Embed Size (px)
Citation preview

Systematic Reviews of the Literature and Meta-analyses:
….problems or panacea?
Daren K. Heyland, MD, FRCPC, MSc
Queen’s University, Kingston, Ontario

www.criticalcarenutrition.com
Updated Jan 2009
Summarizes >200 trials studying 21283 patients
34 topics 17 recommendations
Clinical Practice Guidelines
Validity Homogeneity
SafetyFeasibility
Cost
evidence integration of values+
practiceguidelines
In Search of Truth...…Does it work?
Begins with a hypothesis or question Does Drug X reduce the incidence of problem Y in patients
with condition Z
Application of experimental or observational methods to determine the answer
Results of our observations leads to conclusions that are correct (truth) or incorrect (due to bias or chance)

Levels of Evidence
Systematic reviews RCT’s Cohort Studies Case Control Case Series
less bias/strong inferences
more bias/weaker inferences

198 RCT’s Reviewed in Critical Care Nutrition Guidelines
PLOS 2008;5: e4

Will be able to appraise and incorporate results of systematic reviews into clinical decision making.
understand the role of systematic reviews in research and policy settings.
List the strengths and weakness of meta-analyses
Learning Objectives
Overview
Definition and Classification Usefulness Methodological Quality Making Inferences Conclusions
Systematic Review…
Form of scientific investigation to assess the effectiveness of healthcare interventions
Integrative research Subjects= original or primary studies Employs methods that limit bias and reduce random
error
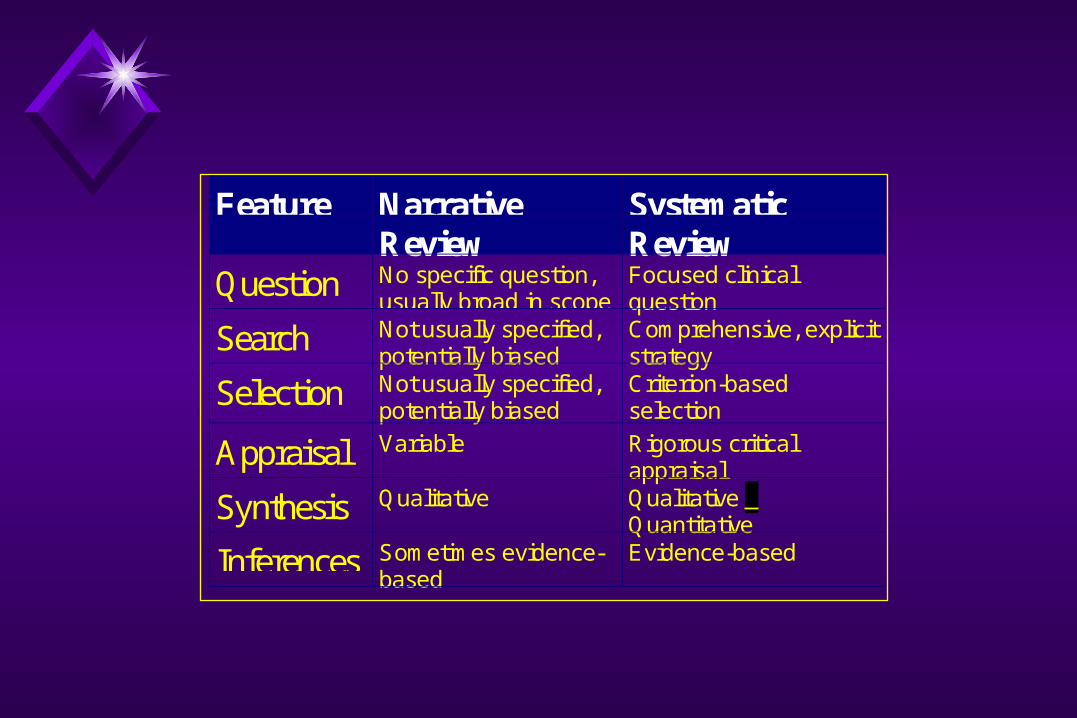
Feature NarrativeReview
SystematicReview
Question No specific question,usually broad in scope
Focused clinicalquestion
Search Not usually specified,potentially biased
Comprehensive, explicitstrategy
Selection Not usually specified,potentially biased
Criterion-basedselection
Appraisal Variable Rigorous criticalappraisal
Synthesis Qualitative Qualitative + Quantitative
Inferences Sometimes evidence-based
Evidence-based
Systematic Reviews and Meta-analysis
Narrative Reviews
Systematic Reviews
Meta-analysis
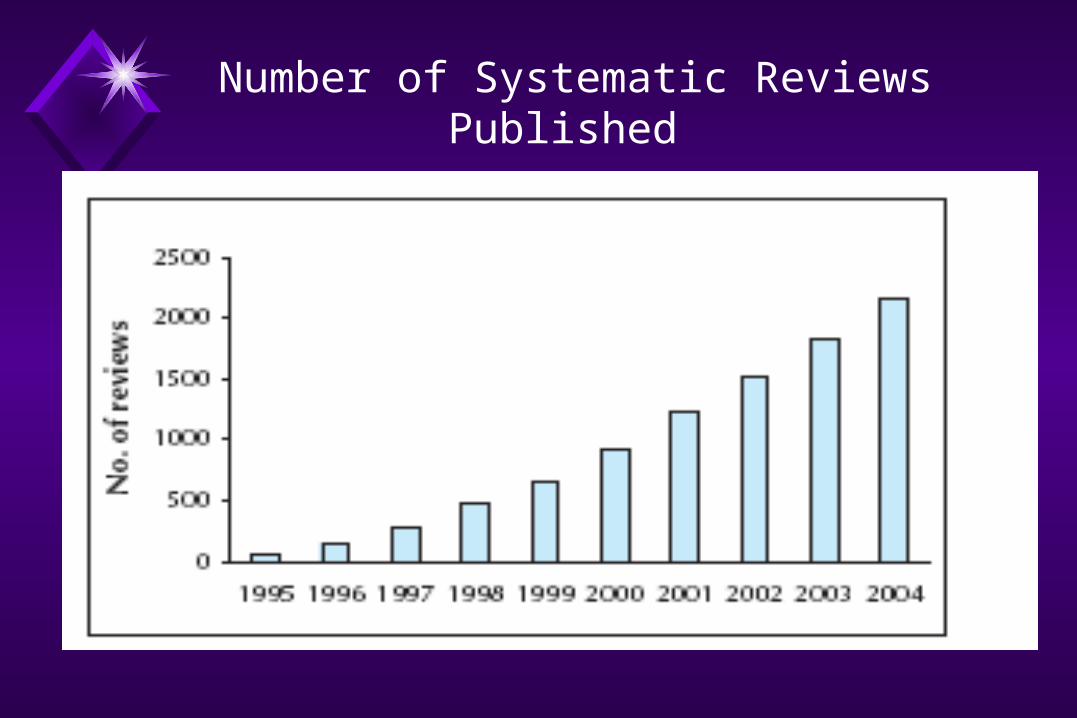
Number of Systematic Reviews Published

The Frailties of Narrative Reviews
If the original studies of thrombolytics therapies had been subject to a systematic review, the treatment effect would have been apparent in the 1970s instead of 1980s.
Narrative reviews omitted effective therapies and endorsed ineffective therapies.
Antman JAMA1992;268;240 and Lau NEJM 1992;327:248

Clinical Decision Making and Systematic Reviews
Case Scenario 77 y.o. male with presumptive Dx of Urosepsis PMHX: MI, Prostate BMI 21 After initial resuscitation
FiO2 = 100%, PO2 = 55 MAP = 65, CVP 13, levophed 20 mcg/kgk/min rising Cr, 20 ml of urine, acidemic High NG drainage
Going to start on EN but not likely to tolerate Role for early supplemental PN?
Clinical Decision Making and Systematic Reviews
Problem 100s of citations across scores of journals published over
the last 20 years In diverse patient populations or diverse settings with variable or inconsistent results!
How do you make sense of this all?

Impact of Caloric Debt
Caloric debt associated with:
Longer ICU stay
Days on mechanical ventilation
Complications
Mortality
Adequacy of EN
Rubinson CCM 2004; Villet Clin Nutr 2005; Dvir Clin Nutr 2006; Petros Clin Nutr 2006
0200
400600
8001000
12001400
16001800
2000
1 3 5 7 9 11 13 15 17 19 21
Days
kcal
Prescribed Engergy
Energy Received From Enteral Feed
Caloric Debt

2007 International Nutrition Practice Survey
Point prevalence survey of nutrition practices in ICU’s around the world conducted Jan. 27, 2007
Enrolled 2772 patients from 158 ICU’s over 5 continents
Included ventilated adult patients who remained in ICU >72 hours

HypothesisHypothesis
There is a relationship between amount of energy and protein received and clinical outcomes (mortality and # of days on ventilator)
The relationship is influenced by nutritional risk BMI is used to define chronic nutritional risk
What Study Patients Actually Rec’d
Average Calories in all groups: 1034 kcals and 47 gm of protein
Result: Average caloric deficit in Lean Pts:
7500kcal/10days Average caloric deficit in Severely Obese:
12000kcal/10days
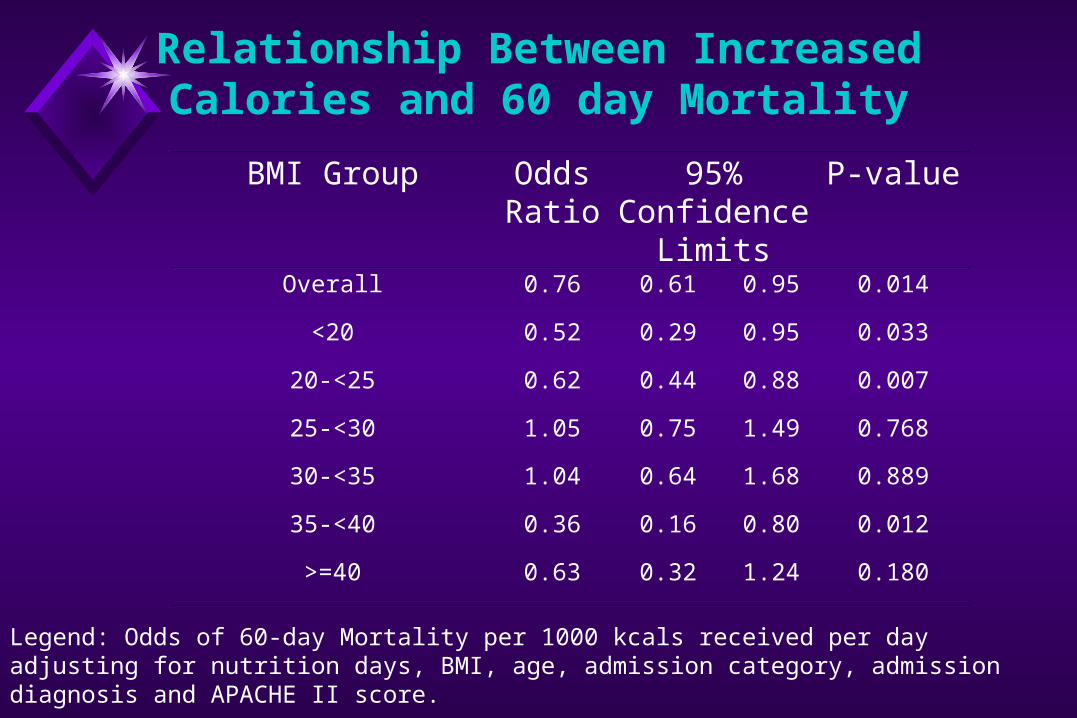
Relationship Between Increased Calories and 60 day Mortality
BMI Group Odds Ratio
95% Confidence
Limits
P-value
Overall 0.76 0.61 0.95 0.014
<20 0.52 0.29 0.95 0.033
20-<25 0.62 0.44 0.88 0.007
25-<30 1.05 0.75 1.49 0.768
30-<35 1.04 0.64 1.68 0.889
35-<40 0.36 0.16 0.80 0.012
>=40 0.63 0.32 1.24 0.180
Legend: Odds of 60-day Mortality per 1000 kcals received per day adjusting for nutrition days, BMI, age, admission category, admission diagnosis and APACHE II score.
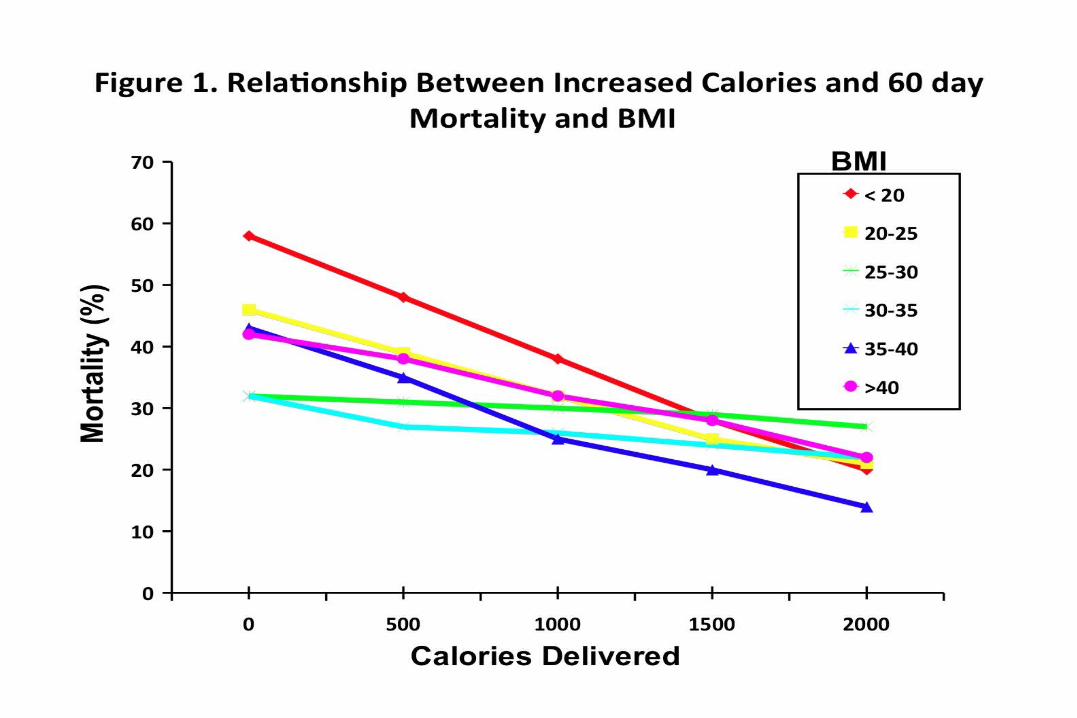
RESULTS: WHO IS AT RISK?
RCT Level of Evidence that More EN= Improved Outcomes
RCTs of aggressive feeding protocols Results in better protein-energy intake Associated with reduced complications and improved survival
Taylor et al Crit Care Med 1999; Martin CMAJ 2004
Meta-analysis of Early vs Delayed EN Reduced infections: RR 0.76 (.59,0.98),p=0.04 Reduced Mortality: RR 0.68 (0.46, 1.01) p=0.06
www.criticalcarenutrition.com

More is Better!
Our Field of DreamIf you feed them (better!)
They will leave (sooner!)
ICU patients are not all created equal…should we expect the impact of nutrition therapy to be the
same across all patients?b
What if you can’t provide adequate nutrition enterally?
… to TPN or not to TPN,
that is the question!
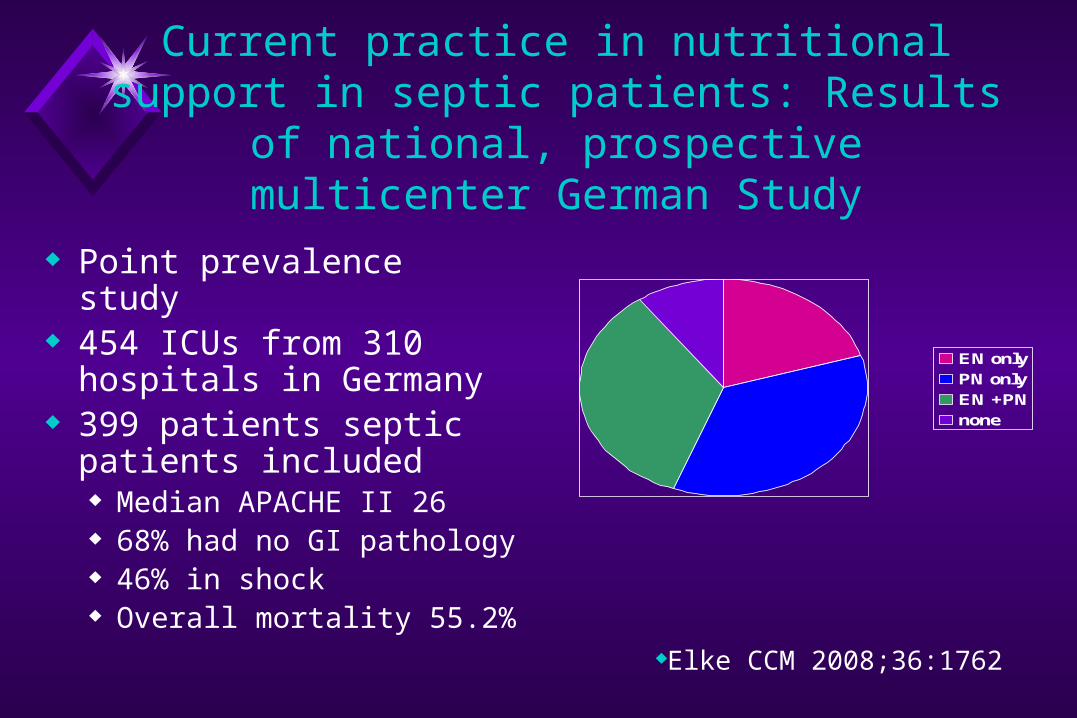
Current practice in nutritional support in septic patients: Results of national,
prospective multicenter German Study
Point prevalence study 454 ICUs from 310 hospitals
in Germany 399 patients septic patients
included Median APACHE II 26 68% had no GI pathology 46% in shock Overall mortality 55.2%
EN onlyPN onlyEN +PNnone
Elke CCM 2008;36:1762

Current practice in nutritional support in septic patients: Results of national,
prospective multicenter German Study
Point prevalence study 454 ICUs from 310 hospitals
in Germany 399 patients septic patients
included Median APACHE II 26 68% had no GI pathology 46% in shock Overall mortality 55.2%
0
10
20
30
40
50
60
70
EN only PN only EN +PN
none
%mortality
P=0.005
Multivariate analysis:
PN independent predictor for mortality
(OR 2.09, 95% CI 1.29-3.37)
Early Supplemental PN is Associated with Increased Infection in
Critically Ill Trauma Patients
Retrospective, multicenter, cohort study of 597 severely injured patients
Compared those that rec’d PN within 7 to those who did not.
Also compared early PN group to subgroup of ‘EN tolerant’ (tolerated 1000 kcal any day during first week)
Adjusted for differences in key baseline demographics
Sena J Am Coll Surg 2008;207:459

Early Supplemental PN is Associated with Increased Infection in Critically Ill Trauma Patients
Differences not due to differences in glycemic control
No Early PN Early PN Odds RatioP value
Overall Adjusted
Nosocomial Infections 27% 56% 2.1 (1.3-3.5)P=0.003
Late ARDS 1% 8% 3.4 (1.0-11.0)P=0.04
Death 8% 23% 1.5 (0.8-3.0)P=0.24
EN tolerant analysis
Nosocomial Infections 42% 69% 2.5 (1.1-5.9)P=0.03
Late ARDS 2% 9% 5.4 (1.1-27.4)P=0.04
Death 8% 19% 2.7 (0.8-9.3)P=0.10
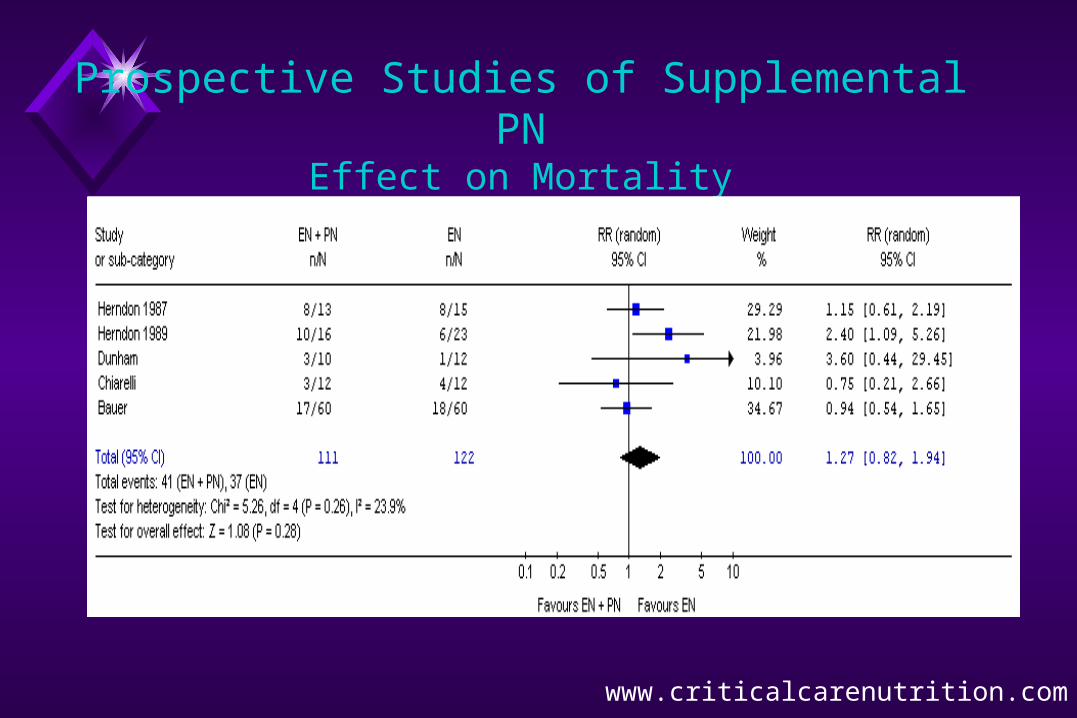
Prospective Studies of Supplemental PNEffect on Mortality
www.criticalcarenutrition.com

What if you can’t provide adequate nutrition enterally?
… to TPN or not to TPN,
that is the question!
Maximize EN delivery prior to initiating PN
Use of Supplemental PN in Sepsis?
Results of meta-analysis Results of single RCTs of Septic Patients Results of observational studies Consideration of Individual Patient
Characteristics
Using Systematic Reviews in Clinical Practice
Summarizes large body of knowledge Answers specific clinical question Less likely to be biased than narrative reviews More accurate and precise estimate of treatment
effect
Research Question: What is the effect of Glutamine and Antioxidant
supplementation on survival in critically ill patients?
Methods: A meta-analysis
Using Systematic Reviews in Research Setting
Effect of Glutamine in Critically Ill:
A Systematic Review of the Literature Comprehensive search
Selection criteria Randomized
Surgical or critically ill adults
Glutamine (EN or PN) vs. placebo
Clinically important outcomes
20 RCT’s
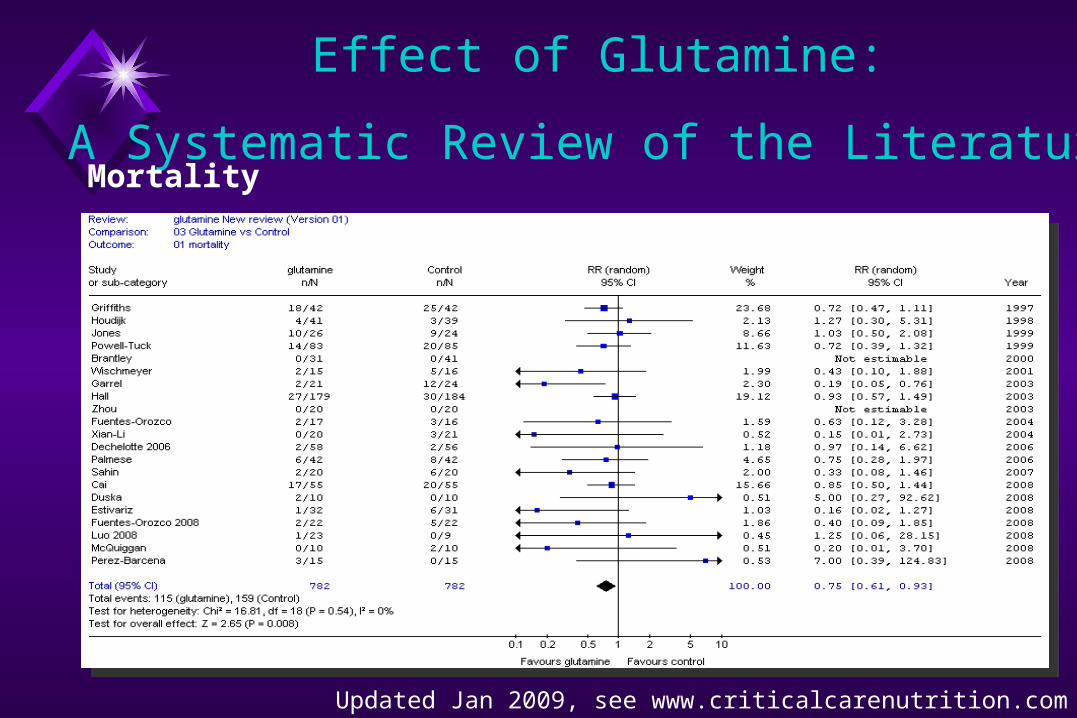
Effect of Glutamine:
A Systematic Review of the Literature
Updated Jan 2009, see www.criticalcarenutrition.com
Mortality
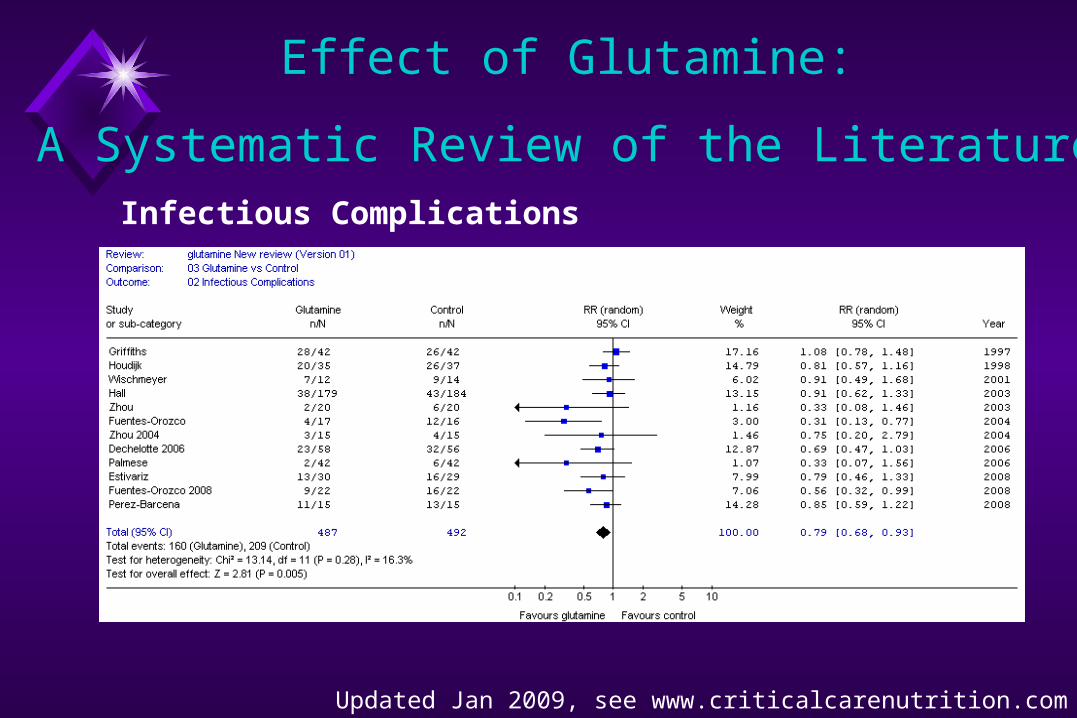
Effect of Glutamine:
A Systematic Review of the LiteratureInfectious Complications
Updated Jan 2009, see www.criticalcarenutrition.com
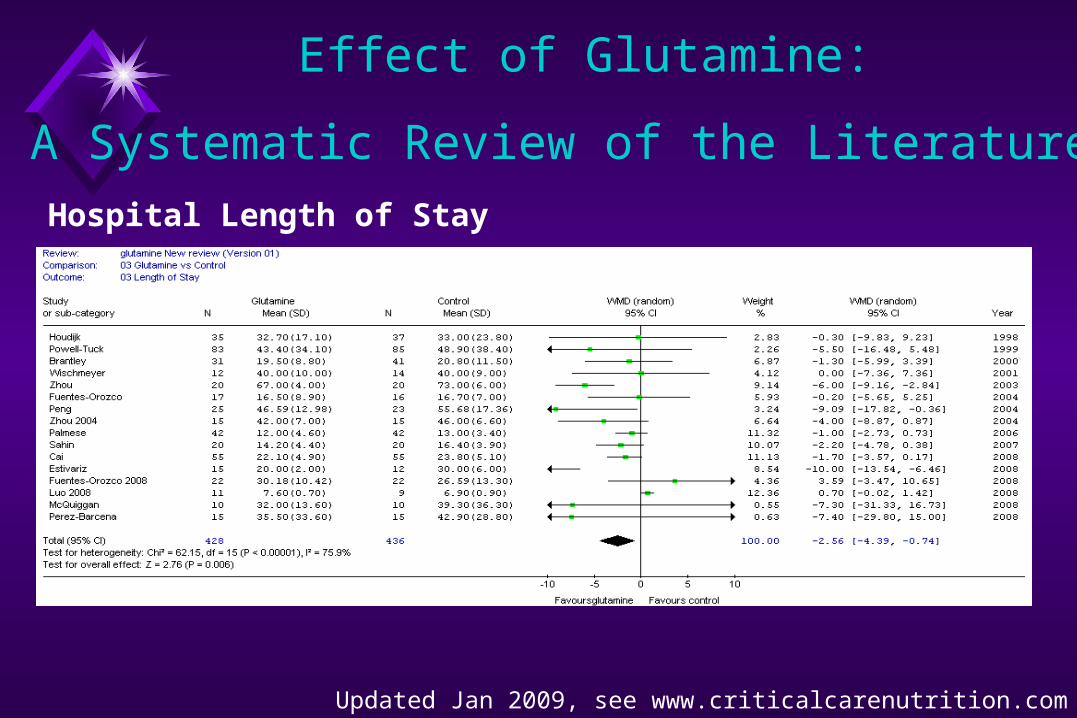
Effect of Glutamine:
A Systematic Review of the LiteratureHospital Length of Stay
Updated Jan 2009, see www.criticalcarenutrition.com
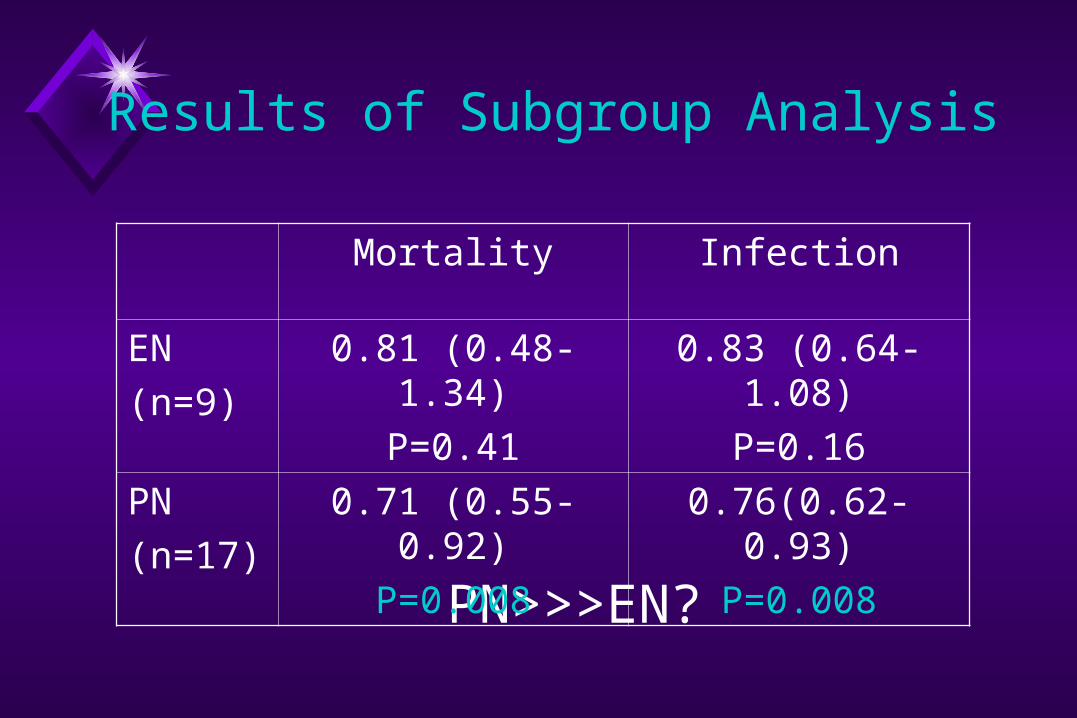
Results of Subgroup Analysis
PN>>>EN?
Mortality Infection
EN(n=9)
0.81 (0.48-1.34)P=0.41
0.83 (0.64-1.08)P=0.16
PN(n=17)
0.71 (0.55-0.92)P=0.008
0.76(0.62-0.93)P=0.008
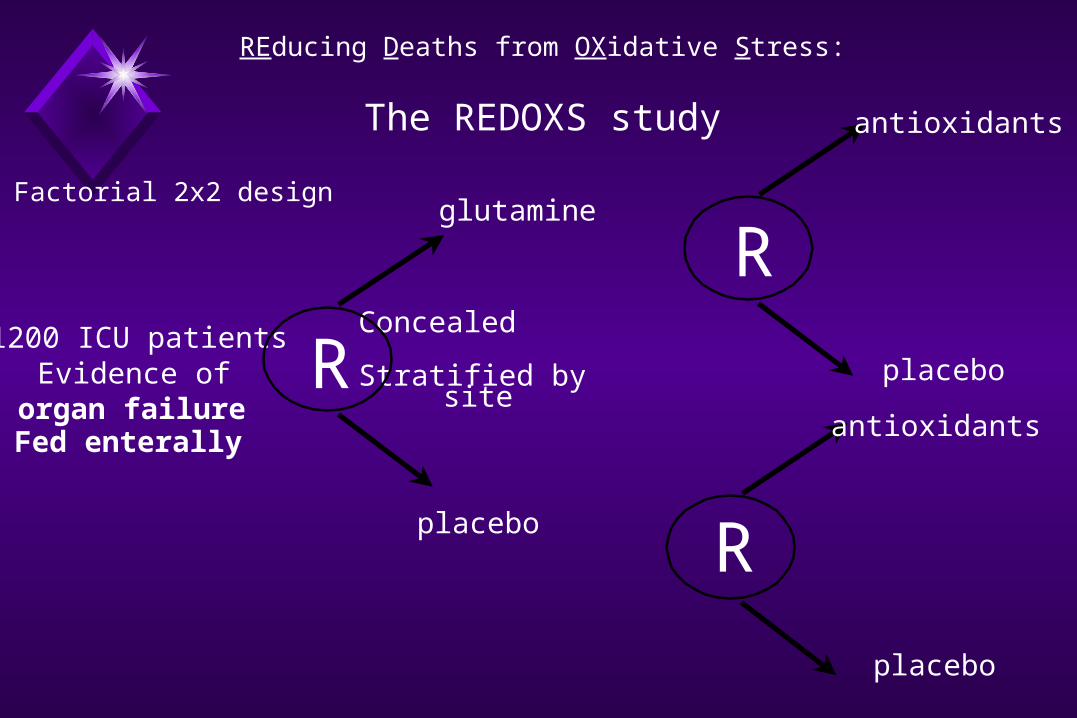
1200 ICU patientsEvidence of
organ failureR
glutamine
placebo
Concealed
Stratified by site
R
R
antioxidants
placebo
Factorial 2x2 design
placebo
antioxidants
REducing Deaths from OXidative Stress:
The REDOXS study
Fed enterally

Using Systematic Reviews in Research Setting
Summarizes what is known; identifies gaps Background of grant proposals Generates hypotheses Estimate of treatment effect N Subgroup analysis
Using Systematic Reviews in Policy Making
As an ICU, should you make an arginine-supplemented diet available for general use in your institution?
Meta-analyses of Meta-analyses of Arginine-supplemented DietsArginine-supplemented Diets
o 22 RCTs of IEDs All arginine-containing IED, not just IMPACT/IMMUNAID Non english, more recently published studies Excluded duplicates Excluded single agents
Heyland JAMA 2001;286:944
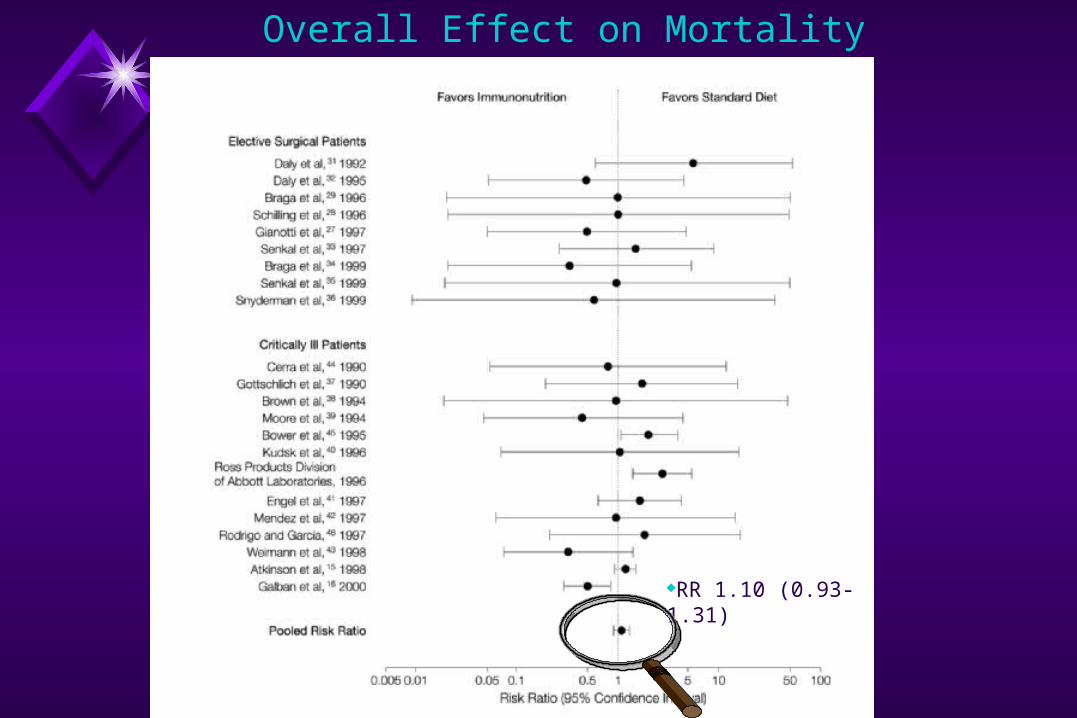
Overall Effect on Mortality
RR 1.10 (0.93-1.31)

Overall Effect on Complications
RR 0.66 (0.54-0.80)

1.18 (0.88,1.58)
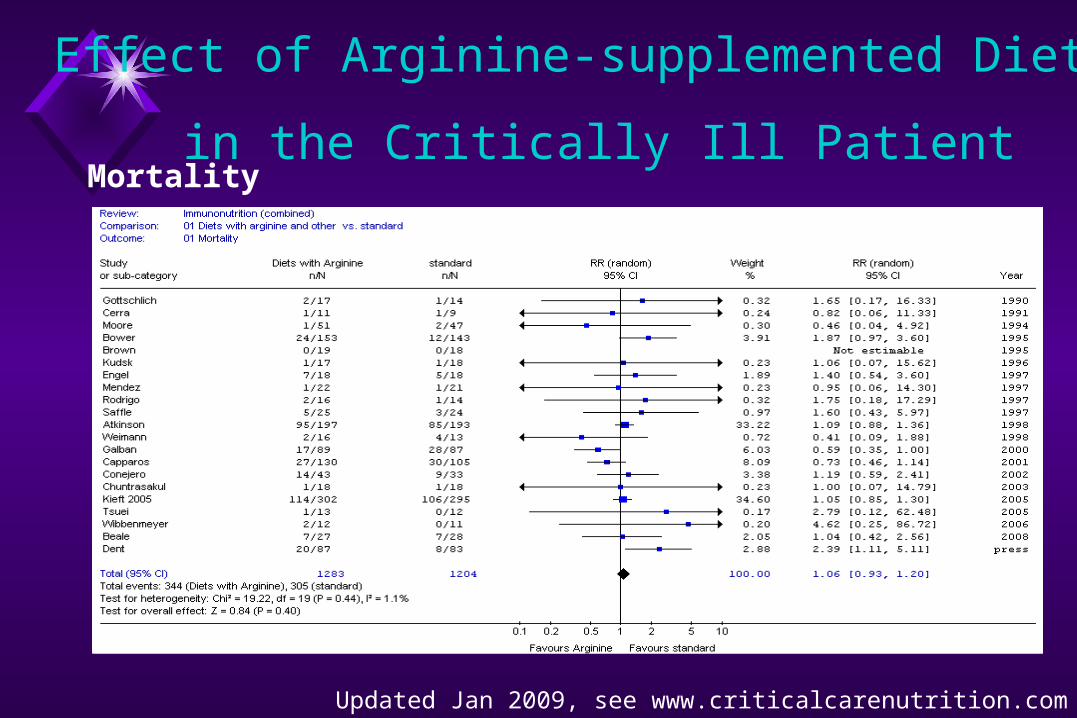
Effect of Arginine-supplemented Diets
in the Critically Ill Patient
Updated Jan 2009, see www.criticalcarenutrition.com
Mortality
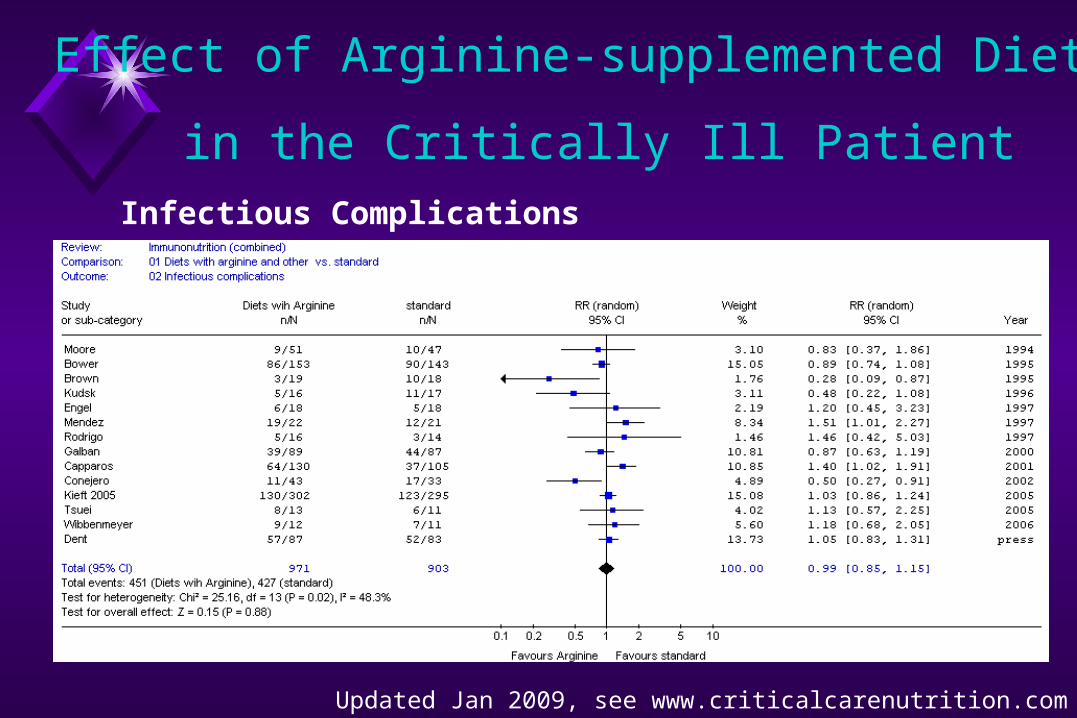
Infectious Complications
Updated Jan 2009, see www.criticalcarenutrition.com
Effect of Arginine-supplemented Diets
in the Critically Ill Patient

Hospital Length of Stay
Updated Jan 2009, see www.criticalcarenutrition.com
Effect of Arginine-supplemented Diets
in the Critically Ill Patient
Using Systematic Reviews in Policy Making
Greatest generalizability Consistent with perspective of policy makers Related to other forms of integrative research
Assessing the Validity of Systematic Reviews
Validity= fxn { inputs, process, results }
Inputs selection of studies
clinical homogeneity explicit, reproducible criteria
methodological quality of studies outdated/unmeasured co-interventions
Assessing the Validity of Systematic Reviews
Process comprehensive search strategy
publication/timing bias data excess language bias
judgements about inclusion explicit/reproducible data abstraction reproducible
Assessing the Validity of Systematic Reviews
Results few studies few clinical endpoints statistical heterogeneity
Assessing the Validity of Systematic Reviews

Methdological Quality of Methdological Quality of Meta-analysesMeta-analyses
lots of bias little bias
weak inferences
strong inferences
Strong clinical recommendations
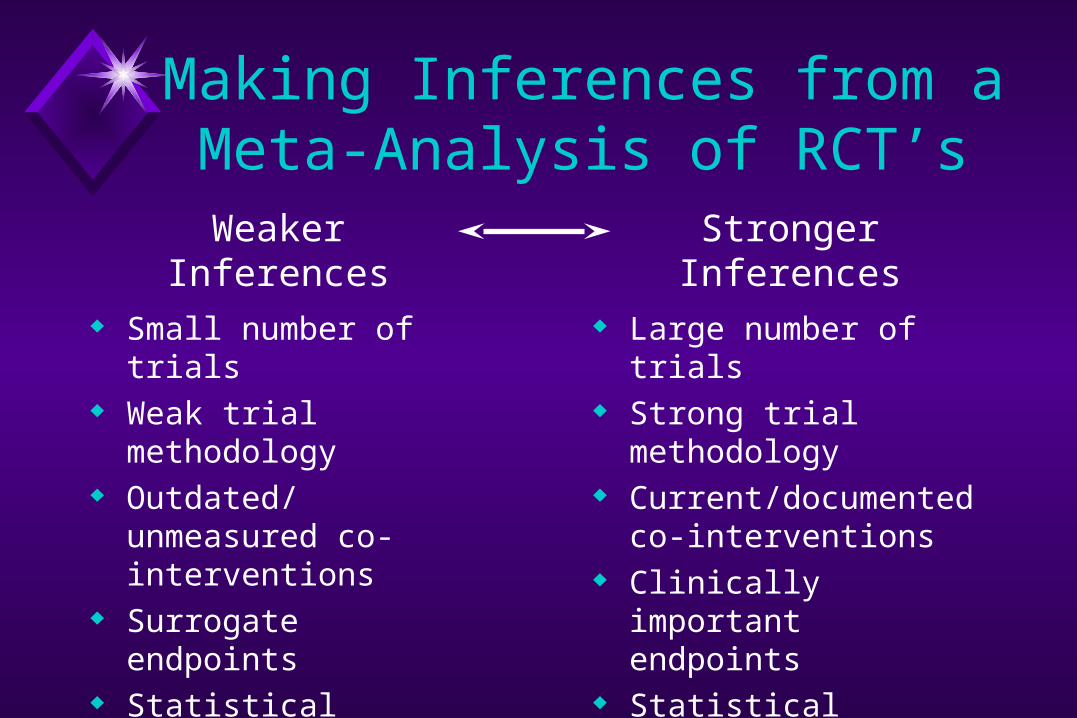
Making Inferences from a Meta-Analysis of RCT’s
Small number of trials Weak trial methodology Outdated/unmeasured
co-interventions Surrogate endpoints Statistical heterogeneity Fixed effects model
Large number of trials Strong trial methodology Current/documented co-
interventions Clinically important
endpoints Statistical homogeneity Random effects model
Weaker Inferences Stronger Inferences

Meta-analysis vs. Large RCT’s
“…if no subsequent randomized, clinical trial, the meta-analysis would have led to the adoption of an ineffective treatment in 32% cases and rejection of useful treatment in 33% cases.”
LeLorier NEJM 1997;337:536
“I still prefer conventional narrative reviews …Editorial, NEJM
Meta-analysis vs. Large RCT’s
RCT #1 RCT #2
RCT #3 RCT #4
RCT #5
Meta-analysis vs. Large RCT’s
Argument is with Meta-analysis, not the concept of systematic reviews
Assumes the latest single large trial is the GOLD standard
Assumes RCT and Meta-analysis are measuring the same thing
Differences in Generalizability Bias exists in both TOOLS.

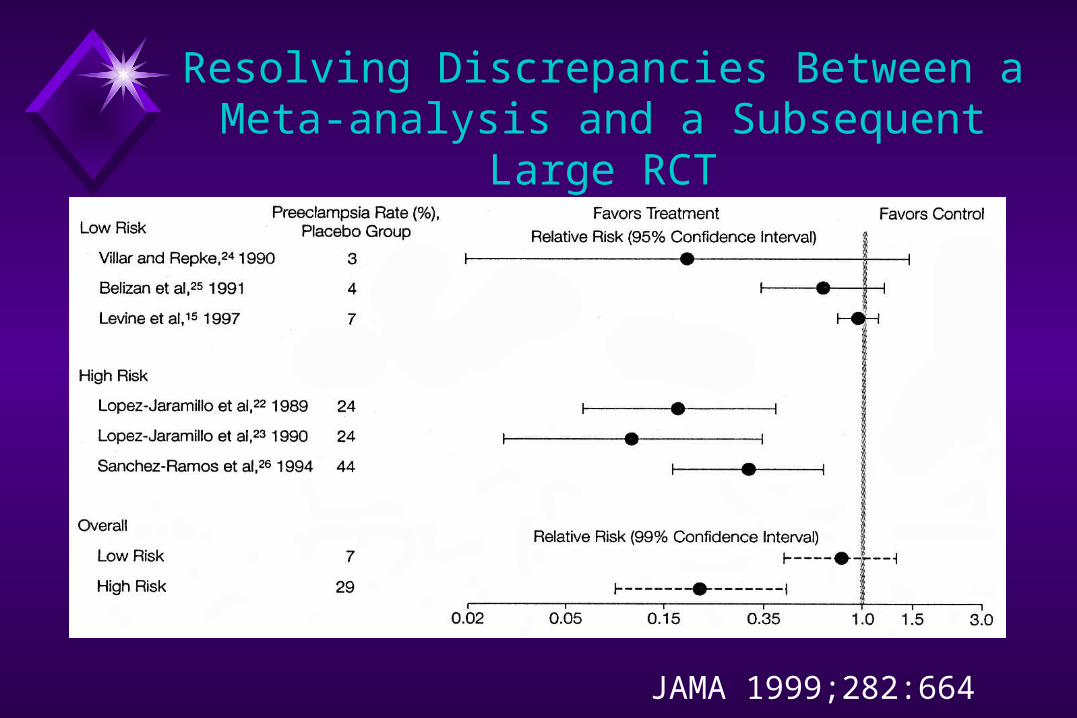
Resolving Discrepancies Between a Meta-analysis and a Subsequent Large
RCT
Recent meta-analysis found calcuim supplementation to be effective in preventing preeclampsia
Large RCT found no risk reduction in health nulliparous women
Exploration of heterogeneity across studies Stratify for high and low baseline risk
JAMA 1999;282:664
Resolving Discrepancies Between a Meta-analysis and a Subsequent Large
RCT
JAMA 1999;282:664
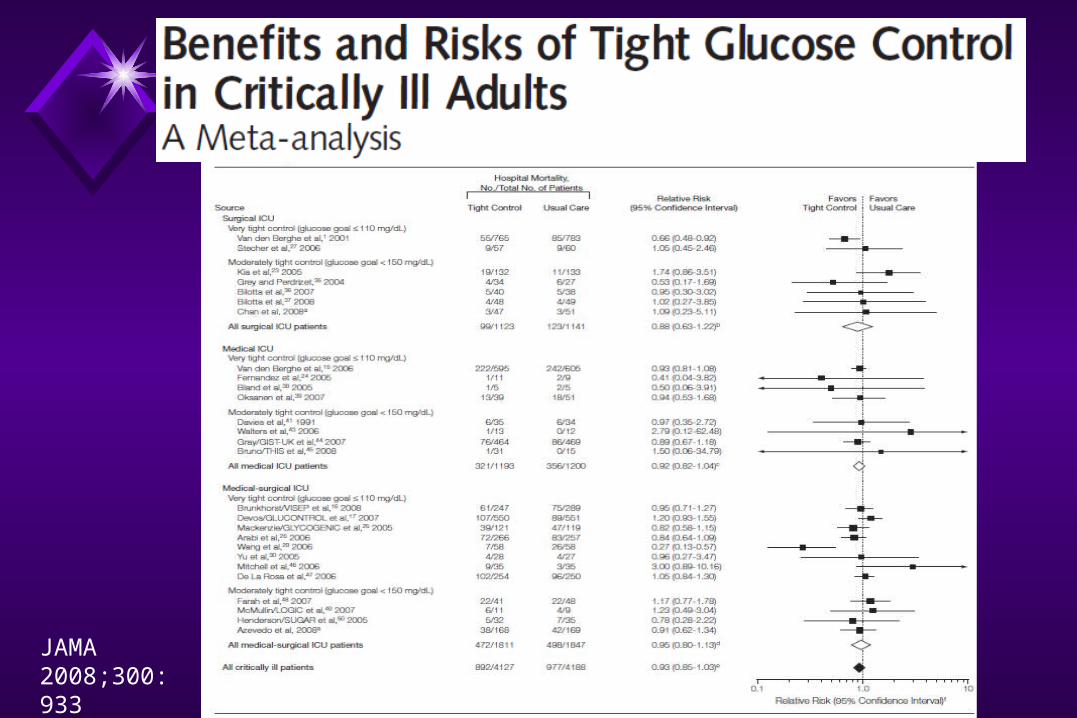
JAMA 2008;300:933
Role of Systematic Reviews in Medical Education
Good source of medical knowledge Promotes EBM practices Helps locate original articles Facilitates critical appraisal of original research Considered a scholarly research activity
Conclusions
Important tool to determine the effectiveness of therapeutic interventions
Need to understand the strengths, weaknesses and limitations
Useful in clinical and policy decision making and research setting
Encourage use of and generation of systematic reviews amongst learners.