Embed Size (px)
Citation preview
A818 AGA ABSTRACTS GASTROENTEROLOGY, Vol. 108, No. 4
• EFFICACY AND TOLERANCE OF MESALAZINE suPPOSITORIES (PENTASA®, If/D) VS. HYDROCORTISONE FOAM (COLOFOAM®, 100 rag/D) IN CRYPTOGENETIC PROCTITIS: A RANDOMIZED PARALLEL OPEN STUDY. 13. Filocl~e. Ph, Marteau, M. Foucault, B. Vautrin. Free University. Lille & Ferring SA Laboratory, Gentilly, France.
iALva: To compare the efficacy and tolerance of Pentasa® suppositories vs Col0foam® in cryptogenetic proctitis. Patients and methods: 252 patients with active cryptogenetic proctitis (disease extent < reetosigmoid junction) were randomized to receive once dally either 1 Pentasa® suppository (lg) or 100rag hydrocortisone (Colofoam®) for 14-21 days (till remission). Disease activity was assessed and followed at dO, d14, and d21 (when remission was not achieved at d14) on a) a dally questionnaire quotating the presence of blood i n stools, mucous in stools, abdominal or rectal pain, b) physician assessment c) endoscopical examination. Local and general tolerance of the treatments was assessed by mean of a questionnaire and by report of adverse events. Results: Both groups did not differ for age (39 + 13 yr. vs 41 + 16 for Pentasa® and Colofoam® respectively), symptoms, endoscopic score, and duration of the actual episode. 21 patients dropped out, and the questionnaires were filled by 210 of the remaining. Both treatments induced a significant decline in disease activity. Pentasa® suppository treatment was significantly more effective than Colofoam® on blood (p=0.002) and mucous (1o=0.02) parameters. Endoscopic score was signifieuntly decreased in both groups but there was no significant difference between groups. No significant difference was observed concerning the tolerance of both treatments. Conclusion: Pentasa® suppositories were equally tolerated and more efficient in clinical symptoms of cryptogenetic proctitis than a 100mg hydrocortisone foam. References: 1) W!lloughby CP, Campieri M, Lanfranchi GA, Truelove SC, Jewel D. 5-ASA (Pentasa®) in enema for the treatment of ulcerative colitis. Ital J Gastroenterol 1986,18:15-17.
• SYSTEMIC INFLAMMATORY CYTOKINES INDUCED BY ACUTE PANCREATITIS ORIGINATE WITHIN THE PANCREAS Gre~ Fink. Michael Franz, James Norman. Department of Surgery, University of South Florida. Tampa, Florida.
Systemic eytokine levels have been shown to correlate with the severity of aente pancreatitis in humans mad expetimental animals yet the site of their production has not been established. Tbe curt'eat study wes designed to determine intrapancreatic eytokine levels and to establish the role of the inflamed pancreas in the production of these mediators.
Acute neerotizing pancreatitis was induced in adult male NIH Swiss mice by the administration ofeaemlein (50pg/kghar IP x 4). Control animals received IP saline. Twelve animals were sacrificed at 0 1 2 4 6 and 8 hours after induction ofpancreatitis with the sevetity ofpanematitis established by histologie grading and serum arnylase and lipase. IL-1, IL-6, and TNF-c~ were quantitatcd in serum and pancreatic tissue by ELISA and immtmohistochemistry. Intrapanereatie cytokine mRNA was established by rtPCR.
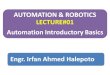
Pancreatilis developed within one hOur ofeaerdein injection and peaked at Six hours as evidenced by histologic scoring and elevations in amylase and lipase (both p<0.001 compared to Control). There was no detectable eytokine mRNA or protein within the pancrealh or serum of Control animals at any lime point. One hour after onset ofpancreatitis, mRNA for TNF-¢ was detectable within the pancreas, with IL-I and IL-6 mRNA appearing 1 and 2 hours later, respectively. This was associated with elevation of serum and intrapancreatie IL-1, IL-6, and TNF-¢ (both p<0.001 compared to Control) with in~rapanereatie levels of all three eytokines increasing faster and sustaining concentrations several fold higher than time matched serum levels '(all intrapancreati¢ levels' greater than
I k - 1 I L - 6 . T N F . . . . . . . . . . . . . . . . . . . . . . ; . ; ~ z ~ - -.- . . . . . . . . - _- ~ L - ~ - - _ - - - - . _ 7 - - - ~
-e ~ ' 2 0 ' - ~ . . . . . . . . . . . . . . . . . . . . . . ~,~;,~'-
e*e . . . . . . . , . . . . . -¢~,- : ) o o ~ . . . . . -"
o O l e $ 4 s e 7 e o 1 2 3 t s e 7 e o 1 a = 4 s 1 r •
H o u r i H o u r i H o u r i
senm~ p<0.05), Inmmnohistochemiea] s~dning demonstrated a progn~ssive ir~filffation of leukoeytes into the pancreas which stained for all three cytokines, but were absent at time zero and in all Control ainnmls. Antibody staining directed against the CDI4 myeloid differentiation antigen identified nearly all of the eylokine secreting inflammatory cells as macrophages.
We conclude that the pancreas is a primzay site of inflammatory cytokine production during acute pancreatitis with the infiltrating macroplmge contributing significantly to this process. Importantly, intrapancrcefie levels nflL-l, IL-6, and TNF-a exceed systemic levels at al! time points and correlate directly with the severity oftbe disease.
• ANTINEUTROPHIL CYTOPLASMIC ANTIBODIES (ANCA) AND INDETERMINATE COLITIS. IS THERE AN ASSOCIATION? P.R. Fleshner, L. Weston, S.E. Plevy, C.J. Landers, DJ. Schoetz, Jr., S.R. Targan. Division of Colorectal Surgery and the Inflammatory Bowel Disease Center, Cedars-Sina~ Medical Center, Los Angeles CA, andthe Deparlment of Colorectal Surgery; Lahey Clinic, Burlington MA
Although a distinct subset of ANCA has been commonly observed in ulcerative colitis (UC), the association between indeterminate colitis (IC) and ANCA is unknown. ANCA was retrospectively measured in the sera of patients who had undergone ileoanal pullthrough at two Inflammatory Bowel Disease Centers. ANCA was measured by fixed neutrophil ELISA at a 1:100 serum dilutio n greater than 2 standard deviations above the mean of the control group, of the 23 study group patients, 16 were male, and the mean age was 38 years. Eleven patients hadUC while l~il~atients had IC. The diagnosis of IC was based on macroscopic or micr'6scopic transmural inflammation (n=7), fistulization (n=2), terminal ileal inflammation extending beyond 3 cm from the ileocecal valve (n=2), and linear 'rake' ulceration (n=l). ANCA was expressed in 10 of the l lUC patients (89%) compared to only 6 of the 12 IC patients (50%) (p=0:03). Tefi of the 16 (63%) ANCA+ patients had UC while 6 (37%)ANCA+ patients had IC. The mean antibody titre in the ANCA+ UC patient group was 368 + 82 ng/ml compared to 814 + 177 in the IC patient group (p=0.02). Of the 7 ANCA- patients, 6 (86%) had IC and 1 (14%) had~ldC. Although IC patients have a significantly lower incidence of ANCA expresslon than UC patients, antibody titres in those IC patients who have ANCA are significantly higher than in the UC patients who express ANCA. These data suggest that IC may be a heterogeneous disease which could be better defined by the presence or absence of ANCA. Additionally, the high incidence of ANCA positive UC patients (89%) in this surgically treated series further points to ANCA as a predictor of aggressive disease as previously shown for left-sided UC (Sandbom WJ; et al. Gastroenterology 1994;106(4):A766) and post ileoanal pullthrough pouchitis (Sandborn WJ, et al. Gastroenterology 1993;104(4):A774)~ Future studies using larger populations 0f patients will further Correlate ANCA status to clinical phenotype and perhaps lead to improved definition and clinical management 0f IC~ Supported by USPHS Grant Nos. DK43026& DK46763.
CROHN'S DISEASE (CD) WITH GRANULOMAS IN THE UPPER GASTROINTESTINAL TRACT (UGIT) MUCOSAo H.J .Freeman. Dept. of Medicine, University oflBritish Columbia, Vancouver, BC, Canada.
Oastroduodenal abnormalities occur in C D . A group of 25 patients diagnosed with CD from 1981 ~o 1993 with granulomatous disease in the UGIT mucosa were reviewed. To :evaluate a "reagent-grade" group, CD patients with gastroduodenal changes (eg., ulcers) were excluded if no UGI T granulomas were seen. There were 13 males and 12 females, ages 15 to 60 years with a mean age of 34 years, at the time that U GIT disease was diagnosed. In 7, disease was :only in the UGIT: 1 with granulomatous oropharyngeal disease (GOP)a lone , 5 with granulomatous gastritis (GG) alone, 1 with granulomatous duodenitis (GD) alone. In 5, disease was concurrently diagnosed in the upper and lower gastrointestinal tracts. In 1, GOP was detected 1 year prior to diagnosis of lower gastrointestinal tract disease: In 12, U G I T disease was detected after disease was detected in the ileum and/or colon: 5 w i t h GG alone, 4 with GD alone, 2 with both GG and GD, 1 with GOP alone. Upper abdominal pain was most c o m m o n (over 90%). Weight loss (over 50%), nausea and vomiting (over 30%) were also seen and, occasionally, UGIT bleeding (2 patients) occured. Endoscopic features included erosions, thickened folds, ulceration, granularity, nodularity and cobblestoning. The most common radiographic change was mucosal thickening but barium studies were most often normal Mean follow- up is 5.4 years (range, 1 to 11 years). Only 2 patients have required Surgical treatment for UG! T disease. CD in the UGIT with mueosal granulomas has an apparentiy benign initial clinical course.