Embed Size (px)
Citation preview

I Med Genet 1995;32:39-43
Syndrome of the month
Cartilage-hair hypoplasia
0 Makitie, T Sulisalo, A de la Chapelle, I Kaitila
Cartilage-hair hypoplasia (CHH) or McKusicktype metaphyseal chondrodysplasia (MIM No250250)' is a rare autosomal recessive chon-drodysplasia with short limbed short stature,hypoplastic hair, and defective immunity anderythrogenesis.2' The major radiological ab-normalities are confined to the metaphysealregions of the tubular bones.67 The disease isprevalent among the Old Order Amish in theUnited States and in the Finnish population.28While genealogical data confirm autosomal re-cessive inheritance, segregation analysis showsa lack of affected persons among both theAmish and Finnish CHH families; this has beeninterpreted as a possible example of reducedpenetrance.28 The CHH gene was recently as-signed to chromosome 9 by linkage analysis,9and its localisation refined.'0 This has allowedprenatal diagnosis in four cases. IOA
Department ofMedical Genetics,Helsinki UniversityHospital,Haartmaninkatu 2B,SF-00290 Helsinki,FinlandO MakitieI Kaitila
Children's Hospital,Helsinki UniversityHospital, 00290Helsinki, FinlandO Makitie
Department ofMedical Genetics,PO Box 21, 00014University of Helsinki,FinlandT SulisaloA de la ChapelleI Kaitila
Folkhiilsan Institute ofGenetics, 00250Helsinki, FinlandT SulisaloA de la Chapelle
Correspondence to:Dr Kaitila.
Clinical descriptionGROWTH FAILUREThe growth failure has its onset prenatally;the shortness of limbs or stature or both wasnoticed neonatally in 76% and by the age ofyear in 98% of 108 Finnish CHH patients."All segments of the limbs are affected. Thegrowth failure is progressive, owing in part to aweak or absent pubertal growth spurt; pubertalmaturation is normal. Adult heights range from103-7 cm to 149-0 cm with medians of131 1 cm for males and 122 5 cm for females. 1
The growth failure is disproportionate witha long trunk in relation to the short limbs. Themore severe the growth failure, the greater thedisproportion." Proportionate short stature hasbeen described in some CHH patients."213Median relative weight is above the normal
mean in childhood and is further augmentedaround puberty; most adult patients are clin-ically obese. The head circumference is closeto normal at all ages."
OTHER CLINICAL FEATURESThe majority of affected persons have sparse,
fine, and silky hair; the eyebrows, eyelashes,and body hair are similarly affected. In some
patients, however, the hair appears normal.This was observed in 7% of the Finnish CHHpatients.'
Other clinical features include laxity of lig-aments, limited extension of the elbows, in-creased lumbar lordosis, bowing of the lower
limbs, chest deformity (narrow thorax, Har-rison's grooves, prominent sternum, or asym-metry), and mild scoliosis (figs 1 and 2).'
IMMUNE DEFICIENCYThe defective cellular immunity is char-acterised by mild to moderate lymphopenia,decreased delayed hypersensitivity, and im-paired in vitro responsiveness of lymphocytesto PHA; humoral immunity is usuallyintact.""" A few patients with normalimmunity" 1 or combined immuno-deficiency"7-2 have been reported. Defectivecellular immunity results in suscepti-bility to and mortality from infections. Theinfection problems are most pronounced inearly childhood but occasionally persist to adultage. Varicella infection has been fatal in a fewcases. In the Finnish series impaired in vitrocellular immunity was observed in 88% of thepatients.' Fifty-six percent had been unusuallyprone to infections. Six patients (6%) had diedof primary infections. On the other hand, 44%of the patients had shown no unusual sus-ceptibility to infections even though deficientcellular immunity had been confirmed in halfof them.'The incidence of malignancies is increased
as observed in the Finnish series' and casesdescribed earlier.22-24 Francomano et al2' re-ported an incidence of 10% of malignancies in113 Amish CHH patients: lymphoma in threepatients, leukaemia in two, skin neoplasms infive, ocular cancer in one, and bile duct car-cinoma in one patient.2' Among the Finnishpatients the incidence was six out of 108patients (6%): skin neoplasms in three patients,lymphoma in one, lymphosarcoma in one, andtesticular tumour in one patient.'
ANAEMIADeficient erythrocyte production presents usu-ally as mild macrocytic anaemia in early child-hood with spontaneous recovery beforeadulthood.26 Occasionally, however, thepatients have severe, even fatal, congenital hy-poplastic anaemia.4 132'2325-27 Sixty-seven out of85 Finnish patients (79%) had been anaemicduring childhood; in 14 patients (16%) theanaemia had been severe (lowest haemoglobinvalue 30-75 g/l) with a fatal course in sixpatients.5
39
on May 11, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.32.1.39 on 1 January 1995. Dow
nloaded from

Makitie, Sulisalo, de la Chapelle, Kaitila
.X..X...r X~~..4 .....
i i! @
:':..A'......e...tWW;5Nfijff ; gfiff;fffffffg;; j2gffff ; gaffgfff ff;~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~..........
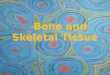
Figure I Six CHH patients, front view. Age and absolute and relative values of height (from left to right): (1) 3 6years, 74 5cm (-68 SD); (2) 35 years, 84-3cm (-41 SD); (3) 55 years, 94 8cm (-41 SD) (4) 105 years,113 2cm (-4-7SD); (5) 15-2years, 123-9cm (-6 1 SD); (6) 28-7years, 134-2cm (-5-8SD).
INTESTINAL MANIFESTATIONSThere have been several descriptions of CHHpatients with congenital megacolon (Hirsch-sprung's disease) 2416212228-31 The Finnishseries included eight patients (7%) with con-genital megacolon.5 These cases clearly indicateincreased prevalence of Hirschsprung's diseaseamong CHH patients.
Intestinal malabsorption was suspected in sixAmish patients who had diarrhoea and failureto thrive in the first two years of life.2 However,primary malabsorption was not observed in anyof the 108 Finnish CHH patients; instead,gastrointestinal infection was confirmed in twopatients with symptoms suggesting mal-absorption.5 These and other reported cases3233suggest that primary malabsorption is only ex-ceptionally associated with CHH; mimickingsymptoms may reflect an underlying gastro-intestinal infection.
ORTHOPAEDIC PROBLEMS
Orthopaedic problems in CHH are rare com-
pared with many other chondrodysplasias. Lig-amentous laxity and increased lumbar lordosismay cause arthralgic pains in the knees, ankles,or lumbar region of the spine. Bow legs maynecessitate corrective osteotomy (in 14% of theFinnish patients).'
Radiographic featuresThe tubular bones are short for age and theirmetaphyseal ends are flared, scalloped, andirregularly sclerotic, often with cystic areas (fig3); the epiphyses are less affected.67 The meta-physeal changes are most pronounced in theknees and ankles; the hips are only mildlyaffected (fig 4). The metaphyseal irregularitiesdisappear after the closure of the epiphysealplates but the ends remain somewhat flaredand angulated. The spine shows only minorabnormalities: the vertebral bodies are usuallynormal and caudal widening of the inter-pediculate distances, though less obvious thannormal, is present in most patients (fig 5).Lumbar lordosis is increased and further ac-
'U.K~~~~~~~1
ME E,1|W,|
AF_Se.tlM
|--. F I _ _ 1_F l:NNEW
liSS|C~~~~~~~-.MmWg ~aal_;:lm
Figure 2 Six CHH patients, side view. Same patients as in fig 1. Note the variation in the degree of disproportion, hairhypoplasia, lumbar lordosis, and chest deformity.
40
on May 11, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.32.1.39 on 1 January 1995. Dow
nloaded from

Cartilage-hair hypoplasia
Figure 3 Radiograph of the legs of a 9 year old boy. Themetaphyseal ends are flared and irregularly sclerotic. Notethe excessive distal length of the fibula.
Figure 4 Radiograph of the hips of a 9 year old boy(same patient as in fig 3) showing only mild metaphysealinvolvement in the proximal femora.
Figure 5 Constant interpediculate distances of 17mm atthe levels offirst, third, and fifth lumbar vertebrae. Themoderate lumbar lordosis (520) is accentuated by ahorizontally tilted sacrum (male, 9 5 years).
centuated by a horizontally tilted sacrum (fig5).7
Differential diagnosisMost of the 150 different osteochondro-dysplasias result in disproportionate short stat-ure and progressive problems in the joints andspine. The clinical features of CHH resemblethose of hypochondroplasia (MIM 14600)1which, however, is a dominantly inherited con-dition and does not present with abnormal hair.It is easily differentiated from CHH by normalmetaphyses in childhood skeletal radiographs.Murk Jansen (MIM 156400) and Schmid(MIM 156500) metaphyseal dysplasias aredominantly inherited conditions and result insevere growth failure but patients have normalimmunity and erythrogenesis; these are easilydistinguished from CHH. Recently, a type Xcollagen mutation was reported as the cause ofSchmid chondrodysplasia.34 Shwachman-Bod-ian syndrome (MIM 260400), an autosomalrecessive condition with metaphyseal in-volvement, is associated with pancreatic in-sufficiency, malabsorption, and leucopenia; themild skeletal changes are most evident in theproximal femora.
EpidemiologyCHH was originally described among the OldOrder Amish, a religious isolate in the UnitedStates.2 At least 113 Amish CHH patients havebeen recognised25; the incidence is estimatedat 1-2: 1000 corresponding to a carrier fre-quency of 1:10.2 Another accumulation of thedisease has been observed among Finns with120 patients in a population of 5 million; theincidence is estimated at 1:23 000 live birthsand the carrier frequency at 1 :76.8 The numberof diagnosed patients among other populationsis low: 13 patients have been reported amongthe French, eight among the Dutch, sevenamong the British, and sporadic cases amongthe Germans, Danes, Algerians, Italians, Pol-ish, Spanish, and Mexicans.35 Whether this isbecause of underdiagnosis, under-reporting, orlow incidence cannot be determined with cer-tainty.
Mapping of the gene for CHH by linkageand linkage disequilibrium analysisAssignment of the CHH gene to the proximalpart of 9p was accomplished by a randomsearch for linkage in 14 Finnish families.9 Sub-sequently, linkage to the same locus was shownin a large series of Amish families.'0 No signsof heterogeneity within or between the twopopulations were detected.As there were no recombinations within the
highly polymorphic marker D9S 163 (lod score26-30 at 0=0) CHH could be placed in thevicinity ofD9S 163 in the 4 cM interval betweenmarkers D9S 165 and D9S50. As both theFinnish and Amish populations had few found-ers and have remained highly isolated, it couldbe assumed that the number of ancestral mut-ations would be small, possibly with a single
41
on May 11, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.32.1.39 on 1 January 1995. Dow
nloaded from

Mdkitie, Sulisalo, de la Chapelle, Kaitila
mutation accounting for the majority of thepatients in each population. Haplotype analysesand linkage disequilibrium studies confirmedthis assumption.'0 Moreover, the strength oflinkage disequilibrium was used to assess thedistance between D9S163 and CHH by a re-cently developed method.36-3' The current bestestimate of this distance is 0-3 cM.39
Genetics and penetranceGenetic studies among Amish and Finnish fam-ilies have confirmed the recessive mode of in-heritance in CHH.28 However, segregationanalyses showed a slightly lower number ofaffected members than expected according tothe recessive hypothesis. This has been ex-plained by reduced penetrance or by the lossof affected children in utero or in infancy.2835The mapping of CHH and availability of
closely linked polymorphic markers provide atool to examine the question of penetrance. Ifreduced penetrance were responsible for theunexpectedly low proportion of affected chil-dren in CHH sibships, healthy persons withhaplotypes identical to their affected sibs shouldbe found. Such a phenomenon was looked forin a total of 66 unaffected sibs but was not
found.910 This finding is indeed credible as
reduced penetrance appears to be very rare inrecessively inherited disorders. Several othermechanisms might account for the observedunder-representation of affected children,40which is more pronounced in the Amish2 thanin the Finnish series.8 The haplotype analysesdone in unaffected sibs appear to exclude not
only reduced penetrance, but also geneticheterogeneity.910 Remaining explanations are
uniparental disomy, monosomy owing to de-letion, biased ascertainment of families, earlylethality in a fraction ofhomozygotes, and gam-etic selection.
Prenatal diagnosisAs CHH may in some cases be severe or even
fatal, some families with an affected child haverequested prenatal testing for CHH. The pre-cise mapping of the CHH gene with respectto several highly polymorphic DNA markersprovides an excellent opportunity for accurate
predictive testing based on the segregation ofthose markers in families with a previous historyof CHH. Four prenatal determinations haveso far been done; in three cases the fetus was
predicted to be unaffected, and in one case an
affected fetus was predicted.l"A In all cases theoutcome was as predicted.
Hypotheses regarding the pathogenesisThe pathogenesis of the disorder remains un-
known. However, since previous studies haveestablished defective cellular proliferation ofT and B lymphocytes and fibroblasts,4 anddefective erythrogenesis,26 it is suggested thatthe clinical manifestations (growth failure,sparse hair, recurrent infections, anaemia,Hirschsprung's disease) in CHH may resultfrom a generalised defect of cellular pro-liferation. It is intriguing to note that a gene
causing isolated Hirschsprung's disease locatedon chromosome 10 has recently beencloned.4 42 It follows that one of the pleiotropiceffects of the CHH gene, Hirschsprung's dis-ease, arises either by a different mechanismfrom that in the isolated form of the disease, or
by the interaction of the two genes. Additionalstudies are needed to elucidate further the mo-lecular mechanisms in the pathogenesis ofCHH. The solution will probably have to awaitthe cloning and characterisation of the geneitself.
These studies have been supported by the Academy of Finland,the Sigrid Juselius Foundation, the March of Dimes BirthDefects Foundation, the Human Growth Foundation, the Pai-vikki and Sakari Sohlberg Foundation, the Finnish MedicalFoundation, the University of Helsinki, and the Foundation forPaediatric Research.
1 McKusick VA. Mendelian inheritance in nman. Baltimore:Johns Hopkins University Press, 1991.
2 McKusick VA, Eldrige R, Hostetler JA, Ruangwit U, Ege-land JA. Dwarfism in the Amish. II. Cartilage-hair hy-poplasia. Bull johns Hopkins Hosp 1965;116:285-326.
3 Virolainen M, Savilahti E, Kaitila I, Perheentupa J. Cellularand humoral immunity in cartilage-hair hypoplasia. PediatrRes 1978;12:961-6.
4 Polmar SH, Pierce GF. Cartilage hair hypoplasia: im-munological aspects and their clinical implications. ClinImmunol Immunopathol 1986;40:87-93.
5 Makitie 0, Kaitila I. Cartilage-hair hypoplasia clinicalmanifestations in 108 Finnish patients. Eur3rPediatr 1993;152:211-7.
6 Ray HC, Dorst JP. Cartilage-hair hypoplasia. Prog PediatrRadiol 1973;4:270-98.
7 Makitie 0, Marttinen E, Kaitila I. Skeletal growth in car-
tilage-hair hypoplasia - a radiological study of 82 patients.Pediatr Radiol 1992;22:434-9.
8 Makitie 0. Cartilage-hair hypoplasia in Finland: epi-demiological and genetic aspects of 107 patients. _7 MedGenet 1992;29:652-5.
9 Sulisalo T, Sistonen P, Hastbacka J, et al. Cartilage-hairhypoplasia gene assigned to chromosome 9 by linkageanalysis. Nature Genet 1993;3:338-41.
10 Sulisalo T, Francomano CA, Sistonen P, et al. High res-
olution genetic mapping of the cartilage-hair hypoplasiagene in Amish and Finnish families. Genomics 1994;20:347-53.
IOA Sulisalo T, Sillence D, Wilson M, Ryynanen M, Kaitila I.Early prenatal diagnosis of cartilage-hair hypoplasia(CHH) with polymorphic DNA markers. PrenatDiagn (inpress).
11 Makitie 0, Perheentupa J, Kaitila I. Growth in cartilage-hair hypoplasia. Pediatr Res 1992;31:176-80.
12 Savage MO. Metaphyseal dysplasia in siblings: A variant ofcartilage-hair hypoplasia (case report). Proc R Soc Med1 972;65:727.
13 Van der Burgt I, Haraldsson A, Oosterwijk JC, van EssenAJ, Weemaes C, Hamel B. Cartilage hair hypoplasia,metaphyseal chondrodysplasia type McKusick: de-scription of seven patients and review of the literature.AmJMed Genet 1991;41:371-80.
14 Trojak JE, Polmar SH, Winkelstein JA, et al. Immunologicstudies of cartilage-hair hypoplasia in the Amish. JohnsHopkins MedJ7 1981;148:157-64.
15 Ranki A, Perheentupa J, Andersson LC, Hayry P. In vitroT- and B-cell reactivity in cartilage hair hypoplasia. ClinExp Immunol 1978;32:352-60.
16 Lischka A, Frisch H, Weissenbacher G. Radiologische Ver-anderungen bei metaphysarer Chondrodystrophie TypMcKusick (Knorpel-Haar-Hypoplasie). Monatsschr Kin-derheilkd 1984;132:550-3.
17 Ammann AJ, Sutliff W, Millinchick E. Antibody-mediatedimmunodeficiency in short-limbed dwarfism. _7 Pediatr1 974;84:200-3.
18 Rubie H, Graber D, Fischer A, et al. Hypoplasie du cartilageet des cheveux avec deficit immunitaire combine. AnnPediatr (Paris) 1989;36:390-2.
19 Saulsbury FT, Winkelstein JA, Davis LE, et al. Combinedimmunodeficiency and vaccine-related poliomyelitis in a
child with cartilage-hair hypoplasia. _7 Pediatr 1975;86:868-72.
20 Steele RW, Britton HA, Anderson CT, Kniker WT. Severecombined immunodeficiency with cartilage-hair hy-poplasia: in vitro response to thymosin and attemptedreconstitution. Pediatr Res 1 976;1O: 1003-55.
21 Wilson WG, Aylsworth AS, Folds JD, Whisnant JK. Car-tilage-hair hypoplasia (metaphyseal chondrodysplasia,type McKusick) with combined immune deficiency: vari-able expression and development of immunologic func-tions in sibs. Birth Defects 1978;14:117-29.
22 Harris RE, Baehner RL, Gleiser S, Weaver DD, Hodes ME.Cartilage-hair hypoplasia, defective T-cell function, andDiamond-Blackfan anemia in an Amish child. Am _7 MedGenet 1981;8:291-7.
23 Hensley MF. McKusick's dwarfism and resistant Hodgkin'sdisease (letter). JAm Osteopath Assoc 1984;84:159.
42
on May 11, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.32.1.39 on 1 January 1995. Dow
nloaded from

Cartilage-hair hypoplasia
24 Roberts MA, Arnold RM. Hodgkin's lymphoma in a childwith cartilage-hair hypoplasia (case report). Milit Med1984;149:280-1.
25 Francomano CA, Trojak JE, McKusick VA. Cartilage-hairhypoplasia in the Amish: increased susceptibility to malig-nancy (abstract). Am J7 Hum Genet 1983;35:89A.
26 Makitie 0, Rajantie J, Kaitila I. Anaemia and macrocytosis- unrecognized features in cartilage-hair hypoplasia. ActaPaediatr 1992;81:1030-4.
27 Sacrez R, Levy JM, Godar G, Castanier J. Anemie deBlackfan-Diamond associe a des malformations multiples.Med Infantile 1965;72:493-9.
28 Roberts PAL, Mann TP, Rubin J. Hirschsprung's diseaseassociated with a variant form of achondroplasia, in sisterand brother (case report). Proc R Soc Med 1969;62:329.
29 Fauchier C, Regy JM, Combe P. Nanisme diastrophiquefamilial avec maladie de Hirschsprung. Ann Pediatr (Paris)1969;16:496-502.
30 Boothby CB, Bower BD. Cartilage hair hypoplasia. ArchDis Child 1973;48:919-21.
31 Le Merrer M, Briard ML, Chauvet ML, Maroteaux P.Autosomal recessive metaphyseal chondrodysplasia andHirschsprung's disease. Ann Pediatr (Paris) 1991;38:27-30.
32 Wood DJ, David TJ, Chrystie LL, Totterdell B. Chronicenteric virus infection in two T-cell immunodeficient chil-dren. JMed Virol 1988;24:435-44.
33 Lux SE, Johnston RB, August CS, et al. Chronic neutropeniaand abnormal cellular immunity in cartilage-hair hypo-plasia. N Engl _J Med 1970;282:231-6.
34 Warman ML, Abbot M, Apte SS, et al. A type X collagenmutation causes Schmid metaphyseal chondrodysplasia.Nature Genet 1993;5:79-82.
35 Makitie 0. Cartilage-hair hypoplasia. Clinical, radiologicaland genetic study of an inherited skeletal dysplasia. Thesis,University of Helsinki, 1992.
36 Luria SE, Delbruck M. Mutations of bacteria from virussensitivity to virus resistance. Genetics 1943;28:491-511.
37 Hastbacka J, de la Chapelle A, Kaitila I, Sistonen P, WeaverA, Lander E. Linkage disequilibrium mapping in isolatedpopulations: diastrophic dysplasia in Finland. Nature Genet1992;2:204-1 1.
38 Lehesjoki AE, Koskiniemi M, Norio R, et al. Localizationof the EPM1 gene for progressive myoclonus epilepsyon chromosome 21: linkage disequilibrium allows highresolution mapping. Hum Molec Genet 1993;2: 1229-34.
39 Sulisalo T, Klockars J, Makitie, 0, Francomano CA, de laChapelle A, Kaitila I. High-resolution linkage-dis-equilibrium mapping of the cartilage-hair hypoplasia gene.Am3JHum Genet 1994;55:937-45.
40 Bundey S, Young ID. Low segregation ratios in autosomalrecessive disorders. Med Genet 1993;30:449-5 1.
41 Romeo G, Ronchotto P, Luo Y, et al. Point mutationsaffecting the tyrosine kinase domain of the RET proto-oncogene in Hirschsprung's disease. Nature 1994;367:377-8.
42 Edery P, Lyonnet S, Mulligan LM, et al. Mutations of theRET proto-oncogene in Hirschsprung's disease. Nature1994;367:378-80.
43
on May 11, 2021 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.32.1.39 on 1 January 1995. Dow
nloaded from