93 meq/l100 mmol/l114 meq/l104 meq/l97 mmoL/l110 mmoul103 meq/lNANA
NA = not available, CPM = central pontine myelinolysis,EPM = extrapontine myelinolysis, NSS = normal saline solutionLiver tx = liver transplantation, DI = diabetes insipidus*Pathological examination, generally autopsy
rapidly corrected to normal or supranormallevels.234950 It is not clear whether the lowsodium or the rate of correction of thesodium is instrumental in creating the tissuedamage. It has been noted that hypona-traemia has long been recognised as a com-mon electrolyte disturbance, but CPM wasnot noticed before 1959. As diuretic treat-ment of hypertension is a common predispos-ing factor for CPM, the occurrence of thecondition in the past three decades has beencorrelated with the advent of potent thiazidesand with the treatment of hyponatraemia withintravenous fluids.3951
Extrapontine myelinolysis (EPM) occurs inthe same clinical setting but is seen infre-
quently.4252 The first case was described byMathieson and Olszewski in 1960,53 withpathological changes seen in the cerebellumand putamen in addition to the central pons.Since that time, symmetrical demyelinatinglesions are recognised to occur, in addition,in the thalamus, corpus callosum, subcorticalwhite matter, claustrum, caudate, hypothala-mus, lateral geniculate bodies, amygdala,subthalamic nuclei, substantia nigra, andmedial lemnisci.3338425254 EPM is thought tocoexist with CPM in 10% of all cases,4246 butcan also occur in the absence of a pontinelesion.35 5
The aetiology of the thalamic and nigralpetechial haemorrhages in our patient 3 is
5% NaClHypertonic NaHypertonic Na0-9% NSS5% NaClHypertonic Na3% NaCV/NSSNSSNSS3% NaClNSSNSS5% NaCl3% NaCl3% NaClNSSNSSNANANANANANANANANANAHypertonic NaHypertonic NaHypertonic Na3% NaCl3% NaCIVNSSNANANANANANANANANANANANSSNSS3-5% NaClNSSNSS/3% NaClNANSSNANA3% NaClNANSSNSS + others2% NaCV/NSSNSS3% NaCV/NSS"Rapid2-4/h"NSSNSS1-8% NaClNANANANA
125 meq/1138 mmoUl137 mmol/l"Ni" after 5d125 meq/l130 meq/l134 meq/lNA156 mmol/146 mmoUl132 mmoUl133 mmoMl138 mmol/l130 mmoYl127 mmol/l132 mmoUl133 mmoUl144 mmol/156 mmoUl162 mmoUl159 mmol/130 mmoUl136 mmol/l139 mmol/ -143 mmoUl/132 mmol/ -130 mmoUl137 mmol/154 mmol/l124 meq/l123 mmol/l129 mmoUlNA151 meq/l143 meq/l149 meq/l145 meq/l146 meq/l138 meq/l139 meq/l148 meq/l147 meq/l151 meq/l130 meq/l135 meq/l147 mmol/125 mmol/118 meq/l135 meq/l130 meq/lNA121 meq/lNANA145 meq/l136 meq/l123 mmoUl135 mmol/133 meq/lNA133 meq/l130 meq/l124 mmoUlNA143 meq/l161 meq/l188 meq/l
24 hours30 hours20 hours5 days
24 hours24 hours24 hoursNA72 hours72 hoursNA29 hours24 hours21 hours96 hours72 hours5 days
24 hours48 hours48 hours61 hours15 hours53 hours48 hours34 hours30 hours45 hours37 hours45 hours48 hours24 hours24 hoursNANA4 daysNA24 hours24 hours3 days
48 hours3 days
24 hoursNA24 hours15 hours24 hours6 hours
17 hours24 hours24 hoursNA24 hours48 hoursNA48 hours24 hours3 days4 days
24 hours48 hours17 hours48 hours24 hours5 days"Few days"NANA
CPMIEPMCPM/EPMCPM/EPMNANACPMNANACPM/EPMNANANANANACPMNANADemyelinationDemyelinationDemyelinationDemyelinationDemyelinationDemyelinationDemyelinationDemyelinationDemyelinationDemyelinationDemyelinationDemyelinationCPM/EPMCPMNACPM/EPMCPMCPMCPMCPMCPM/EPMCPM/EPMCPM/EPMCPMCPMCPMCPMCPM/EPMCPM/EPMCPMNANANACPMCPMCPM/EPMCPMNANANACPM/EPMCPMCPMCPMCPM/EPMCPM/EPMCPM/EPMCPM/EPMCPM/EPMEPM
629 on 16 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.6.626 on 1 June 1993. Dow
nloaded from

Harris, Townsend, Baninger
uncertain. Histological abnormalities in capil-laries have been described in CPM, andCPM tends to be worse perivascularly.'6Perhaps the petechiae were related to thepatient's persistent thrombocytopenia in con-junction with the ongoing myelinolysis.CPM has occurred in patients ranging in
age from 3 to 77 years, and there appears tobe no gender predilection;43 of 67 patientsreported since 1983, 34 are women and 33are men. The incidence of the condition hasbeen reported to range from 0.28% to 9.8%in necropsy series.
CLINICAL PRESENTATION OF PATIENTSThe conditions of patients with CPM/EPMrange from asymptomatic to coma or a"locked-in syndrome",'6'9 probably depend-ing on the extent of the areas affected by thedemyelination. Common findings includebehavioural abnormalities, pseudobulbarpalsies, tetraplegia, hyperreflexia, ophthalmo-paresis, seizures, and coma.3 364660 Frequentunderlying systemic conditions include alco-holism, dehydration due to vomiting or diar-rhoea, malnutrition, and burns.'658 Thecondition has also been described with anincreased frequency in patients undergoingorthotopic liver transplantation.6'
ANIMAL MODELS OF CPM/EPMAlthough occasional patients with CPM/EPMhave had normal serum sodium levels or havebeen hypernatraemic, the majority of the ear-liest described patients were hyponatraemicat some point in the course of their illness.'744This finding spawned research into experi-mental hyponatraemia and the production ofCPM/EPM in animal models. Hypo-natraemic rats,45 rabbits,47 and dogs46 treatedrapidly with hypertonic saline developedCPM or EPM or both, whereas animals with-out treatment for their hyponatraemia devel-oped no neuropathological changes. Thiscaused more attention to be devoted to therate of correction of hyponatraemia inhumans rather than the hyponatraemia itself.
RECOMMENDATIONS FOR TREATINGHYPONATRAEMIASubstantial disparity of opinion exists regard-ing the treatment of hyponatraemia. Oneconsideration frequently used to guide ther-apy is the presence of symptoms, as mortalityis minimal in asymptomatic patients.4'48Many authors agree with Arieff, a prominentresearcher in the field of hyponatraemia,48who advises treating symptomatic patients,but recommendations for "rates" of treat-ment vary widely. Arbitrarily, slow correctionhas been defined as changing the serumsodium by less than 0 7 mmol/hour and rapidcorrection as exceeding 2 mmollhour.'Increasing the serum sodium by 2 mmollhouris advised by many studies,' 4162 though otherauthors prefer the slower rate of 0 5mmol/hour.' Arieff, however, has notedthat the rate of correction is probably not asimportant as the absolute change in serumsodium,48 and suggests not increasing the
serum sodium by more than 25 mmol overthe first 24 hours. A general consensus is thatthe patient should not be made hyperna-traemic.' 2 64The agents used to treat the hypo-
natraemia have also been subjected toscrutiny: rapid correction of hyponatraemiais usually accomplished by the use of hyper-tonic saline, though CPM/EPM has alsooccurred in patients treated with isotonicsaline."1 1161719 22 28 32 Frusemide used in con-junction with intravenous fluids may diminishthe incidence of CPM/EPM.46'
Analysis of the treatments reported in table1 in patients who ultimately developed CPMor EPM would suggest that the concentrationof sodium chloride and the rate of adminis-tration make no difference to the rate ofdevelopment of CPM or EPM.
ANALYSIS OF PRESENT CASESThe three patients described here presentedwith very low serum sodium levels and weretreated differently, yet all suffered fromincreasing obtundation leading to coma.None of the patients were malnourished, norwas there a history of significant alcoholintake. Two patients developed EPM andcortical neuronal death while the third patienthad both pontine and extrapontine myelinol-ysis. Cortical neuronal death mimicking thechanges seen in anoxia is uncommon inextrapontine myelinolysis but has beenreported in several cases.5 42 53
These three cases emphasise the dilemmafacing clinicians concerning treatment ofhyponatraemia. Of the three patients pre-sented, one was treated over the course ofthree days with isotonic saline, hypona-traemia in the second patient was rapidly cor-rected with hypertonic saline, and serumsodium in the third patient was rapidly over-corrected with hypertonic saline.An analysis of 185 patients with sympto-
matic hyponatraemia reported since 1954 wasundertaken. The initial serum sodium rangedfrom 95 mmol/l to 124 mmol/l and symptomsvaried from weakness and lethargy to seizuresand frank coma. Fifty three patients treatedwith hypertonic saline improved and the clini-cal condition of 43 worsened. Eighteenpatients treated with normal saline improvedand nine worsened. Twenty seven patientswere treated only with water restriction: allwere felt to have improved. Thirty fivepatients were treated only by the withdrawalof diuretics and all improved. It should benoted that these numbers do not reflect thethousands of hyponatraemic patients, treatedin various fashions, with both favourable andpoor outcomes, all ofwhom are unreported.The absolute change in serum sodium,
suggested to be the inciting factor of myeli-nolysis by Arieff,48 in our three patients was 9mmol/24 hours, 23 mmol/8 hours, and 41mmol/24 hours. In the 67 reported cases ofCPM since 1983, information concerningabsolute change of serum sodium was avail-able in 51 patients. Twenty patients had anincrease in serum sodium of less than 15
630 on 16 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.6.626 on 1 June 1993. Dow
nloaded from

Symptomatic hyponatraemia: can myelinolysis be prevented by treatment?
mmol/24 hours, although the hyponatraemiain five of the patients was overcorrected. Theincrease in 12 patients ranged from 16 to 25mmol/24 hours, with three overcorrections.Seventeen patients sustained an increase inserum sodium ranging from 26 to 40mmol/24 hours (with one overcorrection).Successive sodium levels 24 hours apart weremore than 40 mmol greater in two additionalpatients. Although these numbers are toosmall to prove or disprove a theory, correc-
tion of the hyponatraemia in 34 of thesepatients (including two of the current cases)fall into the recommended 25 mmol/24 hourincrease in serum sodium,48 yet the patientsstill suffered from myelinolysis.Our three cases of CPMIEPM, combined
with a review of reported cases since 1983,seem to suggest that none of these factors(the rate of serum sodium correction, theabsolute sodium change, or the solutionemployed) are the critical factors in the pre-
vention of central or extrapontine myelinoly-sis. There have been no patients withhyponatraemia documented to have CPM or
EPM either by radiological studies or autopsy
who have been treated with water restrictiononly, and allowed to "self-correct" theirhyponatraemia. This review would suggest
that water restriction combined with cessa-
tion of diuretic therapy and observation may
lead to a more salutary outcome, and may bereasonable in some patients with sympto-
matic hyponatraemia and normal renal func-tion. Further research based on animalmodels might identify an additional factor inthe treatment of hyponatraemia which willenable clinicians to prevent this frequentlyfatal condition.
We thank Mr Don Morse for photographic assistance.
1 Ayus JC, Krothapalli RK, Arieff Al. Changing concepts intreatment of severe symptomatic hyponatremia. AmMed 1985;78:897-902.
2 Ayus JC, Krothapalli RK, Arieff Al. Treatment of sympto-matic hyponatremia and its relation to brain damage. NEnglJMed 1987;317:1190-5.
3 Stems RH, Riggs JE, Schochet SS. Osmotic demyelina-tion syndrome following correction of hyponatremia. NEnglJMed 1986;314:1535-42.
4 Cluitmans FHM, Meinders AE. Management of severe
hyponatremia: rapid or slow correction? Am Med1990;88:161-6.
5 Hazratji SMA, Kim RC, Lee SH, et al. Evolution of pon-tine and extrapontine myelinolysis. Comput AssistTomogr 1983;7:356-61.
6 Kainins RM, Berkovic SF, Bladin PF. Central pontinemyelinolysis with widespread extrapontine lesions: a
report of two cases. Clin Exp Neurol 1984;20:189-202.7 Stam J, van Oers MHJ, Verbeeten B. Recovery after cen-
tral pontine myelinolysis. JNeurol 1984;231:52-3.8 Brunner JE. Central pontine myelinolysis in a patient with
adrenal insufficiency. Henry Ford Hosp Med Jf1985,33:45-7.
9 Kold A, Johansen 0, Reintoft I, et al. Central pontinemyelinolysis-a case report with typical neuropathologi-cal findings. Acta Neurol Scand 1986;73:260-3.
10 De Cunha C, Bertotini TE, Lawrence J, et al. Centralpontine myelinolysis-a preventable condition. TennMed Assoc 1986;79:469-72.
11 Nielsen JM. Central pontine myelinolysis complicatinghyponatremia. Med JAust 1987;146:492-4.
12 Peces R, Ablanedo P, Alvarez J Central pontine and
extrapontine myelinolysis following correction of severe
hyponatremia. Nephron 1988;49:160-3.13 Walker JV, Englander RN. Central pontine myelinolysis
following rapid correction of hyponatremia in an alco-holic. Am Kidney Dis 1988;12:531-3.
14 Weissman JD, Weissman BM. Pontine myelinolysis anddelayed encephalopathy following the rapid correctionof acute hyponatremia. Arch Neurol 1989;46:926-7.
15 Estol CJ, Faris AA, Martinez AJ, et al. Central pontine
myelinolysis after liver transplantation. Neurology1989;39:493-8.
16 Oh MS, Uribarri J, Barrido D, et al. Case report: dangerof central pontine myelinolysis in hypotonic dehydrationand recommendation for treatment. Am J Med Sci1989;298:41-3.
17 Castillo RA, Ray RA, Yaghmai F. Central pontine myeli-nolysis and pregnancy. Obstet Gynecol 1989;3:459-61.
18 Clifford DB, Gado MH, Levy BK. Osmotic demyelina-tion syndrome-lack of pathologic and radiologic imag-ing correlation. Arch Neurol 1989;46:343-7.
19 Marra TR. Hemiparesis apparently due to central pontinemyelinolysis following hyponatremia. Ann Neurol1983;14:687-8.
20 Kandt RS, Heldrich FJ, Moser HW. Recovery from prob-able central pontine myelinolysis associated withAddison's disease. Arch Neurol 1983;40: 118-9.
21 Gerber 0, Geller M, Stiller J, et al. Central pontine myeli-nolysis-resolution shown by computed tomography.Arch Neurol 1983;40:116-8.
22 Price DB, Kramer J, Hotman GC, et al. Central pontinemyelinolysis: report of a case with distinctive appearanceon MR imaging. AJNR 1987;8:576-7.
23 Rosenbloom S, Buchholz D, Kumar AJ, et al. Evolution ofcentral pontine myelinolysis on CT. AJNR1984;5:110-2.
24 DeWitt LD, Buonanno FS, Kistler JP, et al. Central pon-tine myelinolysis: demonstration by nuclear magneticresonance. Neurology 1984;34:570-6.
25 Takeda K, Sakuta M, Saeli F. Central pontine myelinoly-sis diagnosed by magnetic resonance imaging. AnnNeurol 1985;17:310-1.
26 Steinsapir KD, Vinters HV. Central pontine myelinolysisin a child with the Shwachman-Diamond syndrome.Hum Pathol 1985;16:741-3.
27 Thompson PD, Gledhill RF, Quinn NP, et al.Neurological complications associated with parenteraltreatment: central pontine myelinolysis and Wernicke'sencephalopathy. BMJ 1986;292:684-5.
28 Rodriguez ML, Hankey GJ. The "locked-in syndrome"and alcoholism-a preventable complication. Med JfAust 1987;146:487-92.
29 Redmond J, Brunner J, Haggar A, et al. Central pontinemyelinolysis: evolution following correction of acutehyponatremia shown by MRI (abstract). Neurology1987;37(suppl):306.
30 Grafton ST, Bahls F, Bell KR. Acquired dystonia follow-ing central pontine myelinolysis (abstract). Neurology1987;37(suppl):276.
31 Price BH, Mesulam MM. Behavioral manifestations ofcentral pontine myelinolysis. Arch Neurol1987;44:671-3.
32 Rippe DJ, Edwards MK, D'Amour PG, et al. MR imagingof central pontine myelinolysis. Jf Comput Assist Tomogr1987;11:724-6.
33 Boon AP, Potter AE. Extensive extrapontine and centralpontine myelinolysis associated with correction of pro-found hyponatremia. Neuropathol Appl Neurobiol1987;13: 1-9.
34 Zegers de Beyl D, Flament-Durand J, Borenstein S, et al.Ocular bobbing and myoclonus in central pontinemyelinolysis. J Neurol Neurosurg Psychiatry1983;46:564-5.
35 Okeda R, Kitano M, Sawabe M, et al. Distribution ofdemyelinating lesions in pontine and extrapontinemyelinolysis-three autopsy cases including one casedevoid of central pontine myelinolysis. Acta Neuropathol1986;69:259-66.
36 Adams RD, Victor M, Mancall EL. Central pontinemyelinolysis-a hitherto undescribed disease occurringin alcoholic and malnourished patients. Arch NeurolPsychiat 1959;81:154-72.
37 Conger JD, McIntyre JA, Jacoby WJ. Central pontinemyelinolysis associated with inappropriate antidiuretichormone secretion. Am J Med 1969;47:813-7.
38 Finlayson MH, Snider S, Oliva LA, et al. Cerebral andpontine myelinolysis-two cases with fluid and elec-trolyte imbalance and hypotension. J7 Neurol Sci1973;18:399-409.
39 Messert B, Orrison WW, Hawkins MJ, et al. Central pon-tine myelinolysis-considerations on etiology, diagnosisand treatment. Neurology 1979;29: 147-60.
40 Telfer RB, Miller EM. Central pontine myelinolysis fol-lowing hyponatremia, demonstrated by computerizedtomography. Ann Neurol 1979;6:455-6.
41 Arieff Al. Hyponatremia, convulsions, respiratory arrestand permanent brain damage after elective surgery inhealthy women. NEnglJ Med 1986;314:1529-35.
42 Tomlinson BE, Pierides AM, Bradley WG. Central pon-tine myelinolysis-two cases with associated electrolytedisturbance. QJMed 1976;179:373-86.
43 Monseu G, Flament-Durand J. Pathogenesis of centralpontine myelinolysis. A clinical and pathologicaldescription of three cases. Path Europ 197 1;6 1:75-94.
44 Burcar PJ, Norenberg MD, Yarnell PR. Hyponatremiaand central pontine myelinolysis. Neurology1977;27:223-6.
45 Kleinschmidt-DeMasters BK, Norenberg MD. Rapid cor-rection of hyponatremia causes demyelination: relationto central pontine myelinolysis. Science 1981;211:1068-70.
46 Laureno R. Central pontine myelinolysis following rapidcorrection of hyponatremia. Ann Neurol 1983;13:232-42.
47 Illowsky BP, Laureno R. Encephalopathy and myelinolysis
631
on 16 March 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.56.6.626 on 1 June 1993. D
ownloaded from

Harris, Townsend, Baringer
after rapid correction of hyponatremia. Brain 1987;l1O:855-67.
48 Arieff Al. Hyponatremia (Grand Rounds). Mt SinaiMed 1990;57: 125-35.
49 Leslie KO, Robertson AS, Norenberg MD. Central pon-tine myelinolysis: an osmotic gradient pathogenesis(abstract). Neuropathol Exp Neurol 1980;39:370.
50 Norenberg MD, Leslie KO, Robertson AS. Associationbetween rise in serum sodium and central pontinemyelinolysis. Ann Neurol 1982;11: 128-35.
51 Aleu FP, Terry RD. Central pontine myelinolysis. ArchPathol 1963;76: 140-6.
52 Wright DG, Laureno R, Victor M. Pontine and extrapon-tine myelinolysis. Brain 1979;102:361-85.
53 Mathieson G, Olszewsti J. Central pontine myelinolysiswith other cerebral changes. Neurology 1960;10:345-54.
54 Monteiro L. La myelinolyse du centre du pont dans lecadre d'un nouveau syndrome histopathologique detopographie systematisee. Neurol Sci 1971;13:293-314.
55 Laureno R, Karp BI. Pontine and extrapontine myelinoly-sis following rapid correction of hyponatremia. Lancet1988;i: 1439-41.
56 Norenberg MD. A hypothesis of osmotic endothelialinjury-a pathogenetic mechanism in central pontinemyelinolysis. Arch Neurol 1983;40:66-9.
57 Endo Y, Oda M, Hara M. Central pontine myelinolysis-
a study of 37 cases in 1000 consecutive autopsies. ActaNeuropathol 1981;53:145-53.
58 McKee AC, Winkelman MD, Banker BQ. Central pon-tine myelinolysis in severely burned patients: relation-ship to serum hyperosmolality. Neurology 1988;38:1211-7.
59 Gocht A, Colmant HJ. Central pontine and extrapontinemyelinolysis: a report of 58 cases. Clin Neuropathol1987;6:262-70.
60 McCormick SF, Danneel CM. Central pontine myelinoly-sis. Arch Intern Med 1967;119:444-78.
61 Starzl TE, Schneck SA, Mazzoni G, et al. Acute neurolog-ical complications after liver transplantation with partic-ular reference to intraoperative cerebral air embolus.Ann Surg 1978;187:236-40.
62 Narins RG. Therapy of hyponatremia-does haste makewaste? N EnglJ Med 1986;314:1573-5.
63 Valenstein E, Watson RT, Quisling RG. Neostriatallesions in the osmotic demyelination (abstract).Neurology 1987;37 (suppl):178.
64 Ayus JC, Krothapalli RK, Arieff AI, et al. Overcorrectionrather than rapid correction induces central pontinemyelinolysis in patients with severe hyponatremia(abstract). Kidney Int 1985;27:132.
65 Worthley LIG, Thomas PD. Treatment of hyponatremicseizures with intravenous 29-2% saline. BMJ1986;292:168-70.
632 on 16 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.56.6.626 on 1 June 1993. Dow
nloaded from