Embed Size (px)
Citation preview

Research ArticleSynthetic Apparent Diffusion Coefficient for High b-ValueDiffusion-Weighted MRI in Prostate
Prativa Sahoo 1 Russell C Rockne 1 Alexander Jung2 Pradeep K Gupta3
Ram K S Rathore4 and Rakesh K Gupta3
1Division of Mathematical Oncology City of Hope Duarte USA2Department of Diagnostic Radiology City of Hope Duarte USA3Department of Radiology and Imaging Fortis Memorial Research Institute Gurgaon India4Department of Mathematics amp Statistics Indian Institute of Technology Kanpur Kanpur India
Correspondence should be addressed to Prativa Sahoo iitkprativagmailcom
Received 11 October 2019 Revised 9 January 2020 Accepted 16 January 2020 Published 10 February 2020
Academic Editor Cristina Magi-Galluzzi
Copyright copy 2020 Prativa Sahoo et al+is is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Purpose It has been reported that diffusion-weighted imaging (DWI) with ultrahigh b-value increases the diagnostic power ofprostate cancer DWI with higher b-values is challenging as it commonly suffers from low signal-to-noise ratio (SNR) distortionand longer scan time +e aim of our study was to develop a technique for quantification of apparent diffusion coefficient (ADC)for higher b-values from lower b-value DW images Materials and Methods Fifteen patients (7 malignant and 8 benign) wereincluded in this study retrospectively with the institutional ethical committee approval All images were acquired at a 3T MRscanner +e ADC values were calculated using a monoexponential model Synthetic ADC (sADC) for higher b-value wascomputed using a log-linear model Contrast ratio (CR) between prostate lesion and normal tissue on synthetic DWI (sDWI) wascomputed and compared with original DWI and ADC images Results No significant difference was observed between actualADC and sADC for b-2000 in all prostate lesions However CR increased significantly (p 0002 paired t-test) in sDWI ascompared to DWIMalignant lesions showed significantly lower sADC as compared to benign lesions (p 00116 independent t-test) Mean (plusmnstandard deviation) of sADC of malignant lesions was 0601plusmn 006 and for benign lesions was 092plusmn 009(10minus 3mm2s) DiscussionConclusion Our initial investigation suggests that the ADC values corresponding to higher b-value canbe computed using log-linear relationship derived from lower b-values (ble 1000) Our method might help clinicians to decide theoptimal b-value for prostate lesion identification
1 Introduction
In the past few years the use of diffusion-weighted magneticresonance imaging (DWI-MRI) for disease detection andcharacterization has increased substantially For instanceseveral studies have assessed the importance of DWI-derivedapparent diffusion coefficient (ADC) in characterization ofprostate cancer aggressiveness [1ndash4] Quantification of ADCis based on at least two diffusion-weighted (DW) imageswith different b-values In general a monoexponential fitbetween the natural logarithm of the signal intensity againstthe b-value yields the ADC In the literature various othermathematical models have been suggested for ADC
quantification such as stretched-exponential Gaussian andKurtosis [5 6] However in the prostate a monoexponentialfit for ADC calculation is sufficient to discriminate prostatecancer from normal tissue [5] Moreover different ADCvalues can be found in the literature due to the variation inthe b-value used to compute the ADC [7]
Deciding the optimal b-value for prostate cancer char-acterization is an active area of research [8ndash11] Inmost DWIstudies b-values of 1000 secmm2 or less are used forprostate cancer detection or evaluation [4 6 7] Normalparenchyma can show higher signal intensity in DWI with b-values of 1000 secmm2 or less which can make it difficult todistinguish normal tissue from cancer tissue It has been
HindawiProstate CancerVolume 2020 Article ID 5091218 7 pageshttpsdoiorg10115520205091218
reported that use of higher b-values improves disease vi-sualization and detection by increasing contrast betweencancerous and noncancerous lesions [10 12 13] Althoughthe use of higher b-values (gt1000 secmm2) is desirableobtaining higher b-value DW images is challenging as itleads to decreased signal-to-noise ratio (SNR) increaseddistortion susceptibility artifact and increased scan timeComputed DWI techniques have been proposed to over-come these difficulties [14ndash18]
Computed DWI is a mathematical technique whichgenerates images of higher b-values by using at least twodifferent lower b-value (ble 1000) images It involves com-puting the ADCmap from two lower b-value DW images byusing the following equation
ADC minus1bln
Sb
S01113888 1113889 (1)
where S0 is the signal intensity at b 0 smm2 Once ADC forthe lower b-value is known computed DW images of thehigher b-value can be extrapolated by solving equation (1)for Sb
Sbhigh S0e
minus bhigh middotADC (2)
+e underlying assumption of the computed DWImethod is that the ADC is independent of b-values whichcontradicts the observation that ADC can vary significantlywith the b-value as reported in the literature [19 20] Usingthis technique DW images for higher b-values can begenerated but the ADC value for the higher b-value cannotbe obtained Computed DWI technique might be useful forthe visualization purpose however for quantitative DWimage analysis it might not be sufficient+erefore there is aneed of methods for generating synthetic ADC maps forhigher b-values To the best of our knowledge methods forcreating synthetic ADC maps have not been reported
+e primary objective of this study was to explore therelationship between ADC and b-values and use that rela-tionship to extrapolate synthetic ADC corresponding tohigher b-values A secondary objective was to investigate thefeasibility of this technique to improve visualization of le-sions in prostate cancer cases for which higher b-value DWImay be desirable
11 +eory Diffusion of water through biological tissue isoften quantified using the apparent diffusion coefficientcalculated from pairs of b-value DW images using themonoexponential model (equation (1)) However as manystudies have demonstrated the ADC follows a multi-exponential law with respect to higher b-value DWI signalintensity moreover this multiexponential behavior is notonly related to the perfusion artifact [6 7 15 21 22] +emultiexponential behavior depends upon the intravoxelproton pools that contribute to the signal decay To over-come the difficulty of making assumptions about thenumber of intravoxel proton pools with different diffusioncoefficients in biological tissue Bennett et al [6] introduced
the stretched-exponential model +e stretched-exponentialmodel is described as follows
S(b)
S(0) exp (minus b times DDC)
α( 1113857 (3)
where α represents intravoxel heterogeneity and DDC is thedistributed diffusion coefficient representing the meanintravoxel diffusion rate where α 1 is equivalent to themonoexponential signal decay Comparing equations (1)and (3) the ADC computed from the monoexponentialmodel can be written as a function of b
ADC bαminus 1DDCα
⟹ ln(ADC) (α minus 1)ln(b) + α ln(DDC)
or ln(ADC) P1 ln(b) + P1(4)
(4)
where P1 and P2 are constants +erefore we hypothesized alog-linear relationship between ADC derived from themonoexponential model and the b-value+e purpose of thisstudy was to derive the log-linear relation for lower b-valueADCs and use that relationship to extrapolate ADCs forhigher b-values
2 Materials and Methods
21 Patient Selection A total of 15 patients with a medianage of 625 years suspected to have prostate cancer wereincluded in this retrospective study with the institutionalethical committee approval All patients were treatmentnaıve and from a single center Image-guided biopsy wasperformed after the imaging +e diffusion images werefused to USG images and the biopsy from the abnormaldiffusion lesion was taken using image guidance +eGleason scores (GS) for the biopsies of the malignant tissuewere recorded [23] Out of 15 cases only two patients hadGS 7 and 5 patients had GS 6 +e remaining 8 patientswere reported as benign Henceforth we have consideredGS 6 and 7 as malignant (N 7) and rest as benign (N 8)All benign lesions had benign hypertrophy of the prostatewith no evidence of malignancy and all malignant lesionswith biopsy positive had PI-RADs 4 (n 3) or PI-RADS 5(n 4)
22 Imaging Protocol All imaging was performed on a30TMR scanner (Ingenia Philips Medical System Best+eNetherlands) T2-weighted turbo spin-echo (TSE) imagescovering the whole prostate gland were acquired in theaxial plane with parameters TR 4401ms TE 120ms slicethickness 3mm number of slices 80 acquisition matrix504 times 415 and FOV 377 times 377mm2 DWI images wereacquired in the axial plane with seven different b-values (0200 400 700 1000 1500 and 2000 smm2) TR 3709msTE 778ms slice thickness 3mm number of slices 23acquisition matrix 92times 92 and FOV 275times 275mm2 Ac-quisition time for all 7 b-value DWI sequences was 3min26 sec
2 Prostate Cancer
23 Statistical Analysis ADC values for different b-valueswere computed using the monoexponential model (equation(1))voxel-wise Regions of interest (ROIs) of size(15ndash20mm2) were placed on the transitional zone (TZ) andperipheral zone (PZ) of the prostate for each patientVariations in the mean ADC value within the ROI withrespect to the b-values used for the quantification of ADCwere analyzed with a one-way ANOVA test +e log-linearmodel (equation (4))was fitted voxel-wise to the lower b-value ADCs (ADC0ndash400 ADC0ndash700 ADC0ndash1000) to estimatethe model parameters P1 and P2 Synthetic ADC (sADC)calculated from equation (4) for b-1500 and b-2000 wasextrapolated using themodel parameters and compared withthe true ADC0ndash1500 and ADC0ndash2000 +e error in the sADC atb-1500 and b-2000 relative to the observed ADC wascomputed as
relative error |ADC minus sADC|
ADCtimes 100 (5)
Synthetic DWI (sDWI) images for b-1500 and b-2000were generated using DWI of b0 and sADC using themonoexponential model and compared with originalDWI1500 and DWI2000 Contrast ratio (CR) between normaland lesion for DWI and sDWI were computed usingCR (Scancer minus Snormal tissue)(Scancer + Snormal tissue) CR fororiginal DWI and sDWI for b-1500 and b-2000 sADCvalues of malignant and benign lesions were assessed by apaired t-test p values lt005 were considered as statisticallysignificant Statistical analysis was performed using Prism(GraphPad Software Version 70)
24 Regions of Interest Regions of interest (ROIs) wereplaced at the normal appearing muscle area and at thelesion on the original DWI image and computed DWIimage Two radiologists one with 10 years of experienceand another with more than 20 years of experience blindedto each other and to histological finding placed the ROIsOverlapping of the ROIs from the two radiologists was
95 For cases with an area suspicious for tumor ROIswere placed on axial high b-value diffusion weighted im-ages (b 2000 smm2) on a hyperintense area suspicious fortumor and a normal intensity area within the gland on thesame image For cases in which the area suspicious fortumor was in the peripheral zone of the gland the normalintensity region of interest was selected from a location inthe peripheral zone on the same image For cases with noarea suspicious for tumor regions of interest were placed inthe relatively hyperintense peripheral zone and in thetransition zonemdashwhich is normally hypointense to theperipheral zonemdashon the same image
3 Results
In the one-way ANOVA test ADC shows highly significantchange (plt 00001) with respect to the b-value both in thetransitional zone (TZ) and peripheral zone (PZ) (Figure 1)of the prostate in all the patient data +is observationsupports our initial assumption that the ADC is notconstant with respect to b-values +e log-linear modelgives the best fit to the data (R2sim09) from the prostatetissue (Figure 2)
No significant difference was observed in the paired t-testbetween sADC as compared to actual ADC in the prostatelesions however the change was significant in the normaltissue (plt 0001) at b-2000 Contrast ratio increased signif-icantly between original DWI images and sDWI images(p 0002) (Figure 3)
Mean sADC of prostate lesions was significantly lowerthan that of surrounding normal tissue (plt 0001) for b-2000 when considered for all data (N 15) A significantlylower sADC was observed using an independent t-test inmalignant lesions (GS 67) as compared to benign lesions(GSlt 6) (Figure 4) In addition sADC at b-1000 b-1500and b-2000 was found to be significantly distinguish lesionswith GSlt 6 from the lesions with GSge 6 +e mean sADCvalue confidence interval (CI) and the p values are given inTable 1
0
1
2
3
4
b0-2
00
b0-4
00
b0-2
000
b0-1
500
b0-1
000
b0-7
00
N = 15p lt 0001
AD
C (times
10ndash3
mm
2 s)
(a)
0
2
4
6
8
b0-2
00
b0-4
00
b0-2
000
b0-1
500
b0-1
000
b0-7
00
N = 15p lt 0001
AD
C (times
10ndash3
mm
2 s)
(b)
Figure 1 Estimated apparent diffusion coefficient (ADC) using monoexponential model in the transitional zone (TZ) (a) and peripheralzone (PZ) (b) of prostate +e change in ADC value for each choice of b-value from the other was found to be highly significant withplt 00001 using the one-way ANOVA test in both the regions
Prostate Cancer 3
4 Discussion and Conclusion
Choice of b-values can significantly influence ADC esti-mation using the monoexponential diffusion model in theprostate in agreement with variations in ADC found in the
literature [7 19 20] Our study shows a log-linear rela-tionship between ADC and b-values Using the log-linearrelationship derived from ADCs of the lower b-value(b 400 700 and 1000) ADCs for higher b-values (b 1500and 2000) can be extrapolated with a small relative error
04
06
08
1
12
0 1000 2000
1
15
2
25
0 500 1000 1500 2000
05
1
15
2
0 500 1000 1500 2000b-value (smm2) b-value (smm2)
b-value (smm2) b-value (smm2)
04
06
08
1
12
0 500 1000 1500 2000
ADCADC
1
15
2
25
0 1000 2000
05
1
15
2
0 1000 2000
sADC
b-value (smm2) b-value (smm2)
ADCADCsADC
ADCADCsADC
(a) (d)
(e)
(f)
(j)
(g)
(h)
(i)
(b)
(c)
sDWIb2000 ADCb2000 sADCb200090
70
50
30
10
Error
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
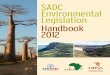
Figure 2 Log-linear relationship between ADC and b-value Example of log-linear model fit to targeted tissue of a 69-year-old patient withadenocarcinoma in peripheral zone (PZ) of prostate Axial DWI images of b-1000 with regions of interest (ROIs) in PZ lesion (a) normal PZ(b) normal transition zone (c) and corresponding graphs with b-value (x-axis) ADC (y-axis) and log-linear fit for each ROI (d e and f)+e plots (g) (h) and (i) show the log-linear model fit to ADC value at b-400 b-700 and b-1000 (black solid line) and extrapolation of sADCat b-1500 and b-2000(dotted line) Bottom row shows the sDWI ADC and sADC maps at b-2000 and color-coded error map of thecorresponding slice
4 Prostate Cancer
(10plusmn 5) Contrast ratio of lesion and normal tissue sig-nificantly increases in synthetic DW images
+e technique of generating synthetic ADC gives cli-nicians extra degrees of freedom with the choice of b-values +e optimal b-value for disease detection dependsupon image contrast that is likely to change with tissuetype and histological findings Rather than deciding theoptimal b-value prior to imaging to get optimal contrastbetween normal and cancer tissue the use of syntheticADCmay be able to modify the b-value and get the optimalimage contrast even after imaging Furthermore thetechnique allows extrapolation of ADC values for higher b-values which cannot be obtained by the computed DWImethod However this technique may not reduce theoverall scan time as in our scanning protocol the scanningtime to get three different b-values (b-400 700 and 1000)
is 1 min 39 sec and scanning time for one high b-value (b-2000) is 1 min 5 sec +is technique provides a method toobtain DW images and ADC values for a wide range of b-values
According to the diffusion equation b-value has a[time]3 dependency thus a very high b-value can beachieved in a clinical scanner with a moderate increase inthe echo time (TE) However the signal loss due to dif-fusion is a limiting factor at high b-values +e initialsignal-to-noise ratio (SNR) and the tissue diffusion de-termine how quickly the signal goes below the noise levelAs the tissue diffusivity is higher in normal tissue as comparedto cancer tissue normal region signal decay reaches to thenoise level at a relatively faster rate Hence the observed signalat high b-values is dominated by the noise and appears todecay at a slower rate +is explains the reason of significant
00
05
10
15
20
25
NS
ADC sADC
N = 15
AD
C (times
10ndash3
mm
2 s)
(a)
ADC sADC00
05
10
15
20
25
NS
N = 12
AD
C (times
10ndash3
mm
2 s)
(b)
00
05
10
15
20
25
ADC sADC
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(c)
ADC sADC00
05
10
15
20
25
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(d)
00
02
04
06
08
10
Con
tras
t rat
io
DWI sDWI
lowastlowast
(e)
DWI sDWI00
02
04
06
08
10
Con
tras
t rat
io
lowast
(f )
Figure 3 Inter-reader variation of ADC and contrast ratio +ere was no significant difference between ADC values and synthetic ADC(sADC) values in the lesion (a and b) at b-2000 +e difference between ADC and sADC in ROIs placed in normal tissue was significantlydifferent (c and d) However the contrast ratio of lesion and surrounding normal tissue increased significantly between DWI and sDWI forb-2000 (e and f) lowastplt 005 lowastlowastplt 001 +e top row shows the result of Reader 1 (N 15) and the bottom row shows that of Reader 2(N 12) (a) Reader 1 lesion (b) Reader 1 normal (c) Reader 1 DWI (b-2000) (d) Reader 2 lesion (e) Reader 2 normal (f ) Reader 2 DWI (b-2000)
Prostate Cancer 5
difference between ADC and sADC values at normal regionsAs DWI signal attenuation is exponentially dependent onADC small changes in ADC can make a significant change inDWI contrast this results in the significant increase of CR insDWI images as compared to DWI
+e present study demonstrates that although the higherb-value sDWI increases the contrast between lesion andnormal tissue the sADC shows similar contrast for b-1000b-1500 and b-2000 +is could be due to small cohort size ofthe patient with different Gleason scores consistent withresults in other studies [12 24] ADC computed from high b-value DWI has been shown to be more accurate in dis-tinguishing prostate lesions from benign and normal tissues[25 26] Further investigation could be done for the clinicalapplication of sDWI with larger patient populations One ofthe limitations of our study was MRI examinations were notcompared with a radical prostatectomy specimen Howeverimage-guided MR-overlayed biopsy could be a good alter-native to radical prostatectomy where patient refuses toundergo prostatectomy
Our initial investigation suggests that the ADC valuescorresponding to higher b-value DWI can be computedusing a log-linear relationship derived from lower b-values(ble 1000) Moreover this computational method can also
be manipulated to determine optimized b-values to createADC maps +e synthetic ADC technique could be a usefultool to provide optimized image contrast for quantitativeDW-MR imaging applications in oncology where ADC isroutinely used in clinical practice
Data Availability
+e data that support the findings of this study are availablefrom the corresponding author upon reasonable request
Disclosure
Partial results of this manuscript have been presented at theEuropean Society for Magnetic Resonance in Medicine andBiology (ESMRMB) 2017 Barcelona Spain with the ab-stract titled ldquoSynthetic Apparent Diffusion Coefficient forUltra High b-value DiffusionWeighted Imaging in Prostaterdquo(abstract number esmrmb201758233ce)
Conflicts of Interest
+e authors declare that they have no conflicts of interest
Malignant Benign00
05
10
15
20
sAD
C (times
10ndash3
mm
2 s)
lowast
(a)
Malignant BenignsA
DC
(times10
ndash3 m
m2 s
)
lowast
00
05
10
15
20
(b)
Malignant Benign
sAD
C (times
10ndash3
mm
2 s)
lowast
00
05
10
15
20
(c)
Figure 4 Comparison between synthetic ADC (sADC) values of malignant and benign tissue Distribution of sADC values for malignant(Gleason score 6 and 7 N 7) and benign lesions (Gleason score lt6 N 8) in patients at b-1000 (a) b-1500 (b) and b-2000 (c) +e centerhorizontal line indicates the median value lowastplt 005
Table 1 Comparison between sADC values in lesions with Gleason score (GS) lt6 and GS ge6 at b-1000 b-1500 and b-2000
MalignantGS (67)N 7
sADC (10minus 3mm2s)(meanplusmn SD)
BenignGSlt 6N 8
sADC (10minus 3mm2s)(meanplusmn SD)
95 CI p value
b-1000 0818plusmn 0067 1131plusmn 0084 0075ndash0550 00138lowastb-1500 0682plusmn 0059 1007plusmn 0090 0084ndash0567 00121lowastb-2000 0601plusmn 0057 0935plusmn 0094 0088ndash0581 00116lowastlowastStatistically significant 95 CI 95 confidence interval sADC synthetic apparent diffusion coefficient GS Gleason score
6 Prostate Cancer
References
[1] H A Vargas O Akin T Franiel et al ldquoDiffusion-weightedendorectal MR imaging at 3 T for prostate cancer tumordetection and assessment of aggressivenessrdquo Radiologyvol 259 no 3 pp 775ndash784 2011
[2] T Tamada V Prabhu J Li J S Babb S S Taneja andA B Rosenkrantz ldquoAssessment of prostate cancer aggres-siveness using apparent diffusion coefficient values impact ofpatient race and agerdquo Abdominal Radiology vol 42 no 6pp 1744ndash1751 2017
[3] T H Kim C K Kim B K Park et al ldquoRelationship betweenGleason score and apparent diffusion coefficients of diffusion-weighted magnetic resonance imaging in prostate cancerpatientsrdquo Canadian Urological Association Journal vol 10no 11-12 pp E377ndashE382 2016
[4] A Lebovici S A Sfrangeu D Feier et al ldquoEvaluation of thenormal-to-diseased apparent diffusion coefficient ratio as anindicator of prostate cancer aggressivenessrdquo BMC MedicalImaging vol 14 no 1 p 15 2014
[5] M Quentin D Blondin J Klasen et al ldquoComparison ofdifferent mathematical models of diffusion-weighted prostateMR imagingrdquo Magnetic Resonance Imaging vol 30 no 10pp 1468ndash1474 2012
[6] K M Bennett K M Schmainda R Bennett (Tong)D B Rowe H Lu and J S Hyde ldquoCharacterization ofcontinuously distributed cortical water diffusion rates with astretched-exponential modelrdquo Magnetic Resonance in Medi-cine vol 50 no 4 pp 727ndash734 2003
[7] M M Jafar A Parsai and M E Miquel ldquoDiffusion-weightedmagnetic resonance imaging in cancer reported apparentdiffusion coefficients in-vitro and in-vivo reproducibilityrdquoWorld Journal of Radiology vol 8 no 1 pp 21ndash49 2016
[8] C Kyo Kim B Kwan Park B Kim and C K Kim ldquoHigh-b-value diffusion-weighted imaging at 3 Tto detect prostate cancercomparisons between b values of 1000 and 2000 smm2rdquoAmerican Journal of Roentgenology vol 194 pp W33ndashW372010
[9] T de Perrot M Scheffler J Boto et al ldquoDiffusion in prostatecancer detection on a 3T scanner how many b-values areneededrdquo Journal of Magnetic Resonance Imaging vol 44no 3 pp 601ndash609 2016
[10] G Manenti M Nezzo F Chegai E Vasili E Bonanno andG Simonetti ldquoDWI of prostate cancer optimal b-value inclinical practicerdquo Prostate Cancer vol 2014 Article ID868269 9 pages 2014
[11] E U Saritas J H Lee and D G Nishimura ldquoSNR depen-dence of optimal parameters for apparent diffusion coefficientmeasurementsrdquo IEEE Transactions on Medical Imagingvol 30 no 2 pp 424ndash437 2011
[12] T Tamada N Kanomata T Sone et al ldquoHigh b value(2000 smm2) diffusion-weighted magnetic resonanceimaging in prostate cancer at 3 tesla comparison with 1000smm2 for tumor conspicuity and discrimination of ag-gressivenessrdquo PLoS One vol 9 Article ID e96619 2014
[13] K Katahira T Takahara T C Kwee et al ldquoUltra-high-b-value diffusion-weighted MR imaging for the detection ofprostate cancer evaluation in 201 cases with histopathologicalcorrelationrdquo European Radiology vol 21 no 1 pp 188ndash1962011
[14] Y Ueno S Takahashi K Kitajima et al ldquoComputed diffu-sion-weighted imaging using 3-Tmagnetic resonance imagingfor prostate cancer diagnosisrdquo European Radiology vol 23no 12 pp 3509ndash3516 2013
[15] M D Blackledge M O Leach D J Collins and D-M KohldquoComputed diffusion-weighted MR imaging may improvetumor detectionrdquo Radiology vol 261 no 2 pp 573ndash5812011
[16] M Takeuchi K Matsuzaki and M Harada ldquoComputeddiffusion-weighted imaging for differentiating decidualizedendometrioma from ovarian cancerrdquo European Journal ofRadiology vol 85 no 5 pp 1016ndash1019 2016
[17] Y Ueno S Takahashi Y Ohno et al ldquoComputed diffusion-weighted MRI for prostate cancer detection the influence ofthe combinations of b-valuesrdquo +e British Journal of Radi-ology vol 88 no 1048 Article ID 20140738 2015
[18] R Yoshida T Yoshizako T Katsube Y Tamaki N Ishikawaand H Kitagaki ldquoComputed diffusion-weighted imagingusing 15-T magnetic resonance imaging for prostate cancerdiagnosisrdquo Clinical Imaging vol 41 pp 78ndash82 2017
[19] G+ormer J Otto M Reiss-Zimmermann et al ldquoDiagnosticvalue of ADC in patients with prostate cancer influence of thechoice of b valuesrdquo European Radiology vol 22 no 8pp 1820ndash1828 2012
[20] Y Peng Y Jiang T Antic et al ldquoApparent diffusion coef-ficient for prostate cancer imaging impact of b valuesrdquoAmerican Journal of Roentgenology vol 202 no 3pp W247ndashW253 2014
[21] Y Oto A Afaq D B Rowe Y Lu A Shukla-Dave andJ Grover ldquoDiffusion-weighted magnetic resonance imagingof the prostate improved robustness with stretched expo-nential modelingrdquo Journal of Computer Assisted Tomographyvol 36 no 6 pp 695ndash703 2012
[22] M Iima and D Le Bihan ldquoClinical intravoxel incoherentmotion and diffusion MR imaging past present and futurerdquoRadiology vol 278 no 1 pp 13ndash32 2016
[23] Understanding Your Pathology Report Prostate Cancer[24] A B Rosenkrantz N Hindman R P Lim et al ldquoDiffusion-
weighted imaging of the prostate comparison of b1000 andb2000 image sets for index lesion detectionrdquo Journal ofMagnetic Resonance Imaging vol 38 no 3 pp 694ndash700 2013
[25] K Taneja Y Kaji K Kuroda and K Sugimura ldquoHigh b-valuediffusion-weighted imaging in normal and malignant pe-ripheral zone tissue of the prostate effect of signal-to-noiseratiordquo Magnetic Resonance in Medical Sciences vol 7 no 2pp 93ndash99 2008
[26] K Kitajima S Takahashi Y Ueno et al ldquoClinical utility ofapparent diffusion coefficient values obtained using highb-value when diagnosing prostate cancer using 3 tesla MRIcomparison between ultra-high b-value (2000 smm2) andstandard high b-value (1000 smm2)rdquo Journal of MagneticResonance Imaging vol 36 no 1 pp 198ndash205 2012
Prostate Cancer 7

reported that use of higher b-values improves disease vi-sualization and detection by increasing contrast betweencancerous and noncancerous lesions [10 12 13] Althoughthe use of higher b-values (gt1000 secmm2) is desirableobtaining higher b-value DW images is challenging as itleads to decreased signal-to-noise ratio (SNR) increaseddistortion susceptibility artifact and increased scan timeComputed DWI techniques have been proposed to over-come these difficulties [14ndash18]
Computed DWI is a mathematical technique whichgenerates images of higher b-values by using at least twodifferent lower b-value (ble 1000) images It involves com-puting the ADCmap from two lower b-value DW images byusing the following equation
ADC minus1bln
Sb
S01113888 1113889 (1)
where S0 is the signal intensity at b 0 smm2 Once ADC forthe lower b-value is known computed DW images of thehigher b-value can be extrapolated by solving equation (1)for Sb
Sbhigh S0e
minus bhigh middotADC (2)
+e underlying assumption of the computed DWImethod is that the ADC is independent of b-values whichcontradicts the observation that ADC can vary significantlywith the b-value as reported in the literature [19 20] Usingthis technique DW images for higher b-values can begenerated but the ADC value for the higher b-value cannotbe obtained Computed DWI technique might be useful forthe visualization purpose however for quantitative DWimage analysis it might not be sufficient+erefore there is aneed of methods for generating synthetic ADC maps forhigher b-values To the best of our knowledge methods forcreating synthetic ADC maps have not been reported
+e primary objective of this study was to explore therelationship between ADC and b-values and use that rela-tionship to extrapolate synthetic ADC corresponding tohigher b-values A secondary objective was to investigate thefeasibility of this technique to improve visualization of le-sions in prostate cancer cases for which higher b-value DWImay be desirable
11 +eory Diffusion of water through biological tissue isoften quantified using the apparent diffusion coefficientcalculated from pairs of b-value DW images using themonoexponential model (equation (1)) However as manystudies have demonstrated the ADC follows a multi-exponential law with respect to higher b-value DWI signalintensity moreover this multiexponential behavior is notonly related to the perfusion artifact [6 7 15 21 22] +emultiexponential behavior depends upon the intravoxelproton pools that contribute to the signal decay To over-come the difficulty of making assumptions about thenumber of intravoxel proton pools with different diffusioncoefficients in biological tissue Bennett et al [6] introduced
the stretched-exponential model +e stretched-exponentialmodel is described as follows
S(b)
S(0) exp (minus b times DDC)
α( 1113857 (3)
where α represents intravoxel heterogeneity and DDC is thedistributed diffusion coefficient representing the meanintravoxel diffusion rate where α 1 is equivalent to themonoexponential signal decay Comparing equations (1)and (3) the ADC computed from the monoexponentialmodel can be written as a function of b
ADC bαminus 1DDCα
⟹ ln(ADC) (α minus 1)ln(b) + α ln(DDC)
or ln(ADC) P1 ln(b) + P1(4)
(4)
where P1 and P2 are constants +erefore we hypothesized alog-linear relationship between ADC derived from themonoexponential model and the b-value+e purpose of thisstudy was to derive the log-linear relation for lower b-valueADCs and use that relationship to extrapolate ADCs forhigher b-values
2 Materials and Methods
21 Patient Selection A total of 15 patients with a medianage of 625 years suspected to have prostate cancer wereincluded in this retrospective study with the institutionalethical committee approval All patients were treatmentnaıve and from a single center Image-guided biopsy wasperformed after the imaging +e diffusion images werefused to USG images and the biopsy from the abnormaldiffusion lesion was taken using image guidance +eGleason scores (GS) for the biopsies of the malignant tissuewere recorded [23] Out of 15 cases only two patients hadGS 7 and 5 patients had GS 6 +e remaining 8 patientswere reported as benign Henceforth we have consideredGS 6 and 7 as malignant (N 7) and rest as benign (N 8)All benign lesions had benign hypertrophy of the prostatewith no evidence of malignancy and all malignant lesionswith biopsy positive had PI-RADs 4 (n 3) or PI-RADS 5(n 4)
22 Imaging Protocol All imaging was performed on a30TMR scanner (Ingenia Philips Medical System Best+eNetherlands) T2-weighted turbo spin-echo (TSE) imagescovering the whole prostate gland were acquired in theaxial plane with parameters TR 4401ms TE 120ms slicethickness 3mm number of slices 80 acquisition matrix504 times 415 and FOV 377 times 377mm2 DWI images wereacquired in the axial plane with seven different b-values (0200 400 700 1000 1500 and 2000 smm2) TR 3709msTE 778ms slice thickness 3mm number of slices 23acquisition matrix 92times 92 and FOV 275times 275mm2 Ac-quisition time for all 7 b-value DWI sequences was 3min26 sec
2 Prostate Cancer
23 Statistical Analysis ADC values for different b-valueswere computed using the monoexponential model (equation(1))voxel-wise Regions of interest (ROIs) of size(15ndash20mm2) were placed on the transitional zone (TZ) andperipheral zone (PZ) of the prostate for each patientVariations in the mean ADC value within the ROI withrespect to the b-values used for the quantification of ADCwere analyzed with a one-way ANOVA test +e log-linearmodel (equation (4))was fitted voxel-wise to the lower b-value ADCs (ADC0ndash400 ADC0ndash700 ADC0ndash1000) to estimatethe model parameters P1 and P2 Synthetic ADC (sADC)calculated from equation (4) for b-1500 and b-2000 wasextrapolated using themodel parameters and compared withthe true ADC0ndash1500 and ADC0ndash2000 +e error in the sADC atb-1500 and b-2000 relative to the observed ADC wascomputed as
relative error |ADC minus sADC|
ADCtimes 100 (5)
Synthetic DWI (sDWI) images for b-1500 and b-2000were generated using DWI of b0 and sADC using themonoexponential model and compared with originalDWI1500 and DWI2000 Contrast ratio (CR) between normaland lesion for DWI and sDWI were computed usingCR (Scancer minus Snormal tissue)(Scancer + Snormal tissue) CR fororiginal DWI and sDWI for b-1500 and b-2000 sADCvalues of malignant and benign lesions were assessed by apaired t-test p values lt005 were considered as statisticallysignificant Statistical analysis was performed using Prism(GraphPad Software Version 70)
24 Regions of Interest Regions of interest (ROIs) wereplaced at the normal appearing muscle area and at thelesion on the original DWI image and computed DWIimage Two radiologists one with 10 years of experienceand another with more than 20 years of experience blindedto each other and to histological finding placed the ROIsOverlapping of the ROIs from the two radiologists was
95 For cases with an area suspicious for tumor ROIswere placed on axial high b-value diffusion weighted im-ages (b 2000 smm2) on a hyperintense area suspicious fortumor and a normal intensity area within the gland on thesame image For cases in which the area suspicious fortumor was in the peripheral zone of the gland the normalintensity region of interest was selected from a location inthe peripheral zone on the same image For cases with noarea suspicious for tumor regions of interest were placed inthe relatively hyperintense peripheral zone and in thetransition zonemdashwhich is normally hypointense to theperipheral zonemdashon the same image
3 Results
In the one-way ANOVA test ADC shows highly significantchange (plt 00001) with respect to the b-value both in thetransitional zone (TZ) and peripheral zone (PZ) (Figure 1)of the prostate in all the patient data +is observationsupports our initial assumption that the ADC is notconstant with respect to b-values +e log-linear modelgives the best fit to the data (R2sim09) from the prostatetissue (Figure 2)
No significant difference was observed in the paired t-testbetween sADC as compared to actual ADC in the prostatelesions however the change was significant in the normaltissue (plt 0001) at b-2000 Contrast ratio increased signif-icantly between original DWI images and sDWI images(p 0002) (Figure 3)
Mean sADC of prostate lesions was significantly lowerthan that of surrounding normal tissue (plt 0001) for b-2000 when considered for all data (N 15) A significantlylower sADC was observed using an independent t-test inmalignant lesions (GS 67) as compared to benign lesions(GSlt 6) (Figure 4) In addition sADC at b-1000 b-1500and b-2000 was found to be significantly distinguish lesionswith GSlt 6 from the lesions with GSge 6 +e mean sADCvalue confidence interval (CI) and the p values are given inTable 1
0
1
2
3
4
b0-2
00
b0-4
00
b0-2
000
b0-1
500
b0-1
000
b0-7
00
N = 15p lt 0001
AD
C (times
10ndash3
mm
2 s)
(a)
0
2
4
6
8
b0-2
00
b0-4
00
b0-2
000
b0-1
500
b0-1
000
b0-7
00
N = 15p lt 0001
AD
C (times
10ndash3
mm
2 s)
(b)
Figure 1 Estimated apparent diffusion coefficient (ADC) using monoexponential model in the transitional zone (TZ) (a) and peripheralzone (PZ) (b) of prostate +e change in ADC value for each choice of b-value from the other was found to be highly significant withplt 00001 using the one-way ANOVA test in both the regions
Prostate Cancer 3
4 Discussion and Conclusion
Choice of b-values can significantly influence ADC esti-mation using the monoexponential diffusion model in theprostate in agreement with variations in ADC found in the
literature [7 19 20] Our study shows a log-linear rela-tionship between ADC and b-values Using the log-linearrelationship derived from ADCs of the lower b-value(b 400 700 and 1000) ADCs for higher b-values (b 1500and 2000) can be extrapolated with a small relative error
04
06
08
1
12
0 1000 2000
1
15
2
25
0 500 1000 1500 2000
05
1
15
2
0 500 1000 1500 2000b-value (smm2) b-value (smm2)
b-value (smm2) b-value (smm2)
04
06
08
1
12
0 500 1000 1500 2000
ADCADC
1
15
2
25
0 1000 2000
05
1
15
2
0 1000 2000
sADC
b-value (smm2) b-value (smm2)
ADCADCsADC
ADCADCsADC
(a) (d)
(e)
(f)
(j)
(g)
(h)
(i)
(b)
(c)
sDWIb2000 ADCb2000 sADCb200090
70
50
30
10
Error
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
Figure 2 Log-linear relationship between ADC and b-value Example of log-linear model fit to targeted tissue of a 69-year-old patient withadenocarcinoma in peripheral zone (PZ) of prostate Axial DWI images of b-1000 with regions of interest (ROIs) in PZ lesion (a) normal PZ(b) normal transition zone (c) and corresponding graphs with b-value (x-axis) ADC (y-axis) and log-linear fit for each ROI (d e and f)+e plots (g) (h) and (i) show the log-linear model fit to ADC value at b-400 b-700 and b-1000 (black solid line) and extrapolation of sADCat b-1500 and b-2000(dotted line) Bottom row shows the sDWI ADC and sADC maps at b-2000 and color-coded error map of thecorresponding slice
4 Prostate Cancer
(10plusmn 5) Contrast ratio of lesion and normal tissue sig-nificantly increases in synthetic DW images
+e technique of generating synthetic ADC gives cli-nicians extra degrees of freedom with the choice of b-values +e optimal b-value for disease detection dependsupon image contrast that is likely to change with tissuetype and histological findings Rather than deciding theoptimal b-value prior to imaging to get optimal contrastbetween normal and cancer tissue the use of syntheticADCmay be able to modify the b-value and get the optimalimage contrast even after imaging Furthermore thetechnique allows extrapolation of ADC values for higher b-values which cannot be obtained by the computed DWImethod However this technique may not reduce theoverall scan time as in our scanning protocol the scanningtime to get three different b-values (b-400 700 and 1000)
is 1 min 39 sec and scanning time for one high b-value (b-2000) is 1 min 5 sec +is technique provides a method toobtain DW images and ADC values for a wide range of b-values
According to the diffusion equation b-value has a[time]3 dependency thus a very high b-value can beachieved in a clinical scanner with a moderate increase inthe echo time (TE) However the signal loss due to dif-fusion is a limiting factor at high b-values +e initialsignal-to-noise ratio (SNR) and the tissue diffusion de-termine how quickly the signal goes below the noise levelAs the tissue diffusivity is higher in normal tissue as comparedto cancer tissue normal region signal decay reaches to thenoise level at a relatively faster rate Hence the observed signalat high b-values is dominated by the noise and appears todecay at a slower rate +is explains the reason of significant
00
05
10
15
20
25
NS
ADC sADC
N = 15
AD
C (times
10ndash3
mm
2 s)
(a)
ADC sADC00
05
10
15
20
25
NS
N = 12
AD
C (times
10ndash3
mm
2 s)
(b)
00
05
10
15
20
25
ADC sADC
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(c)
ADC sADC00
05
10
15
20
25
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(d)
00
02
04
06
08
10
Con
tras
t rat
io
DWI sDWI
lowastlowast
(e)
DWI sDWI00
02
04
06
08
10
Con
tras
t rat
io
lowast
(f )
Figure 3 Inter-reader variation of ADC and contrast ratio +ere was no significant difference between ADC values and synthetic ADC(sADC) values in the lesion (a and b) at b-2000 +e difference between ADC and sADC in ROIs placed in normal tissue was significantlydifferent (c and d) However the contrast ratio of lesion and surrounding normal tissue increased significantly between DWI and sDWI forb-2000 (e and f) lowastplt 005 lowastlowastplt 001 +e top row shows the result of Reader 1 (N 15) and the bottom row shows that of Reader 2(N 12) (a) Reader 1 lesion (b) Reader 1 normal (c) Reader 1 DWI (b-2000) (d) Reader 2 lesion (e) Reader 2 normal (f ) Reader 2 DWI (b-2000)
Prostate Cancer 5
difference between ADC and sADC values at normal regionsAs DWI signal attenuation is exponentially dependent onADC small changes in ADC can make a significant change inDWI contrast this results in the significant increase of CR insDWI images as compared to DWI
+e present study demonstrates that although the higherb-value sDWI increases the contrast between lesion andnormal tissue the sADC shows similar contrast for b-1000b-1500 and b-2000 +is could be due to small cohort size ofthe patient with different Gleason scores consistent withresults in other studies [12 24] ADC computed from high b-value DWI has been shown to be more accurate in dis-tinguishing prostate lesions from benign and normal tissues[25 26] Further investigation could be done for the clinicalapplication of sDWI with larger patient populations One ofthe limitations of our study was MRI examinations were notcompared with a radical prostatectomy specimen Howeverimage-guided MR-overlayed biopsy could be a good alter-native to radical prostatectomy where patient refuses toundergo prostatectomy
Our initial investigation suggests that the ADC valuescorresponding to higher b-value DWI can be computedusing a log-linear relationship derived from lower b-values(ble 1000) Moreover this computational method can also
be manipulated to determine optimized b-values to createADC maps +e synthetic ADC technique could be a usefultool to provide optimized image contrast for quantitativeDW-MR imaging applications in oncology where ADC isroutinely used in clinical practice
Data Availability
+e data that support the findings of this study are availablefrom the corresponding author upon reasonable request
Disclosure
Partial results of this manuscript have been presented at theEuropean Society for Magnetic Resonance in Medicine andBiology (ESMRMB) 2017 Barcelona Spain with the ab-stract titled ldquoSynthetic Apparent Diffusion Coefficient forUltra High b-value DiffusionWeighted Imaging in Prostaterdquo(abstract number esmrmb201758233ce)
Conflicts of Interest
+e authors declare that they have no conflicts of interest
Malignant Benign00
05
10
15
20
sAD
C (times
10ndash3
mm
2 s)
lowast
(a)
Malignant BenignsA
DC
(times10
ndash3 m
m2 s
)
lowast
00
05
10
15
20
(b)
Malignant Benign
sAD
C (times
10ndash3
mm
2 s)
lowast
00
05
10
15
20
(c)
Figure 4 Comparison between synthetic ADC (sADC) values of malignant and benign tissue Distribution of sADC values for malignant(Gleason score 6 and 7 N 7) and benign lesions (Gleason score lt6 N 8) in patients at b-1000 (a) b-1500 (b) and b-2000 (c) +e centerhorizontal line indicates the median value lowastplt 005
Table 1 Comparison between sADC values in lesions with Gleason score (GS) lt6 and GS ge6 at b-1000 b-1500 and b-2000
MalignantGS (67)N 7
sADC (10minus 3mm2s)(meanplusmn SD)
BenignGSlt 6N 8
sADC (10minus 3mm2s)(meanplusmn SD)
95 CI p value
b-1000 0818plusmn 0067 1131plusmn 0084 0075ndash0550 00138lowastb-1500 0682plusmn 0059 1007plusmn 0090 0084ndash0567 00121lowastb-2000 0601plusmn 0057 0935plusmn 0094 0088ndash0581 00116lowastlowastStatistically significant 95 CI 95 confidence interval sADC synthetic apparent diffusion coefficient GS Gleason score
6 Prostate Cancer
References
[1] H A Vargas O Akin T Franiel et al ldquoDiffusion-weightedendorectal MR imaging at 3 T for prostate cancer tumordetection and assessment of aggressivenessrdquo Radiologyvol 259 no 3 pp 775ndash784 2011
[2] T Tamada V Prabhu J Li J S Babb S S Taneja andA B Rosenkrantz ldquoAssessment of prostate cancer aggres-siveness using apparent diffusion coefficient values impact ofpatient race and agerdquo Abdominal Radiology vol 42 no 6pp 1744ndash1751 2017
[3] T H Kim C K Kim B K Park et al ldquoRelationship betweenGleason score and apparent diffusion coefficients of diffusion-weighted magnetic resonance imaging in prostate cancerpatientsrdquo Canadian Urological Association Journal vol 10no 11-12 pp E377ndashE382 2016
[4] A Lebovici S A Sfrangeu D Feier et al ldquoEvaluation of thenormal-to-diseased apparent diffusion coefficient ratio as anindicator of prostate cancer aggressivenessrdquo BMC MedicalImaging vol 14 no 1 p 15 2014
[5] M Quentin D Blondin J Klasen et al ldquoComparison ofdifferent mathematical models of diffusion-weighted prostateMR imagingrdquo Magnetic Resonance Imaging vol 30 no 10pp 1468ndash1474 2012
[6] K M Bennett K M Schmainda R Bennett (Tong)D B Rowe H Lu and J S Hyde ldquoCharacterization ofcontinuously distributed cortical water diffusion rates with astretched-exponential modelrdquo Magnetic Resonance in Medi-cine vol 50 no 4 pp 727ndash734 2003
[7] M M Jafar A Parsai and M E Miquel ldquoDiffusion-weightedmagnetic resonance imaging in cancer reported apparentdiffusion coefficients in-vitro and in-vivo reproducibilityrdquoWorld Journal of Radiology vol 8 no 1 pp 21ndash49 2016
[8] C Kyo Kim B Kwan Park B Kim and C K Kim ldquoHigh-b-value diffusion-weighted imaging at 3 Tto detect prostate cancercomparisons between b values of 1000 and 2000 smm2rdquoAmerican Journal of Roentgenology vol 194 pp W33ndashW372010
[9] T de Perrot M Scheffler J Boto et al ldquoDiffusion in prostatecancer detection on a 3T scanner how many b-values areneededrdquo Journal of Magnetic Resonance Imaging vol 44no 3 pp 601ndash609 2016
[10] G Manenti M Nezzo F Chegai E Vasili E Bonanno andG Simonetti ldquoDWI of prostate cancer optimal b-value inclinical practicerdquo Prostate Cancer vol 2014 Article ID868269 9 pages 2014
[11] E U Saritas J H Lee and D G Nishimura ldquoSNR depen-dence of optimal parameters for apparent diffusion coefficientmeasurementsrdquo IEEE Transactions on Medical Imagingvol 30 no 2 pp 424ndash437 2011
[12] T Tamada N Kanomata T Sone et al ldquoHigh b value(2000 smm2) diffusion-weighted magnetic resonanceimaging in prostate cancer at 3 tesla comparison with 1000smm2 for tumor conspicuity and discrimination of ag-gressivenessrdquo PLoS One vol 9 Article ID e96619 2014
[13] K Katahira T Takahara T C Kwee et al ldquoUltra-high-b-value diffusion-weighted MR imaging for the detection ofprostate cancer evaluation in 201 cases with histopathologicalcorrelationrdquo European Radiology vol 21 no 1 pp 188ndash1962011
[14] Y Ueno S Takahashi K Kitajima et al ldquoComputed diffu-sion-weighted imaging using 3-Tmagnetic resonance imagingfor prostate cancer diagnosisrdquo European Radiology vol 23no 12 pp 3509ndash3516 2013
[15] M D Blackledge M O Leach D J Collins and D-M KohldquoComputed diffusion-weighted MR imaging may improvetumor detectionrdquo Radiology vol 261 no 2 pp 573ndash5812011
[16] M Takeuchi K Matsuzaki and M Harada ldquoComputeddiffusion-weighted imaging for differentiating decidualizedendometrioma from ovarian cancerrdquo European Journal ofRadiology vol 85 no 5 pp 1016ndash1019 2016
[17] Y Ueno S Takahashi Y Ohno et al ldquoComputed diffusion-weighted MRI for prostate cancer detection the influence ofthe combinations of b-valuesrdquo +e British Journal of Radi-ology vol 88 no 1048 Article ID 20140738 2015
[18] R Yoshida T Yoshizako T Katsube Y Tamaki N Ishikawaand H Kitagaki ldquoComputed diffusion-weighted imagingusing 15-T magnetic resonance imaging for prostate cancerdiagnosisrdquo Clinical Imaging vol 41 pp 78ndash82 2017
[19] G+ormer J Otto M Reiss-Zimmermann et al ldquoDiagnosticvalue of ADC in patients with prostate cancer influence of thechoice of b valuesrdquo European Radiology vol 22 no 8pp 1820ndash1828 2012
[20] Y Peng Y Jiang T Antic et al ldquoApparent diffusion coef-ficient for prostate cancer imaging impact of b valuesrdquoAmerican Journal of Roentgenology vol 202 no 3pp W247ndashW253 2014
[21] Y Oto A Afaq D B Rowe Y Lu A Shukla-Dave andJ Grover ldquoDiffusion-weighted magnetic resonance imagingof the prostate improved robustness with stretched expo-nential modelingrdquo Journal of Computer Assisted Tomographyvol 36 no 6 pp 695ndash703 2012
[22] M Iima and D Le Bihan ldquoClinical intravoxel incoherentmotion and diffusion MR imaging past present and futurerdquoRadiology vol 278 no 1 pp 13ndash32 2016
[23] Understanding Your Pathology Report Prostate Cancer[24] A B Rosenkrantz N Hindman R P Lim et al ldquoDiffusion-
weighted imaging of the prostate comparison of b1000 andb2000 image sets for index lesion detectionrdquo Journal ofMagnetic Resonance Imaging vol 38 no 3 pp 694ndash700 2013
[25] K Taneja Y Kaji K Kuroda and K Sugimura ldquoHigh b-valuediffusion-weighted imaging in normal and malignant pe-ripheral zone tissue of the prostate effect of signal-to-noiseratiordquo Magnetic Resonance in Medical Sciences vol 7 no 2pp 93ndash99 2008
[26] K Kitajima S Takahashi Y Ueno et al ldquoClinical utility ofapparent diffusion coefficient values obtained using highb-value when diagnosing prostate cancer using 3 tesla MRIcomparison between ultra-high b-value (2000 smm2) andstandard high b-value (1000 smm2)rdquo Journal of MagneticResonance Imaging vol 36 no 1 pp 198ndash205 2012
Prostate Cancer 7

23 Statistical Analysis ADC values for different b-valueswere computed using the monoexponential model (equation(1))voxel-wise Regions of interest (ROIs) of size(15ndash20mm2) were placed on the transitional zone (TZ) andperipheral zone (PZ) of the prostate for each patientVariations in the mean ADC value within the ROI withrespect to the b-values used for the quantification of ADCwere analyzed with a one-way ANOVA test +e log-linearmodel (equation (4))was fitted voxel-wise to the lower b-value ADCs (ADC0ndash400 ADC0ndash700 ADC0ndash1000) to estimatethe model parameters P1 and P2 Synthetic ADC (sADC)calculated from equation (4) for b-1500 and b-2000 wasextrapolated using themodel parameters and compared withthe true ADC0ndash1500 and ADC0ndash2000 +e error in the sADC atb-1500 and b-2000 relative to the observed ADC wascomputed as
relative error |ADC minus sADC|
ADCtimes 100 (5)
Synthetic DWI (sDWI) images for b-1500 and b-2000were generated using DWI of b0 and sADC using themonoexponential model and compared with originalDWI1500 and DWI2000 Contrast ratio (CR) between normaland lesion for DWI and sDWI were computed usingCR (Scancer minus Snormal tissue)(Scancer + Snormal tissue) CR fororiginal DWI and sDWI for b-1500 and b-2000 sADCvalues of malignant and benign lesions were assessed by apaired t-test p values lt005 were considered as statisticallysignificant Statistical analysis was performed using Prism(GraphPad Software Version 70)
24 Regions of Interest Regions of interest (ROIs) wereplaced at the normal appearing muscle area and at thelesion on the original DWI image and computed DWIimage Two radiologists one with 10 years of experienceand another with more than 20 years of experience blindedto each other and to histological finding placed the ROIsOverlapping of the ROIs from the two radiologists was
95 For cases with an area suspicious for tumor ROIswere placed on axial high b-value diffusion weighted im-ages (b 2000 smm2) on a hyperintense area suspicious fortumor and a normal intensity area within the gland on thesame image For cases in which the area suspicious fortumor was in the peripheral zone of the gland the normalintensity region of interest was selected from a location inthe peripheral zone on the same image For cases with noarea suspicious for tumor regions of interest were placed inthe relatively hyperintense peripheral zone and in thetransition zonemdashwhich is normally hypointense to theperipheral zonemdashon the same image
3 Results
In the one-way ANOVA test ADC shows highly significantchange (plt 00001) with respect to the b-value both in thetransitional zone (TZ) and peripheral zone (PZ) (Figure 1)of the prostate in all the patient data +is observationsupports our initial assumption that the ADC is notconstant with respect to b-values +e log-linear modelgives the best fit to the data (R2sim09) from the prostatetissue (Figure 2)
No significant difference was observed in the paired t-testbetween sADC as compared to actual ADC in the prostatelesions however the change was significant in the normaltissue (plt 0001) at b-2000 Contrast ratio increased signif-icantly between original DWI images and sDWI images(p 0002) (Figure 3)
Mean sADC of prostate lesions was significantly lowerthan that of surrounding normal tissue (plt 0001) for b-2000 when considered for all data (N 15) A significantlylower sADC was observed using an independent t-test inmalignant lesions (GS 67) as compared to benign lesions(GSlt 6) (Figure 4) In addition sADC at b-1000 b-1500and b-2000 was found to be significantly distinguish lesionswith GSlt 6 from the lesions with GSge 6 +e mean sADCvalue confidence interval (CI) and the p values are given inTable 1
0
1
2
3
4
b0-2
00
b0-4
00
b0-2
000
b0-1
500
b0-1
000
b0-7
00
N = 15p lt 0001
AD
C (times
10ndash3
mm
2 s)
(a)
0
2
4
6
8
b0-2
00
b0-4
00
b0-2
000
b0-1
500
b0-1
000
b0-7
00
N = 15p lt 0001
AD
C (times
10ndash3
mm
2 s)
(b)
Figure 1 Estimated apparent diffusion coefficient (ADC) using monoexponential model in the transitional zone (TZ) (a) and peripheralzone (PZ) (b) of prostate +e change in ADC value for each choice of b-value from the other was found to be highly significant withplt 00001 using the one-way ANOVA test in both the regions
Prostate Cancer 3
4 Discussion and Conclusion
Choice of b-values can significantly influence ADC esti-mation using the monoexponential diffusion model in theprostate in agreement with variations in ADC found in the
literature [7 19 20] Our study shows a log-linear rela-tionship between ADC and b-values Using the log-linearrelationship derived from ADCs of the lower b-value(b 400 700 and 1000) ADCs for higher b-values (b 1500and 2000) can be extrapolated with a small relative error
04
06
08
1
12
0 1000 2000
1
15
2
25
0 500 1000 1500 2000
05
1
15
2
0 500 1000 1500 2000b-value (smm2) b-value (smm2)
b-value (smm2) b-value (smm2)
04
06
08
1
12
0 500 1000 1500 2000
ADCADC
1
15
2
25
0 1000 2000
05
1
15
2
0 1000 2000
sADC
b-value (smm2) b-value (smm2)
ADCADCsADC
ADCADCsADC
(a) (d)
(e)
(f)
(j)
(g)
(h)
(i)
(b)
(c)
sDWIb2000 ADCb2000 sADCb200090
70
50
30
10
Error
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
Figure 2 Log-linear relationship between ADC and b-value Example of log-linear model fit to targeted tissue of a 69-year-old patient withadenocarcinoma in peripheral zone (PZ) of prostate Axial DWI images of b-1000 with regions of interest (ROIs) in PZ lesion (a) normal PZ(b) normal transition zone (c) and corresponding graphs with b-value (x-axis) ADC (y-axis) and log-linear fit for each ROI (d e and f)+e plots (g) (h) and (i) show the log-linear model fit to ADC value at b-400 b-700 and b-1000 (black solid line) and extrapolation of sADCat b-1500 and b-2000(dotted line) Bottom row shows the sDWI ADC and sADC maps at b-2000 and color-coded error map of thecorresponding slice
4 Prostate Cancer
(10plusmn 5) Contrast ratio of lesion and normal tissue sig-nificantly increases in synthetic DW images
+e technique of generating synthetic ADC gives cli-nicians extra degrees of freedom with the choice of b-values +e optimal b-value for disease detection dependsupon image contrast that is likely to change with tissuetype and histological findings Rather than deciding theoptimal b-value prior to imaging to get optimal contrastbetween normal and cancer tissue the use of syntheticADCmay be able to modify the b-value and get the optimalimage contrast even after imaging Furthermore thetechnique allows extrapolation of ADC values for higher b-values which cannot be obtained by the computed DWImethod However this technique may not reduce theoverall scan time as in our scanning protocol the scanningtime to get three different b-values (b-400 700 and 1000)
is 1 min 39 sec and scanning time for one high b-value (b-2000) is 1 min 5 sec +is technique provides a method toobtain DW images and ADC values for a wide range of b-values
According to the diffusion equation b-value has a[time]3 dependency thus a very high b-value can beachieved in a clinical scanner with a moderate increase inthe echo time (TE) However the signal loss due to dif-fusion is a limiting factor at high b-values +e initialsignal-to-noise ratio (SNR) and the tissue diffusion de-termine how quickly the signal goes below the noise levelAs the tissue diffusivity is higher in normal tissue as comparedto cancer tissue normal region signal decay reaches to thenoise level at a relatively faster rate Hence the observed signalat high b-values is dominated by the noise and appears todecay at a slower rate +is explains the reason of significant
00
05
10
15
20
25
NS
ADC sADC
N = 15
AD
C (times
10ndash3
mm
2 s)
(a)
ADC sADC00
05
10
15
20
25
NS
N = 12
AD
C (times
10ndash3
mm
2 s)
(b)
00
05
10
15
20
25
ADC sADC
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(c)
ADC sADC00
05
10
15
20
25
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(d)
00
02
04
06
08
10
Con
tras
t rat
io
DWI sDWI
lowastlowast
(e)
DWI sDWI00
02
04
06
08
10
Con
tras
t rat
io
lowast
(f )
Figure 3 Inter-reader variation of ADC and contrast ratio +ere was no significant difference between ADC values and synthetic ADC(sADC) values in the lesion (a and b) at b-2000 +e difference between ADC and sADC in ROIs placed in normal tissue was significantlydifferent (c and d) However the contrast ratio of lesion and surrounding normal tissue increased significantly between DWI and sDWI forb-2000 (e and f) lowastplt 005 lowastlowastplt 001 +e top row shows the result of Reader 1 (N 15) and the bottom row shows that of Reader 2(N 12) (a) Reader 1 lesion (b) Reader 1 normal (c) Reader 1 DWI (b-2000) (d) Reader 2 lesion (e) Reader 2 normal (f ) Reader 2 DWI (b-2000)
Prostate Cancer 5
difference between ADC and sADC values at normal regionsAs DWI signal attenuation is exponentially dependent onADC small changes in ADC can make a significant change inDWI contrast this results in the significant increase of CR insDWI images as compared to DWI
+e present study demonstrates that although the higherb-value sDWI increases the contrast between lesion andnormal tissue the sADC shows similar contrast for b-1000b-1500 and b-2000 +is could be due to small cohort size ofthe patient with different Gleason scores consistent withresults in other studies [12 24] ADC computed from high b-value DWI has been shown to be more accurate in dis-tinguishing prostate lesions from benign and normal tissues[25 26] Further investigation could be done for the clinicalapplication of sDWI with larger patient populations One ofthe limitations of our study was MRI examinations were notcompared with a radical prostatectomy specimen Howeverimage-guided MR-overlayed biopsy could be a good alter-native to radical prostatectomy where patient refuses toundergo prostatectomy
Our initial investigation suggests that the ADC valuescorresponding to higher b-value DWI can be computedusing a log-linear relationship derived from lower b-values(ble 1000) Moreover this computational method can also
be manipulated to determine optimized b-values to createADC maps +e synthetic ADC technique could be a usefultool to provide optimized image contrast for quantitativeDW-MR imaging applications in oncology where ADC isroutinely used in clinical practice
Data Availability
+e data that support the findings of this study are availablefrom the corresponding author upon reasonable request
Disclosure
Partial results of this manuscript have been presented at theEuropean Society for Magnetic Resonance in Medicine andBiology (ESMRMB) 2017 Barcelona Spain with the ab-stract titled ldquoSynthetic Apparent Diffusion Coefficient forUltra High b-value DiffusionWeighted Imaging in Prostaterdquo(abstract number esmrmb201758233ce)
Conflicts of Interest
+e authors declare that they have no conflicts of interest
Malignant Benign00
05
10
15
20
sAD
C (times
10ndash3
mm
2 s)
lowast
(a)
Malignant BenignsA
DC
(times10
ndash3 m
m2 s
)
lowast
00
05
10
15
20
(b)
Malignant Benign
sAD
C (times
10ndash3
mm
2 s)
lowast
00
05
10
15
20
(c)
Figure 4 Comparison between synthetic ADC (sADC) values of malignant and benign tissue Distribution of sADC values for malignant(Gleason score 6 and 7 N 7) and benign lesions (Gleason score lt6 N 8) in patients at b-1000 (a) b-1500 (b) and b-2000 (c) +e centerhorizontal line indicates the median value lowastplt 005
Table 1 Comparison between sADC values in lesions with Gleason score (GS) lt6 and GS ge6 at b-1000 b-1500 and b-2000
MalignantGS (67)N 7
sADC (10minus 3mm2s)(meanplusmn SD)
BenignGSlt 6N 8
sADC (10minus 3mm2s)(meanplusmn SD)
95 CI p value
b-1000 0818plusmn 0067 1131plusmn 0084 0075ndash0550 00138lowastb-1500 0682plusmn 0059 1007plusmn 0090 0084ndash0567 00121lowastb-2000 0601plusmn 0057 0935plusmn 0094 0088ndash0581 00116lowastlowastStatistically significant 95 CI 95 confidence interval sADC synthetic apparent diffusion coefficient GS Gleason score
6 Prostate Cancer
References
[1] H A Vargas O Akin T Franiel et al ldquoDiffusion-weightedendorectal MR imaging at 3 T for prostate cancer tumordetection and assessment of aggressivenessrdquo Radiologyvol 259 no 3 pp 775ndash784 2011
[2] T Tamada V Prabhu J Li J S Babb S S Taneja andA B Rosenkrantz ldquoAssessment of prostate cancer aggres-siveness using apparent diffusion coefficient values impact ofpatient race and agerdquo Abdominal Radiology vol 42 no 6pp 1744ndash1751 2017
[3] T H Kim C K Kim B K Park et al ldquoRelationship betweenGleason score and apparent diffusion coefficients of diffusion-weighted magnetic resonance imaging in prostate cancerpatientsrdquo Canadian Urological Association Journal vol 10no 11-12 pp E377ndashE382 2016
[4] A Lebovici S A Sfrangeu D Feier et al ldquoEvaluation of thenormal-to-diseased apparent diffusion coefficient ratio as anindicator of prostate cancer aggressivenessrdquo BMC MedicalImaging vol 14 no 1 p 15 2014
[5] M Quentin D Blondin J Klasen et al ldquoComparison ofdifferent mathematical models of diffusion-weighted prostateMR imagingrdquo Magnetic Resonance Imaging vol 30 no 10pp 1468ndash1474 2012
[6] K M Bennett K M Schmainda R Bennett (Tong)D B Rowe H Lu and J S Hyde ldquoCharacterization ofcontinuously distributed cortical water diffusion rates with astretched-exponential modelrdquo Magnetic Resonance in Medi-cine vol 50 no 4 pp 727ndash734 2003
[7] M M Jafar A Parsai and M E Miquel ldquoDiffusion-weightedmagnetic resonance imaging in cancer reported apparentdiffusion coefficients in-vitro and in-vivo reproducibilityrdquoWorld Journal of Radiology vol 8 no 1 pp 21ndash49 2016
[8] C Kyo Kim B Kwan Park B Kim and C K Kim ldquoHigh-b-value diffusion-weighted imaging at 3 Tto detect prostate cancercomparisons between b values of 1000 and 2000 smm2rdquoAmerican Journal of Roentgenology vol 194 pp W33ndashW372010
[9] T de Perrot M Scheffler J Boto et al ldquoDiffusion in prostatecancer detection on a 3T scanner how many b-values areneededrdquo Journal of Magnetic Resonance Imaging vol 44no 3 pp 601ndash609 2016
[10] G Manenti M Nezzo F Chegai E Vasili E Bonanno andG Simonetti ldquoDWI of prostate cancer optimal b-value inclinical practicerdquo Prostate Cancer vol 2014 Article ID868269 9 pages 2014
[11] E U Saritas J H Lee and D G Nishimura ldquoSNR depen-dence of optimal parameters for apparent diffusion coefficientmeasurementsrdquo IEEE Transactions on Medical Imagingvol 30 no 2 pp 424ndash437 2011
[12] T Tamada N Kanomata T Sone et al ldquoHigh b value(2000 smm2) diffusion-weighted magnetic resonanceimaging in prostate cancer at 3 tesla comparison with 1000smm2 for tumor conspicuity and discrimination of ag-gressivenessrdquo PLoS One vol 9 Article ID e96619 2014
[13] K Katahira T Takahara T C Kwee et al ldquoUltra-high-b-value diffusion-weighted MR imaging for the detection ofprostate cancer evaluation in 201 cases with histopathologicalcorrelationrdquo European Radiology vol 21 no 1 pp 188ndash1962011
[14] Y Ueno S Takahashi K Kitajima et al ldquoComputed diffu-sion-weighted imaging using 3-Tmagnetic resonance imagingfor prostate cancer diagnosisrdquo European Radiology vol 23no 12 pp 3509ndash3516 2013
[15] M D Blackledge M O Leach D J Collins and D-M KohldquoComputed diffusion-weighted MR imaging may improvetumor detectionrdquo Radiology vol 261 no 2 pp 573ndash5812011
[16] M Takeuchi K Matsuzaki and M Harada ldquoComputeddiffusion-weighted imaging for differentiating decidualizedendometrioma from ovarian cancerrdquo European Journal ofRadiology vol 85 no 5 pp 1016ndash1019 2016
[17] Y Ueno S Takahashi Y Ohno et al ldquoComputed diffusion-weighted MRI for prostate cancer detection the influence ofthe combinations of b-valuesrdquo +e British Journal of Radi-ology vol 88 no 1048 Article ID 20140738 2015
[18] R Yoshida T Yoshizako T Katsube Y Tamaki N Ishikawaand H Kitagaki ldquoComputed diffusion-weighted imagingusing 15-T magnetic resonance imaging for prostate cancerdiagnosisrdquo Clinical Imaging vol 41 pp 78ndash82 2017
[19] G+ormer J Otto M Reiss-Zimmermann et al ldquoDiagnosticvalue of ADC in patients with prostate cancer influence of thechoice of b valuesrdquo European Radiology vol 22 no 8pp 1820ndash1828 2012
[20] Y Peng Y Jiang T Antic et al ldquoApparent diffusion coef-ficient for prostate cancer imaging impact of b valuesrdquoAmerican Journal of Roentgenology vol 202 no 3pp W247ndashW253 2014
[21] Y Oto A Afaq D B Rowe Y Lu A Shukla-Dave andJ Grover ldquoDiffusion-weighted magnetic resonance imagingof the prostate improved robustness with stretched expo-nential modelingrdquo Journal of Computer Assisted Tomographyvol 36 no 6 pp 695ndash703 2012
[22] M Iima and D Le Bihan ldquoClinical intravoxel incoherentmotion and diffusion MR imaging past present and futurerdquoRadiology vol 278 no 1 pp 13ndash32 2016
[23] Understanding Your Pathology Report Prostate Cancer[24] A B Rosenkrantz N Hindman R P Lim et al ldquoDiffusion-
weighted imaging of the prostate comparison of b1000 andb2000 image sets for index lesion detectionrdquo Journal ofMagnetic Resonance Imaging vol 38 no 3 pp 694ndash700 2013
[25] K Taneja Y Kaji K Kuroda and K Sugimura ldquoHigh b-valuediffusion-weighted imaging in normal and malignant pe-ripheral zone tissue of the prostate effect of signal-to-noiseratiordquo Magnetic Resonance in Medical Sciences vol 7 no 2pp 93ndash99 2008
[26] K Kitajima S Takahashi Y Ueno et al ldquoClinical utility ofapparent diffusion coefficient values obtained using highb-value when diagnosing prostate cancer using 3 tesla MRIcomparison between ultra-high b-value (2000 smm2) andstandard high b-value (1000 smm2)rdquo Journal of MagneticResonance Imaging vol 36 no 1 pp 198ndash205 2012
Prostate Cancer 7

4 Discussion and Conclusion
Choice of b-values can significantly influence ADC esti-mation using the monoexponential diffusion model in theprostate in agreement with variations in ADC found in the
literature [7 19 20] Our study shows a log-linear rela-tionship between ADC and b-values Using the log-linearrelationship derived from ADCs of the lower b-value(b 400 700 and 1000) ADCs for higher b-values (b 1500and 2000) can be extrapolated with a small relative error
04
06
08
1
12
0 1000 2000
1
15
2
25
0 500 1000 1500 2000
05
1
15
2
0 500 1000 1500 2000b-value (smm2) b-value (smm2)
b-value (smm2) b-value (smm2)
04
06
08
1
12
0 500 1000 1500 2000
ADCADC
1
15
2
25
0 1000 2000
05
1
15
2
0 1000 2000
sADC
b-value (smm2) b-value (smm2)
ADCADCsADC
ADCADCsADC
(a) (d)
(e)
(f)
(j)
(g)
(h)
(i)
(b)
(c)
sDWIb2000 ADCb2000 sADCb200090
70
50
30
10
Error
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
AD
C (times
10ndash3
mm
2 s)
Figure 2 Log-linear relationship between ADC and b-value Example of log-linear model fit to targeted tissue of a 69-year-old patient withadenocarcinoma in peripheral zone (PZ) of prostate Axial DWI images of b-1000 with regions of interest (ROIs) in PZ lesion (a) normal PZ(b) normal transition zone (c) and corresponding graphs with b-value (x-axis) ADC (y-axis) and log-linear fit for each ROI (d e and f)+e plots (g) (h) and (i) show the log-linear model fit to ADC value at b-400 b-700 and b-1000 (black solid line) and extrapolation of sADCat b-1500 and b-2000(dotted line) Bottom row shows the sDWI ADC and sADC maps at b-2000 and color-coded error map of thecorresponding slice
4 Prostate Cancer
(10plusmn 5) Contrast ratio of lesion and normal tissue sig-nificantly increases in synthetic DW images
+e technique of generating synthetic ADC gives cli-nicians extra degrees of freedom with the choice of b-values +e optimal b-value for disease detection dependsupon image contrast that is likely to change with tissuetype and histological findings Rather than deciding theoptimal b-value prior to imaging to get optimal contrastbetween normal and cancer tissue the use of syntheticADCmay be able to modify the b-value and get the optimalimage contrast even after imaging Furthermore thetechnique allows extrapolation of ADC values for higher b-values which cannot be obtained by the computed DWImethod However this technique may not reduce theoverall scan time as in our scanning protocol the scanningtime to get three different b-values (b-400 700 and 1000)
is 1 min 39 sec and scanning time for one high b-value (b-2000) is 1 min 5 sec +is technique provides a method toobtain DW images and ADC values for a wide range of b-values
According to the diffusion equation b-value has a[time]3 dependency thus a very high b-value can beachieved in a clinical scanner with a moderate increase inthe echo time (TE) However the signal loss due to dif-fusion is a limiting factor at high b-values +e initialsignal-to-noise ratio (SNR) and the tissue diffusion de-termine how quickly the signal goes below the noise levelAs the tissue diffusivity is higher in normal tissue as comparedto cancer tissue normal region signal decay reaches to thenoise level at a relatively faster rate Hence the observed signalat high b-values is dominated by the noise and appears todecay at a slower rate +is explains the reason of significant
00
05
10
15
20
25
NS
ADC sADC
N = 15
AD
C (times
10ndash3
mm
2 s)
(a)
ADC sADC00
05
10
15
20
25
NS
N = 12
AD
C (times
10ndash3
mm
2 s)
(b)
00
05
10
15
20
25
ADC sADC
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(c)
ADC sADC00
05
10
15
20
25
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(d)
00
02
04
06
08
10
Con
tras
t rat
io
DWI sDWI
lowastlowast
(e)
DWI sDWI00
02
04
06
08
10
Con
tras
t rat
io
lowast
(f )
Figure 3 Inter-reader variation of ADC and contrast ratio +ere was no significant difference between ADC values and synthetic ADC(sADC) values in the lesion (a and b) at b-2000 +e difference between ADC and sADC in ROIs placed in normal tissue was significantlydifferent (c and d) However the contrast ratio of lesion and surrounding normal tissue increased significantly between DWI and sDWI forb-2000 (e and f) lowastplt 005 lowastlowastplt 001 +e top row shows the result of Reader 1 (N 15) and the bottom row shows that of Reader 2(N 12) (a) Reader 1 lesion (b) Reader 1 normal (c) Reader 1 DWI (b-2000) (d) Reader 2 lesion (e) Reader 2 normal (f ) Reader 2 DWI (b-2000)
Prostate Cancer 5
difference between ADC and sADC values at normal regionsAs DWI signal attenuation is exponentially dependent onADC small changes in ADC can make a significant change inDWI contrast this results in the significant increase of CR insDWI images as compared to DWI
+e present study demonstrates that although the higherb-value sDWI increases the contrast between lesion andnormal tissue the sADC shows similar contrast for b-1000b-1500 and b-2000 +is could be due to small cohort size ofthe patient with different Gleason scores consistent withresults in other studies [12 24] ADC computed from high b-value DWI has been shown to be more accurate in dis-tinguishing prostate lesions from benign and normal tissues[25 26] Further investigation could be done for the clinicalapplication of sDWI with larger patient populations One ofthe limitations of our study was MRI examinations were notcompared with a radical prostatectomy specimen Howeverimage-guided MR-overlayed biopsy could be a good alter-native to radical prostatectomy where patient refuses toundergo prostatectomy
Our initial investigation suggests that the ADC valuescorresponding to higher b-value DWI can be computedusing a log-linear relationship derived from lower b-values(ble 1000) Moreover this computational method can also
be manipulated to determine optimized b-values to createADC maps +e synthetic ADC technique could be a usefultool to provide optimized image contrast for quantitativeDW-MR imaging applications in oncology where ADC isroutinely used in clinical practice
Data Availability
+e data that support the findings of this study are availablefrom the corresponding author upon reasonable request
Disclosure
Partial results of this manuscript have been presented at theEuropean Society for Magnetic Resonance in Medicine andBiology (ESMRMB) 2017 Barcelona Spain with the ab-stract titled ldquoSynthetic Apparent Diffusion Coefficient forUltra High b-value DiffusionWeighted Imaging in Prostaterdquo(abstract number esmrmb201758233ce)
Conflicts of Interest
+e authors declare that they have no conflicts of interest
Malignant Benign00
05
10
15
20
sAD
C (times
10ndash3
mm
2 s)
lowast
(a)
Malignant BenignsA
DC
(times10
ndash3 m
m2 s
)
lowast
00
05
10
15
20
(b)
Malignant Benign
sAD
C (times
10ndash3
mm
2 s)
lowast
00
05
10
15
20
(c)
Figure 4 Comparison between synthetic ADC (sADC) values of malignant and benign tissue Distribution of sADC values for malignant(Gleason score 6 and 7 N 7) and benign lesions (Gleason score lt6 N 8) in patients at b-1000 (a) b-1500 (b) and b-2000 (c) +e centerhorizontal line indicates the median value lowastplt 005
Table 1 Comparison between sADC values in lesions with Gleason score (GS) lt6 and GS ge6 at b-1000 b-1500 and b-2000
MalignantGS (67)N 7
sADC (10minus 3mm2s)(meanplusmn SD)
BenignGSlt 6N 8
sADC (10minus 3mm2s)(meanplusmn SD)
95 CI p value
b-1000 0818plusmn 0067 1131plusmn 0084 0075ndash0550 00138lowastb-1500 0682plusmn 0059 1007plusmn 0090 0084ndash0567 00121lowastb-2000 0601plusmn 0057 0935plusmn 0094 0088ndash0581 00116lowastlowastStatistically significant 95 CI 95 confidence interval sADC synthetic apparent diffusion coefficient GS Gleason score
6 Prostate Cancer
References
[1] H A Vargas O Akin T Franiel et al ldquoDiffusion-weightedendorectal MR imaging at 3 T for prostate cancer tumordetection and assessment of aggressivenessrdquo Radiologyvol 259 no 3 pp 775ndash784 2011
[2] T Tamada V Prabhu J Li J S Babb S S Taneja andA B Rosenkrantz ldquoAssessment of prostate cancer aggres-siveness using apparent diffusion coefficient values impact ofpatient race and agerdquo Abdominal Radiology vol 42 no 6pp 1744ndash1751 2017
[3] T H Kim C K Kim B K Park et al ldquoRelationship betweenGleason score and apparent diffusion coefficients of diffusion-weighted magnetic resonance imaging in prostate cancerpatientsrdquo Canadian Urological Association Journal vol 10no 11-12 pp E377ndashE382 2016
[4] A Lebovici S A Sfrangeu D Feier et al ldquoEvaluation of thenormal-to-diseased apparent diffusion coefficient ratio as anindicator of prostate cancer aggressivenessrdquo BMC MedicalImaging vol 14 no 1 p 15 2014
[5] M Quentin D Blondin J Klasen et al ldquoComparison ofdifferent mathematical models of diffusion-weighted prostateMR imagingrdquo Magnetic Resonance Imaging vol 30 no 10pp 1468ndash1474 2012
[6] K M Bennett K M Schmainda R Bennett (Tong)D B Rowe H Lu and J S Hyde ldquoCharacterization ofcontinuously distributed cortical water diffusion rates with astretched-exponential modelrdquo Magnetic Resonance in Medi-cine vol 50 no 4 pp 727ndash734 2003
[7] M M Jafar A Parsai and M E Miquel ldquoDiffusion-weightedmagnetic resonance imaging in cancer reported apparentdiffusion coefficients in-vitro and in-vivo reproducibilityrdquoWorld Journal of Radiology vol 8 no 1 pp 21ndash49 2016
[8] C Kyo Kim B Kwan Park B Kim and C K Kim ldquoHigh-b-value diffusion-weighted imaging at 3 Tto detect prostate cancercomparisons between b values of 1000 and 2000 smm2rdquoAmerican Journal of Roentgenology vol 194 pp W33ndashW372010
[9] T de Perrot M Scheffler J Boto et al ldquoDiffusion in prostatecancer detection on a 3T scanner how many b-values areneededrdquo Journal of Magnetic Resonance Imaging vol 44no 3 pp 601ndash609 2016
[10] G Manenti M Nezzo F Chegai E Vasili E Bonanno andG Simonetti ldquoDWI of prostate cancer optimal b-value inclinical practicerdquo Prostate Cancer vol 2014 Article ID868269 9 pages 2014
[11] E U Saritas J H Lee and D G Nishimura ldquoSNR depen-dence of optimal parameters for apparent diffusion coefficientmeasurementsrdquo IEEE Transactions on Medical Imagingvol 30 no 2 pp 424ndash437 2011
[12] T Tamada N Kanomata T Sone et al ldquoHigh b value(2000 smm2) diffusion-weighted magnetic resonanceimaging in prostate cancer at 3 tesla comparison with 1000smm2 for tumor conspicuity and discrimination of ag-gressivenessrdquo PLoS One vol 9 Article ID e96619 2014
[13] K Katahira T Takahara T C Kwee et al ldquoUltra-high-b-value diffusion-weighted MR imaging for the detection ofprostate cancer evaluation in 201 cases with histopathologicalcorrelationrdquo European Radiology vol 21 no 1 pp 188ndash1962011
[14] Y Ueno S Takahashi K Kitajima et al ldquoComputed diffu-sion-weighted imaging using 3-Tmagnetic resonance imagingfor prostate cancer diagnosisrdquo European Radiology vol 23no 12 pp 3509ndash3516 2013
[15] M D Blackledge M O Leach D J Collins and D-M KohldquoComputed diffusion-weighted MR imaging may improvetumor detectionrdquo Radiology vol 261 no 2 pp 573ndash5812011
[16] M Takeuchi K Matsuzaki and M Harada ldquoComputeddiffusion-weighted imaging for differentiating decidualizedendometrioma from ovarian cancerrdquo European Journal ofRadiology vol 85 no 5 pp 1016ndash1019 2016
[17] Y Ueno S Takahashi Y Ohno et al ldquoComputed diffusion-weighted MRI for prostate cancer detection the influence ofthe combinations of b-valuesrdquo +e British Journal of Radi-ology vol 88 no 1048 Article ID 20140738 2015
[18] R Yoshida T Yoshizako T Katsube Y Tamaki N Ishikawaand H Kitagaki ldquoComputed diffusion-weighted imagingusing 15-T magnetic resonance imaging for prostate cancerdiagnosisrdquo Clinical Imaging vol 41 pp 78ndash82 2017
[19] G+ormer J Otto M Reiss-Zimmermann et al ldquoDiagnosticvalue of ADC in patients with prostate cancer influence of thechoice of b valuesrdquo European Radiology vol 22 no 8pp 1820ndash1828 2012
[20] Y Peng Y Jiang T Antic et al ldquoApparent diffusion coef-ficient for prostate cancer imaging impact of b valuesrdquoAmerican Journal of Roentgenology vol 202 no 3pp W247ndashW253 2014
[21] Y Oto A Afaq D B Rowe Y Lu A Shukla-Dave andJ Grover ldquoDiffusion-weighted magnetic resonance imagingof the prostate improved robustness with stretched expo-nential modelingrdquo Journal of Computer Assisted Tomographyvol 36 no 6 pp 695ndash703 2012
[22] M Iima and D Le Bihan ldquoClinical intravoxel incoherentmotion and diffusion MR imaging past present and futurerdquoRadiology vol 278 no 1 pp 13ndash32 2016
[23] Understanding Your Pathology Report Prostate Cancer[24] A B Rosenkrantz N Hindman R P Lim et al ldquoDiffusion-
weighted imaging of the prostate comparison of b1000 andb2000 image sets for index lesion detectionrdquo Journal ofMagnetic Resonance Imaging vol 38 no 3 pp 694ndash700 2013
[25] K Taneja Y Kaji K Kuroda and K Sugimura ldquoHigh b-valuediffusion-weighted imaging in normal and malignant pe-ripheral zone tissue of the prostate effect of signal-to-noiseratiordquo Magnetic Resonance in Medical Sciences vol 7 no 2pp 93ndash99 2008
[26] K Kitajima S Takahashi Y Ueno et al ldquoClinical utility ofapparent diffusion coefficient values obtained using highb-value when diagnosing prostate cancer using 3 tesla MRIcomparison between ultra-high b-value (2000 smm2) andstandard high b-value (1000 smm2)rdquo Journal of MagneticResonance Imaging vol 36 no 1 pp 198ndash205 2012
Prostate Cancer 7

(10plusmn 5) Contrast ratio of lesion and normal tissue sig-nificantly increases in synthetic DW images
+e technique of generating synthetic ADC gives cli-nicians extra degrees of freedom with the choice of b-values +e optimal b-value for disease detection dependsupon image contrast that is likely to change with tissuetype and histological findings Rather than deciding theoptimal b-value prior to imaging to get optimal contrastbetween normal and cancer tissue the use of syntheticADCmay be able to modify the b-value and get the optimalimage contrast even after imaging Furthermore thetechnique allows extrapolation of ADC values for higher b-values which cannot be obtained by the computed DWImethod However this technique may not reduce theoverall scan time as in our scanning protocol the scanningtime to get three different b-values (b-400 700 and 1000)
is 1 min 39 sec and scanning time for one high b-value (b-2000) is 1 min 5 sec +is technique provides a method toobtain DW images and ADC values for a wide range of b-values
According to the diffusion equation b-value has a[time]3 dependency thus a very high b-value can beachieved in a clinical scanner with a moderate increase inthe echo time (TE) However the signal loss due to dif-fusion is a limiting factor at high b-values +e initialsignal-to-noise ratio (SNR) and the tissue diffusion de-termine how quickly the signal goes below the noise levelAs the tissue diffusivity is higher in normal tissue as comparedto cancer tissue normal region signal decay reaches to thenoise level at a relatively faster rate Hence the observed signalat high b-values is dominated by the noise and appears todecay at a slower rate +is explains the reason of significant
00
05
10
15
20
25
NS
ADC sADC
N = 15
AD
C (times
10ndash3
mm
2 s)
(a)
ADC sADC00
05
10
15
20
25
NS
N = 12
AD
C (times
10ndash3
mm
2 s)
(b)
00
05
10
15
20
25
ADC sADC
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(c)
ADC sADC00
05
10
15
20
25
AD
C (times
10ndash3
mm
2 s)
lowastlowast
(d)
00
02
04
06
08
10
Con
tras
t rat
io
DWI sDWI
lowastlowast
(e)
DWI sDWI00
02
04
06
08
10
Con
tras
t rat
io
lowast
(f )
Figure 3 Inter-reader variation of ADC and contrast ratio +ere was no significant difference between ADC values and synthetic ADC(sADC) values in the lesion (a and b) at b-2000 +e difference between ADC and sADC in ROIs placed in normal tissue was significantlydifferent (c and d) However the contrast ratio of lesion and surrounding normal tissue increased significantly between DWI and sDWI forb-2000 (e and f) lowastplt 005 lowastlowastplt 001 +e top row shows the result of Reader 1 (N 15) and the bottom row shows that of Reader 2(N 12) (a) Reader 1 lesion (b) Reader 1 normal (c) Reader 1 DWI (b-2000) (d) Reader 2 lesion (e) Reader 2 normal (f ) Reader 2 DWI (b-2000)
Prostate Cancer 5
difference between ADC and sADC values at normal regionsAs DWI signal attenuation is exponentially dependent onADC small changes in ADC can make a significant change inDWI contrast this results in the significant increase of CR insDWI images as compared to DWI
+e present study demonstrates that although the higherb-value sDWI increases the contrast between lesion andnormal tissue the sADC shows similar contrast for b-1000b-1500 and b-2000 +is could be due to small cohort size ofthe patient with different Gleason scores consistent withresults in other studies [12 24] ADC computed from high b-value DWI has been shown to be more accurate in dis-tinguishing prostate lesions from benign and normal tissues[25 26] Further investigation could be done for the clinicalapplication of sDWI with larger patient populations One ofthe limitations of our study was MRI examinations were notcompared with a radical prostatectomy specimen Howeverimage-guided MR-overlayed biopsy could be a good alter-native to radical prostatectomy where patient refuses toundergo prostatectomy
Our initial investigation suggests that the ADC valuescorresponding to higher b-value DWI can be computedusing a log-linear relationship derived from lower b-values(ble 1000) Moreover this computational method can also
be manipulated to determine optimized b-values to createADC maps +e synthetic ADC technique could be a usefultool to provide optimized image contrast for quantitativeDW-MR imaging applications in oncology where ADC isroutinely used in clinical practice
Data Availability
+e data that support the findings of this study are availablefrom the corresponding author upon reasonable request
Disclosure
Partial results of this manuscript have been presented at theEuropean Society for Magnetic Resonance in Medicine andBiology (ESMRMB) 2017 Barcelona Spain with the ab-stract titled ldquoSynthetic Apparent Diffusion Coefficient forUltra High b-value DiffusionWeighted Imaging in Prostaterdquo(abstract number esmrmb201758233ce)
Conflicts of Interest
+e authors declare that they have no conflicts of interest
Malignant Benign00
05
10
15
20
sAD
C (times
10ndash3
mm
2 s)
lowast
(a)
Malignant BenignsA
DC
(times10
ndash3 m
m2 s
)
lowast
00
05
10
15
20
(b)
Malignant Benign
sAD
C (times
10ndash3
mm
2 s)
lowast
00
05
10
15
20
(c)
Figure 4 Comparison between synthetic ADC (sADC) values of malignant and benign tissue Distribution of sADC values for malignant(Gleason score 6 and 7 N 7) and benign lesions (Gleason score lt6 N 8) in patients at b-1000 (a) b-1500 (b) and b-2000 (c) +e centerhorizontal line indicates the median value lowastplt 005
Table 1 Comparison between sADC values in lesions with Gleason score (GS) lt6 and GS ge6 at b-1000 b-1500 and b-2000
MalignantGS (67)N 7
sADC (10minus 3mm2s)(meanplusmn SD)
BenignGSlt 6N 8
sADC (10minus 3mm2s)(meanplusmn SD)
95 CI p value
b-1000 0818plusmn 0067 1131plusmn 0084 0075ndash0550 00138lowastb-1500 0682plusmn 0059 1007plusmn 0090 0084ndash0567 00121lowastb-2000 0601plusmn 0057 0935plusmn 0094 0088ndash0581 00116lowastlowastStatistically significant 95 CI 95 confidence interval sADC synthetic apparent diffusion coefficient GS Gleason score
6 Prostate Cancer
References
[1] H A Vargas O Akin T Franiel et al ldquoDiffusion-weightedendorectal MR imaging at 3 T for prostate cancer tumordetection and assessment of aggressivenessrdquo Radiologyvol 259 no 3 pp 775ndash784 2011
[2] T Tamada V Prabhu J Li J S Babb S S Taneja andA B Rosenkrantz ldquoAssessment of prostate cancer aggres-siveness using apparent diffusion coefficient values impact ofpatient race and agerdquo Abdominal Radiology vol 42 no 6pp 1744ndash1751 2017
[3] T H Kim C K Kim B K Park et al ldquoRelationship betweenGleason score and apparent diffusion coefficients of diffusion-weighted magnetic resonance imaging in prostate cancerpatientsrdquo Canadian Urological Association Journal vol 10no 11-12 pp E377ndashE382 2016
[4] A Lebovici S A Sfrangeu D Feier et al ldquoEvaluation of thenormal-to-diseased apparent diffusion coefficient ratio as anindicator of prostate cancer aggressivenessrdquo BMC MedicalImaging vol 14 no 1 p 15 2014
[5] M Quentin D Blondin J Klasen et al ldquoComparison ofdifferent mathematical models of diffusion-weighted prostateMR imagingrdquo Magnetic Resonance Imaging vol 30 no 10pp 1468ndash1474 2012
[6] K M Bennett K M Schmainda R Bennett (Tong)D B Rowe H Lu and J S Hyde ldquoCharacterization ofcontinuously distributed cortical water diffusion rates with astretched-exponential modelrdquo Magnetic Resonance in Medi-cine vol 50 no 4 pp 727ndash734 2003
[7] M M Jafar A Parsai and M E Miquel ldquoDiffusion-weightedmagnetic resonance imaging in cancer reported apparentdiffusion coefficients in-vitro and in-vivo reproducibilityrdquoWorld Journal of Radiology vol 8 no 1 pp 21ndash49 2016
[8] C Kyo Kim B Kwan Park B Kim and C K Kim ldquoHigh-b-value diffusion-weighted imaging at 3 Tto detect prostate cancercomparisons between b values of 1000 and 2000 smm2rdquoAmerican Journal of Roentgenology vol 194 pp W33ndashW372010
[9] T de Perrot M Scheffler J Boto et al ldquoDiffusion in prostatecancer detection on a 3T scanner how many b-values areneededrdquo Journal of Magnetic Resonance Imaging vol 44no 3 pp 601ndash609 2016
[10] G Manenti M Nezzo F Chegai E Vasili E Bonanno andG Simonetti ldquoDWI of prostate cancer optimal b-value inclinical practicerdquo Prostate Cancer vol 2014 Article ID868269 9 pages 2014
[11] E U Saritas J H Lee and D G Nishimura ldquoSNR depen-dence of optimal parameters for apparent diffusion coefficientmeasurementsrdquo IEEE Transactions on Medical Imagingvol 30 no 2 pp 424ndash437 2011
[12] T Tamada N Kanomata T Sone et al ldquoHigh b value(2000 smm2) diffusion-weighted magnetic resonanceimaging in prostate cancer at 3 tesla comparison with 1000smm2 for tumor conspicuity and discrimination of ag-gressivenessrdquo PLoS One vol 9 Article ID e96619 2014
[13] K Katahira T Takahara T C Kwee et al ldquoUltra-high-b-value diffusion-weighted MR imaging for the detection ofprostate cancer evaluation in 201 cases with histopathologicalcorrelationrdquo European Radiology vol 21 no 1 pp 188ndash1962011
[14] Y Ueno S Takahashi K Kitajima et al ldquoComputed diffu-sion-weighted imaging using 3-Tmagnetic resonance imagingfor prostate cancer diagnosisrdquo European Radiology vol 23no 12 pp 3509ndash3516 2013
[15] M D Blackledge M O Leach D J Collins and D-M KohldquoComputed diffusion-weighted MR imaging may improvetumor detectionrdquo Radiology vol 261 no 2 pp 573ndash5812011
[16] M Takeuchi K Matsuzaki and M Harada ldquoComputeddiffusion-weighted imaging for differentiating decidualizedendometrioma from ovarian cancerrdquo European Journal ofRadiology vol 85 no 5 pp 1016ndash1019 2016
[17] Y Ueno S Takahashi Y Ohno et al ldquoComputed diffusion-weighted MRI for prostate cancer detection the influence ofthe combinations of b-valuesrdquo +e British Journal of Radi-ology vol 88 no 1048 Article ID 20140738 2015
[18] R Yoshida T Yoshizako T Katsube Y Tamaki N Ishikawaand H Kitagaki ldquoComputed diffusion-weighted imagingusing 15-T magnetic resonance imaging for prostate cancerdiagnosisrdquo Clinical Imaging vol 41 pp 78ndash82 2017
[19] G+ormer J Otto M Reiss-Zimmermann et al ldquoDiagnosticvalue of ADC in patients with prostate cancer influence of thechoice of b valuesrdquo European Radiology vol 22 no 8pp 1820ndash1828 2012
[20] Y Peng Y Jiang T Antic et al ldquoApparent diffusion coef-ficient for prostate cancer imaging impact of b valuesrdquoAmerican Journal of Roentgenology vol 202 no 3pp W247ndashW253 2014
[21] Y Oto A Afaq D B Rowe Y Lu A Shukla-Dave andJ Grover ldquoDiffusion-weighted magnetic resonance imagingof the prostate improved robustness with stretched expo-nential modelingrdquo Journal of Computer Assisted Tomographyvol 36 no 6 pp 695ndash703 2012
[22] M Iima and D Le Bihan ldquoClinical intravoxel incoherentmotion and diffusion MR imaging past present and futurerdquoRadiology vol 278 no 1 pp 13ndash32 2016
[23] Understanding Your Pathology Report Prostate Cancer[24] A B Rosenkrantz N Hindman R P Lim et al ldquoDiffusion-
weighted imaging of the prostate comparison of b1000 andb2000 image sets for index lesion detectionrdquo Journal ofMagnetic Resonance Imaging vol 38 no 3 pp 694ndash700 2013
[25] K Taneja Y Kaji K Kuroda and K Sugimura ldquoHigh b-valuediffusion-weighted imaging in normal and malignant pe-ripheral zone tissue of the prostate effect of signal-to-noiseratiordquo Magnetic Resonance in Medical Sciences vol 7 no 2pp 93ndash99 2008
[26] K Kitajima S Takahashi Y Ueno et al ldquoClinical utility ofapparent diffusion coefficient values obtained using highb-value when diagnosing prostate cancer using 3 tesla MRIcomparison between ultra-high b-value (2000 smm2) andstandard high b-value (1000 smm2)rdquo Journal of MagneticResonance Imaging vol 36 no 1 pp 198ndash205 2012
Prostate Cancer 7

difference between ADC and sADC values at normal regionsAs DWI signal attenuation is exponentially dependent onADC small changes in ADC can make a significant change inDWI contrast this results in the significant increase of CR insDWI images as compared to DWI
+e present study demonstrates that although the higherb-value sDWI increases the contrast between lesion andnormal tissue the sADC shows similar contrast for b-1000b-1500 and b-2000 +is could be due to small cohort size ofthe patient with different Gleason scores consistent withresults in other studies [12 24] ADC computed from high b-value DWI has been shown to be more accurate in dis-tinguishing prostate lesions from benign and normal tissues[25 26] Further investigation could be done for the clinicalapplication of sDWI with larger patient populations One ofthe limitations of our study was MRI examinations were notcompared with a radical prostatectomy specimen Howeverimage-guided MR-overlayed biopsy could be a good alter-native to radical prostatectomy where patient refuses toundergo prostatectomy
Our initial investigation suggests that the ADC valuescorresponding to higher b-value DWI can be computedusing a log-linear relationship derived from lower b-values(ble 1000) Moreover this computational method can also
be manipulated to determine optimized b-values to createADC maps +e synthetic ADC technique could be a usefultool to provide optimized image contrast for quantitativeDW-MR imaging applications in oncology where ADC isroutinely used in clinical practice
Data Availability
+e data that support the findings of this study are availablefrom the corresponding author upon reasonable request
Disclosure
Partial results of this manuscript have been presented at theEuropean Society for Magnetic Resonance in Medicine andBiology (ESMRMB) 2017 Barcelona Spain with the ab-stract titled ldquoSynthetic Apparent Diffusion Coefficient forUltra High b-value DiffusionWeighted Imaging in Prostaterdquo(abstract number esmrmb201758233ce)
Conflicts of Interest
+e authors declare that they have no conflicts of interest
Malignant Benign00
05
10
15
20
sAD
C (times
10ndash3
mm
2 s)
lowast
(a)
Malignant BenignsA
DC
(times10
ndash3 m
m2 s
)
lowast
00
05
10
15
20
(b)
Malignant Benign
sAD
C (times
10ndash3
mm
2 s)
lowast
00
05
10
15
20
(c)
Figure 4 Comparison between synthetic ADC (sADC) values of malignant and benign tissue Distribution of sADC values for malignant(Gleason score 6 and 7 N 7) and benign lesions (Gleason score lt6 N 8) in patients at b-1000 (a) b-1500 (b) and b-2000 (c) +e centerhorizontal line indicates the median value lowastplt 005
Table 1 Comparison between sADC values in lesions with Gleason score (GS) lt6 and GS ge6 at b-1000 b-1500 and b-2000
MalignantGS (67)N 7
sADC (10minus 3mm2s)(meanplusmn SD)
BenignGSlt 6N 8
sADC (10minus 3mm2s)(meanplusmn SD)
95 CI p value
b-1000 0818plusmn 0067 1131plusmn 0084 0075ndash0550 00138lowastb-1500 0682plusmn 0059 1007plusmn 0090 0084ndash0567 00121lowastb-2000 0601plusmn 0057 0935plusmn 0094 0088ndash0581 00116lowastlowastStatistically significant 95 CI 95 confidence interval sADC synthetic apparent diffusion coefficient GS Gleason score
6 Prostate Cancer
References
[1] H A Vargas O Akin T Franiel et al ldquoDiffusion-weightedendorectal MR imaging at 3 T for prostate cancer tumordetection and assessment of aggressivenessrdquo Radiologyvol 259 no 3 pp 775ndash784 2011
[2] T Tamada V Prabhu J Li J S Babb S S Taneja andA B Rosenkrantz ldquoAssessment of prostate cancer aggres-siveness using apparent diffusion coefficient values impact ofpatient race and agerdquo Abdominal Radiology vol 42 no 6pp 1744ndash1751 2017
[3] T H Kim C K Kim B K Park et al ldquoRelationship betweenGleason score and apparent diffusion coefficients of diffusion-weighted magnetic resonance imaging in prostate cancerpatientsrdquo Canadian Urological Association Journal vol 10no 11-12 pp E377ndashE382 2016
[4] A Lebovici S A Sfrangeu D Feier et al ldquoEvaluation of thenormal-to-diseased apparent diffusion coefficient ratio as anindicator of prostate cancer aggressivenessrdquo BMC MedicalImaging vol 14 no 1 p 15 2014
[5] M Quentin D Blondin J Klasen et al ldquoComparison ofdifferent mathematical models of diffusion-weighted prostateMR imagingrdquo Magnetic Resonance Imaging vol 30 no 10pp 1468ndash1474 2012
[6] K M Bennett K M Schmainda R Bennett (Tong)D B Rowe H Lu and J S Hyde ldquoCharacterization ofcontinuously distributed cortical water diffusion rates with astretched-exponential modelrdquo Magnetic Resonance in Medi-cine vol 50 no 4 pp 727ndash734 2003
[7] M M Jafar A Parsai and M E Miquel ldquoDiffusion-weightedmagnetic resonance imaging in cancer reported apparentdiffusion coefficients in-vitro and in-vivo reproducibilityrdquoWorld Journal of Radiology vol 8 no 1 pp 21ndash49 2016
[8] C Kyo Kim B Kwan Park B Kim and C K Kim ldquoHigh-b-value diffusion-weighted imaging at 3 Tto detect prostate cancercomparisons between b values of 1000 and 2000 smm2rdquoAmerican Journal of Roentgenology vol 194 pp W33ndashW372010
[9] T de Perrot M Scheffler J Boto et al ldquoDiffusion in prostatecancer detection on a 3T scanner how many b-values areneededrdquo Journal of Magnetic Resonance Imaging vol 44no 3 pp 601ndash609 2016
[10] G Manenti M Nezzo F Chegai E Vasili E Bonanno andG Simonetti ldquoDWI of prostate cancer optimal b-value inclinical practicerdquo Prostate Cancer vol 2014 Article ID868269 9 pages 2014
[11] E U Saritas J H Lee and D G Nishimura ldquoSNR depen-dence of optimal parameters for apparent diffusion coefficientmeasurementsrdquo IEEE Transactions on Medical Imagingvol 30 no 2 pp 424ndash437 2011
[12] T Tamada N Kanomata T Sone et al ldquoHigh b value(2000 smm2) diffusion-weighted magnetic resonanceimaging in prostate cancer at 3 tesla comparison with 1000smm2 for tumor conspicuity and discrimination of ag-gressivenessrdquo PLoS One vol 9 Article ID e96619 2014
[13] K Katahira T Takahara T C Kwee et al ldquoUltra-high-b-value diffusion-weighted MR imaging for the detection ofprostate cancer evaluation in 201 cases with histopathologicalcorrelationrdquo European Radiology vol 21 no 1 pp 188ndash1962011
[14] Y Ueno S Takahashi K Kitajima et al ldquoComputed diffu-sion-weighted imaging using 3-Tmagnetic resonance imagingfor prostate cancer diagnosisrdquo European Radiology vol 23no 12 pp 3509ndash3516 2013
[15] M D Blackledge M O Leach D J Collins and D-M KohldquoComputed diffusion-weighted MR imaging may improvetumor detectionrdquo Radiology vol 261 no 2 pp 573ndash5812011
[16] M Takeuchi K Matsuzaki and M Harada ldquoComputeddiffusion-weighted imaging for differentiating decidualizedendometrioma from ovarian cancerrdquo European Journal ofRadiology vol 85 no 5 pp 1016ndash1019 2016
[17] Y Ueno S Takahashi Y Ohno et al ldquoComputed diffusion-weighted MRI for prostate cancer detection the influence ofthe combinations of b-valuesrdquo +e British Journal of Radi-ology vol 88 no 1048 Article ID 20140738 2015
[18] R Yoshida T Yoshizako T Katsube Y Tamaki N Ishikawaand H Kitagaki ldquoComputed diffusion-weighted imagingusing 15-T magnetic resonance imaging for prostate cancerdiagnosisrdquo Clinical Imaging vol 41 pp 78ndash82 2017
[19] G+ormer J Otto M Reiss-Zimmermann et al ldquoDiagnosticvalue of ADC in patients with prostate cancer influence of thechoice of b valuesrdquo European Radiology vol 22 no 8pp 1820ndash1828 2012
[20] Y Peng Y Jiang T Antic et al ldquoApparent diffusion coef-ficient for prostate cancer imaging impact of b valuesrdquoAmerican Journal of Roentgenology vol 202 no 3pp W247ndashW253 2014
[21] Y Oto A Afaq D B Rowe Y Lu A Shukla-Dave andJ Grover ldquoDiffusion-weighted magnetic resonance imagingof the prostate improved robustness with stretched expo-nential modelingrdquo Journal of Computer Assisted Tomographyvol 36 no 6 pp 695ndash703 2012
[22] M Iima and D Le Bihan ldquoClinical intravoxel incoherentmotion and diffusion MR imaging past present and futurerdquoRadiology vol 278 no 1 pp 13ndash32 2016
[23] Understanding Your Pathology Report Prostate Cancer[24] A B Rosenkrantz N Hindman R P Lim et al ldquoDiffusion-
weighted imaging of the prostate comparison of b1000 andb2000 image sets for index lesion detectionrdquo Journal ofMagnetic Resonance Imaging vol 38 no 3 pp 694ndash700 2013
[25] K Taneja Y Kaji K Kuroda and K Sugimura ldquoHigh b-valuediffusion-weighted imaging in normal and malignant pe-ripheral zone tissue of the prostate effect of signal-to-noiseratiordquo Magnetic Resonance in Medical Sciences vol 7 no 2pp 93ndash99 2008
[26] K Kitajima S Takahashi Y Ueno et al ldquoClinical utility ofapparent diffusion coefficient values obtained using highb-value when diagnosing prostate cancer using 3 tesla MRIcomparison between ultra-high b-value (2000 smm2) andstandard high b-value (1000 smm2)rdquo Journal of MagneticResonance Imaging vol 36 no 1 pp 198ndash205 2012
Prostate Cancer 7

References
[1] H A Vargas O Akin T Franiel et al ldquoDiffusion-weightedendorectal MR imaging at 3 T for prostate cancer tumordetection and assessment of aggressivenessrdquo Radiologyvol 259 no 3 pp 775ndash784 2011
[2] T Tamada V Prabhu J Li J S Babb S S Taneja andA B Rosenkrantz ldquoAssessment of prostate cancer aggres-siveness using apparent diffusion coefficient values impact ofpatient race and agerdquo Abdominal Radiology vol 42 no 6pp 1744ndash1751 2017
[3] T H Kim C K Kim B K Park et al ldquoRelationship betweenGleason score and apparent diffusion coefficients of diffusion-weighted magnetic resonance imaging in prostate cancerpatientsrdquo Canadian Urological Association Journal vol 10no 11-12 pp E377ndashE382 2016
[4] A Lebovici S A Sfrangeu D Feier et al ldquoEvaluation of thenormal-to-diseased apparent diffusion coefficient ratio as anindicator of prostate cancer aggressivenessrdquo BMC MedicalImaging vol 14 no 1 p 15 2014
[5] M Quentin D Blondin J Klasen et al ldquoComparison ofdifferent mathematical models of diffusion-weighted prostateMR imagingrdquo Magnetic Resonance Imaging vol 30 no 10pp 1468ndash1474 2012
[6] K M Bennett K M Schmainda R Bennett (Tong)D B Rowe H Lu and J S Hyde ldquoCharacterization ofcontinuously distributed cortical water diffusion rates with astretched-exponential modelrdquo Magnetic Resonance in Medi-cine vol 50 no 4 pp 727ndash734 2003
[7] M M Jafar A Parsai and M E Miquel ldquoDiffusion-weightedmagnetic resonance imaging in cancer reported apparentdiffusion coefficients in-vitro and in-vivo reproducibilityrdquoWorld Journal of Radiology vol 8 no 1 pp 21ndash49 2016
[8] C Kyo Kim B Kwan Park B Kim and C K Kim ldquoHigh-b-value diffusion-weighted imaging at 3 Tto detect prostate cancercomparisons between b values of 1000 and 2000 smm2rdquoAmerican Journal of Roentgenology vol 194 pp W33ndashW372010
[9] T de Perrot M Scheffler J Boto et al ldquoDiffusion in prostatecancer detection on a 3T scanner how many b-values areneededrdquo Journal of Magnetic Resonance Imaging vol 44no 3 pp 601ndash609 2016
[10] G Manenti M Nezzo F Chegai E Vasili E Bonanno andG Simonetti ldquoDWI of prostate cancer optimal b-value inclinical practicerdquo Prostate Cancer vol 2014 Article ID868269 9 pages 2014
[11] E U Saritas J H Lee and D G Nishimura ldquoSNR depen-dence of optimal parameters for apparent diffusion coefficientmeasurementsrdquo IEEE Transactions on Medical Imagingvol 30 no 2 pp 424ndash437 2011
[12] T Tamada N Kanomata T Sone et al ldquoHigh b value(2000 smm2) diffusion-weighted magnetic resonanceimaging in prostate cancer at 3 tesla comparison with 1000smm2 for tumor conspicuity and discrimination of ag-gressivenessrdquo PLoS One vol 9 Article ID e96619 2014
[13] K Katahira T Takahara T C Kwee et al ldquoUltra-high-b-value diffusion-weighted MR imaging for the detection ofprostate cancer evaluation in 201 cases with histopathologicalcorrelationrdquo European Radiology vol 21 no 1 pp 188ndash1962011
[14] Y Ueno S Takahashi K Kitajima et al ldquoComputed diffu-sion-weighted imaging using 3-Tmagnetic resonance imagingfor prostate cancer diagnosisrdquo European Radiology vol 23no 12 pp 3509ndash3516 2013
[15] M D Blackledge M O Leach D J Collins and D-M KohldquoComputed diffusion-weighted MR imaging may improvetumor detectionrdquo Radiology vol 261 no 2 pp 573ndash5812011
[16] M Takeuchi K Matsuzaki and M Harada ldquoComputeddiffusion-weighted imaging for differentiating decidualizedendometrioma from ovarian cancerrdquo European Journal ofRadiology vol 85 no 5 pp 1016ndash1019 2016
[17] Y Ueno S Takahashi Y Ohno et al ldquoComputed diffusion-weighted MRI for prostate cancer detection the influence ofthe combinations of b-valuesrdquo +e British Journal of Radi-ology vol 88 no 1048 Article ID 20140738 2015
[18] R Yoshida T Yoshizako T Katsube Y Tamaki N Ishikawaand H Kitagaki ldquoComputed diffusion-weighted imagingusing 15-T magnetic resonance imaging for prostate cancerdiagnosisrdquo Clinical Imaging vol 41 pp 78ndash82 2017
[19] G+ormer J Otto M Reiss-Zimmermann et al ldquoDiagnosticvalue of ADC in patients with prostate cancer influence of thechoice of b valuesrdquo European Radiology vol 22 no 8pp 1820ndash1828 2012
[20] Y Peng Y Jiang T Antic et al ldquoApparent diffusion coef-ficient for prostate cancer imaging impact of b valuesrdquoAmerican Journal of Roentgenology vol 202 no 3pp W247ndashW253 2014
[21] Y Oto A Afaq D B Rowe Y Lu A Shukla-Dave andJ Grover ldquoDiffusion-weighted magnetic resonance imagingof the prostate improved robustness with stretched expo-nential modelingrdquo Journal of Computer Assisted Tomographyvol 36 no 6 pp 695ndash703 2012
[22] M Iima and D Le Bihan ldquoClinical intravoxel incoherentmotion and diffusion MR imaging past present and futurerdquoRadiology vol 278 no 1 pp 13ndash32 2016
[23] Understanding Your Pathology Report Prostate Cancer[24] A B Rosenkrantz N Hindman R P Lim et al ldquoDiffusion-
weighted imaging of the prostate comparison of b1000 andb2000 image sets for index lesion detectionrdquo Journal ofMagnetic Resonance Imaging vol 38 no 3 pp 694ndash700 2013
[25] K Taneja Y Kaji K Kuroda and K Sugimura ldquoHigh b-valuediffusion-weighted imaging in normal and malignant pe-ripheral zone tissue of the prostate effect of signal-to-noiseratiordquo Magnetic Resonance in Medical Sciences vol 7 no 2pp 93ndash99 2008
[26] K Kitajima S Takahashi Y Ueno et al ldquoClinical utility ofapparent diffusion coefficient values obtained using highb-value when diagnosing prostate cancer using 3 tesla MRIcomparison between ultra-high b-value (2000 smm2) andstandard high b-value (1000 smm2)rdquo Journal of MagneticResonance Imaging vol 36 no 1 pp 198ndash205 2012
Prostate Cancer 7





![Quality Report · 2018. 8. 15. · 0.006 -0.003 0.003 -0.001 0.002 Uncertainties (Sigma) 1.990 [pixel] 0.005 [mm] 0.664 [pixel] 0.002 [mm] 0.787 [pixel] 0.002 [mm] 0.000 0.000 0.000](https://img.pdfslide.net/doc/110x75/60fd4e48c8d80d2d9761f76c/quality-report-2018-8-15-0006-0003-0003-0001-0002-uncertainties-sigma.jpg)