Embed Size (px)
Citation preview
ARTICLE IN PRESS
The Breast (2006) 15, 246–252
THE BREAST
KEYWORDBreast carLymphoma
0960-9776/$ - sdoi:10.1016/j.b
�CorrespondHospital North0191 333 2491.
E-mail addr
www.elsevier.com/locate/breast
CASE REPORT
Synchronous presentation of breast carcinoma andlymphoma in the axillary nodes
Julie Cox�, Linsley Lunt, Lesley Webb
Breast Screening Unit, Queen Elizabeth Hospital, Gateshead, NE9 6SX, UK
Received 21 February 2005; received in revised form 23 May 2005; accepted 23 June 2005
Scinoma;
ee front matter & 2005reast.2005.06.009
ing author. DepartmentDurham, North Rd., Du
ess: [email protected]
Summary We report the first series of cases in the literature of three femalepatients with a synchronous presentation of breast carcinoma with coincidentalaxillary lymphoma. Aspects of each case are described and learning points forclinician discussed.& 2005 Elsevier Ltd. All rights reserved.
Introduction
While the occurrence of a second tumour is a well-recognised phenomenon in patients with treatedmalignancy, the simultaneous presentation with asecond synchronous non-breast primary malignancyis rare.
We report three interesting patients who pre-sented over 15 years with breast carcinomas andcoincidental findings of axillary non-Hodgkin’slymphoma and review the published literatureconcerning this unusual topic.
Case 1
A 63-year-old woman presented as a symptomaticreferral from her GP in 2001 with a 4-week history
Elsevier Ltd. All rights reserve
of Radiology, Universityrham, DH1 5TW, UK. Tel.:
(J. Cox).
of a lump in the upper outer quadrant of her leftbreast.
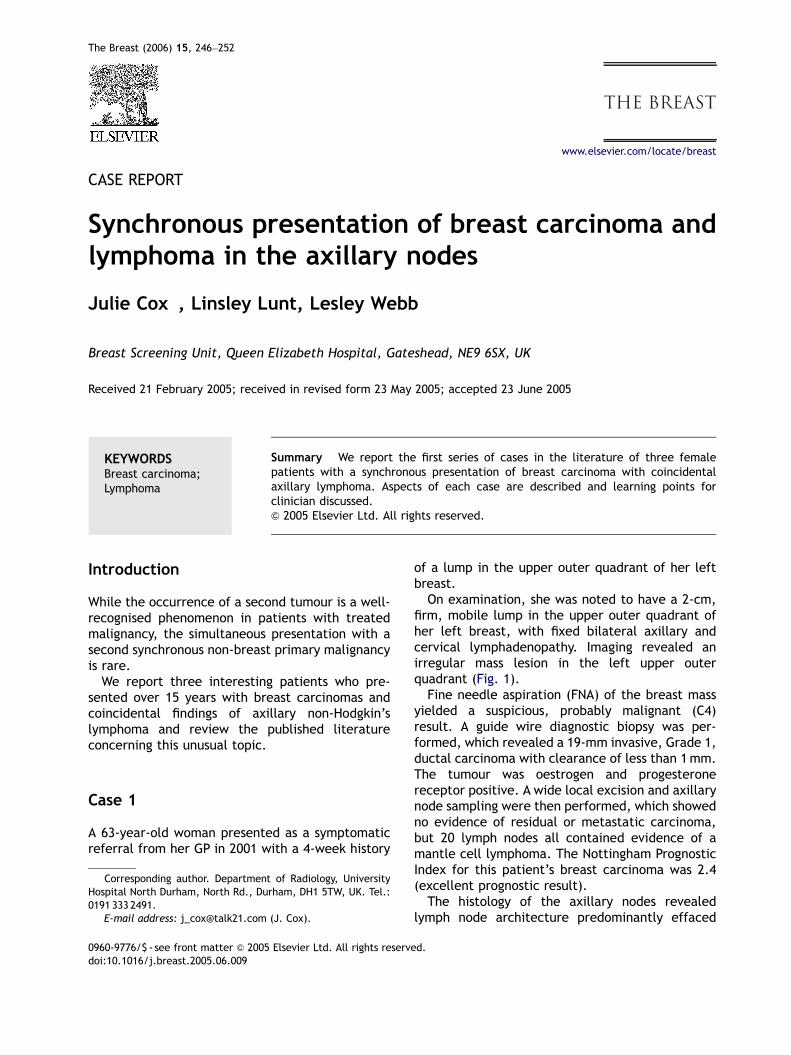
On examination, she was noted to have a 2-cm,firm, mobile lump in the upper outer quadrant ofher left breast, with fixed bilateral axillary andcervical lymphadenopathy. Imaging revealed anirregular mass lesion in the left upper outerquadrant (Fig. 1).
Fine needle aspiration (FNA) of the breast massyielded a suspicious, probably malignant (C4)result. A guide wire diagnostic biopsy was per-formed, which revealed a 19-mm invasive, Grade 1,ductal carcinoma with clearance of less than 1mm.The tumour was oestrogen and progesteronereceptor positive. A wide local excision and axillarynode sampling were then performed, which showedno evidence of residual or metastatic carcinoma,but 20 lymph nodes all contained evidence of amantle cell lymphoma. The Nottingham PrognosticIndex for this patient’s breast carcinoma was 2.4(excellent prognostic result).
The histology of the axillary nodes revealedlymph node architecture predominantly effaced
d.
ARTICLE IN PRESS
Figure 1 A 63-year-old woman presented as a symptomatic referral from her GP with a 4-week history of a lump in theupper outer quadrant of her left breast. Please note right axillary lymphadenopathy on the right medio-lateral oblique(MLO) mammogram (a). Bilateral mammography (a–d) reveals an ill-defined mass in the left upper outer quadrant.Ultrasound confirmed the presence of an ill-defined hypoechoic mass (e, f). The eventual diagnosis was of an invasiveGrade 1 ductal carcinoma in the left breast with coexistent mantel cell lymphoma.
Synchronous presentation of breast carcinoma and lymphoma in the axillary nodes 247
by a diffuse infiltrate of small centrocyte-like cells.Some residual germinal centres were seen sur-rounding the small cells in a mantle/marginal zonepattern.
Immunohistochemistry demonstrated that theinfiltrating cells expressed the B cell antigensCD20 and CD79a, as well as CD5 and cyclin D1.Immunostaining for CD10 and BCL6 highlighted theresidual reactive germinal centres. The tumourcells did not express CD23. The K167 proliferationfraction was low (less than 5%). The final WHOclassification was of a B cell lymphoma, withperipheral mantle cells.
The patient was treated with radiotherapyto her left breast and was started on tamox-ifen.
Staging investigations showed evidence of aStage IIIa lymphoma. She underwent chemotherapywith four courses of adriamycin, carmustine,cyclophosphamide, and melphalan, which resultedin a complete remission.
Ten months later in September 2002 at a routinereview, she presented with a small right axillarynode. The node was biopsied and showed recurrentmantle cell lymphoma.
Computed tomography demonstrated extensivemediastinal, abdominal and pelvic disease with amass arising from the small bowel mesentery. Shewas then treated with further chemotherapy withfludarabine and cyclophosphamide. She had a goodresponse and was well at the last clinical review inNovember 2004.
ARTICLE IN PRESS
J. Cox et al.248
Case 2
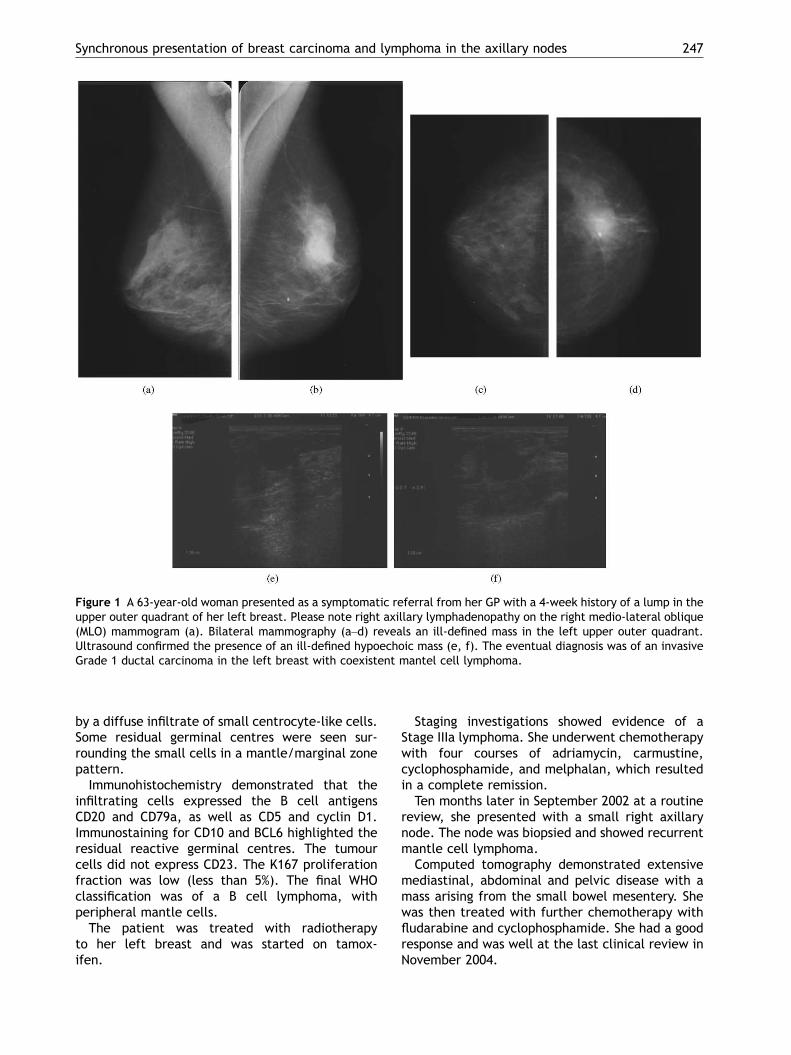
A 50-year-old woman was recalled from theincident screening round in 2003 for furtherassessment of a 1.8-cm spiculated mass in theupper outer quadrant of her left breast. Lympha-denopathy within the left axilla was also noted onthe screening mammograms.
At assessment, an ultrasound of the left breastdemonstrated a 1.5-cm hypoechoic lesion alongwith numerous enlarged pathological axillary lymphnodes (Fig. 2).
Figure 2 Bilateral mammography and ultrasound (a–f) of around for further assessment of a 1.8-cm spiculated massLymphadenopathy within the left axilla was also noted on the(e, f) demonstrated a 1.5-cm hypoechoic lesion along withdiagnosis was a 14-mm Grade 1 ductal carcinoma, which sho
FNA cytology of the breast lesion produced amalignant result (C5), and an FNA of the largest leftaxillary node yielded cells with suspected malig-nancy (C4).
A guide wire wide local excision of the breastlesion was performed with axillary node sampling.The histology of the breast lesion showed a 14-mmGrade 1 invasive ductal carcinoma, which wascompletely excised. The tumour was oestrogenand progesterone receptor positive. The Notting-ham Prognostic Index for this patient’s breastcarcinoma was 2.3 (excellent prognostic result).
50-year-old woman recalled from the incident screeningin the left upper outer quadrant of her left breast.
screening mammograms (b). Ultrasound of the left breastnumerous enlarged axillary lymph nodes. The eventualwed evidence of a low-grade B cell follicular lymphoma.
ARTICLE IN PRESS
Synchronous presentation of breast carcinoma and lymphoma in the axillary nodes 249
None of the nine lymph nodes contained meta-static carcinoma, but there was evidence of a low-grade B cell follicular lymphoma (Grade 1) in theaxillary nodes.
Further immunohistochemical staining revealedthe lymphoma to be positive for CD20 and CD79a,and negative for CD3. The tumour was positive forthe follicular cell-associated antigens CD10 andBCL6. Immunostaining for CD23 revealed thefollicular dendritic cell networks supporting thetumour and the lymphoma cells also to be positivefor this antigen. The tumour was also positive forthe BCL2 protein. CD5 and cyclin D1 were negative.The WHO classification was that of B cell type non-Hodgkin’s lymphoma (NHL), mature, follicular (allfollicular, Grade 1).
She underwent radiotherapy to the left breastand was started on tamoxifen (20mg daily).
A staging CT examination was performed toassess the extent of the lymphoma, and low-volumelymphadenopathy was demonstrated in the rightaxilla, and both the iliac and inguinal regions(stage IIIa.) She was treated with six courses ofchlorambucil and dexamethasone, and has re-mained well from both diseases up to the presentdate.
Case 3
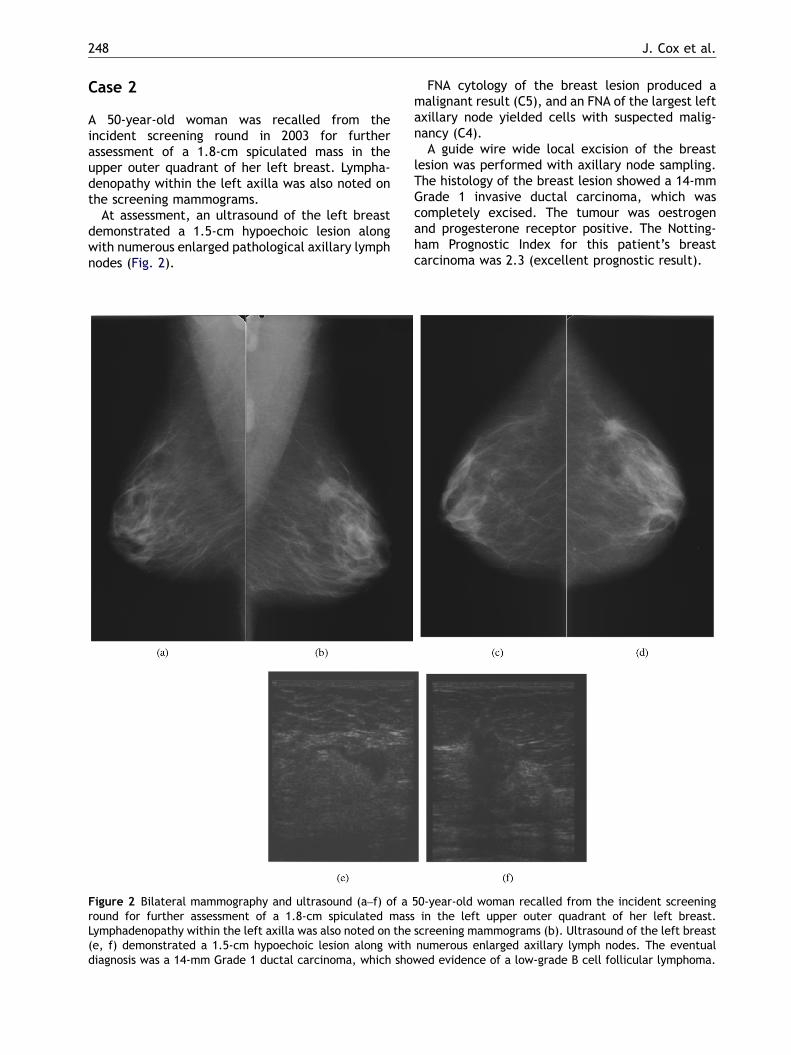
A 58-year-old was recalled from the prevalentscreening round for further assessment of a smallcluster of microcalcification in the upper outerquadrant of her left breast in 1991. On furthermammography and ultrasound examination en-larged left axillary lymph nodes were noted (Fig.3). FNA of the area under stereotactic guidance hadyielded an inadequate result. A guide wire wastherefore inserted into the microcalfication toobtain a diagnosis, as was the practice at thattime. The excised specimen revealed ductal carci-noma in situ of the comedo type. The patientelected to have a left mastectomy, which showedno evidence of residual disease, but 12 abnormalaxillary lymph nodes showed infiltration by low-grade follicular NHL, of centroblastic–centrocytictype, with no evidence of metastatic breastcarcinoma. Staging investigations were performedand were normal, indicating that the disease waslocalised, stage Ia. She was referred to the care ofa haematologist at a hospital closer to her home forsurveillance.
In 1994, 3 years after the original diagnosis, shewas again recalled from her annual follow-upmammography, because of the development of an
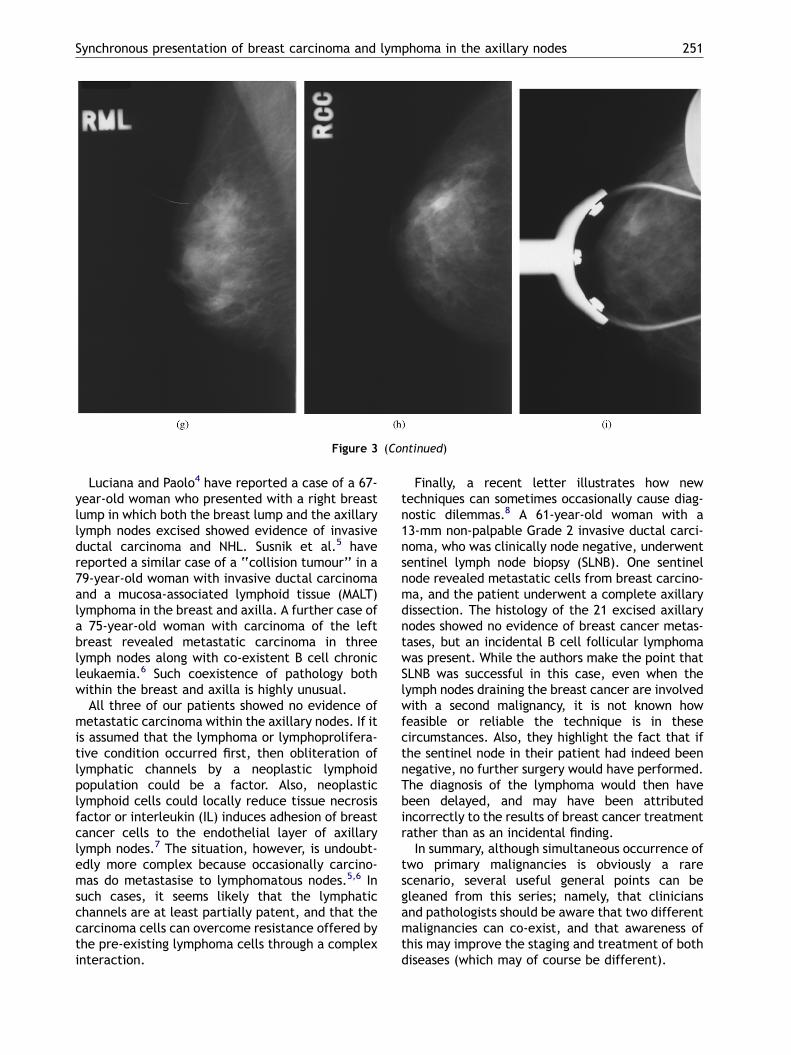
asymmetric density in the lower outer quadrant ofher right breast (Fig. 3g–i.)
On ultrasound a 5-mm hypoechoic lesion wasvisible in this area. FNA was inconclusive, and asecond guide wire excision biopsy revealed recur-rence of a low-grade lymphomatous process,similar to that in the left axilla in 1991. Therewas no evidence of disseminated disease clinically.
She was observed until 1996, when anotherabnormality was demonstrated on surveillancemammography in the right breast. This againproved to be recurrent lymphoma. She again hadno systemic treatment and was observed until2002, when she was discharged from haematologi-cal follow-up. She remains well to date.
This interesting (and stoical) patient illustratesthe fascinating (and previously unreported) phe-nomenon of axillary lymphoma recurring in thecontralateral breast after mastectomy. This ap-pears to have been her only site of recurrence over14 years and was managed by local excision.
Discussion
It is well documented that patients who have hadbreast carcinoma and have undergone adjuvantradiotherapy and chemotherapy are at increasedrisk of developing second malignancies. Also, it isknown that patients treated with mantle radio-therapy for lymphoma are at increased risk ofbreast cancer. This sequence of events, however,usually involves an interval of several years.
Synchronous malignancies (i.e., tumours diag-nosed within a 6-month period) in which theinfluence of therapy is a predisposing factor areuncommon. In an autopsy study1 of 68 patients withmultiple malignancies in 1870 cancer deaths, only15 (0.8%) of the total had multiple synchronousprimaries. The association of breast cancer (thesecond commonest primary tumour in the series)with another primary tumour was the lowest.
Synchronous presentation of breast carcinomawith axillary lymphoma is an exceedingly rarephenomenon; only one small series of patients haspreviously been documented in the literature.2
A number of cases reports have documentedbroadly similar presentations. One case of anincidental finding of Stage 1 mantle cell lymphomain an axillary lymph node has been reported in a 67-year-old women who self-referred for breastscreening. She had a 10-mm Grade 2 ductalcarcinoma diagnosed and excised from her leftbreast. Evidence of mantle cell lymphoma wasdetected in all four of the sampled left axillary

ARTICLE IN PRESS
J. Cox et al.250
lymph nodes, which showed no evidence of meta-static breast carcinoma.3
Due to the early stage of her disease, sheunderwent no specific lymphoma treatment, and
Figure 3 Bilateral mammography (a–d), extended craniocaudyear-old recalled from the prevalent screening round for asseupper outer quadrant. Mammography and ultrasound examnodes. The eventual diagnosis was ductal carcinoma in situlow-grade non-Hodgkin’s mixed cell lymphoma in the axillarypatient elected to have a mastectomy) in 1994 (g–i) revealerevealed recurrent low-grade NHL. Another recurrence in th
given the case has only very recently been reportedit is too early to state whether she, like our twopatients above (Cases 1 and 3), will develop diseaserecurrence.
al view (e) and magnification views (f) performed on a 58-ssment of a small cluster of microcalcification in the leftination demonstrated enlarged bilateral axillary lymphof comedo type with malignant microcalcification with anodes. Mammography of the remaining right breast (thed a small mass in the right lower outer quadrant. Biopsye right breast occurred in 1996.
ARTICLE IN PRESS
Figure 3 (Continued)
Synchronous presentation of breast carcinoma and lymphoma in the axillary nodes 251
Luciana and Paolo4 have reported a case of a 67-year-old woman who presented with a right breastlump in which both the breast lump and the axillarylymph nodes excised showed evidence of invasiveductal carcinoma and NHL. Susnik et al.5 havereported a similar case of a ‘‘collision tumour’’ in a79-year-old woman with invasive ductal carcinomaand a mucosa-associated lymphoid tissue (MALT)lymphoma in the breast and axilla. A further case ofa 75-year-old woman with carcinoma of the leftbreast revealed metastatic carcinoma in threelymph nodes along with co-existent B cell chronicleukaemia.6 Such coexistence of pathology bothwithin the breast and axilla is highly unusual.
All three of our patients showed no evidence ofmetastatic carcinoma within the axillary nodes. If itis assumed that the lymphoma or lymphoprolifera-tive condition occurred first, then obliteration oflymphatic channels by a neoplastic lymphoidpopulation could be a factor. Also, neoplasticlymphoid cells could locally reduce tissue necrosisfactor or interleukin (IL) induces adhesion of breastcancer cells to the endothelial layer of axillarylymph nodes.7 The situation, however, is undoubt-edly more complex because occasionally carcino-mas do metastasise to lymphomatous nodes.5,6 Insuch cases, it seems likely that the lymphaticchannels are at least partially patent, and that thecarcinoma cells can overcome resistance offered bythe pre-existing lymphoma cells through a complexinteraction.
Finally, a recent letter illustrates how newtechniques can sometimes occasionally cause diag-nostic dilemmas.8 A 61-year-old woman with a13-mm non-palpable Grade 2 invasive ductal carci-noma, who was clinically node negative, underwentsentinel lymph node biopsy (SLNB). One sentinelnode revealed metastatic cells from breast carcino-ma, and the patient underwent a complete axillarydissection. The histology of the 21 excised axillarynodes showed no evidence of breast cancer metas-tases, but an incidental B cell follicular lymphomawas present. While the authors make the point thatSLNB was successful in this case, even when thelymph nodes draining the breast cancer are involvedwith a second malignancy, it is not known howfeasible or reliable the technique is in thesecircumstances. Also, they highlight the fact that ifthe sentinel node in their patient had indeed beennegative, no further surgery would have performed.The diagnosis of the lymphoma would then havebeen delayed, and may have been attributedincorrectly to the results of breast cancer treatmentrather than as an incidental finding.
In summary, although simultaneous occurrence oftwo primary malignancies is obviously a rarescenario, several useful general points can begleaned from this series; namely, that cliniciansand pathologists should be aware that two differentmalignancies can co-exist, and that awareness ofthis may improve the staging and treatment of bothdiseases (which may of course be different).

ARTICLE IN PRESS
J. Cox et al.252
Numerous enlarged axillary lymph nodes,whether clinically evident or present on imaging,should be treated with caution, particularly inpatients with small breast cancers. Such lympha-denopathy does not inevitably indicate metastaticdisease. Biopsy of both the primary breast tumourand the axillary disease may be required in thesecircumstances to clarify the diagnosis, particularlybefore neoadjuvant chemotherapy.
Also, when recurrence of a malignancy occurs inthe context of synchronous primaries, as happenedin Cases 1 and 3 in our series, it is vital to make thecorrect diagnosis as to which disease process hasrecurred in order to tailor further management.
References
1. Lee TK, Myers RT, Scharyj M, Marshall RB. Multiple primarymalignant tumors (MPMT): study of 68 autopsy cases(1963–1980). J Am Geriatr Soc 1982;30:744–53.
2. Frey BM, Morant R, Senn HJ, Fisch T, Schid U. Simultaneousoccurence of breast carcinoma and malignant lymphoma.Case observations and literature review. Schweiz MedWochenschr 1994;124(23):1010–6.
3. Roy SD, Stafford JA, Scally J, Selvachandran SN. A rare case ofbreast carcinoma coexisting with axillary mantle cell lym-phoma. World J Surg Oncol 2003;1:27.
4. Luciana S, Paolo E. Breast carcinoma metastatic to lympho-ma: a report of a case with review of the literature.Histopathology 1999;34(1):87.
5. Susnik B, Rowe JJM, Redlich PN, Chitambar C, et al. A uniquecollision tumour within the breast: invasive ductal carcinomaand mucosa-associated lymphoid tissue lymphoma. ArchPathol Lab Med 2004;128(1):99–101.
6. Pandey U, Maraynan M, Karnik U, Sinha B. Carcinomametastasis to unexpected synchronous lymphoproliferativedisorder: report of three cases and review of the literature.J Clin Pathol 2003;56:970–1.
7. Mannel DN, Orosz P, Hafner M, Falk W. Mechanisms involved inmetastasis enhanced by inflammatory mediators. Circ Shock1994;1:9–13.
8. Barranger E, Marpeau O, Uzan S. Axillary sentinel nodeinvolvement by breast cancer coexisting with B-cellfollicular lymphoma in nonsentinel nodes. Breast 2005;J11(3):227–8.



















![Annals of Clinical Case Reports Case Report · epithelium are found in axillary lymph nodes [14,15]. Ectopic thyroid tissueis found occasionally in cervical lymph nodes. Among nonepithelial](https://img.pdfslide.net/doc/110x75/5f1cd159d6b56138e82777d7/annals-of-clinical-case-reports-case-epithelium-are-found-in-axillary-lymph-nodes.jpg)








