Embed Size (px)
Citation preview
Synopsis of Management on Ventricular arrhythmias
M. Soni MD
Interventional Cardiologist
No financial disclosure
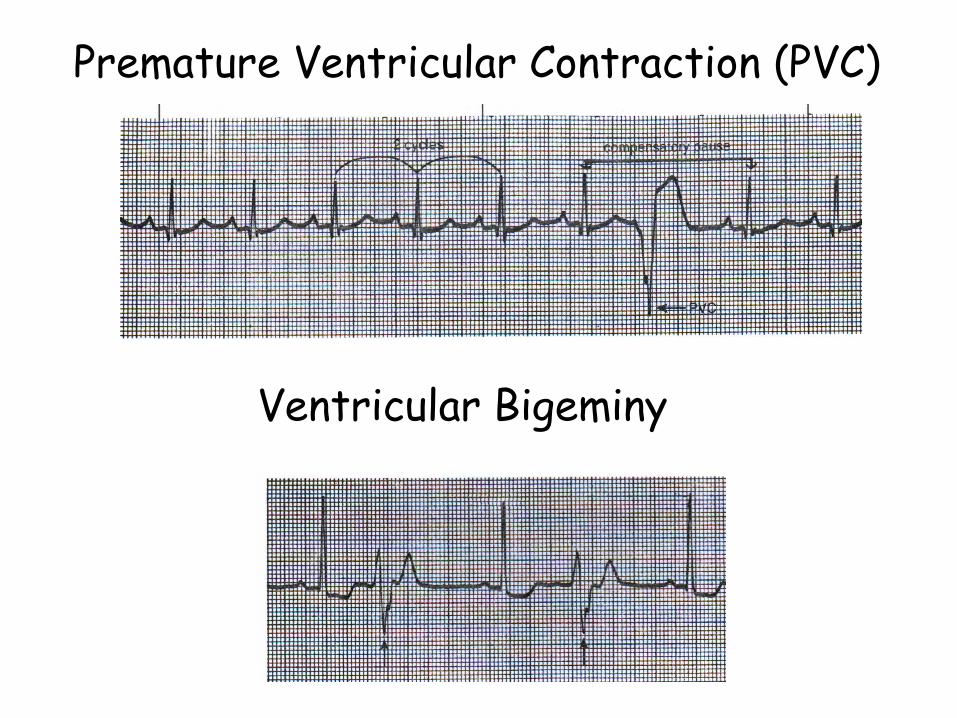
Premature Ventricular Contraction (PVC)
Ventricular Bigeminy
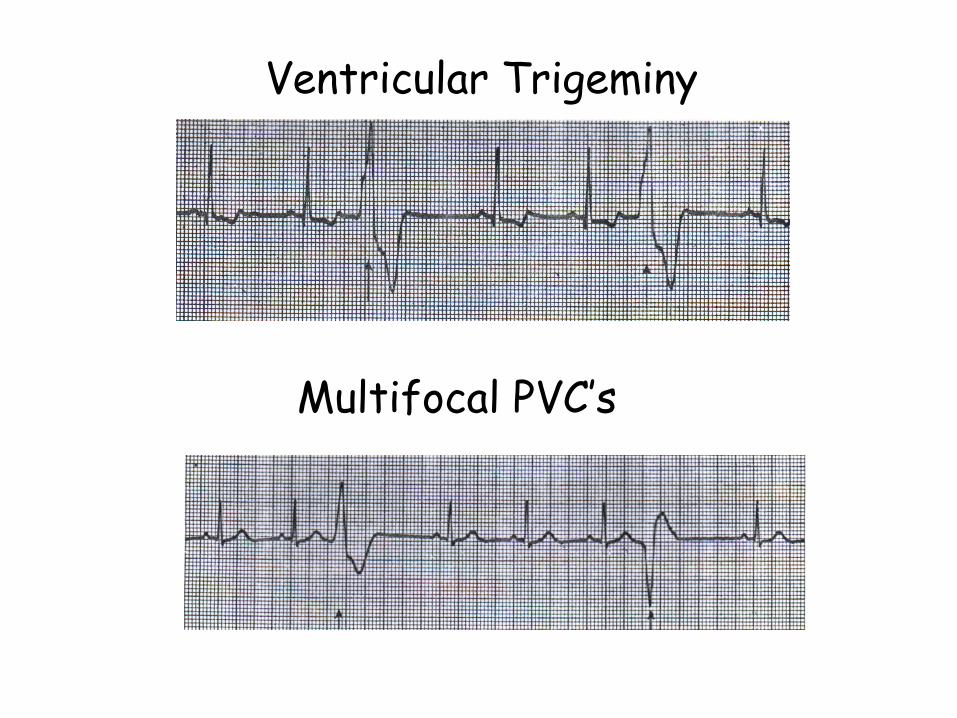
Ventricular Trigeminy
Multifocal PVC’s
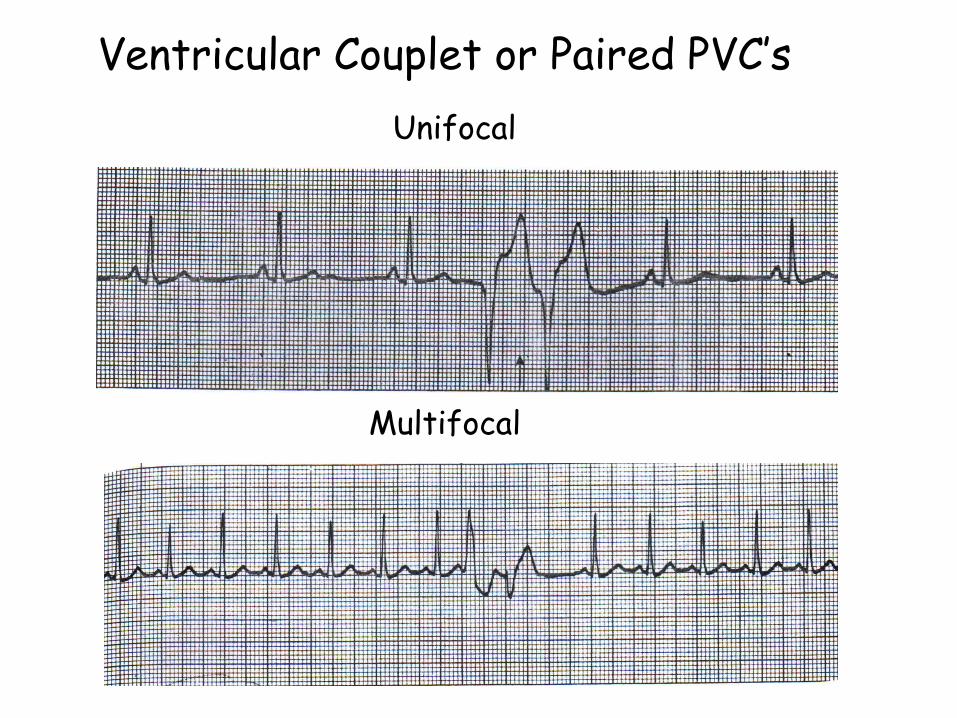
Ventricular Couplet or Paired PVC’s
Multifocal
Unifocal
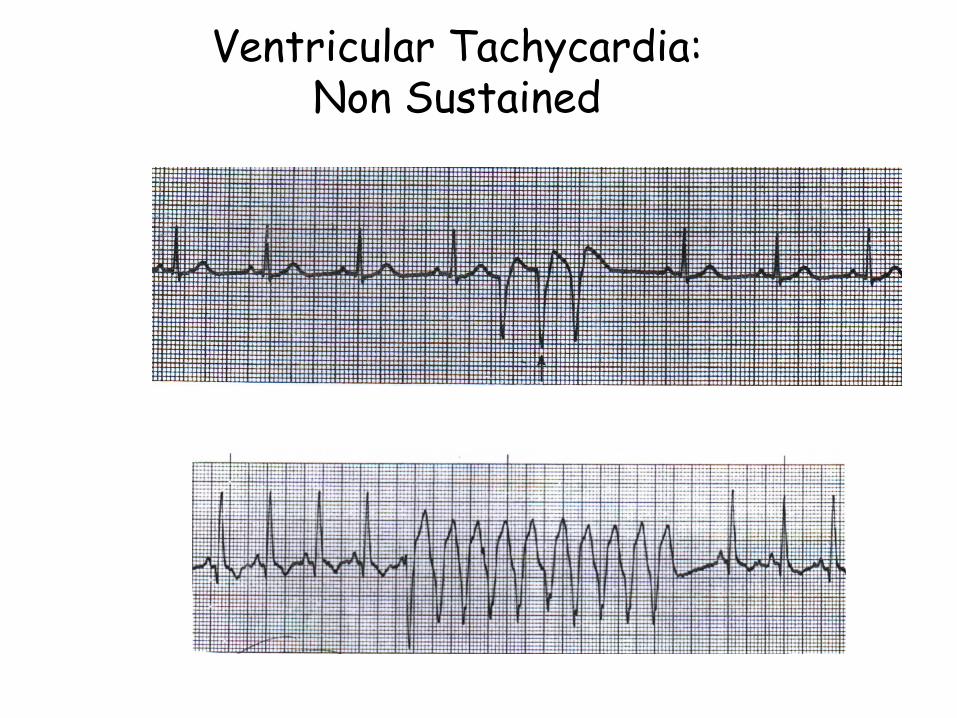
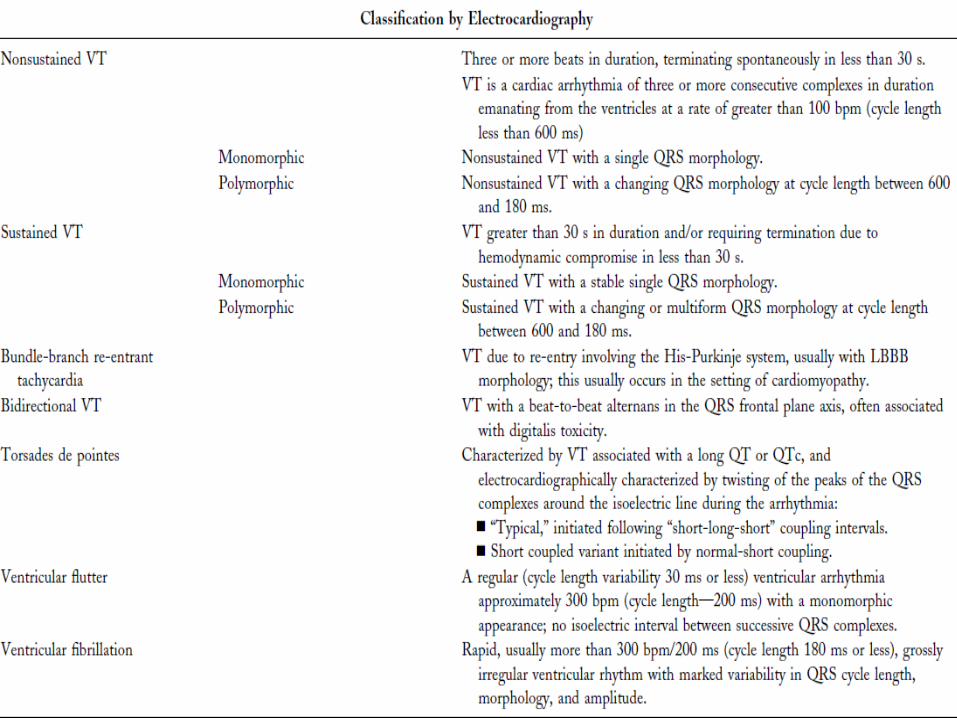
Ventricular Tachycardia:Non Sustained
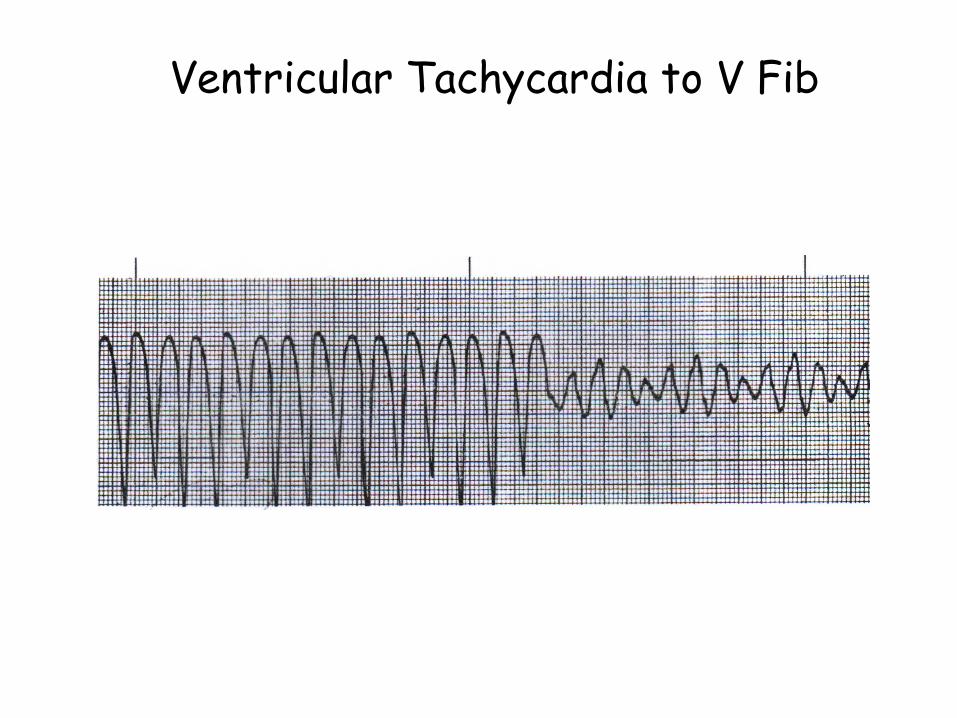
Ventricular Tachycardia to V Fib
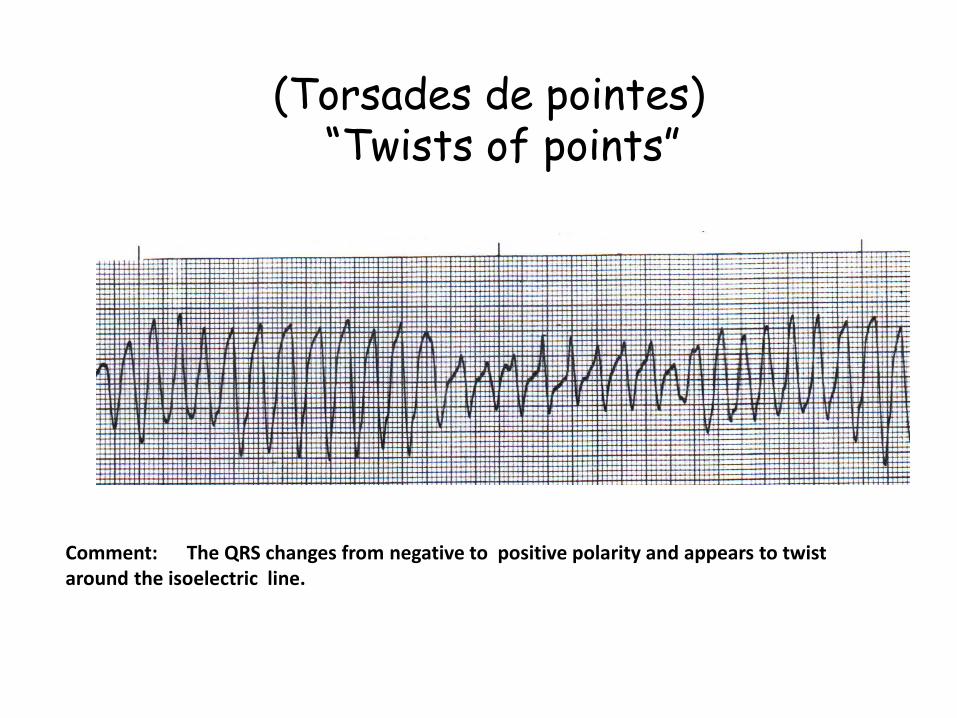
(Torsades de pointes)“Twists of points”
Comment: The QRS changes from negative to positive polarity and appears to twist around the isoelectric line.
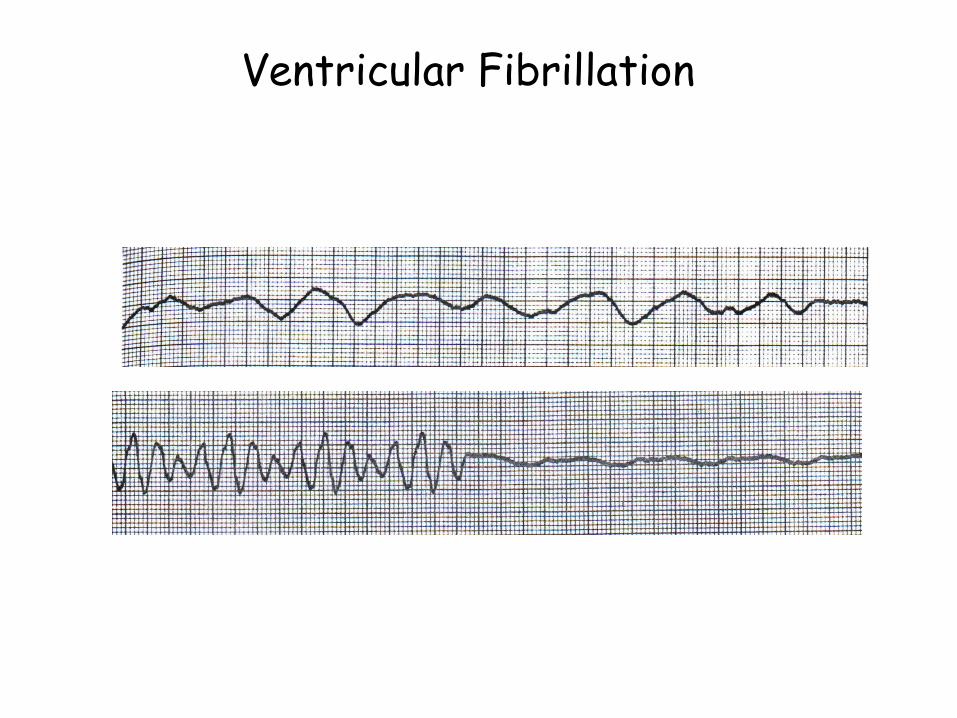
Ventricular Fibrillation
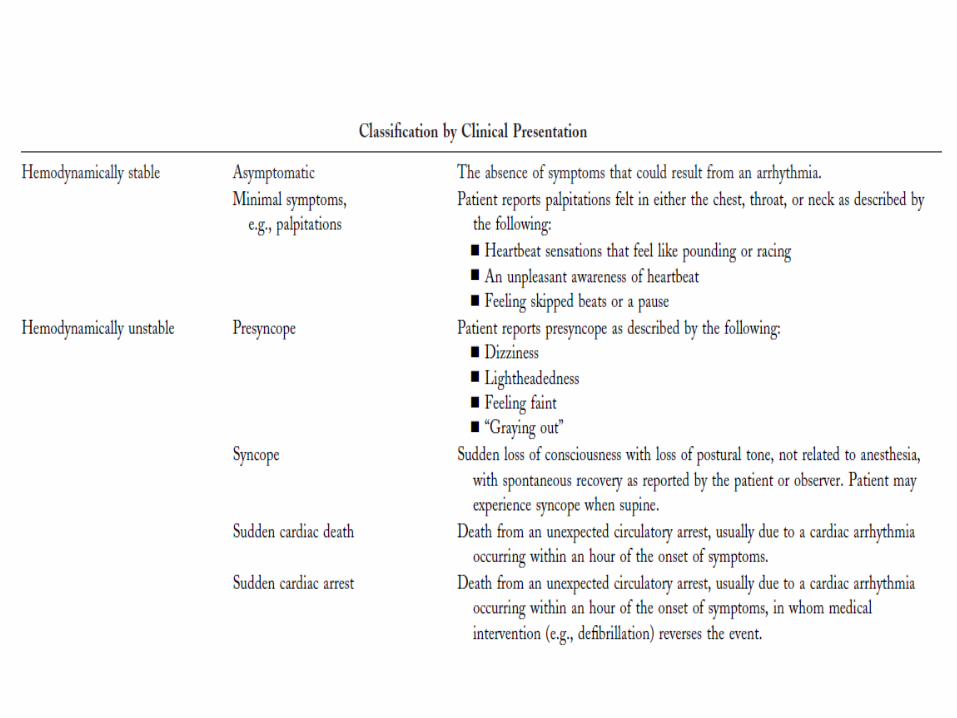
Clinical presentation
Ventricular arrhythmias
• Asymptomatic ventricular arrhythmias in the absence of identifiable heart disease predicted a small increase in risk (Ann Intern Med 1992;117:990–6) , while another study suggested no increased risk.(J Intern Med 1999;246:363–72)
• PVCs and runs of NSVT in subjects with structural heart disease contribute to an increased mortality risk.
• Suppression of PVCs – Severe and disabling symptoms.
• Beta blocker – Antiarrhythmic
• Refractory cases: Radiofrequency catheter ablation.
Ventricular arrhythmias
• SCD is leading cause of death in USA. estimates in the range of 300,000 to 350,000 SCDs annually.
• At least 50% of all SCDs due to CHD occur as a first clinical event or among subgroups of patients thought to be at relatively low risk for SCD.
• The rhythm most often recorded at the time of sudden cardiac arrest is ventricular tachyarrhythmia (VF>>VT).
Automated external defibrillator
• Approximately 80% of cardiac arrests occur out-of hospital.
• AED saves lives when external defibrillation can be rendered within minutes of onset of VF.
• Its use by both traditional and nontraditional first responders appears to be safe and effective.
• Federal, state and community efforts have been effective in placing AEDs in schools, sporting events, high-density residential sites and airports as well as on airplanes and in police and fire department vehicles.
EVALUATION OF PATIENTS WITH DOCUMENTEDOR SUSPECTED VENTRICULAR ARRHYTHMIAS
• Resting Electrocardiogram
• Exercise Testing
• Ambulatory Electrocardiography
• Left Ventricular Function and Imaging –Echocardiogram, Cardiac CT/MRI, Myocardial perfusion SPECT, Coronary angiogram
• Electrophysiological Testing
• EP testing for the evaluation of VT was introduced in 1972 by Wellens et al.
Ventricular arrhythmias
• Beta blocker
• Antiarrhythmic till 1980 (Class I III)
• ICD (First ICD placed in feb 1980)
• Ischemia
• Electrolytes (K and Mg)
• Drugs
• Ablation
• Surgery
Therapies For Ventricular Arrhythmia
• Beta blockers are effective in suppressing ventricular ectopic beats and arrhythmias as well as in reducing SCD in a spectrum of cardiac disorders in patients with and without HF.
• With the exception of beta blockers, the currently available antiarrhythmic drugs have not been shown in randomized clinical trials to be effective in the primary management of patients with life-threatening ventricular arrhythmias or in the prevention of SCD.
Special Considerations WhereAntiarrhythmic Drugs May Be Indicated
• Patients With Ventricular Tachyarrhythmias Who Do Not Meet Criteria for an Implantable Cardioverter-Defibrillator
• Patients With ICD Who Have Recurrent Ventricular Tachycardia/Ventricular Fibrillation With Frequent Appropriate ICD Firing.
• Patients With ICD Who Have Paroxysmal or Chronic Atrial Fibrillation With Rapid Rates and Inappropriate ICD Firing.
Conclusions:Among survivors of ventricular fibrillationor sustained ventricular tachycardia causingsevere symptoms, the implantable cardioverter–defibrillator is superior to antiarrhythmic drugs forincreasing overall survival.
(N Engl J Med 1997;337:1576-83.)
Conclusions::In patients with a prior myocardial infarctionwho are at high risk for ventricular tachyarrhythmia,prophylactic therapy with an implanted defibrillatorleads to improved survival as comparedwith conventional medical therapy.
(N Engl J Med 1996;335:1933-40.)
ConclusionsIn patients with a prior myocardial infarctionand advanced left ventricular dysfunction,prophylactic implantation of a defibrillator improvessurvival and should be considered as a recommendedtherapy.
(N Engl J Med 2002;346:877-83.)
Conclusions::In patients with NYHA class II or III CHF and LVEF of 35 percent or less, amiodarone has no favorable effect on survival, whereas single-lead, shock-only ICD therapy reduces overall mortality by 23 percent.
NEJM 352;3 January 20, 2005
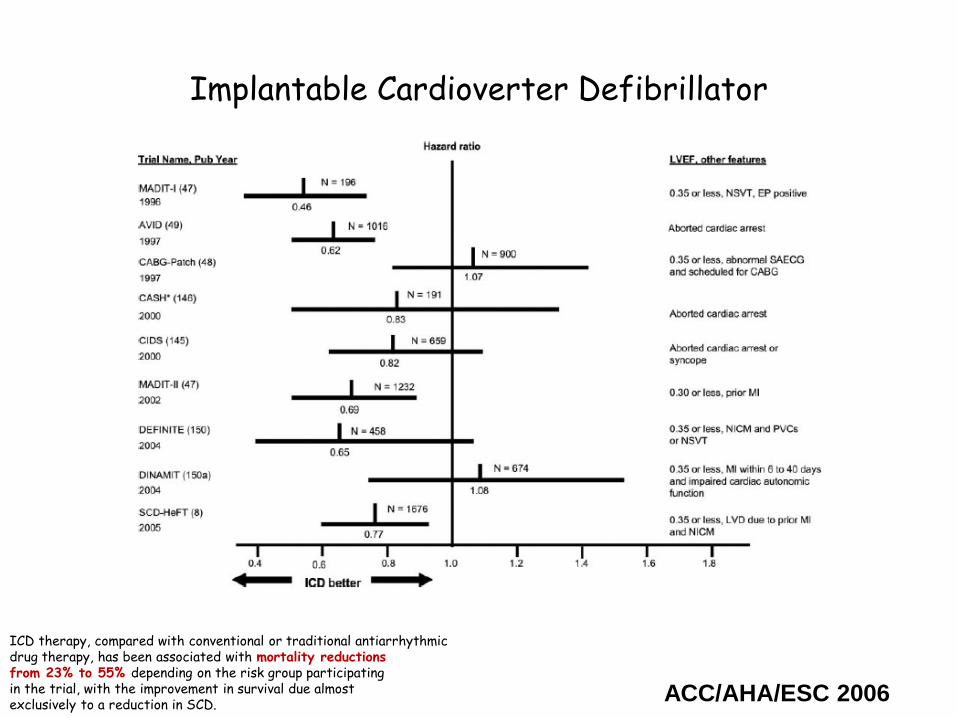
Implantable Cardioverter Defibrillator
ICD therapy, compared with conventional or traditional antiarrhythmicdrug therapy, has been associated with mortality reductionsfrom 23% to 55% depending on the risk group participatingin the trial, with the improvement in survival due almostexclusively to a reduction in SCD.
ACC/AHA/ESC 2006
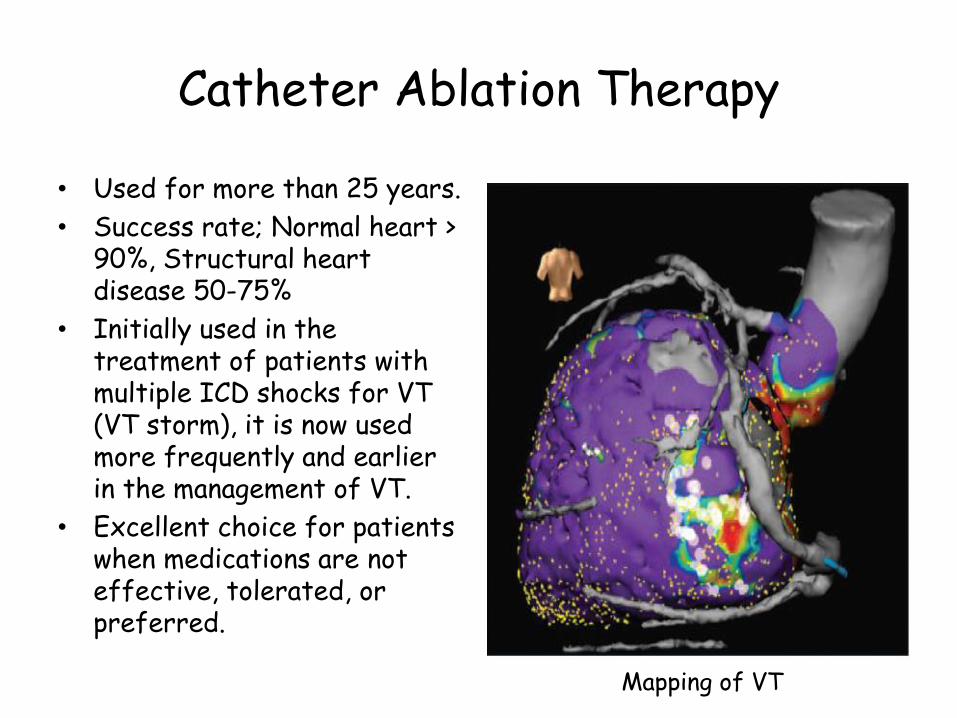
Catheter Ablation Therapy
• Used for more than 25 years.
• Success rate; Normal heart > 90%, Structural heart disease 50-75%
• Initially used in the treatment of patients with multiple ICD shocks for VT (VT storm), it is now used more frequently and earlier in the management of VT.
• Excellent choice for patients when medications are not effective, tolerated, or preferred.
Mapping of VT
Surgical therapy
• EP mapping and surgical resection of an arrhythmogenic focus.
• Left cervicothoracic sympathetic ganglionectomy in LQTS
• Large myocardial aneurysms secondary to MI are associated with hemodynamic compromise and are frequently accompanied by major ventricular arrhythmias.
• In selected patient aneurysm resection can improve cardiac function and may reduce or eliminate the accompanying ventricular arrhythmia.