Embed Size (px)
Citation preview

Systematic review with meta-analysis: clinical manifestationsand management of autoimmune hepatitis in the elderlyJ. Chen*, G. D. Eslick† & M. Weltman*
*Department of Gastroenterology andHepatology, Nepean Hospital, Penrith,NSW, Australia.†The Whiteley-Martin ResearchCentre, Discipline of Surgery, TheSydney Medical School Nepean,Penrith, NSW, Australia.
Correspondence to:Prof. G. D. Eslick, The Whiteley-Martin Research Centre, Discipline ofSurgery, The University of SydneyNepean Hospital, Level 5, SouthBlock, P.O. Box 63, Penrith, NSW2751, Australia.E-mail: [email protected]
Publication dataSubmitted 3 July 2013First decision 21 July 2013Resubmitted 3 November 2013Accepted 5 November 2013EV Pub Online 22 November 2013
As part of AP&T’s peer-review process, atechnical check of this meta-analysis wasperformed by Mr M. Siddiqui.
SUMMARY
BackgroundAutoimmune hepatitis is an uncommon chronic progressive inflammatorydisease of the liver, characterised by hypergammaglobulianemia, circulatingautoantibodies, and interface hepatitis histologically. It is traditionallythought to be a disease of young women. However, recent epidemiologicaland retrospective studies suggest that it might be a disease predominantlyof older women. Studies of AIH in elderly patients have been fairly limited.
AimTo investigate the differences in the clinical presentations and the manage-ment of AIH in the elderly and the younger patients.
MethodsWe conducted a search on MEDLINE (from 1946), PubMed (1946) andEMBASE (1949) through to November 2013 using the terms ‘autoimmunehepatitis in the elderly’, and the combinations of ‘Autoimmune hepatitis’AND the following terms: ‘elderly’, ‘aging’, ‘older patients’, and ‘older’. Thereference lists of relevant articles were also searched for appropriate studies.
ResultsA total of 1063 patients were identified with AIH in 10 retrospective stud-ies. The definition of ‘elderly’ ranged from 60 to 65 years; 264 elderly and592 younger patients were included for analysis. Elderly, 24.8%, were morelikely to present asymptomatically, cirrhotic at presentation and HLA-DR4-positive. They are less likely to be HLA-DR3-positive and to relapse aftertreatment withdrawal after complete remission.
ConclusionsAIH is an important differential in elderly patients with cirrhosis or abnor-mal LFTs. Elderly are more likely to be cirrhotic and asymptomatic at pre-sentation. Glucocorticoids use should be readily considered in the elderlypatients as the current evidence suggests that they respond well to the ther-apy, with less relapse after treatment withdrawal.
Aliment Pharmacol Ther 2014; 39: 117–124
ª 2013 John Wiley & Sons Ltd 117
doi:10.1111/apt.12563
Alimentary Pharmacology and Therapeutics

INTRODUCTIONAutoimmune hepatitis is an uncommon chronic progres-sive inflammatory disease of the liver, characterised by hy-pergammaglobulianemia, circulating autoantibodies andthe histological change of interface hepatitis, which isresponsive to immunosuppressive therapy in the majorityof cases.1–3 It was first described by Waldenstrom, Kunkeland others in the early 1950s as a progressive chronic hep-atitis predominantly in young women.4–6 However, recentepidemiological and retrospective studies suggest that itmight be a disease predominantly of older women.7–9
Studies of AIH in elderly patients have been fairly lim-ited due to the traditional belief that it is a disease ofyoung women. We conducted a literature search andmeta-analysis on the topic of autoimmune hepatitis inthe elderly population, to better understand the disease inthis cohort of patients compared to the younger patientswith autoimmune hepatitis. The aims of the literaturereview are to compare the differences in the presentations– clinically, biochemically, serologically and histologically,between the elderly and the younger patients; in themode of presentation; the associated autoimmune dis-eases; as well as in response and tolerability to treatments.This should produce a better understanding of the diseaseprocess in the elderly and allow better management ofthe elderly patients who present with this condition.
METHODS
Study protocolWe followed the Preferred Reporting Items for System-atic reviews and Meta-Analyses (PRISMA) guidelines.10
A systematic search of the databases MEDLINE (from1946), PubMed (from 1946), EMBASE (from 1949)through to November 2013 was carried out to identifyrelevant articles. The search used the terms ‘autoimmunehepatitis in the elderly’, ‘autoimmune hepatitis’ AND‘elderly’, ‘autoimmune hepatitis’ AND ‘aging’, ‘autoim-mune hepatitis’ AND ‘older patients’, or ‘autoimmunehepatitis’ AND ‘older’, and these terms were searched astext word and as exploded medical subject headingswhere possible. The reference lists of relevant articleswere also searched for appropriate studies. No languagerestrictions were used in either the search or study selec-tion. No quality assessment was undertaken. A searchfor unpublished literature was not performed.
Study selectionWe included studies that specifically looked at the differ-ences in the presentation, and/or the treatment response,
and other aspects of autoimmune hepatitis between theelderly and younger patients.
Data extractionThe data extraction was performed using a standar-dised data extraction form, collecting information onthe publication year, study design, total sample size,the percentage of old patients, temporal direction, pop-ulation type, country, continent, mean age at presenta-tion, number of adjusted variables, the most commonmode of presentation, the differences in presentation,the rate of cirrhosis, the time to diagnosis, the rate ofother autoimmune diseases, the associated HLA haplo-type, the treatment response, the rate of relapses andthe tolerability of the treatment. Quality of the studieswas not assessed and authors were not contacted formissing data.
Statistical analysisPooled odds ratios and 95% confidence intervals werecalculated for the various aspects of autoimmune hepati-tis in the elderly and young patients using a random-effects model.11 We tested heterogeneity with Cochran’sQ statistics, with P < 0.10 indicating heterogeneity, andquantified the degree of heterogeneity using the I2 statis-tics, which represents the percentage of the total variabil-ity across studies, which is due to heterogeneity. Valuesof 25%, 50%, and 75% corresponded to low, moderateand high degrees of heterogeneity respectively.12 Wequantified publication bias using the Egger’s regressionmodel,13 with the effect of bias assessed during the fail-safe number method. The fail-safe number was the num-ber of studies that we would need to have missed forour observed result to be nullified to statistical nonsignif-icance at the P < 0.05 level. Publication bias is generallyregarded as a concern if the fail-safe number is less than5n + 10, with n being the number of studies included inthe meta-analysis.14 All analyses were performed withComprehensive Meta-analysis (version 2.0), Biostat,Englwood, NJ (1995).
RESULTS
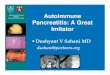
Study characteristicsA total of 10 studies15–24 were identified as appropriatefor and included in the review (Figure 1) (Table 1). Allwere retrospective studies. The sample size of eachstudy was fairly small, with the smallest study having41 patients and the largest 205 patients. The small sam-ple sizes of the studies are a reflection of the rarity of
118 Aliment Pharmacol Ther 2014; 39: 117-124
ª 2013 John Wiley & Sons Ltd
J. Chen et al.

the disease. A total of 1063 patients were identified tohave autoimmune hepatitis in the 10 studies. Therewere 264 elderly (defined as ≥65 in 7 studies and ≥60in 3) patients and 592 younger (any patients below thedefined age for elderly) included for analysis. However,in Czaja and Carpenter’s study, five age brackets wereused and the comparison was made between the oldestage bracket (≥60 years) and the youngest bracket (18–30 years) with 47 and 31 patients, respectively. InSchramm et al.’s study, although 120 patients wereidentified as having AIH, as there were 20 patients aged≥65, data of the 20 of the youngest patients were usedin the study.
Percentage of elderly patientsThe elderly population was defined by the age of 65 orover in seven of the studies,15–19, 23, 24 and 60 or over inthe other three.20–22 The percentages were fairly consis-tent, around 20–25% of the studied population, with oneexception from the study by Parker and Kingham15
showing 56% of the patients with AIH aged over 60,making 1 in 4 patients diagnosed with AIH an elderlypatient.
GenderSeventy-six per cent of the patients in these studies werefemale; elderly female patients account for 21% of thetotal patients from the ten studies.
Publication biasEgger’s regression revealed no evidence of publicationbias for any of the groups assessed (acute onset,P = 0.10; chronic onset, P = 0.07; asymptomatic,P = 0.19; autoimmune diseases, P = 0.69; cirrhosis,P = 0.59; complete response, P = 0.34; partial response,P = 0.09; treatment failure, P = 0.22; HLA DR3,P = 0.86; HLA DR4, P = 0.26).
PresentationsClinical. Asymptomatic: Al-Chalabi et al.21 definedasymptomatic as the patient having no obvious signs orsymptoms of liver disease and his/her AIH beingdetected incidentally in routine health screening or dur-ing investigation of another condition. The asymptom-atic data from the study by Verslype et al.18 wasextracted from numbers given under ‘incidental findings’in Table 1 in their study. Granito et al.19 defined the
49 studies excluded: 25 duplicatearticles; 24 review articles
52 studies retrieved formore detailed evaluation
13 potentially appropriatestudies to be included in the
9 Studies included in meta-analysis
10 studies with usableinformation
39 studies excluded: not specificto the topic of autoimmunehepatitis in the elderly
4 studies were excluded:epidemiological studies,
One study obtainedfrom reference lists
101 potentially relevantstudies identified bysearching MEDLINE,MedPub, and EMBASE
meta-analysis
inadequate comparative data
Figure 1 | Flow chart of thesearch strategy used in thereview.
Aliment Pharmacol Ther 2014; 39: 117-124 119
ª 2013 John Wiley & Sons Ltd
Systematic review with meta-analysis: autoimmune hepatitis in the elderly

asymptomatic pattern as fortuitous detection of abnor-mal liver function tests with no clinical symptoms. Xieet al.’s abstract22 provided the number of asymptomaticpatients with no definition. The elderly patients are morelikely to present asymptomatically.
Acute onset: Granito et al.19 defined the acute pattern ofpresentation as recent onset (<30 days) of symptoms(jaundice and/or fatigue and/or drowsiness and/or fever)together with marked alterations of liver function tests.Acute presentation in Floreani et al’s study23 was definedby the presence of recent onset (<30 days) symptoms(jaundice and/or fatigue and/or drowsiness) in conjunc-tion with serum alanine transferase levels higher than10-fold the upper normal limit. Al-Chalabi et al.21
defined the mode of presentation as acute if symptomonset to diagnosis was ≤6 months. Czaja and Carpenter20
had no definition of acute onset. Patients with acute-on-set liver dysfunction (serum alanine aminotransferase lev-els higher than 10-fold the upper normal limit) andwithout a history of any prior liver disease were diag-nosed as acute-onset autoimmune hepatitis in Miyakeet al’s study.24 We used the definition of presence ofsymptoms for 6 months or less as acute onset.
Chronic onset: Granito et al.19 defined chronic patternof presentation as general malaise for at least 6 monthsin the presence of clinical and biochemical features con-sistent with chronic liver disease (including cirrhosis).Al-Chalabi et al.21 defined ‘insidious’ as symptom onset
Table 1 | Characteristics of the studies included in the meta-analysis
Study
No. of patients
total (F:M)
Elderly: young Time span Country
Concurrent
autoimmune
diseases
Clinical
presentation
Biochemical
parameters
Serological
parameters HLA haplotype Treatment response
Parker and
Kingham
1997
41 (32:9)
23:18
1986–1996 UK Yes, but no
distinction
between the
young and
the old
– – – – Complete response,
partial response,
treatment failure,
relapse
Newton
et al. 1997
54 (43:11)
12:42
1979–1993 UK No Major, minor,
asymptomatic
– – – –
Schramm
et al. 2001
120 (32:8)
20:20
– Germany Yes Symptomatology:
(acute icteric
hepatitis)
ALT,
gamma- globulin
ANA, SMA,
SLA/LP,
LKM-1
HLA DR3, HLA DR4,
HLA A1, HLA B8,
HLA A1-B8
Complete response,
relapse
Verslype
2005
112 (77:35)
28:84
1975–2002 Belgium No Symptomatology ALT, bile, gamma-
globulin
ANA, SMA,
LKM, AMA
– –
Granito
et al. 2005
76 (64:12)
20:56
– Italy Yes Mode of onset:
acute, chronic,
asymptomatic
ALT, AST, ALP,
bilirubin, GGT,
albumin, gamma-
globulin
ANA, SMA HLA DR3, HLA DR4 Complete response,
relapse
Czaja and
Carpenter
2006
205 (175:30)
47:31
1975–2005 USA Yes Mode of onset:
symptom
duration
AST, bilirubin,
gamma-globulin,
immunoglobulin
– HLA DR3+/DR4�,
HLA DR4+/DR3�,
HLA DR3 + -DR4+
Complete response,
partial response,
treatment failure,
relapse
Al-Chalabi
et al. 2006
164 (128:36)
43:121
1971–2004 UK Yes Mode of onset:
acute, insidious,
and asymptomatic
ALP, AST, GGT,
bilirubin, IgG,
IgM, IgA
ANA, SMA,
LKM
HLA DR3,
HLA DR4,
HLA A1,
HLA A8,
HLA A1-B8-DR3
or/and DR4
Complete response,
partial response,
treatment failure,
relapse
Xie
et al. 2006
58 (47:11)
21:37
– – No Symptomatology:
acute icteric
hepatitis and
asymptomatic
AST, ALT,
albumin
ANA, SMA – –
Floreani
et al. 2006
73 (63:10)
16:57
1981–2004 Italy Yes Mode of onset –
Acute and
chronic onset
AST, ALT, GGT,
ALP, IgG, IgA,
IgM, albumin,
bilirubin
– – –
Miyake
et al. 2007
160 (140:20)
34:126
1988 – 2005 Japan Yes, but no
distinction
between the
young and
the old
Mode of onset:
Acute and
classical onset
Bilirubin, albumin,
AST, ALT, IgG
ANA or SMA – –
120 Aliment Pharmacol Ther 2014; 39: 117-124
ª 2013 John Wiley & Sons Ltd
J. Chen et al.

to diagnosis >6 months. Floreani et al.23 definedchronic presentation in those with clinical and bio-chemical features compatible with chronic liver disorderand symptoms that had been persisting for at least6 months and were usually minor and unspecific. Mi-yake et al.24 diagnosed their patients as classical-onsetautoimmune hepatitis if they have abnormalities of liverfunction test on medical check-up or in the past his-tory, or with increased serum alanine transferase levelsunder 10 fold the upper normal limit. Our definitionfor chronic onset is the presence of symptoms for morethan 6 months.
Biochemical. The mean values of each of the ALT, ASTand bilirubin were available from 6 of the 10 studies.17–24
Gamma-globulin levels were available from 4 of the 10studies;17–20 values for albumin were also available from4 of the 10 studies19, 22–24 (Table 2).
Serological. ANA: Five of the ten studies looked at thenumber of patients with autoimmune hepatitis withANA positivity between the elderly and the youngerpatients.17–19, 21, 22 Two studies defined ANA-positive astitre ≥1:80;18, 19 one study as titre >1:40;22 one as titre≥1:4021; and one did not specify the titre of ANA17
which is considered positive.
SMA: The same five studies also looked at the numberof patients SMA-positive in both groups.17–19, 21, 22
Three studies defined SMA positivity as titre≥1:40;18, 19, 21 one as titre >1:40;22 one study did notspecify SMA positivity17 (Table 3).
Histological. Data for number of cirrhotic patients wereavailable from 8 of the 10 studies.15, 17–23
Autoimmune diseasesFive studies looked at the frequency of other autoim-mune conditions in patients with autoimmune hepati-tis17, 19–21, 23 (Table 3).
HLA haplotypeFour studies looked at the frequency of HLA haplotype,DR3+ and DR4+, between age groups17, 19–21 (Table 3).
Treatment responseThe induction regimens in five of the ten studies thatlooked into the treatment responses all comprised eithera corticosteroid alone or a combination of a corticoste-roid and azathioprine.15, 17, 19–21 Glucocorticoids usedinclude prednisone (one study did not specify the dose;20
20–60 mg/day was used in the other study15); predniso-lone (doses used in two studies were 20–40 mg daily21
and 1 mg/kg body weight/day,17 respectively); or methyl-prednisolone (1 mg/kg body weight/day).19 One studydid not specify the dose of azathioprine used.20 Doses ofazathioprine used in other studies were 50 mg/day;19 75–100 mg daily;15 1 mg/kg body weight/day;21 and 1–1.5 mg/kg body weight/day.17
Complete responseFive of the ten studies investigated the difference inrate of complete response between the elderly and theyounger patients.15, 17, 19–21 Definition of completeresponse varies slightly in each study. Parker and
Table 2 | Biochemical parameters in elderly and younggroups with AIH
Average
Elderly Younger P value
ALT 386 U/L 328 U/L 0.06AST 442 U/L 425 U/L 0.53Bilirubin 54 lmol/L 47 lmol/L 0.30Gamma-globulin
30 g/L 27 g/L 0.39
Albumin 33 g/L 38 g/L 0.39Female 208* 428*Male 208* 112*
* Number not included from Floreani et al. as the study didnot provide detailed numbers of elderly and younger patients.
Table 3 | Summary of the odds ratio 95% CI, I2 and Pvalue for all the parameters compared
Parameter OR (95% CI) I2, P value
Cirrhosis 1.58 (1.03–2.43) 10.99, 0.34HLA DR3 0.45 (0.27–0.75) 0.03, 0.39HLA DR4 2.94 (1.21–7.14) 55.70, 0.08Asymptomatic 2.59 (1.11–6.05) 37.33, 0.19Relapse 0.38 (0.23–0.36) 0.00, 0.49Autoimmune diseases 1.25 (0.76–2.08) 22.13, 0.27Autoimmune thyroiddisease
2.71 (1.18–6.19) 30.42, 0.22
ANA 1.24 (0.42–3.66) 71.41, 0.007SMA 0.73 (0.32–1.65) 66.32, 0.02Acute onset 1.83 (0.90–3.74) 61.73, 0.03Chronic onset 0.56 (0.28–1.12) 56.66, 0.08Complete response 1.21 (0.66–2.22) 0.00, 0.88Partial response 1.33 (0.44–4.06) 33.23, 0.22Treatment failure 0.47 (0.09–2.41) 28.94, 0.24
Aliment Pharmacol Ther 2014; 39: 117-124 121
ª 2013 John Wiley & Sons Ltd
Systematic review with meta-analysis: autoimmune hepatitis in the elderly

Kingham15 defined complete response as return of allliver test values to normal. Schramm et al.17 and Grani-to et al.19 defined complete response as proposed byInternational Autoimmune Hepatitis Group (IAIHG).Al-Chalabi et al’s definition21 was according to therevised criteria of the IAIHG. Remission was the termused in the study by Czaja and Carpenter20 and it wasdefined as absence of symptoms, improvement of serumaspartate aminotransferase (AST) levels to normal ornear normal (less than twice the upper limits of nor-mal), and histological improvement to minimal or noinflammatory activity (Table 3).
Partial responseThree of the ten studies address this issue.15, 20, 21 Defi-nition of partial response by Parker and Kingham15 wasan improvement in liver tests that fell short of a returnto normal. Al-Chalabi et al.21 defined partial responseaccording to the original IAIHG criteria. Czaja and Car-penter20 used the term ‘continued treatment’, which wasdefined as clinical, laboratory or histological findingsduring therapy that indicated residual disease activitythat had not worsened or improved sufficiently to satisfyend point criteria (in that study, it was either remissionor treatment failure) (Table 3).
Treatment failureThree of the studies compared the treatment failurerate.15, 20, 21 No response or treatment failure wasdefined according to the IAIHG criteria. Cjaza and Car-penter defined treatment failure as worsening of clinical,laboratory and/or histological features despite compli-ance with therapy (Table 3).
RelapseFive of the ten studies compared the relapse rate betweenthe elderly and the younger patients.15, 17, 19–21 The IA-IHG criteria were used in four of the studies,12, 17, 19, 21
with Al-Chalabi et al.21 specifying that the revised IA-IHG criteria were used. The definition in Cjaza and Car-penter’s study20 was ‘reappearance of symptoms andincrease in the serum AST level to more than threefoldnormal after drug withdrawal.’
DISCUSSIONOur meta-analysis has found that there is a statisticallysignificant difference in the clinical and histologicalpresentations of AIH in the elderly. Elderly patients aremore likely to be asymptomatic and cirrhotic at
diagnosis. They are less likely to have HLA DR3, butmore likely to have HLA DR4. Response to treatment issimilar between the elderly and the younger patients, butelderly patients are less likely to relapse after withdrawalof treatment.
There is a variation in the definition of elderly popu-lation in the studies included. Seven of the studiesdefined elderly patients as aged ≥65,15–19, 23, 24 and theother three as aged ≥60.20–22 We included the studiesthat both defined elderly patients as aged ≥60 and≥65 years because of the rarity of the disease, limitednumber of studies in the literature and because thesethree studies20–22 also addressed the issues investigatedin our study. The meta-analysis revealed that a signifi-cant proportion of the patients diagnosed with AIH areelderly with one in four being the age of 60 or over.This challenges the traditional understanding that AIHis a disease of young females and with a second peakaround the perimenopausal period. It sends a messagethat AIH is an important cause of liver disease in theelderly.
One of the positive findings in this study is thatelderly patients with AIH are more likely to be cirrhoticat presentation. This finding suggests that elderlypatients have a subclinical aggressive disease that iscommonly indolent and unsuspected.25 Newton et alfound that the clinical diagnostic score before treatmentwas lower in the older group, whilst the histologicalgrade, an indicator of the degree of hepatic inflamma-tion, was higher.16 However, it is interesting to notethat in the same study, the mean histological stage atpresentation was similar in both groups. This clearlyindicates that more detailed research is required intothis finding as the implication is that elderly patientsmay need to be treated more aggressively. The presenceof cirrhosis is also important, in that patients withestablished cirrhosis invariably relapse after discontinua-tion of medication.26
The results of the meta-analysis showed that the com-plete response, partial response and the treatment failurerates were similar in both groups. In fact, there is a trendfor less treatment failure in the elderly group, but statis-tical significance was not reached. The elderly tend tohave less relapse after treatment withdrawal, indicatingthat it is easier to maintain elderly patients in remissionwithout continuing treatment. It is important to beaware that the medications used in the treatment of AIHcan have significant side effects. Corticosteroids are asso-ciated with a considerable number of complications,
122 Aliment Pharmacol Ther 2014; 39: 117-124
ª 2013 John Wiley & Sons Ltd
J. Chen et al.

including osteoporosis, immunosuppression, hyperten-sion and myopathy, which could all be potentially morecatastrophic in the elderly. One of our aims was toinvestigate the rate and severity of side effects of thetherapy. However, no numerical data were available,although it was noted in some of the studies that the fre-quency of side effects was not increased in elderlypatients.17, 19 Further studies are needed to investigatethis issue. As high proportion of the patients, 80–85%,will respond to standard therapy,27 treatment should notbe delayed or withheld due to concerns for treatmentcomplications.
In this meta-analysis, the elderly patients are also sig-nificantly more likely to be HLA DR4-positive and lesslikely to have HLA DR3. In the younger group ofpatients, DR3 occurred significantly more frequentlythan DR4 in those with an acute presentation.21 It hasalso been noted that relapses occurred significantlymore frequently in patients with DR3 than in thosewithout this allotype.21, 28 This may explain the lowerrate of relapse in the elderly. Remissions and treatmentfailure also occur more frequently in patients with DR3than in those with DR4.29 HLA haplotype may not onlyinfluence the age at presentation in AIH, but can alsopredict the course of the disease, the response to treat-ments and the prognosis.29, 30 It has also been sug-gested that HLA haplotype be taken into considerationprior to treatment withdrawal,26 and perhaps other clin-ical decisions.
There are limitations to our meta-analysis. All studiesincluded in the meta-analysis were retrospective ones,and this is subject to selection and recall bias. Theparameters examined are variable. Only half of the stud-ies looked into the treatment responses – completeresponse and relapse rates.15, 17, 19–21 Out of those five,only three examined the partial responses and treatmentfailure rates.15, 20, 21 Some studies looked at the mode ofpresentation, others at the symptomatology.17–22 Forthose studies19, 20, 24 that examined the parameter ofmode of presentation, not all provided data for all threecategories – acute, chronic and asymptomatic. There areother studies that compared the frequency of acuteicteric hepatitis vs. asymptomatic presenta-tion.17, 18, 21, 22 Other examples of disease characteristicsaddressed in some studies, but not in others, include thefrequency of HLA haplotype, liver-related death andtreatment side effects, etc. The variability not onlymakes the classification difficult, but also reduces thesample size available for analysis even further. It limitsthe other aspects of the disease we would like to assess,
such as liver-related mortality and the tolerability of thetreatment.
There is a high degree of heterogeneity in some ofthe analysed parameters. This may be due to the use ofabstract only data, which obviously limits the amountof information available. The two major contributingfactors are the small sample size and the differences inthe definition of the parameters. As discussed previ-ously, not all the studies examined the same aspects ofthe disease, data are only limited to those that did,hence the small sample size. The difference in the defi-nition of the parameters is also a major contributingfactor to the high degree of heterogeneity. Examplesinclude the definition of acute onset of the disease pre-sentation, and the positivity of ANA and SMA. Therewas no statistical significance found between the elderlyand the younger patient groups in the parameters withhigh degree of heterogeneity. There is high degree ofheterogeneity in HLA DR4. It is mainly due to the find-ing in the study by Al-Chalabi et al. We are unable toestablish the reason as to why their results differ con-siderably from those of others. There was no evidenceof publication bias.
In conclusion, autoimmune hepatitis needs to be con-sidered seriously as one of the differential diagnoses inan elderly patient with deranged liver function test and/or cirrhosis, as significant proportion of patients withautoimmune hepatitis are elderly. Our study found thatelderly patients are more likely to present asymptomati-cally with cirrhosis, more likely to have HLA DR4, andless likely to have relapse after withdrawal of treatment.There was a trend towards less treatment failure,although it did not reach statistical significance. In themanagement of AIH, glucocorticoids use should be read-ily considered in the elderly patients as the current evi-dence suggests that the older patients respond well tothe therapy with less relapse after treatment withdrawal.
AUTHORSHIPGuarantor of the article: Guy D. Eslick.Author contributions: Jo Chen and Martin Weltman:study concept. Jo Chen: literature searching, data retrie-val, data extraction. Guy D. Eslick: statistical analysis.Guy D. Eslick, Jo Chen and Martin Weltman: datainterpretation, drafting manuscript and editing manu-script. All authors approved the final version of themanuscript.
ACKNOWLEDGEMENTDeclaration of personal and funding interests: None.
Aliment Pharmacol Ther 2014; 39: 117-124 123
ª 2013 John Wiley & Sons Ltd
Systematic review with meta-analysis: autoimmune hepatitis in the elderly

REFERENCES1. Johnson PJ, McFarlane IG. Meeting
report: international autoimmunehepatitis group. Hepatology 1993; 18:998–1005.
2. Alvarez F, Berg PA, Bianchi FB, et al.International autoimmune hepatitisgroup report: review of criteria fordiagnosis of autoimmune hepatitis. JHepatol 1999; 31: 929–38.
3. Lamers MM, van Oijen MG, Pronk M,Drenth JP. Treatment options forautoimmune hepatitis: a systematicreview of randomized controlled trials. JHepatol 2010; 53: 191–8.
4. Waldenstrom J. Leber, Bluetproteineund Nahrungseiweiss StoffwechselKrankheiten, Sonderband. 8(XV). BadKissingen: Tagung, 1950.
5. Kunkel HG, Ahrens JR, EisenmengerWJ, Bougiovanni AM, Slater RJ.Extreme hypergammaglobulinaemia inyoung women with liver disease ofunknown aetiology. J Clin Invest 1951;30: 654.
6. Bearn AG, Kunkel HG, Slater RJ. Theproblem of chronic liver disease inyoung women. Am J Med 1956; 21:3–15.
7. Lee YM, Teo EK, Ng TM.Autoimmune hepatitis in Singapore: arare syndrome affecting middle-agedwomen. J Gastroen Hepatol 2001; 16:1384–9.
8. Ngu JH, Bechly K, Chapman BA, et al.Population-based epidemiology study ofautoimmune hepatitis: a disease ofolder women? J Gastroen Hepatol 2010;25: 1681–6.
9. Abe M, Mashiba T, Zeniya M,Yamamoto K, Onji M, Tsubouchi H.Present status of autoimmune hepatitisin Japan: a nationwide survey. JGastroenterol 2011; 46: 1136–41.
10. Moher D, Liberati A, Tetzlaff J, AltmanDG and the PRISMA Group. Preferredreporting items for systematic reviewsand meta-analyses: the PRISMAstatement. Ann Intern Med 2009; 151:264–9.
11. DerSimonian R, Laird N. Meta-analysisin clinical trials. Control Clin Trials1986; 7: 177–88.
12. Higgins JP, Thompson SG, Deeks JJ,Altman DG. Measuring inconsistencyin meta-analysis. Brit Med J 2003; 327:557–60.
13. Egger M, Davey S, Schneider M,Minder C. Bias in meta-analysisdetected by a simple, graphical test. BritMed J 1997; 315: 629–34.
14. Orwin R. A fail-safe N for effect sizein meta-analysis. J Educ Stat 1983; 8:157–9.
15. Parker DR, Kingham JG. Type Iautoimmune hepatitis is primarily adisease of later life. Q J Med 1997; 90:289–96.
16. Newton JL, Burt AD, Park JB, MatthewJ, Bassendine MF, James OF.Autoimmune hepatitis in older patients.Age Ageing 1997; 26: 441–4.
17. Schramm C, Kanzler S, Meyer zumBuschenfelde KH, Galle PR, Lohse AW.Autoimmune hepatitis in the elderly.Am J Gastroenterol 2001; 96: 1587–91.
18. Verslype C, George C, Buchel E,Nevens F, Van Steenbergen W, FeveryJ. Diagnosis and treatment ofautoimmune hepatitis at age 65 andolder. Aliment Pharm Ther 2005; 21:695–9.
19. Granito A, Muratori L, Pappas G, et al.Clinical features of type 1 autoimmunehepatitis in elderly Italian patients.Aliment Pharm Ther 2005; 21: 1273–7.
20. Czaja AJ, Carpenter HA. Distinctiveclinical phenotype and treatmentoutcome of type 1 autoimmunehepatitis in the elderly. Hepatology2006; 43: 532–8.
21. Al-Chalabi T, Boccato S, Portmann BC,McFarlane IG, Heneghan MA.Autoimmune hepatitis (AIH) in theelderly: a systematic retrospectiveanalysis of a large group of consecutivepatients with definite AIH followed at atertiary referral centre. J Hepatol 2006;45: 575–83.
22. Xie B, Parekh RM, Sood S, et al. S1262Autoimmune hepatitis in elderly isusually an advanced disease atpresentation, is less symptomatic andrelapse is infrequent. Gastroenterology2010; 138: S215–6.
23. Floreani A, Niro G, Rizzotto ER, et al.Type I autoimmune hepatitis: clinicalcourse and outcome in an Italianmulticentre study. Aliment Pharm Ther2006; 24: 1051–7.
24. Miyake Y, Iwasaki Y, Takaki A,Kobashi H, Sakaguchi K, Shiratori Y.Clinical features of Japanese elderlypatients with type 1 autoimmunehepatitis. Internal Med 2007; 46:1945–9.
25. Czaja AJ. Special clinical challenges inautoimmune hepatitis: the elderly,males, pregnancy, mild disease,fulminant onset, and nonwhite patients.Semin Liver Dis 2009; 29: 315–30.
26. Medina J, Garcia-Buey L, Moreno-Otero R. Review article:immunopathogenetic and therapeuticaspects of autoimmune hepatitis.Aliment Pharm Ther 2003; 17: 1–16.
27. Yeoman AD, Longhi MS, HeneghanMA. Review article: the modernmanagement of autoimmunehepatitis. Aliment Pharm Ther 2010; 31:771–87.
28. Kanzler S, Gerken G, Lohr H, Galle PR,Meyer zum Buschenfelde KH, LohseAW. Duration of immunosuppressivetherapy in autoimmune hepatitis. JHepatol 2001; 34: 354–5.
29. Czaja AJ, Carpenter HA, Santrach PJ,Moore SB. Significance of HLA DR4 intype 1 autoimmune hepatitis.Gastroenterology 1993; 105:1502–7.
30. Czaja AJ, Strettell MDJ, Thomson LJ,et al. Associations between allelesof the major histocompatibilitycomplex and type 1 autoimmunehepatitis. Hepatology 1997; 25:317–23.
124 Aliment Pharmacol Ther 2014; 39: 117-124
ª 2013 John Wiley & Sons Ltd
J. Chen et al.