Embed Size (px)
Citation preview

What would happen next?
Gamma blast Heat blast Pressure wave Sudden fierce wind Firestorm Dissipating cloud : spreads throughout
environment: undetectable
HTTP://WWW.ANIMATEDSOFTWARE.COM/ENVIRONM/NO_NUKES/TENW/NUKE_WAR.HTM
Multi-spectral heat blast (mostly x-ray and ultraviolet wavelengths)
People outside the circle: light from the explosion (which is many times hotter than the sun) is so bright that it will immediately and permanently blind every living thing, whether their eyes are opened or closed.
This will happen for 10 miles
Pressure wave
Will cause bleeding from every orifice
Momentary high winds which accompany the pressure wave
Flying debris will cause shrapnel-type wounds and blunt-trauma injuries
Internal molecular structure of the living cells within their bodies starts breaking down
People will begin to suffer from vomiting, skin rashes, and an intense unquenchable thirst as their hair falls out in clumps. Their skin will begin to peel off
Animals will be similarly suffering
Firestorm Intense heat and hurricane-force winds, all
driving towards the center where the radioactive mushroom-shaped cloud will be rising, feeding it, enlarging it, and pushing it miles up into the sky
The firestorm produces hurricane-force winds in a matter of minutes.
The fire burns so hot that the asphalt in the streets begins to melt and then burn, even as people are trying to run across it, literally melting into the pavement themselves as they run.
Victims, on fire, jump into rivers, only to catch fire again when they surface for air
Cloud will reach nearly 10 miles across and equally high. Soon after forming, it will turn white because of water condensation It will have largely dissipated, which
means that its cargo of death can no longer be tracked visually
Difficult to predict where the cloud will travel before it happens, and it is likewise difficult to track the cloud as it moves and dissipates around the globe.
People’s fate??
Instant death Get better, tingling and itching
sensation, and then, Internal organs turn to bloody pulp and slow painful torturous death
After a while, cancers slowly start appearing, genetic damage passed onto offspring
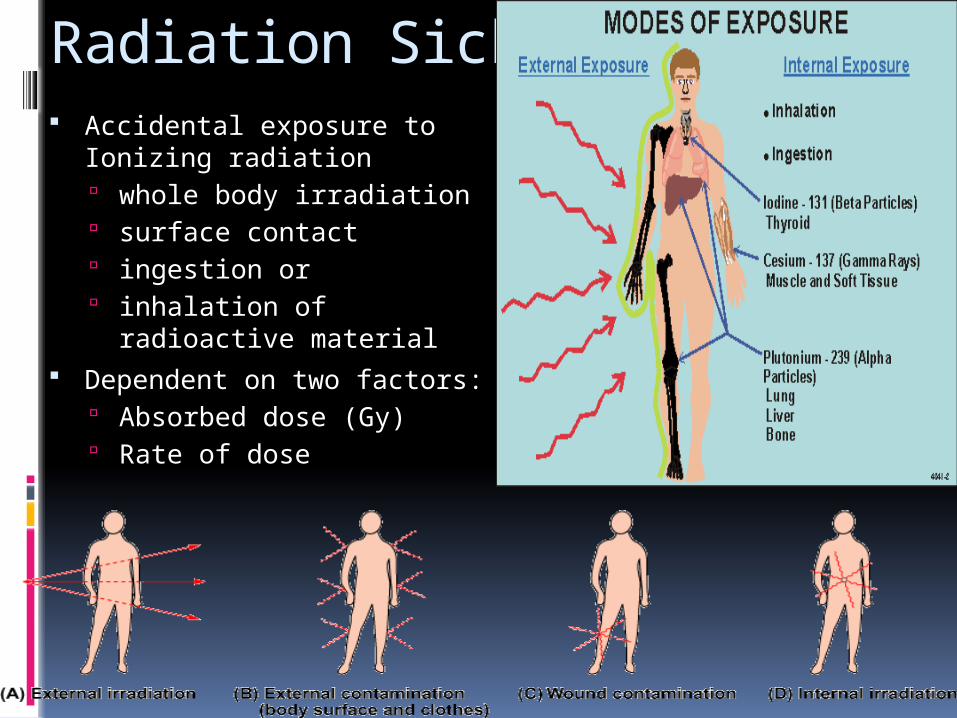
Radiation Sickness Accidental exposure to
Ionizing radiation whole body irradiation surface contact ingestion or inhalation of radioactive
material Dependent on two factors:
Absorbed dose (Gy) Rate of dose
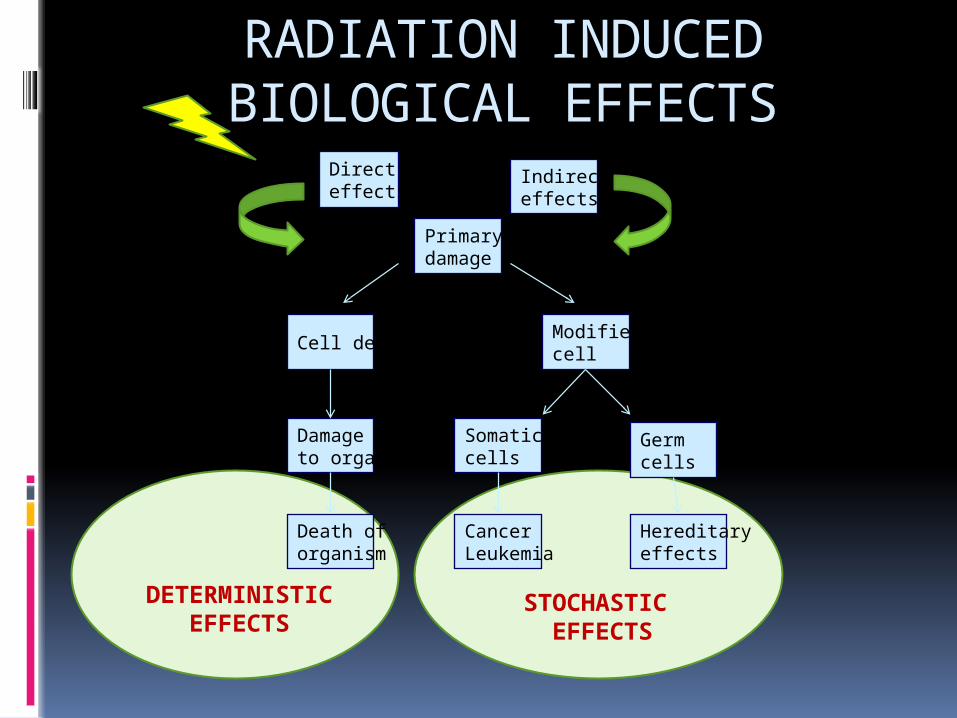
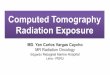
RADIATION INDUCED BIOLOGICAL EFFECTS
Directeffects
Indirecteffects
Primarydamage
Cell deathModifiedcell
Damageto organ
Death oforganism
Somaticcells
Germcells
CancerLeukemia
Hereditaryeffects
DETERMINISTIC EFFECTS
STOCHASTIC EFFECTS
Types: Acute Radiation Sickness (ARS)
single large dose or recurrent small doses of radiation
wide range of symptoms exhibited within a few days or weeks cell death and cellular damage occur due to
metabolic disturbances, permeability and conductivity changes
Chronic Radiation Sickness Exposure to low doses over a large time period symptoms manifest after a longer gap of a few
years to decades
Cell damage: Damage to cell can be:
lethal (the cell dies) OR sublethal (the cell can repair itself)
Effects on cells can be: Deterministic:
Have a threshold of irradiation under which they do not appear The damage they cause depends on the dose: sublethal from 0.25 to
2 Sv (a less pronounced form of disease); lethal from 2 to 5 Sv (a certain percent of the population dies within 60 days); >5 Sv most people die within 60 days; and >6 to 7 Sv all people die
Stochastic: Stochastic effects do not have a threshold of irradiation, are
coincidental, and cannot be avoided. Divided into somatic and genetic effects. Among the somatic effects, secondary cancer is the most important.
It develops because radiation causes DNA mutations directly (by ionizing particles and rays) and indirectly(by free radicals, generated especially in water and oxygen radiolysis).
The genetic effects confer the predisposition of cancer to the offspring
Some organ systems and tissues (GI Tract, Hematopoietic system) have a higher susceptibility to radiation damage, whereas other (Neurovascular) show pathology after prolonged exposure.
The time between exposure to radiation and appearance of earliest symptoms (nausea and vomiting) and their severity are deterministic of absorbed radiation dose.
The threshold dose determines sensitivity of cells and time period depends on proliferation kinetics of cells [rapidly proliferating cells are more radiosensitive than differentiated cells (except for lymphocytes)].
Bergonie and Tribondeu’s law: “X-rays are more effective on cells which have a greater reproductive activity”.
Found untrue: tumor cells hypoxic environment, need higher dose
Other factors which influence the response to radiation: High Linear Energy Transfer or LET
Densely ionizing radiation have higher RBE and are more harmful
Fractionated exposure and a larger time period Less damaging
Lower metabolic rate Increases radioresistance
Gender Estrogens act as radioprotectors
Hypoxia Enhanced radioresistance
Phases of Radiation Sickness Prodromal Phase (N-V-D stage):
Initial appearance of symptoms (nausea, vomiting, fatigue, diarrhea, shock, ataxia, disorientation, etc.)
Within a few hours and up to a week
Latent Phase: Complete lack of illness/ symptoms for 1-4weeks
Manifest illness/ Critical Phase: A relapse into severe symptomatology (GI,
hematopoetic and CNS syndromes) In extremely high doses (2-6 Gy), death within a
few days.
Recovery or death
Hematopoietic Syndrome 2-7 Gy Occurs upon irradiation of bone marrow inflicting
irreversible damage to the proliferative capacity of the spleen and bone marrow
Nausea, vomiting and anorexia within a few hours at the higher dose levels, or after 6 to 12 hours at the lower dose levels. Lasts 24 to 48 hours.
The number of circulating granulocytes, platelets and erythrocytes decreases rapidly
This leads to infection, but can recover as stem cells in the bone marrow are never completely eradicated at 2 to 10 Gy.
Gastrointestinal syndrome 7-15 Gy immediate, prompt and profuse onset of nausea,
vomiting and diarrhea, followed by a short latent period.
Occurs due to destruction of intestinal villi , basal epithelial cells.
GI mucosa becomes increasingly atrophic, Plasma and electrolytes are lost into the intestines, hemorrhages and ulcerations occur, resulting in marked dehydration and vascular effects
The surface gets rapidly infected; combined with Hematopoietic syndrome, septicemia and death occur invariably
Cardiovascular Syndrome
>30 Gy Always fatal, there is immediate nausea,
vomiting, anorexia and prostration, and irreversible hypotension; blood pressure will be markedly unstable.
Within hours after exposure, the victim will be listless, drowsy, tremulous, convulsive, and ataxic.
Death most likely will occur within a matter of days.
CNS syndrome
> 50 Gy Increased pressure in the confining
cranial vault as the result of increased fluid content caused by edema, vasculitis, and meningitis
Uncoordinated movements, disorientation and convulsions
Due to damage to the neurons and brain vasculature
Death occurs in 1-2 days.
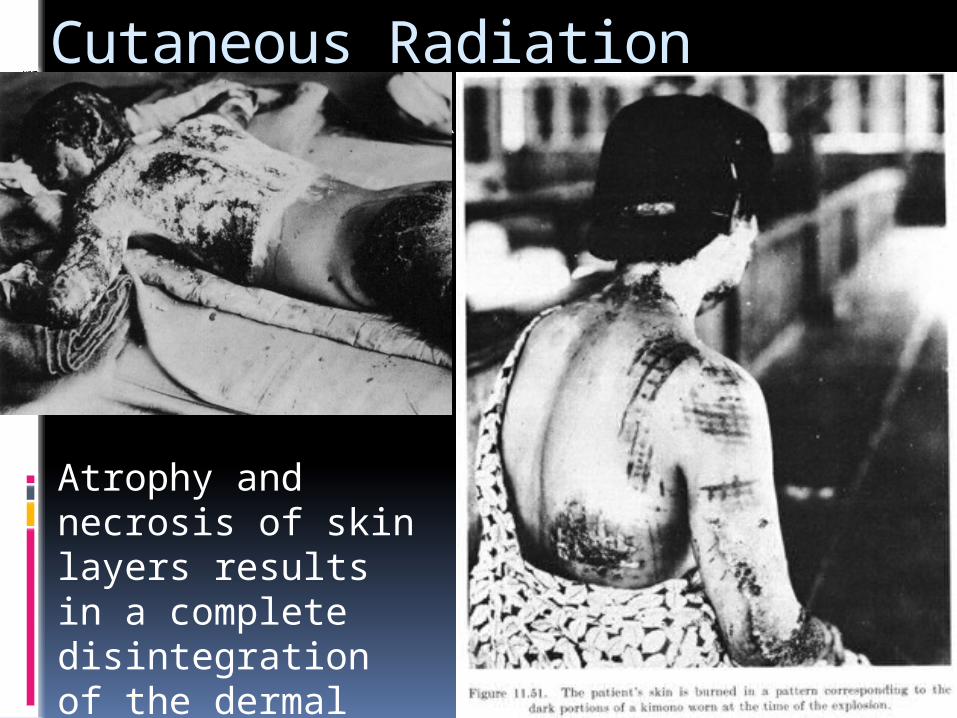
Cutaneous Radiation Syndrome (CRS)
Atrophy and necrosis of skin layers results in a complete disintegration of the dermal vascular system
Other effects
Temporary hair loss (2-6 Gy) Sterility (Males ~ 4 Gy; Females
>6.25 Gy) Cataractogenesis (doses > 2Gy
damage anterior epithelial cells in eye)
Fatal pneumonitis (acute lung exposure)
Nephritis (> 20 Gy) Increased Cardiovascular disease
prevalence
LATENT PERIOD
The time lapse between the exposure to radiation and the appearance of effects is referred to as the "latent period”
The latent time for a specific clinical effect as well as the progression rate, is inversely dependent on dose.
Therefore with increasing follow up time responses are also seen at lower dose levels.
Hence, the isoeffective doses for a defined clinical response decrease with increasing follow-up time.
F type tissues Acc to tissue organization models late-
responding tissues are flexible or F type tissues
As no clear separation can be made between proliferating and functional cells.
Proliferating cells are recruited into the functional population on demand, and vice versa.
Proliferatin
gFunction
al
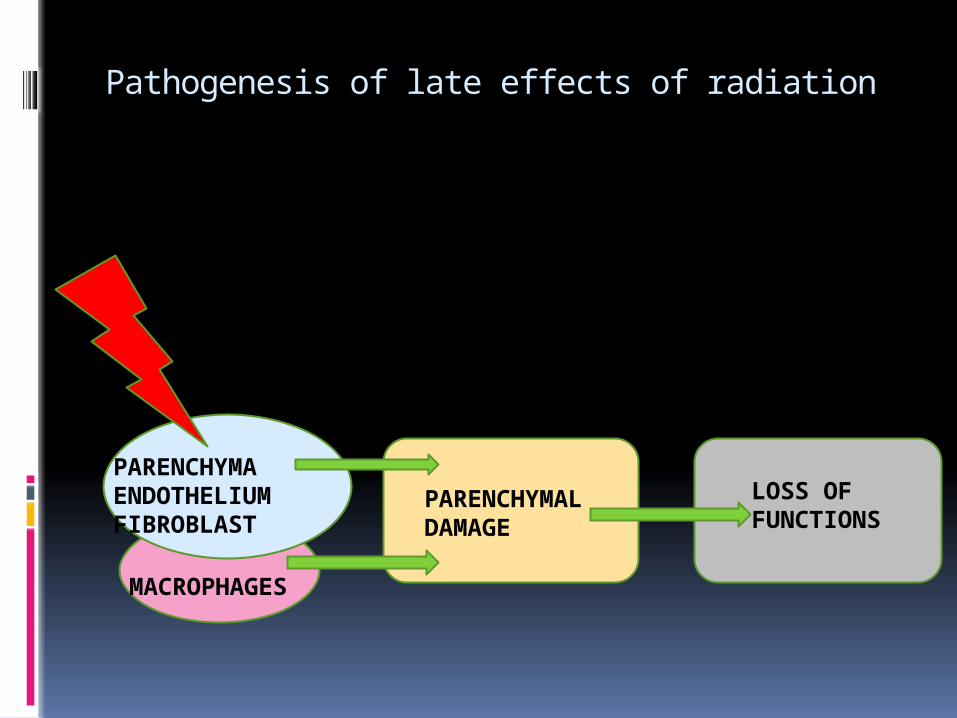
Pathogenesis of late effects of radiation
PARENCHYMAENDOTHELIUMFIBROBLAST
MACROPHAGES
PARENCHYMAL DAMAGE
LOSS OF FUNCTIONS
Models of clinical manifestation of late radiation effect
Parenchymal Effect
Proliferating cells are recruited into the functional population on demand
compensatory proliferation of the surviving parenchymal cells, which were originally functional
mitotic death of parenchymal cells
Cell loss accelerates
loss of organ function
TRU/FSU Damage
organ function loss
Endothelial Damage
Radiation induced endothelial damage
Capillary damage
Loss of oxygen supply
Loss of organ function
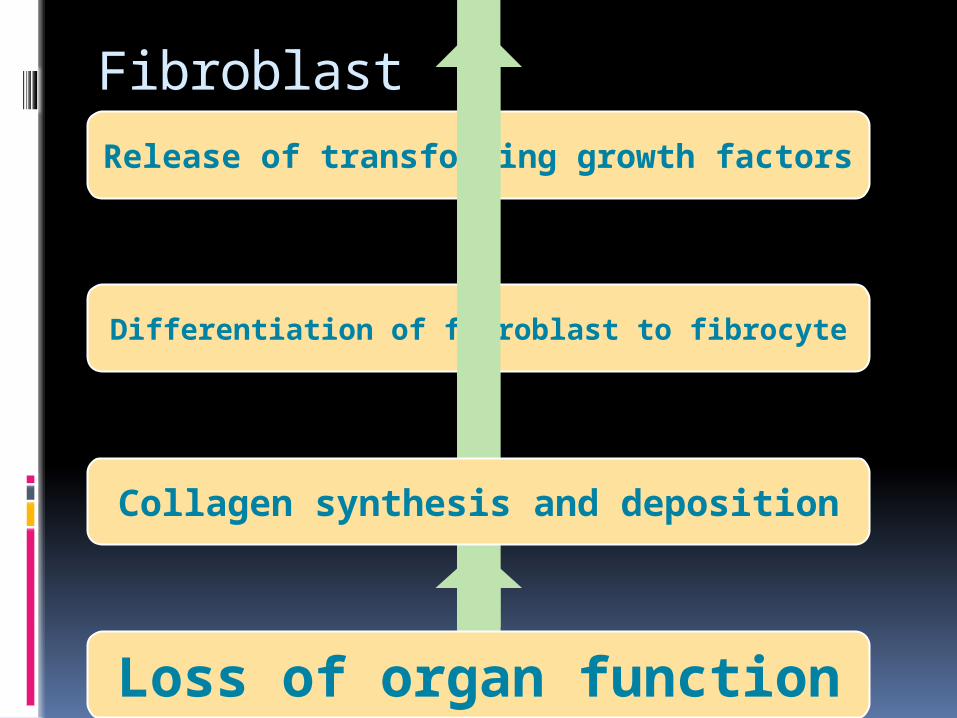
Fibroblast
Release of transforming growth factors
Differentiation of fibroblast to fibrocyte
Collagen synthesis and deposition
Loss of organ function
the definition of tolerance doses for late effects always requires information about the follow-up time on which the estimate is based
Summarising variables in Radiation Response
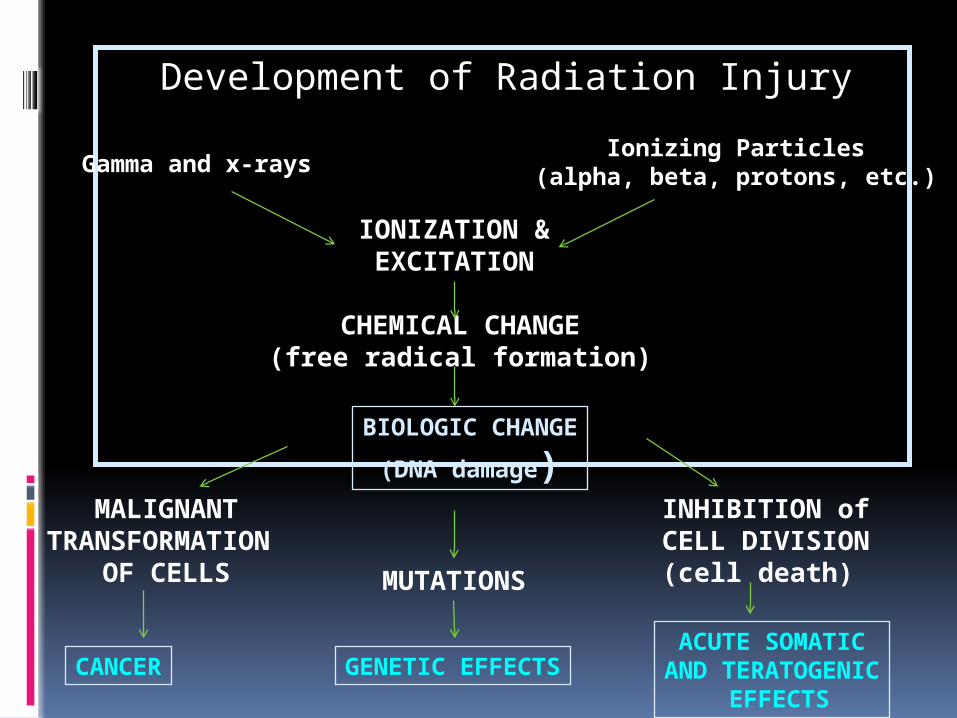
Development of Radiation Injury
Gamma and x-raysIonizing Particles
(alpha, beta, protons, etc.)
IONIZATION &EXCITATION
CHEMICAL CHANGE(free radical formation)
BIOLOGIC CHANGE
(DNA damage)MALIGNANT
TRANSFORMATION OF CELLS MUTATIONS
INHIBITION of CELL DIVISION(cell death)
CANCER GENETIC EFFECTSACUTE SOMATIC
AND TERATOGENIC EFFECTS
CASE STUDY- Whole Body Response
(ACUTE)
On December 30, 1958 an accident occurred in the Los Alamos plutonium-processing facility. Cecil Kelley, an experienced chemical operator was working with a large mixing tank. The solution in tank was supposed to be “lean”, typically less than 0.1 grams of plutonium per liter. However, the concentration on that day was actually 200 times higher. When Kelley switched on the stirrer, the liquid in the tank formed a vortex and the plutonium containing layer went critical releasing a huge burst of neutrons and gamma radiation in a pulse that lasted a mere 200 microseconds.
Kelley, who had been standing on a foot ladder peering into the tank through a viewing window, fell or was knocked to the floor. Two other operators on duty saw a bright flash and heard a dull thud. Quickly, they rushed to help and found Kelley incoherent and saying only, “I’m burning up! I’m burning up!”. He was rushed to the hospital, semiconscious, retching, vomiting, and hyperventilating. At the hospital, Kelly’s bodily excretions were sufficiently radioactive to give a positive reading on a detector.
Two hours after the accident, Kelley’s condition improved as he regained coherence. However, it was soon clear that Kelley would not survive long. Tests showed his bone marrow was destroyed, and the pain in his abdomen became difficult to control despite medication. Kelley died 35 hours after the accident
RADIOACTIVE MAN Eben McBurney Byers was a wealthy
American socialite, athlete, and industrialist. In 1927 while returning via chartered train from the annual Harvard-Yale football game, Byers fell from his berth and injured his arm. He complained of persistent pain and a doctor suggested that he take Radithor, a patent medicine containing high concentrations of radium. Byers drank nearly 1400 bottles over three years. By 1930, when Byers stopped taking the remedy, he had accumulated significant amounts of radium in his bones resulting in the loss of most of his jaw. Byers’ brain was also abscessed and holes were forming in his skull. He died from radium poisoning on March 31, 1932. He is buried in Allegheny Cemetery in Pittsburgh, Pennsylvania in a lead-lined coffin.
? What would you group Case A & Case B as:
Acute response/ Delayed Response Is there a dose dependent severity of
symptoms? Correlation with time of exposure? Organospecificity towards
radiosensitvity?
Somatic Response to radiation may be effected
by: Individual- Age, Sex, Metabolism Species Cellular & tissue Extent of exposure (full or partial body
exposure) LET Oxygen Effect Dose Dependence - Total Dose - Dose Rate
Dosage ; (IRCP values) Threshold Dose : Depend on dose delivery mode:
single high dose most effective fractionation increases threshold dose in most cases
significantly decreasing the dose rate increases threshold in most
cases Threshold may differ in different persons Criteria of dose
< 1 Gy: LOW DOSE 1-10 Gy: MODERATE DOSE > 10 Gy: HIGH DOSE
Lethal Dose It is an expression of the per cent lethal dose as a
function of time. It means: “Dose which would cause death to 50%
of the population in 30 days”. Its value is about 2-3 Gy for humans for whole
body irradiation
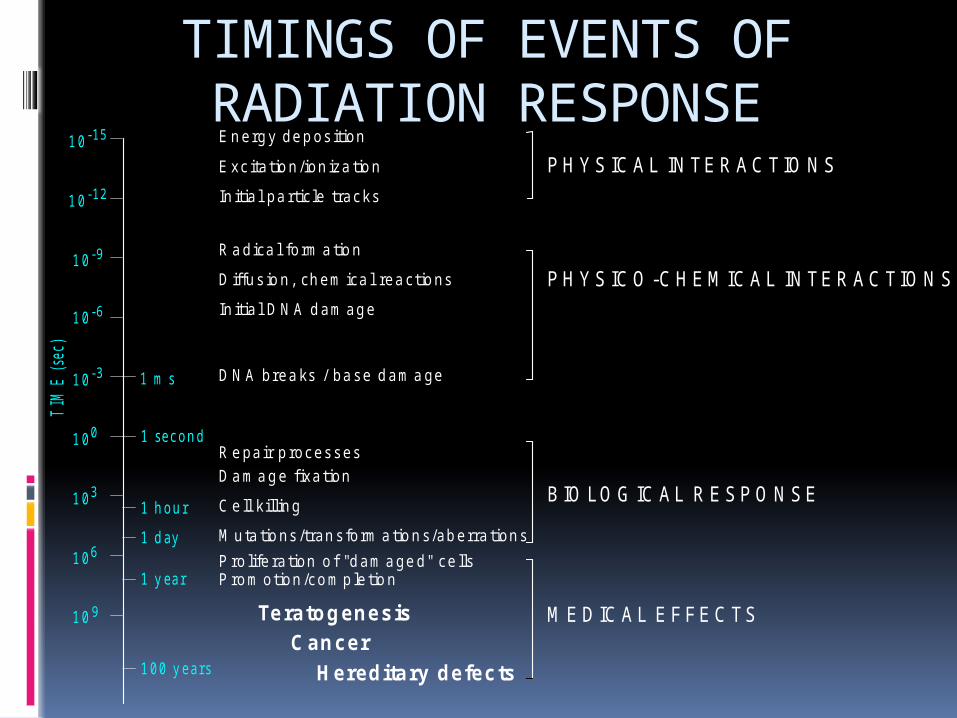
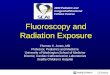
TIMINGS OF EVENTS OF RADIATION RESPONSE
1 0 -6
1 0 -12
1 0 -9
1 0 -15
1 0 -3
1 s e c o n d
1 h o u r
1 d ay
1 y ea r
1 0 0 y e a rs
1 m s
1 0 0
1 0 9
1 0 6
1 0 3
Energy deposition
Excitation/ionization
Initial particle tracks
Radical formation
PHYSICAL INTERACTIONS
PHYSICO-CHEMICAL INTERACTIONS
BIOLOGICAL RESPO NSE
MEDICAL EFFECTS
Diffusion, chemical reactions
Initial DNA damage
DNA breaks / base damage
Repair processes
Damage fixation
Cell killing
Promotion/completion
Teratogenesis
Cancer
Hereditary defects
Proliferation of "damaged" cells
Mutations/transformations/aberrations
TIM
E (
sec)
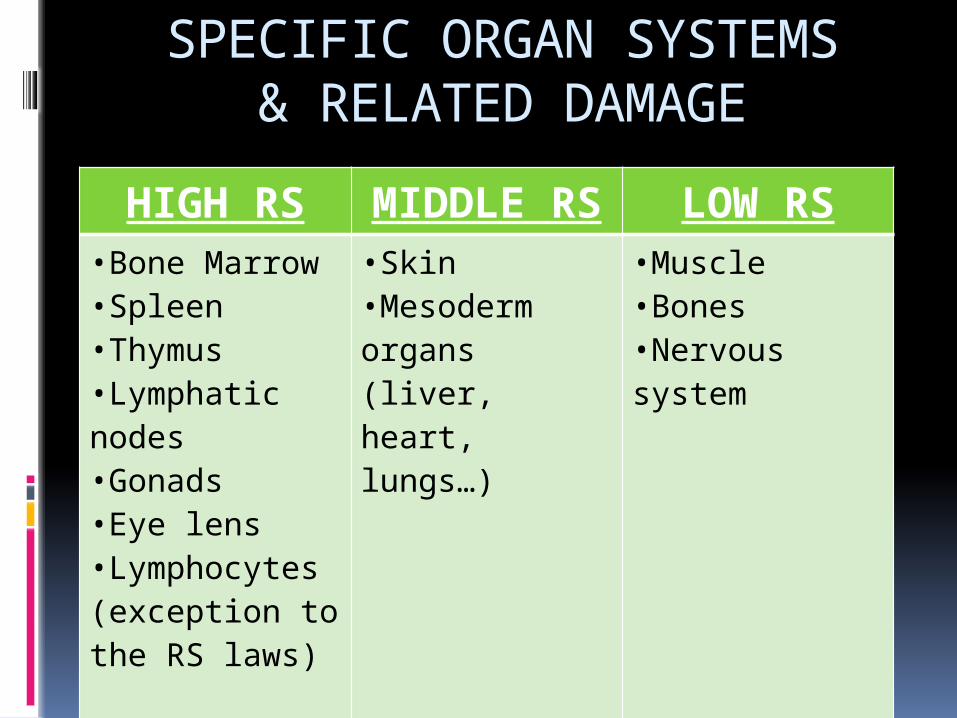
SPECIFIC ORGAN SYSTEMS& RELATED DAMAGE
HIGH RS MIDDLE RS
LOW RS
•Bone Marrow•Spleen•Thymus•Lymphatic nodes•Gonads•Eye lens•Lymphocytes (exception to the RS laws)
•Skin•Mesoderm organs (liver, heart, lungs…)
•Muscle•Bones•Nervous system
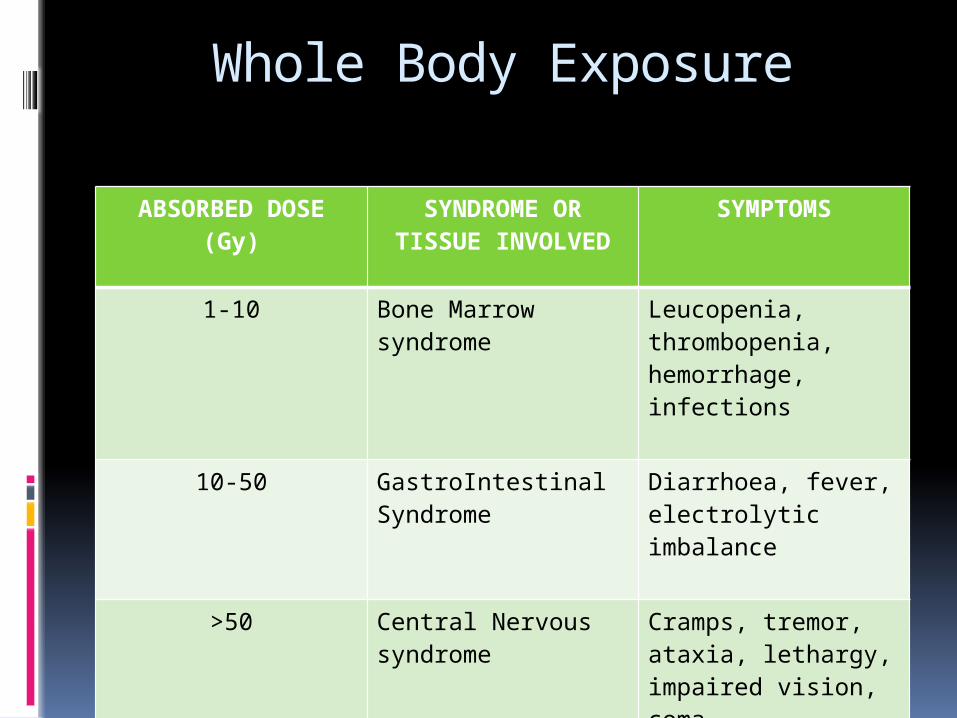
Whole Body Exposure
ABSORBED DOSE (Gy)
SYNDROME OR TISSUE INVOLVED
SYMPTOMS
1-10 Bone Marrow syndrome
Leucopenia, thrombopenia, hemorrhage, infections
10-50 GastroIntestinal Syndrome
Diarrhoea, fever, electrolytic imbalance
>50 Central Nervous syndrome
Cramps, tremor, ataxia, lethargy, impaired vision, coma
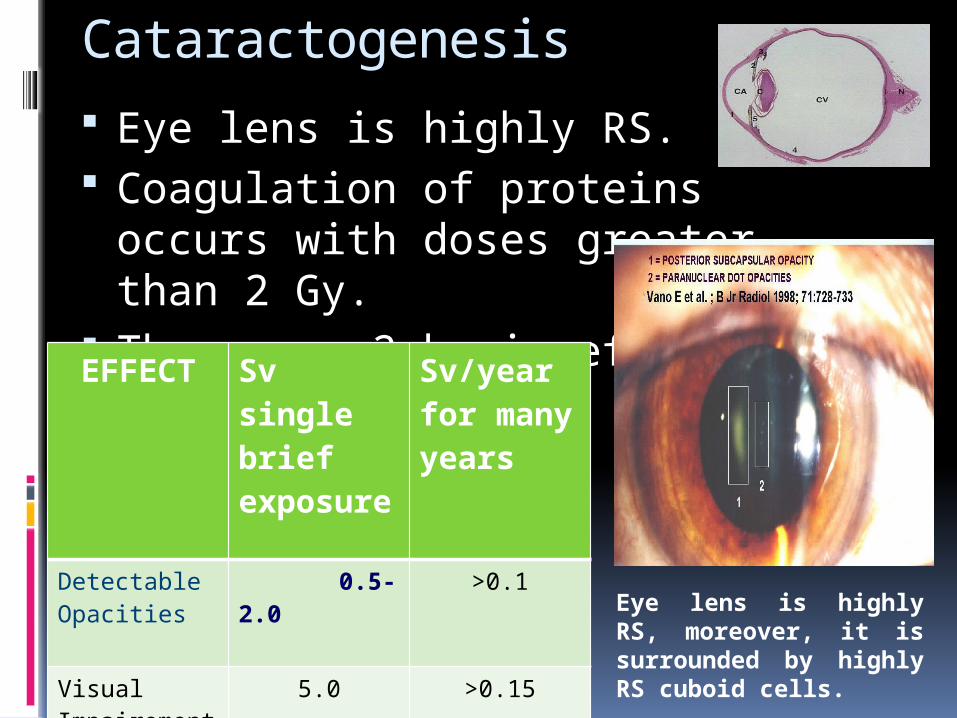
Cataractogenesis
Eye lens is highly RS. Coagulation of proteins occurs
with doses greater than 2 Gy. There are 2 basic effects:
EFFECT Sv single brief exposure
Sv/year for many years
Detectable Opacities
0.5-2.0 >0.1
Visual Impairement(Catarct)
5.0 >0.15
Eye lens is highly RS, moreover, it is surrounded by highly RS cuboid cells.
OTHER ORGAN RELATED DAMAGE In general the viscera exhibits relative radioresistance. Usually the connective tissue and vasculature become the limiting structures, but functional damage can result from high doses.
Lung: Radiation pneumonitis, an acute inflammatory reaction of the functional tissue and vasculature with doses of several thousands centigray after 4 to 6 months.
Lung: Radiation fibrosis, accumulation of fibrin in alveoli and septa, 6 months to years after high doses.
Blood vessels: Hemorrhage followed by progressive thickening and proliferation of endotelial cells known as obliterative endarteritis.
Kidney: Nephrosclerosis, nephritis, hypertension, and renal failure 2 to 3 years after doses of 30 Gy.
EFFECTS ON EMBRYOGENESIS EARLY CONCEPTUS:-Preimplantation - “All or none” - In the human, implantation of the zygote in
the wall of the uterus occurs at approximately days 10 to 12 following conception. Radiation delivered exclusively during this stage may cause prenatal death with failure of implantation; otherwise a normal pregnancy ensues.
-Implantation - Transient Intrauterine Growth Retardation; threshold 10-20 cGy
-
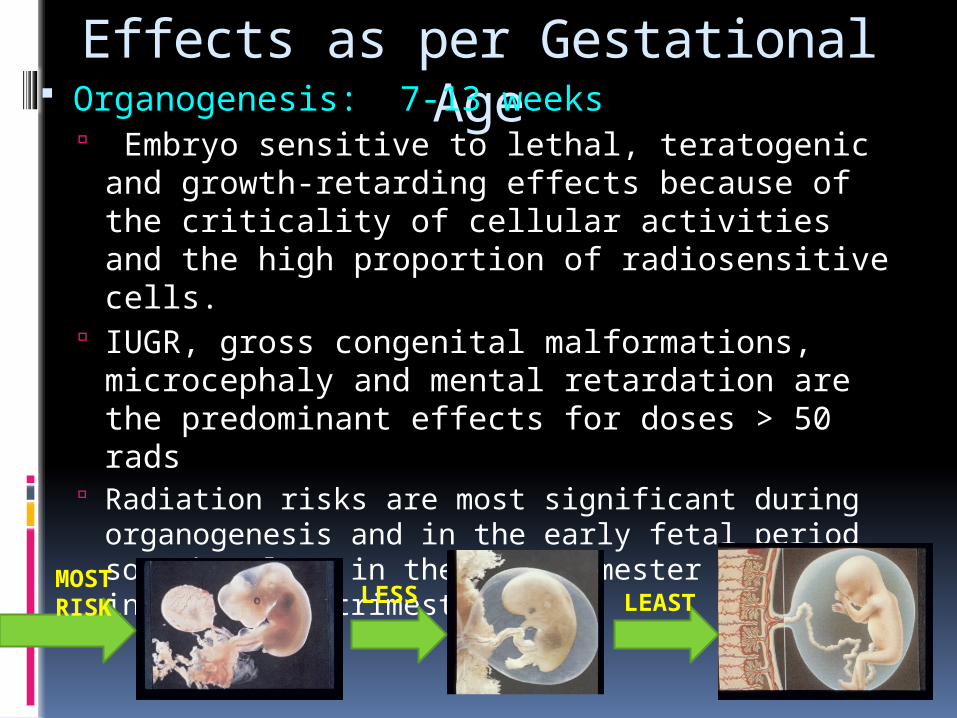
Effects as per Gestational Age Organogenesis: 7-13 weeks
Embryo sensitive to lethal, teratogenic and growth-retarding effects because of the criticality of cellular activities and the high proportion of radiosensitive cells.
IUGR, gross congenital malformations, microcephaly and mental retardation are the predominant effects for doses > 50 rads
Radiation risks are most significant during organogenesis and in the early fetal period somewhat less in the 2nd trimester and least in the third trimesterMOST
RISK LESS
LEAST
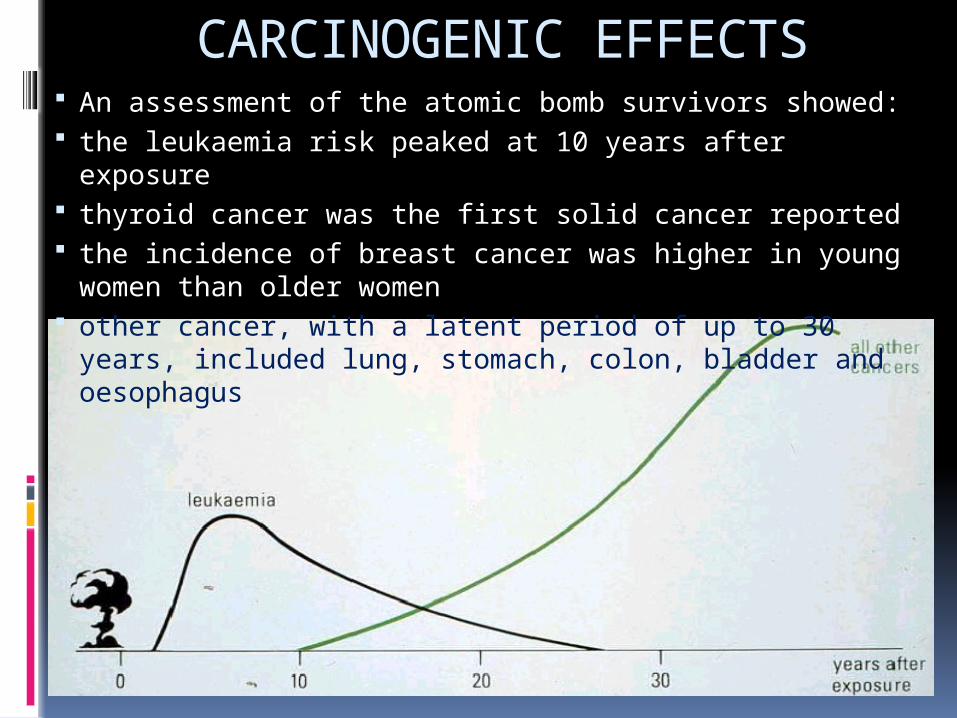
CARCINOGENIC EFFECTS An assessment of the atomic bomb survivors showed: the leukaemia risk peaked at 10 years after exposure thyroid cancer was the first solid cancer reported the incidence of breast cancer was higher in young
women than older women other cancer, with a latent period of up to 30 years,
included lung, stomach, colon, bladder and oesophagus
THANK YOU